
You wake up exhausted. You eat a salad for lunch while your coworkers eat burgers. You take your supplements religiously. Yet, the scale reads exactly the same number it did three weeks ago. It feels like a nightmare you cannot wake up from.
For years, I watched women blame themselves for a lack of discipline. But my experience in analyzing medical data reveals a darker truth. It isn’t about willpower. It is about a hidden collision between two major hormone systems that most doctors treat separately.
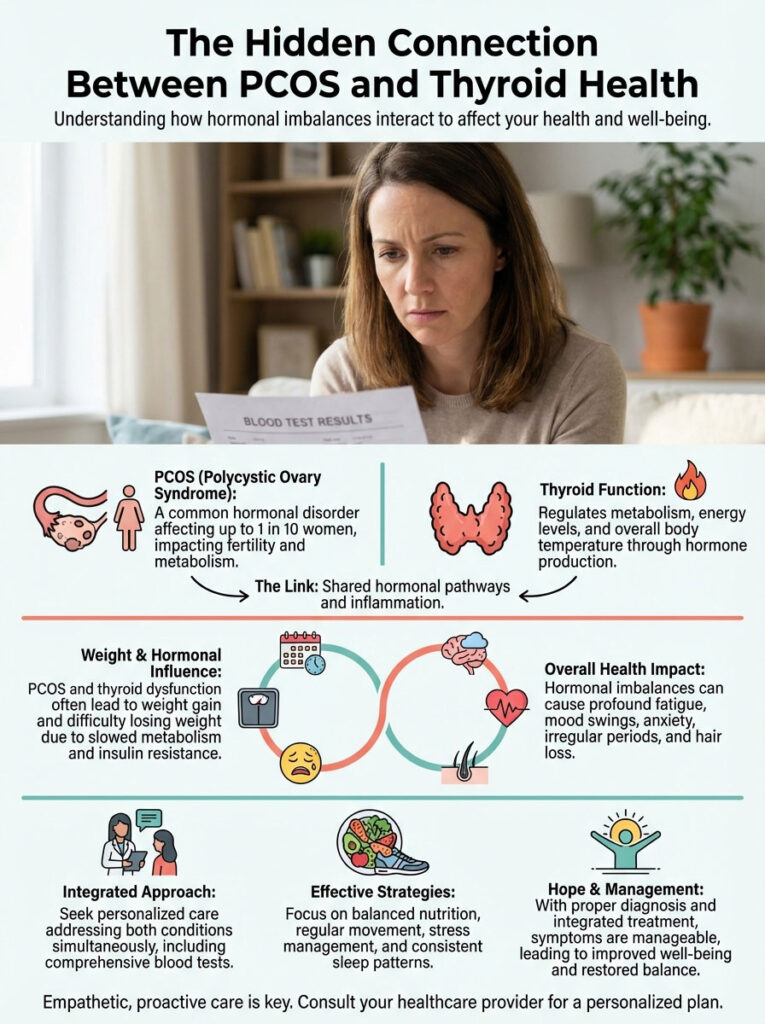
If you have Polycystic Ovary Syndrome (PCOS), your thyroid might be the invisible anchor dragging you down. Here is the shocking reality of how these two conditions conspire against your waistline—and exactly how to break the cycle.
If this raised questions, the full guide answers them: Is It Postpartum Fatigue or Postpartum Thyroiditis?
The “Sponge” Problem No One Talks About
To understand why you feel terrible, you must understand the liver’s role. I like to think of Sex Hormone-Binding Globulin (SHBG) as a master sponge. Its job is to soak up excess hormones in your blood.
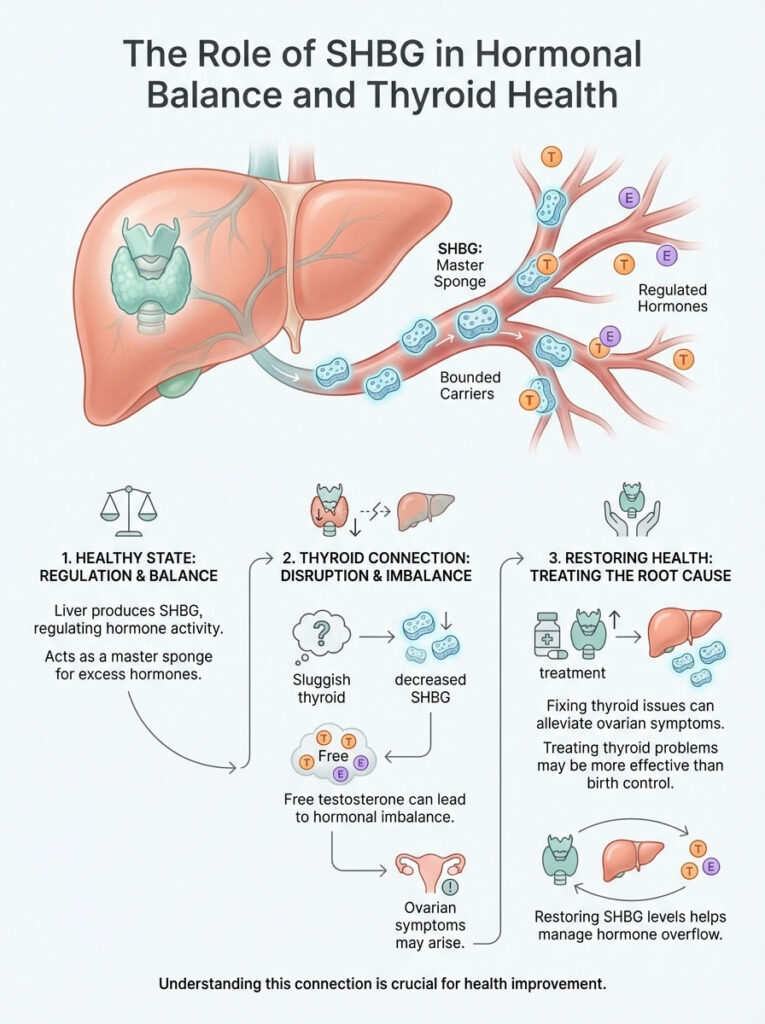
When your thyroid slows down, your liver stops making this sponge. Suddenly, you have no buffer. Testosterone that should be trapped becomes “free” and active.
This creates a dangerous domino effect:
- Acne flares up seemingly overnight.
- Hair thins at the temples.
- Weight clings to the midsection.
I found that treating the thyroid often fixes these “ovarian” symptoms faster than birth control ever could. You fix the sponge, you fix the overflow.
The Insulin-Thyroid Trap
Insulin resistance is the villain in most PCOS stories. But here is the secret mechanism rarely discussed in standard pamphlets. High insulin doesn’t just make you fat; it physically changes your thyroid gland.
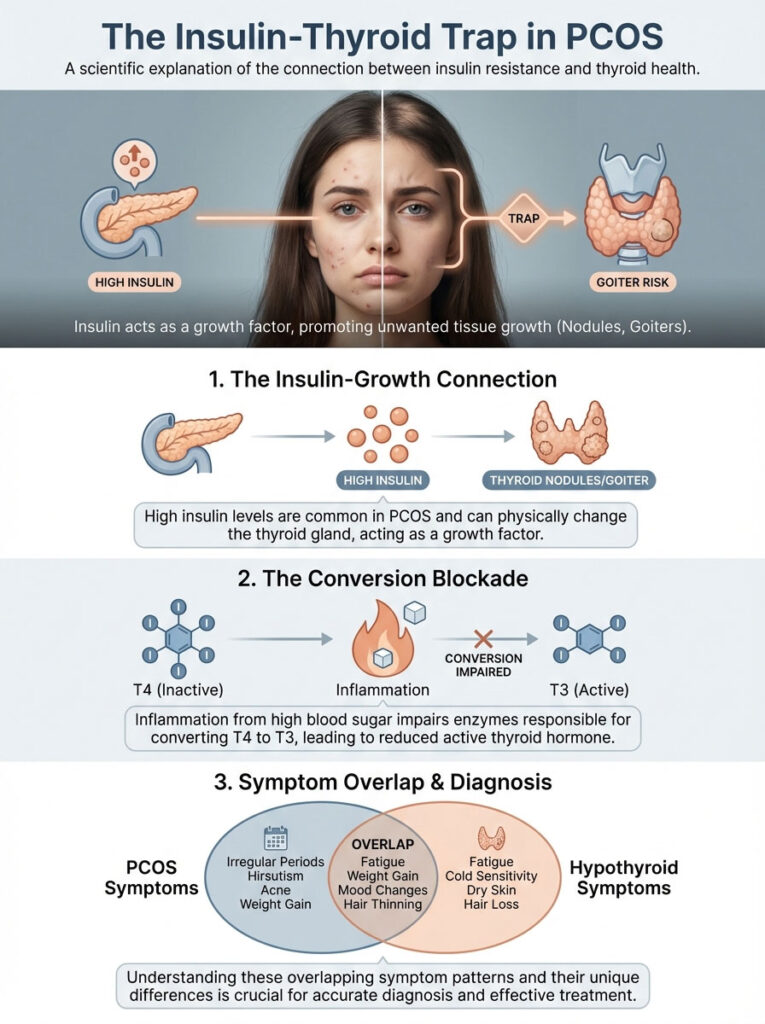
Insulin acts as a growth factor. It tells tissues to grow when they shouldn’t. This is why women with insulin resistance often develop thyroid nodules or goiters.
Furthermore, inflammation from high blood sugar attacks your conversion enzymes. Your body makes T4 (storage hormone), but it cannot turn it into T3 (active fuel). You have plenty of gas in the tank, but the spark plugs are dead.
Symptom Overlap Decoder
It is incredibly difficult to tell which condition is causing which symptom. I created this breakdown to help you spot the difference:
| Feature | Hypothyroidism | PCOS |
|---|---|---|
| Weight Pattern | Fluid retention, all-over puffiness | Visceral belly fat, rapid gain |
| Hair Loss | Diffuse thinning, loss of eyebrows | Male-pattern recession at temples |
| Fatigue Type | sluggish, cold, slow brain | Afternoon crash, “hangry” shakes |
| Skin Issues | Dry, cracking, pale skin | Oily, acne-prone, skin tags |
| Cycle | Heavy, prolonged bleeding | Absent or very infrequent periods |
Why “Normal” Labs Are Dangerous
This is where most patients get gaslit. You go to the doctor, they run a TSH, and say you are fine. But standard lab ranges are based on sick populations, not healthy ones.
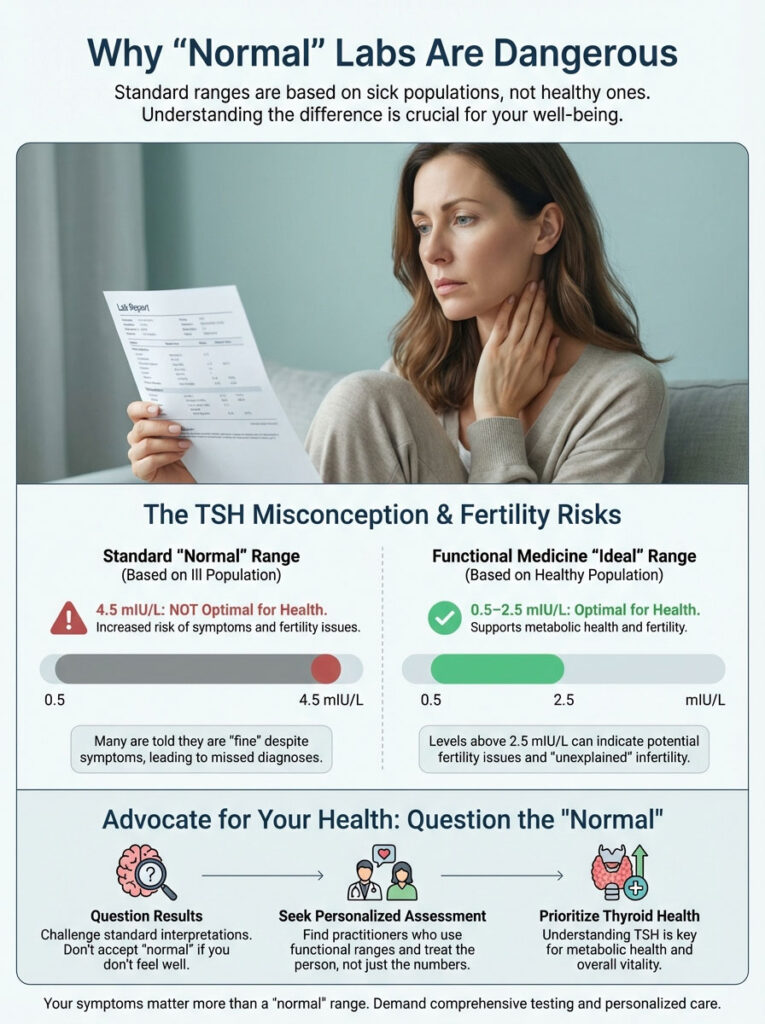
A TSH of 4.5 is not optimal.
In my investigation of functional medicine standards, the sweet spot is actually between 0.5 and 2.5 mIU/L. If you are trying to conceive, anything above 2.5 is a red flag. I have seen countless women suffer from “unexplained” infertility simply because their TSH was technically normal but metabolically sluggish.
The Autoimmune Connection
Here is a terrifying statistic: If you have PCOS, you are three times more likely to have Hashimoto’s. This is an autoimmune attack where your body destroys its own thyroid tissue.
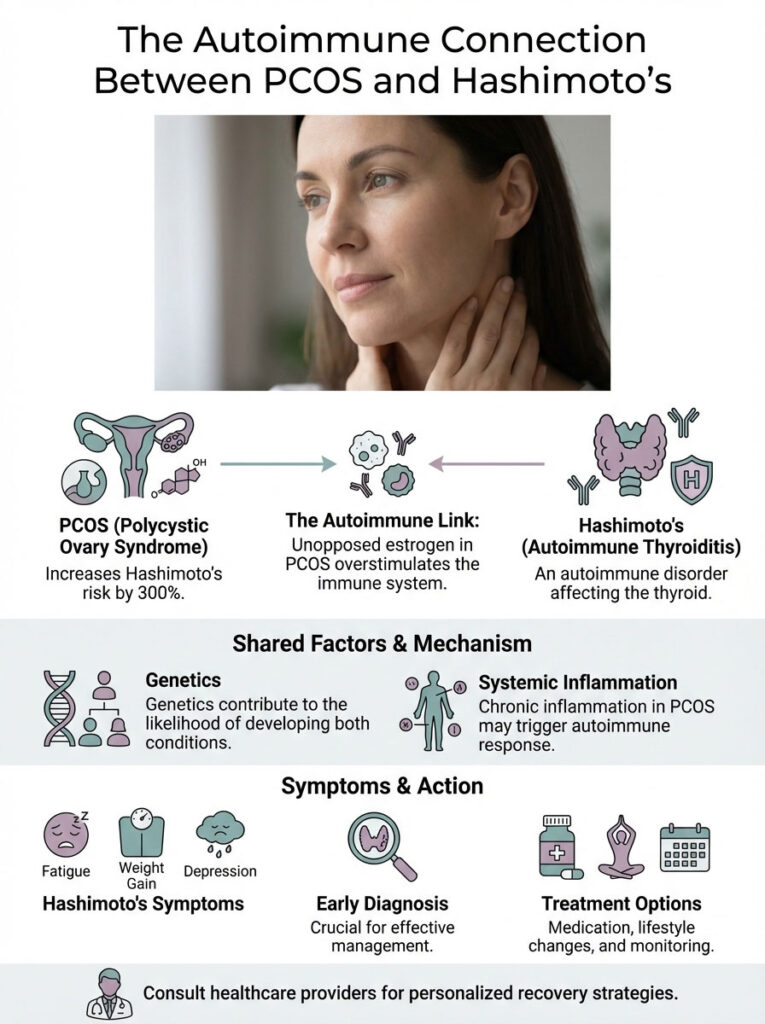
Why? Genetics play a role, but so does estrogen. The “unopposed estrogen” in PCOS bodies overstimulates the immune system. It effectively turns on the self-destruct button for the thyroid.
Key Takeaways for Recovery:
- Check Antibodies: TSH is not enough. You must test for TPO antibodies.
- Gluten Factor: Molecular mimicry means gluten looks like thyroid tissue to your body. Cutting it out is often essential.
- Selenium Power: This mineral lowers antibodies. Just 2-3 Brazil nuts daily can work wonders.
My Protocol for Breaking the Cycle
Treating this requires a dual approach. You cannot fix the thyroid while ignoring the insulin. I learned that the order of operations matters immensely.
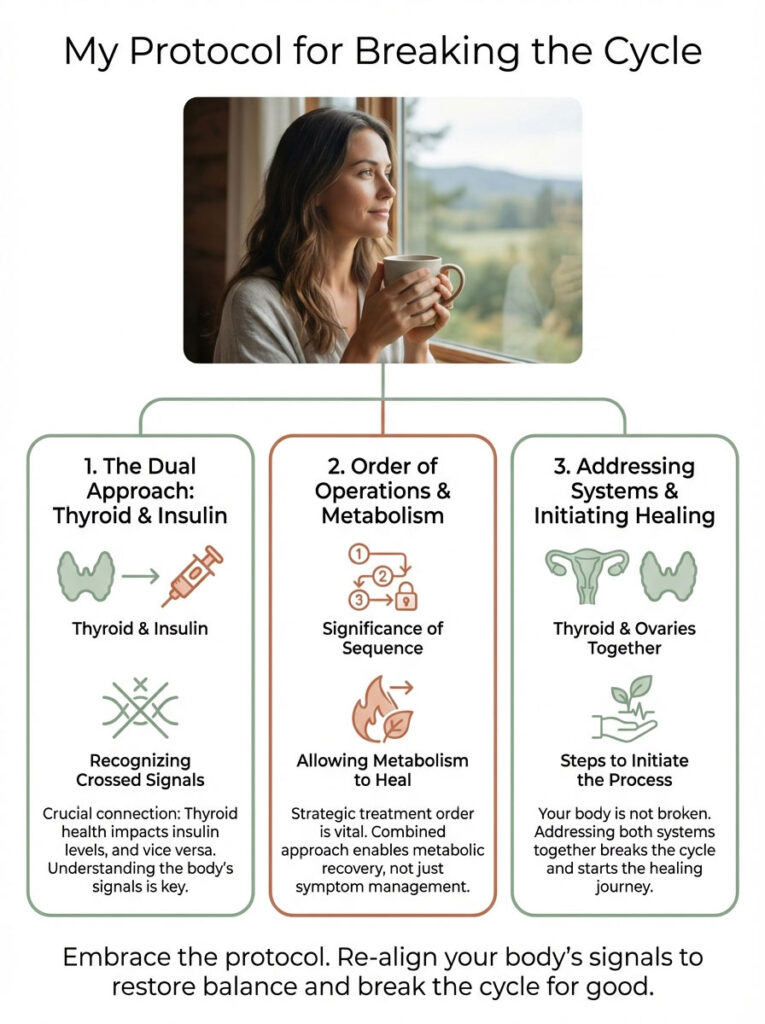
- Stabilize TSH first. Medication like Levothyroxine helps, but many need T3 (Cytomel) to bypass the conversion block.
- Target Insulin. Metformin or Myo-inositol are non-negotiable for lowering the inflammation that hurts the thyroid.
- Timing is Everything. Never take your thyroid med with coffee. Caffeine blocks absorption by up to 30%.
Your body is not broken. It is just receiving crossed signals. By addressing the thyroid and ovaries as a team, you finally give your metabolism permission to heal.





