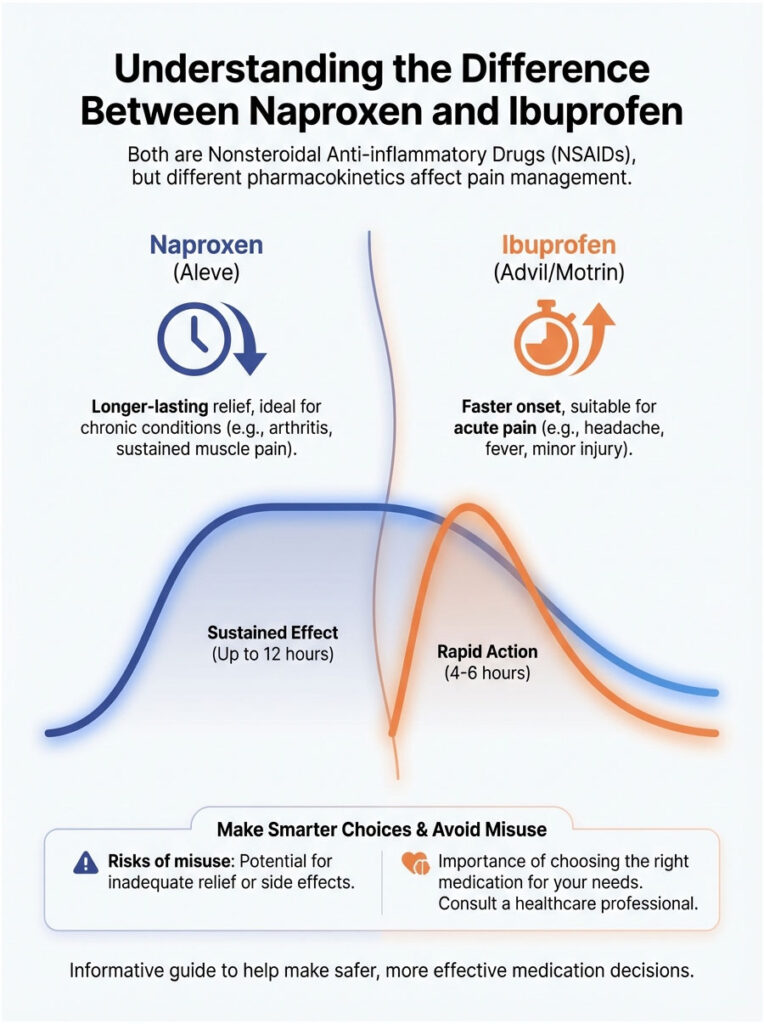
No, naproxen and ibuprofen are not the same medication. They both belong to the NSAID drug class, but they differ in chemical structure, duration of action, dosing, and safety profiles. Ibuprofen is short-acting (4 to 6 hours) and works best for acute pain like headaches or fever. Naproxen is long-acting (up to 12 hours), making it a better fit for chronic conditions like arthritis. They also have different age restrictions and side effect considerations.
Table of Contents
Why This Question Comes Up So Often
Picture yourself in the pharmacy aisle, staring at a wall of pain relievers. On one side, there is a blue bottle of Aleve. On the other, you see Advil or Motrin. You know they both treat pain and reduce inflammation. So what is the difference?
Is naproxen the same as ibuprofen? That is the single most common question I hear at the pharmacy counter. And the short answer is no.
While these two medications are chemical cousins, treating them as interchangeable can lead to poor pain relief, or worse, unexpected side effects. Both are classified as Nonsteroidal Anti-inflammatory Drugs (NSAIDs), and they block the same enzymes in your body. But their pharmacokinetics, meaning how your body absorbs, distributes, and clears each drug, create very different clinical applications.
If you are treating a pounding headache, you need speed. If you are managing arthritis, you need duration. Picking the wrong one can leave you in pain or raise your risk of stomach ulcers. In this guide, we will break down the science, safety, and strategy behind both medications so you can make a smarter choice.
Key NSAID Statistics Worth Knowing
- 30 million Americans use NSAIDs daily for pain management.
- 12-17 hours: the average half-life of naproxen, compared to just 1.8-2 hours for ibuprofen.
- 10 days: the maximum you should take OTC pain relievers without seeing a doctor.
- 15-30%: the estimated rate of peptic ulcers among chronic NSAID users.
- 1994: the year Aleve (naproxen) was approved for OTC use. Advil (ibuprofen) was approved a decade earlier in 1984.
- 6,000+ deaths annually in the US are linked to NSAID-induced gastrointestinal bleeding.
How NSAIDs Work: COX Inhibition Explained
To properly answer whether naproxen is the same as ibuprofen, we need to look at the molecular level, at what actually happens when you swallow that tablet.
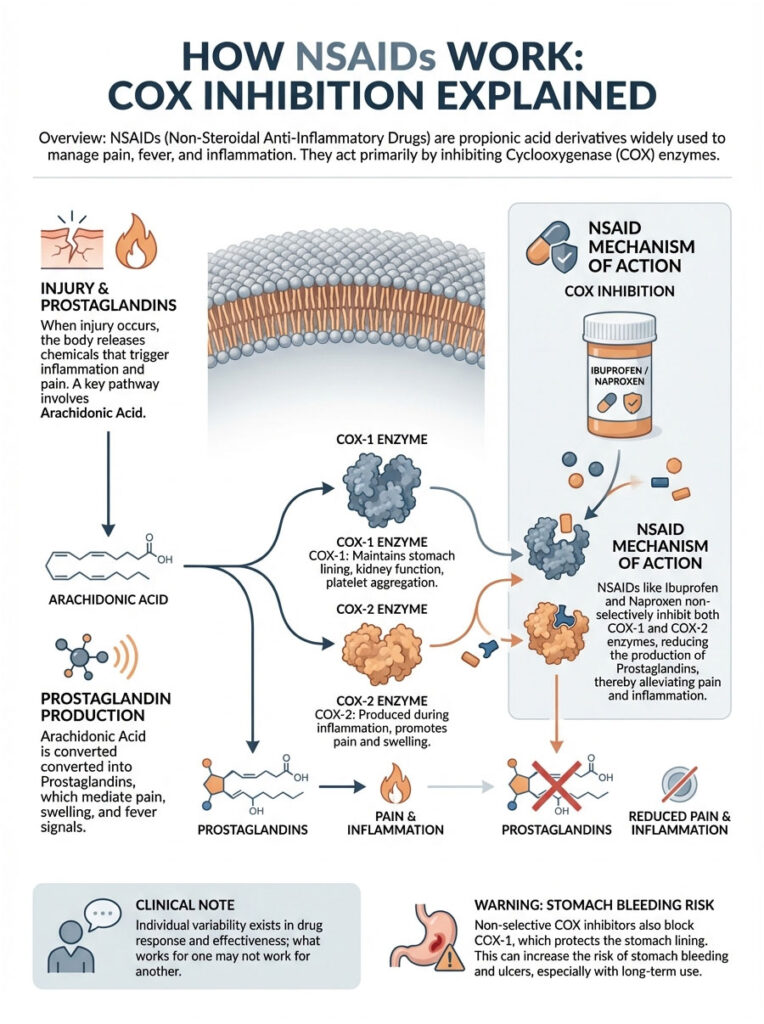
Both drugs belong to a chemical subclass called propionic acid derivatives. Their job is to stop your body from making compounds called prostaglandins, the chemical messengers that signal pain and inflammation.
The Science Behind Pain Signals
Prostaglandins are lipid compounds that act like messengers. When you injure tissue, whether it is a sprained ankle or a menstrual cramp, your body releases enzymes that produce prostaglandins. These messengers tell your brain, “we are hurt,” which creates the sensation of pain. They also dilate blood vessels, causing the redness and swelling we know as inflammation.
Enzyme Inhibition: The Lock and Key
Both ibuprofen and naproxen work by blocking the enzymes that create prostaglandins. These enzymes are called Cyclooxygenase, or COX for short. There are two main types:
- COX-1: The “housekeeping” enzyme. It produces prostaglandins that protect your stomach lining and help your blood clot properly.
- COX-2: The “inflammatory” enzyme. It is produced mainly in response to injury and drives pain and inflammation.
Here is the catch. Both naproxen and ibuprofen are non-selective COX inhibitors. They are blunt instruments that block both COX-2 (stopping your pain) and COX-1 (stripping away stomach protection). This shared mechanism is exactly why both drugs carry warnings for stomach bleeding.
Clinical note: While both drugs block COX-1 and COX-2, the ratio of inhibition varies slightly between individuals. This is why some people respond better to naproxen for back pain while others find relief only with ibuprofen. Individual biological variation plays a major role in drug response.
Pharmacokinetics: The Real Difference Between Naproxen and Ibuprofen
If the mechanism is the same, why do we have two different drugs? The answer comes down to pharmacokinetics, the study of how a drug is absorbed, distributed, metabolized, and excreted.
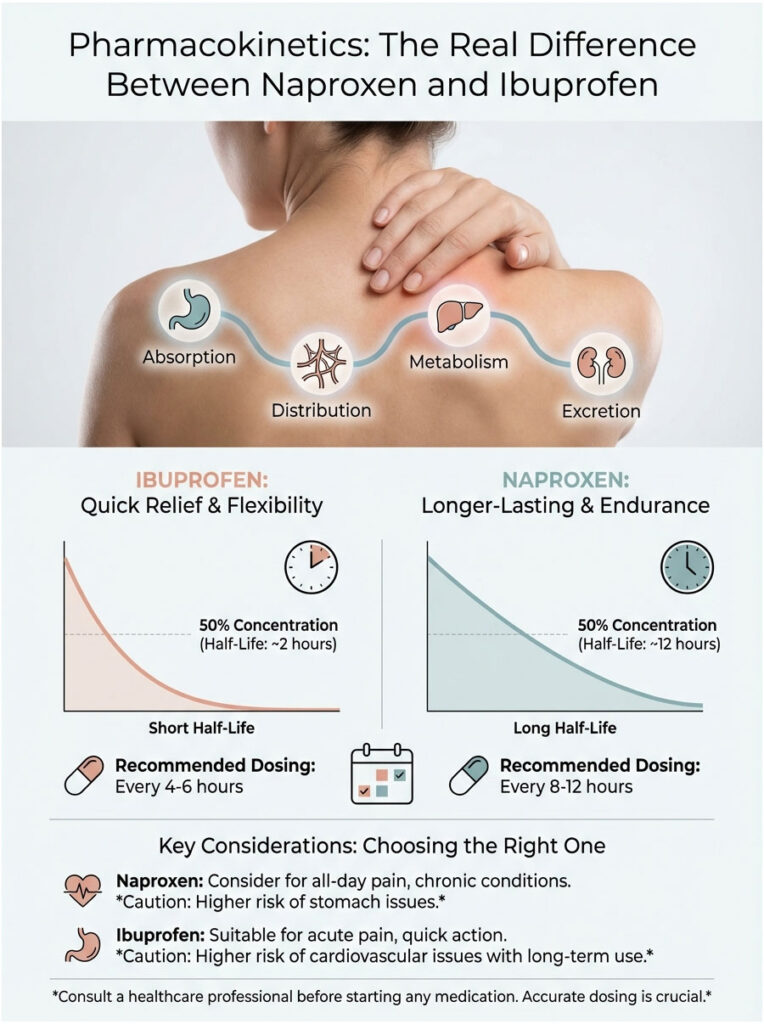
The most significant difference is their half-life. Half-life is the time it takes for the concentration of a drug in your blood to drop by exactly 50%. This single metric dictates how often you need to take a pill to stay ahead of the pain.
Ibuprofen: The Sprinter
Ibuprofen is designed for speed and flexibility.
- Short-acting: It has a half-life of roughly 1.8 to 2 hours.
- The rollercoaster effect: Because it clears your system quickly, pain-relieving effects wear off after 4 to 6 hours. If you are treating continuous pain, you may experience “breakthrough pain” right before your next dose.
- Fast peak levels: It reaches peak plasma concentration within 1 to 2 hours, making it the better choice when you need to hit a headache hard and fast.
Naproxen Sodium: The Marathon Runner
Naproxen is built for endurance.
- Long-acting: It has a half-life of 12 to 17 hours.
- Steady state: Because it stays in the body longer, it maintains a more consistent drug level in the blood, avoiding the peaks and valleys of pain relief.
- Better adherence: It is much easier for a patient to remember two pills a day than dosing every 4 hours.
Naproxen vs. Ibuprofen: Side-by-Side Comparison
When patients ask me whether naproxen is the same as ibuprofen, I often walk them through a comparison chart. The outcome is pain relief either way, but the path to get there is quite different.
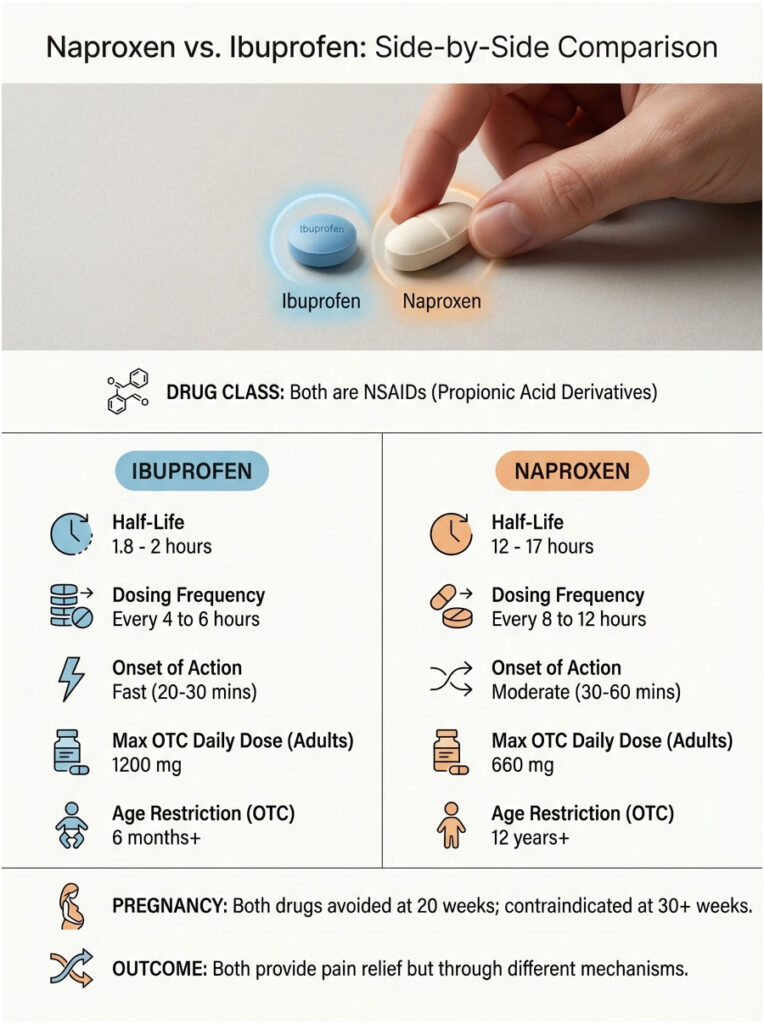
| Feature | Ibuprofen (Advil/Motrin) | Naproxen (Aleve) |
| Drug Class | NSAID (Propionic Acid Derivative) | NSAID (Propionic Acid Derivative) |
| Half-Life | 1.8 – 2 Hours | 12 – 17 Hours |
| Dosing Frequency | Every 4 to 6 Hours | Every 8 to 12 Hours |
| Onset of Action | Fast (20-30 mins) | Moderate (30-60 mins) |
| Max OTC Daily Dose | 1200 mg (Adults) | 660 mg (Adults) |
| Pregnancy | Avoid at 20 weeks; Contraindicated at 30+ weeks | Avoid at 20 weeks; Contraindicated at 30+ weeks |
| Age Restriction (OTC) | 6 Months+ (Pediatric formulations) | 12 Years+ |
Which Drug Works Best for Which Condition?
Not all pain is created equal. Because of the pharmacokinetic differences outlined above, one drug is often clinically preferred over the other depending on what you are treating.

Acute Pain (Headaches, Toothaches, Minor Injuries)
Recommended: Ibuprofen.
When you have a tension headache or a toothache, you want relief right now. Ibuprofen generally has a faster onset. Its formulation, especially in liqui-gel form, dissolves and enters the bloodstream rapidly. Waiting an hour for naproxen to kick in while your head is throbbing is not ideal.
Chronic Inflammation (Osteoarthritis, Rheumatoid Arthritis)
Recommended: Naproxen.
Arthritis is a marathon, not a sprint. Patients with osteoarthritis often deal with morning stiffness. A long-acting naproxen dose taken before bed stays active through the night and into the morning, significantly reducing pain upon waking. Ibuprofen taken at bedtime would likely wear off by 3:00 AM, leaving the patient stiff and uncomfortable.
Menstrual Cramps (Dysmenorrhea)
Recommended: Naproxen (clinical preference).
Menstrual cramps are triggered by a massive release of prostaglandins in the uterus. While both drugs help, naproxen is often favored because its long duration covers the most intense cramping window with fewer pills. Taking fewer pills also reduces the mental burden when you are already feeling unwell.
Fever Reduction (Antipyretic Use)
Recommended: Ibuprofen.
For bringing down a fever, ibuprofen is the go-to. Fevers spike and break unpredictably, and ibuprofen’s shorter half-life allows for more frequent dosing adjustments within safe limits. It also matters that naproxen is not approved for OTC use in children under 12, making ibuprofen the default NSAID for pediatric fevers.
Safety Profiles and FDA Black Box Warnings
Safety is where the question “is naproxen the same as ibuprofen” really matters. While they share side effects, the risk profile shifts depending on your medical history. Both drugs carry FDA Black Box warnings, the strictest labeling requirement, for cardiovascular and gastrointestinal risks.
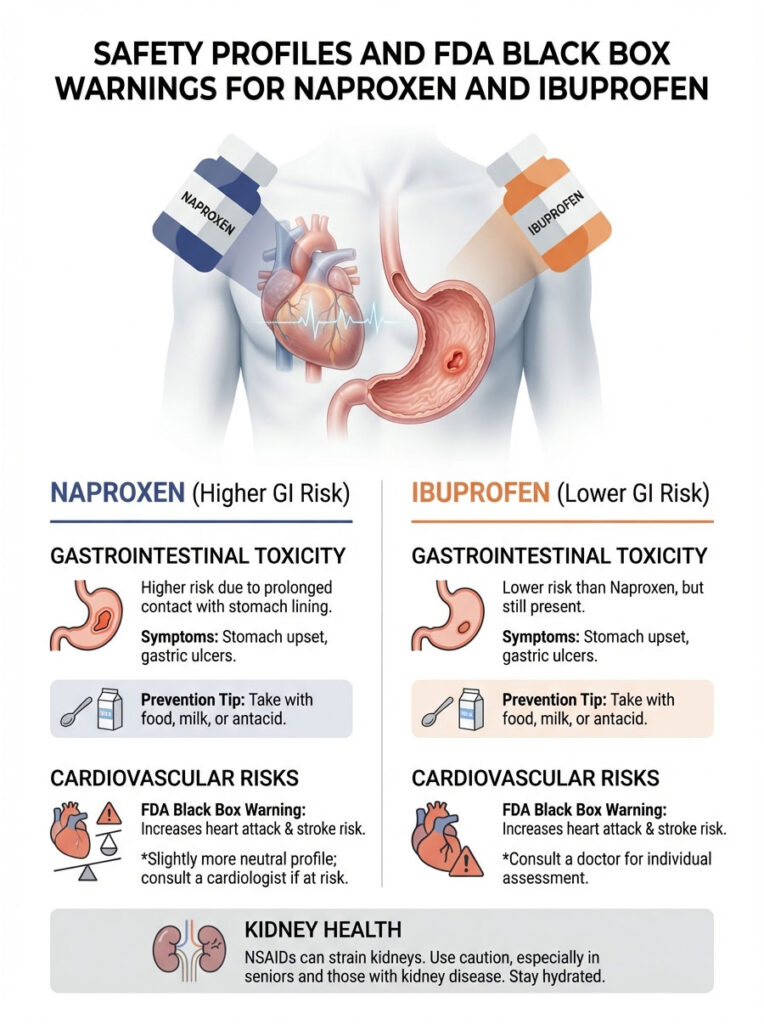
Gastrointestinal (GI) Toxicity
Stomach upset is the most common complaint with NSAIDs. It ranges from mild heartburn to severe gastric ulcers and perforation.
Naproxen generally carries a statistically higher risk of GI issues compared to low-dose ibuprofen. This is not because naproxen is more toxic per milligram, but because it stays in contact with the stomach lining for a longer duration. A drug that lingers in your system for 14 hours has more time to irritate than one that clears in 4 hours.
Prevention tip: Never take these medications on an empty stomach. Taking them with food, milk, or an antacid can buffer your stomach lining against irritation.
Cardiovascular Risk (Heart Attack and Stroke)
With the exception of aspirin, all NSAIDs increase the risk of cardiovascular events including heart attack and stroke. This risk can grow with prolonged use.
Some studies and meta-analyses have suggested that naproxen may have a slightly more neutral cardiovascular profile compared to other NSAIDs, including high-dose ibuprofen. However, the FDA states that no NSAID is completely free of cardiovascular risk. If you have a history of heart disease, talk to your cardiologist before taking either one.
Kidney Health (Renal Clearance)
Your kidneys are your body’s filters, and NSAIDs can put significant strain on them. Both ibuprofen and naproxen constrict the afferent arterioles, the tiny blood vessels that feed blood into the kidney’s filtering units. This reduces the Glomerular Filtration Rate (GFR).
For a healthy young person, this effect is temporary and harmless. But for seniors, people on diuretics, or those with existing Chronic Kidney Disease (CKD), the reduction in blood flow can trigger acute kidney failure.
Important: If you have kidney disease, both naproxen and ibuprofen are generally contraindicated. Acetaminophen (Tylenol) is typically the safer alternative, but always confirm with your doctor.
Drug Interactions You Need to Know About
One of the most dangerous misconceptions is that because these drugs are sold over the counter, they play well with other medications. That is not the case. Understanding drug interactions is a matter of safety.
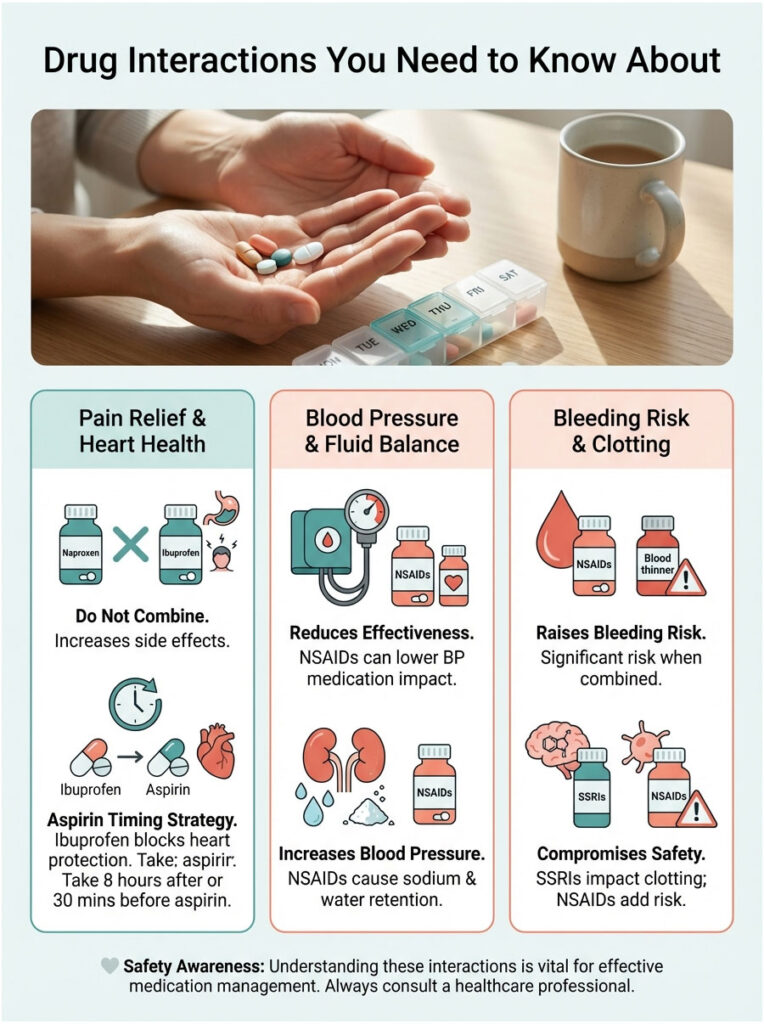
Never Take Naproxen and Ibuprofen Together
I cannot stress this enough. Taking them together does not double your pain relief. Instead, it exponentially increases the risk of side effects through competitive inhibition. They fight for the same receptor sites. Once those receptors are occupied, the extra drug circulates in your blood, attacking your stomach and kidneys without providing any additional benefit.
Aspirin Interference
Millions of Americans take low-dose aspirin (81mg) for heart protection. Ibuprofen can bind to platelets and block aspirin from doing its job, effectively canceling out your heart protection.
Strategy: If you must take ibuprofen, take it at least 8 hours after or 30 minutes before your aspirin. Naproxen also interacts with aspirin, but the timing is more complex due to its long half-life.
Blood Pressure Medications
If you take medication for high blood pressure, including ACE inhibitors like Lisinopril or diuretics, NSAIDs can make them less effective. NSAIDs cause the body to retain sodium and water, which raises blood pressure and directly opposes the medication you are taking to lower it.
SSRIs and Blood Thinners
Combining NSAIDs with blood thinners like Warfarin or Eliquis raises the risk of bleeding significantly. The same applies when combining them with common antidepressants like Zoloft or Prozac. SSRIs affect platelet aggregation, and when you add an NSAID on top, you are removing two of the body’s natural clotting safeguards.
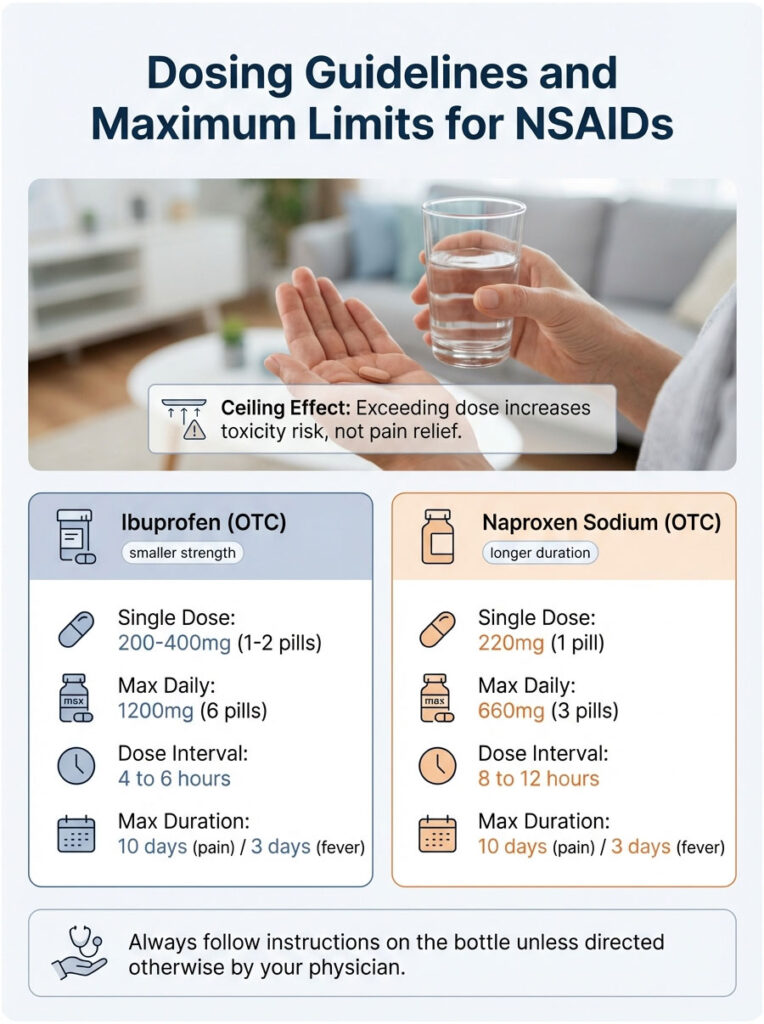
Dosing Guidelines and Maximum Limits
With NSAIDs, there is a ceiling effect. Beyond the maximum recommended dose, you will not get more pain relief. You will only increase your risk of toxicity.
OTC vs. Prescription Strength
The pills you buy at your local pharmacy are lower strength than what a pharmacist dispenses behind the counter.
- Ibuprofen: OTC tablets are typically 200mg. Prescription strength goes up to 800mg per dose.
- Naproxen: OTC Aleve is 220mg (200mg naproxen base plus 20mg sodium). Prescription strength is usually 500mg.
| Medication | Single Dose (OTC) | Max Daily (OTC) | Dose Interval | Max Duration |
| Ibuprofen | 200-400mg (1-2 pills) | 1200mg (6 pills) | 4 to 6 Hours | 10 days (pain) / 3 days (fever) |
| Naproxen Sodium | 220mg (1 pill) | 660mg (3 pills) | 8 to 12 Hours | 10 days (pain) / 3 days (fever) |
Always follow the instructions on the bottle unless directed otherwise by your physician.
Special Populations: Age and Life Stage Considerations
When asking whether naproxen is the same as ibuprofen, the answer partly depends on who is asking. Age and life stage are major factors.
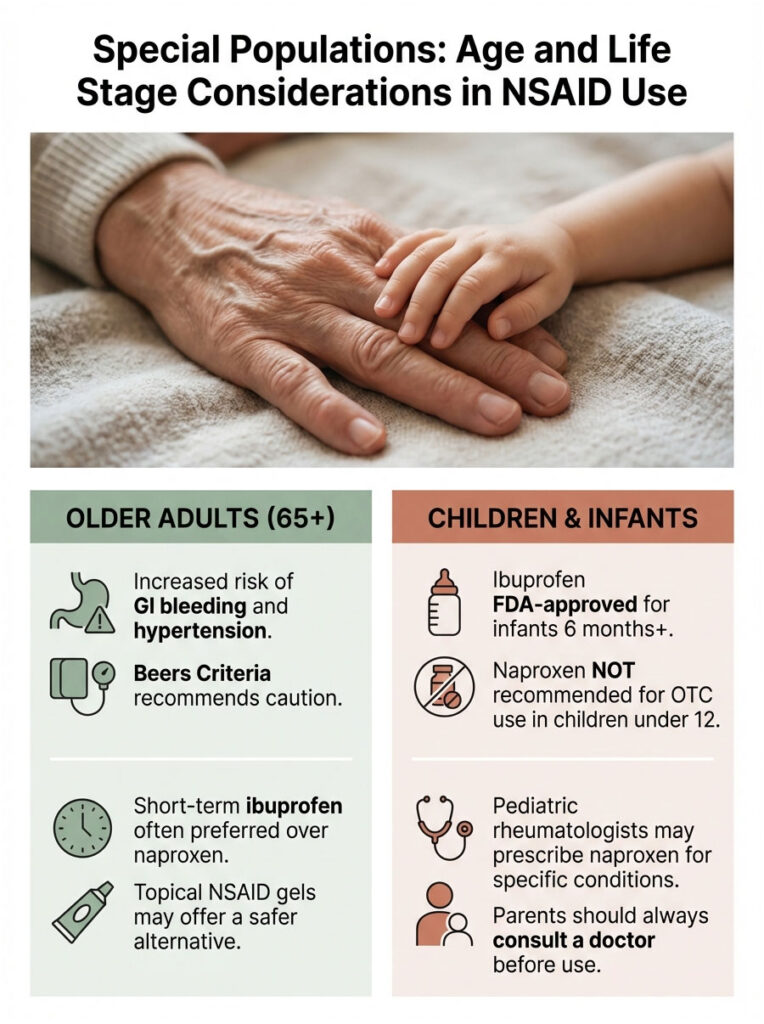
Older Adults (65+)
As we age, kidney function naturally declines and the stomach lining gets thinner. The Beers Criteria, a guideline for healthcare professionals, lists NSAIDs as “potentially inappropriate” for older adults due to elevated risk of GI bleeding and hypertension.
If an NSAID is necessary, short-term use of ibuprofen is often preferred over long-acting naproxen because it reduces the duration of systemic exposure. That said, topical NSAID gels are often an even safer option.
Pregnancy
- First and Second Trimester: Use with extreme caution and only if prescribed. Acetaminophen is the preferred pain reliever.
- Third Trimester: Contraindicated. NSAIDs in the third trimester can cause premature closure of the ductus arteriosus (a vital fetal blood vessel) and low amniotic fluid levels.
Children (Pediatrics)
Here is a major practical difference. Ibuprofen is FDA-approved for infants as young as 6 months and is a staple in pediatric medicine for fevers and ear infections. Naproxen, on the other hand, is not recommended for OTC use in children under 12.
While pediatric rheumatologists may prescribe naproxen for conditions like Juvenile Idiopathic Arthritis, parents should never give OTC Aleve to a young child without a doctor’s explicit approval.
Why Does the Bottle Say “Naproxen Sodium”?
You may have noticed that the label reads “Naproxen Sodium” rather than just “Naproxen.” The sodium is not there for flavor. Adding a salt molecule improves the drug’s solubility, allowing it to dissolve in stomach fluids much faster than the base naproxen molecule.
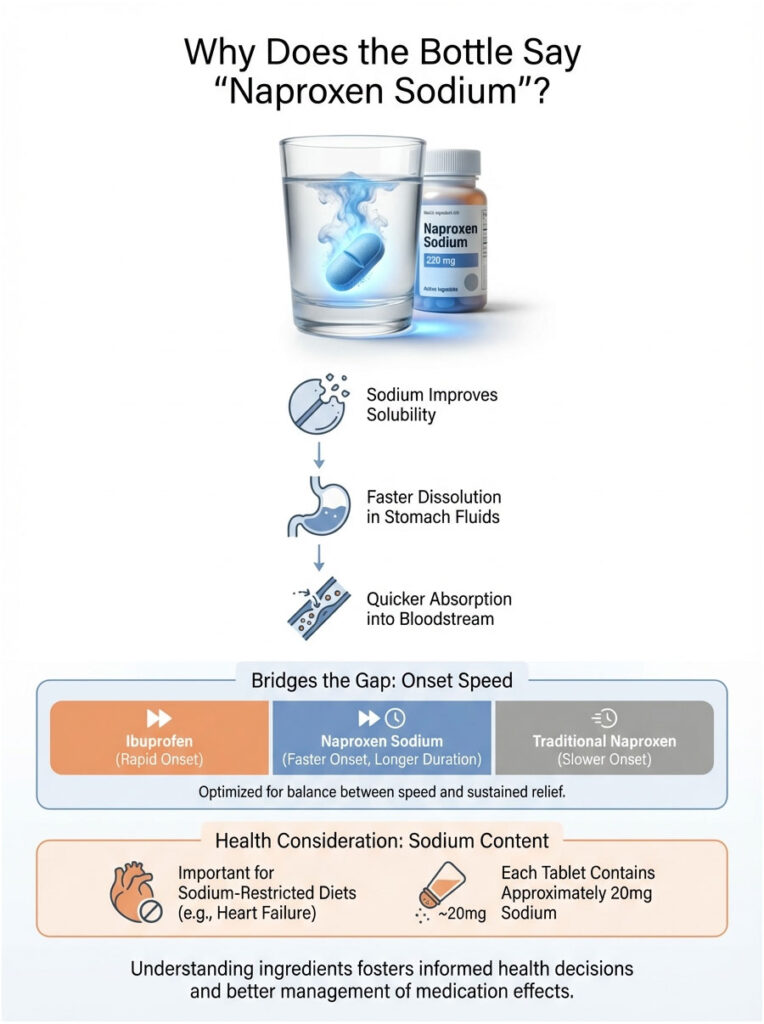
This is a deliberate pharmaceutical engineering choice. By adding sodium, the manufacturer helps the drug enter your bloodstream faster, bridging the gap between ibuprofen’s rapid onset and traditional naproxen’s slower absorption.
However, each OTC tablet contains roughly 20mg of sodium. If you are on a strict sodium-restricted diet for heart failure, this is something you need to account for.
Metabolism, Genetics, and Drug Response
Both drugs are metabolized in the liver through the Cytochrome P450 enzyme system, specifically the CYP2C9 enzyme. This is where genetics become relevant.
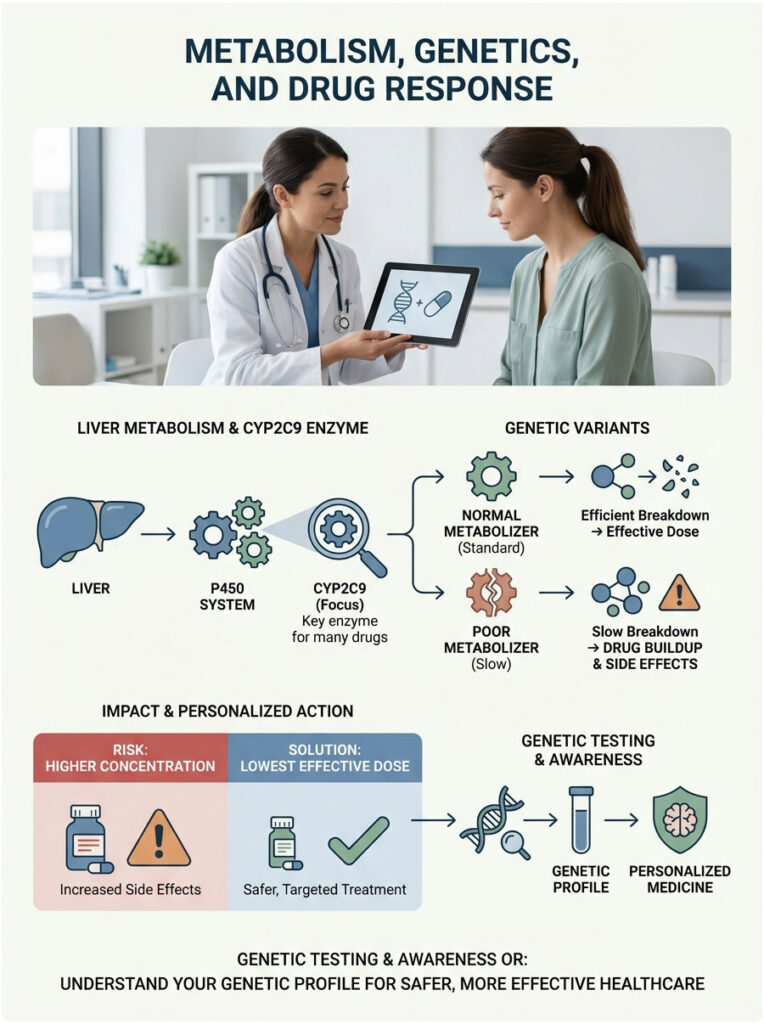
Some people are “poor metabolizers,” meaning they have a genetic variant that makes their CYP2C9 enzyme sluggish. For these individuals, the drug stays in the body much longer than expected, increasing the risk of side effects.
Since most people do not know their genetic profile, this is yet another reason to always start with the lowest effective dose.
Managing Common Side Effects
If you need to take these drugs, managing side effects proactively can make a real difference.
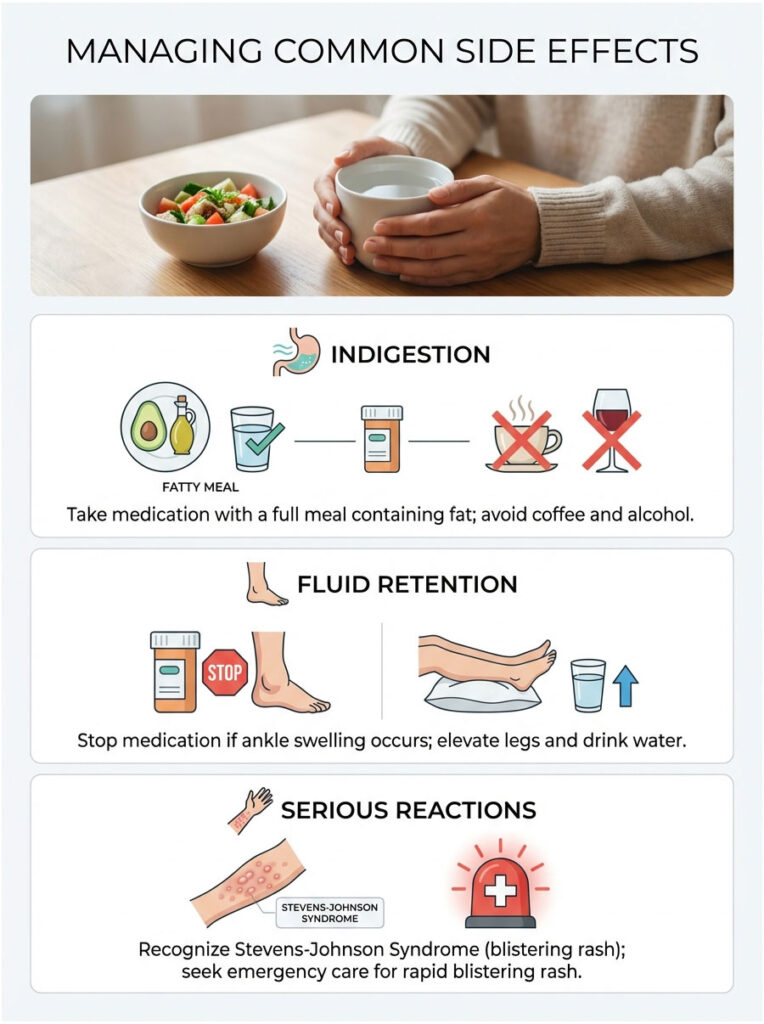
Indigestion (Dyspepsia)
If you feel a burning sensation after taking either medication, avoid combining it with coffee or alcohol. Take it with a full meal that includes some fat. The fat helps slow gastric emptying, which buffers the stomach lining.
Fluid Retention and Swelling
If you notice your ankles swelling (edema) after a few days of use, stop the medication. This is a sign your kidneys are retaining water. Elevate your legs, drink plenty of plain water, and see your doctor if the swelling does not resolve within 24 hours.
Recognizing Serious Reactions
In rare cases, patients can develop a severe skin reaction called Stevens-Johnson Syndrome (SJS). If you see a rash that spreads quickly and causes blistering, go to the emergency room immediately. This is a medical emergency.
Practical Tips from a Clinical Pharmacist
1. Try a Trial Period
Pain relief is subjective. If ibuprofen does not work after two proper doses, it may not be the right molecule for your biology. Wait for it to clear your system (this is called the washout period), then try naproxen next time. Sometimes, simply switching the NSAID is all it takes.
2. Ask About Gastric Protection
If your doctor recommends long-term NSAID use, ask about adding a Proton Pump Inhibitor (PPI) like omeprazole. A PPI can significantly reduce the risk of developing an ulcer during NSAID therapy, especially for patients managing chronic back pain.
3. Stay Well Hydrated
Remember the kidney effects we discussed? You can help reduce the risk of renal strain by staying well hydrated. Water supports blood volume and helps with renal clearance. Never take these pills with just a sip of coffee. Take them with a full glass of water.
Final Verdict: Is Naproxen the Same as Ibuprofen?
No. Naproxen and ibuprofen are distinct tools in the pain management toolkit, and choosing the right one depends on your specific situation.
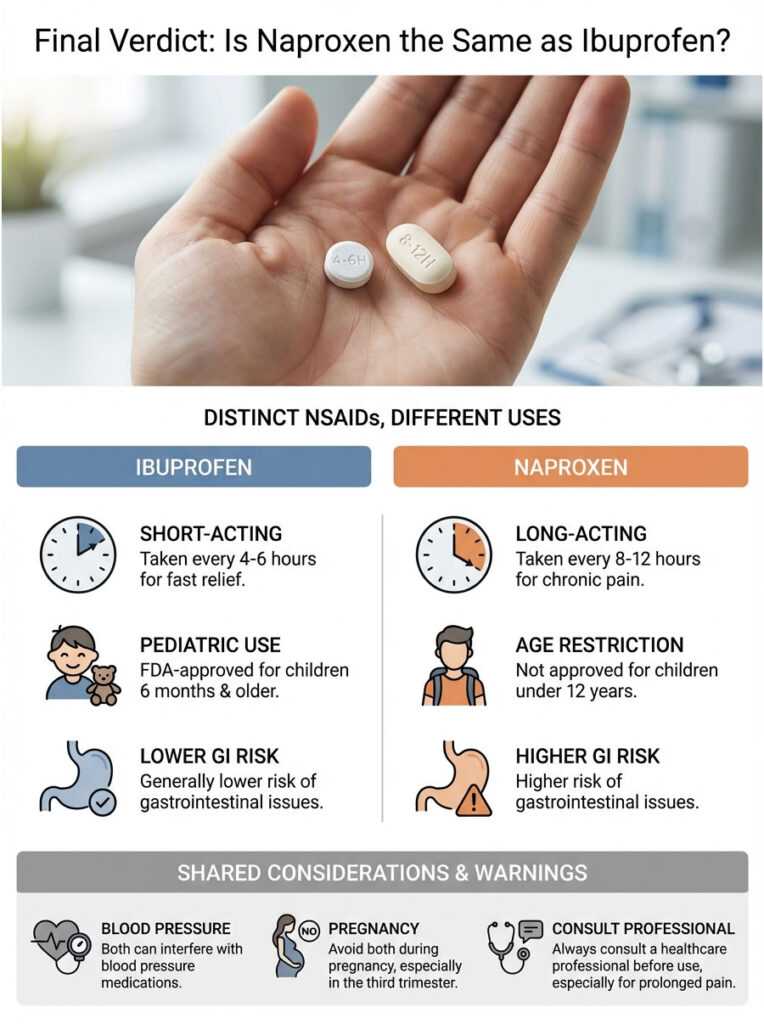
- Ibuprofen is the sprinter. Best for acute pain, pediatric fever, and situations requiring fast relief that wears off quickly.
- Naproxen is the marathon runner. Best for chronic conditions, all-day stiffness, and reducing the number of pills you take.
- Safety: Neither is inherently “safer.” Naproxen is harder on the stomach due to its longer duration. Ibuprofen carries similar cardiovascular and kidney risks.
- Interactions: Both interact dangerously with blood thinners, aspirin, and blood pressure medications.
- Usage: Never combine them. Always take with food. Respect the maximum daily limits.
The “best” drug depends on your body and your condition. If you have a sensitive stomach, be cautious with naproxen. If you need fast relief for a sprained ankle, ibuprofen is likely your better bet. And always consult your doctor or pharmacist before starting a daily regimen, especially if your pain persists beyond 10 days.
Frequently Asked Questions
Is naproxen the same as ibuprofen?
No, while both are nonsteroidal anti-inflammatory drugs (NSAIDs) that block COX enzymes, they have different chemical structures and durations of action. Ibuprofen is a short-acting medication typically taken every 4 to 6 hours, whereas naproxen is long-acting and usually dosed every 8 to 12 hours.
Which medication works faster for immediate pain relief like a headache?
Ibuprofen generally has a faster speed of onset, typically reaching peak plasma concentrations within 1 to 2 hours. This makes it the clinically preferred choice for acute conditions like tension headaches or toothaches where rapid relief is the priority.
Why is naproxen often recommended for chronic arthritis pain?
Naproxen has a much longer half-life of 12 to 17 hours, allowing for steady-state concentrations in the blood with just two doses a day. This provides consistent, all-day inflammation relief and is particularly effective for managing morning stiffness associated with osteoarthritis.
Can I take naproxen and ibuprofen at the same time for better results?
You should never combine different NSAIDs as it does not double the analgesic effect but exponentially increases the risk of gastrointestinal bleeding and kidney strain. This practice leads to competitive inhibition at the receptor sites, leaving excess drug to circulate and cause systemic toxicity.
Which NSAID carries a higher risk of stomach ulcers and GI upset?
While both drugs block the protective COX-1 enzyme, naproxen generally carries a higher statistical risk of gastrointestinal issues because it remains in the system longer. The extended duration of exposure to the gastric mucosa increases the likelihood of irritation compared to short-acting ibuprofen.
Is there a difference in cardiovascular risk between naproxen and ibuprofen?
Some clinical data suggest that naproxen may have a more neutral cardiovascular profile, whereas high-dose ibuprofen has been linked to a slightly higher risk of thrombotic events. However, the FDA mandates a Black Box warning for both, and patients with heart disease must consult a specialist before use.
Do naproxen and ibuprofen interfere with blood pressure medications?
Yes, both medications can reduce the efficacy of antihypertensives like ACE inhibitors and diuretics by causing the body to retain sodium and water. This physiological response can lead to elevated blood pressure levels, directly opposing the therapeutic goals of your cardiac medications.
At what age can children safely take naproxen versus ibuprofen?
Ibuprofen is FDA-approved for pediatric use in infants as young as 6 months, making it the standard for childhood fevers. Conversely, naproxen is not recommended for over-the-counter use in children under 12 years of age unless specifically directed by a pediatrician.
Are naproxen and ibuprofen safe to use during pregnancy?
Both medications should be avoided during pregnancy, particularly after 20 weeks, and are strictly contraindicated in the third trimester. Use during late pregnancy can cause premature closure of the fetal ductus arteriosus and lead to dangerously low amniotic fluid levels.
How do these pain relievers affect kidney function?
Both drugs can impair renal clearance by constricting the blood vessels that supply the kidneys, which may lead to acute kidney injury in vulnerable populations. Seniors or those with chronic kidney disease (CKD) should exercise extreme caution and typically use acetaminophen instead.
What is the purpose of the sodium in naproxen sodium tablets?
The addition of a sodium salt molecule improves the drug’s solubility, allowing it to dissolve and enter the bloodstream more rapidly than the base molecule. While this speeds up the onset of action, patients on strict sodium-restricted diets for heart failure should account for the roughly 20mg of sodium per tablet.
What are the maximum daily over-the-counter doses for these medications?
For healthy adults, the maximum over-the-counter daily limit for ibuprofen is 1200mg (six 200mg tablets). For naproxen sodium, the limit is 660mg (three 220mg tablets) within a 24-hour period to avoid reaching the “ceiling effect” where side effects outweigh benefits.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. The information provided is intended to supplement, not replace, the relationship between a patient and their healthcare professional. Always consult a qualified physician or pharmacist before starting, stopping, or changing any medication regimen, especially if you have underlying health conditions or are taking other drugs.
References
- U.S. Food and Drug Administration (FDA) – www.fda.gov – Official drug labels and Black Box warning requirements for nonsteroidal anti-inflammatory drugs (NSAIDs).
- Mayo Clinic – www.mayoclinic.org – Comparative analysis of over-the-counter pain relievers and their specific clinical applications.
- National Center for Biotechnology Information (NCBI) – PubMed – Research studies on the pharmacokinetics and half-life variations between Naproxen and Ibuprofen.
- American College of Cardiology – www.acc.org – Meta-analysis regarding the cardiovascular safety profiles of various non-selective COX inhibitors.
- Cleveland Clinic – my.clevelandclinic.org – Comprehensive guide on the gastrointestinal risks associated with long-term NSAID therapy.
- The American Journal of Managed Care (AJMC) – www.ajmc.com – Statistics regarding NSAID usage in the United States and associated healthcare complications.