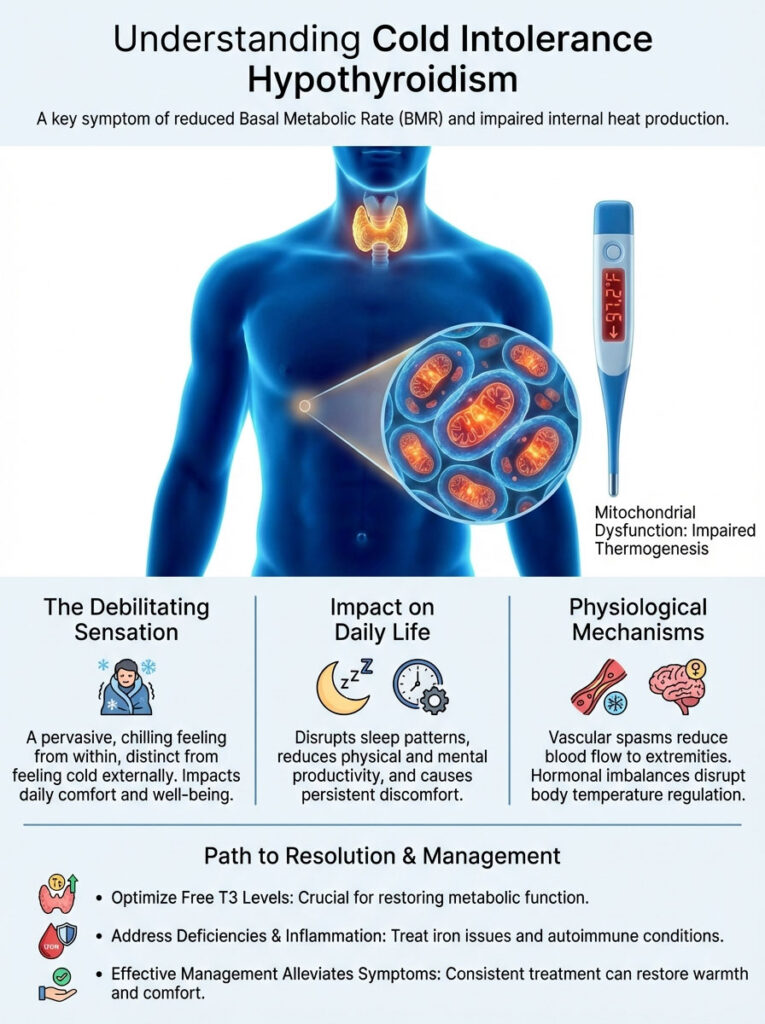
Cold intolerance hypothyroidism is a specific clinical symptom caused by a reduction in Basal Metabolic Rate (BMR) due to a lack of active thyroid hormone (T3) within the cells. Unlike normal sensitivity to weather, this condition is a result of mitochondrial dysfunction where cells fail to generate internal heat (thermogenesis). Resolving it typically requires optimizing Free T3 levels, addressing iron deficiencies, and treating underlying autoimmune inflammation.
Table of Contents
You are likely reading this while wearing a heavy sweater. You might be wrapped in a blanket or holding a warm mug. This happens even if the thermostat reads seventy-five degrees. This is not just a preference for being cozy.
It is a bone-deep, aching chill. It feels impossible to shake. In my clinical practice, I see this symptom every single day. Patients describe it vividly.
They say it feels like ice water is running through their veins instead of blood. This specific medical issue is known as cold intolerance hypothyroidism. It acts as a metabolic “canary in the coal mine.”
Long before the scale stops moving, the body’s internal thermostat fails. Long before hair starts thinning, your heat generation stops. For many, this is the most debilitating aspect of thyroid disease. It is constant.
It affects your sleep quality. It impacts your productivity at work. It destroys your comfort in your own home. This article is written to validate your experience.
We are going to explain the mechanics behind this chill. We are not looking at surface-level symptoms here. We are examining the mitochondrial failures. We will look at vascular spasms.
We will uncover the hormonal imbalances that keep you freezing. More importantly, we will discuss how to turn the heat back on. You do not have to live your life shivering.
Key Statistics: Thyroid and Thermoregulation
- 40%: The potential reduction in Basal Metabolic Rate (BMR) in severe hypothyroidism cases.
- 15-20%: Percentage of treated hypothyroid patients who remain symptomatic despite normal TSH levels.
- 30%: Approximate overlap of patients with Hashimoto’s who also suffer from Raynaud’s Phenomenon.
- 97.8°F: The minimum healthy waking basal body temperature; consistent readings below this suggest metabolic insufficiency.
- T3 Hormone: Responsible for nearly all mitochondrial heat production in the human body.
- 10x: Women are ten times more likely to suffer from thyroid-induced cold intolerance than men.
The Physiology of Thermogenesis: Your Metabolic Furnace
To understand why you are cold, you must understand heat generation. We often think of metabolism only regarding weight loss. We obsess over calorie burning for fat loss. However, the primary evolutionary purpose of metabolism is heat production.
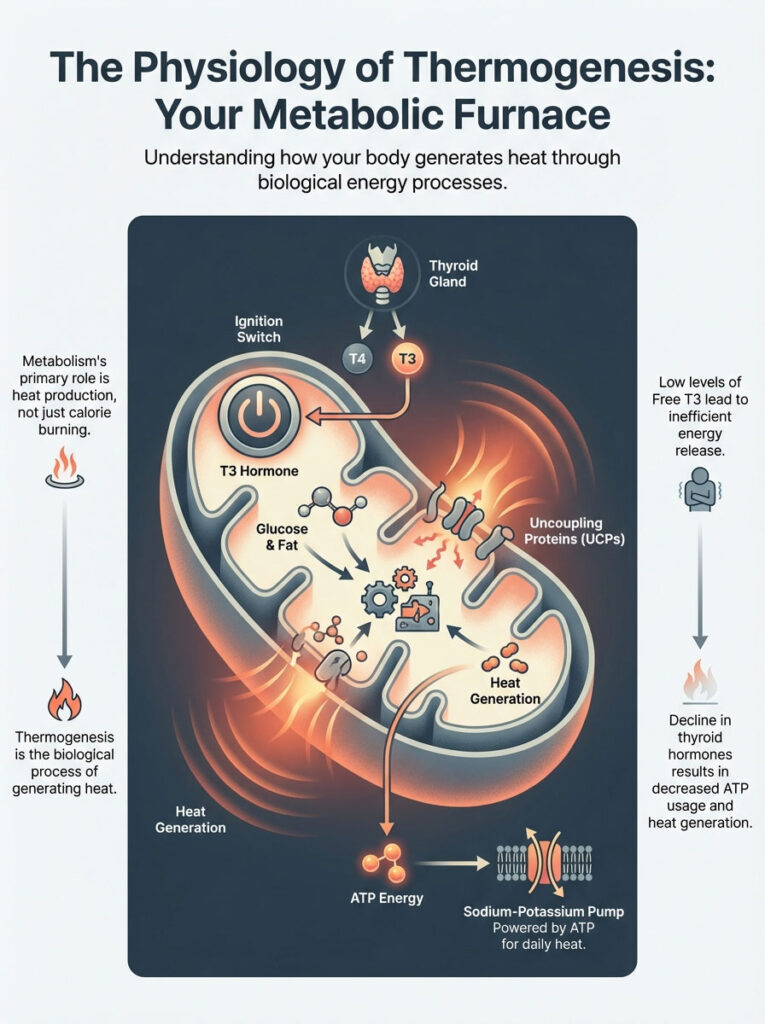
This biological process is called thermogenesis. Every cell in your body contains mitochondria. These are the power plants of your cells. In a healthy individual, mitochondria take fuel sources like glucose and fat.
They convert this fuel into energy known as ATP. A vital byproduct of this conversion is heat. This is your Basal Metabolic Rate (BMR) in action. It keeps you warm from the inside out.
The Role of Triiodothyronine (T3)
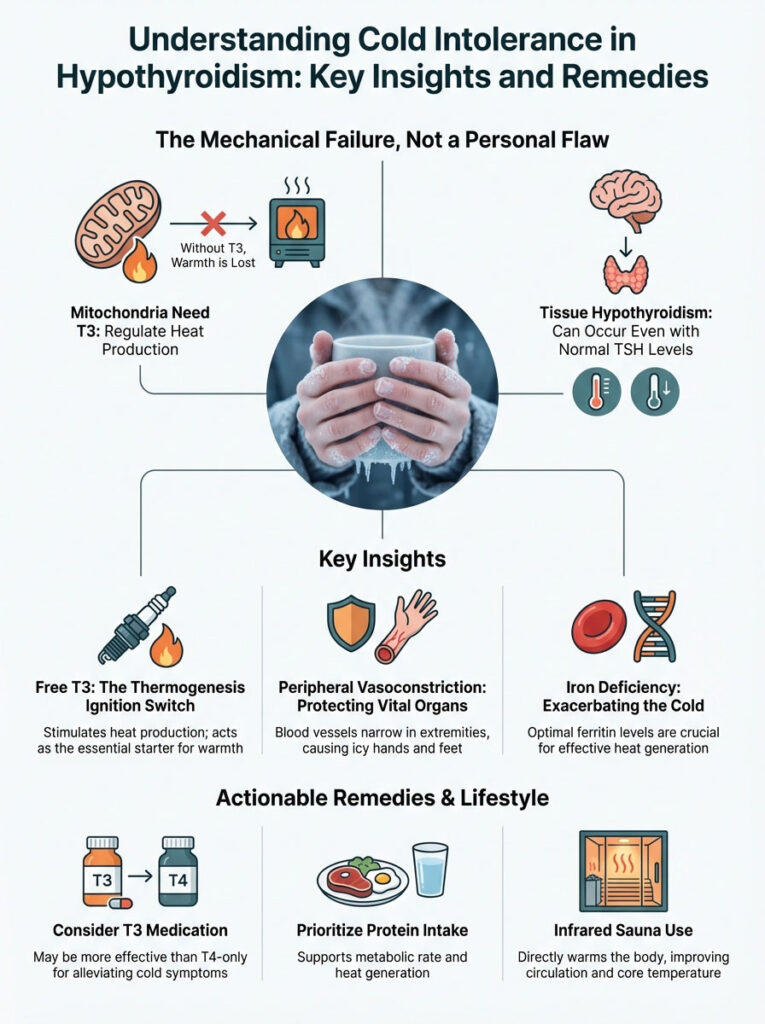
The thyroid gland produces a pro-hormone called T4 (thyroxine). It also produces a small amount of active hormone called T3 (triiodothyronine). T3 is the ignition switch for your furnace. It enters the nucleus of your cells.
Once inside, it binds to specific thyroid receptors. This binding action tells the DNA to produce specific proteins. These proteins work within the mitochondria. One of the most critical proteins is the “uncoupling protein” (UCP).
In a process called mitochondrial thermogenesis, these proteins change energy handling. Instead of trapping all energy as ATP for storage, UCPs release it. They cause the mitochondria to release a significant portion of energy directly as heat.
Without adequate Free T3, your body cannot produce enough UCPs. Consequently, your cells become efficient at storing energy. This leads to weight gain. Simultaneously, they become terrible at releasing energy as warmth.
This is the biological definition of cold intolerance hypothyroidism. Data published in the Journal of Applied Physiology confirms this. Hypothyroid patients can experience a drop in BMR ranging from 15% to 40%.
That is a massive reduction in daily energy output. Imagine your home furnace. If the engine is idling at 60% capacity, it cannot heat the house. The external temperature doesn’t matter; the internal engine is broken.
ATP Production and Energy Failure
There is another layer to this problem. Thyroid hormones regulate the sodium-potassium pump in your cells. This pump consumes a massive amount of energy. It is responsible for a large percentage of your daily basal heat production.
When thyroid hormones are low, this pump slows down. The cell uses less ATP. Less ATP usage means less heat is generated. This creates a compounding effect.
You have fewer uncoupling proteins releasing heat. You also have less cellular machinery working to create heat. The result is a body that feels like a stone. It cannot generate its own warmth.
Brown Adipose Tissue: The Hidden Heater
For decades, scientists thought only babies had Brown Adipose Tissue (BAT). We now know adults have it too. BAT is different from white fat. White fat stores calories.
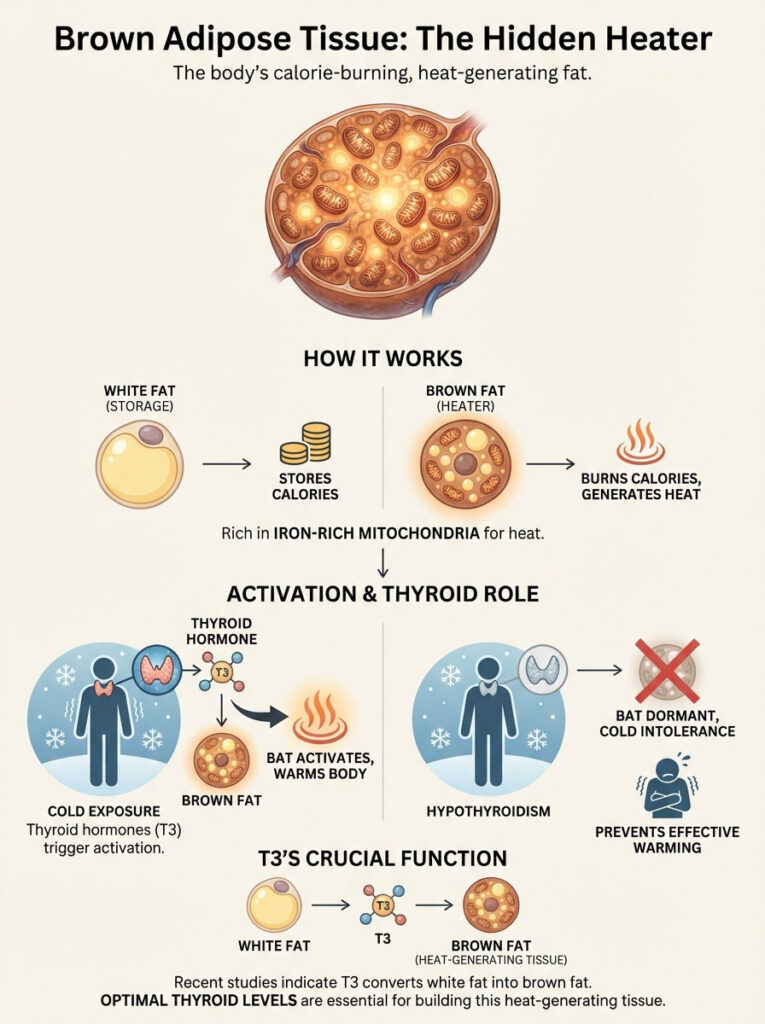
Brown fat burns calories. It is brown because it is densely packed with iron-rich mitochondria. Its sole purpose is to generate heat. This is called non-shivering thermogenesis.
Thyroid hormones are the primary signal that activates BAT. In a healthy person, cold exposure triggers the thyroid. The thyroid signals the brown fat. The brown fat turns on and warms the blood.
In cold intolerance hypothyroidism, this signal is broken. The brown fat remains dormant. This means you lose a critical survival mechanism. Even when you are exposed to cold, your internal heater stays off.
This explains why you cannot “warm up” once you get cold. A healthy person enters a warm room and adjusts. A hypothyroid patient stays cold for hours. Their brown fat is not doing its job.
Expert Insight: Recent studies suggest that T3 is required to convert white fat into beige or brown fat. Without optimal thyroid levels, you lose the ability to build new heat-generating tissue. This makes the cold intolerance progressive over time.
The Hypothalamus and Peripheral Vasoconstriction
Your body operates on a strict hierarchy of survival. The heart, lungs, and brain are the VIPs. The hands, feet, and skin are considered expendable. The hypothalamus is the master thermostat in the brain.
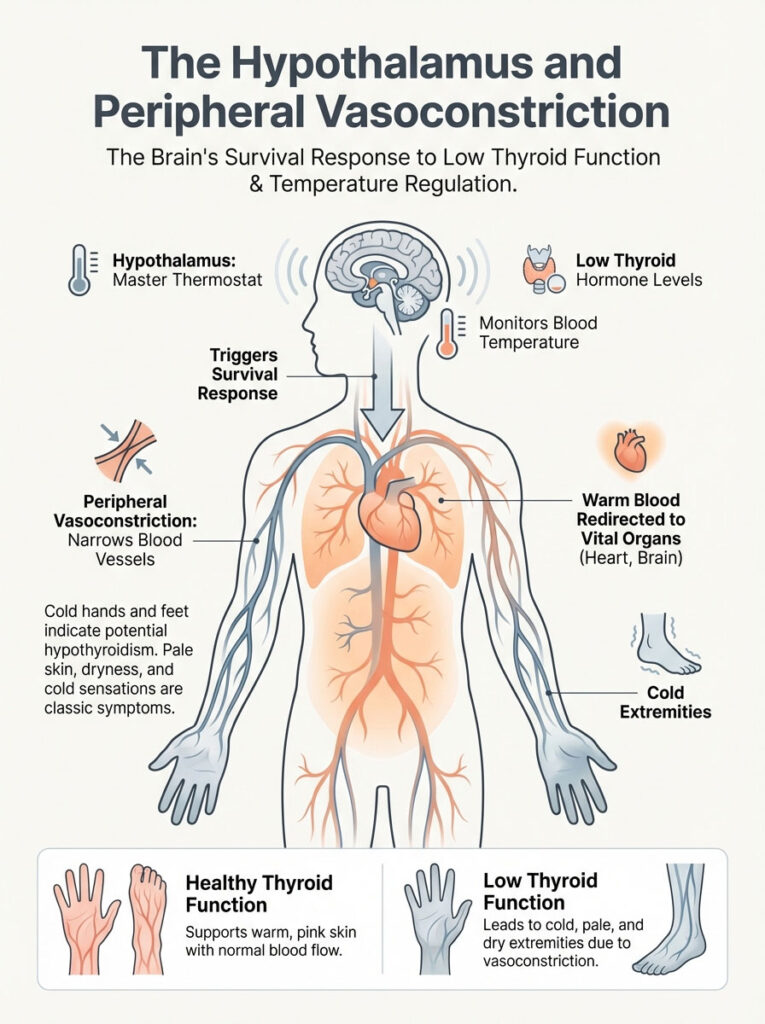
It acts like the control panel for your house. It constantly monitors blood temperature. It also monitors levels of circulating thyroid hormones. When thyroid hormone levels drop, the hypothalamus panics.
It senses a reduction in metabolic heat production. It perceives this as a threat to your core temperature. To protect your vital organs, it initiates a survival mechanism. This is known as peripheral vasoconstriction.
Why Your Hands and Feet Are Icy
Peripheral vasoconstriction is the narrowing of blood vessels. The body clamps down on the arteries feeding the extremities. It shunts warm blood back toward the core. This preserves heat for the heart and brain.
This is why a patient with hypothyroidism presents with cold hands. Their feet feel like ice blocks to the touch. This happens even if their core temperature is only slightly lowered. The body is sacrificing the comfort of your extremities.
This process also affects the skin. Healthy thyroid function supports cutaneous blood flow. This gives skin a warm and pink appearance. In hypothyroid states, blood flow to the skin is reduced.
This leads to the classic triad of symptoms. You get pale skin. You develop a dry texture. You experience a constant cold sensation.
The body is essentially hoarding heat. It refuses to “spend” heat on your hands or nose. It keeps it all in the chest and abdomen. This leaves you feeling frozen on the outside.
If you wear socks to bed even in summer, take note. This is a classic sign of peripheral vasoconstriction. It is driven by low metabolic output. Your body is struggling to pump heat to the furthest points.
The Autoimmune Overlap: Hashimoto’s and Raynaud’s Phenomenon
It is critical to distinguish between metabolic coldness and vascular spasms. The majority of hypothyroidism cases are caused by Hashimoto’s Thyroiditis. This is an autoimmune disease. If you have one autoimmune condition, you are at risk for others.
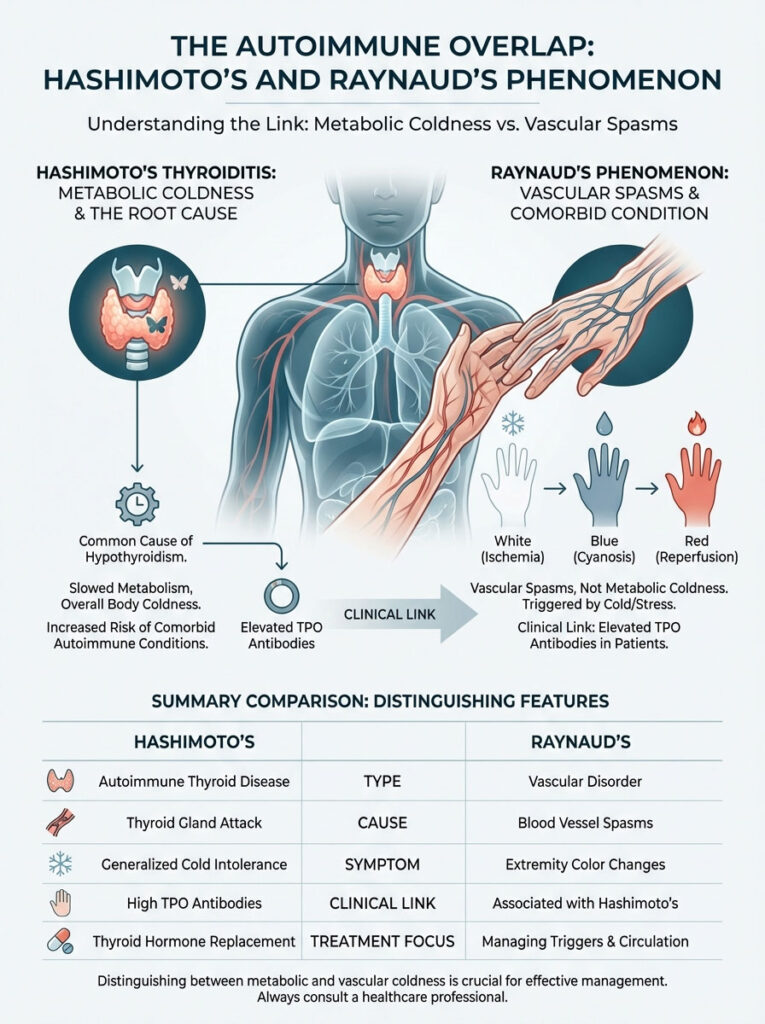
One of the most common comorbidities is Raynaud’s Phenomenon. While cold intolerance hypothyroidism is a constant chill, Raynaud’s is different. It is an aggressive and spasmodic attack on the blood vessels.
The Clinical Link
Research indicates a significant overlap. Patients with elevated Thyroid Peroxidase (TPO) antibodies often have Raynaud’s symptoms. In Raynaud’s, the blood vessels overreact. They react to cold or emotional stress.
They spasm and completely shut off blood flow. This results in a distinct color change sequence. First, the finger turns white. This is because blood flow is cut off.
Next, the finger turns blue. This indicates oxygen depletion in the tissues (cyanosis). Finally, it turns red. This happens when the spasm releases.
Blood rushes back in, causing stinging pain. This is called reperfusion. Understanding this distinction is vital for treatment. Increasing thyroid medication may fix metabolic coldness.
However, if you have secondary Raynaud’s, you may still have spasms. The treatment approaches differ. They are related but distinct.
Comparison Table: Metabolic Cold Intolerance vs. Raynaud’s Phenomenon
| Feature | Metabolic Cold Intolerance (Hypothyroidism) | Raynaud’s Phenomenon (Autoimmune/Vascular) |
|---|---|---|
| Primary Sensation | Deep, systemic chill; feeling cold “to the bone.” | Sharp, stinging pain; numbness in extremities. |
| Visual Signs | Pale, dry skin; general puffiness. | Distinct color changes (White → Blue → Red). |
| Triggers | Constant, regardless of mild temperature drops. | Acute response to cold touch or emotional stress. |
| Mechanism | Low BMR and reduced mitochondrial heat. | Aberrant vasospasms and sympathetic nervous system overactivity. |
| Primary Treatment | Thyroid hormone replacement (T4/T3). | Calcium channel blockers; warming agents; autoimmune management. |
The “Normal TSH” Paradox: Why You Are Still Freezing
The most frustrating experience for a patient is shivering in a doctor’s office. You are told, “Good news, your TSH is normal.” This disconnect is common. The Thyroid Stimulating Hormone (TSH) test is a screening tool.

It measures the pituitary gland’s request for hormone. It does not measure tissue hypothyroidism. It does not measure heat production. You can have a normal TSH and still suffer from cold intolerance hypothyroidism.
This paradox usually stems from poor T4 to T3 conversion. Your gland produces T4. T4 is metabolically inactive. It must be converted into T3 to generate heat.
The Deiodinase Conversion Problem
This conversion happens in the liver and gut. It also happens in peripheral tissues. It uses enzymes called deiodinases. Several factors can impair deiodinase enzyme activity.
If these enzymes are slow, you have plenty of storage hormone (T4). However, you have no active fuel (T3). Common inhibitors include chronic inflammation and insulin resistance. Nutrient deficiencies in Selenium and Zinc also play a role.
The Genetic Link: DIO2 Mutation
We must also look at genetics. There is a gene called DIO2. This gene codes for the Type 2 Deiodinase enzyme. This enzyme converts T4 to T3 inside the cells.
Some people have a polymorphism (mutation) on this gene. Their enzymes are less efficient. They may have normal blood levels of T4 and TSH. Yet, their intracellular T3 levels are low.
These patients often suffer from severe cold intolerance hypothyroidism. Standard T4-only medication (Levothyroxine) often fails them. Their bodies simply cannot process the raw material efficiently.
Reverse T3 (rT3) Dominance
When the body is under stress, it reacts. Stress can be physical, emotional, or from chronic dieting. The body may convert T4 into Reverse T3 (rT3). This is different from Free T3.
Think of Reverse T3 as a metabolic brake. It binds to the thyroid receptors on your cells. However, it does not turn them on. It blocks the active T3 from entering.
This creates a state of “cellular hypothyroidism.” Your blood tests might look acceptable to a general practitioner. But your cells are starving for the signal to produce heat. This is a primary driver of persistent cold intolerance.
Iron Deficiency and The Ferritin Connection
Iron is not just for red blood cells. It is required for thyroid hormone synthesis. The enzyme Thyroid Peroxidase is heme-dependent. This means it needs iron to function.
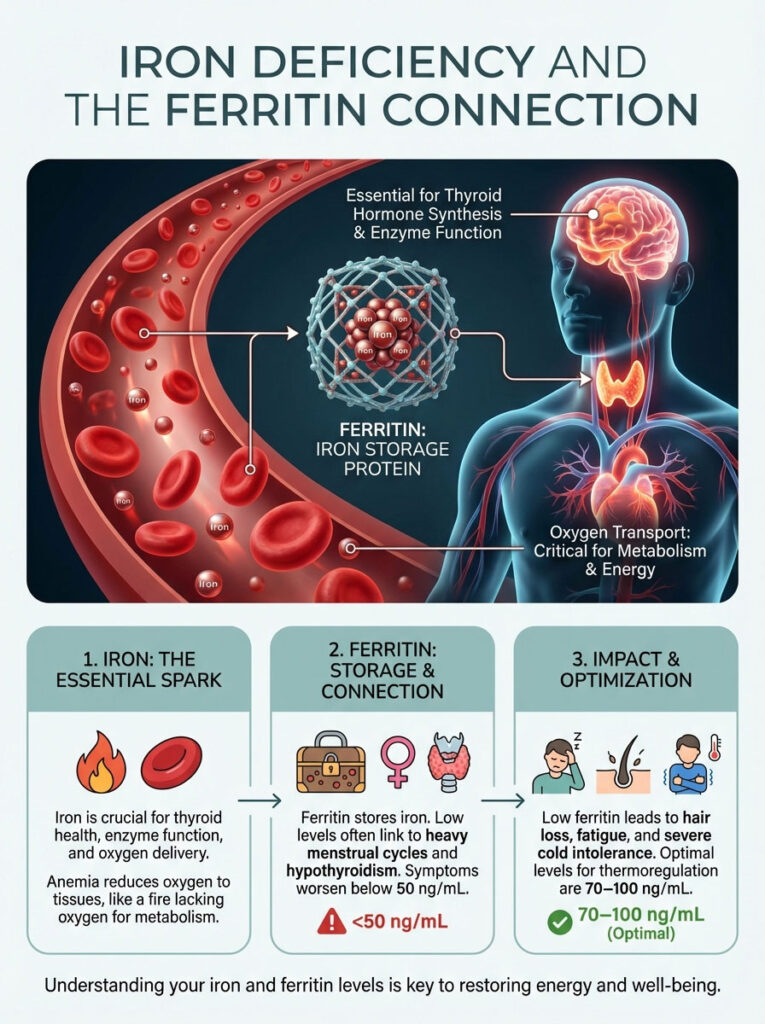
Furthermore, oxygen transport is critical for metabolism. Fire needs oxygen to burn. Your metabolism is a fire. If you are anemic, your tissues do not receive enough oxygen.
Without oxygen, you cannot burn fuel efficiently. This leads to a lower body temperature. We look closely at Ferritin. Ferritin is the iron storage protein.
Ferritin and thyroid function are inextricably linked. Many women with heavy menstrual cycles have low ferritin. Heavy cycles are common in hypothyroidism. It becomes a vicious cycle.
If ferritin drops below 50 ng/mL, symptoms worsen. Hair loss increases. Fatigue sets in. The symptoms of cold intolerance often become severe.
The clinical target for optimal thermoregulation is higher. We typically aim for ferritin levels between 70 and 100 ng/mL. Correcting iron levels can sometimes resolve the coldness without changing thyroid medication.
Diagnostic Protocol: Testing Beyond the TSH
If you are suffering from cold intolerance hypothyroidism, a simple TSH test is insufficient. It is like checking the gas gauge when the engine is broken. To understand why your furnace is failing, we need a complete picture.
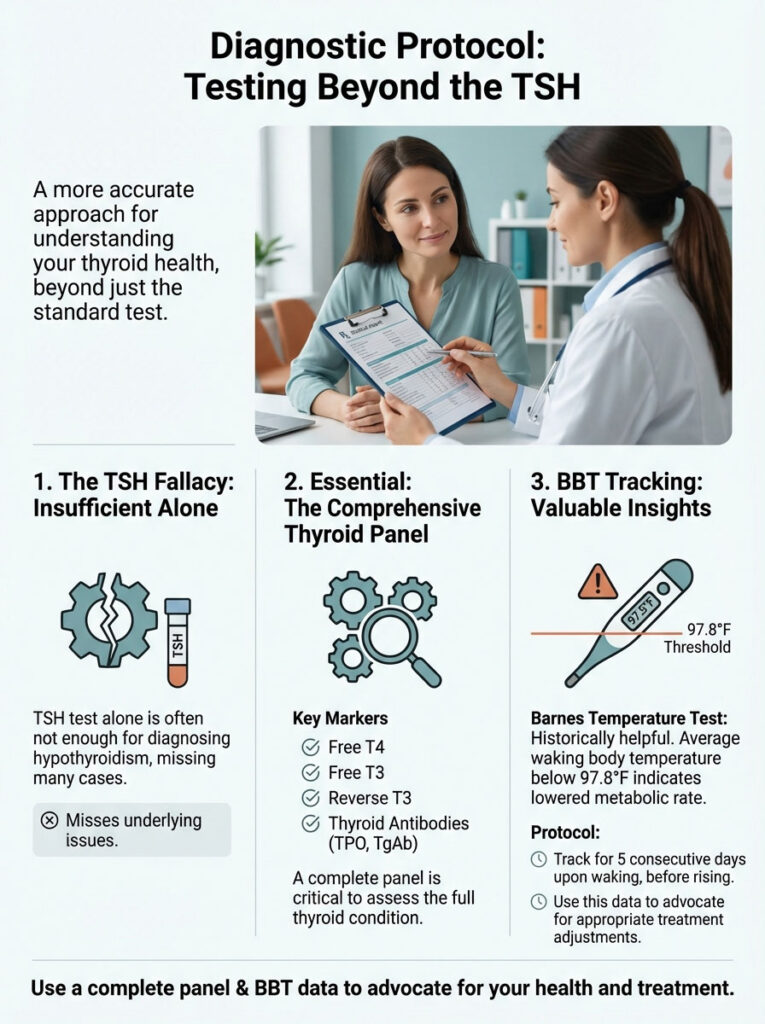
We need to see the fuel supply. We need to check the ignition system. A comprehensive panel should be negotiated with your provider.
The Complete Thyroid Panel
Requesting these specific markers provides the necessary data. It allows us to treat the coldness effectively:
- Free T3: This is the most important marker for cold intolerance. It tells us how much active hormone is available to stimulate mitochondrial thermogenesis.
- Free T4: This shows the available storage hormone.
- Reverse T3: This helps rule out conversion blocking or cellular resistance.
- Thyroid Antibodies (TPO & TgAb): To confirm Hashimoto’s Thyroiditis and assess autoimmune inflammation.
- Ferritin: To rule out iron deficiency as a root cause of metabolic slowing.
Basal Body Temperature (BBT) Tracking
Before modern blood tests, doctors used the “Barnes Temperature Test.” They used it to diagnose hypothyroidism. While we have better tools now, tracking body temperature regulation remains valuable.
Blood levels fluctuate throughout the day. Tissue response is more constant. This data can be a powerful tool. It helps when advocating for treatment adjustments.
How to track: Keep a thermometer by your bedside. Upon waking, do not sit up. Do not drink water yet. Take your temperature immediately.
Do this for five consecutive days. If your average is consistently below 97.8°F (36.5°C), take note. It is a strong physiological indicator of a lowered metabolic rate.
This holds true regardless of what the standard lab ranges say. It proves your body is not generating sufficient heat.
Medical Interventions: Restoring the Heat
Once we identify that cold intolerance hypothyroidism is the culprit, we act. The goal is to restore metabolic heat. The standard treatment is Levothyroxine (synthetic T4). For many patients, this works well.
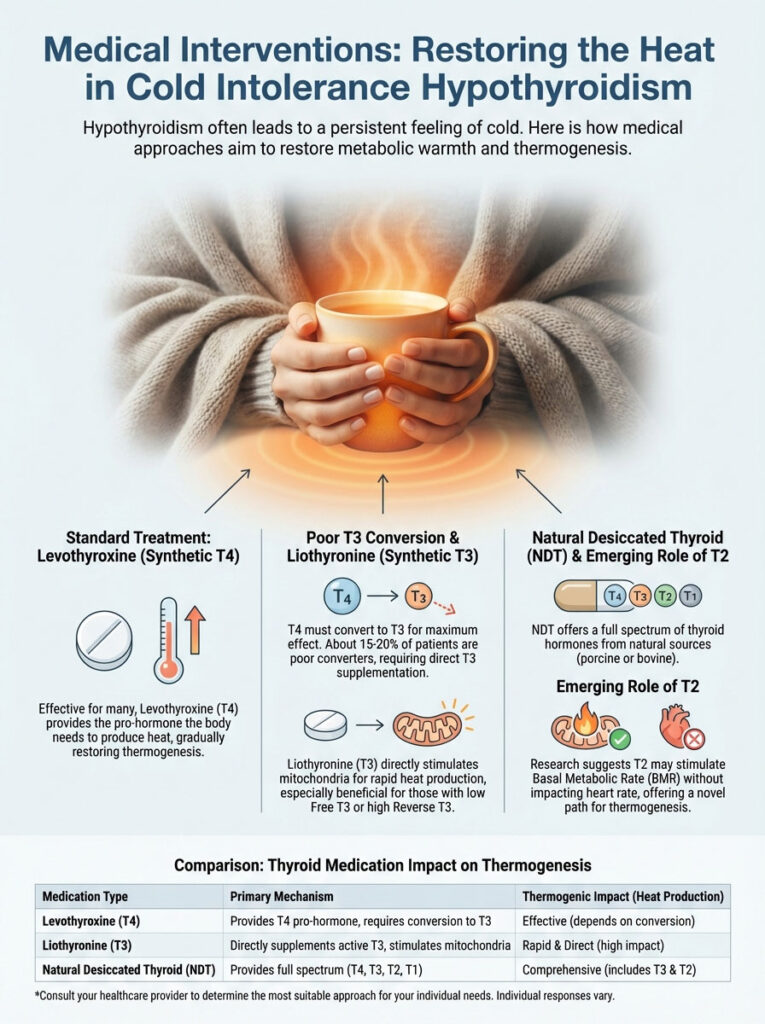
The body converts the T4 to T3. Warmth returns. However, remember the 15-20% of patients who are “poor converters.” For them, T4 alone is insufficient.
It is like putting gas in a car with no spark plugs. The fuel is there, but the ignition is missing.
Liothyronine (T3) Addition
For patients with low Free T3, we consider adding T3. This is also true for those with high Reverse T3. A synthetic T3 medication like Cytomel (Liothyronine) can be life-changing.
T3 does not require conversion. It bypasses the liver issues. It goes straight to the cells. It stimulates the mitochondria directly.
Patients often report rapid changes. Within days of starting T3 therapy, their extremities warm up. For some, it is the first time in years they have felt warm hands.
Natural Desiccated Thyroid (NDT)
Another valid option is Natural Desiccated Thyroid. Brands include Armour Thyroid or NP Thyroid. This medication is derived from porcine glands. It contains a full spectrum of hormones.
It includes T4, T3, T2, and T1. While T3 is the primary heat generator, T2 is interesting. Emerging evidence suggests T2 may also play a role.
It appears to stimulate Basal Metabolic Rate. It does this without affecting the heart rate as much as T3. For patients who prefer a biological match, NDT is often superior. It can often resolve cold intolerance better than synthetic monotherapy.
Comparison Table: Thyroid Medication Impact on Thermogenesis
| Medication Type | Hormones Provided | Impact on Cold Intolerance | Ideal Patient Profile |
|---|---|---|---|
| Levothyroxine | T4 Only | Effective if conversion pathways are healthy. | Standard hypothyroid patients with no conversion issues. |
| Liothyronine | T3 Only | Potent, direct stimulation of heat production. | Patients with normal T4 but low Free T3 or high Reverse T3. |
| Combination Therapy | Synthetic T4 + T3 | Mimics natural physiology; balanced heat restoration. | Patients with lingering symptoms on T4 monotherapy. |
| Desiccated Thyroid (NDT) | T4, T3, T2, T1 | Broad spectrum; T2 may play a specific role in BMR. | Patients preferring natural options or those who fail synthetic therapy. |
Nutritional and Lifestyle Biohacks for Thermoregulation
Medication is the foundation. Lifestyle factors build the house. To fully resolve cold intolerance hypothyroidism, you must support your enzymes. You must support the chemistry of metabolism.
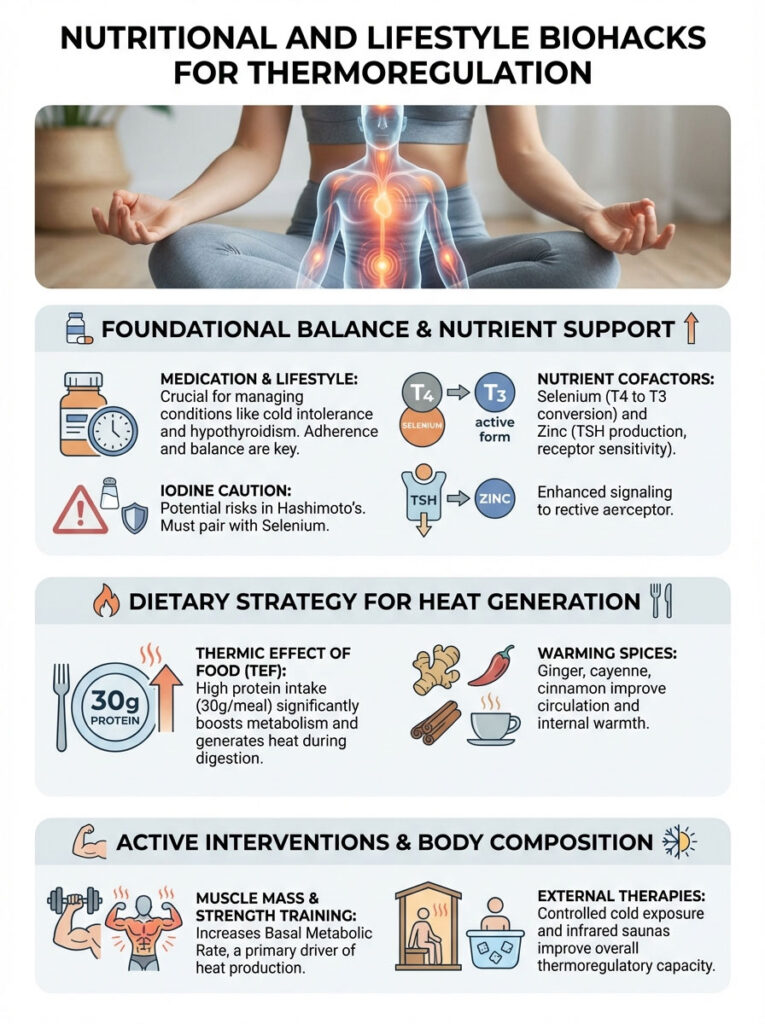
Certain nutrients act as cofactors. These are the “helpers” that allow chemical reactions to occur.
Critical Nutrient Cofactors
Selenium is perhaps the most vital mineral. It is required for the deiodinase enzymes. These enzymes strip an iodine atom off T4 to create T3. Without adequate selenium, conversion stalls.
Zinc is equally important. It supports TSH production. It also improves receptor sensitivity. Tyrosine is the amino acid backbone of thyroid hormones.
A word of caution on Iodine is necessary. It is the building block of the hormone. However, adding high-dose iodine to a Hashimoto’s Thyroiditis patient is risky. It can trigger an inflammatory storm.
This is known as the Wolf-Chaikoff effect. Iodine should be used judiciously. It should always be paired with selenium.
Dietary Strategy: The Thermic Effect of Food
What you eat influences your heat production. This is called the Thermic Effect of Food (TEF). Protein has a much higher TEF than carbohydrates or fats.
Digesting protein requires significant energy. This energy expenditure releases heat. Increasing dietary protein intake provides a boost. It offers a temporary but helpful increase in core temperature.
Aim for 30 grams of protein per meal. This stokes the metabolic fire three times a day. Incorporating warming spices also helps. Ginger, cayenne, and cinnamon can improve circulation.
Physical Interventions and Muscle Mass
Building muscle is a long-term strategy. It is one of the only ways to permanently increase your Basal Metabolic Rate. Muscle tissue is metabolically active.
It generates heat even at rest. Fat tissue is insulating but metabolically quiet. Strength training is therefore a therapeutic intervention. It is a treatment for cold intolerance.
Paradoxically, some patients benefit from cold plunging. This sounds counterintuitive. Why would a freezing person jump in cold water? Brief, controlled cold exposure works.
It forces the body to recruit Brown Adipose Tissue (BAT). It shocks the system into activation. Over time, this trains the body to generate heat more efficiently. However, this should be approached with caution.
Only attempt this when thyroid levels are stabilized. Start with 15 seconds of cold water at the end of a shower.
Infrared saunas are another excellent tool. They penetrate tissues deeply. They improve peripheral vasoconstriction issues. They encourage blood flow to the capillaries in the skin.
This can help retrain the autonomic nervous system. It teaches the vessels to dilate rather than constrict.
The Psychological Toll of Chronic Cold
We must acknowledge the mental impact. Living in a state of constant cold is exhausting. It triggers a low-level survival response in the brain.
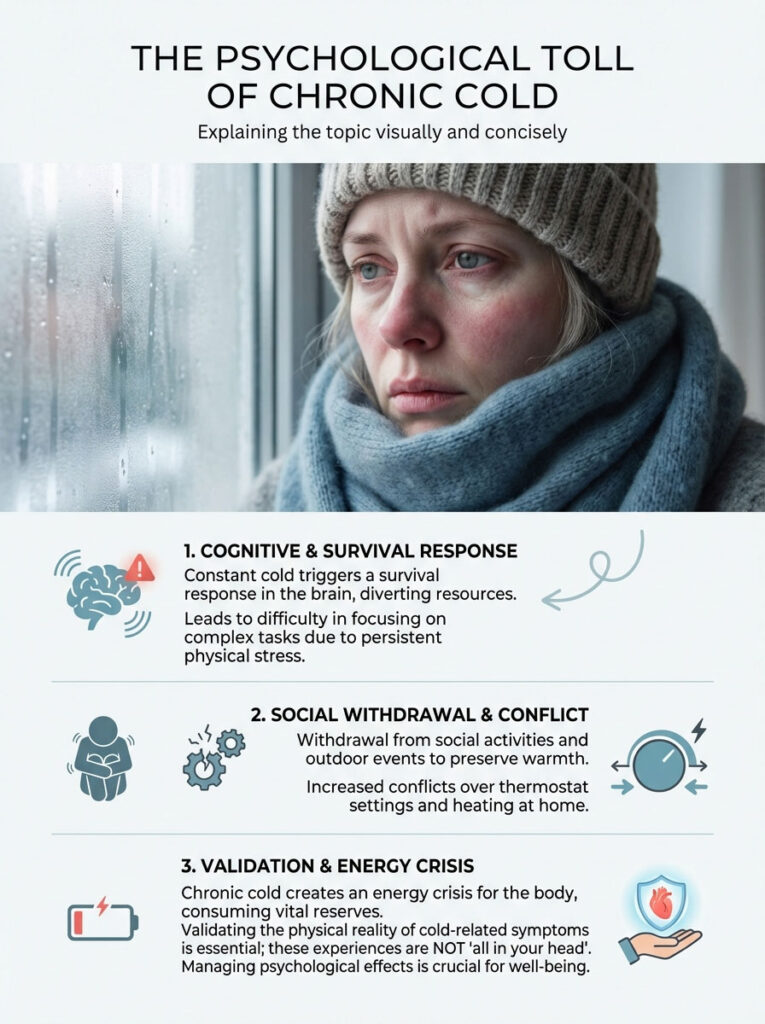
When you are freezing, your brain focuses on seeking warmth. It becomes harder to focus on complex tasks. It creates a background radiation of physical stress.
Patients often withdraw from social activities. They avoid outdoor events. They fight with spouses over the thermostat settings. This is not “all in your head.”
It is a physiological reality. Validating this symptom is the first step to managing it. You are not being difficult. Your body is in an energy crisis.
Differential Diagnosis: What If It Isn’t the Thyroid?
While cold intolerance hypothyroidism is the likely culprit, we must be thorough. If thyroid treatment fails, we look elsewhere. The endocrine system is a web.
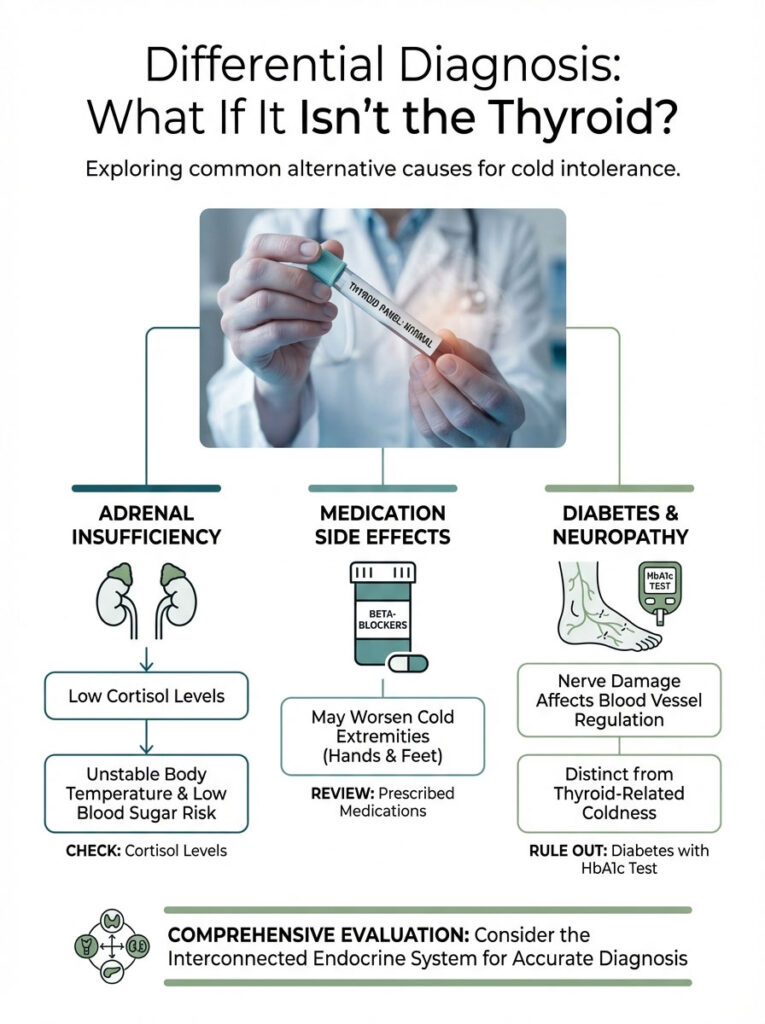
Pulling one string affects the others. We must consider other possibilities.
Adrenal Insufficiency
The adrenal glands produce cortisol. Cortisol works in tandem with thyroid hormones. If you have HPA axis dysfunction, you may struggle.
Low cortisol can lead to low blood sugar. It leads to unstable body temperature. If your temperature fluctuates wildly, check your adrenals. Adrenal support may be necessary to stabilize the system.
Medication Side Effects
Review your current medication list. Beta-blockers are often prescribed for high blood pressure or anxiety. They reduce heart rate.
However, they can worsen peripheral vasoconstriction. This leads to cold hands and feet. Discuss this with your cardiologist if the cold is severe.
Diabetes and Neuropathy
Uncontrolled blood sugar damages nerves. This is called diabetic neuropathy. It can damage the nerves that control blood vessel diameter.
This can lead to feelings of coldness in the feet. It is distinct from thyroid coldness but can coexist. A simple HbA1c test can rule this out.
Summary & Key Takeaways
Living with cold intolerance hypothyroidism is not a character flaw. It is not a result of “getting older.” It is a mechanical failure of the body’s energy systems.
It signifies that your mitochondria are off-line. They are not receiving the T3 signal required to generate heat. To reclaim your warmth, remember this checklist:
- Test, Don’t Guess: Demand a full panel including Free T3, Reverse T3, and Ferritin. Do not settle for TSH alone.
- Track Your Temp: Use morning basal body temperature. This monitors your metabolic state better than a single blood draw.
- Optimize Meds: If T4 alone isn’t working, advocate for yourself. Discuss adding Liothyronine or switching to NDT.
- Check Your Iron: Ensure Ferritin is above 70 ng/mL. This supports the oxygen transport needed for fire.
- Fuel the Conversion: Take Selenium and Zinc. Eat adequate protein to support the thermic effect of food.
There is hope. You do not have to spend your life in a sweater. With the right combination of bio-identical hormones and lifestyle changes, you can recover.
You can stoke the metabolic fire. You can finally put the winter coat away.
Frequently Asked Questions
Why do I feel cold when my TSH lab results are within the normal range?
TSH is a pituitary marker that doesn’t always reflect cellular metabolic activity or T4 to T3 conversion efficiency. You may have “tissue hypothyroidism” where low levels of active Free T3 prevent your mitochondria from generating adequate heat, despite a normal TSH reading.
How does the Free T3 hormone specifically regulate body temperature?
Free T3 acts as the primary ignition switch for mitochondrial thermogenesis by stimulating uncoupling proteins (UCPs) within the cells. These proteins allow mitochondria to release energy as heat rather than just storing it as ATP, effectively keeping your internal furnace running.
What is the difference between metabolic cold intolerance and Raynaud’s phenomenon?
Metabolic cold intolerance is a systemic, deep-seated chill caused by a low basal metabolic rate, whereas Raynaud’s involves acute vasospasms that turn fingers white or blue. While both are common in Hashimoto’s patients, Raynaud’s is a vascular overreaction to stress or cold, while thyroid coldness is a failure of internal heat production.
Why are my hands and feet always icy even when the room is warm?
When your hypothalamus senses low thyroid hormone levels, it initiates peripheral vasoconstriction to protect your vital organs. By shunting warm blood away from the extremities and toward the core, your body sacrifices the comfort of your hands and feet to maintain core temperature.
Can an iron deficiency make hypothyroid cold intolerance worse?
Yes, ferritin is a critical cofactor for the Thyroid Peroxidase enzyme and is necessary for efficient oxygen transport to your tissues. Without optimal ferritin levels (typically between 70-100 ng/mL), your metabolism lacks the “oxygen” needed to fuel the fire of thermogenesis.
What is the best thyroid medication for patients who are always cold?
For patients who are “poor converters,” T4-only medications like Levothyroxine may not resolve coldness. Adding Liothyronine (T3) or switching to Natural Desiccated Thyroid (NDT) can provide the direct active hormone needed to stimulate the mitochondria and restore warmth.
How can I use basal body temperature to track my thyroid health?
By taking your temperature immediately upon waking for five consecutive days, you can assess your true metabolic output. A consistent waking temperature below 97.8°F often indicates a state of metabolic insufficiency or poor thyroid hormone action at the cellular level.
What role does Reverse T3 play in feeling chronically cold?
Reverse T3 acts as a metabolic brake by competing with Free T3 for receptor sites on your cells. When Reverse T3 is dominant—often due to stress or inflammation—it blocks the “heat” signal, leaving you shivering despite having “normal” levels of other thyroid hormones.
Can selenium and zinc supplements improve my internal temperature?
These minerals are essential cofactors for the deiodinase enzymes that convert inactive T4 into active, heat-producing T3. Optimizing your selenium and zinc intake supports the chemical pathways that allow your body to generate its own warmth from the inside out.
How does brown adipose tissue (BAT) affect thermogenesis in thyroid patients?
Brown adipose tissue is a specialized fat that burns calories specifically to produce heat, a process triggered by thyroid hormones. In hypothyroid states, the signal to activate BAT is weakened, meaning you lose your primary biological defense against cold environments.
Does eating more protein help with thyroid-related cold intolerance?
Increasing protein intake boosts the Thermic Effect of Food (TEF), as the body requires significant energy to digest amino acids. This metabolic work generates temporary heat, helping to stoke your internal furnace and raise your core temperature after meals.
Can infrared saunas help retrain my body’s response to cold?
Infrared saunas penetrate deep into the tissues to encourage vasodilation and improve peripheral circulation. This can help counteract the chronic vasoconstriction seen in hypothyroidism, retraining your blood vessels to stay open and keep your skin and extremities warm.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. Cold intolerance can be a symptom of various underlying conditions. Always consult a qualified healthcare professional or endocrinologist before starting new medications, changing your dosage, or beginning a supplement regimen.
References
- Journal of Applied Physiology – “Thyroid Hormone Regulation of Thermogenesis and Metabolic Rate” – Detailed study on how T3 impacts uncoupling proteins (UCPs) in mitochondria.
- American Thyroid Association (ATA) – https://www.thyroid.org – Clinical guidelines on the symptoms of hypothyroidism and the role of T4/T3 replacement.
- Endocrine Reviews – “The Role of Brown Adipose Tissue in Human Metabolism” – Research regarding how thyroid hormones activate BAT for non-shivering thermogenesis.
- National Institutes of Health (NIH) – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3821486/ – Study on the impact of iron deficiency (Ferritin) on thyroid peroxidase activity.
- Journal of Clinical Endocrinology & Metabolism – “The TSH Paradox: Why Tissue Hypothyroidism Persists Despite Normal Serum Levels” – Analysis of T4 to T3 conversion and the DIO2 gene polymorphism.
- The Lancet Diabetes & Endocrinology – “Psychological and Physiological Impacts of Chronic Hypothyroid Symptoms” – Statistical data on the 15-20% of patients who remain symptomatic on T4 monotherapy.