Patients ask me this question every single week. While persistent loose stools can sometimes point to an underlying malignancy, they are most commonly caused by benign conditions like IBS or dietary intolerances. That said, any change in bowel habits lasting longer than four weeks warrants a medical evaluation. When diarrhea pairs with red flags like unexplained weight loss or rectal bleeding, it becomes a serious oncology concern.
Table of Contents
Key Statistics on Gastrointestinal Health
- Over 153,000 new cases of colorectal cancer will be diagnosed in the USA this year, per the American Cancer Society.
- Early-onset colorectal cancer in adults under 50 has risen by 1% to 2% annually since the mid-1990s.
- Chronic diarrhea affects roughly 5% of the American population at any given time.
- Stage 1 colon cancer has a 5-year survival rate above 90% when caught early through proper screening.
- Only about 1% to 2% of chronic diarrhea cases are linked directly to gastrointestinal malignancies.
- The average human large intestine absorbs up to 1.5 liters of water daily to form solid stool.
- Routine colonoscopy screenings can reduce the risk of dying from colorectal cancer by more than 60%.
Every week in my gastroenterology clinic, patients come in with the same anxious question: is frequent diarrhea a sign of cancer? As a board-certified physician, I completely understand the fear that accompanies an unexpected change in bowel habits. You notice something is off, you start rushing to the bathroom more often, and eventually, worry takes over.
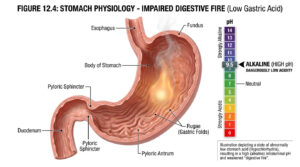
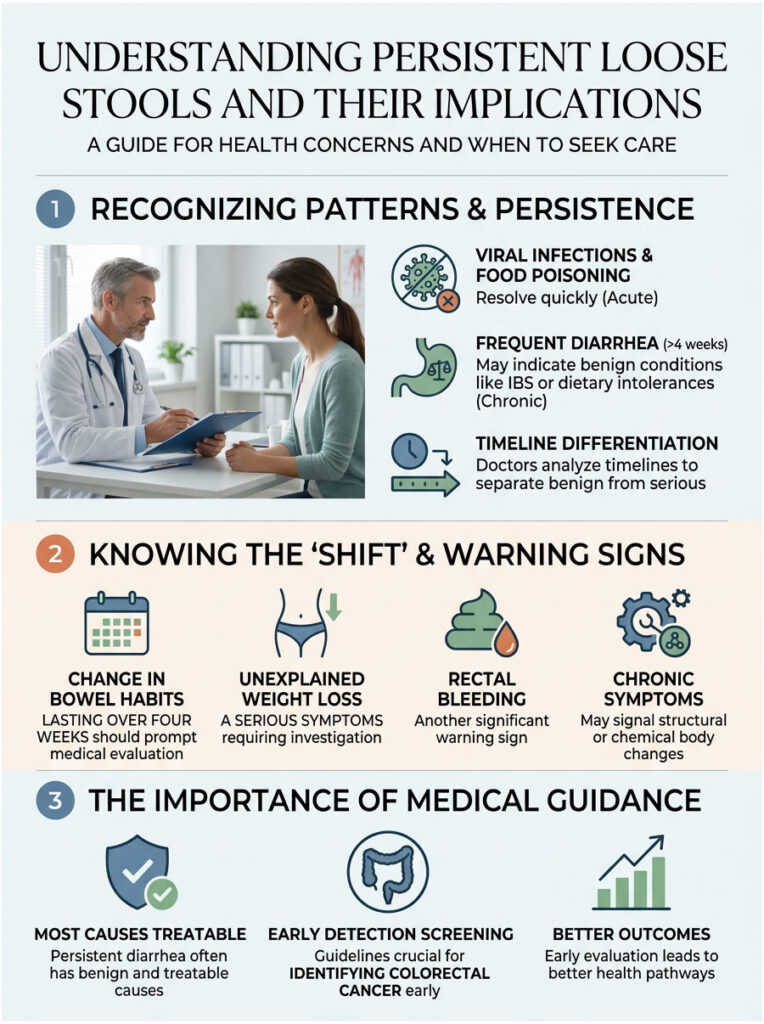
Here is what actually happens in a healthy digestive tract. Viral infections typically clear within a few days. Food poisoning resolves once the offending bacteria leaves your system. But persistent loose stools that drag on for weeks tell a very different story. Chronic symptoms signal a structural or chemical change inside your body that your immune system cannot fix on its own.
Most of the time, the root cause turns out to be completely benign and treatable. Occasionally, though, it points to a more serious medical reality that requires immediate attention.
In modern clinical medicine, we do not rely on guesswork. We look for specific, repeatable patterns in your digestive behavior. We analyze the exact timeline of your symptoms to build a clinical picture. We check for warning signs that separate a simple stomach bug from serious colorectal cancer symptoms.
My goal here is to give you clinical facts without the confusing medical jargon, to replace your late-night internet anxiety with actionable medical knowledge. In this guide, we will explore why tumors change how your bowels function, how doctors separate harmless functional conditions from dangerous organic diseases, and which early detection screening guidelines are saving lives right now.
Is Frequent Diarrhea a Sign of Cancer? The Clinical Reality
Not every digestive issue calls for a frantic emergency room visit at midnight. Your digestive system is highly sensitive to daily stress, new foods, and minor bacterial infections. But when does frequent diarrhea cross the line into dangerous territory? In gastroenterology, we follow strict diagnostic criteria to make this distinction.
Chronic vs. Acute Diarrhea: What Gastroenterologists Look For
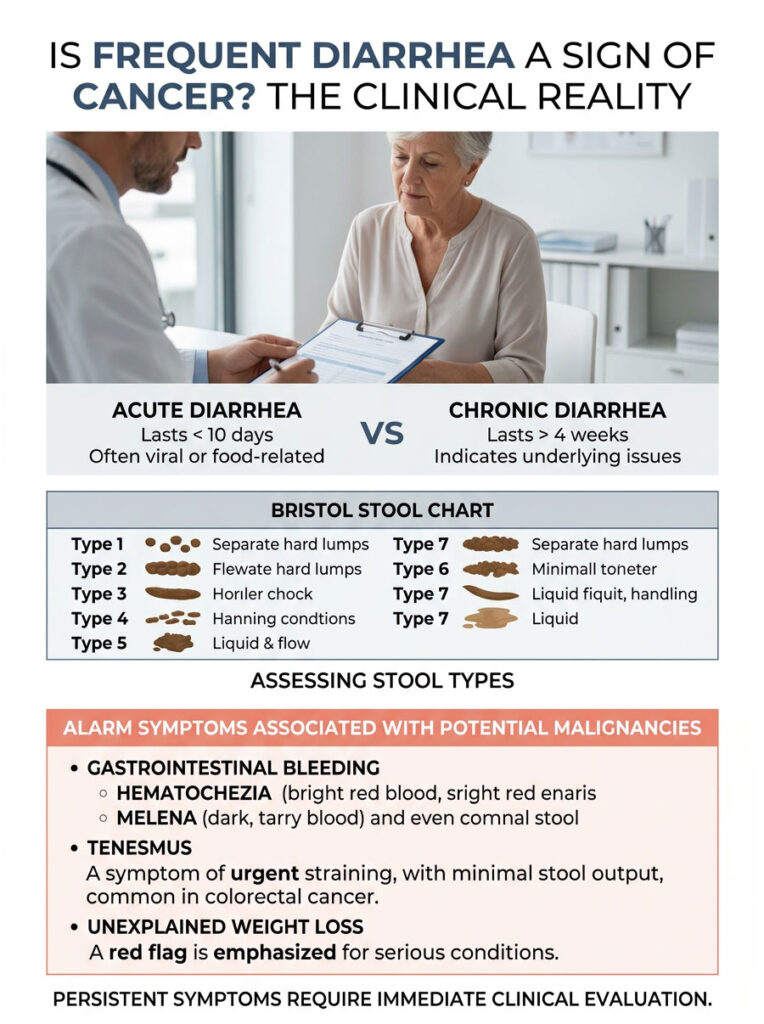
We classify diarrhea based on how long it lasts. Acute diarrhea strikes suddenly and usually comes from viral gastroenteritis or contaminated food. It almost always resolves within a week to ten days. Chronic diarrhea is a completely different clinical entity.
Medical guidelines officially define chronic diarrhea as lasting longer than four consecutive weeks. This timeline represents a clear bowel habit alteration that your body cannot resolve on its own. When symptoms persist that long, we look beyond simple infections and consider structural problems.
To measure severity accurately, doctors use a standardized visual tool called the Bristol Stool Chart. It categorizes stool into seven distinct types. Type 6 represents fluffy pieces with ragged edges, and Type 7 is entirely liquid. If you consistently experience Type 6 or 7 for a month, your large intestine is failing to absorb water properly. Is frequent diarrhea a sign of cancer in this specific scenario? It certainly can be, which is exactly why thorough testing matters.
The Constellation of Oncology Alarm Symptoms
Frequent diarrhea rarely acts alone when a malignancy is present. Tumors create a ripple effect that disrupts multiple biological systems at once. During your consultation, we actively look for a specific group of alarm symptoms. These clinical red flags tell us to dig deeper and order advanced imaging.
First, we look for signs of gastrointestinal bleeding. We carefully differentiate between hematochezia and melena, as they point to very different problems. Hematochezia is bright red, fresh blood in the toilet bowl or on the toilet paper, usually indicating active bleeding in the lower colon, rectum, or anus. Melena refers to dark, black, tarry stools caused by blood digesting as it travels from the upper gastrointestinal tract. Understanding the difference helps us pinpoint the exact location of a potential bleeding tumor.
Tenesmus is another major warning sign patients frequently describe. It is the constant, frustrating feeling that you need to pass stool, even when your bowels are completely empty. Tenesmus often occurs when a rectal mass physically mimics the sensation of waiting stool. It is one of the most common colorectal cancer symptoms we encounter in the clinic.
Unexplained weight loss is also highly concerning in any patient with bowel changes. If you drop ten pounds or more without changing your diet or exercise habits, your body is burning extra energy. Tumors demand massive amounts of calories to fuel their rapid, uncontrolled growth. At the same time, persistent loose stools prevent your intestines from absorbing essential nutrients. This combination leads to rapid weight loss, severe malnutrition, extreme fatigue, and frequently, iron-deficiency anemia.
How Malignancies Actually Alter Your Bowel Habits
How exactly does a tumor cause diarrhea? Many patients incorrectly assume a physical blockage would only cause constipation. In reality, the mechanics are more complex. Different types of tumors disrupt the bowel in completely different ways.
Expert Insight: Patients often ask me whether morning diarrhea specifically signals cancer. Morning urgency is commonly tied to functional issues like IBS. However, if the diarrhea wakes you from a deep sleep at 3:00 AM, that is a major clinical red flag pointing toward organic disease.
Malignant Bowel Obstruction and Overflow Diarrhea
A growing tumor acts like a physical roadblock inside your colon. As the mass enlarges, it creates a partial blockage in the intestinal tube, known as a malignant bowel obstruction. Solid waste cannot pass through the narrowed opening easily.
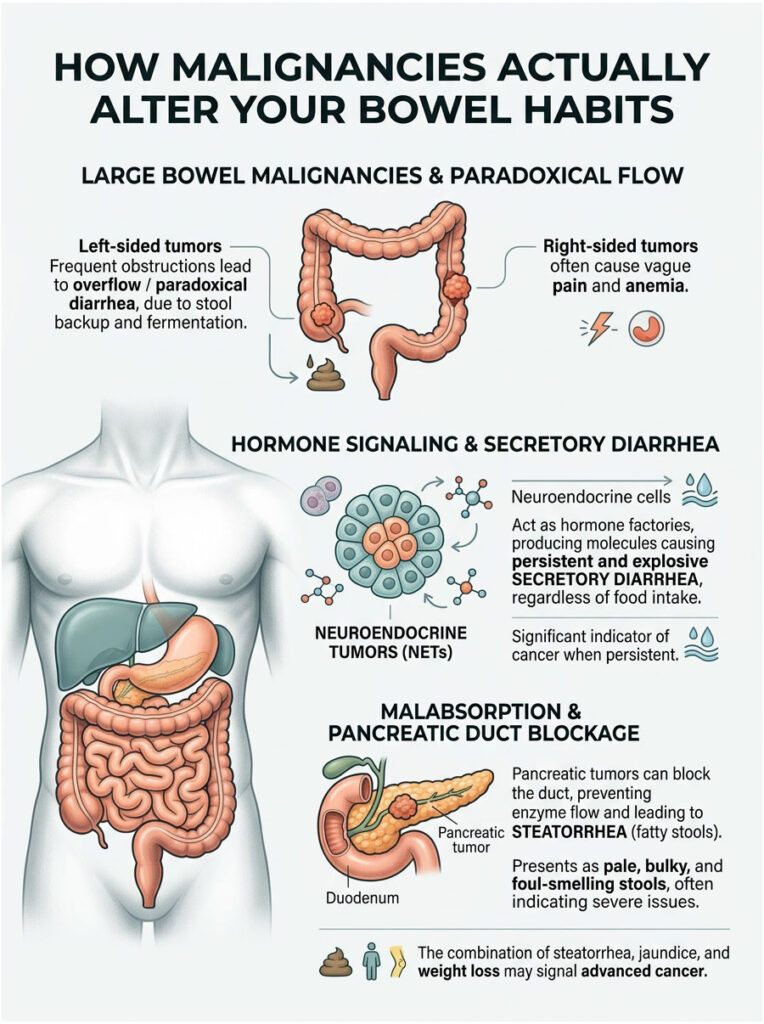
What happens next is counterintuitive. Hard stool gets stuck behind the tumor and begins to back up. Natural bacteria behind the blockage start fermenting the trapped stool. This fermentation draws excess water from your body into the colon cavity. The newly liquefied stool then seeps around the solid blockage and leaks out. We call this “overflow diarrhea” or paradoxical diarrhea. The patient experiences frequent watery stools, but they are actually severely constipated higher up. This is why over-the-counter anti-diarrheal medication can actually make things worse.
The tumor’s anatomical location drastically changes the symptoms you experience. We constantly compare left-sided versus right-sided colon cancer symptoms during diagnosis. The right side of the colon is wider, and stool is still liquid when it arrives there, so right-sided tumors usually cause vague pain and severe anemia rather than blockages. The left side is narrower, and stool has solidified by that point, making left-sided tumors much more likely to cause obstructions, pencil-thin stools, and overflow diarrhea.
Secretory Diarrhea and Neuroendocrine Tumors
Some cancers do not physically block the bowel at all. Instead, they act like rogue hormone factories. Neuroendocrine tumors (NETs) are rare, typically slow-growing malignancies that behave very differently from standard adenocarcinomas. They often develop silently in the stomach, small intestines, or pancreas.
NETs frequently trigger bizarre systemic reactions known as paraneoplastic syndromes. The tumor secretes massive, unnatural amounts of hormones like serotonin or vasoactive intestinal peptides directly into your bloodstream. These hormones force the intestinal lining to dump water and electrolytes into the bowel cavity, resulting in severe, explosive, seemingly unprovoked watery diarrhea. The fluid loss can quickly lead to life-threatening dehydration and kidney damage.
This mechanism directly answers the question: is frequent diarrhea a sign of cancer? Yes, especially when it presents as secretory diarrhea. What makes secretory diarrhea unique is that it does not stop even when you completely stop eating. The tumor keeps pumping out hormones regardless of your diet or fasting state.
Pancreatic Malignancies and Steatorrhea
Your pancreas is essential for digesting food properly. It produces powerful enzymes that break down fats, proteins, and carbohydrates. If a malignant tumor grows in the head of the pancreas, it can physically pinch the main pancreatic duct closed. When this happens, those crucial enzymes can no longer reach your small intestine.
Without these enzymes, your body simply cannot absorb dietary fat. The undigested fat travels straight through your system, causing a very specific symptom called steatorrhea. Steatorrhea produces stools that are noticeably pale, bulky, oily, and exceptionally foul-smelling. They often float stubbornly in the toilet and leave an oil slick in the water.
Seeing steatorrhea is a major red flag for any gastroenterologist. It points directly to severe pancreatic insufficiency and requires immediate imaging. If the patient also has metastatic liver disease, the bile ducts may be physically blocked as well, which prevents bile from reaching the intestines and further worsens the oily diarrhea. The combination of steatorrhea, jaundice, and rapid weight loss is a classic presentation of advanced hepatobiliary cancer.
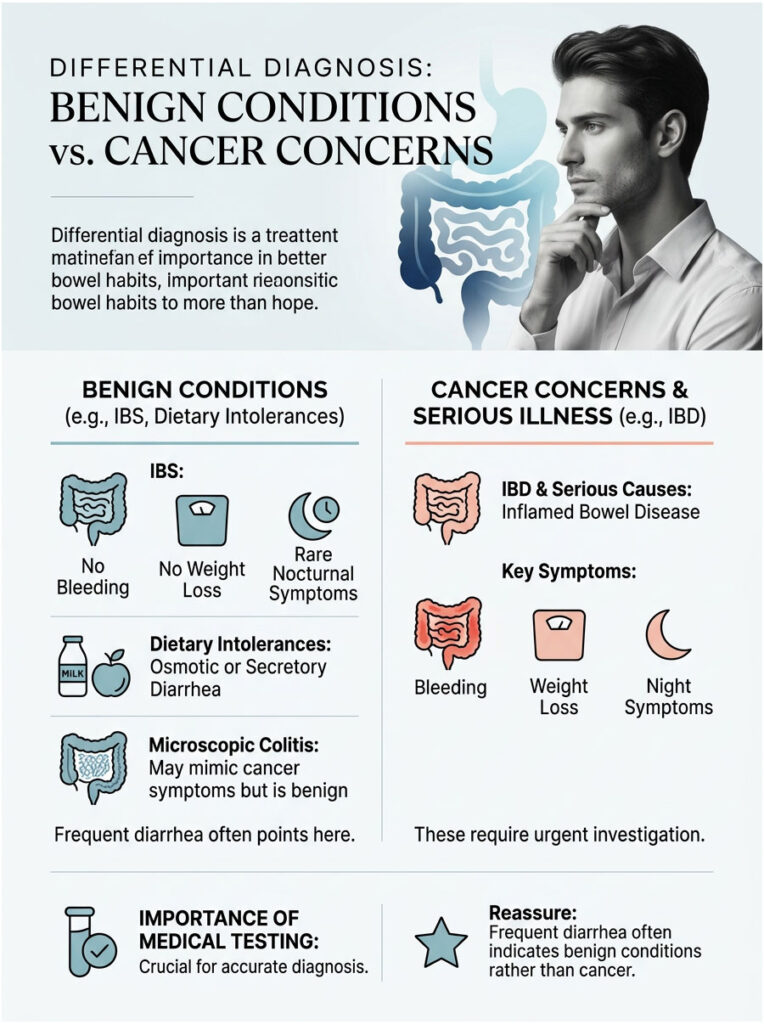
Differential Diagnosis: Benign Conditions vs. Cancer Concerns
When a patient presents with a severe bowel habit alteration, we must systematically rule out common problems first. This process is called a differential diagnosis. We carefully compare harmless functional disorders against potentially dangerous oncology concerns to make sure we do not miss a hidden malignancy.
Irritable Bowel Syndrome and Inflammatory Bowel Disease
Irritable Bowel Syndrome (IBS) is extremely common. It is a functional disorder, not an organic disease. The bowel looks completely normal during a scope, but the nerves and muscles overreact. IBS causes frequent diarrhea, usually triggered by stress, anxiety, or certain heavy meals. However, IBS almost never causes gastrointestinal bleeding or unexplained weight loss.
Inflammatory Bowel Disease (IBD) is a completely different and much more serious condition. It includes autoimmune diseases like Crohn’s disease and Ulcerative Colitis, where the immune system aggressively attacks healthy intestinal tissue. IBD causes severe chronic inflammation, deep bleeding ulcers, and persistent loose stools. Because of the bleeding and weight loss, IBD shares many classic colorectal cancer symptoms, making accurate endoscopic testing and tissue biopsies essential.
One major distinguishing factor we look for is nighttime symptom disruption. IBS rarely wakes a patient from sleep to use the bathroom. If you are consistently waking at 2:00 AM to rush to the toilet, we worry about IBD or malignancy.
Dietary Intolerances and Microscopic Colitis
Dietary issues are another common culprit for chronic bathroom trips. We often compare osmotic versus secretory diarrhea to narrow the cause. Osmotic diarrhea happens when you eat something your body cannot digest, like lactose or artificial sweeteners. The undigested particles pull excess water into the bowel through osmosis.
Differentiating between the two is surprisingly straightforward. If you stop eating the trigger food and the diarrhea stops, it is osmotic and likely benign. If you fast for 24 hours and the diarrhea persists, it is secretory and requires immediate medical attention.
Older adults often develop a frustrating condition called microscopic colitis. It causes chronic, watery, explosive diarrhea. During a standard colonoscopy, the tissue looks perfectly healthy to the naked eye. But under a high-powered microscope, we see a thick, abnormal layer of inflammatory white blood cells. Microscopic colitis mimics cancer symptoms almost perfectly, causing tremendous anxiety. Fortunately, it is highly treatable with specific prescription medications like budesonide.
So, is frequent diarrhea a sign of cancer in every case? It can be, but conditions like IBS, IBD, and microscopic colitis are statistically far more common. That said, we never gamble with your life. We test to be absolutely sure.
| Clinical Feature | Benign Conditions (IBS / Intolerances) | Malignancy-Related Diarrhea |
| Duration and Onset | Long-term, fluctuating over many years | Recent, progressive, unyielding change |
| Nocturnal Symptoms | Extremely rare; sleep stays uninterrupted | Common; patient wakes specifically to evacuate |
| Response to Fasting | Improves significantly when not eating | Persists regardless of food intake |
| Stool Appearance | Variable consistency, normal color, no blood | Pencil-thin, bloody, or oily (steatorrhea) |
| Systemic Symptoms | Mild fatigue linked to poor sleep or stress | Unexplained weight loss, anemia, low-grade fever |
The 45 Rule and Shifting Demographics in Oncology
The demographics of gastrointestinal cancers are changing rapidly. Decades ago, colon cancer was viewed strictly as an older person’s disease. That assumption no longer holds true.
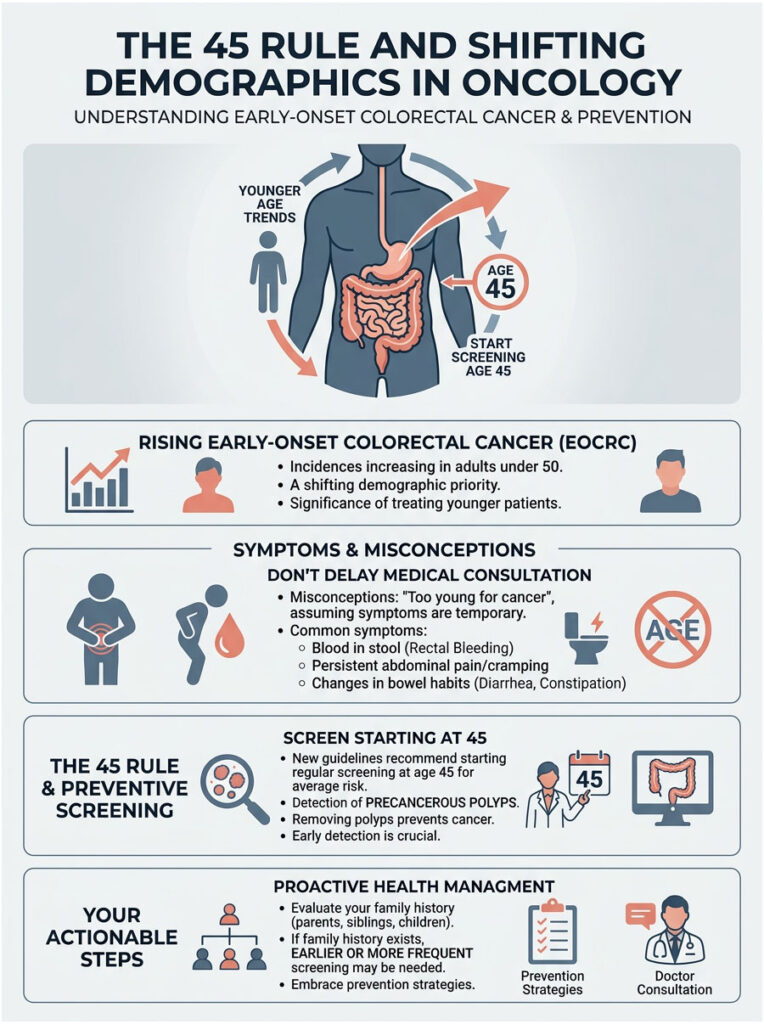
Rising Rates of Early-Onset Colorectal Cancer
Recent research from the American Cancer Society reveals a deeply concerning trend. Colorectal cancer rates in adults under 50 are climbing every year. We refer to this as early-onset colorectal cancer. Young, seemingly healthy adults in their thirties and forties are presenting with advanced stages of the disease.
Scientists are studying environmental factors, highly processed diets, and changes in the gut microbiome. Because younger adults do not expect to get cancer, they often ignore a clear bowel habit alteration. They assume the diarrhea is just stress, anxiety, or bad food. This dangerous delay in seeking help can be fatal. By the time a young person finally visits a gastroenterologist, the tumor has often grown significantly, and tumors in younger patients tend to be biologically more aggressive.
Understanding Modern Screening Guidelines
Because of these shifting trends, national medical guidelines had to change. The United States Preventive Services Task Force officially lowered the recommended screening age from 50 to 45 for all average-risk adults. This early detection screening 45 Rule is a genuine game-changer in preventative medicine. It allows doctors to find and remove precancerous polyps before they turn into a full-blown malignancy.
A polyp is simply a small clump of cells that forms on the colon lining. Most polyps are harmless, but over time some can mutate into cancer. If you have a family history of colon cancer, you should start screening even earlier, generally ten years before the age your family member was diagnosed.
Do not wait until you actively experience severe colorectal cancer symptoms. Prevention is always the best strategy. If you are 45 or older and constantly wondering whether your diarrhea might be cancer-related, schedule a screening immediately. The early detection screening 45 Rule exists to save lives.
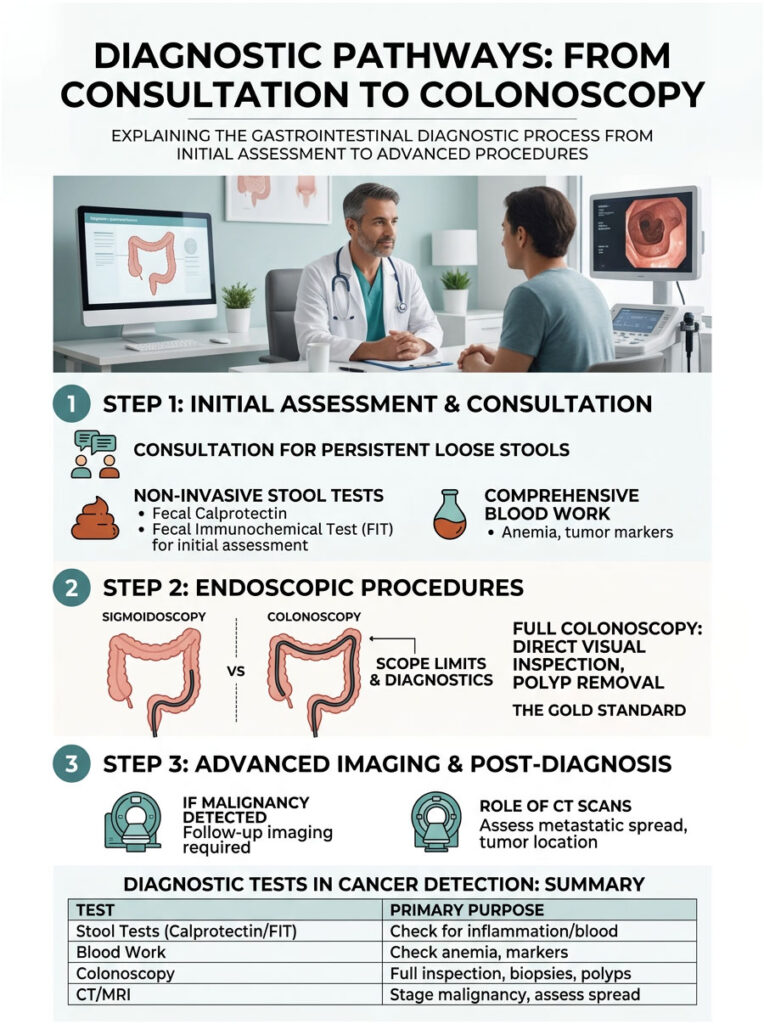
Diagnostic Pathways: From Consultation to Colonoscopy
When you visit a gastroenterologist for persistent loose stools, we follow a structured, evidence-based diagnostic pathway. We start with simple, non-invasive tests to gather basic data. If warning signs appear, we move quickly to direct visual inspection.
Non-Invasive Stool and Blood Tests
Your doctor will likely hand you specimen cups during your first visit. Stool tests provide an incredible amount of information about your internal digestive health. We frequently test for a biomarker called fecal calprotectin, a protein released by white blood cells during active intestinal inflammation. High levels help us rule out IBS and point toward IBD or other inflammatory conditions.
We also rely heavily on the Fecal Immunochemical Test (FIT), which looks specifically for hidden, microscopic blood in your stool. Tumors and large polyps bleed easily as hard stool scrapes past them. A positive FIT result demands immediate, urgent further testing.
Comprehensive blood work is equally essential. We check your complete blood count for signs of iron-deficiency anemia. We may also run Carcinoembryonic Antigen (CEA) testing, which measures a specific tumor marker in your bloodstream. However, CEA is primarily useful for monitoring patients who already have a confirmed cancer diagnosis. Many early-stage cancers do not elevate CEA levels, so it is not a reliable primary screening tool.
Endoscopic Evaluation: Looking Inside
If your symptoms or lab results raise concern, we must look directly inside the colon. We often compare sigmoidoscopy versus colonoscopy when planning care. A sigmoidoscopy uses a flexible tube to examine only the lower third of the colon and rectum. It is faster, but it completely misses right-sided tumors.
A full colonoscopy is universally considered the gold standard. You are comfortably sedated while we examine the entire length of the large intestine using a high-definition camera. If we find a suspicious polyp, we remove it on the spot. If we see a large, concerning mass, we take multiple tissue biopsies for the pathology lab. For chronic diarrhea, the full colonoscopy is vastly superior because it visualizes the entire organ and provides definitive answers in a single visit.
Advanced Imaging Techniques
If a malignancy is found during the colonoscopy, we urgently need to know whether the cancer has spread beyond the colon wall. We order high-resolution CT scans of the abdomen, pelvis, and chest. These scans help detect a malignant bowel obstruction from outside the organ and allow us to check the liver and lungs for tumor deposits.
We are specifically looking for signs of metastatic liver disease, which drastically alters both the prognosis and the treatment plan. MRI may also be used for a detailed cross-sectional view of pelvic tumors, which is particularly crucial in rectal cancer cases to determine how deeply the tumor has invaded surrounding tissue.
| Diagnostic Test | Primary Purpose | Cancer Detection Value |
| Fecal Immunochemical Test (FIT) | Detects hidden blood in stool | High. Blood signals large polyps or bleeding tumors. |
| Fecal Calprotectin | Measures intestinal inflammation | Low for cancer directly, but rules out IBD effectively. |
| Blood Panel (CBC and Iron) | Checks for anemia and infection | High. Unexplained iron deficiency points to chronic GI bleeding. |
| Full Colonoscopy | Direct visual inspection of entire colon | Gold standard. Allows polyp removal and tissue biopsy. |
| CT Scan (Abdomen/Pelvis) | Cross-sectional imaging of organs | Essential for obstruction or distant metastatic spread. |
The Gut Microbiome’s Role in Cancer and Diarrhea
Modern gastroenterology is experiencing a revolution in how we view the human digestive tract. We are no longer focused only on the physical tissue. We now analyze the trillions of microscopic bacteria living inside your gut. This complex ecosystem, known as the gut microbiome, plays a significant role in your daily health.
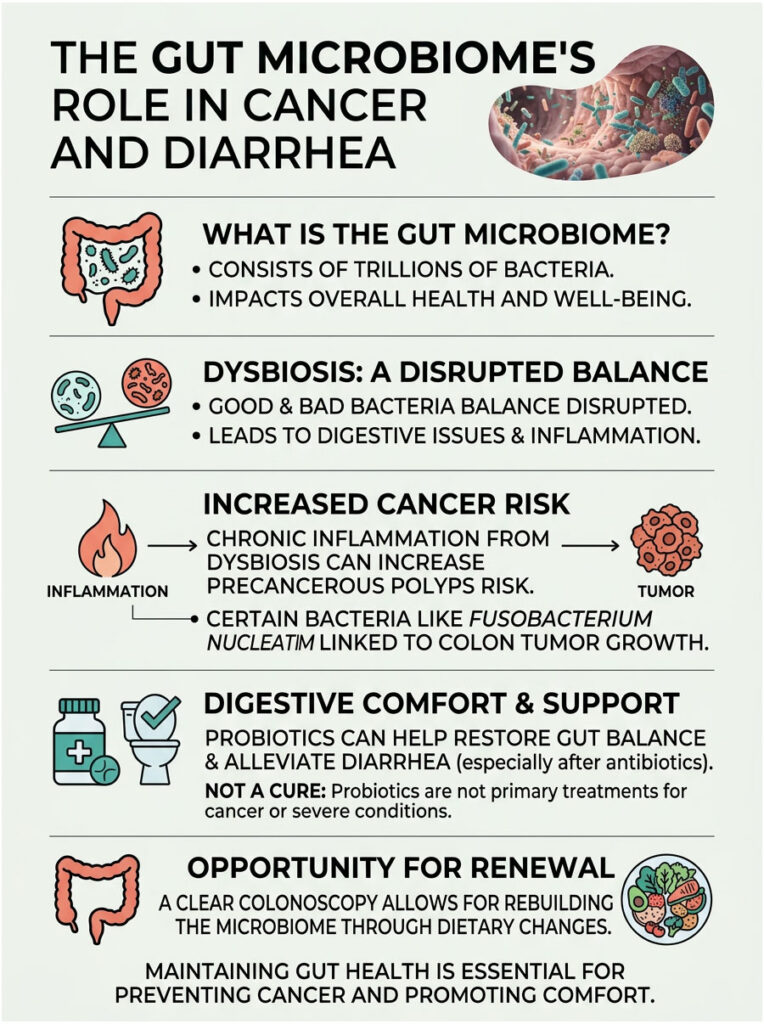
Dysbiosis and Chronic Inflammation
When your gut microbiome is balanced, good bacteria help digest food and protect your intestinal lining. But poor diet, chronic stress, and frequent antibiotic use can destroy this balance, creating a state called dysbiosis. Dysbiosis is a major underlying cause of persistent loose stools and chronic digestive discomfort.
Here is what makes this particularly concerning. Severe dysbiosis creates a constant state of low-grade inflammation in your colon. Bad bacteria produce toxic byproducts that irritate the mucosal lining. Over many years, this chronic inflammation can cause cellular DNA damage, significantly increasing your risk of developing precancerous polyps.
Certain bacterial strains, like Fusobacterium nucleatum, are frequently found in large quantities inside colon tumors. Researchers believe these bacteria may help tumors grow and hide from your immune system. This bacterial connection underscores why maintaining gut health is so important for cancer prevention.
Probiotics and Restoring Gut Harmony
Many patients ask whether daily probiotics will cure their diarrhea or prevent cancer. Probiotics are supplements containing live, beneficial bacteria designed to repopulate the gut microbiome. While not a cure-all, they can be effective for specific types of benign diarrhea, particularly diarrhea caused by a recent course of antibiotics.
However, probiotics cannot shrink a tumor or clear a malignant bowel obstruction. If organic disease is present, adding good bacteria will not solve the underlying mechanical issue. A proper medical evaluation must come first.
If your colonoscopy comes back clear, we may then focus on rebuilding the microbiome with targeted probiotics, prebiotics, and dietary changes. A healthy microbiome ensures proper water absorption, which naturally firms up bowel movements.
Nutritional Interventions and Preventive Care
What you eat every day directly impacts your risk of developing gastrointestinal malignancies. Diet is one of the most powerful, controllable factors in oncology prevention.

The Protective Power of Dietary Fiber
Dietary fiber is essential for maintaining a healthy, cancer-free colon. Fiber adds bulk to your stool, diluting potential carcinogens in the digestive tract. It also speeds up transit time, meaning toxic waste spends less time in contact with your colon walls. Unfortunately, the standard American diet is shockingly deficient in natural fiber.
When you eat high-fiber foods like beans, oats, and leafy greens, gut bacteria ferment them. This process produces short-chain fatty acids, specifically butyrate. Butyrate is the primary energy source for colon cells and has powerful anti-inflammatory properties. It actively helps prevent healthy cells from mutating into cancerous ones.
If you are suffering from frequent diarrhea, you might assume fiber would make things worse. Surprisingly, soluble fiber can absorb excess water in the colon and add form to loose stools. Foods like bananas, rice, applesauce, and toast are excellent sources of soothing soluble fiber.
The Danger of Ultra-Processed Foods
On the other hand, consuming high amounts of ultra-processed foods significantly raises your colon cancer risk. Processed meats like hot dogs, bacon, and deli meats are classified as Group 1 carcinogens by the World Health Organization. They contain chemical preservatives called nitrates and nitrites which, when cooked at high temperatures, form compounds called nitrosamines that severely damage intestinal DNA.
To protect your digestive health, I strongly recommend a Mediterranean-style diet. Focus on lean proteins, healthy fats like olive oil, and an abundance of fresh, colorful vegetables. Changing your diet drastically improves bowel habits and lowers long-term cancer risk.
The Psychological Impact of Chronic Bowel Changes
We cannot discuss chronic diarrhea without addressing the psychological toll it takes. Your brain and gut are deeply connected through a network of nerves called the gut-brain axis. When your gut is sick, your mental health almost always suffers. The anxiety around bathroom access can completely destroy quality of life.
Health Anxiety and the Somatic Symptom Cycle
When a patient constantly worries about whether their diarrhea is cancer-related, anxiety levels skyrocket. This triggers the fight-or-flight response, releasing stress hormones like cortisol and adrenaline. These hormones speed up the digestive tract, making the diarrhea even worse.
This creates a self-reinforcing cycle. You worry about your bowels, the worry causes diarrhea, and the diarrhea causes more worry. Breaking this cycle is incredibly difficult without professional reassurance. Getting a colonoscopy is often a deeply therapeutic experience for anxious patients. Once they see clear images of their healthy colon, the anxiety often vanishes, and stress-induced diarrhea frequently resolves within days of receiving good news.
Coping Strategies for Daily Life
If you are waiting for your gastroenterology appointment, here are practical ways to manage daily life. Practice deep diaphragmatic breathing to calm your overactive nervous system. Map out bathroom locations whenever you leave the house to reduce panic about accidents. Carrying a small emergency kit with wipes and spare clothing provides real psychological comfort.
Most importantly, avoid late-night internet searching about your symptoms. Search engines are notoriously poor at diagnosing complex gastrointestinal issues and almost always suggest the worst-case scenario. Trust the medical process, track your symptoms objectively, and rely on your board-certified physician for answers.
Actionable Strategies Before Your Doctor Visit
If you are currently struggling with persistent loose stools, you play a vital, active role in your own diagnosis. Doctors rely heavily on the information you provide during your initial consultation. Preparing properly can speed up the process significantly.
Documenting Your Symptoms Accurately
Human memory is unreliable, especially under stress. Do not guess how often you are using the bathroom. Keep a detailed, written two-week bowel diary before your appointment. Record the exact time of every bowel movement. Use the Bristol Stool Chart to rate consistency. Note whether you see Type 6 or 7 regularly. Document any visible blood, noting the visual difference between bright red hematochezia and dark melena. Record abdominal pain and whether it improves after passing stool.
This diary gives your gastroenterologist a clear, objective view of your bowel habit alteration. It removes guesswork and lets us see exactly what your body is doing over time. This data is invaluable for building an accurate differential diagnosis.
Preparing for Your Consultation
When you arrive at the clinic, be ready to answer detailed, sometimes uncomfortable questions. Bring a typed list of all your current medications and supplements. Many common drugs, including blood pressure medications and antibiotics, cause diarrhea as a known side effect.
Know your family’s medical history thoroughly. Find out if parents, siblings, or grandparents ever had colon polyps or gastrointestinal cancers. Bring a timeline of your body weight over the past six to twelve months. Unexplained weight loss is a critical piece of the puzzle.
Write your specific questions on paper so you do not forget them. Be completely honest about alcohol and smoking habits, as both heavily impact gut health. The more accurate your information, the faster we can give you a definitive answer.
Summary and Key Takeaways
Is frequent diarrhea a sign of cancer? It certainly can be, but it is rarely the only symptom present. A sudden, persistent bowel habit alteration lasting more than four weeks is a valid medical warning sign that demands attention.
When persistent loose stools are paired with alarm symptoms like rectal bleeding, unexplained weight loss, or nocturnal waking, immediate investigation is required. Remember that the vast majority of chronic diarrhea cases stem from benign, treatable conditions. IBS, dietary intolerances, and microscopic colitis are statistically far more likely than malignancies.
However, the rising rates of early-onset colorectal cancer in young adults cannot be ignored. Adhere strictly to the early detection screening 45 Rule to protect your long-term health. Do not let fear, embarrassment, or anxiety stop you from seeking the medical answers you deserve.
Modern diagnostic tools, from fecal calprotectin tests to high-definition colonoscopies, are safe and effective. If you are experiencing severe colorectal cancer symptoms or unexplained frequent diarrhea, take action. Schedule a comprehensive consultation with a board-certified gastroenterologist today, because early detection truly saves lives.
Frequently Asked Questions
At what point does frequent diarrhea become a clinical concern for cancer?
In gastroenterology, we classify diarrhea as chronic once it persists for longer than four consecutive weeks. While most cases are benign, a bowel habit alteration of this duration suggests a structural or chemical change that your body cannot resolve independently. If your stool consistently matches Bristol Stool Chart Type 6 or 7 for a month, it requires a thorough medical evaluation to rule out gastrointestinal malignancies.
What are the primary ‘alarm symptoms’ that suggest diarrhea is related to oncology?
We look for a specific constellation of red flags: unexplained weight loss (10+ pounds without effort), rectal bleeding, severe iron-deficiency anemia, and nocturnal symptoms that wake you from sleep. When these occur alongside persistent loose stools, they significantly increase the clinical suspicion of a malignancy like colorectal or pancreatic cancer.
How can a tumor cause ‘overflow diarrhea’ if it is physically blocking the colon?
A Malignant Bowel Obstruction acts as a physical roadblock. While solid waste cannot pass, bacteria behind the blockage ferment the trapped stool, drawing excess water into the colon. This newly liquefied stool seeps around the tumor, resulting in ‘overflow’ or paradoxical diarrhea. Patients often feel severely constipated even though they are passing watery stools.
What is the difference between Hematochezia and Melena in stool samples?
These terms describe the location of gastrointestinal bleeding. Hematochezia is bright red blood, typically indicating a source in the lower colon or rectum. Melena refers to dark, black, tarry stools caused by blood being digested as it travels from the upper GI tract. Both are critical markers that help us locate a potential tumor during diagnostic imaging.
How do doctors distinguish between Irritable Bowel Syndrome (IBS) and cancer?
IBS is a functional disorder, meaning the tissue looks healthy but the nerves overreact; it rarely causes weight loss or bleeding. Cancer is an organic disease involving structural changes. A key differentiator is nocturnal urgency: IBS almost never wakes a patient from a sound sleep, whereas malignancy-related diarrhea often occurs at night.
What is ‘Steatorrhea’ and why does it point toward pancreatic issues?
Steatorrhea is a specific type of diarrhea where stools appear pale, oily, and exceptionally foul-smelling. This happens when a tumor in the pancreas blocks digestive enzymes from reaching the small intestine, preventing the absorption of dietary fats. The undigested fat passes through the system, often leaving an oil slick in the toilet water.
What is the ’45 Rule’ in modern colorectal cancer screening?
The 45 Rule refers to the updated clinical guidelines from the USPSTF and American Cancer Society, which lowered the recommended starting age for colon cancer screenings from 50 to 45. This shift addresses the alarming rise in early-onset colorectal cancer among younger adults who may otherwise ignore persistent bowel changes.
How does ‘Secretory Diarrhea’ help identify Neuroendocrine Tumors (NETs)?
Secretory diarrhea is unique because it persists even if the patient stops eating (fasting). Neuroendocrine Tumors act as rogue hormone factories, secreting peptides that force the intestinal lining to dump water and electrolytes into the bowel. Unlike osmotic diarrhea caused by food intolerances, secretory diarrhea remains violent regardless of dietary intake.
Why is a full colonoscopy preferred over a sigmoidoscopy for diagnosing diarrhea?
A sigmoidoscopy only visualizes the rectum and the lower third of the colon, potentially missing right-sided tumors. A full colonoscopy is the gold standard because it allows for high-definition inspection of the entire large intestine, enabling the immediate removal of precancerous polyps and the collection of tissue biopsies.
What does a positive Fecal Immunochemical Test (FIT) indicate?
A FIT test detects hidden (occult) human blood in the stool that isn’t visible to the naked eye. Because tumors and large polyps are fragile and bleed easily when stool passes by, a positive FIT is a significant clinical indicator that requires an urgent follow-up colonoscopy to identify the source of the bleeding.
What is ‘Tenesmus’ and how does it relate to rectal cancer?
Tenesmus is the distressing and constant feeling that you need to evacuate your bowels even when they are empty. In oncology cases, a rectal mass can physically mimic the sensation of stool being present, tricking the nervous system into a state of perpetual urgency. It is one of the most common symptoms reported by patients with lower GI malignancies.
Does the location of a tumor change the symptoms of diarrhea?
Yes. Left-sided tumors occur in a narrower part of the colon where stool is solid, making them more likely to cause obstructions and ‘pencil-thin’ stools. Right-sided tumors occur where the colon is wider and stool is still liquid; these often grow much larger before causing symptoms, typically presenting as vague abdominal pain and severe anemia rather than obvious blockages.
Disclaimer
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Frequent diarrhea can be caused by many conditions; however, persistent symptoms should always be evaluated by a board-certified physician. Always consult a qualified healthcare professional before making health decisions or ignoring potential colorectal cancer symptoms.
References
- American Cancer Society – cancer.org – Provides comprehensive statistics on colorectal cancer incidence and early-onset trends in the USA.
- U.S. Preventive Services Task Force (USPSTF) – uspreventiveservicestaskforce.org – Official source for the updated “45 Rule” screening guidelines for colorectal cancer.
- American Gastroenterological Association (AGA) – gastro.org – Clinical practice updates on the evaluation of chronic diarrhea and functional bowel disorders.
- Centers for Disease Control and Prevention (CDC) – cdc.gov – Data on colorectal cancer prevention, screening rates, and public health initiatives.
- World Health Organization (WHO) – who.int – Research and monographs regarding the carcinogenic risks of processed meats and dietary factors in GI health.
- Bristol Stool Chart – University of Bristol – The standardized clinical tool used to categorize stool consistency and transit time.