

Every week, patients sit in my gastroenterology clinic completely exhausted by their own digestive systems. They are terrified of restaurants, anxious about social events, and desperate for answers. As a board-certified gastroenterologist with over 15 years of clinical experience, I hear this complaint daily.
Table of Contents
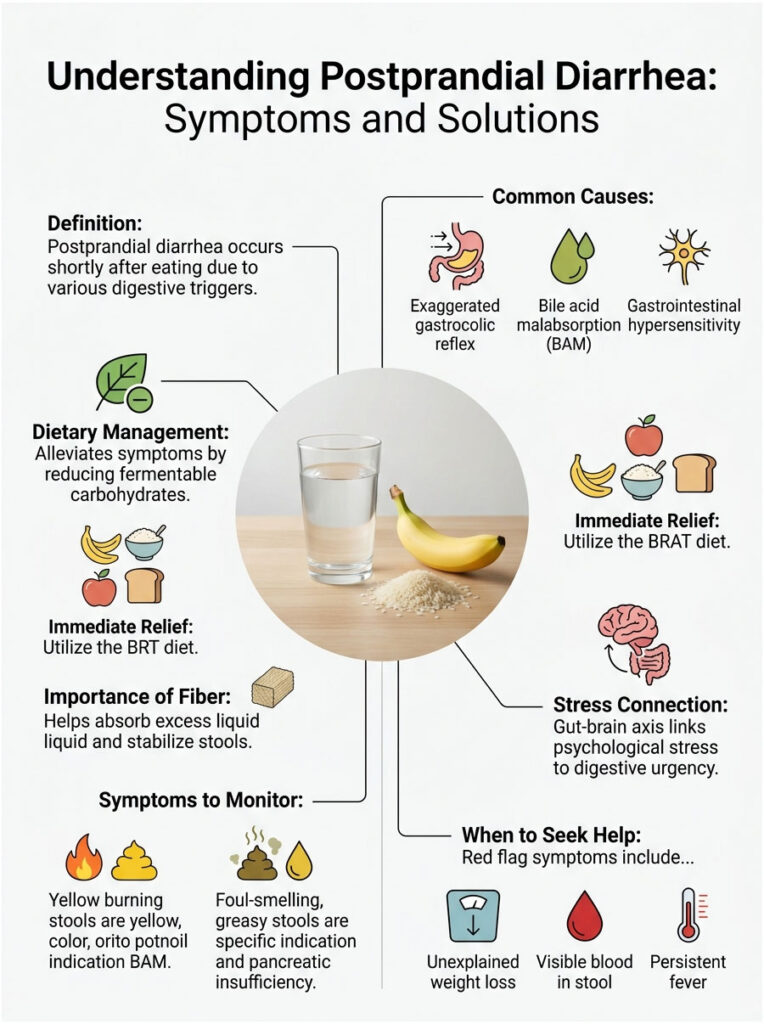
You finish a meal, and within twenty minutes your stomach drops. A sharp, twisting pain hits your lower abdomen. You have to rush to the nearest restroom immediately. This is medically known as postprandial diarrhea, and it is not a disease in itself. It is a warning sign that a mechanical or chemical misfire is happening inside your digestive tract.
This guide covers exactly why this cycle happens, provides immediate relief protocols, explains the underlying causes, and outlines long-term evidence-based strategies for restoring gut health.
Quick Answer: How to Stop Cramps and Diarrhea After Eating
For immediate relief, start with a 24-hour gut rest using the BRAT diet (Bananas, Rice, Applesauce, Toast) to provide binding fibers without irritating the bowel. Loperamide can temporarily slow intestinal motility. Enteric-coated peppermint oil capsules act as natural antispasmodics for sharp pain. For a permanent fix, you need to identify your root cause, which is often an exaggerated gastrocolic reflex, bile acid malabsorption, or a specific food intolerance.
Key Statistics on Digestive Health
- Up to 20% of U.S. adults experience symptoms of irritable bowel syndrome (American College of Gastroenterology, 2023).
- 1 in 3 IBS-D patients actually suffer from undiagnosed bile acid malabsorption.
- The gut contains over 500 million neurons, operating independently from the brain.
- The gastrocolic reflex is most active within 15 to 30 minutes after a high-fat or high-calorie meal.
- Over 70% of functional gut disorder patients report that psychological stress directly triggers their postprandial diarrhea.
- A strict low-FODMAP diet provides significant relief in up to 75% of patients (Monash University, 2022).
Understanding Postprandial Diarrhea and the Enteric Nervous System
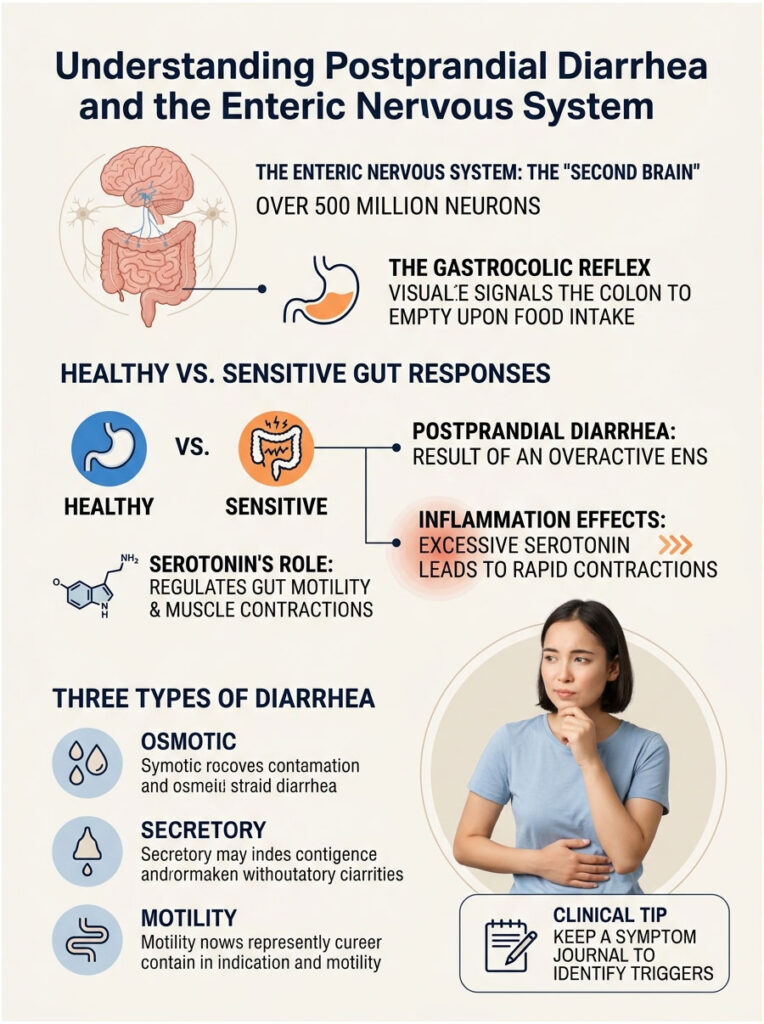
To fix your digestion, you need to understand how it works. Your gut operates using its own independent nervous system, called the enteric nervous system. It is so complex that medical professionals often call it your second brain. This network of over 500 million neurons controls everything from breaking down proteins to moving waste through your body.
When this system becomes hyperactive, postprandial diarrhea is the most common result. The timing of symptoms is not a coincidence. It comes down to a specific neural pathway hardwired into your anatomy.
The Gastrocolic Reflex
Every time you eat, stretch receptors in the stomach wall detect the physical expansion and send rapid signals to the lower colon. This communication pathway, called the gastrocolic reflex, tells the colon to empty its current contents to make room for incoming food.
In a healthy person, this reflex causes a mild, barely noticeable contraction. In patients with sensitive guts, it triggers violent spasms across the entire large intestine. This rapid movement causes severe pain and forces liquid stool out before the colon can absorb water. You are not passing the food you just ate. You are passing yesterday’s food, while the new meal simply pulled the trigger.
Serotonin’s Role in Gut Motility
About 90% of your body’s serotonin is produced inside the digestive tract. In the gut, serotonin acts as a motility director. Specialized cells in the intestinal lining release it to trigger muscle contractions that push food through at a steady pace.
When the gut lining becomes inflamed, these cells dump massive amounts of serotonin at once. The result is wild, rapid contractions that push food through at breakneck speed, completely ruining the water absorption process. Managing gut serotonin levels is critical for lasting digestive relief.
Three Types of Diarrhea
Osmotic diarrhea happens when unabsorbed food particles pull excess water into the intestines. Lactose intolerance is the classic example: undigested milk sugar acts like a sponge and draws water in.
Secretory diarrhea occurs when the intestinal lining actively pumps fluid into the bowel. Bacterial infections and food poisoning typically cause this reaction.
Motility diarrhea happens when food moves too fast through the tract for the colon to absorb water. An exaggerated gastrocolic reflex is the primary driver.
Clinical Tip: Keep a symptom journal for one full week. Note exactly how many minutes pass between your first bite and the rush to the restroom. If it happens within 20 to 30 minutes, you are almost certainly dealing with an overactive gastrocolic reflex rather than food poisoning.
Immediate Relief: How to Ease Stomach Cramps and Diarrhea After Eating Right Now
When you are trapped in a cycle of pain, you need solutions that work today. These interventions halt physical spasms and slow transit time. They will not cure the underlying cause, but they will give you your life back while you investigate deeper issues.
Over-the-Counter Medications
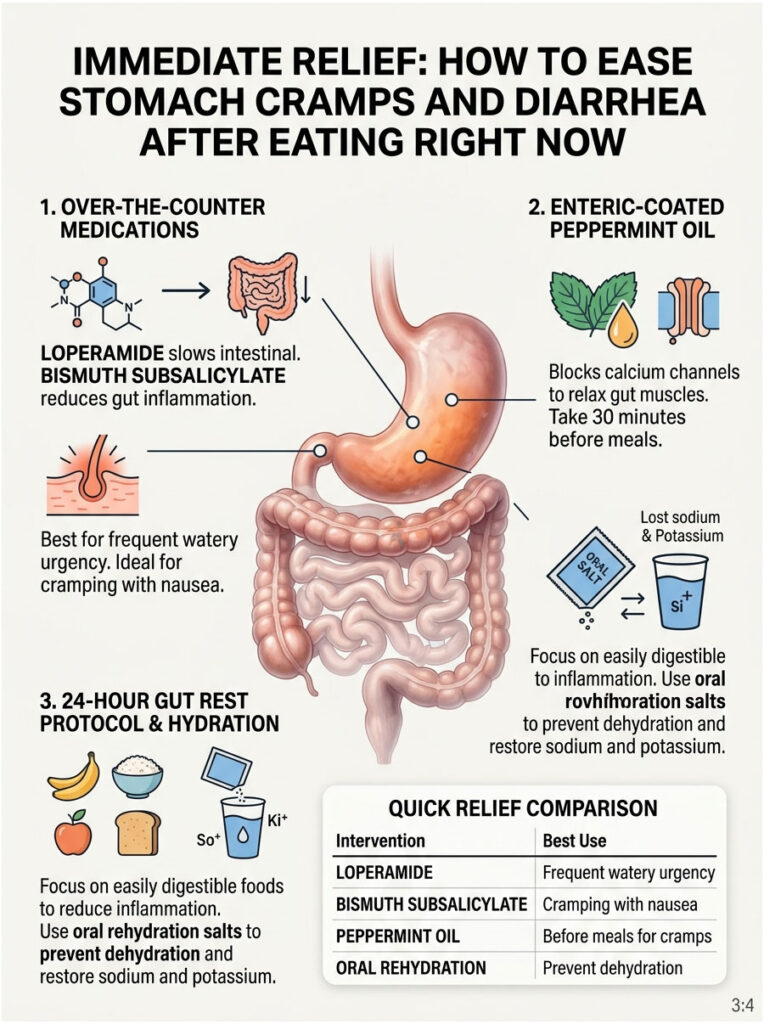
Loperamide (Imodium) binds to opioid receptors in the gut wall, directly slowing intestinal contractions. This gives the colon time to absorb excess water, turning liquid stool into solid, formed stool. It is a reliable rescue medication for social events or long car rides.
Bismuth subsalicylate (Pepto-Bismol) reduces gut inflammation and acts as an anti-secretory agent. If your gut is actively pumping water into the bowel, bismuth helps shut those fluid pumps off. It is particularly useful when postprandial diarrhea comes with mild nausea. Note that it will temporarily turn stool a harmless dark black color.
Enteric-Coated Peppermint Oil
Peppermint oil contains menthol, which acts as a natural calcium channel blocker in the digestive tract. It physically prevents calcium ions from entering gut smooth muscle cells. Without calcium, the muscle cannot contract violently. The key is to buy capsules labeled “enteric-coated” so the pill survives stomach acid and opens where it is needed in the lower intestines. Take one capsule 30 minutes before a large meal.
The 24-Hour Gut Rest Protocol
When your gut is severely inflamed, stop aggravating it with complex foods. A 24-hour gut rest does not mean fasting. It means eating foods that require zero effort to digest. The BRAT diet, consisting of bananas, white rice, applesauce, and plain toast, provides binding fibers that firm up stool without causing fermentation or gas.
Hydration is equally critical. Every bout of diarrhea causes you to lose sodium and potassium. Plain water alone is not enough. Use oral rehydration salts (ORS) mixed into water. These blends of sodium, potassium, and glucose use a special transport system in your gut to pull water into dehydrated cells much faster than water alone.
Quick Relief Comparison
| Intervention | Option | How It Works | Best For |
| OTC Medication | Loperamide (Imodium) | Slows intestinal motility | Frequent watery urgency |
| OTC Medication | Bismuth Subsalicylate | Reduces inflammation and secretion | Cramping with nausea |
| Natural Remedy | Peppermint Oil (enteric-coated) | Blocks calcium channels, relaxes gut | Sharp spasm-like pain |
| Dietary | Oral Rehydration Salts | Restores sodium and potassium | Preventing dehydration |
| Dietary | BRAT Diet | Provides low-fiber, non-irritating food | 24-hour acute gut rest |
Clinical Causes: Why Does Food Trigger Immediate Diarrhea?
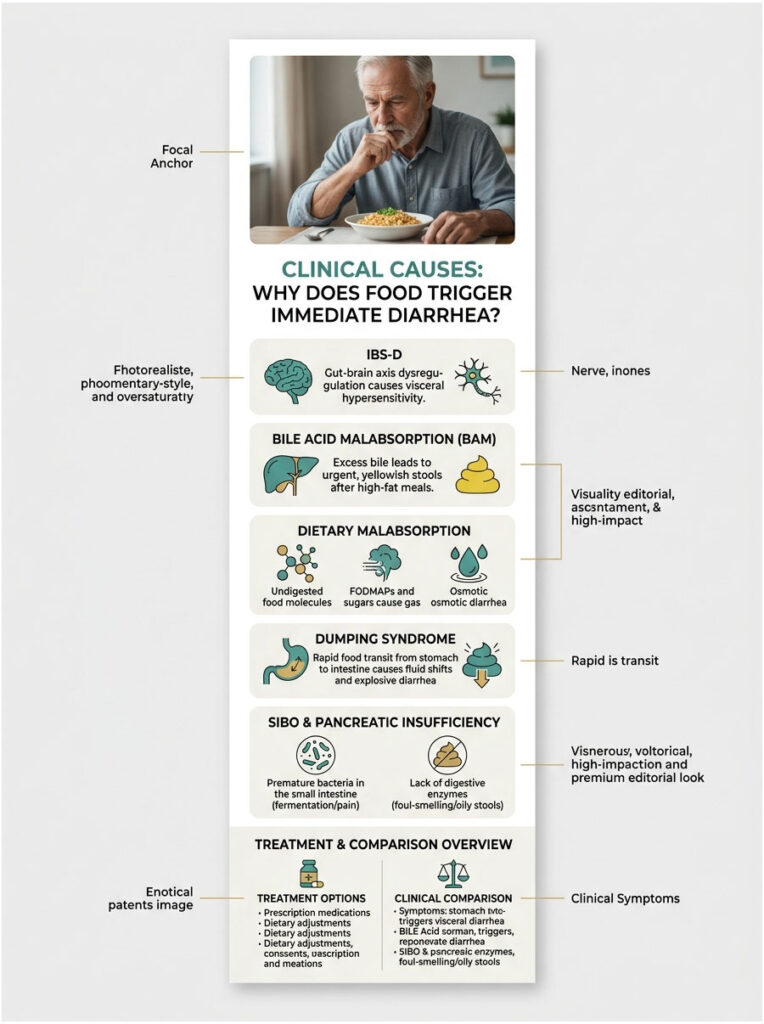
Treating symptoms is only half the battle. To find a permanent solution, you must identify your specific clinical trigger. The digestive tract is a finely tuned chemical environment, and even a minor imbalance can cause severe daily postprandial diarrhea.
IBS-D and Gut-Brain Axis Dysregulation
Irritable Bowel Syndrome with Diarrhea (IBS-D) is the most common diagnosis for after-meal cramping. It is fundamentally a disorder of the gut-brain axis. Your gut and brain communicate constantly via the vagus nerve. Chronic stress or anxiety sends distress signals down this pathway directly to your intestines.
This creates visceral hypersensitivity, where the nerves in your colon become incredibly reactive to normal stimuli. A normal amount of digestive gas feels like a major threat. The gut-brain axis panics and flushes the entire system. This is why symptoms are always worse on stressful days.
Bile Acid Malabsorption (BAM)
BAM is one of the most underdiagnosed conditions in gastroenterology. Your liver produces bile to digest fats. Normally, the end of your small intestine reabsorbs that bile for recycling. In patients with BAM, this reabsorption fails. Excess bile spills into the colon, where it acts as a powerful natural laxative.
This produces urgent, yellowish, burning stools immediately after high-fat meals. We see this frequently in patients who have had their gallbladders removed, a scenario called post-cholecystectomy syndrome. Without a gallbladder to store bile, the liver constantly drips acid into the intestines. Treatment usually requires prescription bile acid binders.
Dietary Malabsorption: FODMAPs, Lactose, and Fructose
Sometimes the body lacks the enzymes needed to break down certain carbohydrates. These fermentable sugars, categorized as FODMAPs, travel undigested to the large intestine. Gut bacteria feast on them, producing massive amounts of gas that stretch intestinal walls and cause sharp pain. Simultaneously, the unabsorbed sugars pull extra water into the bowel, triggering osmotic diarrhea.
Dumping Syndrome
Dumping syndrome occurs when food moves from stomach to small intestine too quickly. It is most common after gastric bypass or bariatric surgery but can happen to anyone with very fast gastric emptying. When a large, sugary meal dumps into the small intestine, the body pulls massive amounts of fluid from the bloodstream to dilute the sugar. This rapid fluid shift causes cramping, cold sweating, a racing heart, and explosive diarrhea. Eating smaller, protein-focused meals is the best defense.
Small Intestinal Bacterial Overgrowth (SIBO)
Most beneficial gut bacteria belong in the large intestine. When they migrate into the small intestine, they begin fermenting food before you can digest it. This damages the gut lining over time, creating increased intestinal permeability (often called “leaky gut”). The constant low-grade inflammation amplifies the gastrocolic reflex, causing immediate pain after meals high in carbohydrates. Treatment typically requires gut-specific antibiotics like Rifaximin.
Pancreatic Insufficiency (EPI)
Your pancreas produces enzymes needed to break down proteins, carbohydrates, and fats. If the pancreas is damaged or sluggish, it cannot produce enough enzymes. Undigested fats pass through the tract, causing steatorrhea: foul-smelling, pale, floating stools that leave a greasy film on toilet water. Treatment requires prescription pancreatic enzyme replacement therapy (PERT) taken with every meal and snack.
Clinical Cause Comparison
| Suspected Cause | Key Triggers | Distinctive Symptoms | Mechanism |
| Bile Acid Malabsorption | High-fat meals, greasy food | Yellow stool, burning urgency | Excess bile irritates colon |
| Lactose/FODMAP Intolerance | Dairy, garlic, onions, wheat | Severe bloating, trapped gas | Osmotic shift + bacterial fermentation |
| Dumping Syndrome | High-sugar meals, large portions | Cold sweating, dizziness, palpitations | Rapid fluid shift into small intestine |
| Pancreatic Insufficiency | Heavy high-fat meals | Foul, floating, oily stools | Lack of digestive enzymes |
| IBS-D | Stress, caffeine, large meals | Pain relief after bowel movement | Visceral hypersensitivity |
The Gut Microbiome and Digestive Health
The trillions of bacteria in your large intestine play a critical role in how you process food. When the ecosystem is balanced, good bacteria produce short-chain fatty acids that nourish colon cells and keep them healthy.
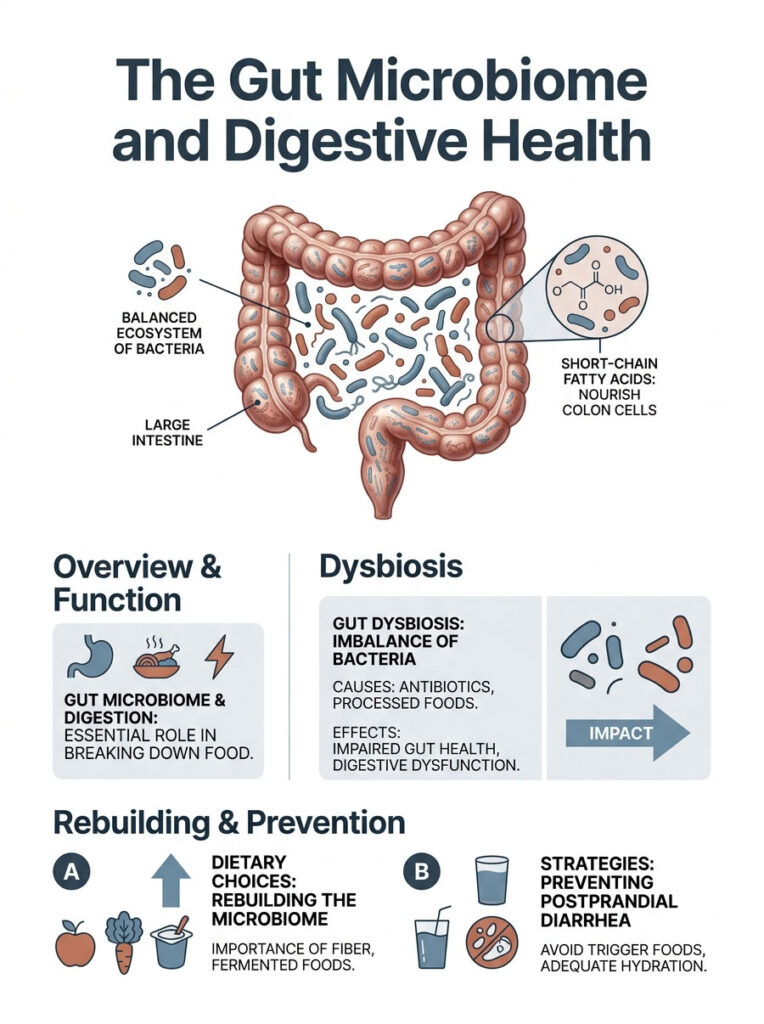
When harmful bacteria outnumber beneficial ones, a state called gut dysbiosis develops. This frequently happens after multiple courses of antibiotics or from a diet heavy in processed foods and refined sugars. Dysbiosis inflames the gut lining and makes the gastrocolic reflex hyperactive. Rebuilding a diverse, robust microbiome through targeted dietary choices is essential for stopping postprandial diarrhea permanently.
Long-Term Strategies for Restoring Gut Health
Once you survive the acute flare-up, lasting healing requires changing the fundamental environment of your digestive tract. You cannot rely on anti-diarrhea pills indefinitely.
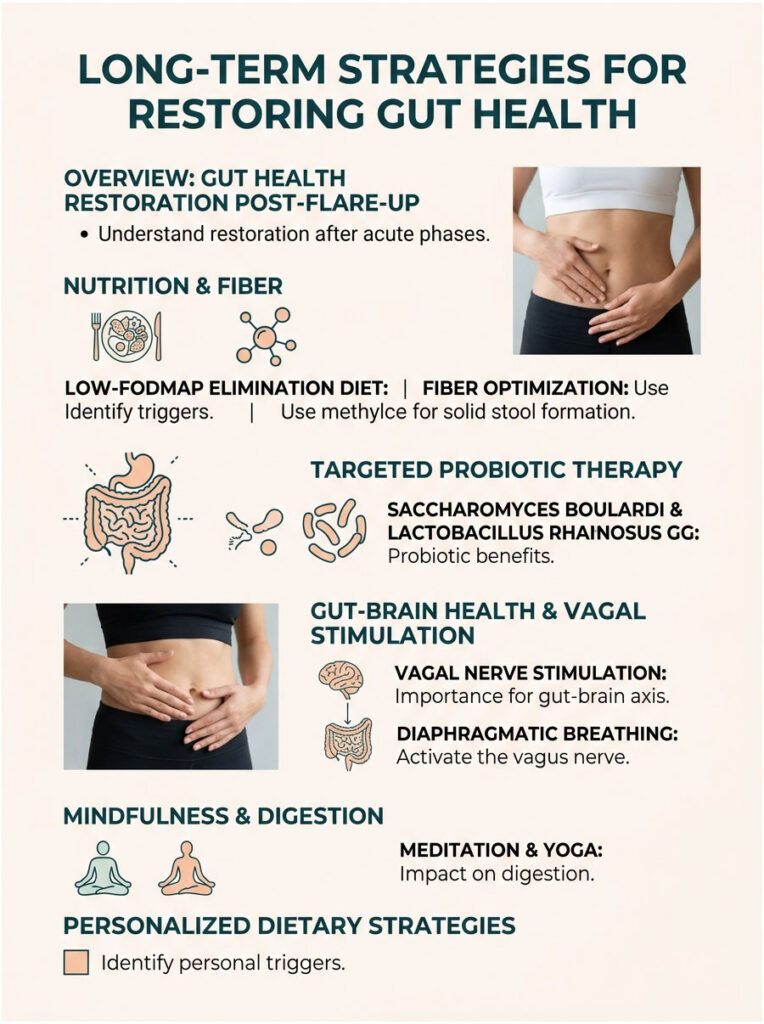
The Low-FODMAP Elimination Diet
Developed by researchers at Monash University, the low-FODMAP diet is the gold standard for treating functional gut disorders. For two to six weeks, you eliminate all highly fermentable carbohydrates: wheat, dairy, certain fruits, garlic, onions, and artificial sweeteners. This starves overgrown gut bacteria of their fuel and reduces internal gas production.
Once inflammation subsides, you slowly reintroduce these foods one at a time. This methodical approach identifies your exact personal triggers. You might find that wheat is fine but garlic causes instant diarrhea. Knowing your specific triggers practically eliminates postprandial symptoms.
Fiber Optimization with Methylcellulose
Adding fiber for diarrhea sounds counterintuitive, but the type of fiber matters. Soluble fiber acts like a sponge, absorbing excess water and turning liquid stool into solid, formed stool. I recommend methylcellulose specifically because, unlike psyllium husk, it is 100% non-fermentable. Gut bacteria cannot eat or ferment it, so it never causes gas, bloating, or cramping. A daily dose provides consistent bulk and slows transit time.
Targeted Probiotic Therapy
Not all probiotics are equal. For diarrhea-predominant patients, I recommend Saccharomyces boulardii, a beneficial yeast that actively fights harmful bacteria and stops secretory diarrhea. The bacterial strain Lactobacillus rhamnosus GG has strong clinical evidence for reducing gut inflammation and soothing aggravated nerve endings. Taking both daily can significantly repair damaged intestinal permeability.
Vagal Nerve Stimulation
Because the gut-brain axis plays such a large role, treating the nervous system is essential. The vagus nerve controls the “rest and digest” parasympathetic system. When anxiety dominates, your sympathetic fight-or-flight system takes over and wrecks digestion.
You can activate the vagus nerve manually through specific exercises. Five minutes of slow diaphragmatic breathing before a meal sends a signal to the brain that you are safe, naturally dampening the gastrocolic reflex before you take your first bite. Daily meditation, yoga, or targeted breathing exercises drastically reduce visceral hypersensitivity over time.
Diagnostic Tests and Red Flag Symptoms
Fecal Calprotectin Testing
One of the most important tests is a stool test for fecal calprotectin. This inflammatory protein is released by white blood cells when your intestines are actively inflamed. Normal levels let us confidently diagnose functional issues like IBS-D or food intolerance. Elevated levels point toward Inflammatory Bowel Disease (Crohn’s or ulcerative colitis), which requires immediate medical therapy.
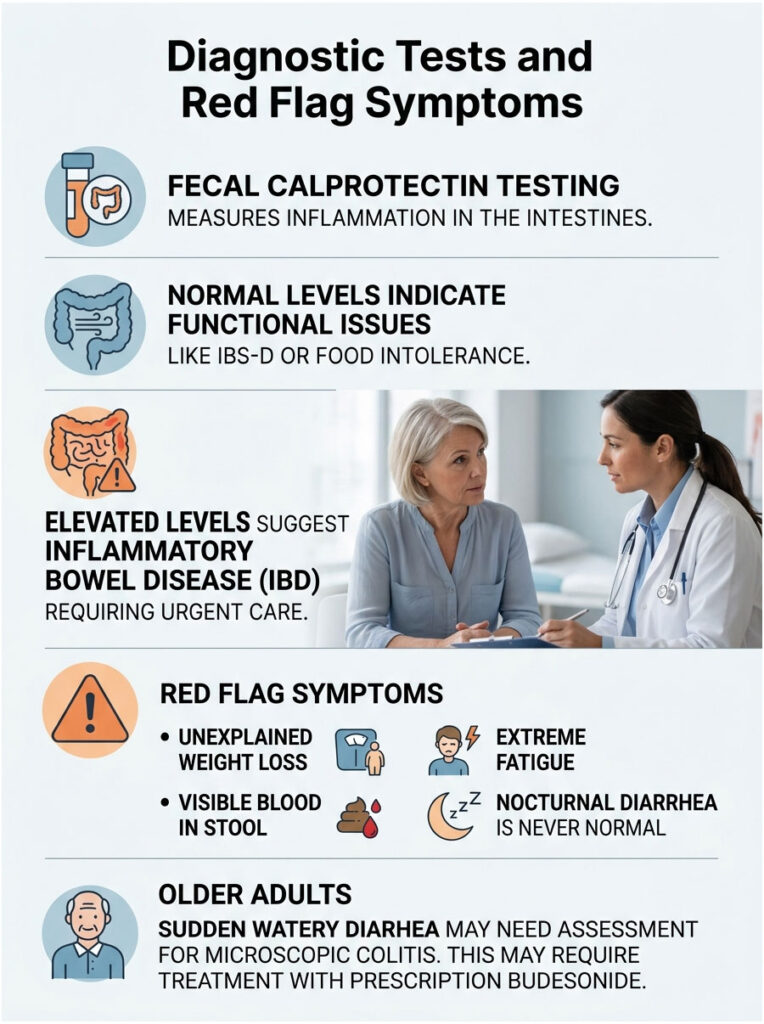
When to See a Gastroenterologist
Certain warning signs demand a doctor’s immediate attention. If you experience unexplained weight loss, visible blood in your stool, or extreme fatigue, contact a specialist right away. Nocturnal diarrhea, where you wake from sleep to use the restroom, is never a normal functional symptom.
For older adults with sudden onset of watery diarrhea, we need to evaluate for microscopic colitis. This condition causes chronic diarrhea from inflammation that is invisible during colonoscopy and can only be seen on biopsy. It often requires prescription budesonide to treat.
Real-World Clinical Examples
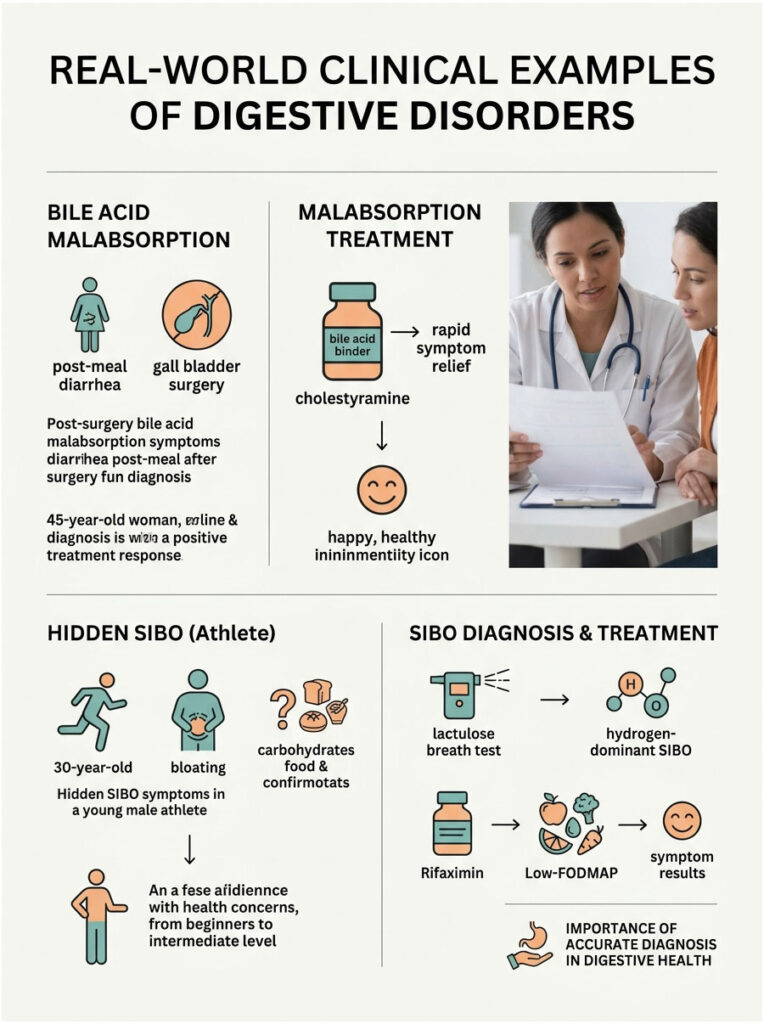
Post-Surgery Bile Acid Malabsorption
A 45-year-old woman who had her gallbladder removed two years earlier experienced explosive yellow diarrhea exactly twenty minutes after dinner. Previous doctors diagnosed IBS and told her to reduce stress. Her symptoms clearly indicated bile acid malabsorption from the missing gallbladder. We prescribed a daily bile acid binder (cholestyramine), and her postprandial diarrhea stopped almost overnight.
Hidden SIBO in a Young Athlete
A 30-year-old male athlete developed severe bloating and immediate diarrhea after eating carbohydrates. A strict gluten-free diet did not help. A lactulose breath test confirmed hydrogen-dominant SIBO. We treated him with a two-week course of Rifaximin followed by a temporary low-FODMAP diet. Within one month, his bloating and post-meal diarrhea were completely resolved.
Summary and Key Takeaways
Living in constant fear of your next meal is no way to live. Your symptoms are a direct physical response to a specific, identifiable trigger. Whether the problem is an overactive gastrocolic reflex, bile acid malabsorption, or a hyper-sensitive gut-brain axis, there is a clear, evidence-based path forward.
- Start with the 24-hour gut rest protocol using the BRAT diet and oral rehydration salts to calm acute inflammation.
- Keep a detailed symptom journal tracking the exact timing of flare-ups after meals.
- Add methylcellulose fiber to bulk stool and slow transit time without causing gas or bloating.
- Identify your root cause through proper diagnostic testing rather than accepting a generic IBS label.
- Seek professional help immediately if you develop red flag symptoms like blood in stool, weight loss, or nocturnal diarrhea.
Understanding how to ease stomach cramps and diarrhea after eating is entirely possible when you partner with the right medical professionals and listen to your body.
Frequently Asked Questions
How can I stop stomach cramps and diarrhea immediately after eating?
For immediate relief of postprandial symptoms, I recommend a 24-hour gut rest protocol using the BRAT diet (Bananas, Rice, Applesauce, Toast) to provide low-irritant binding fibers. You can also utilize over-the-counter loperamide to slow intestinal motility or enteric-coated peppermint oil, which acts as a natural calcium channel blocker to relax the smooth muscles of the gut and stop painful spasms.
Why do I feel the urgent need to use the bathroom within 30 minutes of eating?
This is typically caused by an exaggerated gastrocolic reflex. When food enters the stomach, it sends a neural signal to the colon to make room for the new meal. In patients with visceral hypersensitivity or IBS-D, this reflex becomes hyperactive, triggering violent contractions that force waste through the system before the colon can absorb excess water.
What does it mean if my post-meal diarrhea is yellow and causes a burning sensation?
Yellow, burning stools often indicate Bile Acid Malabsorption (BAM), also known as choleretic diarrhea. This occurs when the small intestine fails to reabsorb bile produced by the liver, causing it to spill into the colon. Because bile is highly acidic and acts as a natural laxative, it irritates the colon lining, leading to urgent, caustic bowel movements, especially after high-fat meals.
Can peppermint oil really help with severe intestinal cramping?
Yes, but it must be enteric-coated. The menthol in peppermint oil is a potent natural antispasmodic that blocks calcium channels in the gut’s smooth muscle, preventing them from contracting violently. The enteric coating ensures the oil bypasses the stomach and releases directly in the intestines where the cramping occurs, preventing heartburn while soothing the gastrocolic reflex.
Why would a gastroenterologist recommend fiber for someone struggling with diarrhea?
We specifically recommend non-fermentable soluble fiber, such as methylcellulose. Unlike other fibers, it does not produce gas through bacterial fermentation. Instead, it acts like a sponge, absorbing excess liquid in the digestive tract to add bulk and structure to the stool, which effectively slows down transit time and reduces the frequency of watery movements.
How do I know if my diarrhea is caused by Small Intestinal Bacterial Overgrowth (SIBO)?
SIBO typically presents with severe bloating and gas immediately following the consumption of complex carbohydrates or FODMAPs. Because bacteria have migrated into the small intestine, they ferment food prematurely, causing inflammation that amplifies the gastrocolic reflex. Diagnosis is usually confirmed through a lactulose breath test which measures hydrogen or methane gases.
What is the ‘Gut-Brain Axis’ and how does it affect my digestion after eating?
The gut-brain axis is the bidirectional communication line between your central nervous system and the enteric nervous system (the 500 million neurons in your gut). Stress or anxiety can trigger the ‘fight or flight’ response, which sends distress signals down the vagus nerve, causing the gut to dump its contents prematurely. This is why many patients see a direct correlation between psychological stress and postprandial urgency.
What are the signs that my diarrhea is caused by Pancreatic Insufficiency (EPI)?
Exocrine Pancreatic Insufficiency (EPI) causes a specific type of fat malabsorption called steatorrhea. If your stools are exceptionally foul-smelling, pale, greasy, or oily, and difficult to flush, it suggests your pancreas is not producing enough enzymes to break down fats. This condition requires medical intervention and is typically treated with Pancreatic Enzyme Replacement Therapy (PERT).
Is it safe to take Loperamide (Imodium) for every flare-up?
Loperamide is generally safe for managing functional diarrhea by binding to opioid receptors in the gut to slow peristalsis. However, it should only be used as a rescue medication. If you find yourself relying on it daily, it is crucial to investigate the underlying cause, such as BAM or SIBO, rather than just masking the symptoms of rapid motility.
How does the Low-FODMAP diet help reduce postprandial cramping?
The Low-FODMAP diet eliminates highly fermentable carbohydrates that draw water into the bowel (osmotic diarrhea) and provide a feast for gas-producing bacteria. By reducing the osmotic load and gas production, you decrease the physical stretching of the intestinal walls, which lowers the pain signals sent to your brain and calms the hyper-reactive gut lining.
What ‘red flag’ symptoms should prompt an immediate visit to a gastroenterologist?
You should seek professional medical evaluation immediately if you experience unexplained weight loss, visible blood in the stool (hematochezia), nocturnal diarrhea (waking up at night to go), or persistent fever. We also look for elevated fecal calprotectin levels, which indicate significant internal inflammation associated with Inflammatory Bowel Disease (IBD) rather than functional IBS.
Can I train my nervous system to reduce digestive urgency?
Yes, through vagal nerve stimulation. Techniques such as deep diaphragmatic breathing or meditation before meals can activate the parasympathetic ‘rest and digest’ system. This helps lower visceral hypersensitivity, making your enteric nervous system less likely to overreact to the physical expansion of the stomach, thereby dampening an overactive gastrocolic reflex.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. Postprandial diarrhea can be a symptom of serious underlying conditions. Always consult a qualified healthcare professional or gastroenterologist before starting new medications, supplements, or restrictive diets, especially if you experience “red flag” symptoms like weight loss or blood in the stool.
References
- American College of Gastroenterology (ACG) – gi.org – Clinical guidelines on the management and diagnostic criteria for Irritable Bowel Syndrome (IBS).
- Monash University – monashfodmap.com – Primary research and data regarding the efficacy of the Low-FODMAP diet for functional gut disorders.
- Rome Foundation – theromefoundation.org – The global standard for the Rome IV diagnostic criteria for functional gastrointestinal disorders.
- Journal of Clinical Gastroenterology – Lippincott Williams & Wilkins – Peer-reviewed studies on Bile Acid Malabsorption and its prevalence in chronic diarrhea patients.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – niddk.nih.gov – Official government data on the physiology of the gastrocolic reflex and dumping syndrome.
- American Gastroenterological Association (AGA) – gastro.org – Clinical practice updates on Small Intestinal Bacterial Overgrowth (SIBO) and fecal calprotectin testing.






