

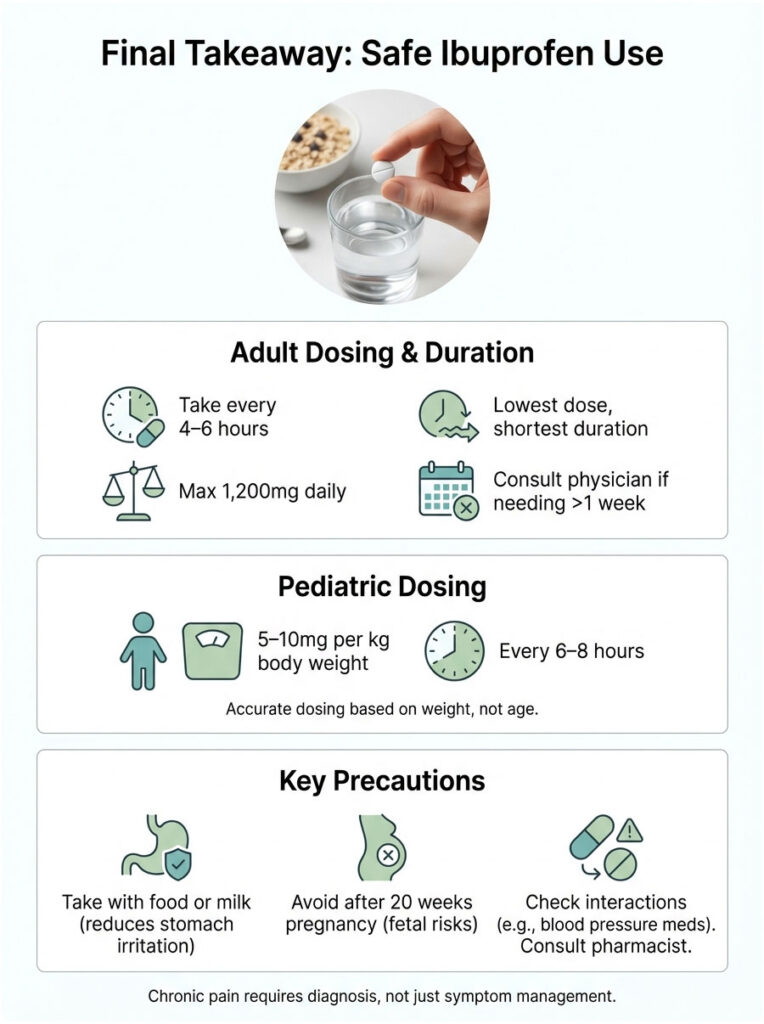
How often can you take ibuprofen? If you’re a healthy adult or teen over 12, you can take it every 4 to 6 hours as needed. A typical single dose is 200mg to 400mg. The hard limit without a prescription is 1,200mg in 24 hours, which works out to six over-the-counter tablets. The golden rule? Take the lowest dose that works, and don’t use it any longer than you have to. Your stomach and kidneys will thank you.
Table of Contents

Why You Need to Get This Right
We’ve all been there. A headache hits in the middle of a workday, or your back locks up after lifting something awkward. You reach for the ibuprofen bottle, glance at the label, and think, “It’s over the counter, so it can’t be that risky.”
That assumption trips people up more than you’d think. As a clinical pharmacist, I see it all the time. People treat the dosing instructions like loose guidelines instead of actual safety boundaries. But understanding how often can you take ibuprofen isn’t just a technicality. It’s one of the simplest things you can do to protect your long-term health.
Ibuprofen is a powerful Non-Steroidal Anti-Inflammatory Drug (NSAID). It’s incredibly effective at reducing inflammation, pain, and fever. But it’s not harmless, and it demands a basic understanding of how it works in your body.
In this guide, we’ll break down the science behind the “every 4 to 6 hours” rule, explain what happens when you take too much, and walk through smarter strategies for managing pain without putting your organs at risk.
Key Numbers Worth Knowing
- 1,200mg is the maximum daily over-the-counter dose set by the FDA.
- 3,200mg is the highest daily dose prescribed under strict medical supervision.
- 1.8 to 2 hours is ibuprofen’s biological half-life in a healthy adult.
- 15% of drug-related acute kidney failure cases are linked to NSAID use.
- 10 days is the longest you should take ibuprofen for pain without seeing a doctor.
The Science Behind “Every 4 to 6 Hours”
That dosing interval on the label isn’t just a rough guess from a marketing department. It’s rooted in how your body processes the drug.
Half-Life and the Therapeutic Window
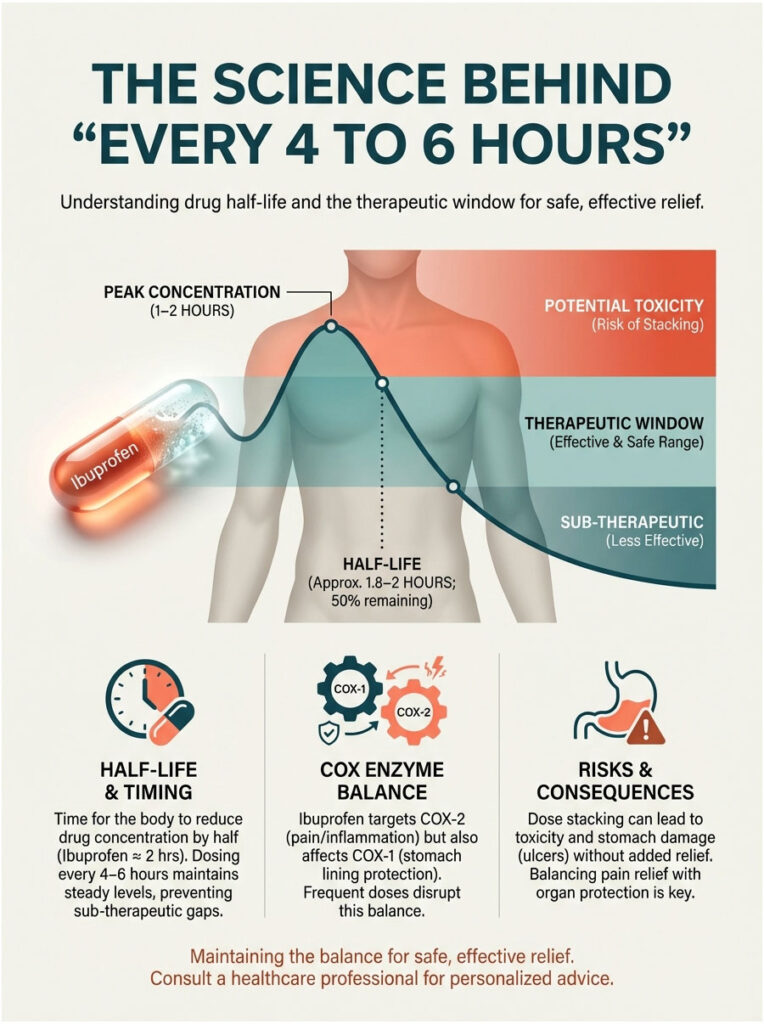
In pharmacology, “half-life” means the time it takes for the drug’s concentration in your blood to drop by 50%. For ibuprofen, that’s roughly 1.8 to 2 hours. So when you take a 400mg dose, your body absorbs it quickly. Blood levels peak within 1 to 2 hours, which is when you feel the most relief. By hour 4, those levels have dropped below what’s needed to keep pain in check.
But lower levels don’t mean the drug is gone.
This is where dose stacking becomes a problem. If you take another dose at hour 2 or 3, you’re adding it on top of whatever the first pill hasn’t cleared yet. Your liver and kidneys haven’t finished their job. The result is higher drug concentrations in your blood, which rarely gives you extra pain relief but significantly raises the risk of toxicity. Your stomach lining and kidneys absorb the damage.
The goal is to stay inside what pharmacologists call the “Therapeutic Window,” the range where you get relief without tipping into organ damage.
How Ibuprofen Actually Stops Pain: COX Inhibition
To understand why dosage limits matter so much, it helps to know the mechanism.
Ibuprofen works by blocking enzymes called Cyclooxygenase, or COX. There are two main types:
- COX-2 is the intended target. It produces prostaglandins that trigger pain, swelling, and fever at the site of an injury.
- COX-1 is the unintended casualty. This enzyme maintains the protective lining of your stomach and helps regulate blood flow to your kidneys.
Here’s the catch: ibuprofen is non-selective. It blocks both. Every time you take a dose to quiet COX-2, you’re also suppressing COX-1. Take it too frequently, and you strip your stomach of the mucosal barrier that protects it from its own acid. That’s when ulcers and erosion start.
Ibuprofen Dosage Guidelines: OTC vs. Prescription
There’s a big gap between what you grab off a pharmacy shelf and what a rheumatologist prescribes. Confusing the two is one of the most common causes of accidental overdose.

Standard Over-the-Counter Dosage (The 1,200mg Rule)
When you’re self-medicating, the FDA sets a firm ceiling. This limit exists because no one is checking your blood work or monitoring your kidney function.
- For general pain or fever: 200mg to 400mg every 4 to 6 hours.
- Daily maximum: 1,200mg in any 24-hour period. That’s six standard 200mg tablets.
- Duration limits: No more than 10 days for pain. No more than 3 days for fever. If symptoms stick around longer, the medication is masking something that needs proper diagnosis.
Prescription-Strength Dosing (The 3,200mg Ceiling)
Doctors sometimes prescribe 800mg three times a day for serious inflammatory conditions like Rheumatoid Arthritis or post-surgical recovery. Under medical supervision, the daily ceiling goes up to 3,200mg, usually split into four 800mg doses.
But patients on this regimen get regular monitoring. Doctors watch for:
- Creatinine levels to make sure the kidneys are clearing waste.
- Hemoglobin to detect silent internal bleeding.
- Blood pressure since NSAIDs can push it higher.
The “Analgesic Ceiling” Effect: More Isn’t Better
This is something most people don’t realize. For acute pain like headaches or toothaches, ibuprofen hits a ceiling around 400mg per dose. Taking 800mg won’t reduce the pain more than 400mg. It will only increase side effects. If 400mg isn’t cutting it, the smarter move is to switch strategies rather than doubling down. Adding acetaminophen (Tylenol), for example, works through a completely different mechanism.
OTC vs. Prescription Ibuprofen: A Quick Comparison
| Feature | Over-the-Counter | Prescription |
|---|---|---|
| Typical Single Dose | 200mg to 400mg | 600mg to 800mg |
| Frequency | Every 4 to 6 hours | Every 6 to 8 hours |
| Max Daily Dose | 1,200mg | 3,200mg |
| Primary Use | Headaches, minor aches, fever | Chronic arthritis, post-surgical pain |
| Risk Level | Low (short-term use) | Moderate to High (requires monitoring) |
| Monitoring Required | Self-watch for stomach pain | Lab tests, blood pressure tracking |
What Happens When You Overdo It: Organ Risks
When you ask how often can you take ibuprofen, you’re really asking how much stress your organs can handle. Let’s look at the specific risks.
Kidney Damage and Acute Kidney Injury
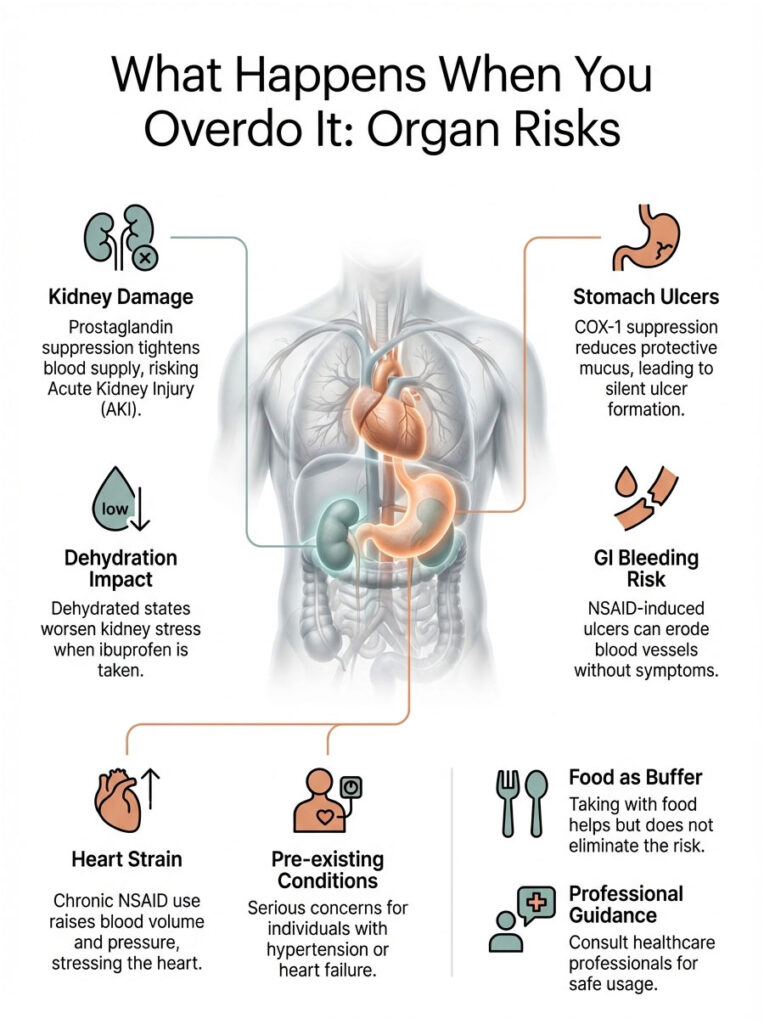
Your kidneys depend on prostaglandins to keep blood flowing through their filtration units. Ibuprofen suppresses those prostaglandins, which effectively tightens the blood supply to the kidneys.
For a healthy, well-hydrated person, this is minor and temporary. But if you’re dehydrated from the flu, a tough workout, or just not drinking enough water, your kidneys are already working harder than usual. Adding ibuprofen in that state is like pinching a garden hose that’s barely running.
The result can be a sudden drop in your Glomerular Filtration Rate (GFR), which leads to Acute Kidney Injury (AKI). This is exactly why athletes should avoid popping ibuprofen before a race. Wait until you’ve rehydrated.
Stomach Ulcers and GI Bleeding
The most common side effect of ibuprofen is gastropathy. With COX-1 suppressed, your stomach produces less protective mucus and less bicarbonate to neutralize acid. Over time, stomach acid starts eating away at the lining itself.
The alarming part? Many NSAID-induced ulcers are completely silent. You might feel nothing until the ulcer erodes into a blood vessel and causes a hemorrhage.
Taking ibuprofen with food helps buffer local acidity, but it doesn’t stop the systemic suppression of COX-1 once the drug is in your bloodstream. Food is helpful, not a fix.
Heart and Blood Pressure Concerns
Both the American Heart Association and the FDA have issued warnings about chronic NSAID use. Ibuprofen causes your kidneys to hold onto sodium and water, which raises blood volume and blood pressure. Over time, this puts extra strain on the heart. For anyone with pre-existing hypertension or heart failure, this is a serious concern.
Safe Dosing for Specific Groups
A dose that’s perfectly fine for a healthy 30-year-old could be risky for an elderly patient or a child. Biology varies, and dosing should reflect that.

Children: Weight-Based Dosing Is Non-Negotiable
In pediatrics, we never dose by age. We dose by weight. The standard pediatric dose is 5mg to 10mg per kilogram of body weight, given every 6 to 8 hours.
One critical safety note for parents: Infant Drops are highly concentrated, while Children’s Liquid Suspension is more diluted. Mixing these formulations up is a surprisingly common cause of accidental overdose. Also, ibuprofen is generally not recommended for infants under 6 months. Their kidneys simply aren’t developed enough to clear the drug efficiently.
Older Adults: Extra Caution Required
Adults over 65 often land on the BEERS Criteria, a widely used list of medications considered potentially inappropriate for seniors. With aging comes decreased kidney mass and lower body water content, which means the drug stays in the system longer and reaches higher concentrations.
For seniors, the answer to how often can you take ibuprofen shifts to “as rarely as possible.” Topical NSAIDs like Diclofenac gel (Voltaren) are often a better choice for localized joint pain. They provide relief right where it’s needed, with much less absorption into the bloodstream.
Pregnancy and Fertility
Ibuprofen is strictly off-limits in the third trimester (after 20 weeks of pregnancy). It can cause premature closure of the ductus arteriosus, a critical vessel in the fetal heart. Early closure can lead to heart failure in the baby. It’s also linked to low amniotic fluid levels.
Women trying to conceive should also be aware that NSAIDs can interfere with ovulation by inhibiting follicle rupture, potentially causing reversible infertility.
A Smarter Approach: Multimodal Pain Management
If your pain is severe, leaning on ibuprofen alone often means hitting the daily limit too fast. There’s a better clinical strategy called Multimodal Analgesia, which attacks pain from two different directions.
The Ibuprofen and Acetaminophen Rotation
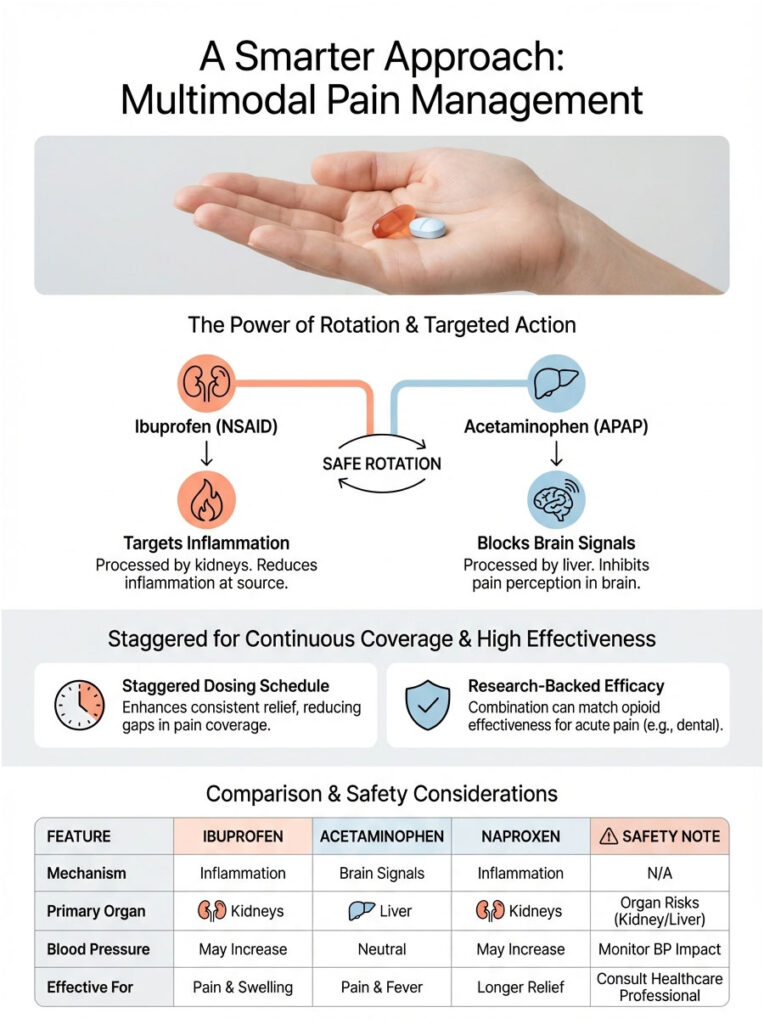
Ibuprofen and acetaminophen (Tylenol) are processed by different organs. Ibuprofen is cleared by the kidneys; acetaminophen is metabolized by the liver. They also work through different mechanisms. Ibuprofen fights inflammation at the site, while acetaminophen blocks pain signals in the brain.
Because they don’t compete, you can stagger them for continuous pain coverage without overdosing on either one. A practical rotation schedule looks like this:
- 12:00 PM: Ibuprofen 400mg
- 3:00 PM: Acetaminophen 500mg
- 6:00 PM: Ibuprofen 400mg
- 9:00 PM: Acetaminophen 500mg
Research has shown this combination can provide pain relief comparable to oral opioids for dental pain, without the addiction risk or sedation.
How Ibuprofen Compares to Other Pain Relievers
| Feature | Ibuprofen (Advil/Motrin) | Acetaminophen (Tylenol) | Naproxen (Aleve) |
|---|---|---|---|
| Drug Type | NSAID | Analgesic / Antipyretic | NSAID |
| Duration | 4 to 6 hours | 4 to 6 hours | 8 to 12 hours |
| Primary Organ Risk | Kidneys and Stomach | Liver | Kidneys and Stomach |
| Best For | Inflammation, swelling, muscle pain | Fever, headache, sensitive stomach | All-day arthritis pain, cramps |
| Safe with Alcohol? | Caution (stomach bleeding risk) | No (severe liver damage risk) | Caution (stomach bleeding risk) |
| Blood Pressure Impact | Can raise BP | Neutral | Can raise BP |
Dangerous Drug Interactions to Avoid
As a pharmacist, the thing that worries me most isn’t ibuprofen by itself. It’s what people combine it with. Certain combinations can turn a perfectly safe dose into a medical emergency.
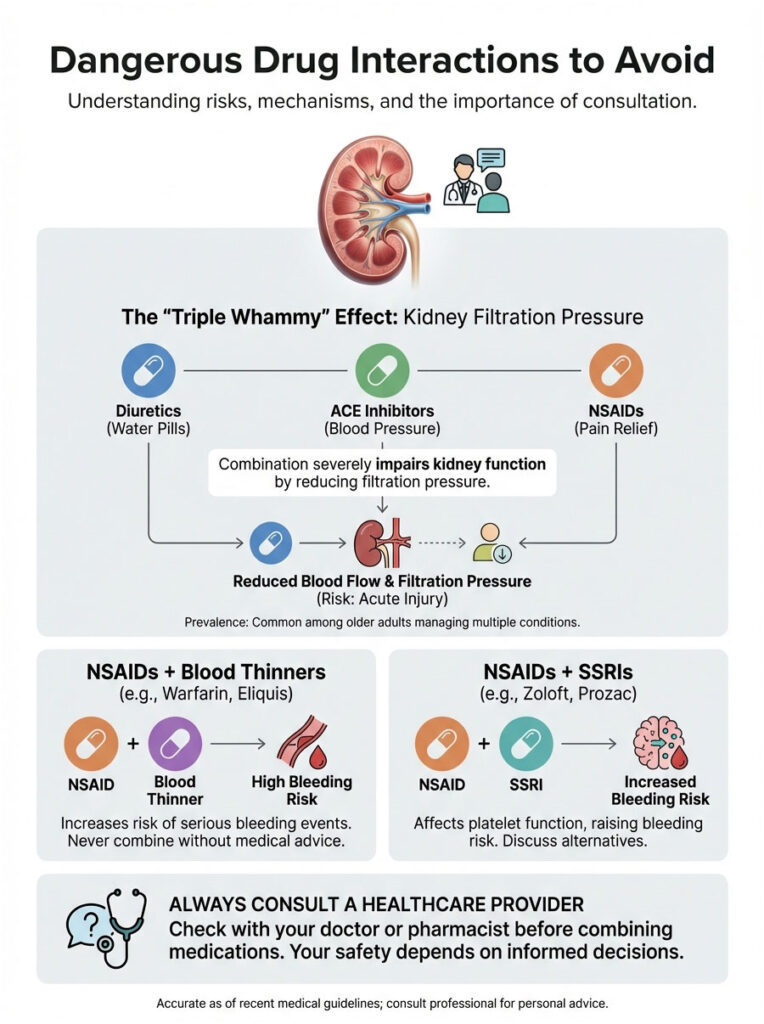
The “Triple Whammy” Effect
This is a term used in clinical practice for a potentially catastrophic drug interaction. It happens when someone takes all three of these at the same time:
- An NSAID like ibuprofen
- A diuretic (water pill) like Hydrochlorothiazide
- An ACE inhibitor or ARB (blood pressure medication) like Lisinopril
The diuretic reduces blood volume. The ACE inhibitor relaxes blood vessels leaving the kidney. The NSAID constricts blood vessels entering the kidney. Together, they cause a near-total collapse of filtration pressure, which can trigger acute kidney failure. If you take blood pressure medication, always talk to your doctor before using ibuprofen.
Blood Thinners and Antidepressants
If you’re on anticoagulants like Warfarin, Eliquis, or Xarelto, ibuprofen is generally off the table. It interferes with platelet function, and combining the two raises bleeding risk significantly.
SSRI antidepressants like Sertraline (Zoloft) or Fluoxetine (Prozac) also affect platelet function. When combined with regular NSAID use, the risk of upper gastrointestinal bleeding goes up.
Liquid Gels vs. Tablets: Does the Formulation Matter?
It does, particularly when it comes to how fast the medication kicks in and how often you feel the urge to take another dose.
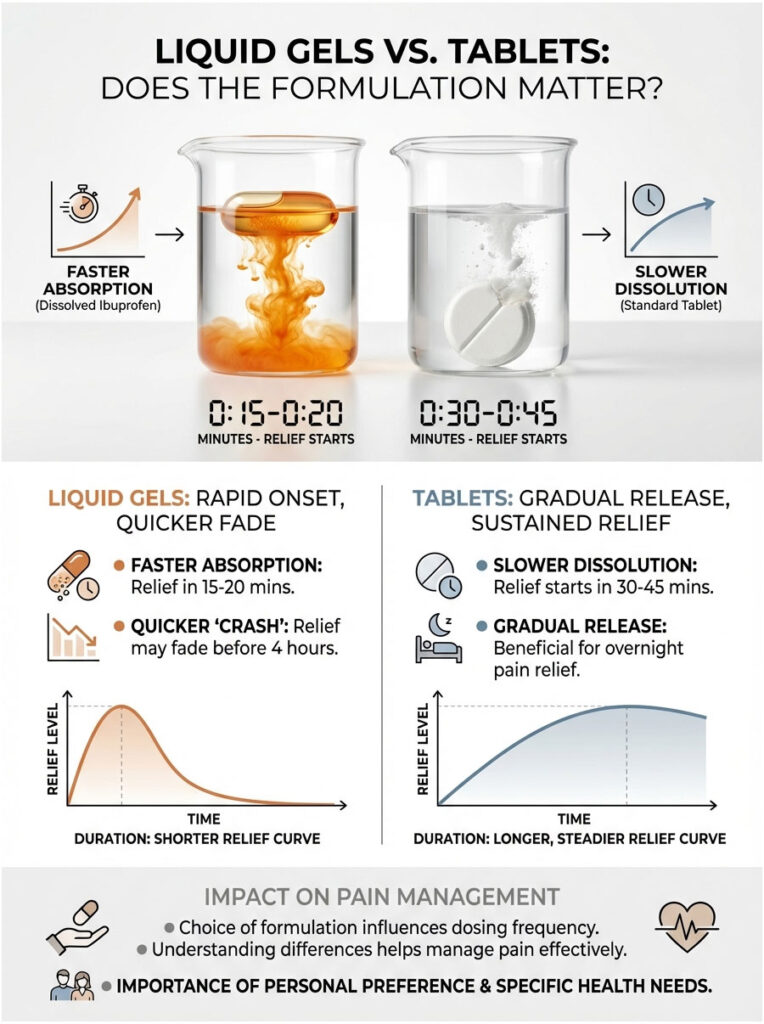
Liquid Gels
These contain ibuprofen that’s already dissolved. Since your body doesn’t need to break down a hard tablet, absorption is faster. You might feel relief in 15 to 20 minutes. The trade-off is that the drug may wear off slightly sooner, which can create a “crash” in pain relief before the 4-hour mark.
Standard Tablets
Compressed powder tablets take longer to dissolve in the stomach. Relief usually starts in 30 to 45 minutes, but the release is more gradual. For overnight pain, a standard tablet often works better than a liquid gel because it covers the full duration of sleep more effectively.
The Myth of “Pre-Dosing” for Athletes
There’s a risky habit in amateur sports where runners and cyclists pop 600mg of ibuprofen before a race to prevent pain. This approach is physiologically unsound.

During intense exercise, your body redirects blood away from the kidneys and toward working muscles. Kidney filtration is already reduced. Adding an NSAID on top of that further tightens the blood supply, creating a perfect setup for kidney injury.
On top of that, research suggests NSAIDs may actually slow muscle recovery by blocking the inflammatory process needed for muscle repair and growth. Pain is your body’s signal system. Silencing it before it has something to say doesn’t help you perform better.
Recognizing Signs of Ibuprofen Overdose
Knowing when you’ve crossed the line is essential. Ibuprofen toxicity shows up in several ways, some subtle, some urgent.
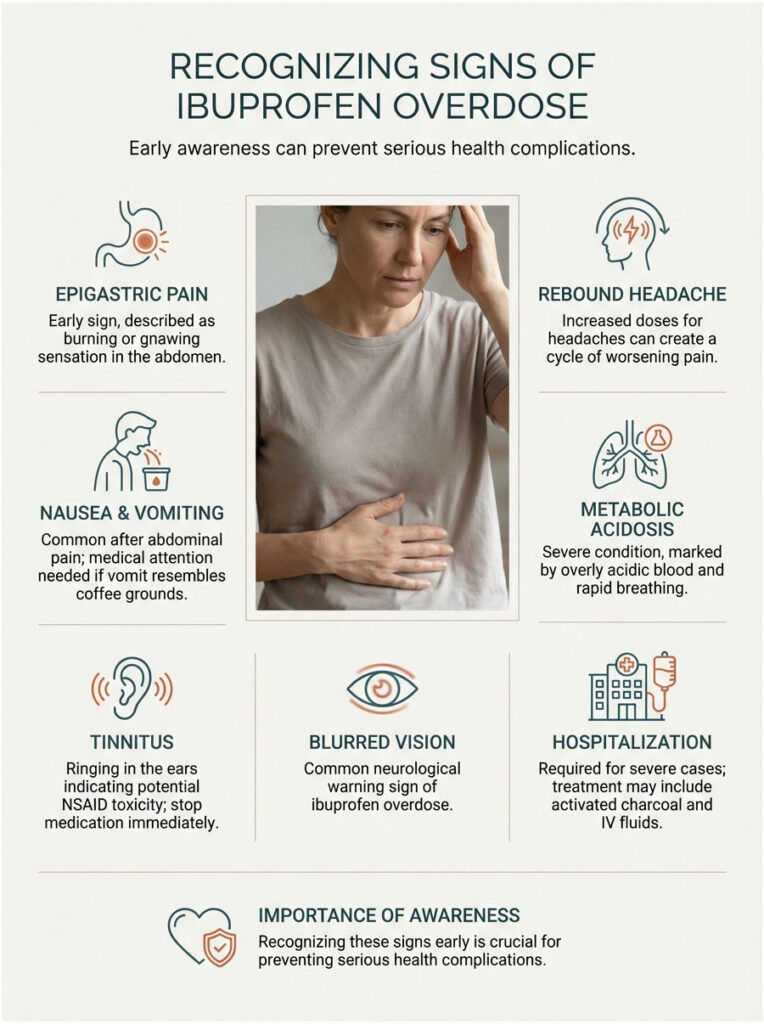
Stomach and Digestive Symptoms
The earliest warning is usually epigastric pain, a burning or gnawing sensation in the upper center of your abdomen. Nausea and vomiting often follow. If vomit looks like coffee grounds (indicating old blood), that’s a medical emergency. Get help immediately.
Neurological Warning Signs
At high doses, ibuprofen affects the central nervous system. Tinnitus, or ringing in the ears, is a classic red flag for NSAID toxicity. If your ears start ringing, stop taking the medication right away. Blurred vision and worsening headaches are also common. In fact, taking too much ibuprofen for a headache can trigger a “rebound headache,” trapping you in a cycle of increasing doses.
Metabolic Acidosis
In severe overdose situations, the blood becomes overly acidic, a condition called metabolic acidosis. It causes rapid breathing as the body tries to blow off carbon dioxide to compensate. This requires hospitalization. Treatment typically involves activated charcoal to bind the drug in the stomach and IV fluids to support kidney function.
Natural Alternatives That Can Reduce Your Ibuprofen Use
You don’t always have to reach for the medicine cabinet. Several non-pharmacological methods can genuinely extend the time between doses.

Ice and Heat Therapy
Ice acts as a natural vasoconstrictor. It physically reduces blood flow and inflammation without chemicals. For acute injuries like sprains, ice in the first 48 hours can significantly cut down the need for NSAIDs.
Heat does the opposite. It boosts blood flow and relaxes muscles. For tension headaches or back spasms, a heating pad often works just as well as, or better than, a pill.
Topical Counter-Irritants
Menthol and capsaicin creams create a strong sensation on the skin that essentially distracts your brain from deeper pain signals. This is based on the “Gate Control Theory” of pain. By stimulating nerve endings at the surface, you can effectively “close the gate” on pain from deeper tissues, buying more time before your next dose.
Final Takeaway
Here’s the bottom line on how often can you take ibuprofen: every 4 to 6 hours, staying under the 1,200mg daily OTC cap. But remember, the limit isn’t the target. Your goal should always be the lowest effective dose for the shortest time.
If you’re reaching for the bottle every 4 hours for more than a week, the ibuprofen isn’t failing. Something else is going on that needs a proper diagnosis.
Chronic pain calls for a root-cause solution, not a stronger chemical mask. Talk to a physician about treating the source of the problem, not just the symptom. Your kidneys, your stomach, and your heart will be better off for it.
Frequently Asked Questions
How many hours should I wait between doses of ibuprofen?
For healthy adults, the standard interval is every 4 to 6 hours to maintain the therapeutic window and prevent serum accumulation. This timing aligns with the drug’s biological half-life of approximately 2 hours, ensuring the previous dose is sufficiently cleared. Always aim for the lowest effective dose for the shortest duration possible to protect your internal organs.
What is the maximum daily limit for over-the-counter ibuprofen?
The FDA-mandated limit for self-medication is 1,200mg within a 24-hour period, which typically equates to six 200mg tablets. While clinical prescriptions may reach 3,200mg under strict medical supervision, exceeding the OTC limit without monitoring significantly increases the risk of gastrointestinal bleeding and renal stress. If your pain requires more than 1,200mg a day, you must consult a healthcare provider for a formal diagnosis.
Does taking a higher dose of ibuprofen provide better pain relief?
Ibuprofen has an “analgesic ceiling” generally around 400mg for acute pain, meaning doses beyond this do not offer proportional increases in relief. Instead of silencing more pain, higher doses primarily increase the risk of side effects like stomach lining erosion and kidney strain. If 400mg is ineffective, switching to a different mechanism of action is scientifically superior to simply doubling the dose.
Can I take ibuprofen and acetaminophen at the same time?
Yes, staggering ibuprofen and acetaminophen is a highly effective clinical strategy known as multimodal analgesia. Since they are metabolized by different organs—the kidneys and liver, respectively—you can alternate them every 3 hours to provide continuous pain coverage without exceeding daily limits for either. This combination often provides relief comparable to oral opioids for dental and orthopedic pain.
Why is it recommended to take ibuprofen with food or milk?
Ibuprofen inhibits the COX-1 enzyme, which is responsible for maintaining the protective mucosal lining of your stomach. Taking it with food or milk provides a physical buffer against local acid irritation, though it does not eliminate the systemic risk of ulceration once the drug is absorbed. If you experience epigastric pain or persistent indigestion, you should discontinue use and seek medical advice.
How does ibuprofen affect kidney function during exercise?
Ibuprofen inhibits prostaglandins that keep the blood vessels leading to your kidneys open, which can reduce the glomerular filtration rate. During intense exercise, blood is already shunted away from the kidneys, and adding an NSAID can lead to acute kidney injury (AKI). We strongly advise athletes to rehydrate fully before considering ibuprofen use after an event.
How do I calculate the correct ibuprofen dose for a child?
Pediatric dosing must always be calculated by weight rather than age, using a standard of 5mg to 10mg per kilogram of body weight every 6 to 8 hours. It is vital to use the specific measuring device provided with the medication and to distinguish between concentrated infant drops and children’s liquid suspension. Never administer ibuprofen to infants under 6 months old without direct medical guidance.
Can ibuprofen interfere with blood pressure medications?
Ibuprofen can reduce the effectiveness of blood pressure medications like ACE inhibitors and diuretics, potentially leading to a “Triple Whammy” effect on the kidneys. This combination can cause a dangerous drop in renal filtration pressure, resulting in acute kidney failure. Patients managing hypertension should always consult their pharmacist before adding an NSAID to their medication regimen.
Are ibuprofen liquid gels faster than standard tablets?
Solubilized ibuprofen in liquid gels is absorbed more rapidly by the body, often providing relief within 15 to 20 minutes because the drug is already in solution. While they offer a faster onset than compressed powder tablets, the relief may also clear the system slightly quicker. For sustained relief, such as managing pain overnight, a standard tablet may provide a more consistent therapeutic profile.
Is it safe to take ibuprofen during the third trimester of pregnancy?
Ibuprofen is strictly contraindicated after 20 weeks of pregnancy because it can cause the premature closure of the fetal ductus arteriosus. This can lead to serious heart and lung issues for the baby or dangerously low levels of amniotic fluid. Acetaminophen is generally the preferred alternative for pain management during pregnancy, but always consult your obstetrician first.
Can ibuprofen cause ringing in the ears or tinnitus?
Yes, high doses or chronic use of NSAIDs like ibuprofen can affect the central nervous system and cause tinnitus, or ringing in the ears. This is often a sign of salicylate-related toxicity and indicates that you have exceeded your body’s tolerance level. If your ears start ringing, you should stop the medication immediately and consult a healthcare professional.
How many days in a row can I safely take ibuprofen for pain?
For self-treatment of pain, you should not exceed 10 consecutive days of ibuprofen use without consulting a physician; for fever, the limit is 3 days. Prolonged use without medical oversight increases the risk of cardiovascular events, silent gastrointestinal ulcers, and “rebound” headaches. If symptoms persist beyond these windows, the medication is likely masking a condition that requires a professional diagnosis.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. The information provided is based on general pharmacological guidelines and should not replace the advice of your physician or pharmacist. Always consult a qualified healthcare professional before starting or changing any medication regimen, especially if you have pre-existing conditions or are taking other medications.
References
- U.S. Food and Drug Administration (FDA) – fda.gov – Official guidelines on Over-the-Counter (OTC) NSAID labeling and maximum daily dosage limits.
- Mayo Clinic – mayoclinic.org – Comprehensive drug profile for ibuprofen including side effects, interactions, and standard dosing intervals.
- American Heart Association (AHA) – heart.org – Research and warnings regarding the cardiovascular risks associated with chronic NSAID use and sodium retention.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – niddk.nih.gov – Data on drug-induced kidney injury and the impact of NSAIDs on renal filtration.
- The BEERS Criteria / American Geriatrics Society – americangeriatrics.org – Guidelines for potentially inappropriate medication use in older adults regarding NSAID toxicity.
- Journal of Clinical Pharmacology – wiley.com – Peer-reviewed studies on the pharmacokinetics, half-life, and “analgesic ceiling” of ibuprofen.






