IMPORTANT HEALTH ADVISORY: NEVER stop taking a prescribed medication like an antibiotic, steroid, or blood thinner before a lab test unless you are specifically instructed to do so by your doctor. The health risks of stopping these critical medications almost always outweigh any potential impact on your lab results. This guide is for informational purposes to help you have a more productive conversation with your healthcare provider.
Sarah stared at her patient portal, her heart sinking. She’d been on a course of prednisone for a nasty bout of poison ivy, and now her lab results were flagged with alarming red letters: “HIGH GLUCOSE,” “HIGH WHITE BLOOD CELL COUNT.” Her mind raced—”Do I have diabetes? Am I fighting some terrible infection?”
- Steroids (Prednisone, Medrol) — The "System Shock" Effect on Your Labs
- Blood Thinners (Warfarin, Eliquis, Plavix) — A Tale of Targets and Red Flags
- Antibiotics — The Expected Changes and the Dangerous Surprises
- The Ultimate Cheat Sheet: Your Medication & Lab Test Summary Table
- Conclusion: From Anxious Patient to Empowered Health Partner
- Frequently Asked Questions (FAQ)
This moment of panic is one that countless patients experience. Your lab results don’t exist in a vacuum; they tell a story that is deeply intertwined with the medications you’re taking.
This guide is different from a standard medical encyclopedia. It’s not just a list of facts. This is a guide to understanding the story your labs are telling, written to feel like a conversation with an experienced and compassionate clinician who has seen these scenarios thousands of times. Our mission is to translate the complex language of your lab report into plain English, to transform your anxiety into understanding, and to empower you to become a true partner in your healthcare. We will go beyond what your results are, and dive deep into the why.
At HealthCareOnTime.com, we believe an informed patient is an empowered one. Let’s decode your results together.
Steroids (Prednisone, Medrol) — The “System Shock” Effect on Your Labs
Think of corticosteroids like a system-wide override switch. They are incredibly effective at shutting down inflammation for conditions ranging from asthma and allergic reactions to autoimmune diseases, but that powerful signal sends ripples through your entire metabolism. Your lab report is where you see the clear evidence of that system shock.
The Most Common Shock: Steroid-Induced Hyperglycemia
This is, without a doubt, the most frequent and dramatic change doctors see in patients taking oral steroids.
The Scenario
You took a Medrol Dosepak for severe back pain, and your routine blood test now shows your blood sugar is 250 mg/dL.
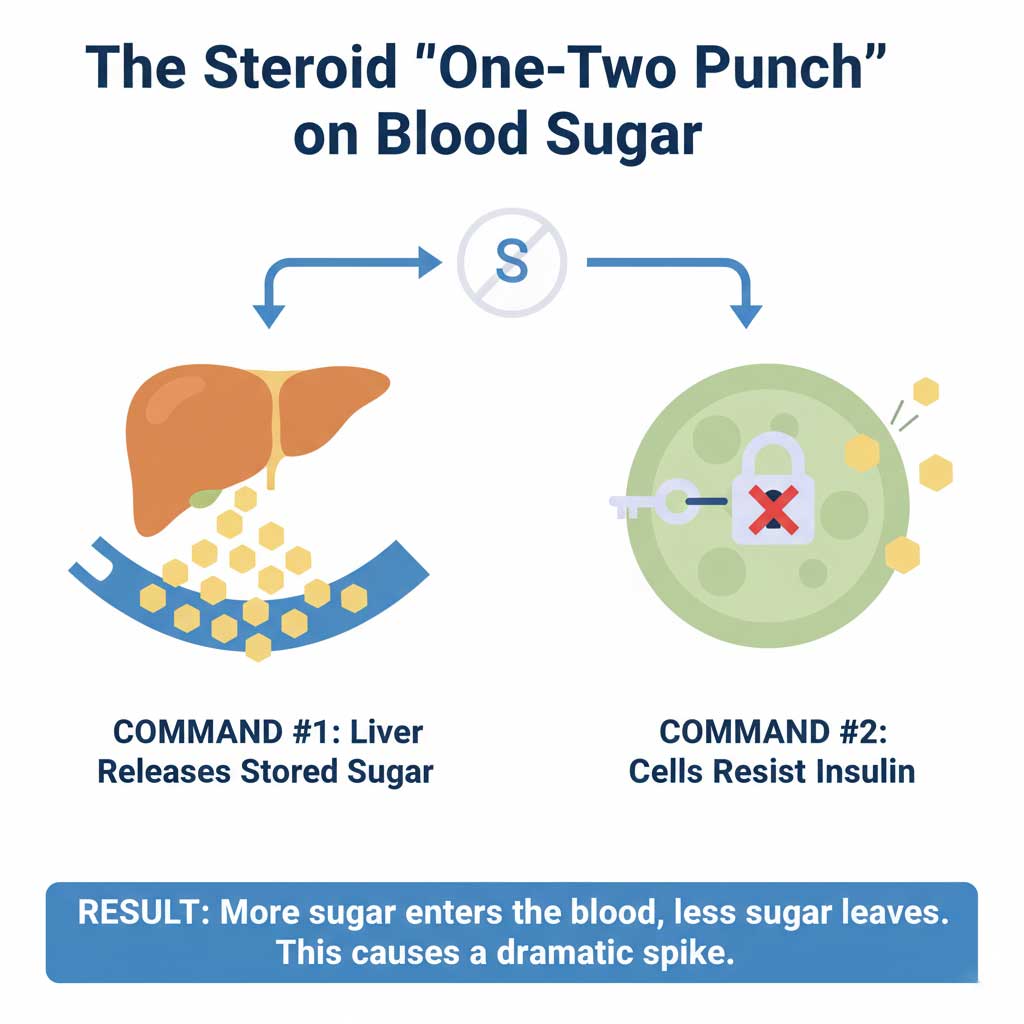
The Clinical Explanation (The Deep “Why”)
This isn’t just a random side effect; it’s a direct command from the medication. Steroids order your liver to dump its stored sugar (a process called gluconeogenesis) into your bloodstream. At the same time, they make your body’s cells more resistant to insulin, the hormone that normally knocks on the cell’s door to let sugar in. This one-two punch of “more sugar in the blood” and “less sugar leaving the blood” is why the spike can be so dramatic, even in people who have never had diabetes.
What It Means For You
For most people, this high blood sugar is temporary and will resolve after they finish the course of steroids. However, it’s still critical to tell your doctor. For patients with pre-diabetes or existing diabetes, this effect can be medically serious and may require temporary medication adjustments to prevent dangerous complications. Be mindful of the classic signs of very high blood sugar: excessive thirst, frequent urination, and unexplained fatigue.
The “Fake Infection”: Why Steroids Inflate Your White Blood Cell Count
This is one of the most misunderstood and anxiety-inducing lab results a patient can see.
The Scenario
Your routine Complete Blood Count (CBC) shows a White Blood Cell (WBC) count of 17,000 cells/mcL (normal is 4,500-11,000), but you don’t feel sick at all.
The Clinical Explanation (The Deep “Why”)
A doctor demonstrates true expertise by not jumping to conclusions here. This is almost never a sign of infection. Imagine your neutrophils (a key type of white blood cell) are soldiers. Most of them aren’t actively patrolling your bloodstream; they’re resting on the “sidelines,” stuck to the inner walls of your blood vessels in reserve. Steroids blow a loud whistle, forcing all those reserves to let go and jump into the main parade—your bloodstream—all at once. The lab test only counts the soldiers currently marching in the parade, so the number looks terrifyingly high.
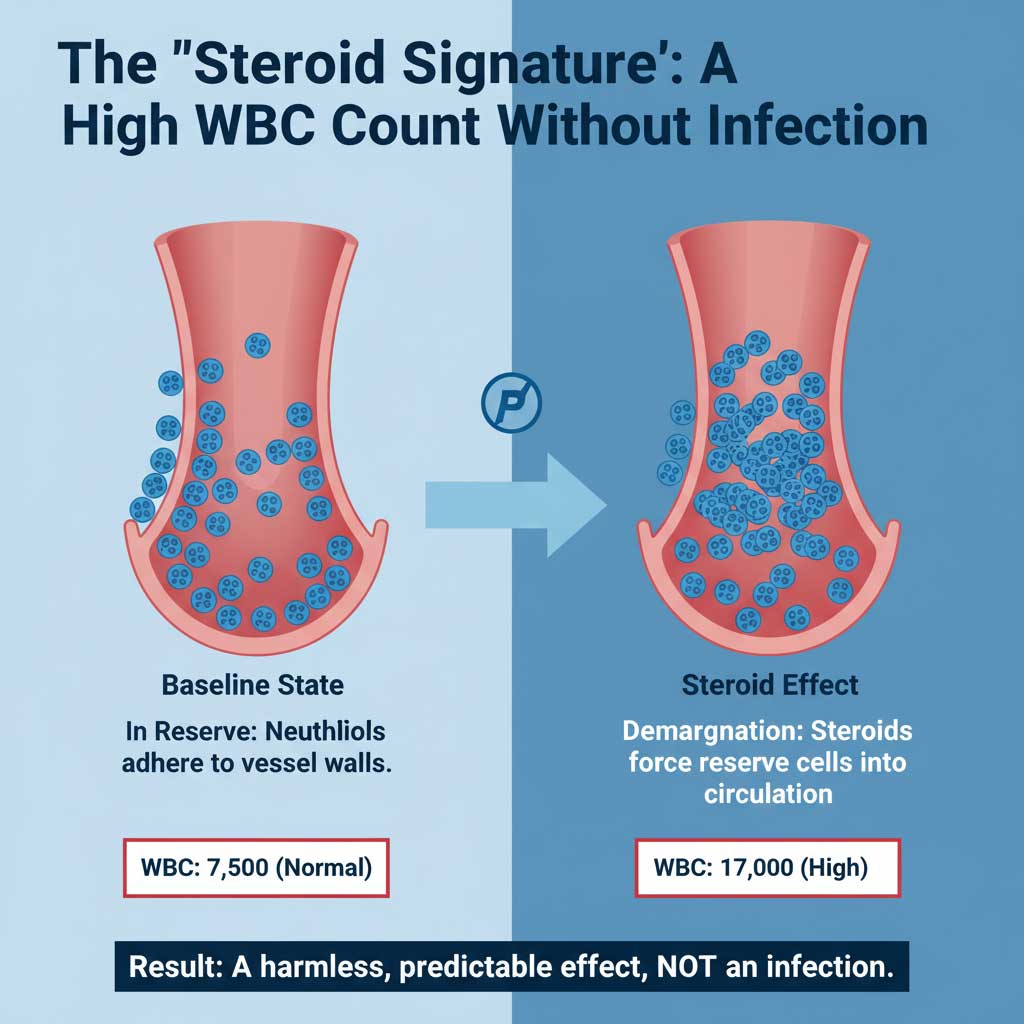
An experienced clinician will look at the WBC differential for the real story. A high total WBC count paired with a very high percentage of neutrophils but very low percentages of other cells like lymphocytes and eosinophils is the classic, harmless “steroid signature.”
What It Means For You
It is absolutely essential that your doctor knows you are on a steroid. This knowledge prevents a misdiagnosis of a serious infection and saves you from a course of unnecessary antibiotics. It’s a perfect example of how one piece of information—”I’m taking prednisone”—can completely change the interpretation of a lab result.
The “Invisible” Inflammation: Masking Disease Activity
This effect is the very reason steroids are prescribed, but it can be a double-edged sword.
The Scenario
You have an autoimmune condition like rheumatoid arthritis and your joints are aching, but your C-Reactive Protein (CRP) test—a key inflammation marker—comes back at a perfect level of <1.0 mg/L.
The Clinical Explanation (The Deep “Why”)
The CRP test is a direct measure of inflammation in your body. Steroids are the most powerful anti-inflammatory drugs we have. They don’t just reduce inflammation; they obliterate the very protein markers that the test is designed to find. Your lab result isn’t a lie, but it’s reflecting the medication’s powerful effect, not the underlying reality of your disease.
What It Means For You
This shows the medicine is working powerfully, but it also means you and your doctor cannot rely on that lab value alone to gauge your condition. Your personal experience and reported symptoms become even more important. You must be the one to tell your doctor, “I know the number looks good, but I’m still feeling…”
Other Key Changes: Cholesterol & Electrolytes
Steroids can also affect your Lipid Panel, sometimes raising LDL (“bad”) cholesterol and triglycerides over the long term. They can also show up on a Basic Metabolic Panel (BMP) by causing the kidneys to waste potassium, potentially leading to low potassium levels (hypokalemia).
Blood Thinners (Warfarin, Eliquis, Plavix) — A Tale of Targets and Red Flags
The term “blood thinner” covers a wide range of medications that work in completely different ways. Understanding your specific medication and its target lab test is one of the most critical aspects of patient safety. For these drugs, lab tests are not a side issue—they are central to the therapy itself.
The Classic: Warfarin (Coumadin) and the PT/INR
For decades, warfarin was the standard, and its monitoring is a perfect example of an intentional lab alteration.
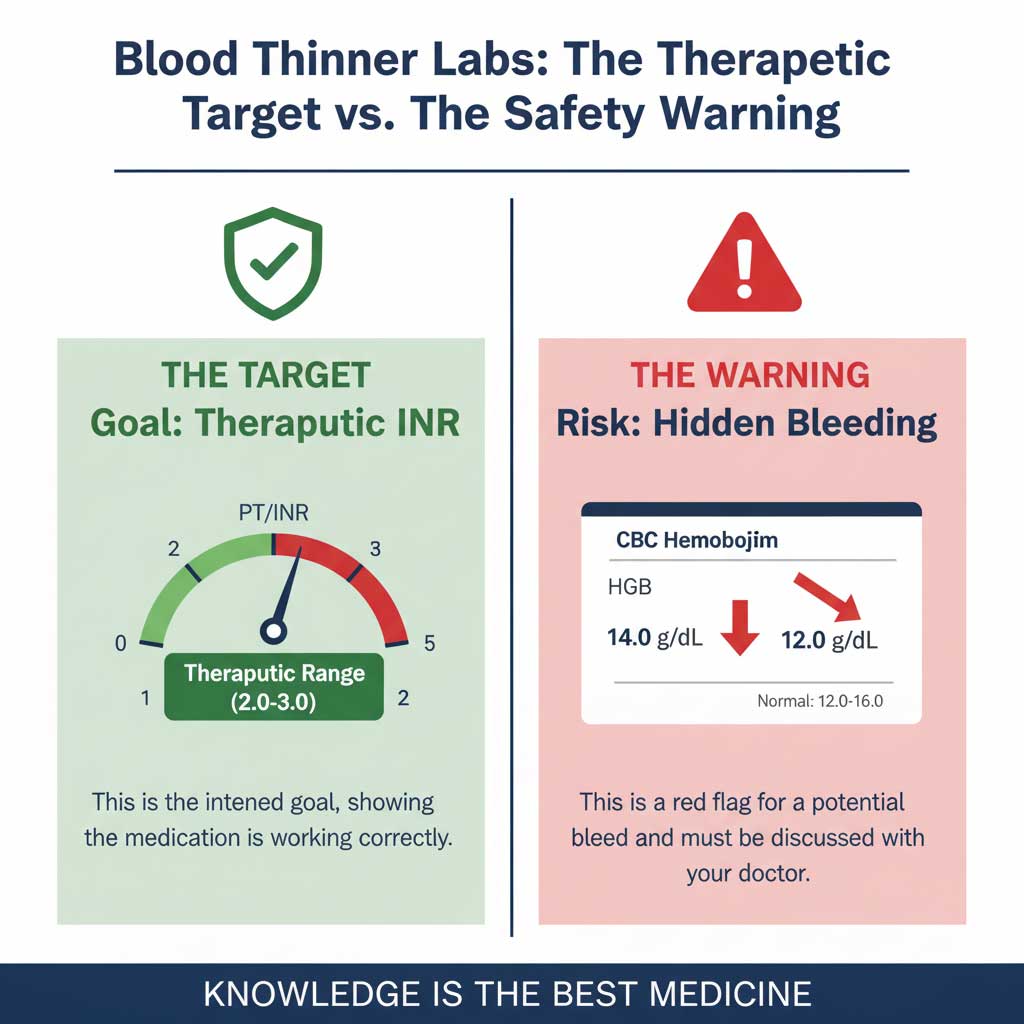
The Goal, Not a Side Effect
The entire purpose of taking warfarin is to intentionally raise your Prothrombin Time/International Normalized Ratio (PT/INR). This test measures how long it takes your blood to clot. If your target therapeutic INR range is 2.0 to 3.0 (typical for atrial fibrillation) and your result is 2.5, that is a perfect success, not a problem.
The Clinical Explanation
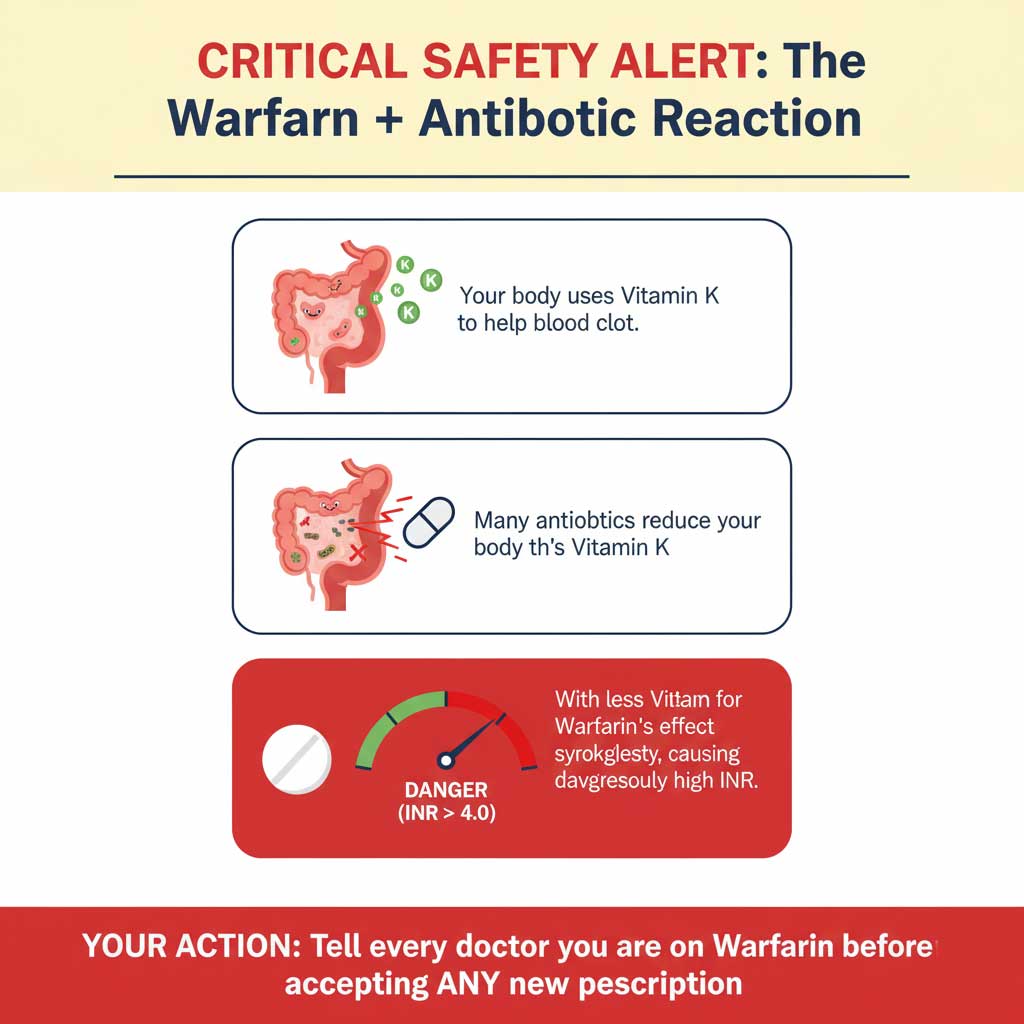
Warfarin works by inhibiting your body’s ability to use Vitamin K to produce key clotting factors. The PT/INR test is a direct, sensitive measure of how well those specific factors are working.
The Interaction Danger Zone
The reason Warfarin INR monitoring is so frequent is because its effect is notoriously easy to disrupt. As we will see, an antibiotic can send your INR soaring. A sudden change in your diet (like starting to eat a lot of spinach and other leafy greens rich in Vitamin K) can make it plummet, increasing your clotting risk. This is why you are the most important member of your monitoring team.
The New Guard: Eliquis, Xarelto (DOACs) and the Hidden Risks
Newer drugs called Direct Oral Anticoagulantes (DOACs) are now more common.
The “No-Monitoring” Myth
These drugs are often marketed as not needing routine monitoring like warfarin, but this is dangerously misinterpreted by many patients. They do not require routine efficacy testing (like the INR), but they absolutely require routine safety testing.
The Critical Safety Test: Your CBC
The number one thing your doctor watches for when you’re on a DOAC is a slow, steady drop in your hemoglobin and hematocrit on a Complete Blood Count. A healthy hemoglobin of 14.0 g/dL that drops to 12.0 g/dL over the course of a year is a massive red flag. It’s a potential sign of a slow, chronic internal bleed (often in the GI tract) that you might not otherwise notice until it becomes severe. The link between Eliquis and low hemoglobin is a critical safety checkpoint.
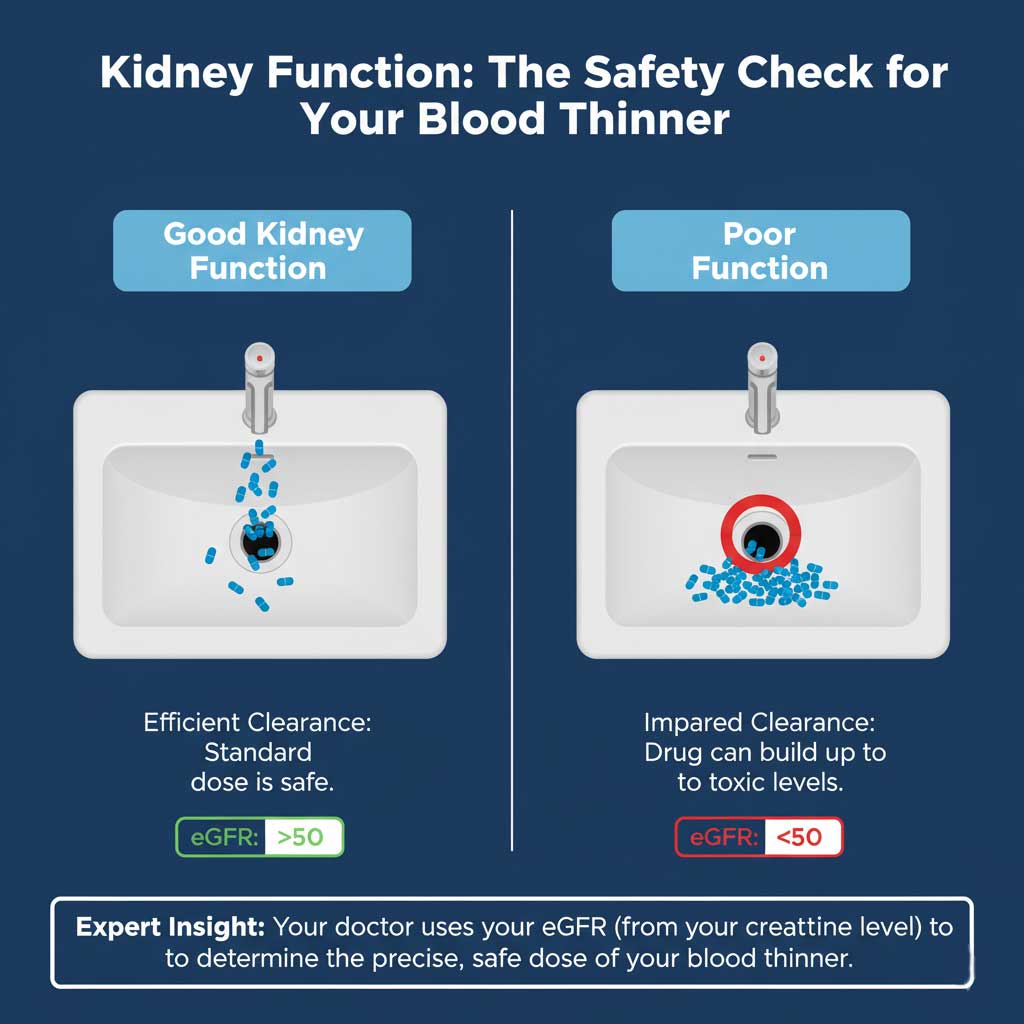
The Kidney Check: Your Creatinine and eGFR
Your kidneys act as the drain for these powerful drugs. Before you are ever prescribed one, your doctor MUST check your creatinine level on a Comprehensive Metabolic Panel (CMP) to calculate your kidney function (eGFR). The wrong dose in a patient with poor kidney function is a recipe for the drug building up to toxic levels, causing a major bleed.
The “Other” Blood Thinners: Plavix (Clopidogrel) and the INR Confusion
This is a point of frequent and dangerous confusion.
The Scenario
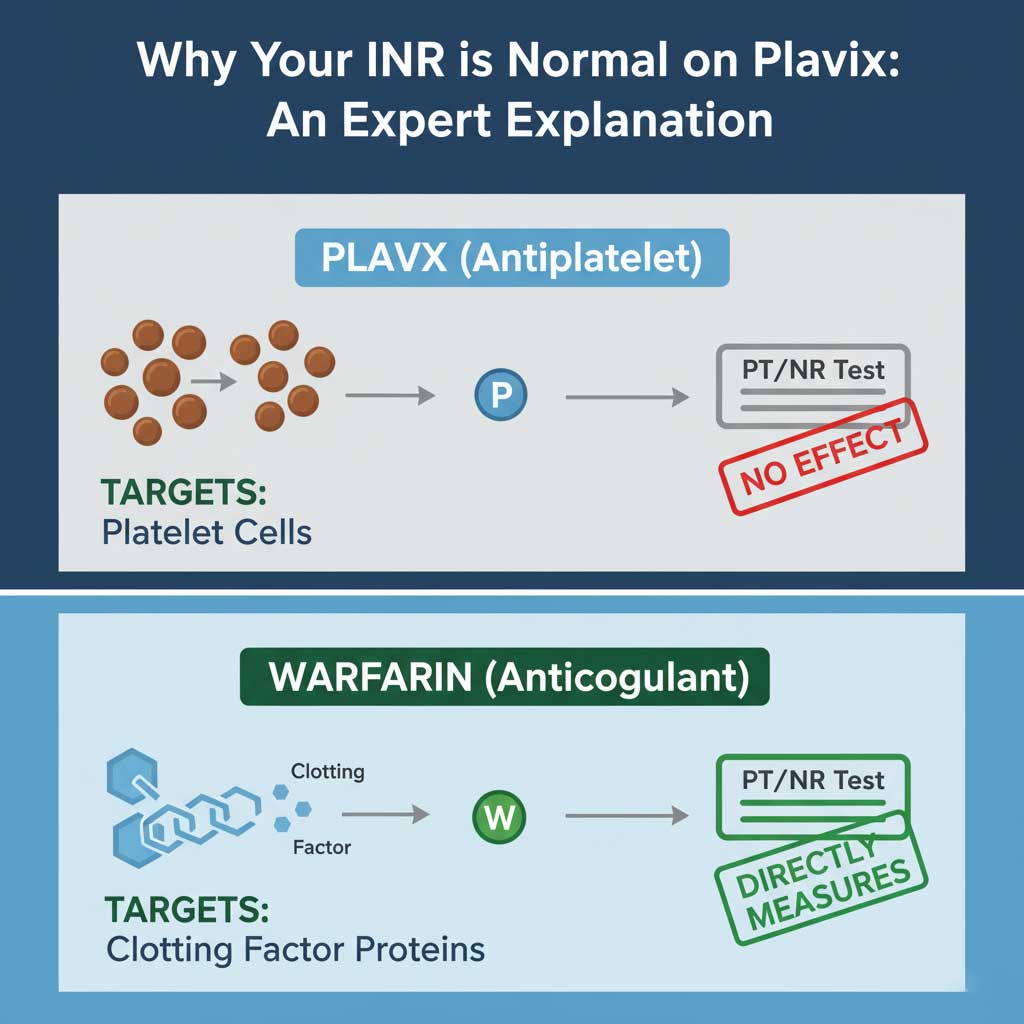
A patient asks, “I’m on Plavix after my heart stent, but my INR is normal. Is my blood thinner working?”
The Clinical Explanation
This is a brilliant question that shows an engaged patient. Plavix is an antiplatelet, not an anticoagulant. It works on the “sticky” little cells called platelets, preventing them from starting a clot. The INR test doesn’t measure platelets at all; it measures the protein clotting factors. Therefore, your INR should be normal while on Plavix. Its effect is measured with a different, specialized test that isn’t part of routine labs.
Antibiotics — The Expected Changes and the Dangerous Surprises
When you’re sick, an antibiotic can feel like a miracle. On your lab report, it can be a source of good news, but also a sign to be cautious.
The Good News: Watching Your WBC Count Fall
As covered earlier, the most welcome change is seeing your elevated White Blood Cell count on a CBC start to come down after a few days on an antibiotic. It’s the clearest sign that the medication is working and you are on the road to recovery.
The Dangerous Surprise: The Warfarin Interaction
This is so critical it bears repeating. The interaction between certain antibiotics (especially Bactrim) and warfarin (Coumadin) is one of the most dangerous and common in outpatient medicine. If you are on warfarin, you must treat any new antibiotic prescription as a major event and ensure your doctor has a plan for more frequent INR monitoring.
The Annoying Surprise: False-Positive Drug Tests
As mentioned, some antibiotics can cause a false-positive urine drug screen. This can be incredibly stressful. The key is open communication. Inform the testing facility of every medication you are taking beforehand. This provides immediate context for any unexpected results.
The “Watchful Waiting”: Liver and Kidney Stress
Potent antibiotics can sometimes cause a temporary spike in liver enzymes (ALT/AST) on a CMP or, in a hospital setting with IV medications, a rise in creatinine. This is usually mild and reversible, but it’s why doctors often monitor your labs during a long or intensive course of treatment.
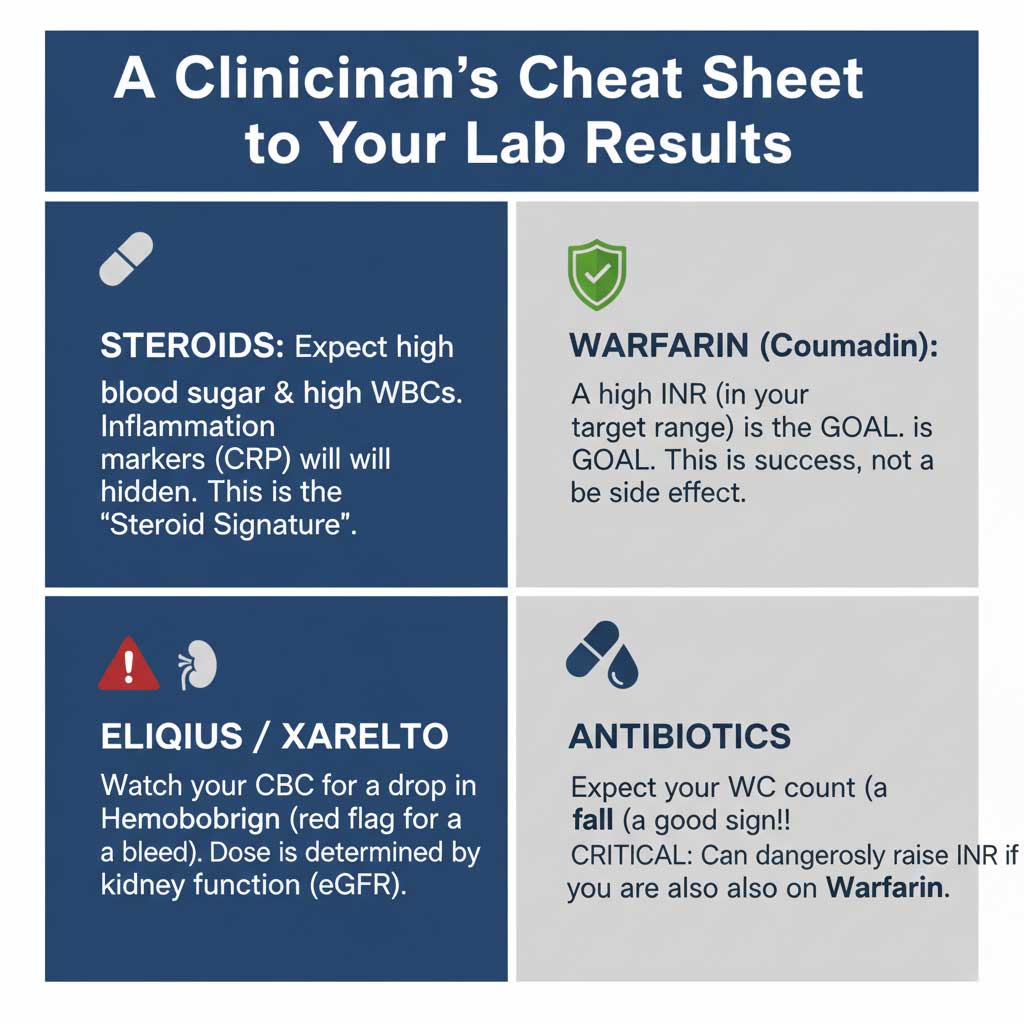
The Ultimate Cheat Sheet: Your Medication & Lab Test Summary Table
| Medication Class | Common Examples | Key Lab Tests | The Story the Lab Tells | Your Role / Key Discussion Point with Your Doctor |
| Corticosteroids | Prednisone, Medrol Dosepak | Blood Glucose (CMP), WBC Count (CBC), CRP | Very High Glucose: A direct, temporary metabolic effect. Very High WBC: A harmless “steroid signature,” not an infection. Very Low CRP: Shows the drug is working but hiding inflammation. | “Given this steroid, should I monitor my blood sugar at home?” “I see my WBC count is high; I assume this is from the prednisone?” |
| Anticoagulants (Warfarin) | Coumadin | PT/INR | The entire goal is to raise the INR into a specific therapeutic range (e.g., 2.0-3.0). | “What is my personal target INR range?” “I was just prescribed an antibiotic; should I get my INR checked sooner?” |
| Anticoagulants (DOACs) | Eliquis, Xarelto, Pradaxa | CBC, Creatinine (CMP) | A slow, steady drop in Hemoglobin on the CBC is a major red flag for a hidden bleed. Creatinine levels determine if your dose is safe. | “Could we review my CBC trend to make sure there are no signs of slow bleeding?” “Is my current kidney function still appropriate for this dose?” |
| Antiplatelets | Plavix, Aspirin | PT/INR, CBC | The INR will be NORMAL, as this test doesn’t measure platelet function. A drop in Hemoglobin on the CBC is a sign of bleeding. | “Just to confirm, this drug isn’t monitored with an INR, correct?” (This shows your expertise to your doctor). |
| Antibiotics | Bactrim, Levaquin, Augmentin | CBC, CMP, PT/INR | A falling WBC count is good news. A suddenly high INR while on warfarin is a medical emergency. High liver enzymes can signal liver stress. | “I’m on warfarin; is this antibiotic safe to take with it?” “I see my WBCs are coming down, so the antibiotic is working, right?” |
Conclusion: From Anxious Patient to Empowered Health Partner
We started with Sarah’s story of anxiety in front of a confusing lab report. Now, you have the knowledge to see that same report not as a source of fear, but as a rich source of data. You can see the “steroid signature” in a WBC count, understand the success of a therapeutic INR, and know to watch your hemoglobin trend while on a blood thinner.
This expertise transforms your role. You are no longer just a patient; you are the leading expert on your own body and a vital partner to your medical team. Your ability to ask sharp questions—”Is this high WBC from my prednisone?” or “Is this antibiotic safe with my warfarin?”—is the foundation of modern, high-quality healthcare.
Your labs tell a story. By understanding the language, you get to help write the ending. Take this knowledge, use it to have smarter conversations, and take confident ownership of your health journey.