A clinical dietitian with 15+ years in digestive health explains the science, the myths, and a practical protocol for lasting relief.
Table of Contents
Quick Answer: How the Alkaline Diet Helps GERD
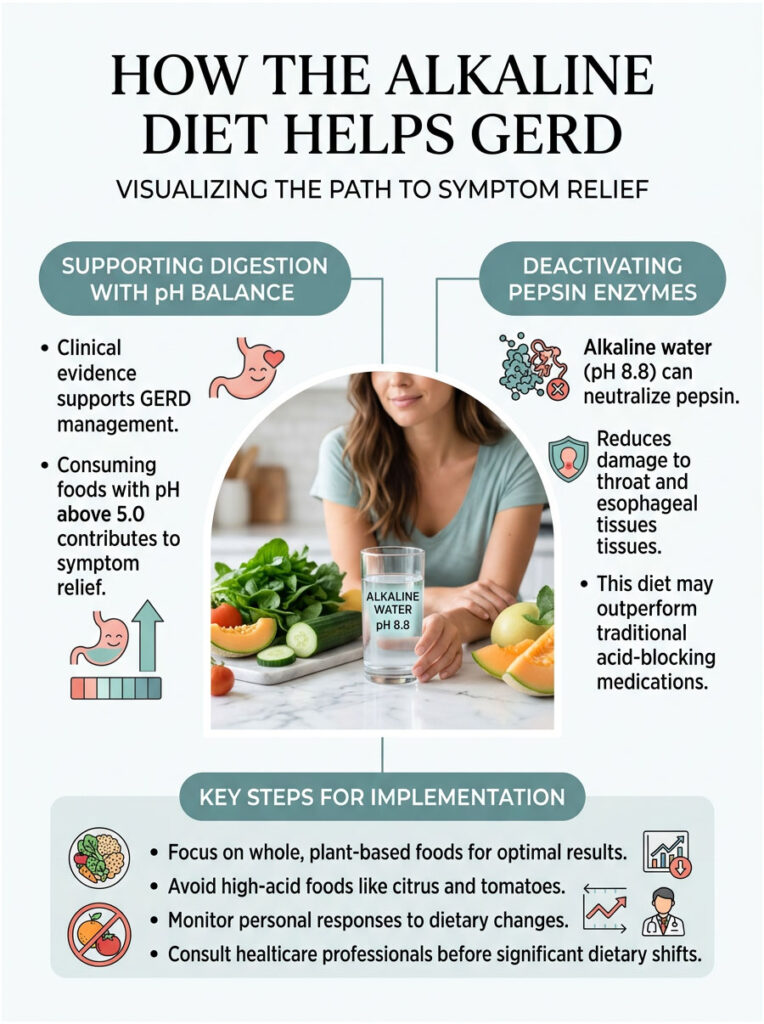
Yes, the connection between an alkaline diet and GERD is backed by solid clinical evidence. By eating foods with a pH above 5.0 and drinking alkaline water at pH 8.8, you can permanently deactivate pepsin, the enzyme responsible for most of the tissue damage in your throat and esophagus. In clinical studies, this dietary approach has matched or outperformed traditional acid-blocking medications for symptom relief.
Key Statistics on Reflux and Diet
- 20%+ of U.S. adults experience chronic reflux symptoms every week.
- Up to 40% of patients on acid blockers still report breakthrough symptoms.
- 62.6% reduction in Reflux Symptom Index scores with a Mediterranean-style alkaline diet (JAMA Otolaryngology).
- Pepsin is permanently destroyed at pH 8.8, but remains stable at neutral pH 7.4.
- 95% of patients on a strict pH 5.0+ diet see significant improvement within 28 days.
- PPI prescriptions have risen over 50% in the last decade, even as dietary interventions gain traction.
Why Your Heartburn Medication May Not Be Enough
If you have been dealing with chronic heartburn, you probably know the frustration of pills that only partly work. You take your medication every morning, yet the burning creeps back by afternoon. That cycle is exhausting, and it is more common than you think.
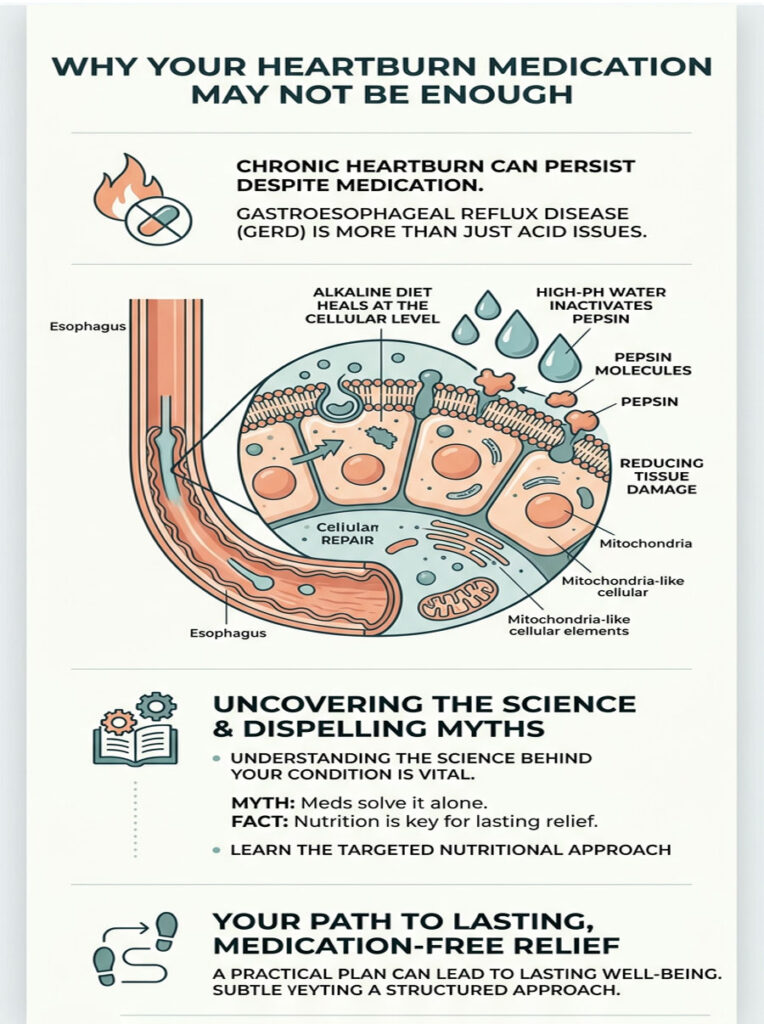
As a Clinical Dietitian Nutritionist and Board-Certified Specialist in Digestive Diseases, I see this pattern daily. Gastroesophageal Reflux Disease is not just an acid problem. It is a tissue damage problem, and fixing it requires more than acid suppression. It requires a targeted nutritional strategy designed to heal your esophagus at the cellular level.
An alkaline diet paired with high-pH water gives you a scientifically supported method to do exactly that. The protocol works by permanently inactivating pepsin, the primary enzyme behind your tissue damage. In this guide, I will walk you through the clinical science, bust the biggest myths, and give you a practical plan for lasting, medication-free relief.
The Real Physiology of Acid Reflux: Acid Is Only Half the Story
Most people think stomach acid is the sole villain. That is a misconception fueled by decades of pharmaceutical marketing. The truth is more nuanced and, honestly, more interesting.
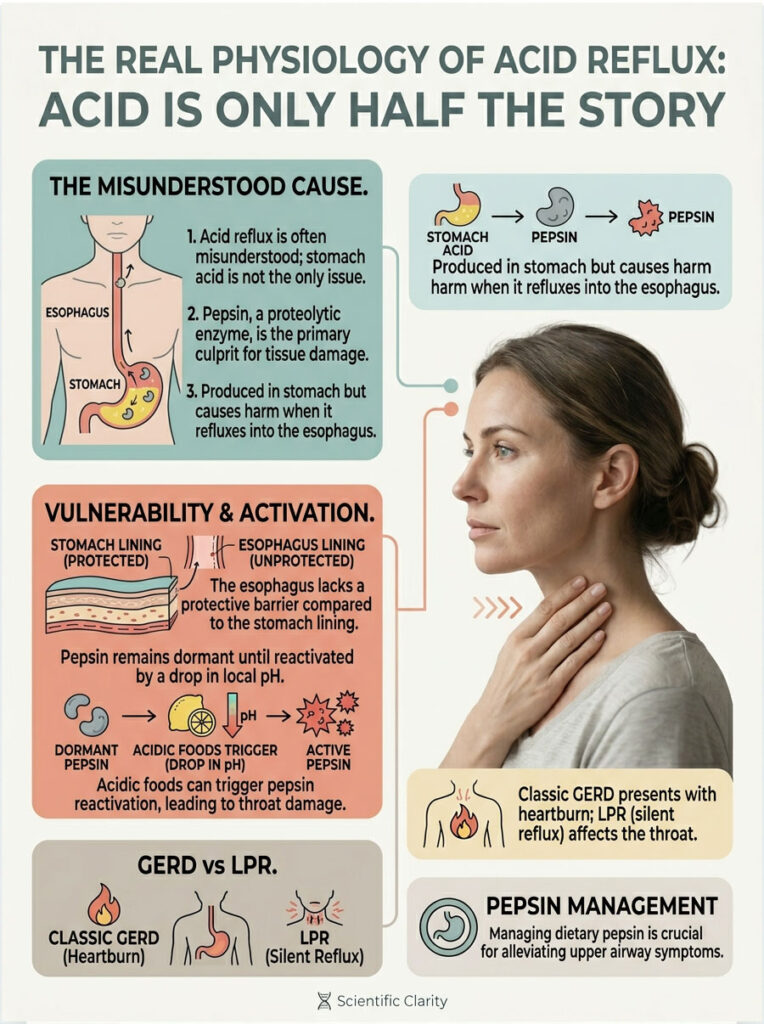
To understand why dietary changes work so well, you need to shift your focus away from hydrochloric acid and toward a proteolytic enzyme called pepsin. Pepsin is the actual biological culprit behind severe tissue damage in your esophagus and throat. It explains why your throat still burns even on maximum-dose acid blockers.
How Pepsin Damages Your Tissue
Pepsin is produced by chief cells deep in the stomach lining. Its job is to break down dietary protein into smaller, absorbable peptides. Inside the acidic stomach, pepsin works perfectly without harming the thick mucosal lining.
The problem starts when gastric contents reflux upward. Your esophagus, throat, and vocal cords do not have the same protective barrier. When pepsin travels up with stomach acid, it coats the sensitive tissues of your upper digestive and respiratory tracts. It physically binds to your cells and sits there in a dormant state, waiting for the right conditions to reactivate.
The Reactivation Cycle
This is where pH becomes critical. When you swallow something acidic, the local pH in your throat drops. That drop acts like a biological alarm clock for the dormant pepsin. The acidic environment reactivates the enzyme, and since pepsin is designed to digest protein, and your esophageal tissue is made of protein, the enzyme starts digesting your own throat.
This cycle is exactly why you feel burning after eating a simple tomato or drinking black coffee. The food itself is not burning you through direct contact. It is lowering the local pH, which wakes up the pepsin, which then causes localized tissue digestion.
Classic GERD vs. Silent Reflux (LPR)
Classic GERD typically causes the familiar burning chest pain known as heartburn, with damage mostly concentrated in the lower esophagus.
Laryngopharyngeal Reflux (LPR), also called silent reflux, is a different animal. It often presents without any heartburn at all. Instead, patients deal with chronic throat clearing, a persistent lump sensation, hoarseness, and a dry cough. The pepsin in LPR travels much higher, reaching the vocal folds, which are microscopically delicate and easily damaged by even trace amounts of the enzyme.
This makes dietary pepsin inactivation the primary clinical goal for anyone dealing with upper airway symptoms.
What the Alkaline Diet Actually Means for GERD
If you search for alkaline diet advice online, you will find a mountain of conflicting information. Wellness influencers have twisted the concept into something barely recognizable to medical professionals. So let us set the record straight.
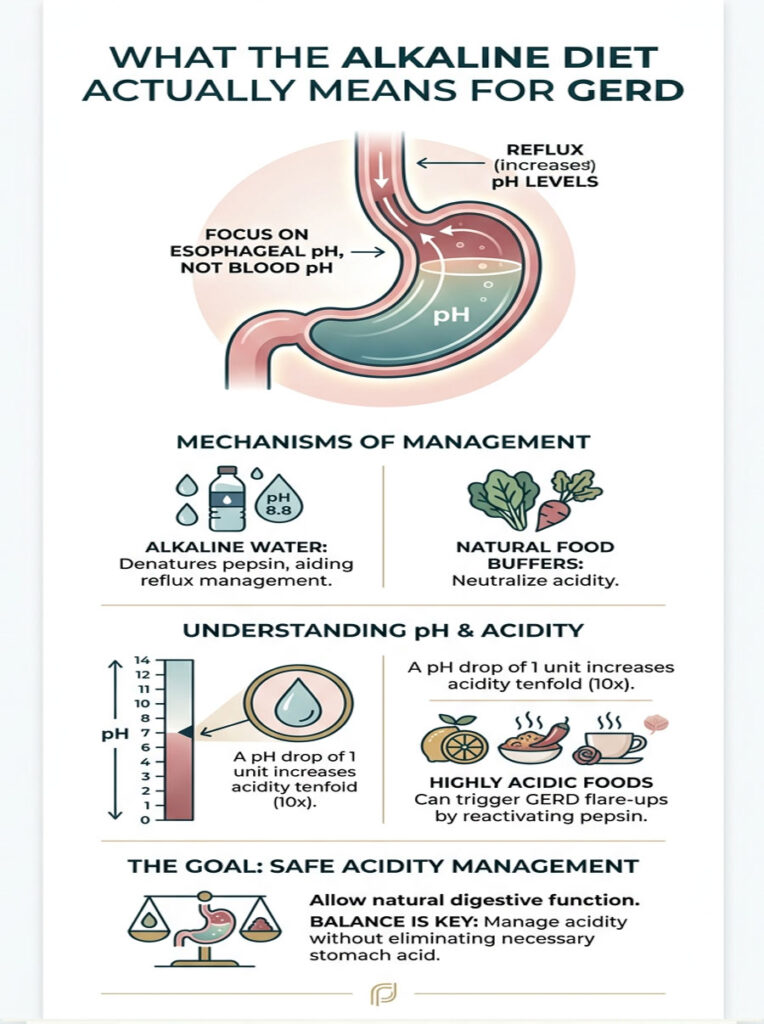
The medical goal of an alkaline diet for reflux is not to change your blood pH. Your body regulates blood pH between 7.35 and 7.45 through complex lung and kidney mechanisms, and no food will change that. The real goal is to control the pH of what passes through your throat and esophagus. By managing this local environment, you achieve direct mucosal protection and healing.
Why Alkaline Water at pH 8.8 Matters
Standard drinking water sits around a neutral pH of 7.0. That is healthy for hydration, but not high enough to neutralize the pepsin bound to your esophageal tissues.
Laboratory data shows that water at pH 8.8 or higher permanently denatures human pepsin. “Denaturing” means the enzyme loses its three-dimensional structure completely. Once pepsin is denatured, it cannot be reactivated, no matter what you eat afterward. This permanent deactivation is the cornerstone of long-term reflux management.
Natural Bicarbonate Buffers in Food
Beyond alkaline water, your everyday food choices provide powerful natural buffers. Dark leafy greens and starchy root vegetables are rich in plant bicarbonates. These compounds act like a chemical sponge for excess acid in your digestive tract.
When you eat a big plate of spinach, kale, or roasted sweet potatoes, you introduce these buffers directly into your stomach. They help neutralize harsh gastric contents right after eating, reducing the destructive potential of any fluid that refluxes upward. It is a completely safe, natural way to manage acidity without shutting down acid production entirely.
Understanding the pH Scale
The pH scale is logarithmic. Each whole number drop represents a tenfold increase in acidity. A food at pH 4.0 is not slightly more acidic than one at pH 5.0. It is ten times more acidic. A soda at pH 3.0 is one hundred times more acidic than a food at pH 5.0.
This exponential math explains why a single slip can trigger a major flare. One highly acidic drink introduces an overwhelming flood of hydrogen ions into your esophagus, reactivating millions of dormant pepsin molecules and undoing weeks of careful healing.
Clinical Evidence: Can Diet Really Compete with Medication?
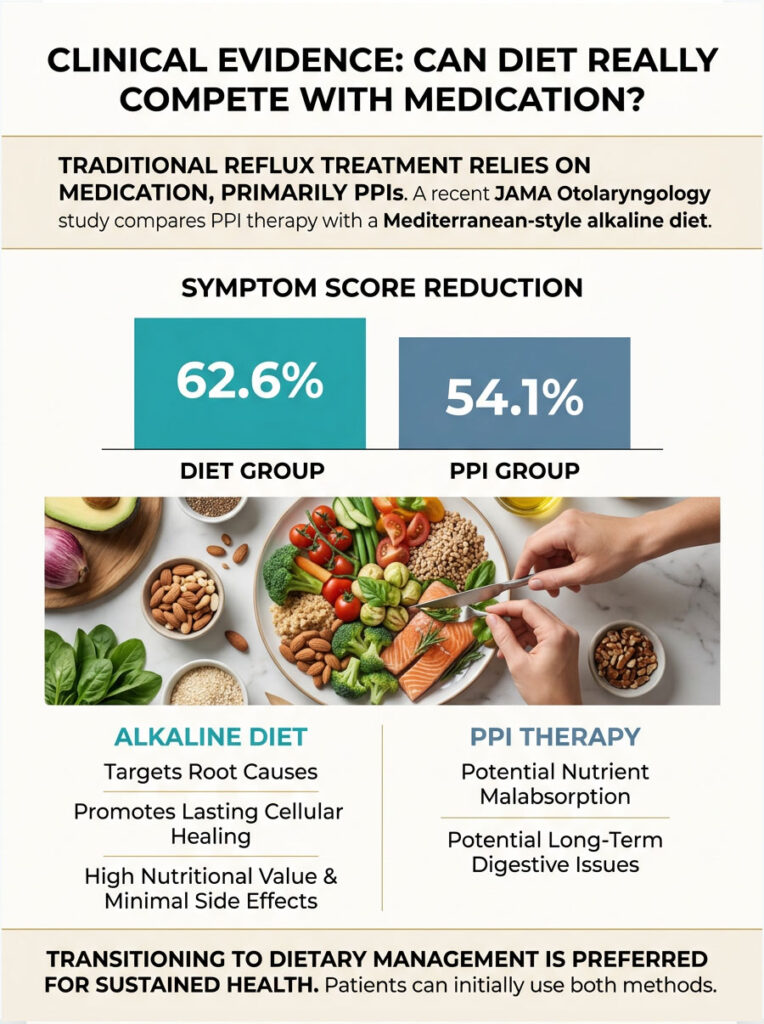
For decades, the standard treatment for reflux has been daily prescription acid blockers, primarily Proton Pump Inhibitors (PPIs). But recent high-quality clinical evidence has seriously challenged that approach..
The JAMA Otolaryngology Study
A pivotal study published in JAMA Otolaryngology directly compared traditional PPI therapy against a strict Mediterranean-style alkaline diet with daily alkaline water. Both patient groups were closely monitored for symptom resolution using the validated Reflux Symptom Index (RSI).
The results were striking. The diet group achieved a 62.6% reduction in total symptom scores. The PPI group achieved only a 54.1% reduction. The dietary intervention matched, and in several metrics outperformed, aggressive pharmaceutical treatment.
This study validated what clinical dietitians have observed for years: a properly structured nutritional plan provides lasting cellular healing by targeting the root cause, not just suppressing a chemical symptom.
Alkaline Diet vs. PPI Therapy: Side-by-Side Comparison
| Feature | PPI Medication | Alkaline Diet Protocol |
| How it works | Shuts down stomach acid production at the parietal cell level | Neutralizes dietary acid and permanently destroys tissue-bound pepsin |
| Side effects | Nutrient malabsorption, gut flora disruption, rebound acid on cessation | High nutritional value, virtually no negative side effects |
| Digestive impact | Can slow gastric emptying due to low acid levels | Plant fiber improves motility and overall digestion |
| Pepsin inactivation | Does nothing to denature pepsin already in the throat | Alkaline water (pH 8.8+) permanently destroys tissue-bound pepsin |
| Long-term outlook | Severe acid rebound if medication is stopped abruptly | Sustainable, lifelong lifestyle modification |
This comparison highlights a critical gap. Pills reduce acid but completely ignore the pepsin already attached to your esophagus. Nutrition therapy targets both sides of the equation simultaneously.
Long-term acid suppression also compromises your body’s absorption of essential minerals like calcium and magnesium. A nutrient-dense, plant-forward diet naturally provides those minerals in bioavailable forms. You replace a nutrient-depleting intervention with a nutrient-restoring one.
Many patients successfully use both approaches during the initial healing phase. But the long-term clinical goal is almost always a full transition to dietary management.
The 28-Day Healing Timeline: What to Expect
When patients first come to my clinic, they want to know how long it takes to feel better. In my experience, 95% of patients who keep their dietary pH strictly above 5.0 see significant relief within 28 days. Consistency during this window is everything.

You cannot cheat. Even one highly acidic meal can reactivate millions of dormant pepsin molecules and reset your healing progress to zero.
Weeks 1 and 2: Desensitization and Early Repair
During the first week, the main goal is calming inflamed tissues. Patients with silent reflux often notice a dramatic drop in throat clearing. That constant burning slowly begins to dull as nerve endings settle down.
By week two, deeper cellular repair begins. Inflammatory markers associated with erosive esophagitis start to drop. Swallowing becomes easier, and the “lump in the throat” feeling usually fades. You might feel mild fatigue as your immune system focuses on localized healing. Stay well hydrated with high-pH water during this phase.
Weeks 3 and 4: Regeneration and Functional Restoration
In week three, your esophagus starts laying down healthy new mucosal tissue. Redness and swelling visible on endoscopy decrease noticeably. Patients often report sleeping through the night for the first time in years.
By week four, the focus shifts to restoring Lower Esophageal Sphincter (LES) function. As tissue inflammation subsides, this muscular valve can close more tightly, preventing future reflux episodes.
Completing the 28-day cycle is a major milestone, but it is not a license to return to old habits. Your newly regenerated tissue is healthy but still somewhat fragile. Reintroduce foods slowly and test your personal tolerance levels.
Expert Tip: Keep a Food and pH Journal
Track everything you eat during your first 28 days, along with the approximate pH and your symptom severity on a 1-to-10 scale. This data is clinically invaluable for identifying hidden triggers that may be stalling your progress.
What to Eat (and What to Avoid) on the Alkaline Diet for GERD
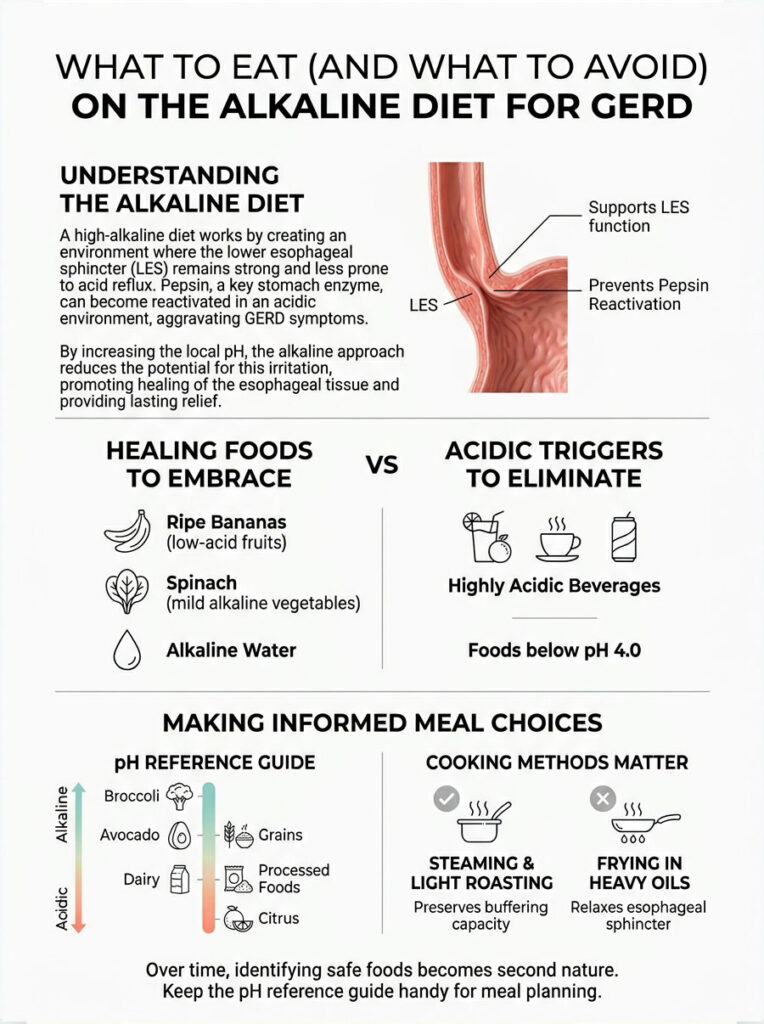
Understanding the science is step one. Translating it into daily meals is where the real work happens. Your goal is to support LES function while preventing pepsin reactivation, and you do that by choosing whole, unprocessed foods that sit high on the pH scale.
Healing Foods to Embrace
- Melons and bananas: Naturally high pH above 5.0. Cantaloupe, honeydew, and watermelon are excellent daily snacks or smoothie bases.
- Leafy greens and root vegetables: Spinach, kale, fennel, carrots, and sweet potatoes are your primary bicarbonate buffers. Build your lunches and dinners around them.
- Oatmeal and whole grains: Plain oatmeal absorbs excess gastric acid like a sponge. Pair it with unsweetened almond milk and sliced bananas.
- Fresh ginger root: A natural pro-kinetic agent that helps your stomach empty faster, reducing upward pressure on the esophageal valve.
Acidic Triggers to Eliminate
To achieve permanent pepsin inactivation, you need to cut any foods that drop your local pH below 4.0.
- Sodas and carbonated drinks: Completely off-limits. Carbonation forces the esophageal valve open, and diet sodas often have a pH between 2.5 and 3.0.
- Caffeinated coffee, raw citrus, cooked tomatoes, and raw onions: All of these dramatically lower esophageal pH and trigger immediate pepsin reactivation.
- Processed foods with hidden acids: Ascorbic acid, citric acid, and phosphoric acid are everywhere in packaged products. Read labels carefully.
pH Reference Guide for Common Foods
| Food / Beverage | Approx. pH | Classification | What to Do |
| Cola and diet soda | 2.5 – 3.0 | Highly acidic | Avoid permanently |
| Black coffee / espresso | 4.8 – 5.0 | Acidic / valve relaxer | Avoid during 28-day healing |
| Ripe bananas | 5.0 – 5.2 | Low acid / safe | Eat daily |
| Cantaloupe / melon | 6.1 – 6.5 | Mildly alkaline | Excellent for healing |
| Fresh spinach (raw) | 6.5 – 6.8 | Mildly alkaline | Eat daily for buffering |
| Alkaline water | 8.8 – 9.5 | Highly alkaline | Drink daily (therapeutic) |
Keep this reference handy when meal planning. Over time, identifying safe foods becomes second nature. And remember: cooking method matters. Steaming and light roasting preserve a food’s natural buffering capacity, while frying in heavy oils introduces compounds that relax the esophageal sphincter.
A Sample Day on the Alkaline Diet for GERD
This meal plan keeps your dietary pH above 5.0 all day, provides continuous bicarbonate buffering, and avoids all known sphincter-relaxing triggers.
Breakfast: The Soothing Start
Start with a large glass of room-temperature alkaline water (pH 8.8) to wash away overnight pepsin. Follow with organic oatmeal prepared with unsweetened almond milk, topped with sliced bananas, crushed walnuts, and a small drizzle of pure maple syrup.
Lunch: The Bicarbonate Buffer
Build a big salad with fresh spinach, cucumbers, shaved fennel, and shredded carrots. Top with grilled, unseasoned chicken breast, extra virgin olive oil, and a pinch of sea salt.
Dinner: The Pro-Kinetic Plate
Keep it light and easy to digest. Bake a wild-caught salmon filet and serve alongside roasted sweet potatoes and steamed zucchini. Grate fresh ginger into a light glaze for the salmon to promote faster gastric emptying before bedtime.
Snacks and Hydration
Reach for fresh cantaloupe chunks, raw almonds, or plain rice cakes with almond butter. Always pair snacks with at least eight ounces of alkaline water.
Timing matters: drink most of your alkaline water between meals, not during them. Large amounts of liquid with food distend the stomach and push the esophageal valve open.
Grocery Shopping: How to Spot Hidden Acids
The modern grocery store is a minefield for reflux sufferers. Manufacturers hide highly acidic preservatives in nearly every packaged product. You need to become an aggressive label reader.
Chemical Preservatives to Watch For
- Ascorbic acid: Concentrated Vitamin C used to extend shelf life. Drops your throat pH and reactivates dormant pepsin.
- Citric acid: Found in canned goods, bottled teas, and flavored waters. Even small amounts make a “safe” food dangerous.
- Phosphoric acid: Used in dark sodas and some processed meats. This chemical is so acidic it is used in industrial rust removal.
The Perimeter Shopping Strategy
Spend 90% of your time in the outer perimeter of the store, where fresh produce, meats, and dairy alternatives live. The inner aisles are mostly shelf-stable processed foods loaded with acidic preservatives.
When you do venture to the middle aisles for staples like oatmeal or olive oil, stick to single-ingredient products. If the ingredient list reads like a chemistry textbook, put the box back.
Three Reflux Myths That Need to Die
The internet is full of well-meaning advice that can actually make your condition worse. Here are three of the most dangerous myths I correct in my clinic every week.
Myth 1: Lemon Water Cures Reflux
The popular theory says lemon juice becomes alkaline after digestion. While lemon ash is alkalizing to urine, this completely ignores the anatomical journey of the liquid. Raw lemon juice has a pH of about 2.0. When you swallow it, that acid washes directly over your raw throat and damaged esophagus, instantly reactivating every dormant pepsin molecule in its path.
For anyone with active LPR, drinking lemon water is like pouring acid on an open wound. Focus on the actual pH of the food as it touches your tissue, not its theoretical post-digestive state.
Myth 2: Apple Cider Vinegar Fixes Reflux
The theory here is that reflux is caused by too little stomach acid, so you should drink ACV. While true low stomach acid (hypochlorhydria) does exist in a small fraction of people, blindly prescribing ACV to someone with an inflamed, ulcerated esophagus is reckless.
Raw ACV has a pH of roughly 2.5 to 3.0. Swallowing concentrated vinegar will severely burn exposed tissue and sabotage any healing progress. If you have erosive esophagitis, avoid it entirely.
Myth 3: Milk Soothes Heartburn
Cold milk does temporarily coat the stomach lining and provide a brief cooling sensation. But dairy milk is high in both animal fat and calcium, both of which are powerful stimulants for gastric acid production.
Once that initial coating wears off, your stomach triggers a massive acid rebound that leaves you in more pain than before. Stick to plant-based milks like oat or almond milk, which soothe without triggering an acid surge.
How to Safely Transition from PPIs to the Alkaline Diet
If you are currently on prescription acid blockers, your first instinct after reading this might be to stop taking them immediately. Please do not do that.
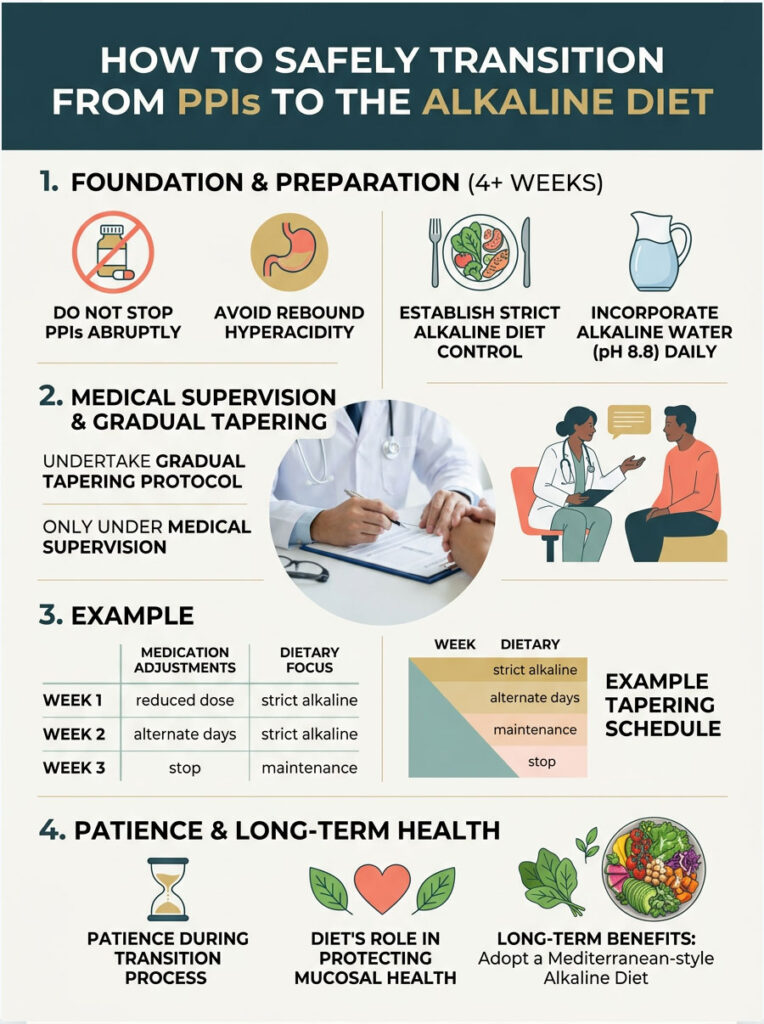
Stopping PPIs abruptly triggers a severe physiological reaction called rebound hyperacidity. When you take PPIs for an extended period, your stomach compensates by increasing gastrin production and physically enlarging its acid-producing cells. The moment you stop the medication, those hyperactive cells go into overdrive, flooding your system with acid.
The Safe Tapering Protocol
Before touching your medication dose, establish strict dietary control. Follow the alkaline diet perfectly for at least four full weeks. Integrate alkaline water at pH 8.8 and master your meal planning. This prepares your digestive tract for the eventual increase in natural stomach acid.
Once your dietary foundation is solid, your doctor will slowly reduce your dosage over weeks or months. By maintaining strict mucosal protection through diet, you can comfortably absorb the mild acid rebound during the taper.
Example Tapering Schedule
| Phase | Medication Adjustment | Dietary Focus |
| Weeks 1-4 | Maintain full dose | Strict pH 5.0+ foods, daily alkaline water |
| Weeks 5-6 | Reduce by 25%, or alternate full dose every other day | Increase raw greens and bicarbonate buffer intake |
| Weeks 7-8 | Reduce to 50% of original dose | Avoid all fats and heavy meals before bedtime |
| Weeks 9-10 | Switch to a milder H2 blocker if needed | Perfect hydration with alkaline water between meals |
| Week 11+ | Discontinue all daily acid blockers | Lifelong Mediterranean-style alkaline protocol |
This gradual approach gives your enlarged parietal cells time to shrink back to normal size and prevents a gastrin surge from overwhelming your esophagus. Patience is essential during this transition.
Long-Term Protection: Why This Is a Lifelong Commitment
Getting initial relief is a wonderful milestone, but it is not the finish line. The ultimate goal of the alkaline diet and GERD protocol is permanent disease prevention.

Chronic, unchecked inflammation in the esophagus is not just painful. It is dangerous. When tissue is repeatedly exposed to acid and reactivated pepsin for years, the cells eventually mutate to survive the harsh environment. This mutation is a serious medical red flag.
Preventing Barrett’s Esophagus
When normal esophageal cells mutate into intestinal-type columnar cells, the condition is called Barrett’s Esophagus. This is a precancerous state directly linked to chronic, unmanaged reflux, and it dramatically raises the risk of esophageal adenocarcinoma.
By maintaining an alkaline, soothing environment in the throat and esophagus, you halt the inflammatory cascade that drives these mutations. Consistent daily pepsin inactivation ensures your vulnerable tissue is never again subjected to the enzymatic digestion that triggers cell changes.
Lifestyle Changes That Amplify the Alkaline Diet
Diet is the foundation, but certain lifestyle adjustments act as powerful force multipliers.

Sleep Mechanics and Gravity
- Stop eating at least three hours before bed. Lying flat with a full stomach removes the benefit of gravity and lets acidic contents press against the esophageal valve all night.
- Elevate the head of your entire bed by six to eight inches. Do not just stack pillows, as this bends the stomach and increases upward pressure. Raise the mattress itself.
- Sleep on your left side. Due to the anatomical shape of the stomach, left-side sleeping keeps the acid pool safely below the sphincter. Right-side sleeping dumps acid onto the valve.
Pressure and Stress Management
Wear loose-fitting clothing around your waist. Tight belts and restrictive shapewear squeeze the stomach and force acid upward. Maintaining a healthy body weight also reduces this physical stress.
Do not underestimate the gut-brain connection. Chronic stress and elevated cortisol increase the frequency of spontaneous valve openings (transient LES relaxations), which cause reflux. Daily meditation, deep breathing, or gentle yoga can calm the nervous system, which directly calms the digestive system.
Summary and Key Takeaways
Healing your digestive tract takes patience, discipline, and a real understanding of the science. The clinical connection between an alkaline diet and GERD is rooted in proven biochemistry: tissue protection and permanent enzyme deactivation.
By controlling the pH of your daily meals, you take full control of your own healing. You stop being a passive participant relying on PPIs to mask pain. You start actively repairing your esophageal mucosa at the cellular level.
The core mechanism is simple but powerful: alkaline water at pH 8.8 permanently destroys pepsin. A diet rich in plant-based buffers continuously neutralizes excess acid. Together, these strategies provide comprehensive relief for both classic heartburn and silent reflux.
Core Takeaways
- Tissue-bound pepsin, not just acid, is the primary enzyme digesting your esophagus.
- Alkaline water at pH 8.8 or higher permanently denatures and destroys dormant pepsin.
- Strictly avoid all foods below pH 5.0 during your initial 28-day healing phase.
- Never stop PPIs abruptly. Work with your doctor on a gradual tapering plan.
- Build your diet around leafy greens, melons, bananas, and root vegetables for natural buffering.
- Read labels aggressively to avoid hidden ascorbic acid, citric acid, and phosphoric acid.
- Stop eating three hours before bed and elevate the head of your mattress six to eight inches.
Frequently Asked Questions
How does an alkaline diet specifically help heal the damage from GERD?
An alkaline diet helps by maintaining a dietary pH above 5.0, which prevents the reactivation of dormant pepsin bound to your esophageal tissue. While traditional medications focus solely on suppressing hydrochloric acid, this nutritional approach targets the proteolytic enzyme pepsin, which is the actual biological culprit behind tissue digestion and chronic inflammation.
Why is alkaline water with a pH of 8.8 recommended over standard purified water?
Clinical research demonstrates that water with a pH of 8.8 or higher is required to permanently denature human pepsin. Standard purified water, which usually has a neutral pH of 7.0, is not alkaline enough to structurally disable the enzyme. By drinking pH 8.8 water, you effectively wash away and deactivate the enzymes responsible for damaging your throat and esophagus.
What is the difference between classic GERD and silent reflux (LPR)?
Classic GERD typically presents with heartburn and localized damage in the lower esophagus. Laryngopharyngeal Reflux (LPR), or silent reflux, often lacks heartburn but involves aerosolized pepsin traveling higher into the respiratory tract. This causes symptoms like chronic throat clearing, hoarseness, and a persistent cough, making it extremely sensitive to even minor pH drops.
Can I use lemon water or apple cider vinegar as a natural remedy for reflux?
As a clinical specialist, I strongly advise against this. While some claim these substances have an ‘alkalizing’ effect after digestion, their initial pH is highly acidic (around 2.0 to 3.0). When swallowed, they immediately reactivate dormant pepsin on contact with your throat and esophagus, causing immediate tissue damage and prolonging the healing process.
How long does it take to see significant improvement on an alkaline diet?
According to the ’95 Percent Rule’ observed in clinical practice, 95 percent of patients who strictly adhere to a dietary pH above 5.0 see significant symptom reduction within 28 days. This timeline allows for neurological desensitization, initial cellular repair, and the regeneration of the esophageal mucosa.
What are the most dangerous ‘hidden’ acids I should look for on food labels?
You must be vigilant for chemical preservatives like citric acid and ascorbic acid, which are frequently added to processed foods and bottled beverages. These additives significantly lower the Hydrogen Ion Concentration of the product, often dropping the pH to destructive levels between 2.5 and 3.0, which triggers immediate enzymatic damage.
Why is drinking milk for heartburn relief considered a myth?
While milk provides a temporary cooling sensation, it is high in animal fat and calcium, both of which are powerful triggers for gastric acid production. This leads to a ‘rebound effect’ where the stomach produces an excess of acid shortly after consumption, often resulting in more severe pain than before the milk was consumed.
Which foods act as the best natural bicarbonate buffers for the stomach?
Dark leafy greens like spinach and kale, along with starchy root vegetables like sweet potatoes and carrots, are excellent natural sources of plant-based bicarbonates. These compounds act as chemical sponges, neutralizing excess gastric acid postprandially without disrupting your body’s natural digestive processes.
Is it safe to stop taking my PPI medication once I start an alkaline diet?
You should never stop Proton Pump Inhibitors (PPIs) abruptly. Long-term use often leads to hypergastrinemia and enlarged acid-producing cells. Stopping suddenly causes rebound hyperacidity. Instead, you should establish strict dietary control for at least four weeks and then work with your physician to implement a slow, phased tapering protocol.
How do sleep mechanics influence the success of an alkaline diet protocol?
Mechanical factors are crucial for protecting the esophageal mucosa. By stopping all food intake three hours before bed and sleeping on your left side with the head of the mattress elevated, you utilize gravity and anatomical positioning to keep gastric contents safely below the Lower Esophageal Sphincter (LES).
What role does fresh ginger play in managing acid reflux?
Fresh ginger root is a potent natural pro-kinetic agent. This means it stimulates the stomach to empty its contents into the small intestine more rapidly. Faster gastric emptying reduces the intra-abdominal pressure against the esophageal valve, significantly lowering the risk of spontaneous reflux episodes.
What is the long-term risk of failing to manage chronic reflux through diet?
Unmanaged reflux can lead to Barrett’s Esophagus, a precancerous condition where normal esophageal cells mutate into intestinal-type cells due to chronic acid and pepsin exposure. A strict alkaline diet protocol is a vital preventative measure to halt the inflammatory cascade and protect against the development of esophageal adenocarcinoma.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. The “Alkaline Diet and GERD” protocol involves significant dietary changes and the potential tapering of prescription medications. Always consult a qualified healthcare professional or gastroenterologist before making health decisions or altering your medication regimen.
References
- JAMA Otolaryngology–Head & Neck Surgery – Comparison of Dietary and Pharmaceutical Interventions for Laryngopharyngeal Reflux – Clinical study showing 62.6% symptom reduction using an alkaline diet.
- Annals of Otology, Rhinology & Laryngology – Potential Benefits of pH 8.8 Alkaline Drinking Water as an Adjunct in the Treatment of Reflux Disease – Research on the permanent denaturation of human pepsin.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – Acid Reflux (GER & GERD) in Adults – Official statistics on prevalence and traditional management of chronic reflux.
- American College of Gastroenterology – Guidelines for the Diagnosis and Management of Gastroesophageal Reflux Disease – Clinical standards for GERD and Barrett’s Esophagus monitoring.
- Journal of Digestive Diseases – The Role of Diet in the Development and Management of Gastroesophageal Reflux Disease – Review of plant-based and high-fiber diets on gastric motility.
- Annals of the New York Academy of Sciences – Pepsin and its Role in the Pathogenesis of Reflux Disease – Detailed analysis of enzymatic tissue damage in the esophagus and throat.