

Yes, diarrhea can absolutely cause piles in adults. Frequent liquid bowel movements create intense pressure inside the anal canal, triggering inflammation. The high acidity of loose stool irritates the perianal skin, while the constant urge to evacuate forces the rectal veins to swell, leading to painful hemorrhoids.
Table of Contents
Every week, patients walk into my clinic confused about their sudden anal pain. Most people believe hemorrhoids only come from constipation and hard stools. They are genuinely surprised to learn that frequent, loose bowel movements are just as damaging to the anal canal. In clinical gastroenterology, the link between diarrhea and piles is well established.
From what we see in practice, treating the swelling without fixing the loose stools is a losing battle. The sheer speed and frequency of watery bowel movements traumatize the soft tissues of the lower rectum. Over time, this repeated injury turns healthy anatomical cushions into painful, bleeding masses.
In this clinical guide, you will learn the exact mechanics behind this painful condition, how digestive acids affect your lower gut, and which gastrointestinal triggers to watch for. We will also cover proven prevention strategies backed by leading medical boards so you can find lasting relief.
Key Clinical Statistics
- Prevalence: According to the National Institute of Diabetes and Digestive and Kidney Diseases, nearly 75% of adults will experience hemorrhoidal issues at some point in their lives.
- Risk Factor: Adults with chronic loose stools are up to 3 times more likely to develop severe anal inflammation than those with normal bowel habits.
- Anatomical Fact: Every human is born with vascular cushions inside the anal canal. They only become a problem when inflamed by excess pressure.
- IBS Connection: Around 40% of patients diagnosed with Irritable Bowel Syndrome with Diarrhea (IBS-D) report ongoing anorectal pain.
- Healing Time: Acute flare-ups usually take 7 to 10 days to resolve once the underlying digestive issue is managed.
- Hygiene Impact: Clinical studies show a 50% drop in perianal skin irritation when patients switch from dry toilet paper to water-based bidets.
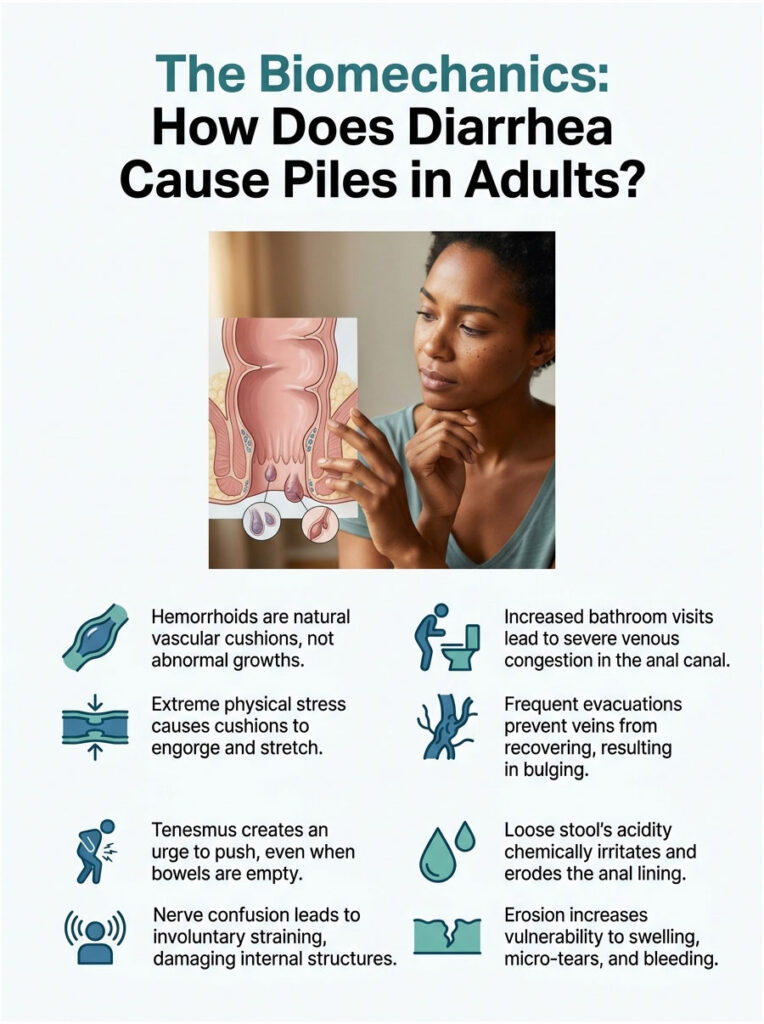
The Biomechanics: How Does Diarrhea Cause Piles in Adults?
To understand why loose stools cause so much damage, we need to look at the anatomy of the lower digestive tract. The process involves a mix of mechanical pressure, nerve confusion, and chemical burns. Here is exactly how it unfolds inside the body.
Hemorrhoids Are Vascular Cushions, Not Growths
A common misconception is that hemorrhoids are abnormal fleshy growths or tumors. That is simply not true. They are natural clusters of veins, smooth muscle, and connective tissue known clinically as the corpus cavernosum recti. Every person has these vascular cushions inside the anal canal.
These cushions play an important role. They act as shock absorbers and watertight seals, helping maintain fecal continence so gas and liquid do not leak out. But under extreme physical stress, they engorge with blood and stretch out of shape.
When someone has repeated bouts of loose stool, these cushions work overtime. The constant rush of fluid prevents the veins from shrinking back to their normal size. This lasting venous congestion is the very first step toward painful piles.
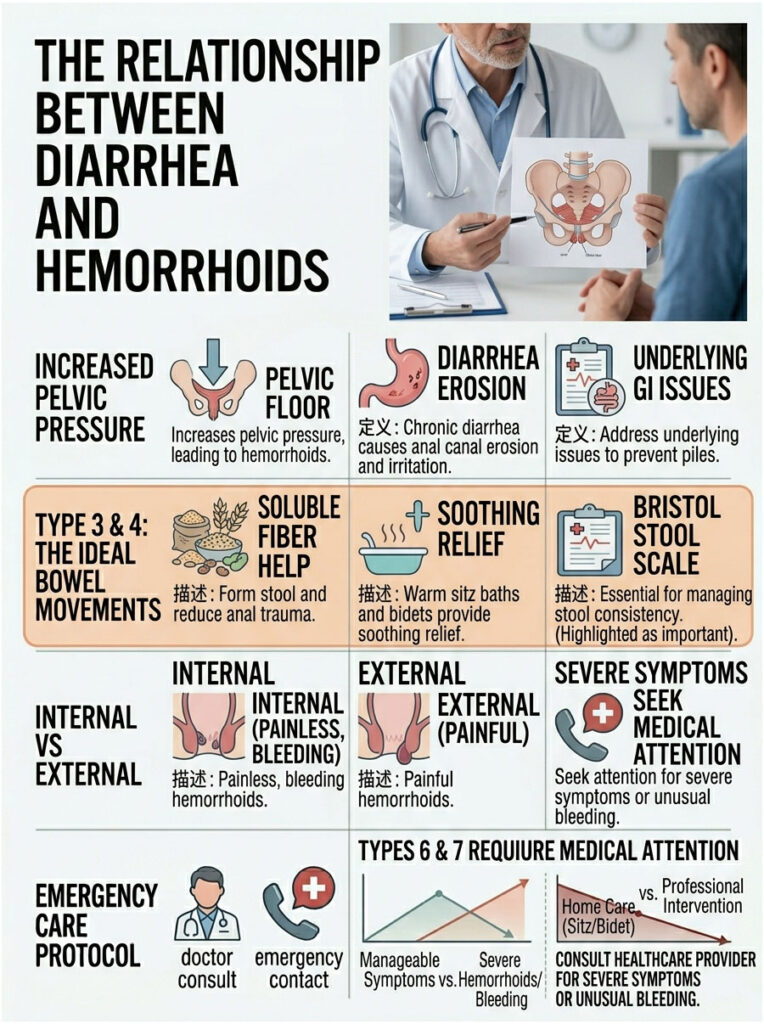
Increased Pressure Inside the Anal Canal
The frequency of bathroom visits during a gastrointestinal flare is a huge physical burden. A healthy adult normally has one or two formed bowel movements a day. During illness, that number can easily climb to ten or more, forcing the anal sphincter to work far beyond its normal limits.
This frequent evacuation causes severe venous congestion. When you sit on the toilet, gravity pulls blood down into the rectal area. Since bathroom visits come so often, the rectal veins stay full and never get time to recover. They stretch, weaken, and eventually bulge outward into the anal canal.
The rush to reach the bathroom also increases intra-abdominal pressure. This downward force traps blood in the lower pelvis. Within a few days, this continuous pressure turns normal internal veins into swollen, painful masses.
The Role of Tenesmus and Nerve Confusion
Here is something many patients do not realize: even when your bowels are empty, you may still feel a desperate urge to push. This exhausting sensation is called tenesmus, and it is a hallmark of lower gastrointestinal distress. It is also a major cause of tissue damage.
Tenesmus happens because severe inflammation from liquid stool tricks the rectal nerves. The pudendal nerve sends false signals to the brain, telling it that solid stool is still present. As a result, you push and strain involuntarily, bearing down on an empty rectum.
This dry straining is extremely harmful. It pushes internal structures toward the anal opening, and over time, the internal vascular cushions can prolapse and fall outside the body.
Chemical Irritation and Mucosal Erosion
Physical pressure is only half of the problem. The chemical makeup of loose stool adds another layer of damage. Liquid stool is highly acidic because it carries raw digestive enzymes and unabsorbed bile salts.
Under normal conditions, food moves slowly through the intestines. This gives the body time to neutralize stomach acids and reabsorb bile salts. When digestion speeds up, this vital neutralization process never happens.
The bile salts reach the rectum in their raw, acidic form and literally erode the delicate anal lining. This chemical stripping leaves the underlying veins highly vulnerable to swelling, micro-tears, and heavy bleeding.
Diagnosing the Root Cause of Chronic Loose Stools
In clinical practice, treating anal swelling without addressing the underlying digestive problem is a flawed approach. If the loose stools do not stop, the painful swelling will keep coming back. You must identify what is causing your gastrointestinal distress in the first place.
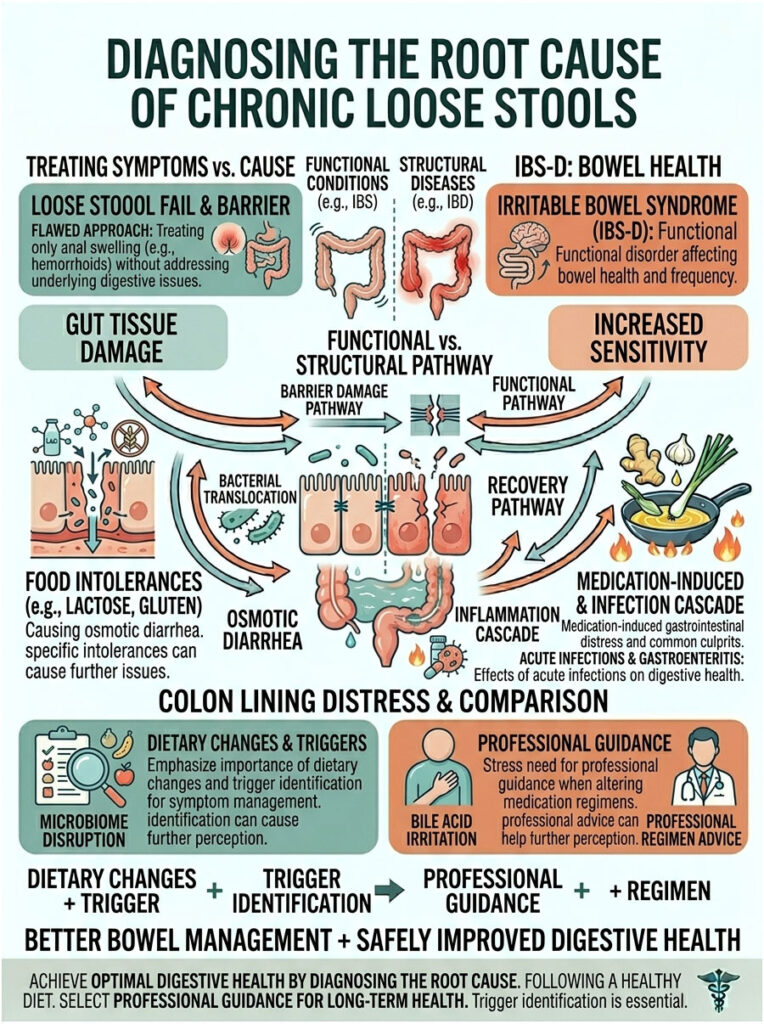
Irritable Bowel Syndrome (IBS-D)
Irritable Bowel Syndrome with diarrhea (IBS-D) is one of the most common culprits we see. This functional disorder causes the colon to spasm and contract too quickly, leading to urgent, frequent bowel movements that traumatize the anal canal almost daily.
Patients with IBS-D get stuck in a brutal cycle of gut distress and anal pain. The unpredictable nature of their bowel movements keeps the rectal veins constantly inflamed. Managing the gut-brain connection is essential for lasting relief.
Doctors often recommend dietary changes like the Low FODMAP diet to help control IBS-D symptoms. Identifying specific carbohydrate triggers can dramatically slow gut motility, which means fewer bathroom visits and less pressure on the vascular cushions.
Inflammatory Bowel Disease (IBD)
It is important to tell the difference between functional conditions like IBS and structural diseases like Inflammatory Bowel Disease (IBD). IBD includes autoimmune conditions such as Crohn’s disease and ulcerative colitis. These diseases cause systemic inflammation that directly damages the digestive tract lining.
According to clinical data from gastroenterology associations, anorectal complications are very common in IBD patients. Chronic internal ulcers and constant liquid output create a toxic environment for the lower rectum. For these patients, the link between chronic loose stools and hemorrhoids is a constant struggle.
Treating IBD requires specialized immunosuppressive therapies and biologics. Over-the-counter creams will not fix piles caused by active Crohn’s disease. You have to achieve clinical remission of the underlying bowel disease before the anorectal tissues can truly heal.
Food Intolerances and Osmotic Diarrhea
Sometimes, the foods you eat directly trigger rapid bowel movements. Lactose intolerance or gluten sensitivity can cause what is called osmotic diarrhea. This happens when unabsorbed nutrients pull excess water into the colon.
The sudden flood of water produces high-velocity stools that shock the anal sphincter. This rapid expansion and violent evacuation stretch the vascular cushions to their breaking point. Identifying and removing trigger foods is a vital prevention step.
Celiac disease works in a similar way. When a celiac patient eats gluten, their immune system attacks the small intestine, causing rapid purging. Strict elimination of gluten is the only way to stop this specific type of tissue damage.
Medication-Induced Gastrointestinal Distress
Many patients do not realize that their daily medications may be wrecking their gut health. Broad-spectrum antibiotics are well known for killing off healthy gut bacteria, and this imbalance often leads to watery stools.
Metformin, a common medication for type 2 diabetes, is another frequent offender. Up to 30% of patients on metformin experience chronic loose stools as a side effect. That steady, medication-induced purging places heavy daily stress on the anal canal.
If you suspect your medication is causing your bowel issues, never stop taking it suddenly. Talk to your prescribing doctor. They can often adjust the dose or switch you to an extended-release version that is gentler on the digestive tract.
Acute Infections and Gastroenteritis
Viral and bacterial infections, commonly called food poisoning, cause short but intense bouts of digestive distress. Viruses like norovirus or bacteria like salmonella force the body to rapidly purge the gut.
These infections are temporary, but the damage they cause to the anal canal can last for weeks. A single weekend of bad food poisoning can trigger an acute thrombosed external hemorrhoid. It shows clearly how rapid fluid loss destroys anorectal health.
During an active infection, focus on hydration and skin protection. You cannot stop the infection from running its course, but you can shield your skin. Applying a thick barrier cream before every bathroom visit can save you from painful chemical burns.
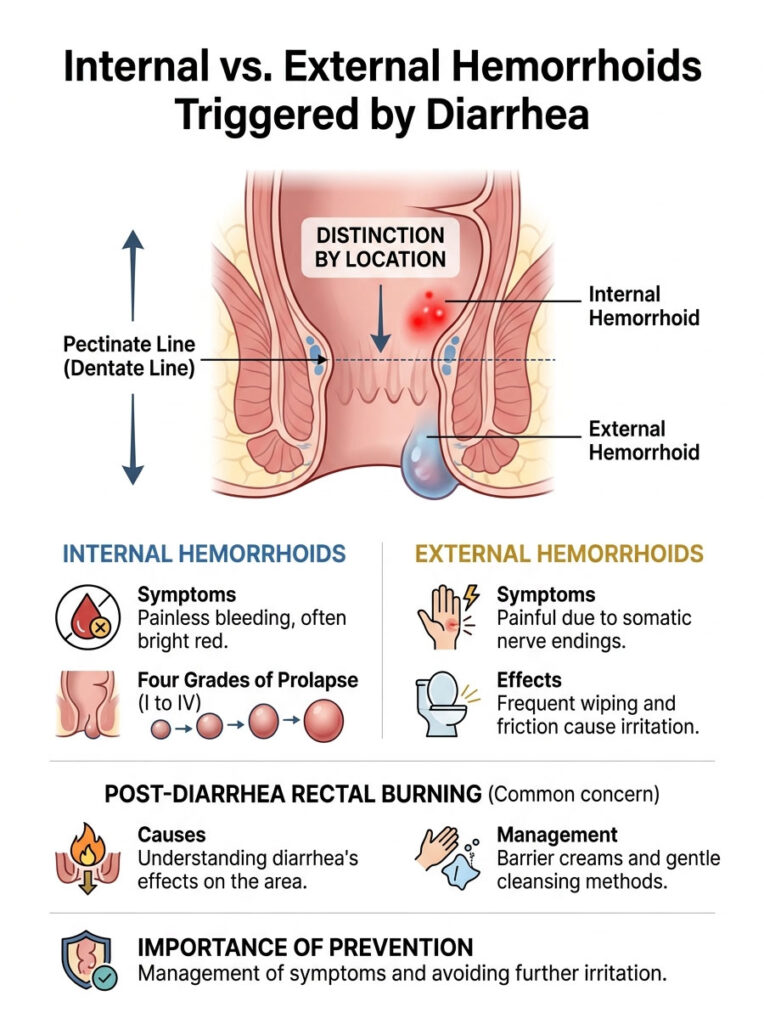
Internal vs. External Hemorrhoids Triggered by Diarrhea
The location of the swollen vein determines the type of symptoms you will feel. The anal canal is divided by an anatomical landmark called the pectinate line, or dentate line. This invisible boundary separates the upper and lower halves of the anal canal.
Internal Hemorrhoids and the Pectinate Line
Veins that swell above the pectinate line are called internal hemorrhoids. The tissue in this upper region has only visceral nerve endings, which do not sense sharp pain. That is why internal swellings are usually painless, even when severely inflamed.
However, internal hemorrhoids bleed easily. When acidic liquid stool rushes past these swollen veins, it tears their fragile surface. Patients often notice bright red blood dripping into the toilet bowl or streaking the toilet paper.
This painless bleeding is the classic sign of internal hemorrhoidal disease. While it can look alarming, bright red blood usually points to a localized lower issue. Dark, tarry blood, on the other hand, is a much more serious warning sign that needs immediate medical attention.
The Four Grades of Internal Prolapse
Over time, the constant downward pressure from loose stools can cause internal veins to prolapse. Gastroenterologists grade the severity from Grade I to Grade IV. Knowing your grade helps guide treatment.
Grade I piles bleed but stay inside the anal canal. Grade II piles prolapse during a bowel movement but retract on their own afterward. These early stages usually respond well to dietary changes and fiber therapy.
Grade III piles prolapse during evacuation and need to be manually pushed back inside. Grade IV piles stay permanently outside and cannot be pushed back in. Chronic loose stools speed up the progression through these stages, often leading to surgery.
External Hemorrhoids and Sphincter Irritation
Veins that swell below the pectinate line are called external hemorrhoids. Unlike the upper canal, this lower area is covered in somatic nerve endings, the same sensitive nerves found on your fingertips and lips.
Because of these nerves, external swellings are excruciatingly painful. Frequent bowel movements mean constant wiping, and dry toilet paper strips away the skin’s natural oils, causing friction burns.
This friction makes external tissues even worse. It often leads to thrombosis, where a solid blood clot forms inside the swollen vein. A thrombosed external pile shows up as a hard, intensely painful blue lump at the edge of the anus.
Understanding Post-Diarrhea Rectal Burning
Patients often describe severe rectal burning after an episode of diarrhea. This symptom happens when acidic stool chemically burns the external somatic nerves. The burning can last for hours after you leave the bathroom.
This type of chemical burn is hard to soothe with standard pain medications. The raw nerve endings are reacting to digestive enzymes left behind on the skin. You need to physically remove those enzymes to stop the burning.
Managing this burning takes specialized barrier creams and water-based cleansing. Protect the skin from more chemical damage before the next bowel movement. Prevention is always more effective than trying to calm an active chemical burn.
Clinical Comparison: Constipation vs. Diarrhea as Triggers
To fully understand anorectal disease, it helps to compare the two extremes of bowel dysfunction. Both ends of the spectrum cause major tissue damage, but in very different ways.
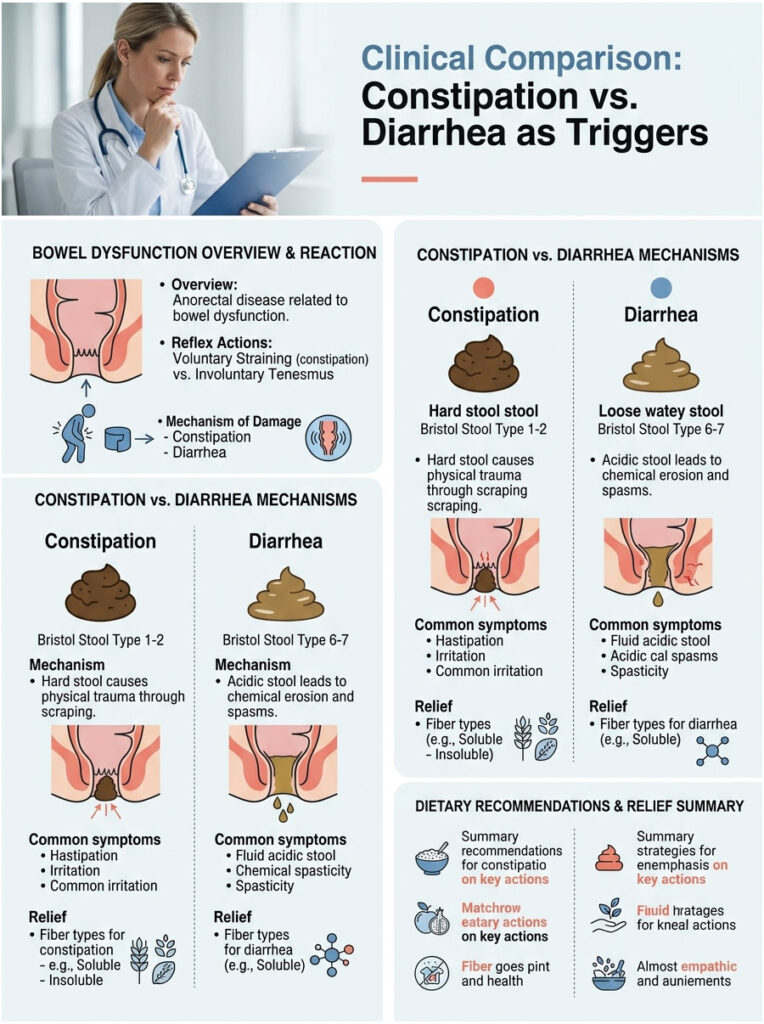
Constipation damages the area through blunt mechanical force. Hard, dry stool acts like sandpaper on the delicate anal lining. The patient voluntarily strains and holds their breath to force the blockage out, which spikes pelvic pressure.
Loose stools, on the other hand, cause damage through chemical erosion and involuntary spasms. The stool is acidic, stripping the mucosal lining away. The patient experiences involuntary tenesmus, meaning the body forces them to strain even when they do not want to.
| Clinical Factor | Constipation-Induced Trauma | Diarrhea-Induced Trauma |
|---|---|---|
| Primary Mechanism | Hard stool injures veins through physical scraping and forceful pushing. | Frequent acidic liquid stool causes mucosal erosion and repeated pressure. |
| Stool Consistency | Bristol Stool Scale Types 1 and 2 (hard lumps). | Bristol Stool Scale Types 6 and 7 (mushy or fully liquid). |
| Associated Reflex | Voluntary straining to push out physical blockages. | Involuntary straining (tenesmus) from rectal nerve irritation. |
| Common Symptoms | Deep aching pain, tissue prolapse, tearing sensations. | Severe chemical burning, intense itching, frequent bright red bleeding. |
| First-Line Dietary Fix | Insoluble fiber, soluble fiber, and much more water. | Soluble fiber only (like psyllium) to absorb excess water in the gut. |
Clinical Benchmarks: Using the Bristol Stool Scale
Gastroenterologists do not just guess about stool consistency during evaluations. We use a standardized chart called the Bristol Stool Scale. This diagnostic tool sorts stool into seven types based on shape and texture.
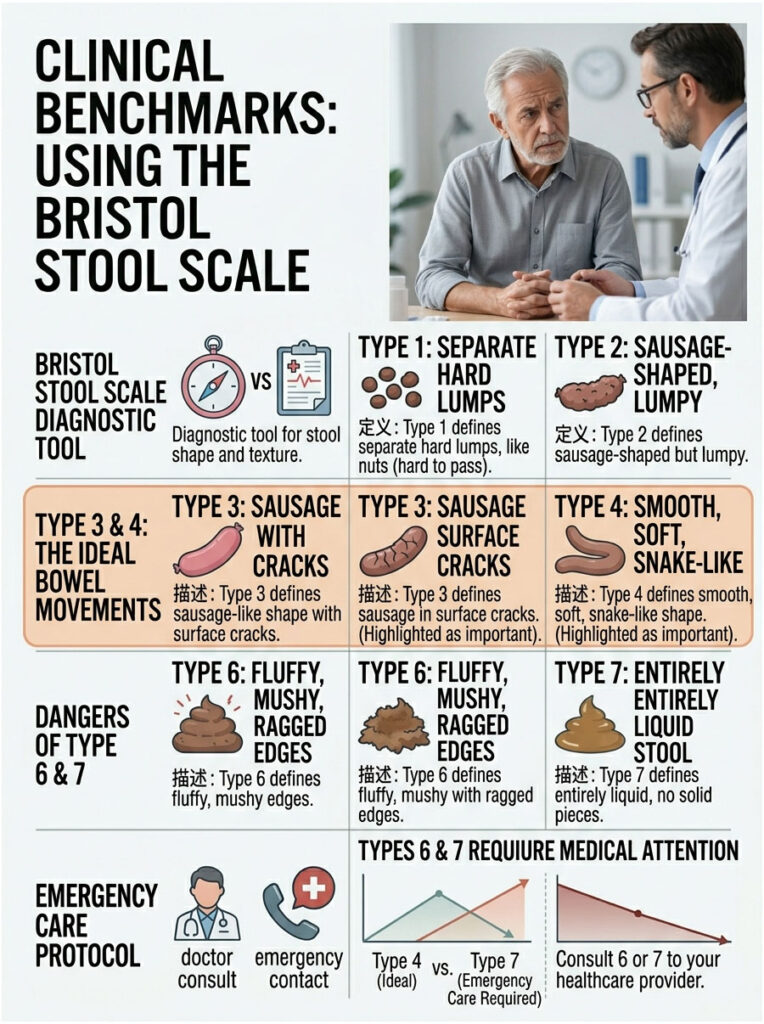
Understanding the Bristol Stool Scale is essential for managing anorectal health. It helps patients communicate clearly with their doctors and gives a clear visual target for dietary and medical treatment.
The goal of any treatment plan is to pull your bowel habits away from the dangerous extremes. Monitoring your daily output on the scale helps you fine-tune your fiber intake. You want to consistently produce a healthy Type 4 stool.
The Healthy Middle: Types 3 and 4
Types 3 and 4 represent the ideal bowel movement. Type 3 looks like a sausage with some cracks on the surface. Type 4 is smooth, soft, and shaped like a snake or hotdog.
These healthy types pass through the anal canal easily without much straining. They are bulky enough to trigger the rectum’s stretch receptors, signaling a complete evacuation. Producing Type 4 stools is the best defense against anorectal disease.
When your output is consistently Type 4, your vascular cushions are not under stress. The veins can rest, heal, and stay in their proper position. Keeping this consistency requires a balance of soluble and insoluble fiber.
The Danger Zones: Types 6 and 7
For our discussion, Types 6 and 7 are the danger zones. Type 6 is fluffy and mushy with ragged edges. Type 7 is entirely liquid with no solid pieces.
When your output stays in Type 6 or 7 territory, your anal canal is taking active damage. Liquid stool moves too fast to bulk up, rushing past the sphincters and causing violent expansion and chemical burns.
You cannot heal swollen rectal veins while producing Type 7 stools. The acidic environment and constant wiping will outpace any healing cream you apply. You have to change the stool consistency first, either through diet or medical help.
Immediate Symptom Management and Clinical Relief
When you are in the middle of a painful flare-up, you need fast relief. The pain, itching, and swelling can be debilitating. Thankfully, there are effective, evidence-based strategies to soothe inflamed tissues during an active episode.
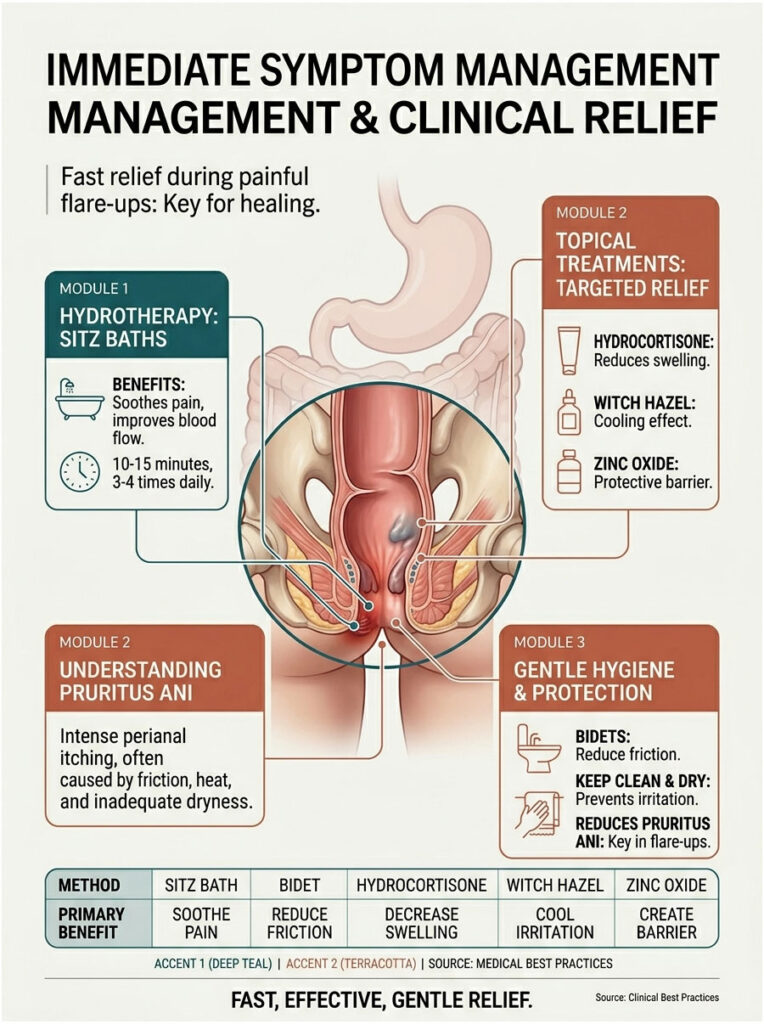
Hydrotherapy: Sitz Baths and Bidets
Major medical institutions strongly recommend daily sitz baths. A sitz bath means soaking the pelvic area in warm, shallow water for 10 to 15 minutes. The warmth relaxes the internal anal sphincter, which is often spasming from tenesmus.
This muscle relaxation lowers the resting pressure in the anal canal. Lower pressure allows trapped venous blood to return to circulation, shrinking the swollen tissue. Aim for three to four warm sitz baths a day during an acute flare-up.
A bidet is also a great daily hygiene tool. Toilet paper is abrasive and damages fragile skin. A bidet uses a gentle stream of water to clean the area without friction, washing away acidic digestive enzymes safely.
Topical Treatments and Barrier Creams
Over-the-counter creams play a supportive role in symptom relief. Hydrocortisone creams can temporarily reduce swelling and calm the localized immune response. Use steroid creams sparingly, for no more than seven days, to avoid thinning the delicate perianal skin.
Witch hazel pads are great for cooling the area naturally. Witch hazel is a gentle astringent that helps shrink swollen tissue. It provides a cooling sensation that works well against post-diarrhea rectal burning. Always pat the area gently, never rub.
Zinc oxide barrier creams are essential for anyone dealing with loose stools. Zinc oxide creates a thick, waterproof barrier over the external skin. This barrier physically blocks acidic bile salts from touching the raw skin, preventing further chemical burns.
Managing Pruritus Ani (Intense Anal Itching)
Why does the area itch so intensely after a bout of diarrhea? This condition is called pruritus ani. It happens because residual liquid stool contains active, highly acidic digestive enzymes.
Left on the skin, these enzymes begin to digest the outer layer. The itching is intense, but scratching causes micro-tears and invites bacterial infection. Resist the urge to scratch at all costs.
To manage pruritus ani, keep the area spotlessly clean and completely dry. After washing with water, pat dry with a soft towel or use a hairdryer on the cool setting. Never leave the skin damp, as trapped moisture fuels fungal growth and more itching.
| Treatment Method | Primary Clinical Benefit | Expert Usage Protocol |
|---|---|---|
| Warm Sitz Bath | Relaxes sphincter spasms and cleans acidic residue safely. | Soak in warm water for 10 to 15 minutes, 3 to 4 times daily. |
| Bidet Attachment | Removes friction from wiping and prevents micro-tears. | Use after every bowel movement instead of dry toilet paper. |
| Witch Hazel Pads | Acts as an astringent to shrink tissue and cool burning nerves. | Gently pat the affected area after washing. Do not rub. |
| Zinc Oxide Paste | Creates a physical, waterproof barrier against acidic bile salts. | Apply a thick layer around the external sphincter before bathroom visits. |
| Oral Ibuprofen | Reduces systemic inflammation and dulls somatic nerve pain. | Take with food to prevent stomach upset. Avoid opioid painkillers. |
Long-Term Prevention and Dietary Interventions
Symptom management is only a temporary fix. For lasting healing, you have to change the physical consistency of your stool. That means specific, targeted dietary steps to stabilize an erratic digestive tract.
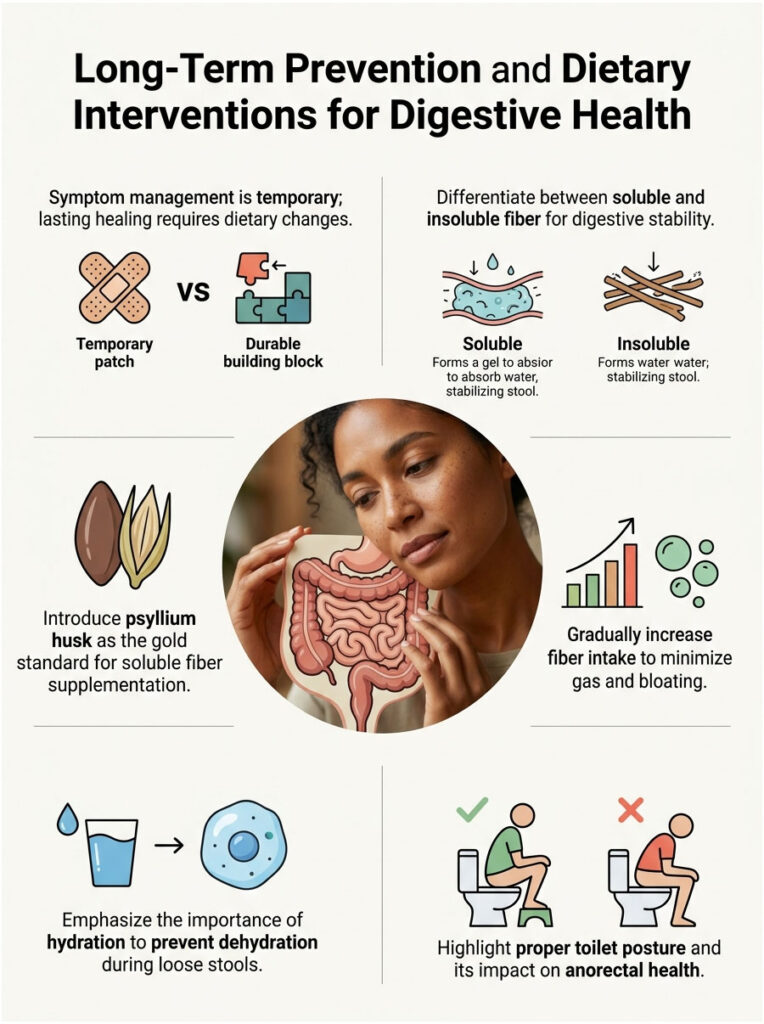
The Paradox of Soluble Fiber
There is a lot of confusion about fiber. Many patients avoid fiber altogether when they have loose stools, thinking it will make things worse. This is a critical misunderstanding of how different types of fiber actually work.
Insoluble fiber (found in wheat bran and raw leafy vegetables) acts like a broom, sweeping food quickly through the gut. Avoid insoluble fiber during an active flare-up. Instead, increase your daily soluble fiber intake.
Soluble fiber works like an absorbent sponge in the digestive tract. When it reaches the colon, it soaks up excess water and forms a thick, soothing gel. This gel binds loose liquid, turning watery stool into a formed, manageable mass.
Building a Daily Fiber Routine
Adding a daily soluble fiber supplement is the single most effective way to break the cycle of anorectal trauma. Psyllium husk is the clinical gold standard. It holds a huge amount of water and works wonders at bulking up loose stools.
Start slowly to avoid gas and bloating. Begin with one teaspoon of psyllium husk in eight ounces of water daily. Gradually increase the dose over two weeks until your stool reaches a healthy Type 4 on the Bristol scale.
If psyllium causes too much gas, try methylcellulose or acacia fiber instead. These options ferment less in the gut, so they produce less gas while still bulking up stool effectively.
Hydration and Electrolyte Balance
It sounds backwards, but you have to drink plenty of water even when you have loose stools. Chronic gastrointestinal distress drains your body of fluids and electrolytes, creating a dangerous dehydration cycle.
Oddly, dehydration makes the rectal mucosa dry, brittle, and weak. Brittle tissue tears easily under pressure. Proper hydration keeps the mucosal lining supple, resilient, and able to stretch safely.
Stick to plain water and medical-grade oral rehydration solutions. Avoid caffeine and alcohol during a flare-up. Both are gastrointestinal stimulants that speed up gut motility and make tenesmus worse.
Pelvic Floor Awareness and Bathroom Ergonomics
Your posture on the toilet plays a big role in anorectal health. Modern western toilets force the body into a strict 90-degree sitting position. This unnatural angle actually pinches the rectum, forcing you to strain harder to evacuate.
Avoid hovering over the toilet or sitting for long periods. Sitting for more than five minutes lets gravity pool blood in the vascular cushions. Get in, do your business, and get out.
Consider using a toilet footstool to raise your knees. Elevating the knees changes the anorectal angle from 90 degrees to a natural 35 degrees. This squatting position straightens the rectum, letting gravity help evacuation without triggering damaging tenesmus.
Advanced Diagnostic Testing for Chronic Bowel Issues
When dietary changes and basic fiber routines fail, guessing is no longer acceptable. Chronic loose stools need advanced diagnostic testing to find the true root cause. Gastroenterologists rely on several specific tests to map out digestive health.
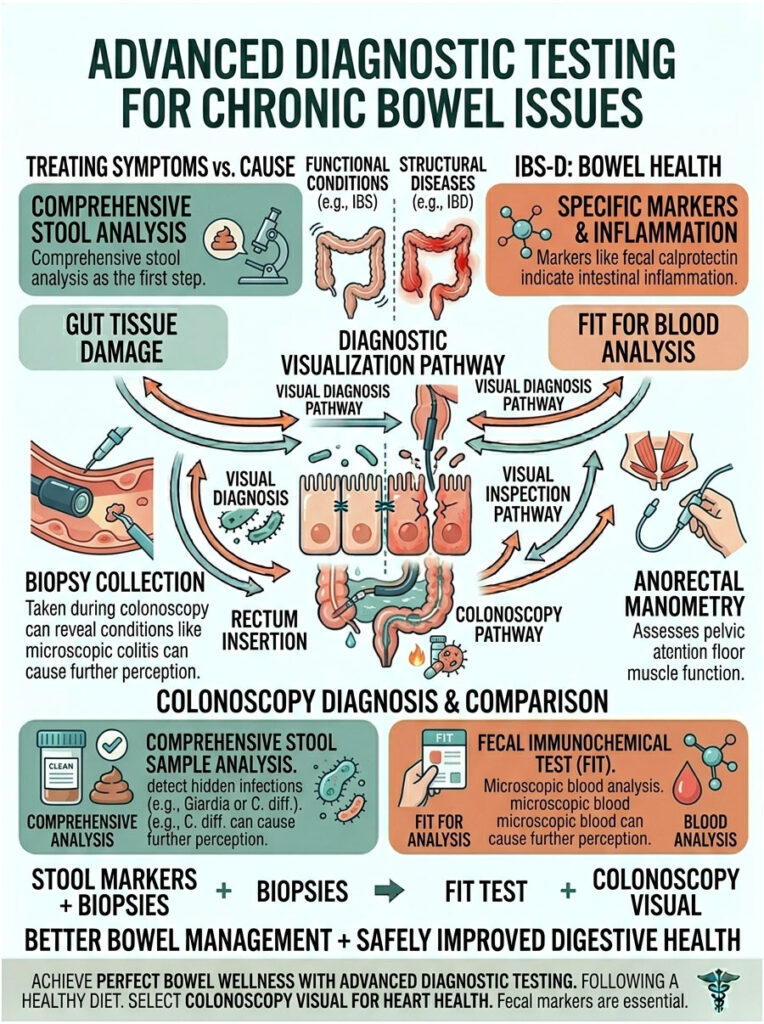
Comprehensive Stool Analysis
The first step in advanced diagnostics is usually a comprehensive stool test. Doctors look for specific inflammatory markers like fecal calprotectin. High levels strongly suggest active intestinal inflammation, pointing toward conditions like Crohn’s disease.
Stool tests also screen for hidden bacterial or parasitic infections. Pathogens like Giardia or C. diff can live in the gut for months, causing chronic, low-grade diarrhea. Finding and treating these pathogens is crucial for restoring normal bowel function.
We also use the Fecal Immunochemical Test (FIT) to check for microscopic blood. Bright red blood usually comes from piles, but hidden blood mixed into the stool calls for deeper investigation to rule out more serious causes.
Endoscopy and Colonoscopy
If non-invasive tests are inconclusive, a colonoscopy is the gold standard for visual diagnosis. A gastroenterologist uses a flexible camera to examine the entire colon, looking for ulcers, polyps, or active inflammatory bowel disease.
A colonoscopy also lets the doctor take tiny tissue samples. These biopsies can reveal microscopic colitis, a condition that causes chronic watery stools but looks completely normal to the naked eye.
Do not let fear keep you from getting a colonoscopy. The procedure is done under deep sedation, so you will not feel pain or remember the exam. It is a life-saving tool for anyone dealing with chronic bowel irregularities.
Anorectal Manometry Testing
Sometimes the problem lies in the nerves and muscles of the pelvic floor. Anorectal manometry is a specialized test that measures the strength and coordination of your anal sphincter muscles.
During the test, a small pressure-sensitive balloon is placed into the rectum. The doctor asks you to squeeze, relax, and push while a computer records the muscle contractions. This shows whether the pelvic floor is spasming or failing to relax.
If manometry reveals pelvic floor dysfunction, specialized physical therapy often helps. Pelvic floor therapists use biofeedback to retrain these muscles, which is highly effective at stopping involuntary tenesmus.
The Psychological Impact of Chronic Diarrhea and Piles
We cannot talk about chronic gastrointestinal issues without addressing the mental toll they take. Living with unpredictable bowels and constant anal pain wears patients down. The anxiety around bathroom access is a real, debilitating condition.
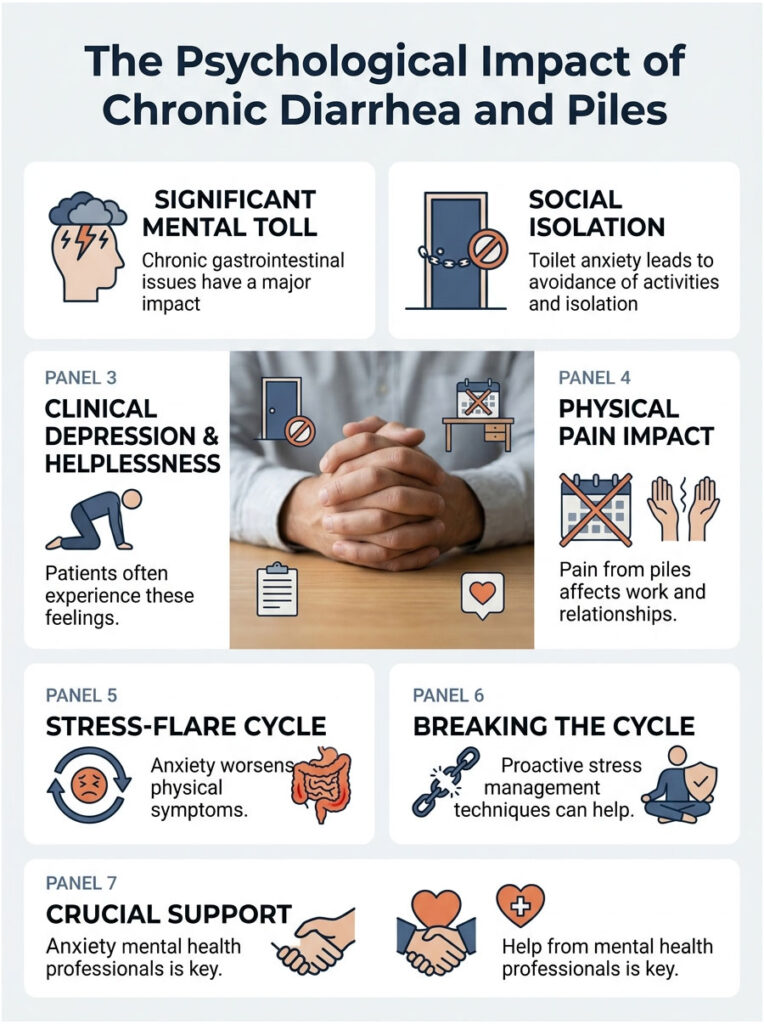
Toilet Anxiety and Social Isolation
Patients with chronic loose stools often develop severe toilet anxiety. They map out public restrooms before leaving the house. Many stop traveling, eating out, or attending social events out of fear of an accident or pain flare.
This isolation often leads to clinical depression and feelings of helplessness. Swollen veins make sitting at a desk or driving a car agonizing, affecting work, relationships, and overall quality of life.
Know that this burden is real and common. You are not alone. Support from a therapist who specializes in chronic illness can be just as valuable as seeing a gastroenterologist.
The Stress-Flare Cycle
Here is the kicker: anxiety directly worsens physical symptoms. The gut and brain are closely connected through the vagus nerve. When you feel stressed, your brain dumps cortisol and adrenaline into the bloodstream.
These stress hormones speed up the digestive tract. That triggers another bout of loose stools, which inflames the vascular cushions further. The pain creates more anxiety, feeding a never-ending stress-flare cycle.
Breaking this cycle takes proactive stress management. Deep diaphragmatic breathing, meditation, and cognitive behavioral therapy (CBT) all calm the vagus nerve. Calming the nervous system slows gut motility and reduces pelvic pressure.
When to Seek Medical Intervention and Surgical Options
Home treatments work for mild cases, but sometimes professional help is non-negotiable. Knowing when to call a proctologist can save you from serious complications.
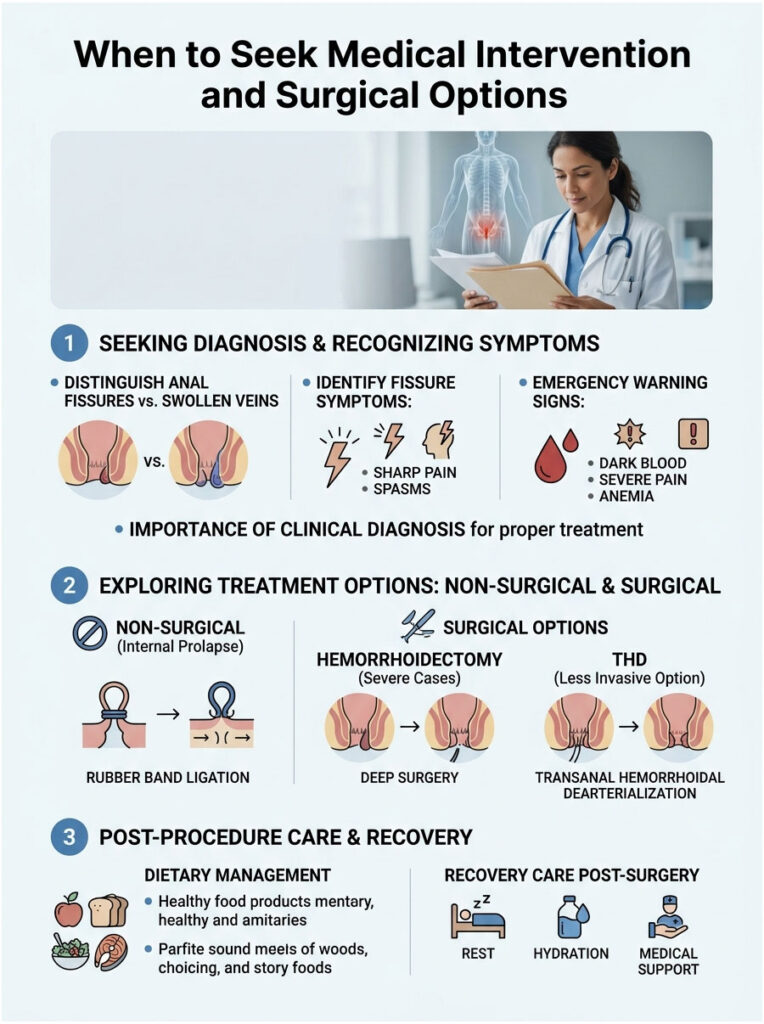
Telling Fissures Apart from Swollen Veins
Patients often confuse swollen veins with anal fissures. Both are triggered by gastrointestinal distress, but they need completely different treatments. A hemorrhoid is a swollen vascular cushion. A fissure is an actual tear in the skin.
Fissures cause sharp, glass-like pain during evacuation, followed by muscle spasms that last for hours. If your pain feels like passing shards of glass, you likely have a fissure caused by acidic stool. A doctor needs to diagnose this because fissures require prescription muscle relaxants to heal properly.
Applying standard pile cream to a fissure will not heal it. In fact, some over-the-counter creams can make it worse. A proper clinical diagnosis is the only way to know you are treating the right problem.
Warning Signs and Clinical Red Flags
Stop home treatment and seek emergency care if you notice clinical red flags. Bright red blood on toilet paper is common, but dark maroon or black, tarry blood points to serious bleeding higher up in the digestive tract. That is a medical emergency.
Also seek help for severe, unrelenting pain that stops you from sitting, walking, or sleeping. Signs of anemia like extreme fatigue, pale skin, or dizziness also need urgent evaluation. Never ignore these warning signs.
If your gastrointestinal distress lasts more than four weeks, get comprehensive testing. Chronic diarrhea is not normal, and it needs thorough investigation to rule out IBD, serious infections, or colorectal cancer.
Office Procedures: Rubber Band Ligation
If internal swellings do not respond to diet and soluble fiber, your doctor may suggest a non-surgical office procedure. Rubber band ligation is highly effective for Grade II and Grade III internal prolapse.
During the quick procedure, the doctor places a tight rubber band at the base of the swollen vein. The band cuts off the blood supply, and within a week, the shrunken tissue and band fall off painlessly during a normal bowel movement.
Ligation leaves a small scar at the base of the vein. That scar tissue anchors the remaining vascular cushions in their proper place. It is a very successful procedure with a low recurrence rate.
Advanced Surgical Options
For Grade IV prolapse or severely thrombosed external masses, a traditional hemorrhoidectomy may be needed. This surgery is done in a hospital under general anesthesia. The surgeon removes the diseased vascular cushions using a scalpel or laser.
A hemorrhoidectomy offers the most permanent cure, but recovery can be painful. Patients usually need two to three weeks off work to heal. Pain management and a strict high-fiber diet are crucial during recovery.
Another advanced option is Transanal Hemorrhoidal Dearterialization (THD). This less invasive surgery uses an ultrasound probe to find the arteries feeding the swollen veins. The surgeon then ties off those arteries, causing the tissue to shrink without cutting any sensitive external skin.
Expert Clinical Insight: Never assume a bleeding anal lump is just a simple swollen vein, especially if you have a history of chronic loose stools. Ongoing bleeding along with unexplained weight loss or severe abdominal cramps calls for an immediate colonoscopy to rule out serious disease.
Summary and Key Takeaways
So, does diarrhea cause piles in adults? Yes, without question. Liquid bowel movements are a destructive, erosive force on the delicate anal canal. The mix of increased pelvic pressure, involuntary tenesmus, and acidic erosion from bile salts creates the perfect storm for severe anorectal disease.
To break this painful cycle for good, you have to treat both the local symptoms and the systemic root cause. Address the underlying gastrointestinal issue, whether it is IBS-D, a food intolerance, a medication side effect, or a hidden infection. Shift your dietary focus to soluble fiber so you can absorb excess water and bulk up your stool safely.
For fast relief, use warm sitz baths, zinc oxide barrier creams, and water-based bidets to protect your skin from chemical burns. Most importantly, listen to your body and avoid long, hard straining on the toilet. By following these evidence-based clinical guidelines, you can restore your digestive health and get rid of the pain for good.
Frequently Asked Questions
Can frequent diarrhea actually cause hemorrhoids in adults?
Yes, chronic diarrhea is a primary driver of hemorrhoidal disease. Frequent liquid bowel movements increase intra-abdominal pressure and force the anal sphincter to work excessively. This constant pressure causes the vascular cushions in the anal canal to engorge with blood, stretch, and eventually swell into painful internal or external piles.
Why does liquid stool cause a burning sensation in the rectal area?
Liquid stool is often highly acidic because it moves through the digestive tract too quickly for stomach acids and bile salts to be neutralized. When these raw digestive enzymes reach the rectum, they cause chemical erosion of the delicate mucosal lining and irritate the somatic nerve endings, leading to intense post-diarrhea rectal burning.
What is tenesmus and how does it contribute to piles?
Tenesmus is the agonizing sensation of needing to evacuate the bowels even when the rectum is empty. During diarrhea, inflammation tricks the pudendal nerve into signaling for more movement. This leads to involuntary straining and bearing down, which puts immense physical stress on the rectal veins and can force internal hemorrhoids to prolapse.
Should I use fiber supplements if I am suffering from loose stools?
In clinical practice, we recommend strictly soluble fiber, such as psyllium husk, for loose stools. Unlike insoluble fiber which speeds up transit, soluble fiber acts like a sponge, absorbing excess water in the colon and transforming liquid output into a formed, Type 4 stool on the Bristol Scale, which reduces trauma to the anal canal.
How do I distinguish between internal and external hemorrhoids caused by diarrhea?
Internal hemorrhoids occur above the pectinate line and are typically painless but prone to profuse, bright red bleeding. External hemorrhoids occur below this line in an area rich with somatic nerves; they are often excruciatingly painful and can become thrombosed (clotted) due to the friction of frequent wiping and chemical irritation.
Is there a link between Irritable Bowel Syndrome (IBS-D) and chronic piles?
Absolutely. Approximately 40% of patients with IBS-D report chronic anorectal pain. The unpredictable and frequent nature of IBS-D bowel movements keeps the vascular cushions in a state of perpetual inflammation. Managing the gut-brain axis and slowing gut motility is essential to allow the anorectal tissues to heal.
Why is a bidet recommended over toilet paper for diarrhea sufferers?
Dry toilet paper is highly abrasive and strips the perianal skin of its natural protective oils, leading to micro-tears and friction burns. A bidet uses a gentle stream of water to cleanse the area without physical contact, effectively removing acidic digestive enzymes and reducing the risk of inflammation by up to 50%.
Can certain medications like Metformin lead to hemorrhoidal flare-ups?
Yes, any medication that causes chronic gastrointestinal distress as a side effect can trigger piles. Metformin and broad-spectrum antibiotics are common culprits that can cause medication-induced purging. This constant mechanical and chemical stress on the rectum leads to venous engorgement and swelling.
What is the clinical benefit of a warm sitz bath for rectal pain?
A warm sitz bath provides hydrotherapy that physically relaxes the internal anal sphincter muscle. This relaxation reduces the high resting pressure in the anal canal, allowing trapped blood to flow out of the swollen veins. It also helps safely cleanse the area of residual acidic stool that causes pruritus ani (anal itching).
When should I seek medical attention for bleeding caused by diarrhea?
While bright red blood on the toilet paper is often from localized piles, you should seek immediate medical evaluation if you notice dark maroon or black, tarry stools, as this indicates bleeding higher in the GI tract. Other red flags include severe unremitting pain, fever, or symptoms of anemia like extreme fatigue.
How does the Bristol Stool Scale help in managing hemorrhoids?
The Bristol Stool Scale is a diagnostic tool used by gastroenterologists to categorize stool consistency. For hemorrhoid prevention and healing, the clinical target is ‘Type 4’—smooth and soft. Consistently producing Type 6 (mushy) or Type 7 (liquid) stools indicates active trauma to the vascular cushions that requires dietary or medical intervention.
What is rubber band ligation and when is it necessary?
Rubber band ligation is a minimally invasive office procedure for Grade II or III internal hemorrhoids that don’t respond to fiber therapy. A small band is placed at the base of the swollen vein to cut off blood supply, causing the tissue to shrink and fall off. It also creates a scar that anchors the remaining tissue in place to prevent future prolapse.
Disclaimer
This article is for informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment. The relationship between diarrhea and hemorrhoidal disease is complex; always consult a qualified healthcare professional or gastroenterologist before beginning any new treatment protocol, especially if you are experiencing rectal bleeding, severe pain, or chronic bowel changes.
References
- American Society of Colon and Rectal Surgeons (ASCRS) – fascrs.org – Clinical practice guidelines for the management of hemorrhoidal disease and anorectal trauma.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – niddk.nih.gov – Official statistics on hemorrhoid prevalence and gastrointestinal triggers in adults.
- Mayo Clinic – mayoclinic.org – Diagnostic and treatment protocols for internal and external hemorrhoids and chronic diarrhea.
- Crohn’s & Colitis Foundation – crohnscolitisfoundation.org – Research regarding anorectal complications in patients with Inflammatory Bowel Disease.
- Journal of Clinical Gastroenterology – journals.lww.com – Peer-reviewed studies on the impact of stool consistency and the Bristol Stool Scale on anal health.
- Harvard Health Publishing – health.harvard.edu – Expert insights on the benefits of fiber, sitz baths, and bidet use for rectal health.






