

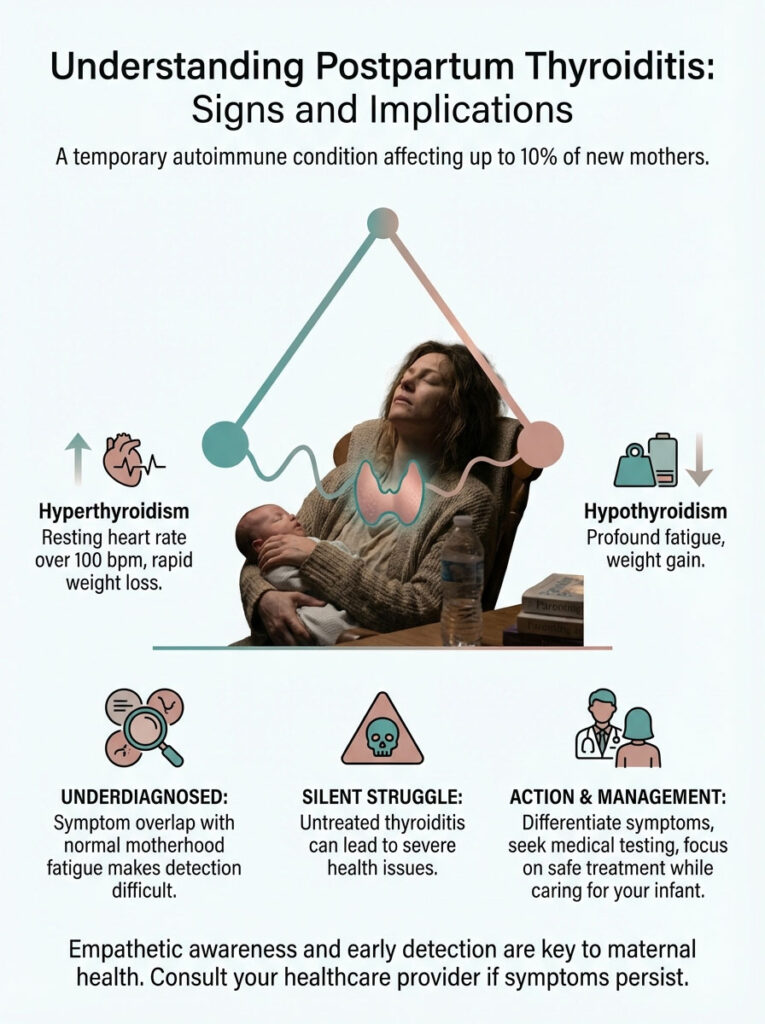
While exhaustion is standard for new mothers, postpartum thyroiditis is a specific medical condition affecting up to 10% of women. It involves a temporary autoimmune attack on the thyroid gland. This causes a swing from high energy and anxiety (hyperthyroidism) to profound lethargy and depression (hypothyroidism). If your resting heart rate is over 100 bpm, you are losing weight rapidly, or your fatigue feels “bone-deep” despite sleep, you need a TSH panel. Do not dismiss this as normal tiredness.
Table of Contents
You are standing in the kitchen at 3 AM. You are rocking a newborn. You feel a level of exhaustion that seems to vibrate in your bones. Everyone told you that the “fourth trimester” would be tiring. They told you about the sleepless nights. They warned you about the physical recovery. But for many of my patients, what they are experiencing isn’t just the standard fatigue of new motherhood. It is a physiological storm taking place inside their endocrine system.
This battle is often silent. It is frequently dismissed. Yet, distinguishing postpartum fatigue vs thyroid dysfunction is one of the most critical steps in protecting a new mother’s health.
Postpartum thyroiditis is a destructive autoimmune inflammation of the thyroid gland. It occurs in the first year after delivery. It is the most common form of thyroid dysfunction in the postpartum period. Yet, it remains one of the most underdiagnosed conditions in obstetrics and endocrinology.
Why is it missed so often? Because its symptoms are the perfect masquerade. The anxiety and palpitations of the first phase mimic the stress of caring for a newborn. The lethargy and brain fog of the second phase look exactly like postpartum depression or simple sleep deprivation. We call this “silent thyroiditis” because it destroys thyroid cells without pain. It often leaves a mother struggling to function while her symptoms are dismissed as “just part of being a mom.”
This is not a failure of your coping skills. This is a medical condition. As an endocrinologist, I have seen untreated thyroid dysfunction lead to breastfeeding failure. I have seen it cause severe mood disorders. I have seen it result in long-term cardiovascular stress. In this comprehensive guide, we will examine the biphasic nature of this condition. We will look at how to interpret your thyroid levels after pregnancy. We will also discuss how to manage treatment safely while caring for your infant.
Key Statistics: Postpartum Thyroiditis
- Prevalence: Affects approximately 5% to 10% of all postpartum women in the USA.
- Recurrence: If you have it once, there is a 70% chance it will recur in future pregnancies.
- Antibody Risk: Women with positive TPO antibodies in the first trimester have a 33% to 50% chance of developing it.
- Long-Term Risk: About 20% to 30% of women will develop permanent hypothyroidism.
- Diabetes Link: Women with Type 1 Diabetes have a 3-fold increased risk.
The Immunology of Pregnancy: The Setup
To understand why your thyroid might turn against you after birth, we have to look at the immunology of pregnancy. During gestation, your body performs a biological miracle. It suppresses your immune system just enough to prevent it from rejecting the fetus. The fetus carries foreign genetic material from the father. Your body knows this.

Your immune system essentially calls a truce. This immune suppression is why many women with autoimmune diseases, like Rheumatoid Arthritis or Hashimoto’s, actually feel better during pregnancy. The attack on their own tissues slows down. However, once the placenta is delivered, that suppression lifts rapidly.
This is the “Immune Rebound.”
The immune system wakes up. It surges back to full strength. Sometimes, it comes back with too much aggression. In women who are genetically susceptible, this rebound triggers an attack on the thyroid gland. This is particularly common in women who carry TPO antibodies pregnancy screenings might have missed if they weren’t specifically requested.
The presence of Thyroid Peroxidase Antibodies (TPOAb) indicates that your immune system has already tagged the thyroid as a target. The massive hormonal shift of delivery is simply the trigger that launches the attack.
The Role of Microchimerism
There is another fascinating factor at play. It is called fetal microchimerism. During pregnancy, cells from the fetus cross the placenta into the mother’s bloodstream. These cells can persist in the mother’s body for years. Usually, they are harmless. Sometimes, they even help repair tissue.
However, in some women, these fetal cells accumulate in the thyroid gland. When the immune system reboots after birth, it spots these “foreign” cells in the thyroid. It launches an attack. The thyroid tissue becomes collateral damage in this immune war. This explains why the condition is specific to the postpartum period.
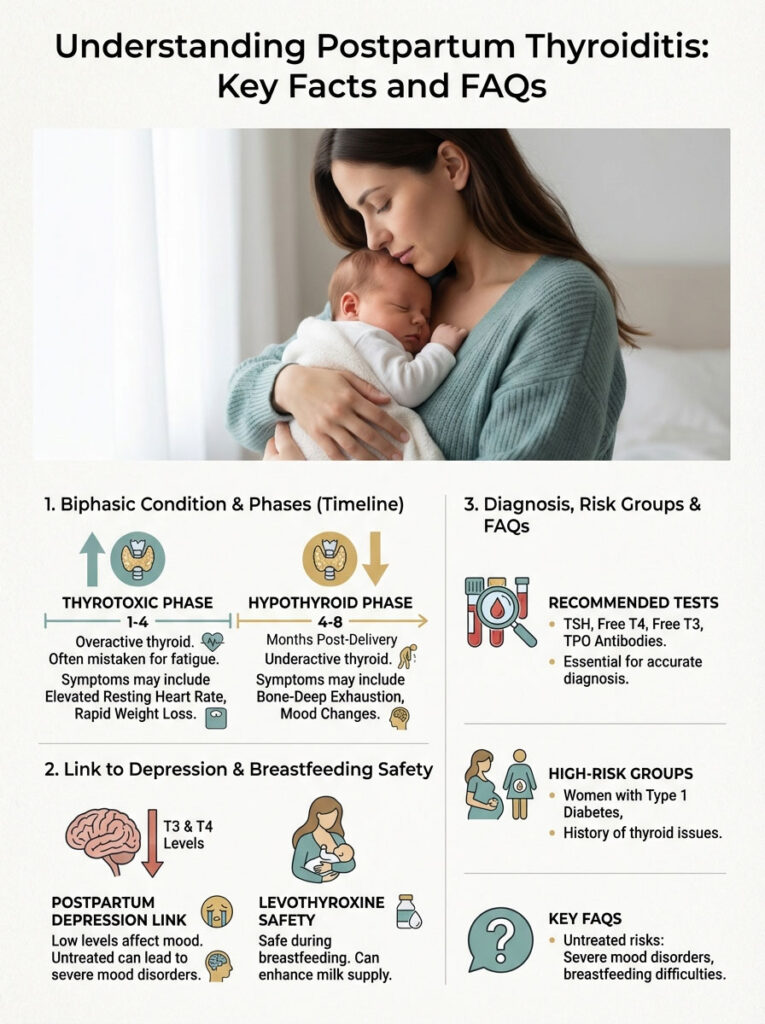
The Biphasic Timeline: A Rollercoaster of Hormones
Thyroid disorders usually pick a lane. Hashimoto’s is typically low thyroid. Graves’ disease is typically high thyroid. Postpartum thyroiditis is unique because it is often “biphasic.” This means it has two distinct phases. It swings from one extreme to the other.
Understanding this timeline is vital. It is the only way to recognize the difference between standard postpartum fatigue vs thyroid dysfunction. If you treat the first phase like the second phase, you can make the patient significantly worse.
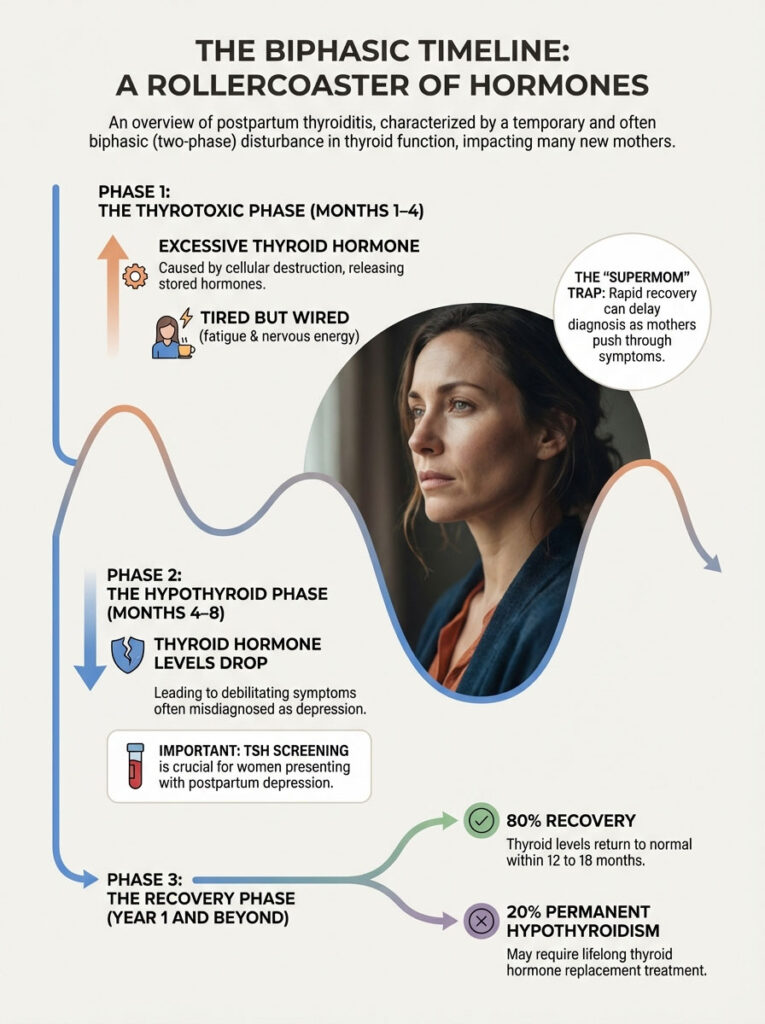
Phase 1: The Thyrotoxic Phase (Months 1–4)
This phase usually occurs between 1 and 4 months postpartum. It is characterized by an excess of thyroid hormone in the blood. However, the mechanism is distinct from other disorders. In standard hyperthyroidism, the gland creates too much hormone. In postpartum thyroiditis, the inflammation destroys the thyroid cells. This causes them to leak their stored hormone into the bloodstream.
We call this “destructive thyrotoxicosis.”
Imagine a warehouse full of energy drinks. Standard hyperthyroidism is the factory producing drinks too fast. Postpartum thyroiditis is an earthquake that breaks the warehouse walls, spilling all the existing inventory into the street at once.
Clinical Presentation: You might feel “tired but wired.” You are exhausted. But when the baby sleeps, you stare at the ceiling with a racing heart. Common postpartum hyperthyroidism symptoms include:
- Rapid, unexplained weight loss (dropping below pre-pregnancy weight quickly).
- Anxiety, irritability, and nervousness.
- Heat intolerance and excessive sweating.
- Tremors in the hands.
- Insomnia that isn’t related to the baby’s schedule.
- Muscle weakness, specifically in the upper arms and thighs.
The “Supermom” trap happens here. Because of the excess thyroid hormone, some mothers have boundless, nervous energy. They clean the house at midnight. They bounce back into their pre-pregnancy jeans instantly. Family and friends might compliment this rapid recovery. This delays the diagnosis until the crash comes.
Phase 2: The Hypothyroid Phase (Months 4–8)
Eventually, the warehouse empties. The thyroid runs out of stored hormone. Because the cells have been damaged by the immune attack, they cannot produce enough new hormone to meet the body’s demands. You swing from high to low.
Clinical Presentation: This is where postpartum hypothyroidism sets in. The symptoms are often severe. They are debilitating. They are frequently misdiagnosed as depression.
- Profound lethargy (naps do not refresh you).
- Inability to lose weight, or sudden weight gain despite breastfeeding.
- Severe constipation.
- Dry skin and significant postpartum hair loss thyroid issues.
- Sensitivity to cold (wearing sweaters when others are warm).
- Depression, apathy, and “brain fog.”
- Puffy face and water retention.
Endocrinologist’s Note: The American Thyroid Association (ATA) recommends that any woman presenting with Postpartum Depression (PPD) should be screened for TSH abnormalities. The overlap between low thyroid function and depression is substantial. Correcting the hormone imbalance can sometimes resolve the mood disorder completely.
Phase 3: The Recovery Phase (Year 1 and Beyond)
The good news is that the thyroid is a resilient organ. In approximately 80% of cases, the gland heals. Thyroid levels return to normal (euthyroid) within 12 to 18 months. The inflammation subsides. The cells regenerate. Production resumes.
However, for the remaining 20%, the damage is too severe. This leads to permanent hypothyroidism. These women will require lifelong medication. We will discuss risk factors for this permanent damage later in this guide.
Detailed Symptom Analysis: Is It Fatigue, Blues, or Thyroid?
Distinguishing between normal “new mom” exhaustion and a medical crisis is difficult. Our culture normalizes extreme fatigue in mothers. We tell women that feeling terrible is part of the job. This is dangerous advice.
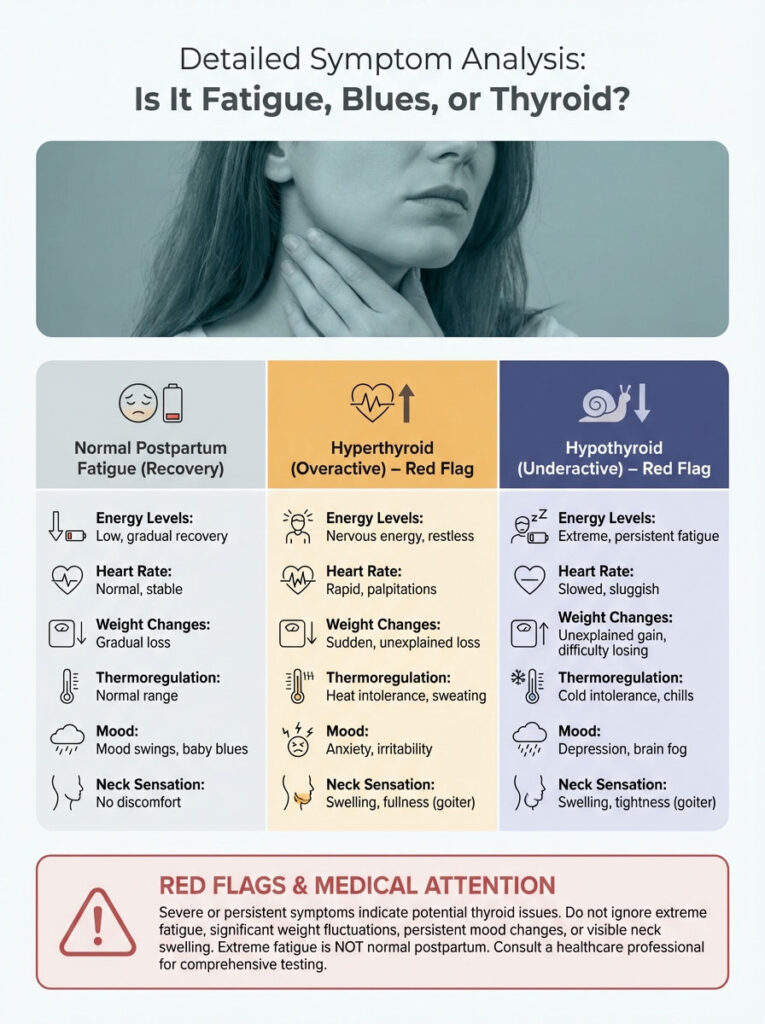
There are specific red flags. Normal fatigue improves when you get a chance to sleep. Thyroid fatigue does not. Normal weight loss is gradual. Thyroid weight loss is rapid and scary. Normal hair loss is diffuse. Thyroid hair loss comes out in clumps.
Below is a comparison to help you distinguish postpartum fatigue vs thyroid issues.
| Feature | Normal Postpartum Fatigue | PPT (Hyper Phase) | PPT (Hypo Phase) |
|---|---|---|---|
| Energy Level | Tired but functional after rest | “Tired but wired,” restless energy | Bone-deep exhaustion, naps don’t help |
| Heart Rate | Normal (60–80 bpm) | Tachycardia (>100 bpm) at rest | Bradycardia (slow heart rate) |
| Weight | Gradual loss or stability | Rapid, unexplained weight loss | Weight gain or inability to lose weight |
| Thermoregulation | Normal | Heat intolerance, sweating | Cold intolerance, chills |
| Mood | “Baby Blues” (mild, transient) | Severe anxiety, panic attacks | Depression, brain fog, apathy |
| Neck Sensation | Normal | Painless fullness (Goiter) | Painless fullness (Goiter) |
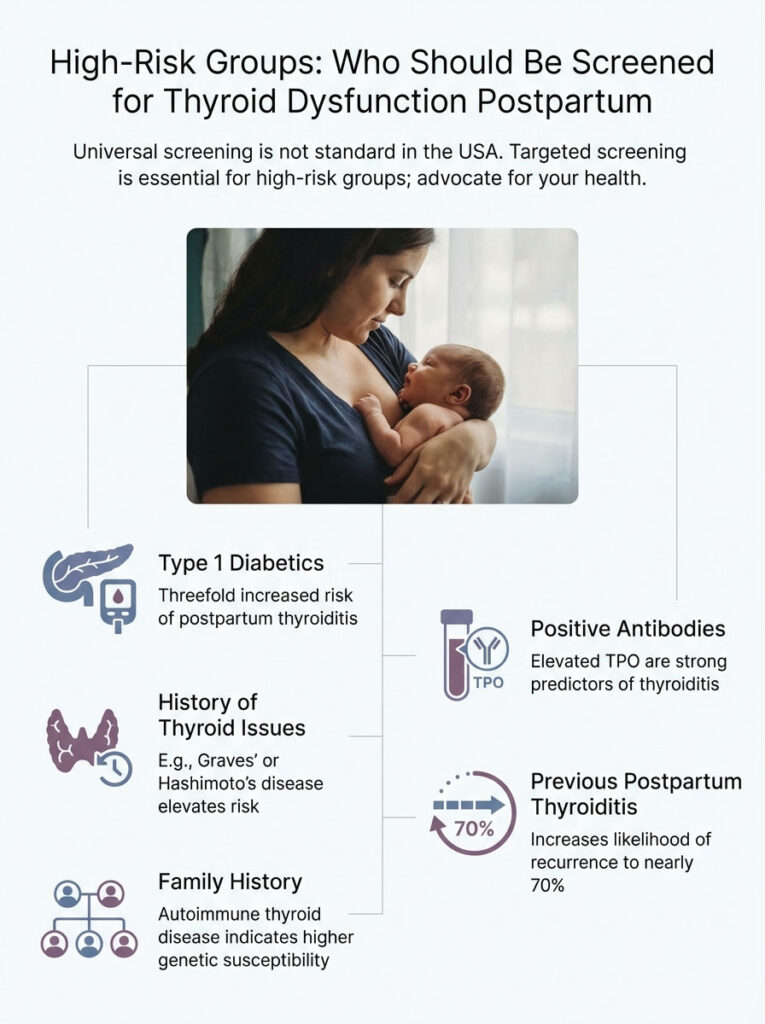
High-Risk Groups: Who Should Be Screened?
Currently, universal screening for thyroid dysfunction is not standard practice in the USA. This is largely due to cost-benefit debates in the medical community. This means the burden often falls on the patient to advocate for testing. You must be your own health advocate.
However, targeted screening is absolutely vital for high-risk groups. The American Thyroid Association has identified specific populations that warrant closer monitoring. If you fall into any of the following categories, you should request a check of your thyroid levels after pregnancy. This should happen at 6 weeks and 3 months postpartum.
Type 1 Diabetics
Because autoimmune diseases cluster together, women with T1D have a significantly higher risk. The risk of developing postpartum thyroiditis is three times higher in this group. The immune system is already prone to attacking endocrine organs. The thyroid is simply the next target.
History of Thyroid Issues
If you have a history of Graves’ disease, you are at risk. If you have Hashimoto’s thyroiditis, you are at risk. Even if your Hashimoto’s was “mild” before pregnancy, the immune rebound can cause a severe flare. This can temporarily swing you into a hyperthyroid state before crashing you back down.
Family History
Genetics play a massive role here. If your mother, sister, or aunt had autoimmune thyroid disease, tell your obstetrician. Autoimmunity runs in families, even if the specific organ targeted varies.
Positive Antibodies
This is the strongest predictor. If you were found to have elevated TPO antibodies pregnancy screening, your risk is high. Up to 50% of women with these antibodies in the first trimester will develop thyroiditis postpartum.
Previous PPT
Did you have this condition with a previous child? If so, your risk of recurrence is nearly 70%. Your medical chart should have a flag for postpartum thyroid screening the moment you confirm a new pregnancy.
Diagnosing Postpartum Thyroiditis: The Lab Panel
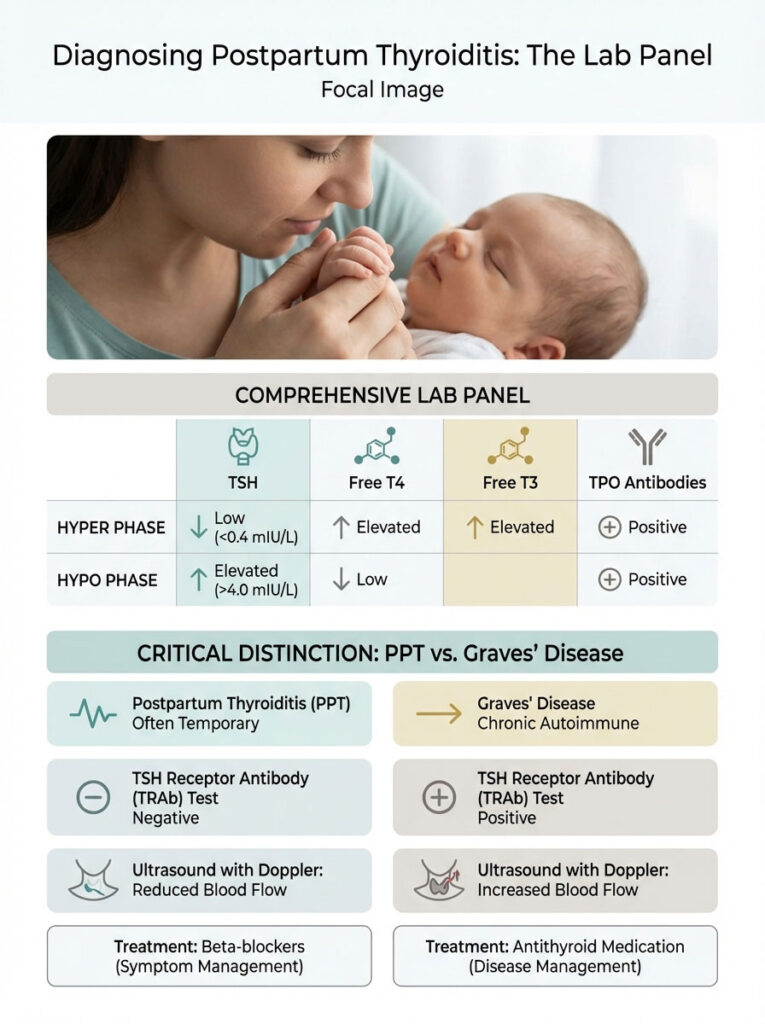
Diagnosis requires more than just a TSH test. A TSH test alone can be misleading in the early stages. We need a full picture of the thyroid’s function. We need to see the immune system’s activity. The gold standard panel includes TSH, Free T4, Free T3, and TPO Antibodies.
Interpreting TSH levels postpartum can be tricky. It depends entirely on which phase you are in.
The “Hyper” Labs
In the first phase, your TSH will be suppressed. It will likely be less than 0.4 mIU/L. Your Free T4 and Free T3 will be elevated. This looks exactly like Graves’ disease on paper. However, the treatment is completely different. This is why further testing is required.
The “Hypo” Labs
In the second phase, your TSH will rise. It acts as a scream for help from the pituitary gland. Levels may exceed 4.0 mIU/L or even go much higher. Your Free T4 will be low. This indicates the gland is failing to produce hormone.
The Critical Differential: PPT vs. Graves’ Disease
This is perhaps the most important distinction an endocrinologist must make. If a woman presents with high thyroid levels (hyperthyroidism) three months postpartum, is it postpartum thyroiditis? Or is it the onset of Graves’ disease?
The distinction saves lives. It also protects breastfeeding. Graves’ disease requires antithyroid medication (like Methimazole). Postpartum thyroiditis does not. In PPT, the gland isn’t overproducing; it’s leaking. Giving Methimazole to a woman with PPT is useless. It does not stop the leak. It can also be harmful by pushing her into hypothyroidism faster.
To tell them apart, we use the TSH Receptor Antibody (TRAb) test. If TRAb is positive, it is likely Graves’. If negative, it is likely PPT. We may also use an ultrasound with Doppler flow. In Graves’, blood flow is increased. We call this a “thyroid inferno.” In PPT, blood flow is decreased due to the inflammation.
| Diagnostic Marker | Postpartum Thyroiditis | Graves’ Disease |
|---|---|---|
| Pathology | Destructive inflammation (Leakage) | Overproduction (Hyperthyroidism) |
| Duration | Temporary (Transient) | Chronic / Progressive |
| TRAb Antibodies | Negative | Positive (90-95% of cases) |
| Thyroid Ultrasound | Decreased blood flow | Increased blood flow (“Thyroid Inferno”) |
| Treatment | Beta-blockers (Symptom management) | Methimazole or PTU (Antithyroid drugs) |
Treatment Protocols: An Endocrinologist’s Perspective
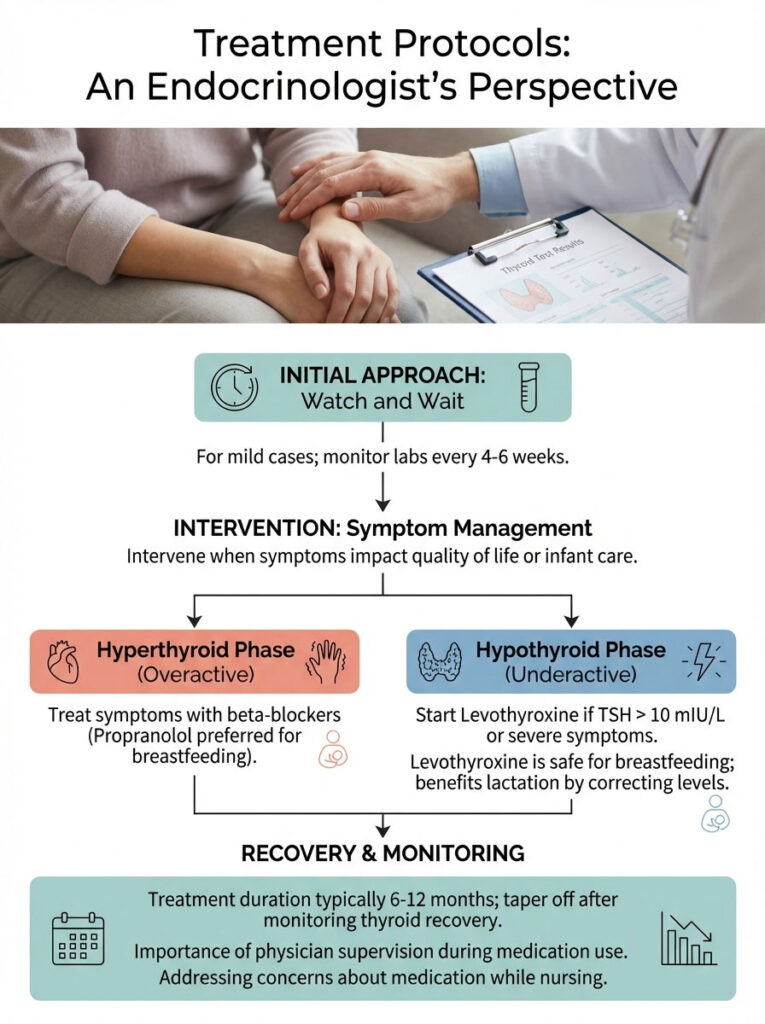
We often adopt a “watch and wait” approach for mild cases. We monitor labs every 4 to 6 weeks. However, treatment is necessary when symptoms impact the mother’s quality of life. If you cannot care for your infant safely, we intervene.
Managing the Hyperthyroid Phase
As mentioned, we do not use antithyroid drugs here. Instead, we treat the symptoms. If a mother is suffering from severe palpitations, tremors, or anxiety, we may prescribe beta-blockers. These drugs slow the heart rate. They reduce the “wired” feeling.
Breastfeeding Safety: Propranolol is the preferred beta-blocker for nursing mothers. It is highly protein-bound. This means very little of it passes into breast milk. It is generally considered safe for the infant when monitored by a physician.
Managing the Hypothyroid Phase
When the crash happens and postpartum hypothyroidism sets in, the treatment changes. We often need to supplement with thyroid hormone replacement (Levothyroxine). We typically start treatment if TSH exceeds 10 mIU/L. We also treat if it is between 4 and 10 mIU/L with severe symptoms. If the mother is attempting to conceive again, we treat aggressively to ensure fertility.
Levothyroxine Breastfeeding Safety: Many mothers worry about taking medication while nursing. Please rest assured. Levothyroxine breastfeeding safety is well-established. According to LactMed and the American College of Obstetricians and Gynecologists (ACOG), thyroid hormone passes into breast milk in incredibly small amounts. Furthermore, it is identical to the hormone your baby already produces. Correcting your thyroid levels is actually beneficial for lactation. Hypothyroidism can inhibit milk supply by interfering with the let-down reflex.
Treatment Duration: Because silent thyroiditis recovery is likely, we don’t assume you need medication forever. We typically treat for 6 to 12 months. Then, we slowly taper off the medication. We monitor to see if the thyroid gland has recovered its own function.
Holistic Support and Lifestyle Factors
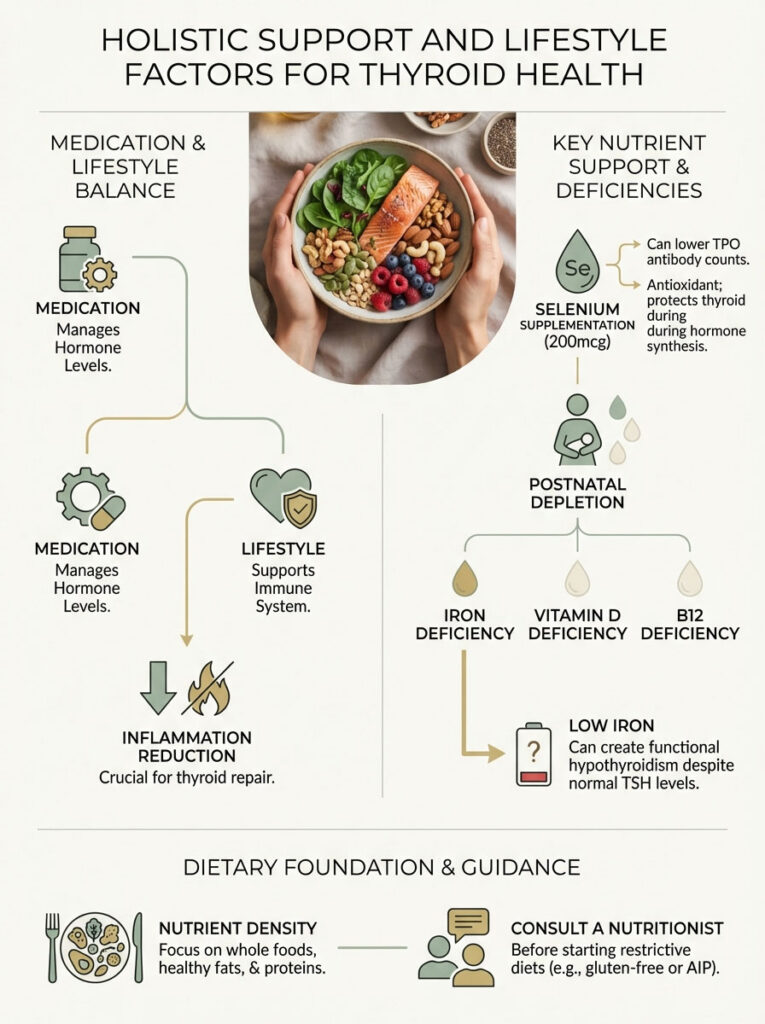
While medication handles the hormone levels, lifestyle factors support the immune system. The goal is to reduce inflammation. We want to support the thyroid gland’s repair process.
Selenium Supplementation
Research regarding Selenium is promising. Some studies suggest that taking 200mcg of Selenium can reduce TPO antibody counts in pregnant and postpartum women. Selenium acts as a shield for the thyroid. It is a powerful antioxidant. It helps neutralize the hydrogen peroxide produced during thyroid hormone synthesis.
You can get this from supplements. You can also get it from food. Eating 2-3 Brazil nuts daily typically provides a sufficient dose. However, do not overdo it. Selenium toxicity is real. Stick to the recommended daily allowance.
Addressing Postnatal Depletion
Pregnancy depletes the body. It drains iron, Vitamin D, and B12 stores. Deficiencies in these nutrients can mimic or exacerbate postpartum fatigue vs thyroid symptoms. Iron deficiency (ferritin) is particularly tricky. Low iron impacts how well your body utilizes thyroid hormone. It creates a “functional” hypothyroidism even if TSH looks okay.
Request a full iron panel, not just a CBC. If your ferritin is below 50 ng/mL, you may need supplementation. This can dramatically improve energy levels.
Dietary Considerations
Many patients ask about the Autoimmune Protocol (AIP) or Gluten-Free diets. There is anecdotal evidence that removing gluten can lower antibodies in Hashimoto’s patients. This is likely due to “molecular mimicry” between gluten proteins and thyroid tissue.
However, I urge caution in the postpartum period. Nursing requires significant caloric intake. Restrictive dieting without medical supervision can hurt milk supply. It can also drain your energy further. Focus on nutrient density first. Eat whole foods, healthy fats, and proteins. If you wish to try a gluten-free diet, do so under the guidance of a nutritionist to ensure you are getting enough calories.
Long-Term Prognosis and Future Pregnancies
While most women recover, the “20% rule” is a serious consideration. Approximately 20% of women will remain hypothyroid permanently. Even if you recover, your thyroid has been scarred. You are at a higher risk of developing overt hypothyroidism 5 to 10 years down the road.
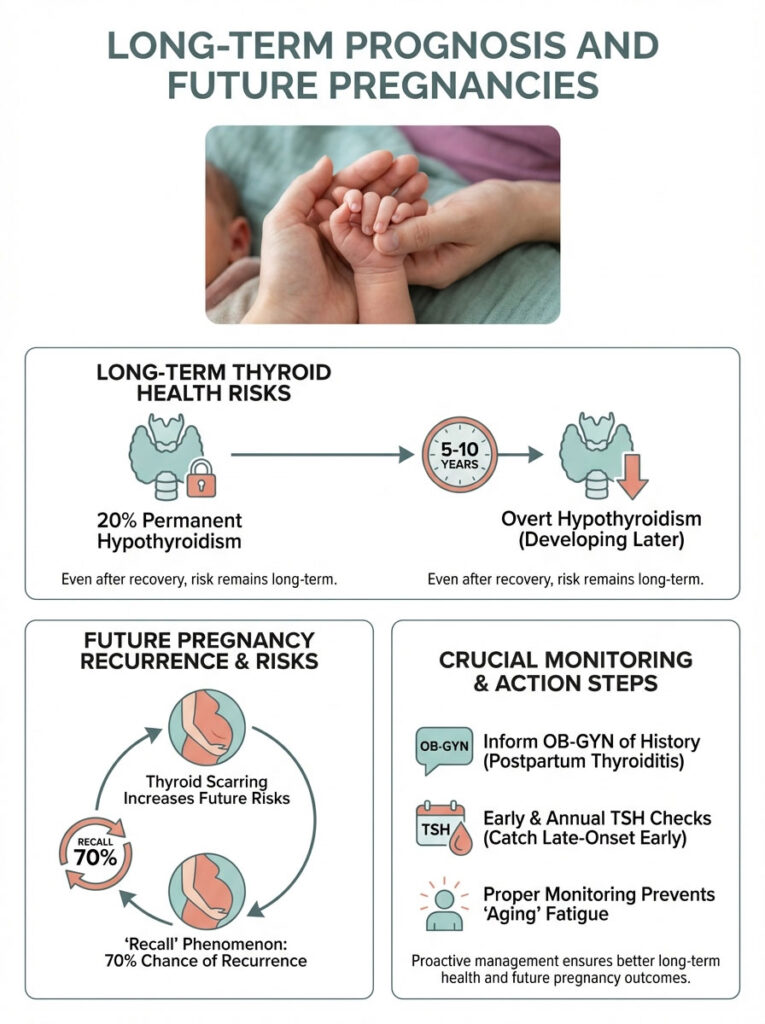
This leads to the “Recall” phenomenon. If you experienced postpartum thyroiditis with your first pregnancy, you have a roughly 70% chance of experiencing it again with subsequent pregnancies. It is vital to inform your OB-GYN of your history as soon as you become pregnant again. They can monitor your TSH early. They can watch for antibody spikes.
Annual monitoring is the best defense. A simple TSH check once a year during your physical is enough. It can catch late-onset hypothyroidism before it affects your health. It prevents the slow slide into fatigue that many women mistakenly attribute to aging.
Mental Health: The Thyroid-Brain Connection
We cannot discuss this condition without addressing mental health. The thyroid hormones T3 and T4 are essential for brain function. They regulate neurotransmitters like serotonin and dopamine. When thyroid levels fluctuate, so does your mental state.
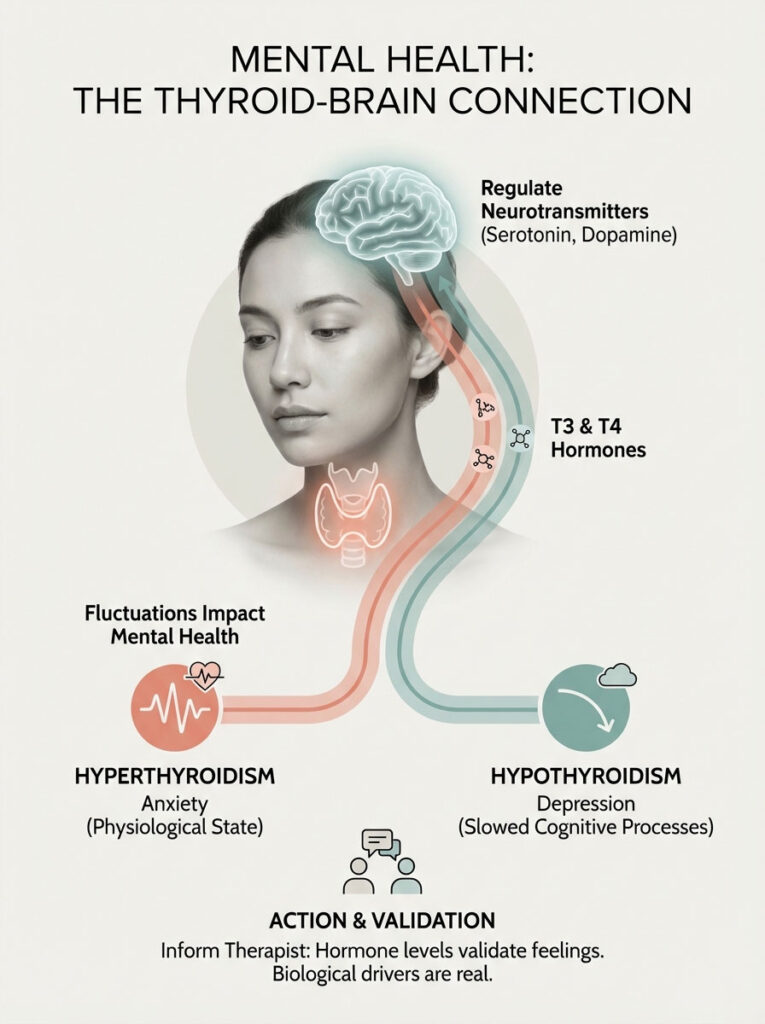
In the hyperthyroid phase, anxiety is chemical. It is not just “new mom worry.” It is a physiological state of fight-or-flight that you cannot think your way out of. In the hypothyroid phase, depression is chemical. It is a slowing down of cognitive processes.
If you are in therapy for PPD, tell your therapist about your thyroid diagnosis. It helps them understand that your symptoms have a biological driver. It validates that you are not “failing” at happiness. You are dealing with a hormonal imbalance.
Navigating the Medical System
Getting a diagnosis can be a struggle. You may face doctors who dismiss your symptoms. They may tell you to “just sleep when the baby sleeps.” Here is how to advocate for yourself.
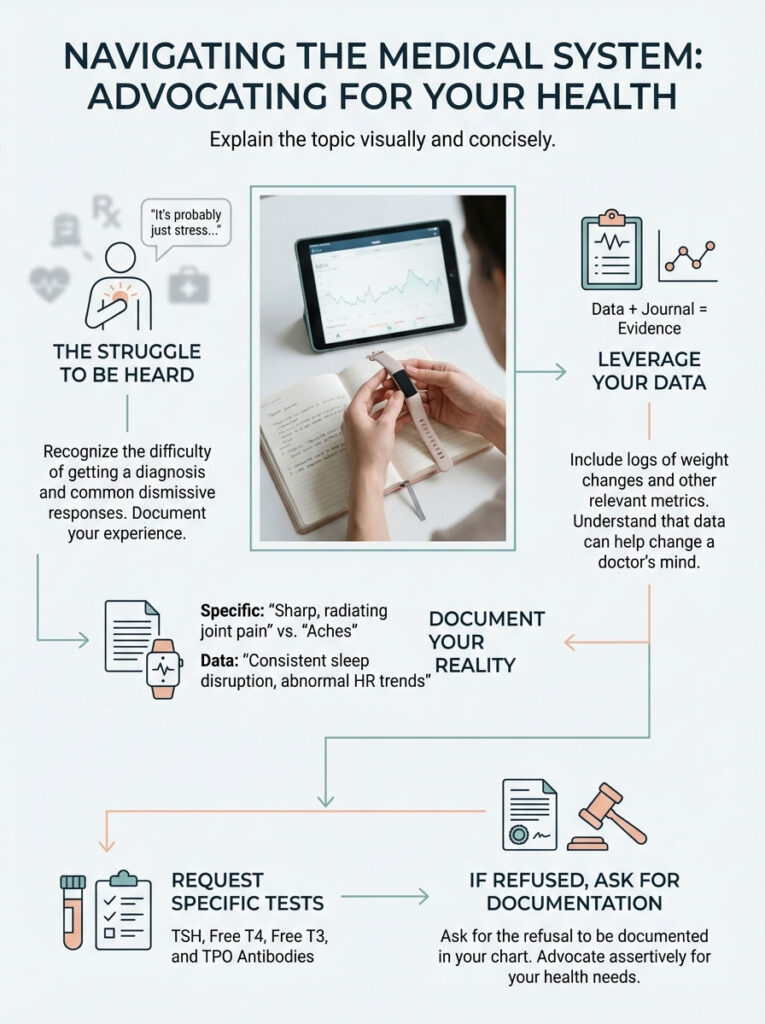
Be specific. Do not just say “I’m tired.” Say “I am falling asleep sitting up.” Say “My hair is falling out in clumps.” Say “My heart rate is 110 while watching TV.”
Bring data. If you have a smartwatch that tracks heart rate, show the doctor the trends. Show them the weight loss or gain log. Data is harder to dismiss than general complaints.
Ask specifically for the tests. Ask for TSH, Free T4, Free T3, and TPO Antibodies. If a doctor refuses, ask them to document their refusal in your chart. This often prompts them to reconsider and order the labs.
Summary & Key Takeaways
Postpartum thyroiditis is a complex, biphasic condition. It affects millions of women. Yet, it remains hidden behind the veil of “normal” new-mom exhaustion. It is a physiological reality, not a psychological failure.
Remember these core points:
- The condition often swings from High (Anxiety/Energy) to Low (Depression/Fatigue).
- Trust your instincts. If the fatigue feels “wrong” or you have physical symptoms like a racing heart or hair loss, push for a TSH, Free T4, and TPO test.
- Treatment is safe. Levothyroxine breastfeeding safety is confirmed by major health organizations. Treating the thyroid often saves the breastfeeding relationship by restoring supply.
- Monitoring is lifelong. Even if you recover, check your TSH levels postpartum annually to prevent future issues.
- You are not alone. This is a common autoimmune response to the massive changes of pregnancy.
You are the expert on your body. If you feel that your exhaustion is more than just sleepless nights, speak up. Your health is the foundation upon which your new family is built. Protecting your thyroid is protecting your ability to be the mother you want to be.
Frequently Asked Questions
How do I distinguish between normal postpartum fatigue and postpartum thyroiditis?
Normal fatigue typically improves with rest, whereas thyroid-related exhaustion is often “bone-deep” and accompanied by physical markers like a resting heart rate over 100 bpm or rapid weight loss. As an endocrinologist, I look for “tired but wired” sensations in the early thyrotoxic phase or profound lethargy that naps cannot resolve during the later hypothyroid phase.
What are the signs of the thyrotoxic phase in postpartum thyroiditis?
Occurring usually one to four months after delivery, this phase is characterized by a “leak” of stored hormones causing tremors, heat intolerance, and unexplained anxiety. You might notice your heart racing even while resting or experience a sudden drop in weight that exceeds your pre-pregnancy baseline due to destructive thyrotoxicosis.
Can thyroid issues after pregnancy cause postpartum depression?
Yes, there is a significant physiological overlap between the hypothyroid phase of thyroiditis and clinical postpartum depression. Low levels of T3 and T4 affect neurotransmitters like serotonin, which is why the American Thyroid Association recommends TSH screening for any mother presenting with persistent mood disorders or brain fog.
Is Levothyroxine safe to take while breastfeeding?
Levothyroxine is identical to the hormone your body naturally produces and passes into breast milk in negligible amounts, making it very safe for nursing infants. In fact, treating hypothyroidism often improves milk supply, as proper thyroid hormone levels are necessary for a healthy let-down reflex and overall lactation support.
Why is postpartum thyroiditis often misdiagnosed as Graves disease?
Both conditions present with high thyroid hormone levels, but thyroiditis is caused by destructive inflammation rather than overproduction. We use the TRAb antibody test and Doppler ultrasound to differentiate them, as thyroiditis requires symptom management with beta-blockers rather than antithyroid medications like Methimazole.
What is the typical timeline for postpartum thyroiditis recovery?
This condition is usually biphasic, starting with a hyperthyroid phase in the first few months, followed by a hypothyroid crash around months four to eight. While approximately 80% of women return to a euthyroid state within 12 to 18 months, the remaining 20% may develop permanent hypothyroidism requiring lifelong medication.
Who is considered high-risk for developing thyroid issues after birth?
Women with Type 1 Diabetes have a three-fold increased risk, and those with positive TPO antibodies in the first trimester have a 33% to 50% chance of developing the condition. A personal history of Hashimoto\’s or a previous episode of postpartum thyroiditis also warrants proactive TSH monitoring at six weeks and three months postpartum.
What specific lab tests should I request to check my thyroid levels after pregnancy?
A standard TSH test alone can be misleading in the early stages, so I recommend a full panel including TSH, Free T4, Free T3, and TPO Antibodies. If hyperthyroidism is detected, a TRAb test is essential to rule out Graves\’ disease before starting a treatment plan that could impact breastfeeding.
Does postpartum thyroiditis cause significant hair loss?
While “telogen effluvium” is common after birth, thyroid-driven hair loss is often more severe and occurs in clumps during the hypothyroid phase. Correcting the underlying hormonal imbalance with appropriate replacement therapy is the most effective way to stop this shedding and encourage healthy regrowth.
Can I use selenium to help manage postpartum thyroid inflammation?
Some clinical evidence suggests that 200mcg of Selenium daily can reduce TPO antibody levels by acting as a powerful antioxidant for thyroid tissue. However, it is vital to consult your physician before starting supplements to avoid toxicity and ensure it fits your specific clinical profile during the recovery phase.
What happens if postpartum thyroiditis is left untreated?
Untreated thyroid dysfunction can lead to breastfeeding failure, severe mood disorders, and unnecessary cardiovascular strain from prolonged tachycardia. Long-term, it increases the risk of permanent hypothyroidism, which is why annual TSH monitoring is recommended for anyone who has experienced a “silent” thyroiditis episode.
Will I have postpartum thyroiditis again in my next pregnancy?
There is approximately a 70% chance of recurrence in subsequent pregnancies if you have experienced it once. It is crucial to flag this in your medical history so your obstetrician can initiate thyroid screenings early in the postpartum period to catch the immune rebound before symptoms become debilitating.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. Postpartum thyroiditis is a complex medical condition that requires professional diagnosis and management. Always consult with a qualified healthcare professional or endocrinologist before making health decisions or starting new medications, especially while breastfeeding.
References
- American Thyroid Association (ATA) – thyroid.org – Clinical guidelines for the diagnosis and management of thyroid disease during pregnancy and postpartum.
- The Endocrine Society – endocrine.org – Comprehensive research on the “Immune Rebound” effect and autoimmune thyroiditis after delivery.
- American College of Obstetricians and Gynecologists (ACOG) – acog.org – Practice bulletins regarding postpartum depression screening and its link to TSH abnormalities.
- National Institutes of Health (NIH) – StatPearls: Postpartum Thyroiditis – Detailed medical pathology of the thyrotoxic and hypothyroid phases.
- LactMed (NCBI) – Drugs and Lactation Database – Safety data for Levothyroxine and Propranolol usage during breastfeeding.
- Journal of Clinical Endocrinology & Metabolism – “Fetal Microchimerism and Maternal Thyroid Autoimmunity” – Research study on the persistence of fetal cells in the maternal thyroid gland.





