If you have ever taken a round of antibiotics and ended up spending more time in the bathroom than you expected, you are not alone. It is one of the most common questions patients bring to my gastroenterology clinic every week: can antibiotics cause diarrhea?
Table of Contents
The short answer is yes, and it happens far more often than most people realize.
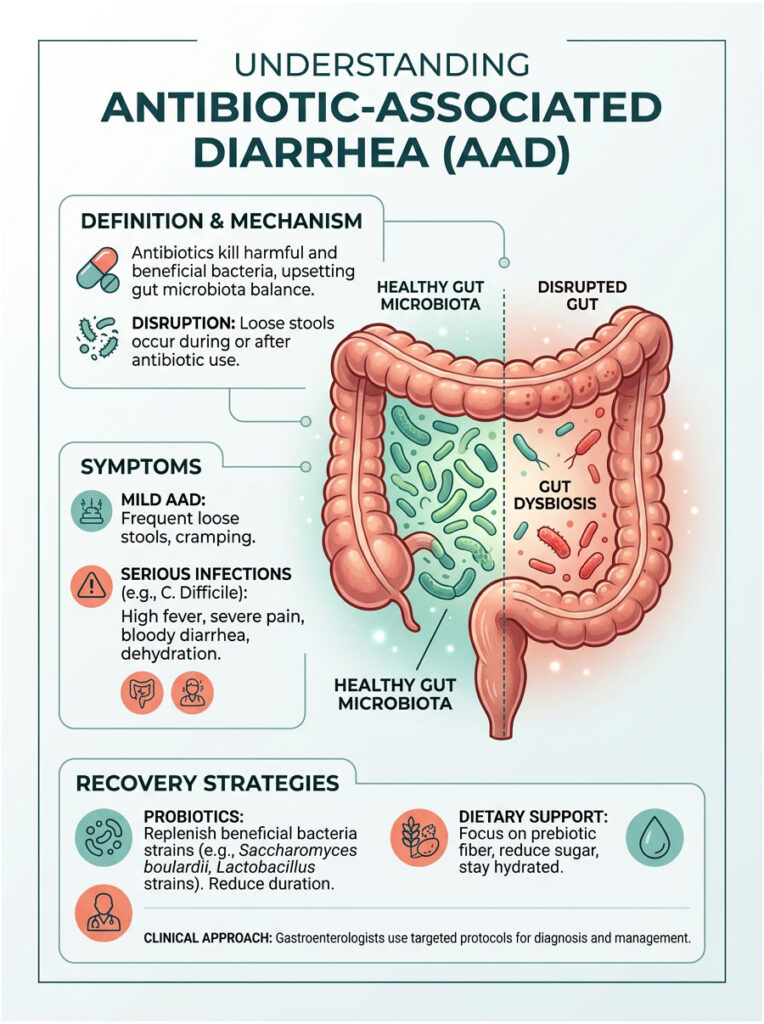
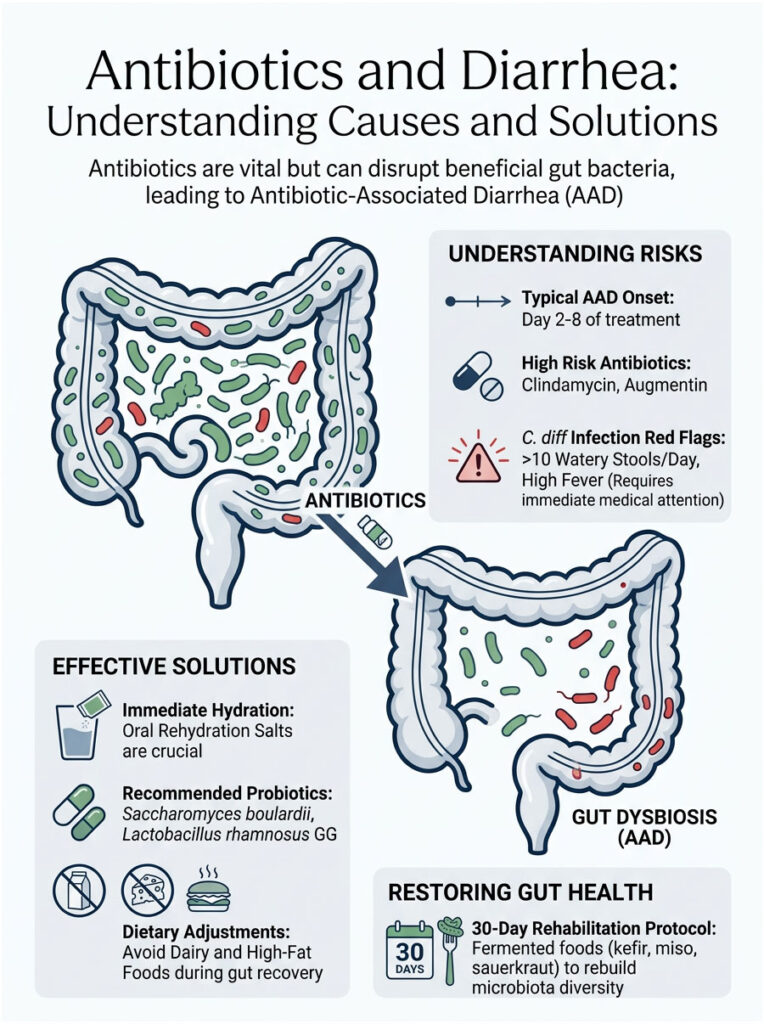
Antibiotics are life-saving medications. They clear dangerous bacterial infections that our bodies cannot fight alone. But here is the trade-off: these drugs do not distinguish between harmful bacteria causing your infection and the beneficial bacteria keeping your gut healthy. When antibiotics wipe out the good bacteria along with the bad, you are left with a condition called Antibiotic-Associated Diarrhea, or AAD.
This disruption creates gut dysbiosis, a severe microbial imbalance inside your intestines. Your colon suddenly loses the protective barrier it depends on. Without that barrier, you become vulnerable to everything from mild loose stools to serious infections like Clostridioides difficile.
In this guide, we will break down exactly why antibiotics upset your stomach, how to tell the difference between a normal side effect and a medical emergency, and what you can do to recover quickly. You will learn about targeted probiotic therapies, precise dietary strategies, and the clinical protocols gastroenterologists actually use to help patients heal.
Quick Answer: Can Antibiotics Cause Diarrhea?
Yes. Antibiotics kill beneficial bacteria in your digestive tract alongside the harmful ones. This sudden loss of healthy flora leads to gut dysbiosis, resulting in loose, watery stools. Most cases resolve within a few days of finishing the medication, but severe cases require immediate medical attention.
Key Clinical Statistics
- Up to 30% of patients taking broad-spectrum antibiotics develop Antibiotic-Associated Diarrhea.
- Clostridioides difficile causes nearly 500,000 infections in the United States every year, according to the CDC.
- AAD symptoms typically begin between the 2nd and 8th day of antibiotic therapy.
- Children under 2 and adults over 65 face the highest risk for severe gastrointestinal complications.
- Specific probiotic strains can reduce AAD risk by up to 42%.
- Fecal Microbiota Transplantation (FMT) cures over 90% of recurrent C. diff infections.
Why Do Antibiotics Cause Diarrhea and Stomach Upset?
To understand why these medications upset your stomach, you need to look at the human microbiome. Your digestive tract is home to trillions of microscopic organisms. These bacteria, fungi, and viruses live in a delicate, symbiotic relationship with your intestinal lining. They help you digest food, produce essential vitamins, and protect against dangerous invaders.

When you swallow an antibiotic, you are essentially dropping a chemical bomb into this ecosystem. The medication travels through your stomach and into your intestines, where it begins destroying bacteria indiscriminately. It simply cannot tell the difference between good and bad cells.
This rapid destruction changes how your colon absorbs water and processes nutrients. That internal disruption is the primary reason so many patients develop sudden digestive issues during antibiotic treatment.
The Anatomy of Gut Dysbiosis
Gut dysbiosis is a clinical term for a severe microbial imbalance inside your intestines. In a healthy gut, beneficial bacteria constantly crowd out harmful ones. They compete for nutrients and physical space along the intestinal wall, keeping dangerous pathogens from multiplying.
When antibiotics kill off those good bacteria, that competition vanishes. Opportunistic pathogens that normally exist in tiny numbers suddenly have room to grow. They feast on available nutrients and expand rapidly.
This imbalance irritates the mucosal lining of your large intestine. The irritation prevents your colon from absorbing water properly. All that unabsorbed water stays in your digestive tract, leading directly to loose, frequent bowel movements.
Broad-Spectrum vs. Narrow-Spectrum Antibiotics
Not all antibiotics cause the same level of disruption. In clinical practice, we divide these drugs into two main categories: narrow-spectrum and broad-spectrum.
Narrow-spectrum antibiotics target very specific types of bacteria. Because they are highly focused, they cause minimal collateral damage to your microbiome. Your risk of developing AAD stays relatively low.
Broad-spectrum antibiotics are a different story. Doctors prescribe them when they are unsure which specific bacterium is causing the infection. These powerful drugs wipe out a massive variety of bacterial strains at once, causing profound gut dysbiosis. Think of it as clear-cutting a forest to eliminate a few bad weeds. The entire ecosystem collapses in the process.
The Role of Short-Chain Fatty Acids (SCFAs)
Your healthy gut bacteria ferment dietary fiber to produce short-chain fatty acids, or SCFAs. The most important one for colon health is butyrate. Butyrate is the primary fuel source for colonocytes, the cells lining your colon.
When antibiotics kill the bacteria that produce SCFAs, your colon cells literally begin to starve. Starving colon cells cannot absorb water efficiently. All that unabsorbed water stays trapped in your intestines and flushes out as urgent, watery diarrhea. This is clinically known as osmotic diarrhea.
Bile Acid Malabsorption
Your liver produces bile acids to help digest dietary fats. Healthy gut bacteria normally break down these bile acids in your lower intestine so they can be recycled. When antibiotics destroy those specific bacteria, raw bile acids dump directly into your colon.
Bile acids are highly irritating to the tissue of the large intestine. They stimulate excess water secretion and speed up muscle contractions. This is exactly why many patients notice bright yellow diarrhea after antibiotics. The yellow color is literally raw, unabsorbed bile moving rapidly through the system.
Recognizing the Symptoms: Normal Side Effects vs. Medical Emergencies
One of the most important things I teach my patients is knowing when to wait it out and when to seek urgent medical care. Mild Antibiotic-Associated Diarrhea is annoying but generally harmless. However, severe infections triggered by gut dysbiosis can become life-threatening if ignored.
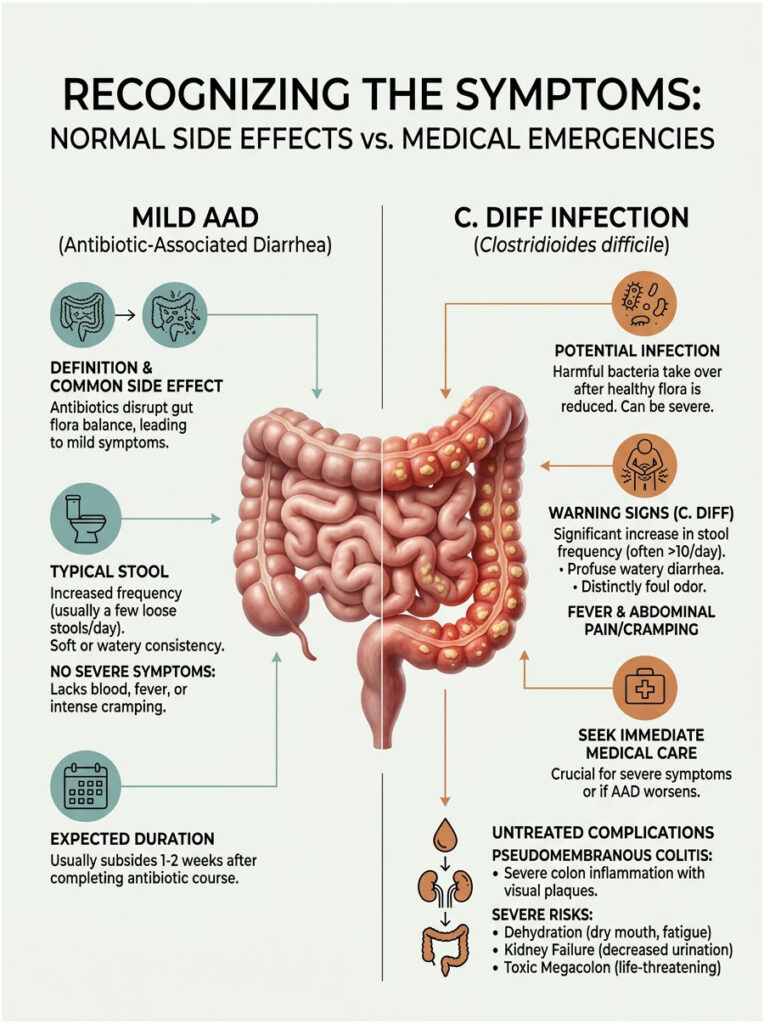
The key is monitoring the frequency, color, and accompanying symptoms closely. This observation will help you determine your actual risk level.
Mild Antibiotic-Associated Diarrhea
Mild AAD is extremely common. Symptoms usually appear a few days after starting a new prescription. You might notice two to four loose stools per day, mild abdominal cramping, gas, and bloating.
The stool is usually soft or somewhat watery, but not explosive. There is no high fever, no visible blood, and no severe pain. Mild AAD typically resolves on its own within one to seven days after you finish the medication, as your microbiome slowly begins to rebuild.
The Danger of Clostridioides difficile (C. diff) Infection
Now for the worst-case scenario. Clostridioides difficile is a highly aggressive, opportunistic bacterium that naturally lives in the environment and sometimes in the human gut as dormant spores.
When antibiotics eradicate your healthy bacteria, C. diff wakes up. Without good bacteria to keep it in check, it multiplies rapidly. The bacteria release powerful toxins that attack and destroy the lining of your colon.
Patients often experience up to 15 watery stools per day with a distinct, incredibly foul odor. High fever, severe abdominal pain, and profound weakness are common. If you experience these symptoms, contact your doctor immediately. Do not wait to see if it improves on its own.
Pseudomembranous Colitis and Systemic Complications
If a C. diff infection goes untreated, it can progress into pseudomembranous colitis, a massive inflammation of the large intestine. The toxins destroy the mucosal lining, causing raised, yellow-white plaques called pseudomembranes to form on the intestinal walls.
This condition causes intense pain, bloody diarrhea, severe dehydration, and can lead to acute kidney failure. In extreme cases, the colon becomes so inflamed that it stops moving entirely, a condition called toxic megacolon. Toxic megacolon can cause intestinal rupture, which is frequently fatal.
Mild AAD vs. C. diff Infection: Clinical Comparison
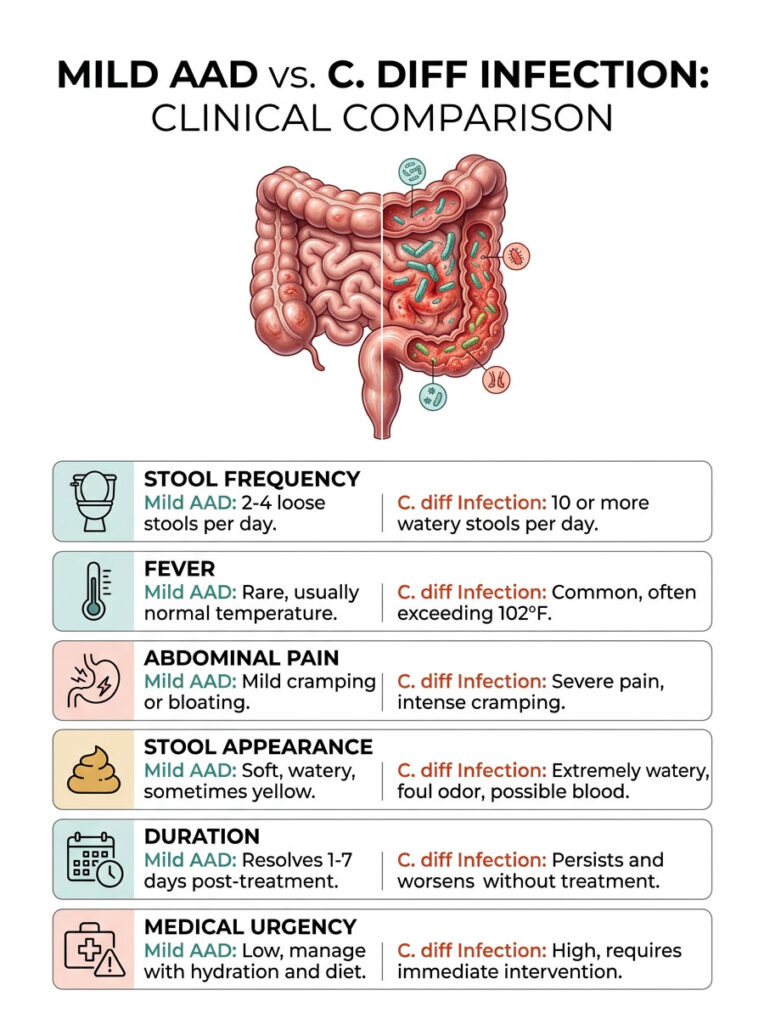
| Clinical Feature | Mild AAD | C. diff Infection |
| Stool Frequency | 2 to 4 loose stools per day | 10 or more watery stools per day |
| Fever | Rare, usually normal temperature | Common, often exceeding 102 F |
| Abdominal Pain | Mild cramping or bloating | Severe pain, intense cramping |
| Stool Appearance | Soft, watery, sometimes yellow | Extremely watery, foul odor, possible blood |
| Duration | Resolves 1 to 7 days post-treatment | Persists and worsens without treatment |
| Medical Urgency | Low, manage with hydration and diet | High, requires immediate intervention |
Which Antibiotics Cause the Most Digestive Disruption?
Not all prescriptions carry the same risk to your digestive system. Some drugs are notorious for destroying gut flora, while others are much gentler. Knowing which medication you are taking helps you anticipate problems before they start.
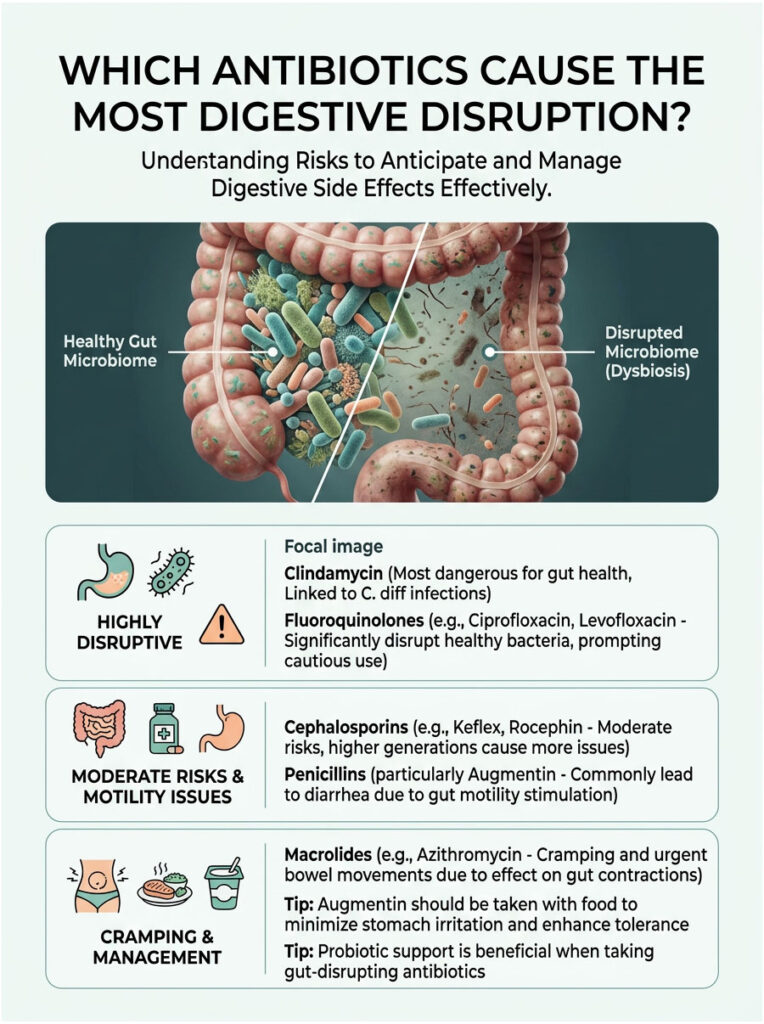
Clindamycin: The Biggest Offender
Clindamycin is historically the most dangerous antibiotic when it comes to triggering C. diff infection. It is a powerful lincosamide used for serious skin, bone, and dental infections. Dentists prescribe it frequently for stubborn tooth abscesses.
Clindamycin causes profound suppression of anaerobic gut flora, wiping out the exact bacteria needed to keep C. diff dormant. Even a single course can alter your microbiome for months. Proactive probiotic support is essential when taking this drug.
Fluoroquinolones: A High-Risk Category
Fluoroquinolones include widely used drugs like Ciprofloxacin (Cipro) and Levofloxacin (Levaquin). Doctors prescribe them for stubborn urinary tract infections and severe pneumonia.
These are potent broad-spectrum agents that eradicate massive amounts of healthy bacteria. The FDA has issued multiple black box warnings about their overuse. Their devastating impact on the digestive system is a primary reason clinicians are increasingly moving away from prescribing them.
Cephalosporins and Their Impact
Cephalosporins like Keflex or Rocephin are considered moderate-risk drugs. They significantly alter microbiota diversity but are slightly less likely to trigger a full C. diff infection than clindamycin.
The risk increases with each successive generation of the drug. First-generation cephalosporins are relatively mild, while third-generation versions are much harsher on the stomach. Expect some digestive discomfort, typically increased gas and softer stools within the first few days.
Penicillins and the Augmentin Problem
Penicillins are incredibly common worldwide. This class includes Amoxicillin and the popular combination drug Augmentin. Diarrhea after taking amoxicillin is one of the most frequent complaints I see in the clinic.
Augmentin combines amoxicillin with clavulanate potassium. The clavulanate acid acts as a direct stimulant to gut motility, chemically forcing your intestines to contract rapidly. Combined with bacterial die-off, this makes diarrhea a near-universal side effect.
Expert Tip: If you are prescribed Augmentin, always take it in the middle of a large meal. Taking it on an empty stomach allows the clavulanate acid to severely irritate your stomach lining, doubling your chances of watery stools.
Macrolides and Gut Motility
Macrolides include the famous Z-Pak (Azithromycin). These drugs chemically mimic a natural hormone called motilin, which triggers stomach contractions. When you take Azithromycin, your stomach and intestines begin to contract vigorously.
This causes cramping and urgent bowel movements. Interestingly, this is often a mechanical side effect rather than gut dysbiosis. The cramping usually stops the day after you finish the prescription.
Antibiotic Risk Levels for Digestive Disruption
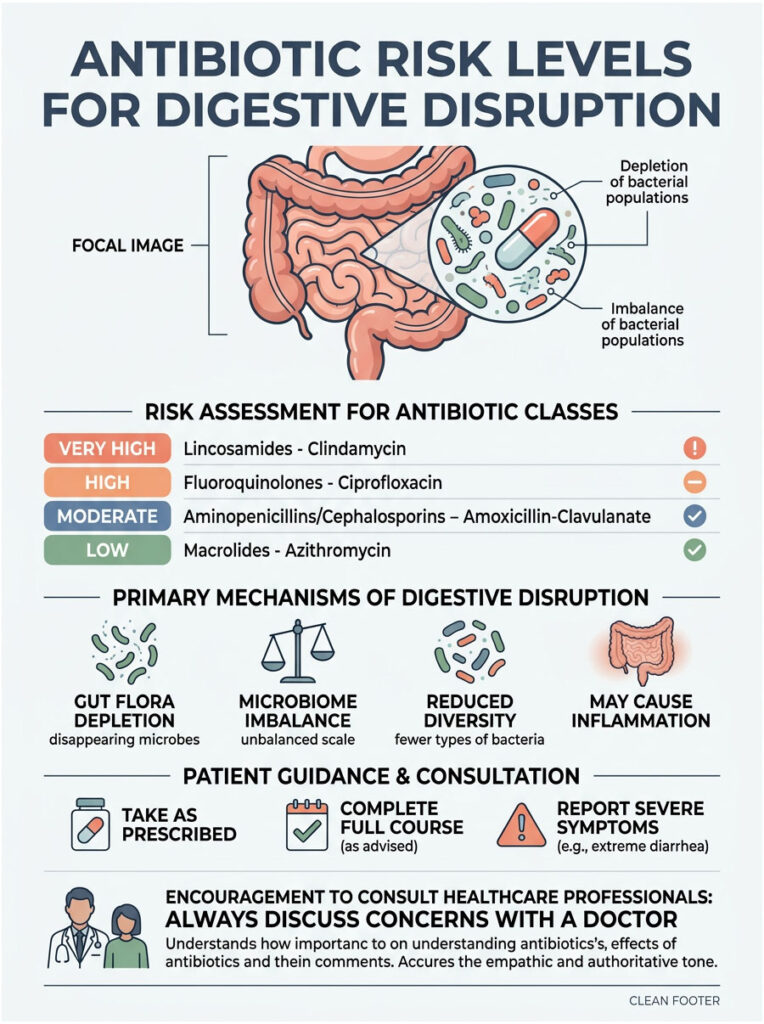
| Antibiotic Class | Common Names | Risk Level | Primary Disruption Mechanism |
| Lincosamides | Clindamycin | Very High | Profound suppression of anaerobic gut flora |
| Fluoroquinolones | Cipro, Levaquin | High | Broad-spectrum eradication of healthy bacteria |
| Penicillins | Augmentin | Moderate to High | Clavulanate stimulates gut motility directly |
| Cephalosporins | Keflex, Rocephin | Moderate | Alters flora diversity across generations |
| Macrolides | Azithromycin | Low to Moderate | Mimics motilin hormone, increases peristalsis |
How to Stop Diarrhea From Antibiotics: Evidence-Based Treatment
When you are running to the bathroom multiple times a day, you want relief fast. The internet is full of home remedies, but many are scientifically baseless. In clinical practice, we rely on evidence-based protocols that address both the symptoms and the root cause.
The primary goal is preventing dehydration while supporting your damaged microbiome. Here is the step-by-step protocol I recommend to my patients.
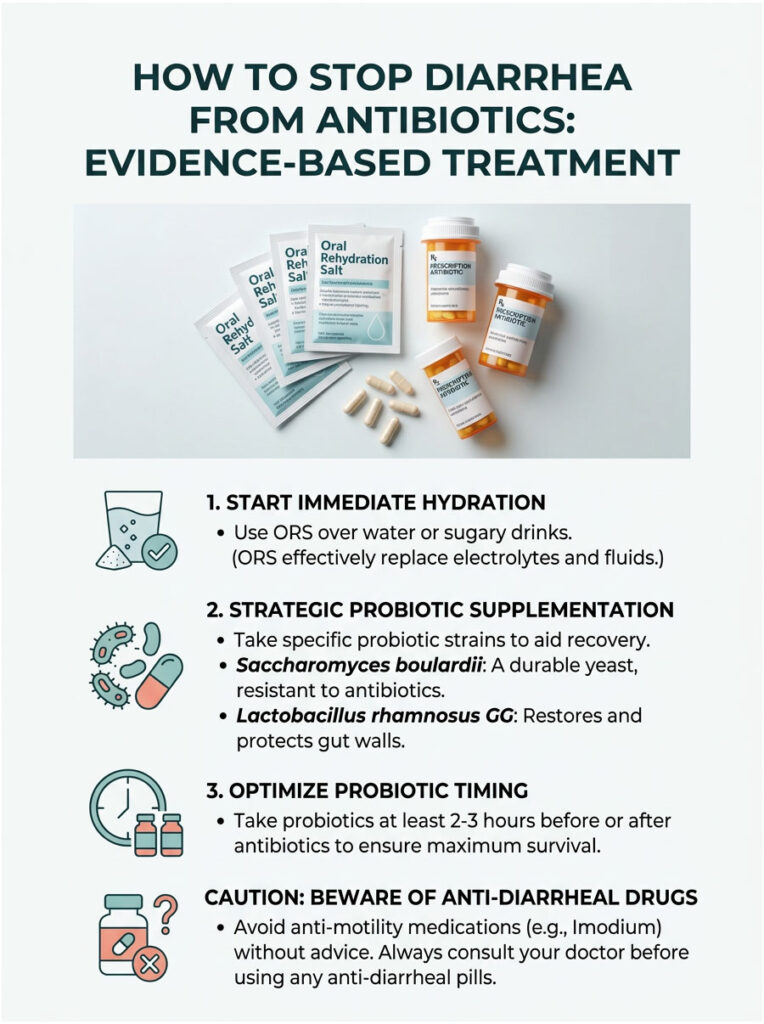
Immediate Hydration With Oral Rehydration Salts (ORS)
Dehydration is the most immediate danger with frequent loose stools. You are losing massive amounts of water, sodium, and potassium with every trip to the bathroom. Drinking plain water alone is not enough.
Plain water lacks the electrolytes needed to pull fluid back into your cells. This is why I recommend Oral Rehydration Salts (ORS), formulated to World Health Organization standards. They contain the precise ratio of sodium and glucose needed to activate the sodium-glucose cotransporters in your intestinal lining, forcing your gut to absorb water immediately.
Skip the sugary sports drinks. They contain too much sugar, which can actually worsen watery stools by drawing more water into the colon.
Strategic Probiotic Supplementation
Probiotics are essential for recovery, but you cannot just buy any random bottle off the shelf. You need specific, clinically backed strains with proven results. Most cheap probiotics are destroyed by stomach acid before they ever reach your colon.
The two strains I recommend most are Saccharomyces boulardii and Lactobacillus rhamnosus GG. Both have decades of clinical research supporting their use for antibiotic-associated diarrhea.
Why Saccharomyces boulardii Works So Well
Saccharomyces boulardii is unique because it is not a bacterium at all. It is a beneficial, non-pathogenic yeast. This distinction matters enormously when you are actively taking antibacterial medication.
Because it is a yeast, antibiotics cannot kill it. You can take S. boulardii at the same time as your medication without the drug destroying the supplement. Clinical studies show it actively secretes enzymes that break down C. diff toxins, acting like a sponge for the harmful chemicals damaging your colon.
Lactobacillus rhamnosus GG Protocol
Lactobacillus rhamnosus GG is a powerful bacterial strain that adheres to the intestinal wall and physically blocks harmful pathogens from taking hold. It acts as a temporary mucosal barrier while your natural flora recovers.
Because it is a bacterium, you must space it correctly. Take it at least two hours after your antibiotic dose so the medication does not immediately destroy the good bacteria you just swallowed. Using this strain alongside S. boulardii provides comprehensive coverage, addressing both toxin neutralization and physical barrier protection.
The Danger of Anti-Motility Medications
When people want to know how to stop diarrhea from antibiotics fast, their first instinct is often to reach for Imodium (Loperamide). Be extremely careful with this approach.
Imodium works by paralyzing the muscles in your intestines, stopping stool from moving forward. For mild AAD, this might be fine for a day or two. But if you have an undiagnosed C. diff infection, taking Imodium is incredibly dangerous.
By stopping your bowel movements, you trap toxic, multiplying bacteria inside your colon. The toxins build up rapidly, drastically increasing your risk of pseudomembranous colitis or toxic megacolon. Always consult a doctor before using anti-diarrheal pills during an active antibiotic course.
What to Eat During Antibiotic-Associated Diarrhea
What you eat plays a huge role in recovery speed. You need foods that bulk up your stool without irritating your inflamed colon. The wrong foods act like sandpaper on a compromised digestive tract.
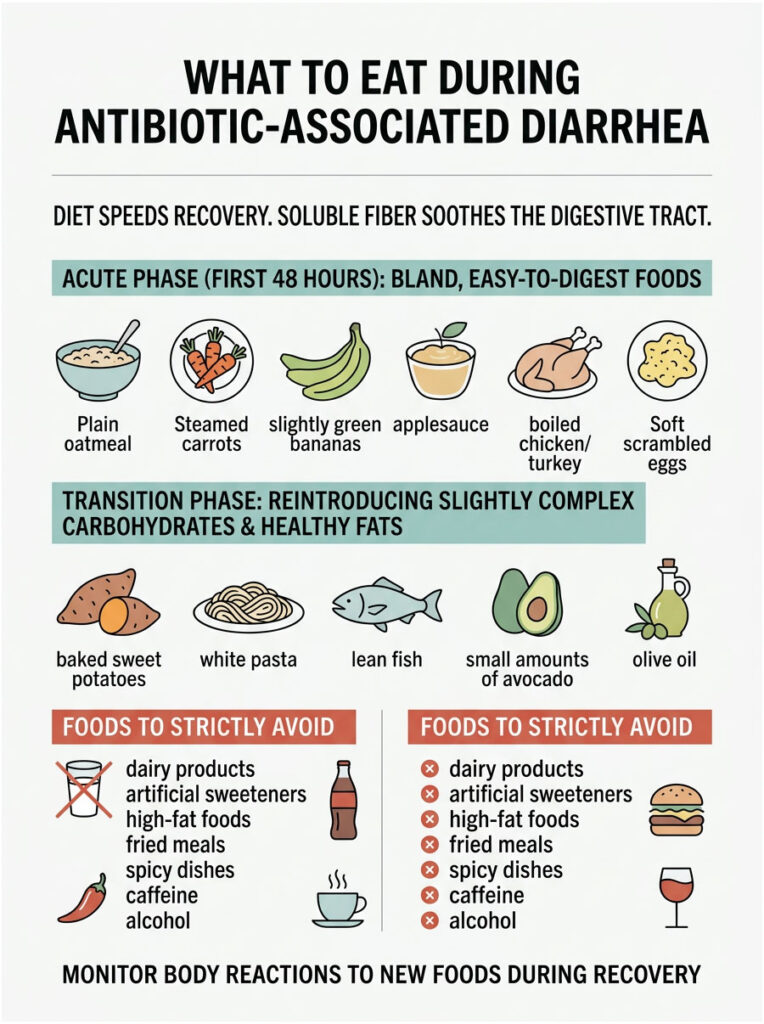
The focus should always be on soluble fiber rather than insoluble fiber. Soluble fiber absorbs excess water in the intestines, forming a soothing, gel-like substance that slows digestion and firms up loose stools.
The First 48 Hours: Acute Phase
During the first two days of severe symptoms, keep your diet incredibly bland and easy to digest. Your colon is highly inflamed and cannot process complex meals. Eat small, frequent meals every three hours instead of three large ones.
Good sources of soluble fiber for this phase include plain oatmeal, steamed carrots, and slightly green bananas. Applesauce is also excellent for binding loose stools. For protein, stick with boiled chicken breast, plain turkey, or soft scrambled eggs. Avoid oils, butter, and heavy seasonings.
The Transition Phase
Once your stool frequency drops to fewer than three times a day, you can enter the transition phase. This usually happens a few days after finishing your medication. Your colon is beginning to heal but remains sensitive.
Start reintroducing slightly more complex carbohydrates: baked sweet potatoes without the skin, white pasta, and lean fish. You can slowly add small amounts of healthy fats like avocado or a teaspoon of olive oil. Pay close attention to how your body reacts to each new food.
Foods to Strictly Avoid
Dairy products top the list of foods to avoid. Gut dysbiosis temporarily stops your body from producing lactase, the enzyme needed to digest milk. Consuming dairy during recovery will cause bloating, painful gas, and explosive stools.
Also avoid artificial sweeteners like sorbitol and sucralose, which pull massive amounts of water into the colon. High-fat foods, fried meals, spicy dishes, caffeine, and alcohol are all severe gut irritants that delay healing.
Long-Term Recovery: Restoring Your Microbiome After Antibiotics
Surviving the acute phase of loose stools is only the first step. Once you finish your prescription, your gut is essentially a barren landscape. You need to actively rebuild your microbiota diversity, or you risk developing long-term digestive problems.
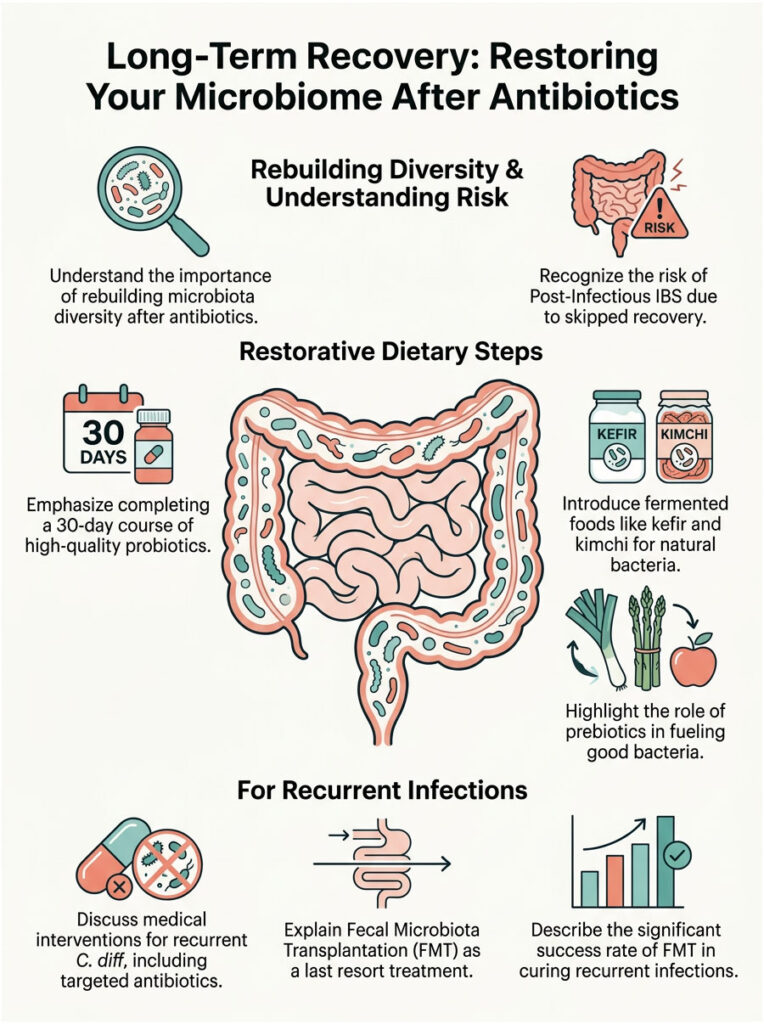
Preventing Post-Infectious IBS
Many patients who skip proper recovery develop Post-Infectious IBS, a form of Irritable Bowel Syndrome triggered by a major intestinal infection or prolonged gut dysbiosis. Even after bacteria normalize, the nerves in your gut remain hypersensitive. You might experience alternating bouts of constipation and diarrhea for months.
Completing a full 30-day course of high-quality probiotics is critical. You must keep the intestinal lining coated with beneficial bacteria while the mucosal barrier heals. Rushing back to a diet of processed foods is a reliable way to trigger chronic IBS.
Prebiotics and Fermented Foods
Once the acute diarrhea stops, you need to re-seed your gut with natural bacteria. Probiotic supplements are helpful, but real food is better for long-term diversity. Slowly introduce fermented foods into your daily diet.
Plain kefir, unpasteurized sauerkraut, authentic kimchi, and natural Greek yogurt are packed with diverse, living bacterial strains. Start with just a tablespoon a day to avoid overwhelming your system, then gradually increase.
Equally important are prebiotics, specific types of dietary fiber that feed your good bacteria. Foods high in inulin, such as asparagus, garlic, onions, and underripe bananas, provide the exact fuel your new bacteria need to thrive.
Medical Interventions for Recurrent C. diff
Sometimes, despite best efforts, C. diff keeps coming back. The bacteria form hard, microscopic spores that hide deep in the colon lining and wait for a chance to reactivate.
We treat recurrent cases with highly targeted antibiotics like oral Vancomycin or the newer drug Fidaxomicin. These kill C. diff without harming the rest of the microbiome. They are often prescribed using a slow taper method over several weeks, allowing normal flora to grow back while keeping spores suppressed.
Fecal Microbiota Transplantation (FMT)
If a patient fails multiple rounds of advanced medications, we turn to our most powerful tool: Fecal Microbiota Transplantation. The procedure involves taking healthy, rigorously processed stool from a screened donor and placing it directly into the patient’s colon during a colonoscopy.
FMT instantly delivers trillions of beneficial bacteria to exactly where they are needed. It restores microbiota diversity in a matter of hours and cures recurrent C. diff infections in over 90% of cases. For patients who have been suffering for months, it is genuinely life-changing.
Clinical Case Studies: Real Patients, Real Recovery
Textbook definitions are helpful, but human bodies are unpredictable. Here are a few anonymized case studies based on common presentations in clinical practice.
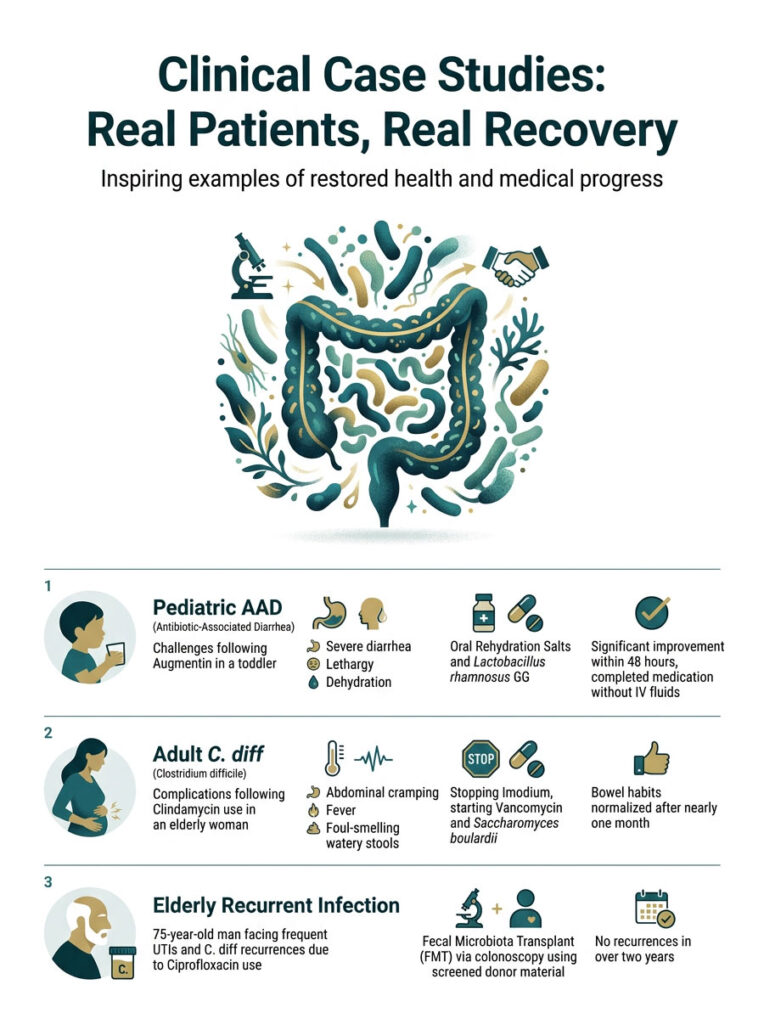
Pediatric AAD: The Augmentin Challenge
A three-year-old toddler was prescribed a ten-day course of Augmentin for a double ear infection. By day four, his parents reported severe, explosive diarrhea. The child was lethargic, slightly dehydrated, and refusing to eat.
We started pediatric Oral Rehydration Salts immediately and introduced Lactobacillus rhamnosus GG twice daily, spaced two hours from his medication. He stayed on a bland diet of mashed bananas and plain oatmeal for three days. Within 48 hours, the watery stools slowed significantly. He finished his prescription without needing IV fluids.
Adult C. diff: The Clindamycin Crisis
A 62-year-old woman was given Clindamycin for an infected tooth abscess. Ten days after finishing the course, she arrived at our clinic with severe cramping, a 101 F fever, and up to twelve foul-smelling watery stools a day. A rapid stool toxin test came back positive for C. diff.
We immediately stopped the over-the-counter Imodium she had been using, which was trapping bacterial toxins inside her body. She was started on a 14-day course of oral Vancomycin and Saccharomyces boulardii. It took nearly a month for her bowel habits to normalize. She eventually made a full recovery through strict dietary management.
Elderly Recurrent Infection: FMT Success
A 75-year-old man in an assisted care facility was frequently prescribed Ciprofloxacin for recurrent urinary tract infections. Over six months, he developed C. diff three separate times. Each time, oral Vancomycin cleared it temporarily, but the infection returned within weeks.
His microbiome was so decimated by constant fluoroquinolone use that it could not recover naturally. We performed a Fecal Microbiota Transplant via colonoscopy using screened donor material. Within 24 hours, his severe diarrhea stopped completely. He has not had a single recurrence in over two years.
The Psychological Impact of Chronic Digestive Issues
We rarely discuss the mental toll that severe GI distress takes on patients. Unpredictable, urgent bowel movements are incredibly anxiety-inducing. Patients often become afraid to leave home or eat normal meals.
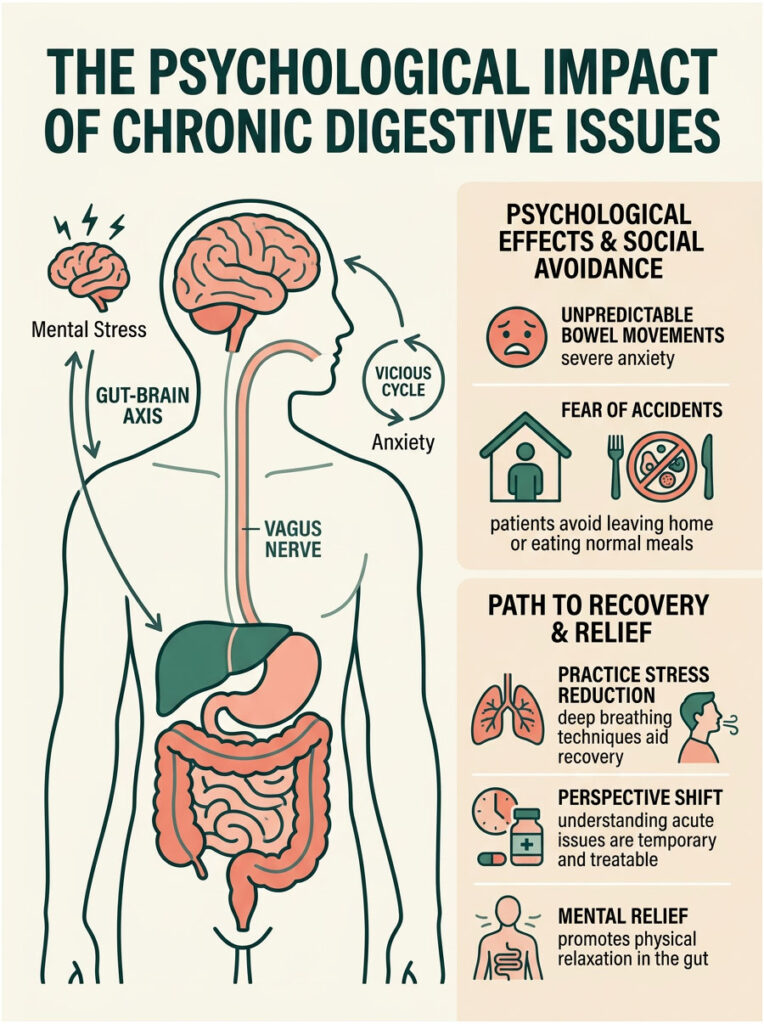
This anxiety creates a vicious cycle through the gut-brain axis. Your brain and digestive tract are connected by the vagus nerve. When you stress about having an accident, your brain sends panic signals directly to your gut, causing your intestines to spasm and contract even faster. Your anxiety about diarrhea can literally cause more diarrhea.
Practicing deep breathing and stress reduction techniques during recovery genuinely helps. Knowing that AAD is temporary and highly treatable often provides the mental relief needed to let the gut relax.
Summary and Key Takeaways
Can antibiotics cause diarrhea? Absolutely. It is one of the most common and predictable side effects in modern medicine. While these drugs are essential for clearing dangerous infections, protecting your gut health during and after treatment is equally critical.
- The primary trigger is severe gut dysbiosis. The loss of healthy bacteria prevents absorption of short-chain fatty acids and causes bile acid malabsorption.
- Know the red flags. Mild, soft stools are a normal side effect. Severe watery stools, high fever, and intense abdominal pain may indicate a C. diff infection requiring emergency care.
- Prioritize hydration. Use clinical Oral Rehydration Salts over plain water or sugary sports drinks. Replace lost electrolytes rapidly.
- Use the right probiotics. Saccharomyces boulardii and Lactobacillus rhamnosus GG offer maximum mucosal protection during antibiotic treatment.
- Avoid anti-motility drugs without medical guidance. Imodium can trap dangerous bacterial toxins inside your colon.
- Rebuild your gut long-term. Consume prebiotics and fermented foods to restore microbiota diversity and prevent chronic Post-Infectious IBS.
Frequently Asked Questions
Why do antibiotics cause diarrhea and stomach upset?
As a gastroenterologist, I explain this through the biological mechanism of gut dysbiosis. Antibiotics are broad-spectrum eradicators that cannot distinguish between harmful pathogens and beneficial gut flora. When these healthy bacteria are destroyed, the colon loses its protective mucosal barrier and its ability to process short-chain fatty acids (SCFAs) like butyrate. This disruption leads to osmotic diarrhea, where the colon fails to absorb water correctly, resulting in loose, watery stools.
How long does antibiotic-associated diarrhea (AAD) typically last?
In most clinical cases, AAD symptoms begin between the second and eighth day of antibiotic therapy. For mild cases, the diarrhea usually resolves naturally within one to seven days after you finish the medication as your microbiota diversity begins to recover. However, if the diarrhea persists or worsens after you stop the medication, it may indicate a more serious underlying infection like C. diff.
What are the red flag symptoms of a Clostridioides difficile (C. diff) infection?
A C. diff infection is a medical emergency that presents much more severely than standard AAD. Key warning signs include experiencing more than 10 watery stools per day, a high fever exceeding 102°F, intense abdominal pain or tenderness, and a distinctively foul stool odor. If left untreated, this can progress to pseudomembranous colitis, a life-threatening inflammation of the colon.
Which antibiotics carry the highest risk for causing digestive issues?
Clindamycin is historically the most significant offender for triggering C. diff infections because it profoundly suppresses anaerobic gut flora. Fluoroquinolones (like Cipro) and broad-spectrum cephalosporins are also high-risk. Additionally, Augmentin frequently causes rapid bowel movements because the clavulanate component acts as a direct chemical stimulant to gut motility.
What is the best probiotic for Augmentin-induced diarrhea?
Clinical evidence strongly supports a combination of Saccharomyces boulardii and Lactobacillus rhamnosus GG. S. boulardii is particularly effective because it is a beneficial yeast, meaning it cannot be killed by the antibiotics you are taking. It works to neutralize bacterial toxins, while L. rhamnosus GG helps restore the physical mucosal barrier of the intestines.
How can I stop diarrhea from antibiotics fast and safely?
To manage symptoms quickly, focus on immediate hydration using clinical-grade oral rehydration salts (ORS) rather than sugary sports drinks, which can worsen osmotic diarrhea. Simultaneously, implement a targeted probiotic protocol using S. boulardii and adopt a bland diet rich in soluble fiber, such as oatmeal and steamed carrots, to help bind and firm the stool.
Is it safe to take Imodium (Loperamide) for antibiotic-related diarrhea?
I generally advise against using anti-motility agents like Imodium without a doctor’s supervision. If your diarrhea is caused by a C. diff infection, Imodium can be dangerous because it paralyzes the gut and traps harmful bacterial toxins inside your colon. This significantly increases the risk of severe complications like toxic megacolon.
Why is my diarrhea bright yellow after taking antibiotics?
Bright yellow diarrhea is a classic sign of bile acid malabsorption. Healthy gut bacteria normally break down bile acids so they can be recycled by the body. When antibiotics wipe out these bacteria, raw bile acids dump into the colon, where they irritate the intestinal lining and stimulate the secretion of excess water and mucus.
What foods should I strictly avoid while recovering from gut dysbiosis?
You must strictly avoid dairy products, as gut dysbiosis often causes temporary lactose intolerance. Additionally, stay away from artificial sweeteners like sorbitol, which pull water into the colon, as well as high-fat fried foods, spicy seasonings, caffeine, and alcohol, all of which act as potent gastrointestinal irritants.
How do I restore my gut flora and microbiota diversity after antibiotics?
Long-term recovery requires a dedicated 30-day gut rehabilitation protocol. Start by slowly reintroducing fermented foods like kefir, sauerkraut, and kimchi to ‘re-seed’ your gut with living bacteria. You must also consume prebiotics—found in garlic, onions, and asparagus—which provide the specific fiber needed to fuel the growth of your beneficial microbes.
Can antibiotics cause long-term Irritable Bowel Syndrome (IBS)?
Yes, some patients develop Post-infectious IBS following a severe bout of antibiotic-associated dysbiosis. This happens when the nerves in the gut remain hypersensitive even after the infection is cleared. Preventing this requires proactive management of visceral inflammation through consistent probiotic use and a slow, careful transition back to a normal diet.
What is a Fecal Microbiota Transplant (FMT) and when is it used?
Fecal Microbiota Transplantation is a highly effective procedure used for recurrent C. diff infections that don’t respond to standard antibiotics. We transplant processed, healthy donor stool into the patient’s colon to instantly restore a diverse microbial ecosystem. This procedure has a success rate of over 90% in curing stubborn, chronic dysbiosis.
Disclaimer
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The content is written by a medical professional but does not replace a one-on-one consultation with your healthcare provider. Always seek the advice of your physician before starting new supplements like probiotics or changing your medication regimen.
References
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/cdiff/index.html – Statistical data on Clostridioides difficile infections and antibiotic safety.
- National Institutes of Health (NIH) – PubMed Central – Clinical studies on the efficacy of Saccharomyces boulardii in preventing Antibiotic-Associated Diarrhea.
- World Health Organization (WHO) – Official Guidelines – Standards for Oral Rehydration Salts (ORS) and management of acute diarrheal diseases.
- American College of Gastroenterology (ACG) – Clinical Guidelines – Professional protocols for the diagnosis and management of C. diff and gut dysbiosis.
- U.S. Food and Drug Administration (FDA) – Drug Safety Communications – Information regarding Black Box warnings for Fluoroquinolone antibiotics.
- Journal of Clinical Gastroenterology – Research Paper – Findings on the success rates of Fecal Microbiota Transplantation (FMT) for recurrent infections.