
If you are dealing with a burning stomach and frequent trips to the bathroom, you are probably wondering whether the two are connected. Can gastric ulcers cause diarrhea? It is one of the most common questions I hear in my gastroenterology practice, and the answer is more layered than a simple yes or no.
Table of Contents
As a board-certified gastroenterologist with over 15 years of clinical experience, I can tell you this: a localized sore in your stomach lining does not directly force your colon to empty. But the underlying triggers that created the ulcer, and the medications used to treat it, frequently cause lower intestinal distress and loose stools.
Your digestive tract is one continuous, deeply connected ecosystem. What happens at the top inevitably impacts the bottom. In this guide, we will explore the exact mechanisms linking upper abdominal pain to changes in bowel habits, walk through diagnostic pathways, cover dietary management, and flag the emergency warning signs you should never ignore.
Quick Answer
Can gastric ulcers cause diarrhea? A stomach ulcer itself does not directly cause diarrhea. However, the same factors that created the ulcer, including H. pylori infection, chronic NSAID use, and gastrointestinal bleeding, frequently trigger loose stools and lower bowel distress. The medications prescribed to heal ulcers also commonly disrupt gut flora, leading to secondary bowel problems.
Key Statistics on Peptic Ulcer Disease and GI Symptoms
- About 10% of Americans will develop a stomach ulcer at some point, requiring medical intervention (American College of Gastroenterology, 2023).
- Up to 30% of patients undergoing standard antibiotic treatment for H. pylori experience antibiotic-associated diarrhea.
- Chronic NSAID users face a 65% to 70% chance of developing intestinal inflammation known as NSAID enteropathy.
- Upper gastrointestinal bleeding accounts for over 300,000 hospital admissions annually in the United States.
- Roughly 50% of the global population carries Helicobacter pylori, the bacterium responsible for most gastric ulcers.
- Small Intestinal Bacterial Overgrowth (SIBO) develops in nearly 25% of patients using proton pump inhibitors for more than six consecutive months.
Understanding the Link Between Gastric Ulcers and Diarrhea
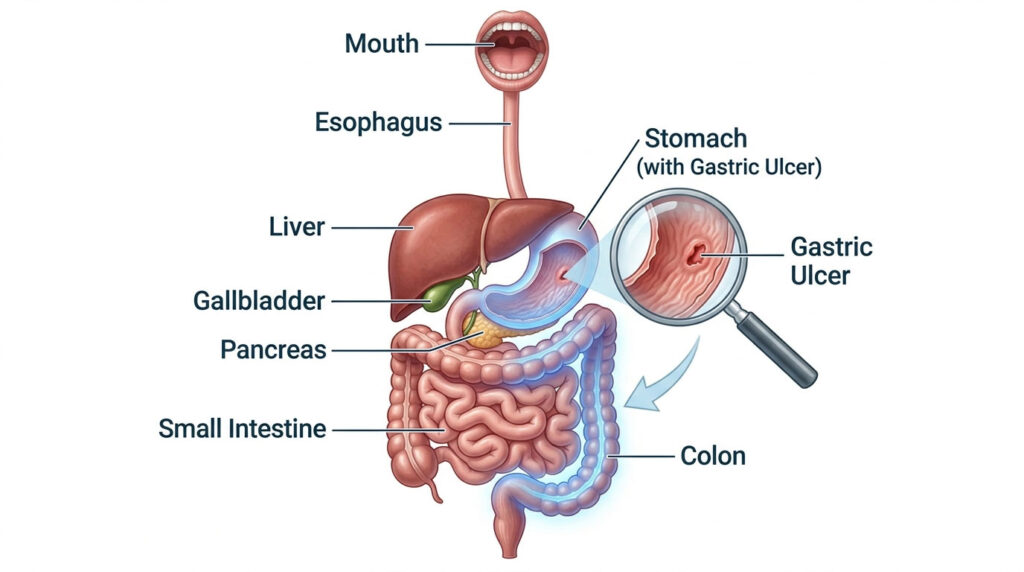
Peptic Ulcer Disease occurs when painful sores develop on the inner lining of your stomach or the upper part of your small intestine. When these sores form in the stomach, they are called gastric ulcers. If they develop just past the stomach in the duodenum, they are duodenal ulcers. Both fall under the broader category of Peptic Ulcer Disease.
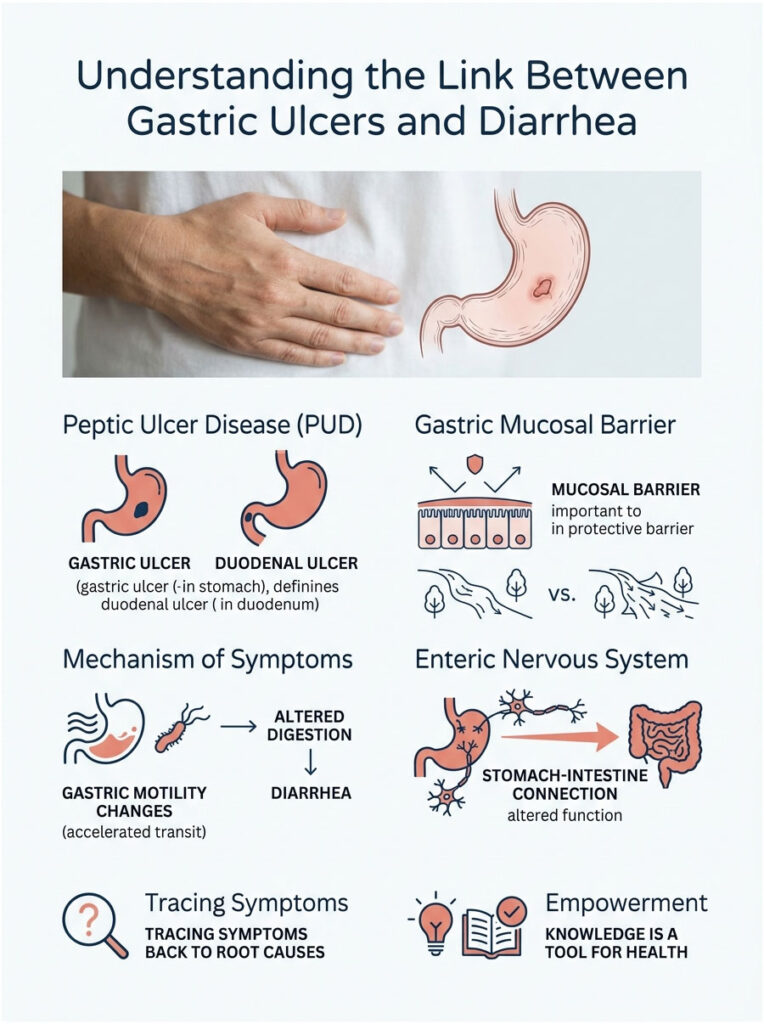
Your stomach has a built-in defense called the gastric mucosal barrier, a thick, specialized layer of mucus that protects delicate tissue from the corrosive digestive acids needed to break down food. When this barrier is compromised, acid burns into the unprotected tissue, creating the classic gnawing, burning sensation that often wakes patients at night.
Why Symptoms Spread from the Stomach to the Bowel
Many patients assume their upper and lower digestive tracts work independently. In practice, they are deeply connected through a complex network of nerves, hormones, and bacteria called the enteric nervous system, sometimes referred to as the body’s second brain.
When you have a stomach ulcer, normal gastric motility changes. Your stomach may empty too quickly or slow to a crawl. This altered digestion dumps poorly processed, highly acidic food into the small intestine before it is ready. Your lower intestines then work overtime to compensate, and that sudden shift in workload easily irritates the bowel lining.
Think of it like a river ecosystem. If a factory dumps pollutants upstream, the fish downstream eventually suffer. Your digestive tract operates on the same principle. The question of can gastric ulcers cause diarrhea is often best answered by tracing this domino effect back to its root cause.
What Actually Causes Diarrhea in Peptic Ulcer Disease
If the ulcer itself is a symptom of a larger problem, what is the real culprit? There are three primary triggers that connect upper stomach pain to lower bowel urgency.
H. pylori Infection and Gut Dysbiosis
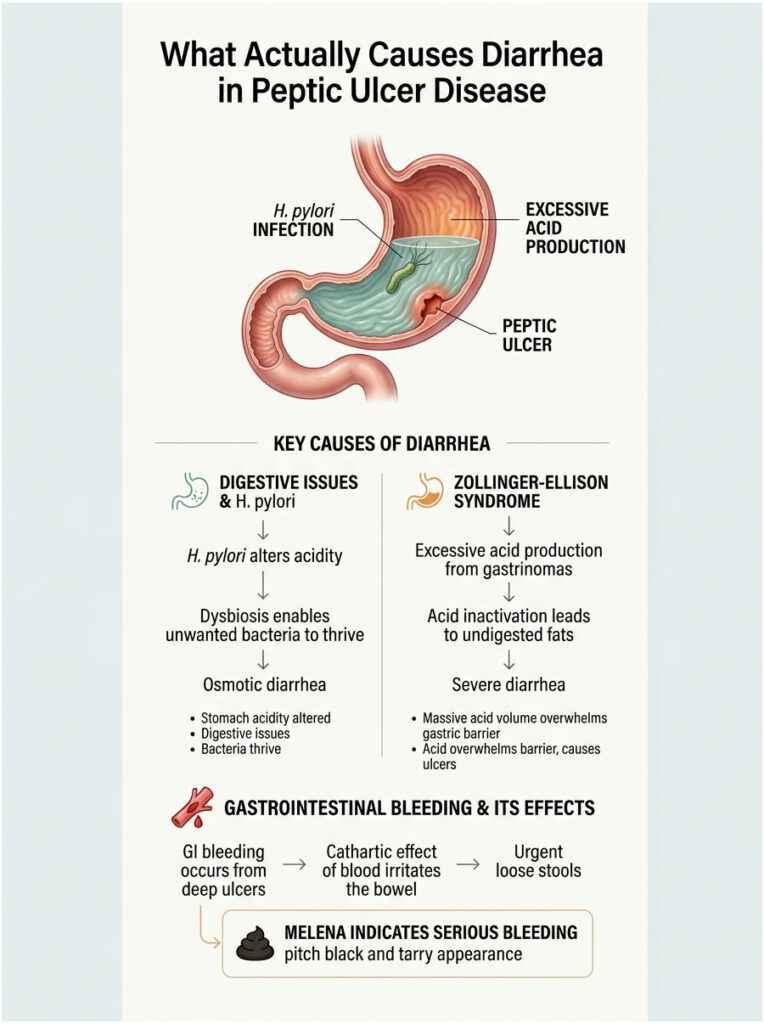
The majority of gastric ulcers are caused by Helicobacter pylori, a spiral-shaped bacterium uniquely adapted to survive in the acidic stomach environment. It secretes an enzyme called urease that neutralizes the acid immediately surrounding it, then burrows into the stomach lining and destroys the gastric mucosal barrier.
H. pylori does not just stay in the stomach. It fundamentally alters your overall stomach acidity and digestive function. This pH shift allows other unwanted bacteria to survive the stomach and travel further down the tract. Because the stomach is not breaking down food properly, unabsorbed nutrients pull excess water into the colon. This osmotic imbalance results in mild to moderate, persistent diarrhea.
Zollinger-Ellison Syndrome and Acid Hypersecretion
While rare, Zollinger-Ellison Syndrome deserves consideration when a patient has both severe, treatment-resistant stomach pain and chronic loose stools. This condition involves gastrin-producing tumors (gastrinomas), usually in the pancreas or duodenum, that force the stomach to produce extreme levels of digestive acid.
The massive acid volume overwhelms the gastric mucosal barrier, causing multiple stubborn ulcers. It also spills into the small intestine, inactivating the pancreatic enzymes needed to digest dietary fats. The undigested fat rushes through the bowel, causing severe, watery, foul-smelling diarrhea. In these cases, the answer to can gastric ulcers cause diarrhea is a clear yes, driven entirely by acid volume.
Gastrointestinal Bleeding and the Cathartic Effect of Blood
The most alarming connection between an ulcer and diarrhea involves active internal bleeding. If an ulcer erodes deeply enough to strike a blood vessel, blood pours into the digestive tract. The human bowel is highly sensitive to free blood, a reaction known as the cathartic effect of blood.
Blood acts as a powerful natural laxative. As it breaks down in the intestines, the proteins and iron irritate the bowel lining and dramatically increase intestinal motility. Patients experience sudden, urgent, uncontrollable loose movements. These stools are typically pitch black and tarry, a dangerous condition called melena.
How Painkillers Cause Both Ulcers and Diarrhea
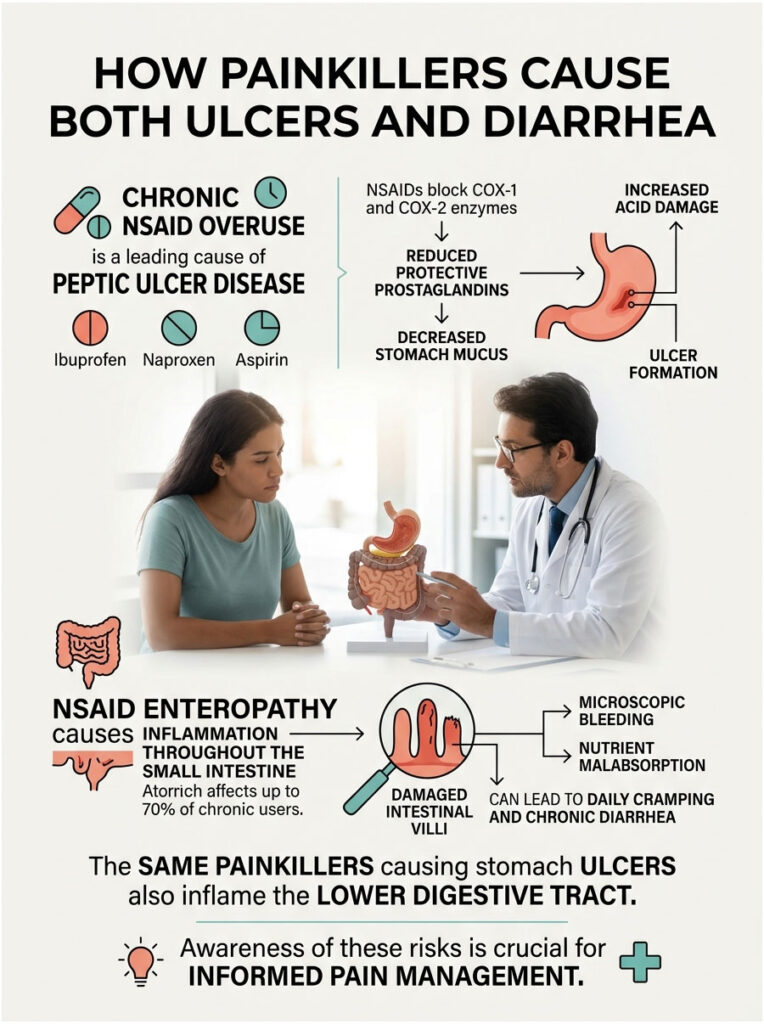
Beyond bacterial infections, the most common cause of Peptic Ulcer Disease is chronic overuse of over-the-counter painkillers like Ibuprofen, Naproxen, and Aspirin. Millions of people take them daily without a second thought. But the damage they cause is far more extensive than most patients realize.
Prostaglandin Disruption
NSAIDs relieve pain by blocking cyclooxygenase enzymes (COX-1 and COX-2). Unfortunately, these same enzymes produce prostaglandins, the lipid compounds that signal your body to produce protective stomach mucus and bicarbonate. When NSAID use causes prostaglandin levels to drop, the stomach stops producing enough protective mucus, and acid eats into the unprotected tissue.
NSAID Enteropathy: Damage Beyond the Stomach
Here is the detail most people miss: NSAIDs do not just damage the stomach. They cause widespread inflammation throughout the entire small intestine, a condition called NSAID enteropathy. Clinical data shows that up to 70% of chronic NSAID users develop some degree of small bowel damage.
The intestinal villi become blunted and inflamed, causing microscopic bleeding, protein loss, and severe irritation. This directly results in daily cramping, nutrient malabsorption, and chronic diarrhea. The exact same pills causing the stomach ulcer are simultaneously inflaming the lower tract. It is a dual attack on the digestive system.
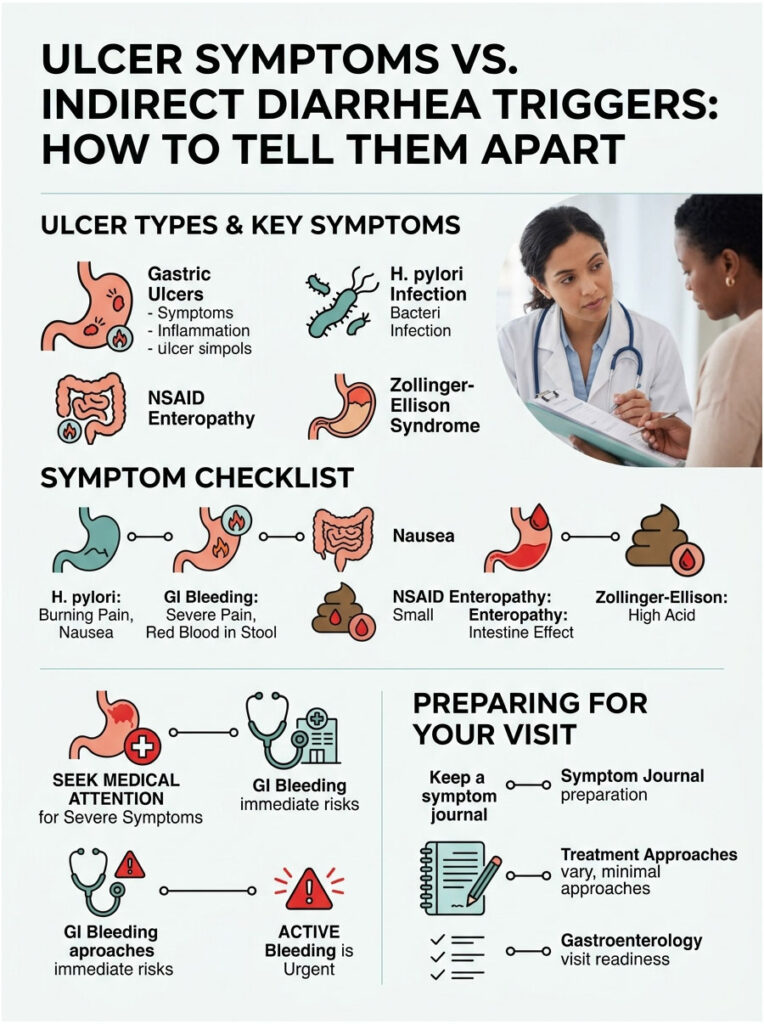
Ulcer Symptoms vs. Indirect Diarrhea Triggers: How to Tell Them Apart
| Symptom Origin | How It Presents | Underlying Mechanism | Treatment Approach |
| Gastric Ulcer | Epigastric burning, pain after eating, early satiety | Acid erosion of the gastric mucosal barrier | Proton pump inhibitors, dietary changes |
| H. pylori Infection | Chronic dyspepsia, nausea, mild diarrhea, bad breath | Bacterial overgrowth altering gastric pH and flora | Triple Therapy (antibiotics plus acid suppressors) |
| NSAID Enteropathy | Lower cramping, chronic diarrhea, unexplained anemia | Prostaglandin inhibition causing intestinal inflammation | Stop all NSAIDs, switch to safer alternatives |
| Zollinger-Ellison | Severe heartburn, persistent watery diarrhea, weight loss | Gastrinomas causing massive acid hypersecretion | High-dose acid suppressors, surgical removal |
| Active GI Bleeding | Black tarry stools (melena), dizziness, sudden loose stools | Cathartic effect of blood as a natural laxative | Emergency endoscopic intervention |
If you identify with the bottom two rows, seek immediate medical attention. Active bleeding and rapid weight loss are absolute red flags. For the top three rows, schedule an outpatient visit with a gastroenterologist. Keeping a detailed symptom journal that tracks when pain occurs relative to meals and bathroom habits will help your doctor pinpoint the cause.
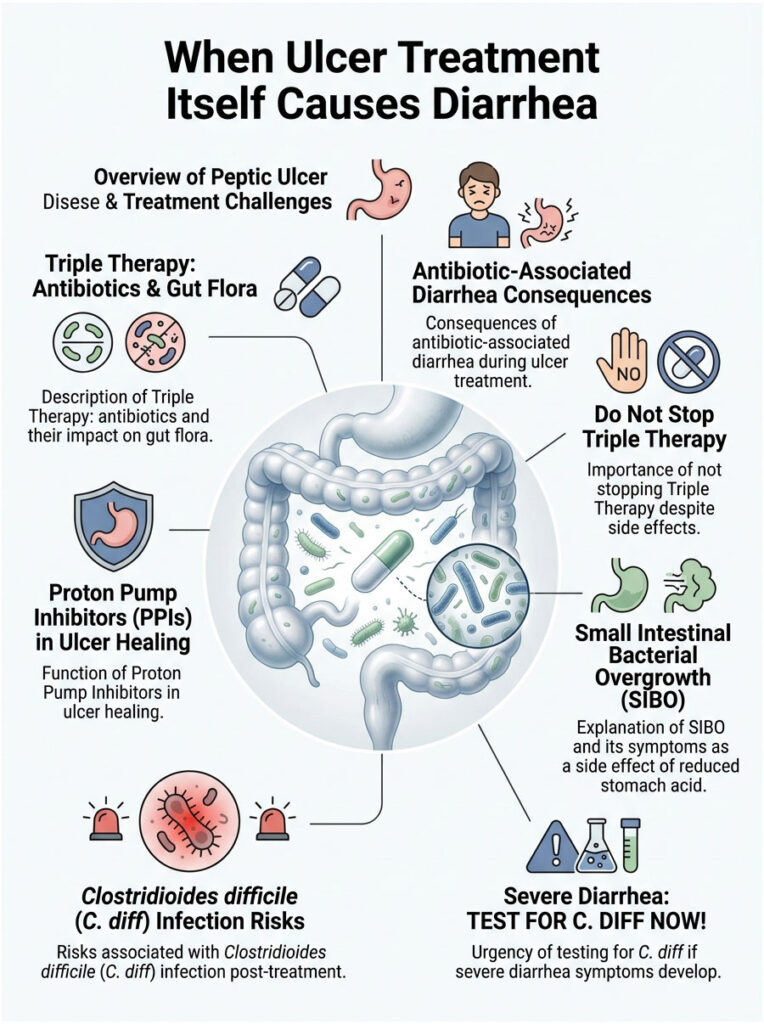
When Ulcer Treatment Itself Causes Diarrhea
Sometimes the medications required to heal Peptic Ulcer Disease have their own disruptive effects on the bowel. This is one of the most frustrating parts of the healing process.
Triple Therapy and Antibiotic-Associated Diarrhea
If your doctor confirms H. pylori, they will prescribe Triple Therapy: two heavy-duty antibiotics (typically Amoxicillin, Clarithromycin, or Metronidazole) alongside a strong acid reducer. These antibiotics are effective at killing the stubborn bacteria, but they are entirely indiscriminate. They travel to your colon and decimate your healthy gut flora.
Without good bacteria to properly digest food and absorb water, the colon struggles to form solid waste. The result is severe, daily antibiotic-associated diarrhea. For many patients, this side effect is actually more disruptive than the original ulcer pain.
Important: Do not stop Triple Therapy just because you develop loose stools. Stopping antibiotics early allows H. pylori to mutate and become antibiotic-resistant. Always contact your prescribing physician for guidance on managing side effects while completing the full course.
Proton Pump Inhibitors and SIBO
To heal an ulcer, we need to turn off the acid tap. Proton Pump Inhibitors like Omeprazole, Pantoprazole, and Esomeprazole are the gold standard for this. They work remarkably well, giving the gastric mucosal barrier time to regenerate.
But stomach acid serves an evolutionary purpose: it acts as a chemical firewall, killing swallowed bacteria before they reach the lower intestines. When you drastically lower stomach acid for prolonged periods, bacteria from the mouth and colon migrate into the small intestine. This unnatural colonization is called Small Intestinal Bacterial Overgrowth, or SIBO.
SIBO causes severe bloating, excessive gas, and chronic loose stools. When patients come back weeks after starting medication asking can gastric ulcers cause diarrhea, SIBO is my immediate suspicion. The treatment essentially created a new problem.
The Risk of C. diff Infection
By wiping out healthy gut flora and lowering stomach acid, you create a vulnerable environment where harmful pathogens thrive. The most dangerous of these is Clostridioides difficile (C. diff), an opportunistic bacterium that releases potent toxins and severely inflames the colon lining.
C. diff causes aggressive, watery diarrhea up to 15 times daily, severe abdominal cramping, and high fever. It requires immediate specialized treatment. If you develop these symptoms after treating a stomach ulcer, get tested for C. diff right away.
Diagnostic Tests: How Doctors Find the Root Cause
Because Peptic Ulcer Disease symptoms overlap with many other conditions, precise diagnostic tools are essential. Here is how gastroenterologists investigate when a patient presents with both upper pain and lower bowel changes.

Upper Endoscopy (EGD)
The gold standard for diagnosing a stomach ulcer is an Upper Gastrointestinal Endoscopy. You receive mild IV sedation and will not feel or remember the procedure. A thin, flexible tube with a high-definition camera is guided into the stomach for direct visualization of the lining. If an active ulcer or erosive gastritis is found, tiny instruments take a painless biopsy to test for H. pylori or precancerous cells.
Non-Invasive Tests
Not every patient needs an immediate endoscopy. The Urea Breath Test detects active H. pylori by having you drink a liquid containing a specific carbon isotope. If the bacteria are present, their urease enzymes break down the liquid and release measurable carbon dioxide in your breath. It is fast, painless, and highly accurate.
Stool Antigen tests analyze a fecal sample for proteins shed by H. pylori bacteria. This is an excellent, non-invasive way to confirm whether an infection has been successfully eradicated after antibiotic treatment.
Fecal Occult Blood and Gastrin Testing
When patients ask can gastric ulcers cause diarrhea, my immediate concern is microscopic bleeding. A Fecal Occult Blood Test detects hidden traces of blood in stool that are invisible to the naked eye. A positive result strongly suggests the ulcer is weeping into the digestive tract and the cathartic effect of blood is triggering the diarrhea.
If you also have massive watery diarrhea and severe heartburn, a fasting serum gastrin test measures hormone levels to rule out the rare Zollinger-Ellison Syndrome.
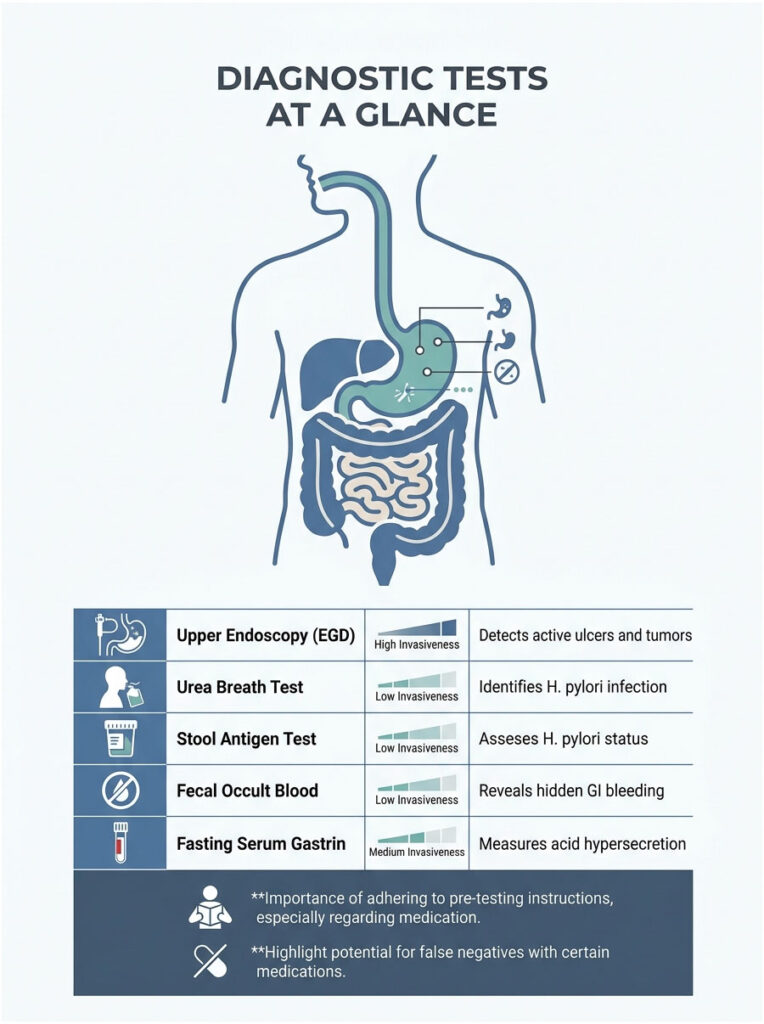
Diagnostic Tests at a Glance
| Test | Purpose | Invasiveness | What It Detects |
| Upper Endoscopy (EGD) | Direct visual inspection of stomach lining | High (IV sedation) | Active ulcers, bleeding, mucosal damage, tumors |
| Urea Breath Test | Detect active bacterial infection via exhaled gases | Low (non-invasive) | Active H. pylori in the stomach |
| Stool Antigen Test | Check for bacterial protein shedding in feces | Low (home sample) | H. pylori status and post-treatment eradication |
| Fecal Occult Blood | Identify hidden microscopic GI bleeding | Low (home sample) | Blood from ulcers or NSAID enteropathy |
| Fasting Serum Gastrin | Measure digestive hormone levels | Medium (blood draw) | Acid hypersecretion linked to Zollinger-Ellison |
Note: certain medications can cause false negatives. You must stop Proton Pump Inhibitors at least two weeks before a breath or stool test. Always follow your gastroenterologist’s pre-testing instructions carefully.
Emergency Red Flags: When to Go to the ER
Most Peptic Ulcer Disease is treatable in an outpatient setting. But specific warning signs elevate your situation from a painful inconvenience to a medical emergency. You cannot afford to ignore these.
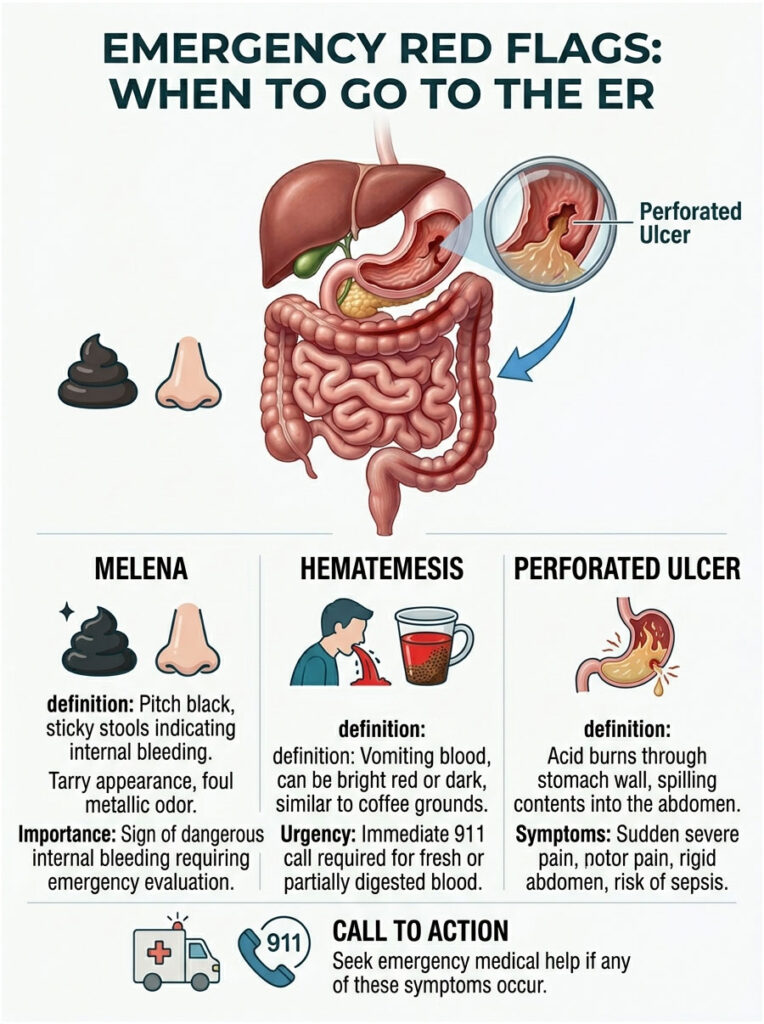
How to Identify Melena
Standard loose stools from medication or mild irritation are usually brown, yellow, or green. If your ulcer is bleeding heavily, the blood travels through your entire digestive tract. By the time it exits, iron in the blood has been oxidized by digestive enzymes, creating melena.
Melena is visually unmistakable: pitch black, incredibly sticky and tarry, resembling road asphalt, with a uniquely foul, metallic odor. If you see this in the toilet, the question of can gastric ulcers cause diarrhea is no longer academic. It is a signal of an active, dangerous internal bleed requiring immediate emergency evaluation.
Hematemesis and Perforation
Hematemesis, or vomiting blood, requires an immediate 911 call. The blood may be bright red (fresh arterial bleed) or look like dark, wet coffee grounds (partially digested blood). Both indicate a severe crisis.
The most dangerous complication is a perforated ulcer, where acid burns completely through the stomach wall, spilling contents into the sterile abdominal cavity. This causes sudden, excruciating pain, a rigid “board-like” abdomen, and rapidly leads to deadly sepsis without emergency surgery.
Practical Strategies for Healing
Managing Antibiotic Diarrhea with Probiotics
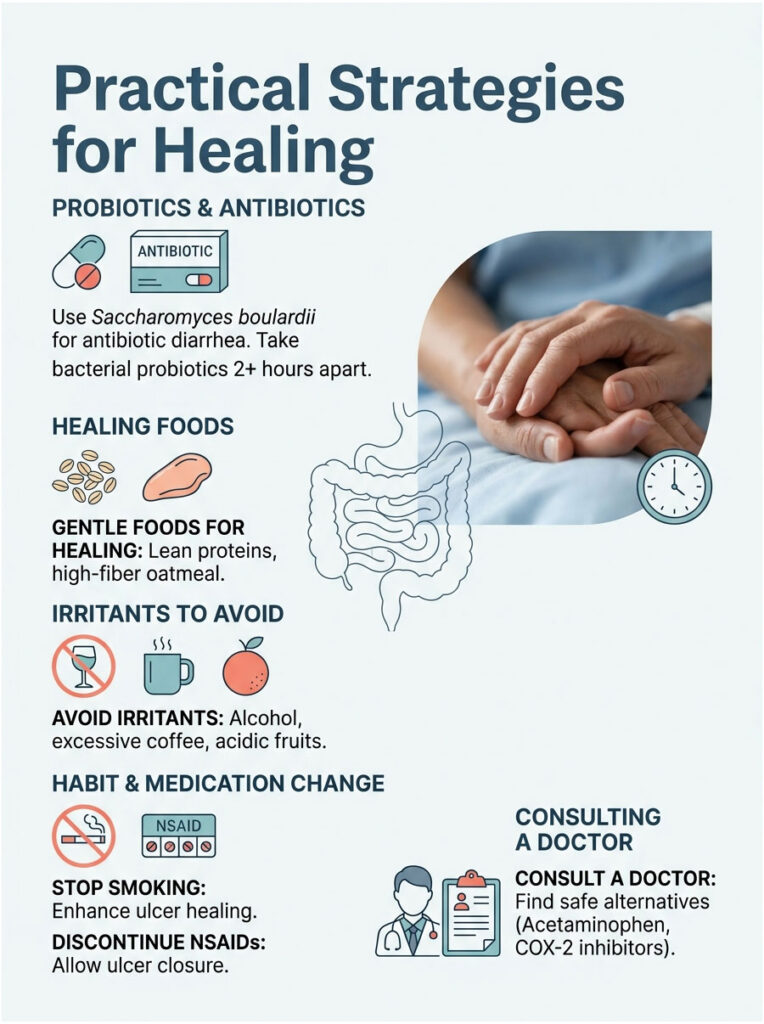
If you are on Triple Therapy, protect your gut microbiome with targeted probiotics. The yeast-based probiotic Saccharomyces boulardii is particularly effective because antibiotics cannot kill it. Clinical studies show it significantly reduces antibiotic-associated diarrhea and helps prevent C. diff colonization.
Lactobacillus rhamnosus GG is another excellent option. Take bacterial probiotics at least two hours apart from your antibiotic doses to ensure maximum survival.
Dietary Modifications for Healing
What you eat directly impacts healing time. Focus on gentle, easy-to-digest foods: lean proteins like baked chicken, steamed vegetables, and high-fiber foods like plain oatmeal. Fiber buffers harsh stomach acid and promotes healthy, formed bowel movements, naturally reducing diarrhea episodes.
Strictly avoid chemical irritants that further damage the gastric mucosal barrier: alcohol, excessive black coffee, and highly acidic citrus fruits. Stop smoking immediately, as nicotine restricts blood flow and slows ulcer healing.
Safe Alternatives to NSAIDs
If your ulcer was caused by painkillers, stop traditional NSAIDs immediately. Continuing Ibuprofen or Naproxen prevents the ulcer from closing. Acetaminophen is generally stomach-safe since it does not inhibit prostaglandin synthesis, though you must follow dosing instructions to protect your liver.
If you have a condition like rheumatoid arthritis that absolutely requires anti-inflammatory medication, consult your rheumatologist about selective COX-2 inhibitors like Celecoxib, or a daily PPI to shield the stomach while you take your joint medication.
Real-World Clinical Scenarios
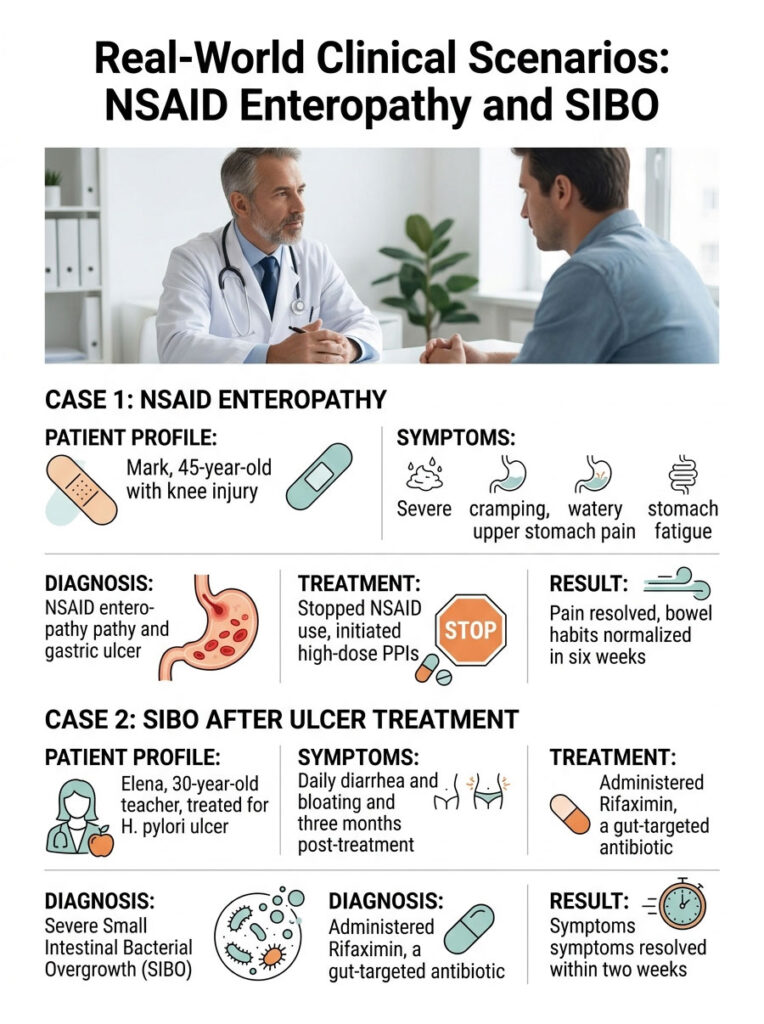
Case 1: NSAID Enteropathy Mistaken for IBS
Mark, a 45-year-old, presented with severe lower cramping and persistent watery stools. He was initially misdiagnosed with Irritable Bowel Syndrome. A month later, he developed gnawing upper stomach pain and profound fatigue. He came to my clinic asking, can gastric ulcers cause diarrhea?
A detailed history revealed he had been taking high doses of Ibuprofen daily for a knee injury. His Fecal Occult Blood Test came back positive, and hemoglobin had dropped significantly. Endoscopy revealed a 1-centimeter bleeding ulcer and widespread erosive gastritis. The diagnosis: NSAID enteropathy causing lower GI distress alongside a bleeding gastric ulcer.
We stopped all NSAID use and started high-dose PPIs. Within six weeks, his stomach pain vanished. Without the constant NSAID-induced inflammation, his bowel habits returned to normal.
Case 2: SIBO After Successful Ulcer Treatment
Elena, a 30-year-old teacher, was treated for an H. pylori ulcer with antibiotics and a long PPI course. Her stomach pain resolved, but three months later she developed severe daily diarrhea and bloating. She assumed her ulcer had returned.
Endoscopy showed a perfectly healed stomach lining. A specialized breath test revealed severe Small Intestinal Bacterial Overgrowth. Prolonged acid suppression had allowed colon bacteria to migrate into her small intestine. We treated the SIBO with Rifaximin, a gut-targeted antibiotic, and within two weeks her diarrhea and bloating were completely resolved.
Key Takeaways: Can Gastric Ulcers Cause Diarrhea?
The physical crater in your stomach lining does not directly force your colon to empty. But the underlying mechanisms that created the ulcer absolutely trigger lower bowel distress.
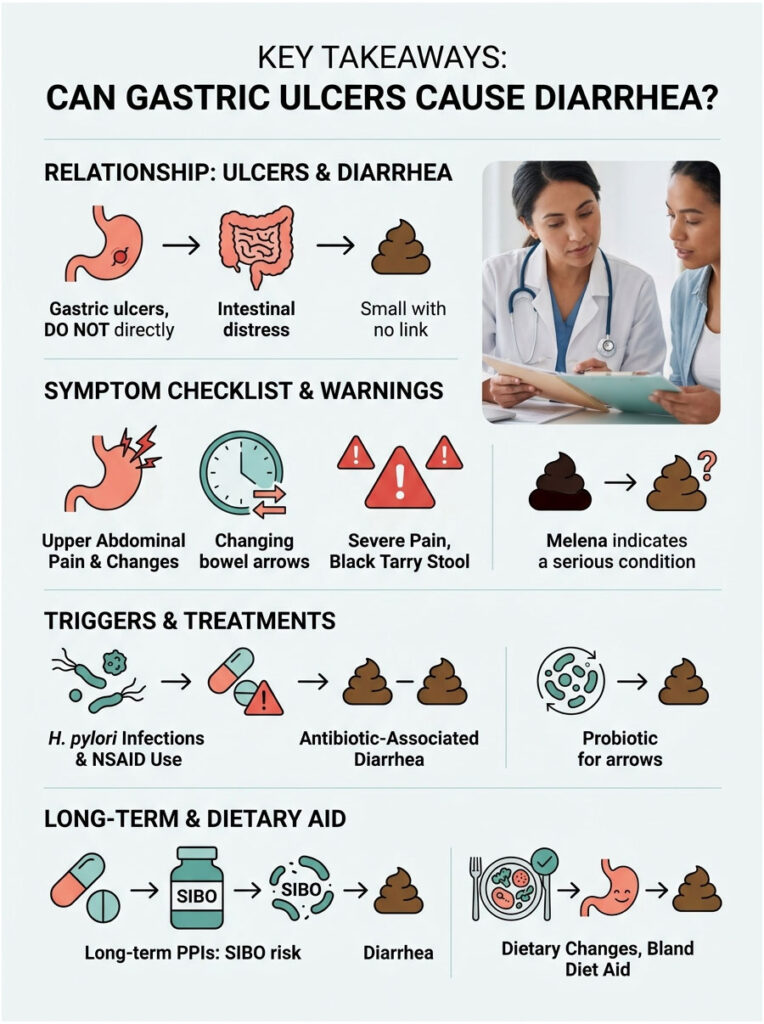
- H. pylori infection disrupts your microbiome and causes osmotic diarrhea through nutrient malabsorption.
- NSAID enteropathy inflames the small intestine, causing chronic cramping and loose stools alongside the stomach ulcer.
- The cathartic effect of blood from an actively bleeding ulcer acts as a powerful natural laxative, producing black, tarry melena.
- Triple Therapy antibiotics decimate healthy gut flora, causing antibiotic-associated diarrhea.
- Long-term Proton Pump Inhibitors can trigger Small Intestinal Bacterial Overgrowth (SIBO), creating a new source of chronic loose stools.
Never ignore sudden changes in bowel habits when you are also experiencing upper abdominal pain. Your digestive tract is a deeply connected system that requires comprehensive care. Peptic Ulcer Disease is highly treatable with modern, evidence-based medicine. Work closely with your gastroenterologist to heal your stomach lining and restore peace to your lower gut.
Frequently Asked Questions
Can a gastric ulcer directly cause diarrhea?
As a gastroenterologist, I often explain that a localized gastric ulcer does not physically force the colon to empty. However, the underlying triggers for the ulcer—such as an H. pylori infection, chronic NSAID use, or internal bleeding—frequently cause secondary intestinal distress and loose stools. We view the GI tract as a single ecosystem where upper abdominal pathology often creates a domino effect leading to lower bowel changes.
Why do I have diarrhea while taking Triple Therapy for H. pylori?
Antibiotic-associated diarrhea is extremely common during Triple Therapy. The heavy-duty antibiotics required to eradicate H. pylori are indiscriminate, meaning they decimate your healthy commensal flora alongside the harmful bacteria. This gut dysbiosis prevents the colon from properly absorbing water and processing waste, leading to the frequent loose stools many patients experience during their 14-day treatment course.
What is the ‘cathartic effect of blood’ in relation to stomach ulcers?
When a gastric ulcer erodes into a blood vessel, the resulting internal bleed introduces free blood into the digestive tract. Blood acts as a powerful natural laxative because its proteins and iron irritate the intestinal lining, significantly increasing motility. This ‘cathartic effect’ causes the bowels to empty rapidly and urgently, often resulting in the classic clinical presentation of melena.
How can I tell the difference between normal diarrhea and melena?
This is a critical distinction for patient safety. Normal diarrhea is typically brown, green, or yellow. Melena, which indicates an active upper GI bleed, is unmistakable: the stools appear pitch black, have a sticky, tarry consistency similar to road asphalt, and carry a distinctively foul, metallic odor. If you observe black, tarry stools, you must seek emergency medical evaluation immediately.
Can long-term use of Proton Pump Inhibitors (PPIs) cause diarrhea?
Yes, through a condition known as Small Intestinal Bacterial Overgrowth (SIBO). PPIs like Omeprazole heal ulcers by drastically reducing stomach acid, which normally acts as a chemical firewall against pathogens. Without this acid barrier, bacteria from the mouth or colon can migrate and colonize the small intestine, leading to chronic bloating, gas, and persistent diarrhea weeks or months after starting the medication.
What is NSAID enteropathy and how does it relate to ulcers?
While NSAIDs like Ibuprofen cause gastric ulcers by inhibiting protective prostaglandins in the stomach, they also cause widespread inflammation in the small intestine known as NSAID enteropathy. Up to 70% of chronic NSAID users develop this condition, which involves blunted villi and mucosal irritation. This dual-pronged attack means the same pills causing your stomach pain are likely the direct cause of your lower abdominal cramping and diarrhea.
Does H. pylori infection cause malabsorption and loose stools?
H. pylori fundamentally alters your gastric pH and disrupts the normal digestive process. By neutralizing stomach acid with the urease enzyme, the bacteria interfere with the breakdown of nutrients. This leads to nutrient malabsorption, where undigested particles pull excess water into the colon via osmosis, resulting in chronic dyspepsia and mild to moderate diarrhea.
Is diarrhea a symptom of Zollinger-Ellison Syndrome?
In cases of Zollinger-Ellison Syndrome, diarrhea is a hallmark symptom. The condition involves gastrin-producing tumors that force the stomach to secrete massive amounts of acid. This acid volume overwhelms the small intestine and inactivates pancreatic enzymes needed for fat digestion. The result is severe, watery, and foul-smelling diarrhea (steatorrhea) alongside multiple, difficult-to-heal gastric ulcers.
Can I take probiotics to stop diarrhea while treating an ulcer?
I frequently recommend specific probiotic strains to my patients during ulcer treatment. Saccharomyces boulardii, a yeast-based probiotic, is particularly effective because antibiotics cannot kill it. It helps maintain the gut barrier and significantly reduces the risk of antibiotic-associated diarrhea and C. diff infections. Lactobacillus rhamnosus GG is also highly beneficial, provided it is taken at least two hours apart from antibiotic doses.
When is stomach pain and diarrhea considered a medical emergency?
You should seek immediate emergency care if you experience ‘red flag’ symptoms: hematemesis (vomiting bright red blood or dark coffee-ground material), melena (black, tarry stools), or signs of a perforation. A perforated ulcer causes sudden, excruciating pain and a ‘board-like’ rigidity in the abdomen. These symptoms indicate life-threatening complications like major hemorrhage or systemic sepsis.
How do doctors diagnose the cause of concurrent upper and lower GI symptoms?
We utilize a multi-faceted diagnostic approach. The gold standard is an Upper Endoscopy (EGD) to visually inspect the gastric mucosal barrier for ulcers. To investigate the diarrhea, we may use Urea Breath Tests or Stool Antigen tests for H. pylori, Fecal Occult Blood Tests to detect microscopic bleeding, and occasionally fasting serum gastrin levels to rule out rare acid-secreting tumors.
What dietary changes help heal a gastric ulcer and stabilize the bowels?
During recovery, focus on a ‘bland’ diet that supports both the stomach and the colon. Lean proteins, steamed vegetables, and high-fiber foods like oatmeal help buffer stomach acid and promote well-formed stools. You must strictly avoid irritants like alcohol, caffeine, and nicotine, as these chemicals further damage the gastric lining and stimulate excessive intestinal motility, worsening diarrhea.
Disclaimer
This article is for informational and educational purposes only and does not substitute for professional medical advice, diagnosis, or treatment. Always consult with a board-certified physician or gastroenterologist regarding any severe gastrointestinal symptoms, sudden changes in bowel habits, or before starting new medications or supplements.
References
- American College of Gastroenterology (ACG) – https://gi.org/ – Provides clinical guidelines on the treatment of Helicobacter pylori infection and management of peptic ulcers.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – https://www.niddk.nih.gov/ – Official government data on Peptic Ulcer Disease and the mechanics of GI bleeding.
- Journal of Gastroenterology – “NSAID Enteropathy and Small Bowel Mucosal Damage Pathophysiology” – Peer-reviewed research detailing how painkillers damage the lower intestinal tract.
- Cleveland Clinic – https://my.clevelandclinic.org/ – Expert insights on Zollinger-Ellison Syndrome and acid hypersecretion.
- Mayo Clinic – https://www.mayoclinic.org/ – Statistical data on the prevalence of H. pylori and complications of gastrointestinal procedures.






