Every week in my gastroenterology clinic, patients walk in carrying bottles of antacids. They tell me about the bloating, the trapped gas, the fatigue that never seems to lift. And almost every time, they assume they have too much acid. But here is the thing most people get wrong: their symptoms are not caused by excess acid. They are caused by not having enough.
Table of Contents
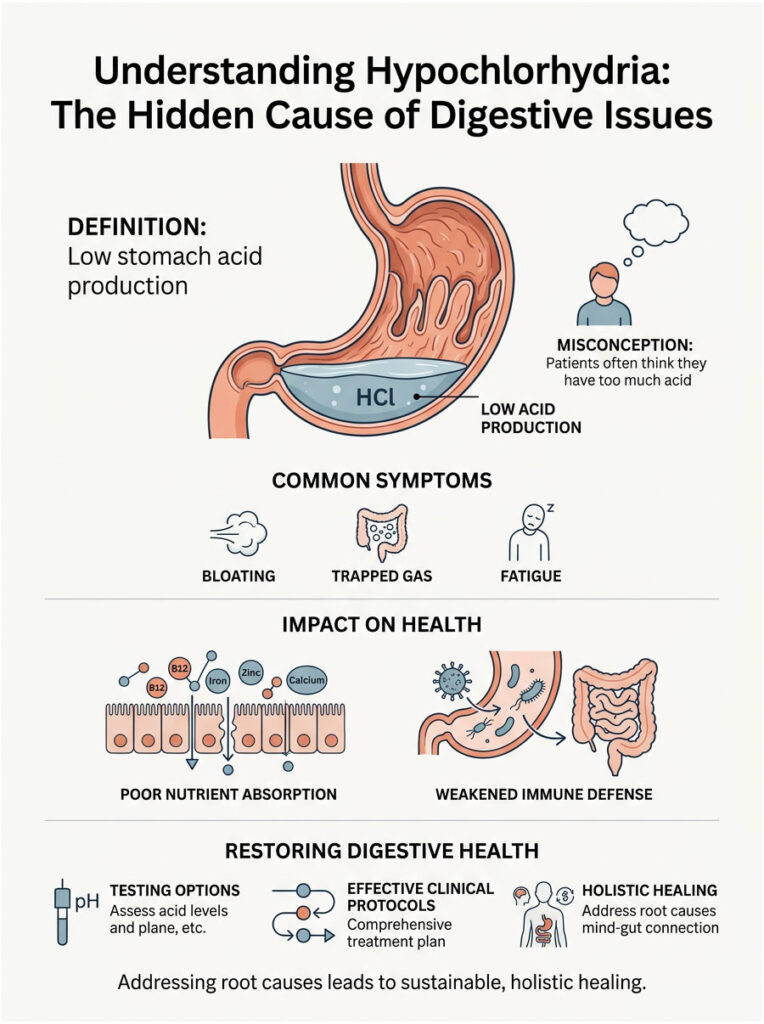
This condition is called hypochlorhydria. It means your parietal cells are not producing enough hydrochloric acid to properly digest your food. When this happens, nutrient absorption tanks, your immune defense weakens, and a chain reaction of health problems follows.
In this guide, I am going to walk you through the real physiology behind low stomach acid symptoms, the hidden root causes, the testing options, and the clinical protocols that actually work. This is not about masking discomfort with another pill. It is about restoring your digestive system from the ground up.
Quick Answer: What You Need to Know
Low stomach acid symptoms show up when the stomach cannot produce enough hydrochloric acid, a condition doctors call hypochlorhydria. Instead of breaking food down, a low-acid stomach lets it sit and ferment. This leads to bloating, reflux, and poor nutrient absorption. Common triggers include chronic stress, H. pylori infection, and long-term use of acid-blocking medications. Recovery involves proper testing, identifying the root cause, and carefully restoring healthy gastric pH levels.
Key Clinical Statistics Worth Knowing
| Factor | What the Data Shows |
| Age Factor | Up to 30% of adults over 60 have naturally reduced gastric acid output. |
| Medication Impact | More than 15 million Americans take Proton Pump Inhibitors (PPIs), raising their risk of acid deficiency. |
| Infection Rates | H. pylori, a major cause of acid suppression, infects roughly 35% of the U.S. population. |
| Bone Health | Long-term acid suppression raises hip fracture risk by up to 44% due to calcium malabsorption. |
| Bacterial Overgrowth | About 78% of patients with chronic low acid eventually develop SIBO. |
| Nutrient Deficits | Nearly 40% of low-acid patients show clinical B12 deficiency within two years. |
How Stomach Acid Production Actually Works
Before we can fix the problem, we need to understand what a healthy stomach does. Your stomach is essentially a chemical processing plant. When it works right, it sterilizes everything you eat and breaks complex proteins into usable amino acids.
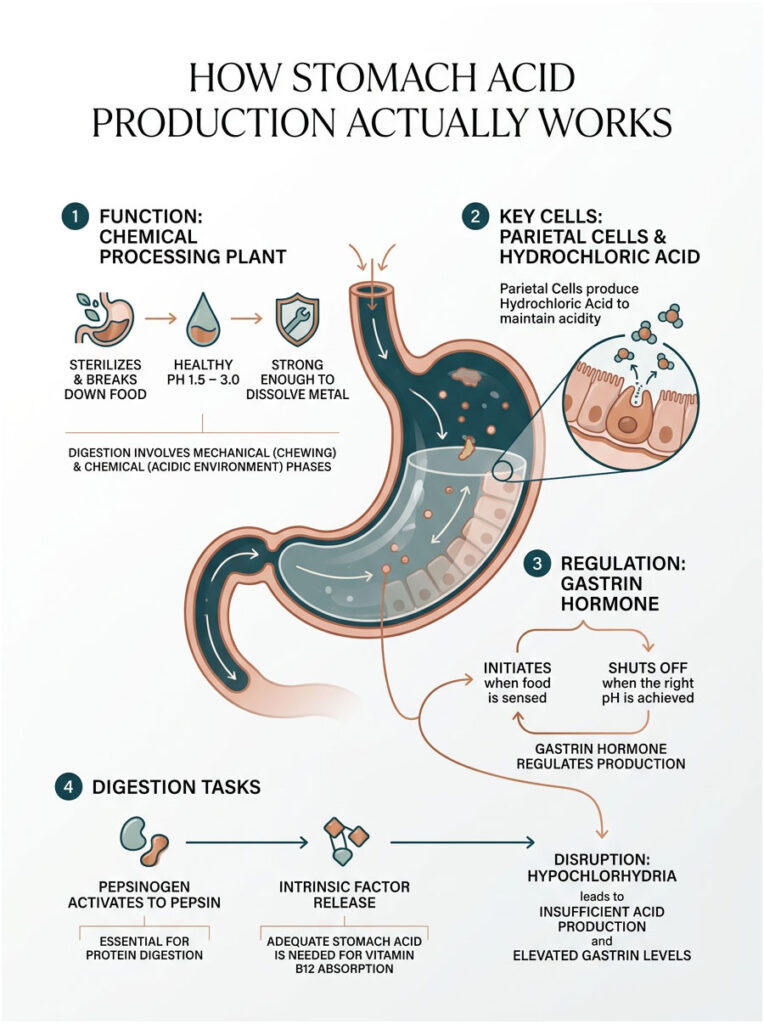
In a healthy person, the stomach maintains a pH between 1.5 and 3.0. That is incredibly acidic, strong enough to dissolve a small piece of metal over a few days. Your stomach lining is packed with millions of tiny structures called parietal cells, and their sole job is pumping hydrochloric acid into the gastric chamber.
Parietal Cells and the Gastrin Feedback Loop
This acid production is regulated by a hormone called gastrin. When your stomach senses food, it releases gastrin to signal the parietal cells to ramp up acid output. Once the stomach reaches the right acidity, gastrin release shuts off automatically. It is a tightly controlled feedback loop.
Here is where it breaks down: if you have hypochlorhydria, your stomach never hits that target pH. Your body panics. It keeps pumping out more gastrin, trying to force the parietal cells to produce acid they cannot deliver. That is why we often see elevated serum gastrin levels in patients with chronic acid deficiencies. High gastrin on a blood test usually means the stomach is too alkaline and the body is desperately calling for more acid.
Chemical vs. Mechanical Digestion
Digestion happens in two phases. Mechanical digestion starts in your mouth when you chew food into smaller pieces. Chemical digestion kicks in the moment food hits the stomach. The highly acidic environment converts an inactive enzyme called pepsinogen into its active form, pepsin, which acts like chemical scissors for protein molecules.
Without enough acid, pepsinogen never activates. Your dietary protein just sits there and ferments. On top of that, adequate acid is required to release Intrinsic Factor, a binding protein you need for Vitamin B12 absorption. No acid means no B12, and that is where serious problems begin.
Recognizing Low Stomach Acid Symptoms in Everyday Life
Most people confuse low acid with high acid because the symptoms feel similar on the surface. But the timing and nature of the discomfort tell a completely different story. Catching these signs early can save you years of frustration.
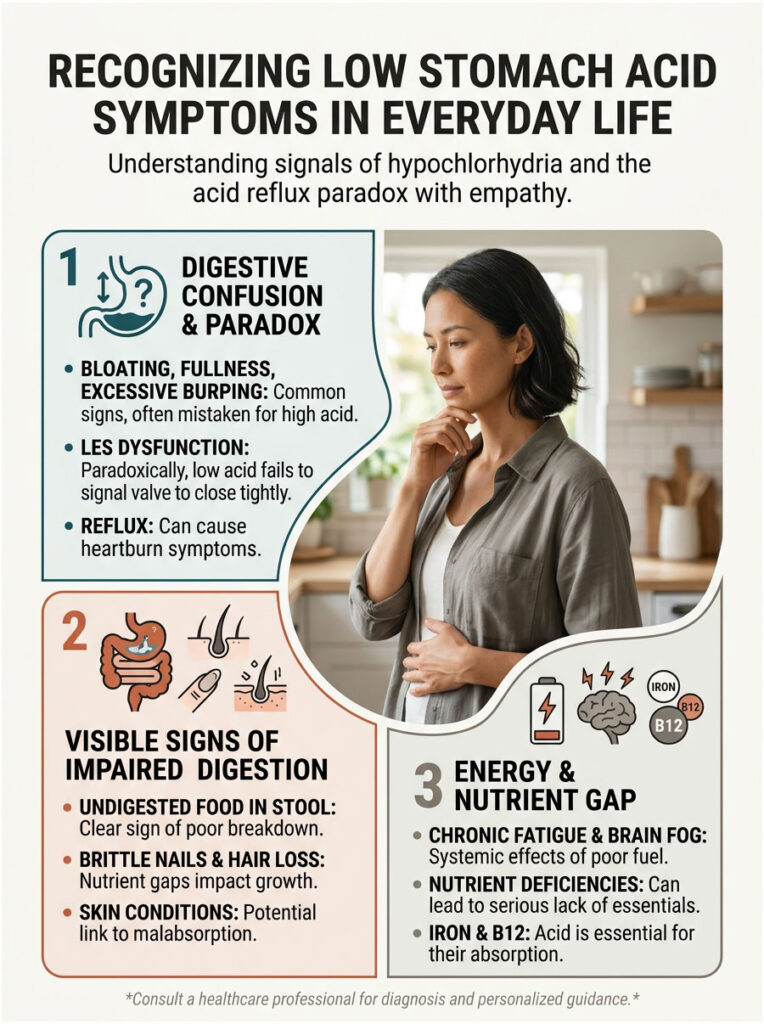
The most obvious signs of hypochlorhydria center on your upper digestive tract. When acid is low, food does not break down efficiently. Instead, it sits in the warm, dark environment of your stomach and starts to ferment. That fermentation produces large amounts of trapped gas.
You end up feeling uncomfortably full and bloated about 30 to 60 minutes after eating. You might burp excessively as the gas tries to escape. Many patients describe it as having a brick sitting in their upper abdomen.
The Acid Reflux Paradox
This is one of the most misunderstood issues in digestive health. Plenty of people with low acid experience acid reflux. How?
The valve between your stomach and esophagus, called the lower esophageal sphincter, is pH-sensitive. It needs a highly acidic environment to close tightly. With hypochlorhydria, that valve stays partially open. The fermenting food and weak acid splash upward into the esophagus, causing a burning sensation.
You feel the burn and naturally assume you have too much acid. In reality, the acid is just in the wrong place because the valve never received the signal to shut. And if you look closely, you might also notice undigested food particles in your stool, which is a clear sign the chemical digestion phase failed.
Skin, Hair, and Nail Warning Signs
Your outer appearance often mirrors what is happening inside your gut. Because low stomach acid blocks proper absorption of proteins and trace minerals, your body starts rationing nutrients. It pulls resources from non-essential tissues to keep vital organs running.
Patients commonly show up with brittle, weak nails and deep vertical ridges running down the nail surface. This is a classic indicator of protein, iron, and zinc malabsorption. Unexplained hair loss or thinning is also incredibly common. Skin conditions like acne rosacea have a strong clinical connection to hypochlorhydria as well, since poor digestion throws off gut flora and triggers systemic inflammation.
Fatigue, Brain Fog, and Energy Crashes
The link between your stomach and your energy levels runs deeper than most people realize. If you cannot break down food properly, you cannot extract the fuel your cells need. Chronic fatigue is one of the most draining low stomach acid symptoms patients report.
Much of this fatigue comes from specific nutrient deficiencies. Without adequate acid, Intrinsic Factor does not activate, and B12 absorption collapses. Over time, this leads to pernicious anemia, bringing extreme exhaustion, brain fog, and muscle weakness.
Iron deficiency anemia is just as common in these cases. Iron needs a highly acidic environment to convert into an absorbable form. No matter how much spinach or red meat you eat, without acid, that iron passes right through your system unused.
High vs. Low Stomach Acid: How to Tell the Difference
Understanding the differences between these two conditions is the first step toward getting the right treatment.
| Clinical Feature | High Stomach Acid | Low Stomach Acid |
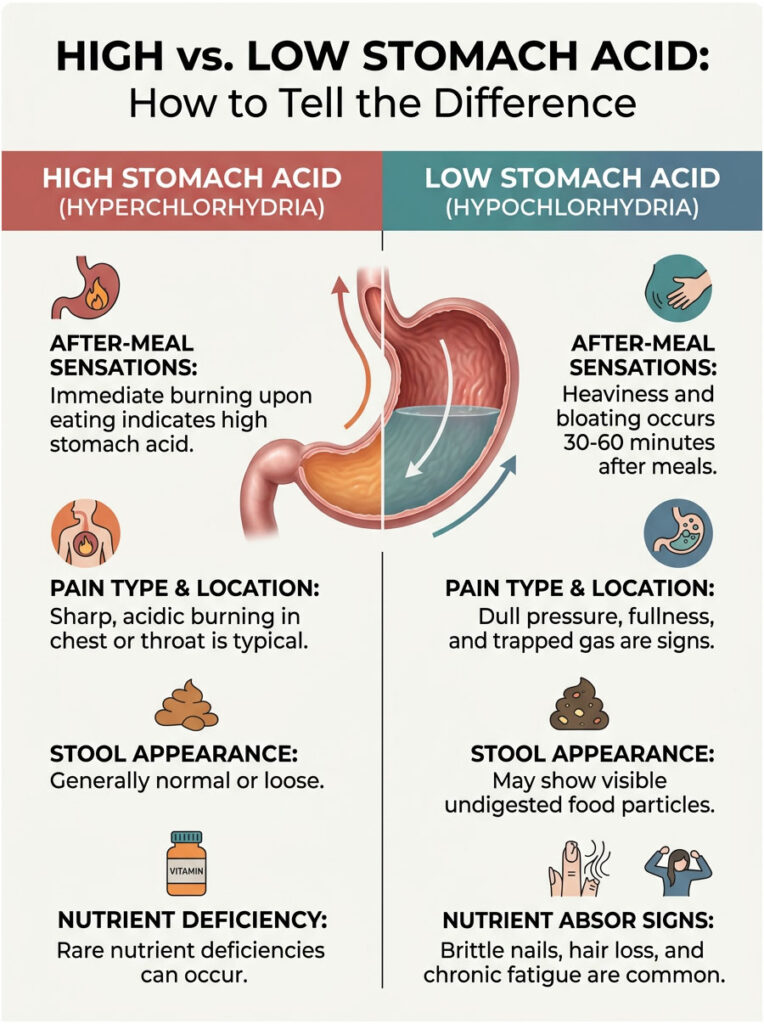
| Onset of Discomfort | Immediate burning upon eating | Heaviness and bloating 30-60 min after meals |
| Primary Sensation | Sharp, acidic burning in chest or throat | Dull pressure, fullness, and trapped gas |
| Stool Appearance | Generally normal or loose | Visible undigested food particles |
| Systemic Signs | Rare nutrient deficiencies | Brittle nails, hair loss, chronic fatigue |
| Response to Antacids | Temporary relief of burning | Worsening bloating and digestive sluggishness |
The Hidden Root Causes of Low Stomach Acid
If you want to actually heal, you need to stop treating symptoms and start acting like a detective. Several distinct factors can shut down your parietal cells, and identifying your specific trigger is essential for recovery.
H. Pylori Infection and Atrophic Gastritis
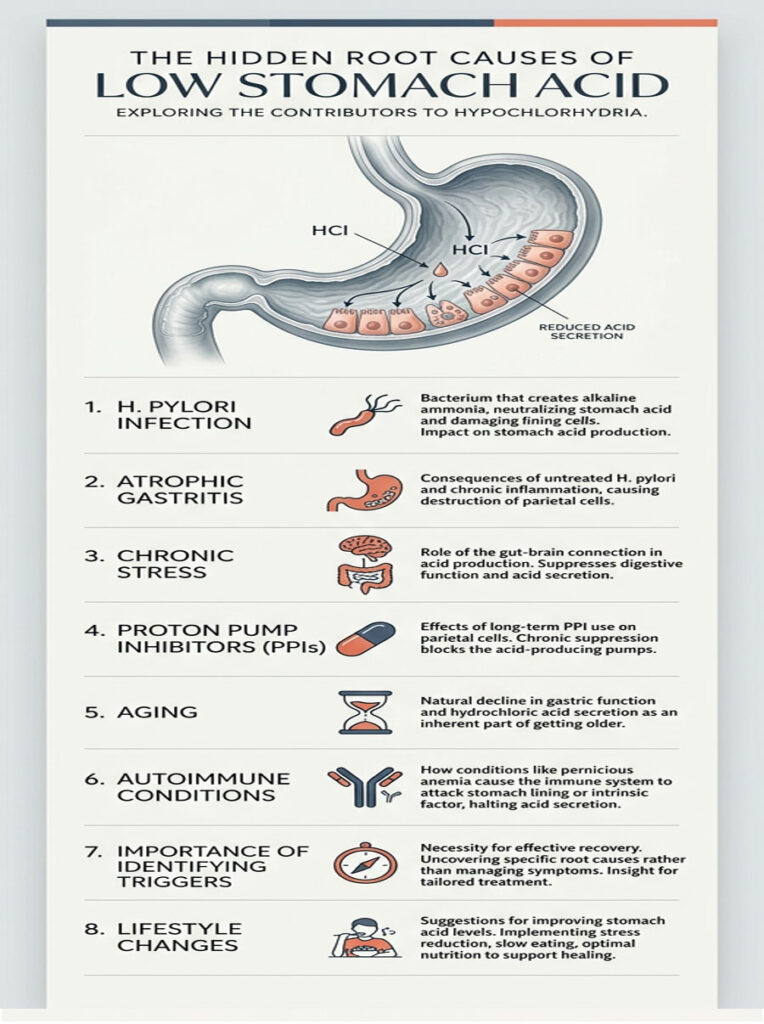
One of the most aggressive causes of low stomach acid is an infection with Helicobacter pylori. This spiral-shaped bacterium burrows into the protective mucosal lining of the stomach to hide from the immune system. To survive, it secretes an enzyme called urease, which produces ammonia and directly neutralizes surrounding stomach acid.
Over time, this prolonged infection triggers chronic inflammation that degrades the gastric mucosa. Eventually, this leads to atrophic gastritis, the physical shrinking and death of parietal cells. Left untreated, it can permanently destroy your ability to produce acid.
Chronic Stress and the Gut-Brain Connection
Your nervous system operates in two main modes: the sympathetic mode (fight or flight) and the parasympathetic mode (rest and digest). When you are chronically stressed, cortisol floods your system and the sympathetic side takes over.
Blood flow gets diverted away from your stomach and sent to your muscles and heart. The vagus nerve signals your parietal cells to halt acid production entirely. Your body has decided that digesting a meal is not a priority when it thinks you are under threat. This is not a minor issue. Chronic stress is one of the most overlooked causes of low stomach acid.
Long-Term Proton Pump Inhibitor (PPI) Use
Proton Pump Inhibitors like omeprazole and pantoprazole are prescribed far too freely for minor digestive complaints. These drugs are designed to completely block the enzyme system in parietal cells. While they can be lifesaving for severe, bleeding ulcers, they were never meant for long-term use.
Months or years on PPIs essentially forces your stomach into artificial hypochlorhydria. Your parietal cells gradually lose the ability to function. In severe cases, this progresses to achlorhydria, the complete absence of stomach acid. And when patients try to stop cold turkey, they experience intense acid rebound that keeps them trapped on the medication.
Aging and Autoimmune Conditions
As we age, gastric function naturally declines. Up to 30% of adults over 60 experience significantly reduced acid secretion. The parietal cells become less efficient, and blood supply to the gastric mucosa diminishes.
Autoimmune conditions also play a role. Pernicious anemia is an autoimmune disease where the body creates antibodies that attack and destroy parietal cells. If you already have another autoimmune condition like Hashimoto’s thyroiditis, your risk of autoimmune-related low stomach acid goes up significantly.
The Serious Risks of Ignoring Low Stomach Acid
Leaving hypochlorhydria untreated is not just about dealing with some bloating. The stomach is the gateway to the rest of your body. When the gateway fails, everything downstream suffers.
Small Intestinal Bacterial Overgrowth (SIBO)
Your small intestine is meant to be a relatively clean environment for nutrient absorption, not a breeding ground for bacteria. Stomach acid acts as a powerful sterilizing wash. Every time you swallow, the acidic fluid flows down and kills bacteria trying to migrate upward from the colon.
When acid is missing, bacteria from the large intestine easily migrate into the small intestine and set up camp. This is SIBO, and it is both stubborn and painful. The misplaced bacteria feast on undigested carbohydrates, producing hydrogen and methane gas that causes severe abdominal distension.
Mineral Malabsorption and Bone Loss
Your bones depend on a steady supply of ionized minerals to maintain density. Calcium, magnesium, and zinc all require a highly acidic environment to become ionized and absorbable. With severe hypochlorhydria, these minerals pass through your body completely unabsorbed.
Over time, your body starts pulling calcium from your bones to maintain blood levels. This accelerates the onset of osteopenia and osteoporosis, especially in postmenopausal women. Research shows that long-term acid suppression raises hip fracture risk by up to 44%.
Vulnerability to Foodborne Infections
Stomach acid is your immune system’s first line of defense. Every day, you ingest millions of microscopic pathogens on your food, your hands, and in your water. A healthy stomach destroys these invaders on contact.
When acid levels drop, bacteria like Salmonella, Campylobacter, and E. coli can survive the passage through a weakened stomach and reach the intestines, causing severe infections. Patients with achlorhydria also face a much higher risk of dangerous Clostridium difficile infections, which can lead to life-threatening colitis.
How to Test for Low Stomach Acid
Guessing is never a sound medical strategy. If you suspect low stomach acid, you need real data. Thankfully, functional medicine offers several precise tools to measure what is actually going on inside your stomach.
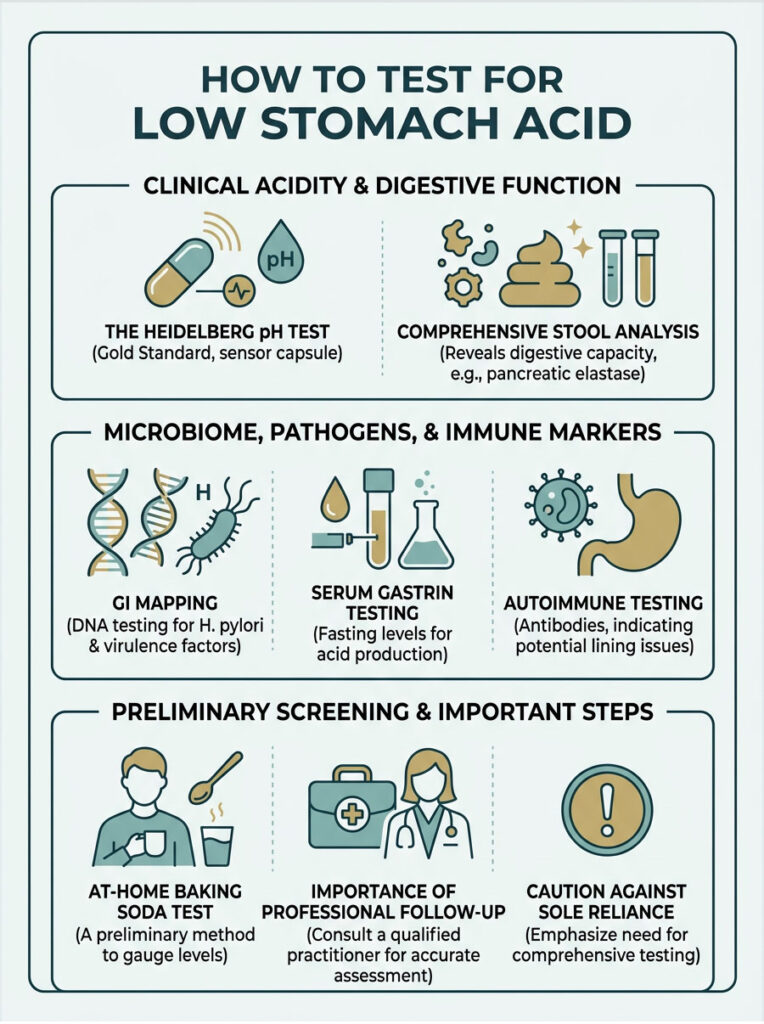
The Heidelberg pH Test (Gold Standard)
The Heidelberg Test is widely considered the gold standard for diagnosing acid levels. The patient swallows a small electronic capsule containing a pH sensor and a tiny radio transmitter. The capsule is tethered by a thin thread to keep it positioned in the stomach.
After establishing a baseline pH, the clinician introduces a sodium bicarbonate challenge. The patient drinks an alkaline solution, and the test measures exactly how long the parietal cells take to re-acidify the stomach back to a pH of 1.5. This produces a precise, real-time graph of gastric function.
Comprehensive Stool Analysis and GI Mapping
While stool cannot directly measure acid, a comprehensive stool analysis reveals important clues about digestive capacity. One key marker is pancreatic elastase. If stomach acid is low, it will not trigger the pancreas to release its enzymes, so low elastase often points back to an acid problem.
Advanced DNA stool testing like a GI Map can also detect H. pylori DNA and even identify whether the specific strain carries virulence factors linked to ulcers or atrophic gastritis. This information is essential for building an eradication plan.
Serum Gastrin and Antibody Testing
Blood testing provides another valuable window into stomach health. Measuring fasting serum gastrin levels reveals how hard your body is struggling to produce acid. Highly elevated gastrin strongly suggests the stomach is too alkaline.
Testing for Intrinsic Factor antibodies and parietal cell antibodies can reveal whether an autoimmune process is attacking the stomach lining. Identifying this autoimmune component completely changes the treatment approach.
The At-Home Baking Soda Test
If you want a safe, preliminary screening method you can try at home, the baking soda challenge is a reasonable starting point. First thing in the morning on an empty stomach, mix a quarter teaspoon of baking soda into four ounces of cold water. Drink it quickly and start a timer.
Baking soda is alkaline. When it mixes with hydrochloric acid, the reaction produces carbon dioxide gas. If your stomach is producing adequate acid, you should burp within two to three minutes. If nothing happens within five minutes, it suggests low acid levels.
Important: Never rely on the baking soda test alone to start acid supplementation. Always follow up with a comprehensive stool analysis or Heidelberg test under the supervision of a qualified practitioner.
Diagnostic Methods at a Glance
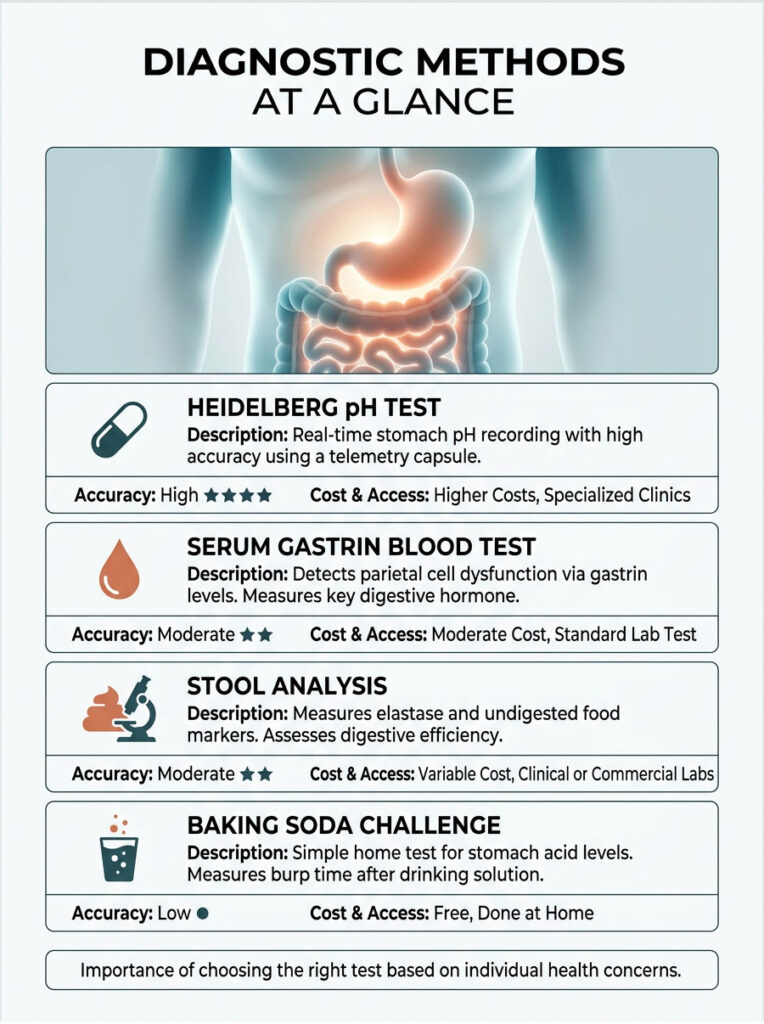
| Test | How It Works | Accuracy | Cost and Access |
| Heidelberg pH Test | Electronic capsule records real-time stomach pH | Very High (Gold Standard) | Higher cost, specialized clinics only |
| Stool Analysis | Measures elastase and checks for undigested food markers | Moderate | Medium cost, widely available |
| Serum Gastrin Blood Test | Measures gastrin levels to detect parietal cell dysfunction | Moderate to High | Low to medium cost, standard lab draw |
| Baking Soda Challenge | Sodium bicarbonate triggers a chemical reaction (burping) | Low (screening only) | Free, done at home |
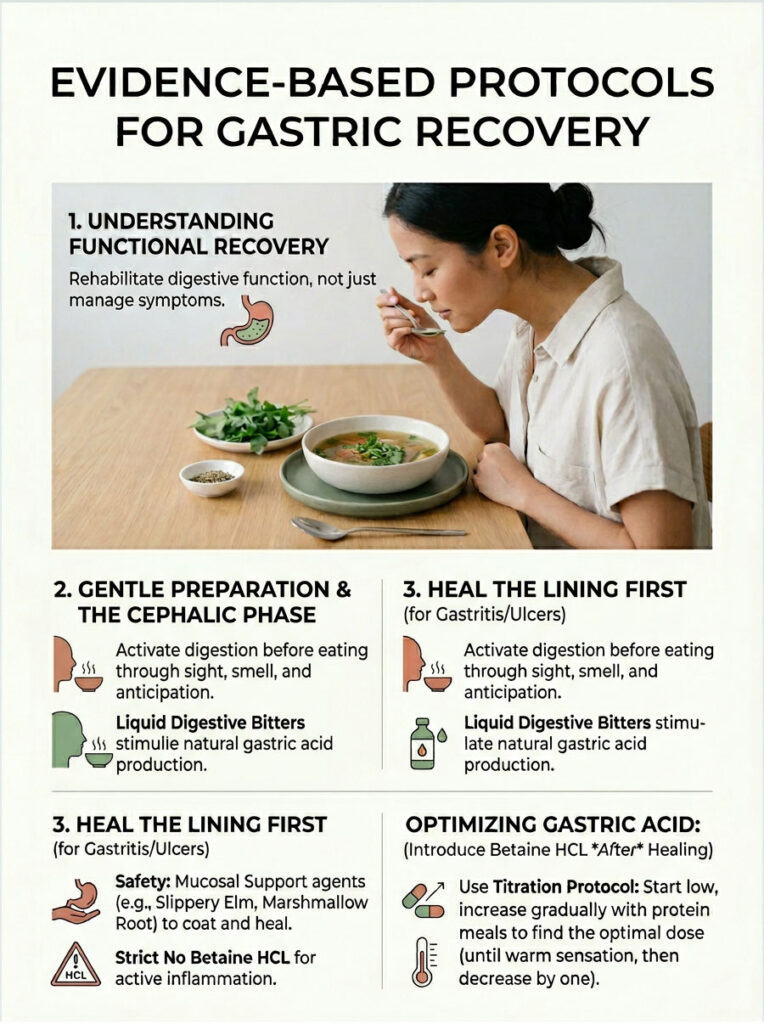
Evidence-Based Protocols for Gastric Recovery
Once hypochlorhydria is confirmed, the goal is not just managing symptoms. It is fundamentally rehabilitating your digestive system. This requires a multi-layered approach: replace the missing acid, stimulate natural production, and heal any underlying mucosal damage.
Betaine Hydrochloride Supplementation
The most direct way to address acid deficiency is to temporarily replace the missing acid using Betaine Hydrochloride, a naturally derived form of hydrochloric acid bound to a beet-derived amino acid. Taking it with protein-heavy meals immediately lowers gastric pH, sterilizes food, activates enzymes, and stops postprandial bloating. Many patients notice a significant improvement within the first week.
The key is a careful titration protocol. Start with one capsule in the middle of a protein-rich meal. If you feel no warmth, increase to two capsules at the next similar meal. Keep increasing by one capsule until you feel a slight warming sensation, then drop back by one. That is your maintenance dose.
Heal the Stomach Lining First
There is a critical safety point here. If you have active gastritis, an H. pylori infection, or a gastric ulcer, adding acid will cause severe pain and can injure the mucosal lining further.
In these cases, I start patients on a gut-healing protocol first. Mucosal support agents like Zinc Carnosine, Deglycyrrhizinated Licorice (DGL), and slippery elm bark coat the stomach lining and promote cellular repair. Only after the lining is fully healed do we introduce Betaine Hydrochloride.
Digestive Bitters and the Cephalic Phase
Digestion actually begins before food enters your mouth. When you smell or even think about food, your brain sends signals down the vagus nerve to wake up the stomach. This is called the cephalic phase, and it accounts for up to 30% of total gastric acid production. In our fast-paced, distracted world, most people completely skip this phase.
Liquid digestive bitters are a simple fix. Placing a few drops on your tongue about 15 minutes before a meal triggers the vagus nerve. The bitter taste sends an immediate signal to the brain, which tells the stomach to start producing acid.
Dietary Changes That Support Acid Recovery
How you eat matters just as much as what you eat. Poor meal habits are one of the leading drivers of low stomach acid symptoms, and fixing them is a non-negotiable part of recovery.
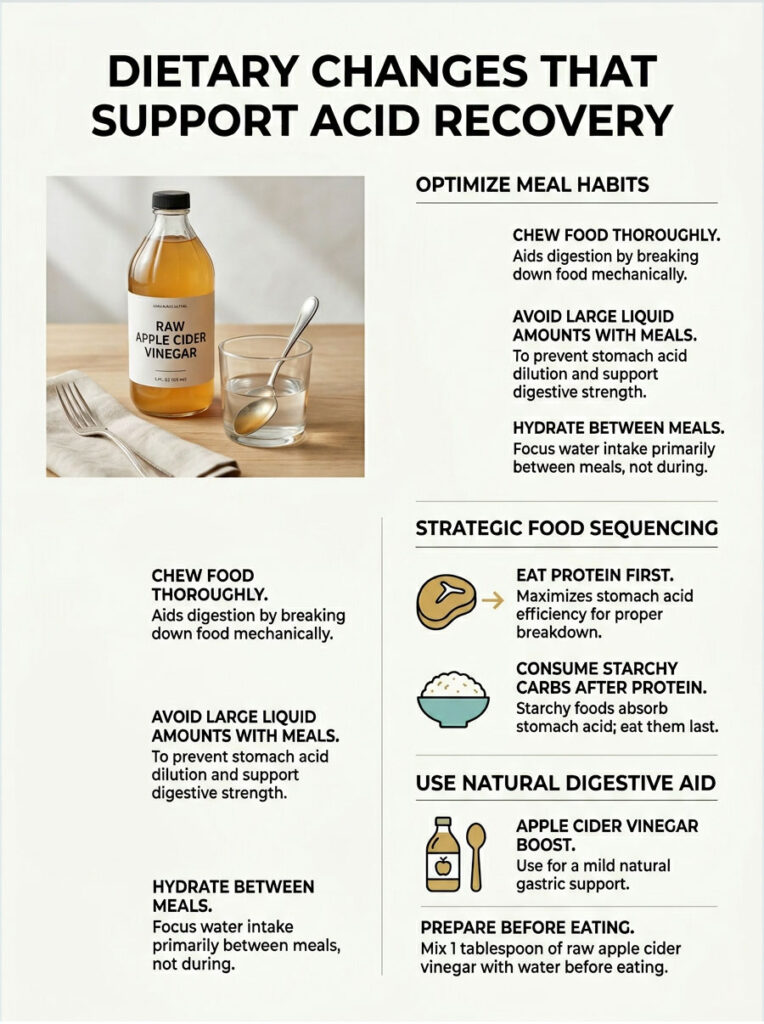
Chewing, Hydration, and Meal Hygiene
First, chew your food thoroughly. Aim for 20 to 30 chews per bite. Your food should be the consistency of applesauce before you swallow. If you send large, unchewed chunks into a weak stomach, it simply cannot handle the job. Undigested food will rot and ferment, feeding the bacteria that drive SIBO.
Second, stop flooding your meals with liquid. Drinking large amounts of water or iced beverages with food dilutes your already limited gastric juices and raises the stomach pH. Stick to small sips during meals and hydrate between them instead.
Protein-First Eating and Apple Cider Vinegar
The order you eat your food in matters. If you have low stomach acid, eat your protein first. Protein demands the most acid to break down, so you want it hitting the stomach while acid reserves are highest. If you fill up on starchy carbs first, they soak up the limited acid like a sponge, and there is nothing left for the meat.
For a gentle, natural boost, try mixing one tablespoon of raw apple cider vinegar into a small splash of water right before eating. The acetic acid helps lower gastric pH slightly. It is not as powerful as Betaine Hydrochloride, but it works well for mild cases.
Vagus Nerve Stimulation for Long-Term Recovery
Supplements are a temporary bridge, not the final answer. If chronic stress is driving your low acid, you need to address the neurological root. That means actively stimulating the vagus nerve, the master controller of your parasympathetic nervous system.
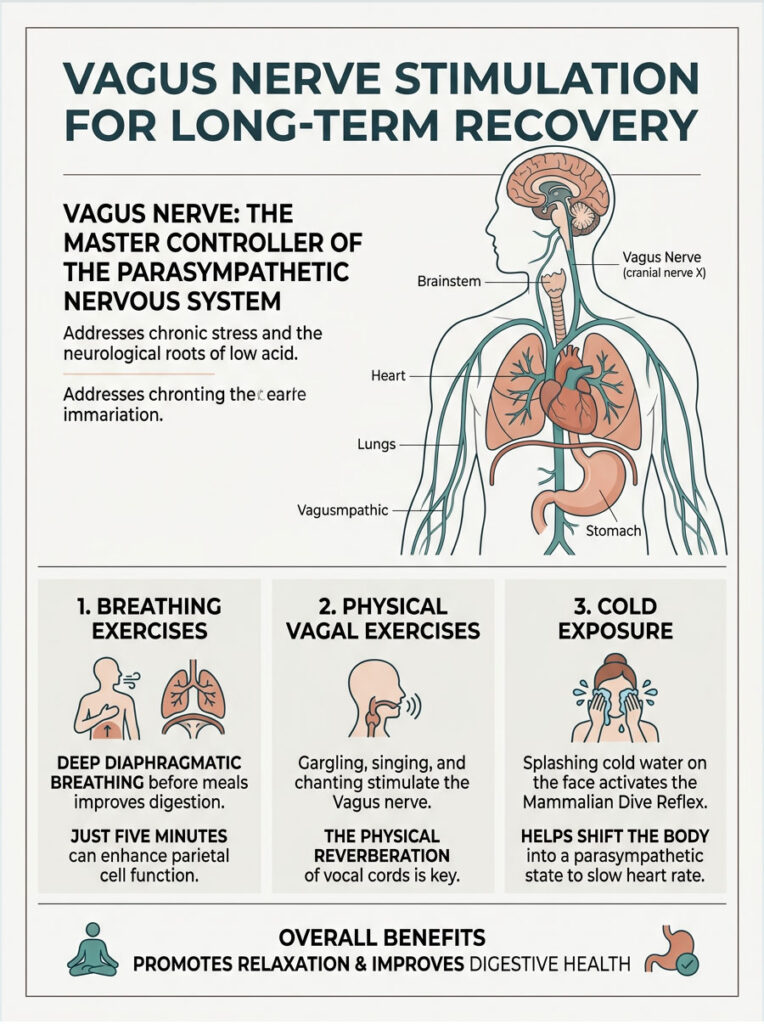
Breathing Exercises Before Meals
Deep diaphragmatic breathing before meals physically stimulates the vagus nerve and shifts your body from fight-or-flight mode into rest-and-digest mode. Breathe deeply into your belly, not shallowly into your chest. Just five minutes of this before eating can meaningfully improve parietal cell function and blood flow to your digestive organs.
Physical Vagal Nerve Exercises
You can also stimulate the vagus nerve mechanically. Gargling forcefully with water until your eyes water is an effective method. Singing loudly or chanting also works because the vibrations stimulate the vocal cords, which are innervated by the vagus nerve. I often suggest patients sing along to music while cooking dinner. It sounds unusual, but it is backed by science.
Cold exposure is another powerful tool. Splashing cold water on your face activates the mammalian dive reflex, which instantly triggers the vagus nerve and drops your heart rate, pushing the body into a parasympathetic state.
Real-World Clinical Outcomes
When we stop chasing symptoms and address the acidic root cause, the body’s natural healing capacity kicks in. Here are three clinical examples that illustrate what proper gastric optimization can accomplish.
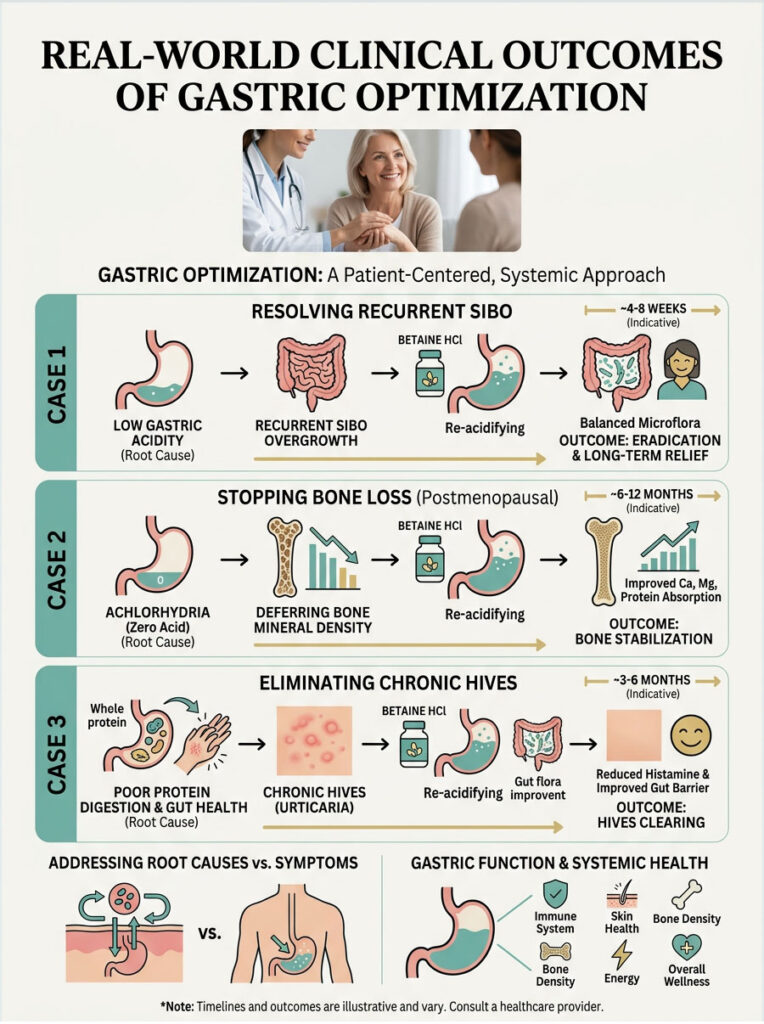
Resolving Recurrent SIBO
A 45-year-old woman presented with chronic SIBO. She had completed three rounds of expensive antibiotics, and each time her bloating and gas returned within a month. Her previous doctors kept treating the small intestine while ignoring the stomach.
We tested her gastric function and found severe hypochlorhydria. Her stomach was essentially alkaline, letting bacteria constantly reinfect the small bowel. We stopped the antibiotics and focused on restoring her acid barrier with Betaine Hydrochloride and digestive bitters. Within six weeks, her SIBO symptoms completely resolved because the restored acid wash killed migrating bacteria at the source.
Stopping Bone Loss in a Postmenopausal Patient
A 62-year-old woman had been taking PPIs daily for over a decade for mild reflux. Despite high-dose calcium supplements, her bone mineral density kept declining. The drug-induced achlorhydria was preventing any of that supplemental calcium from being absorbed.
We initiated a careful three-month weaning protocol to get her off the medication without severe rebound. We introduced mucosal support to heal the lining, followed by gentle acid stimulation. Once her natural acid production returned, her body finally started absorbing calcium and magnesium. A follow-up DEXA scan a year later showed complete stabilization of bone density. The rapid loss had stopped.
Eliminating Chronic Hives Through Gut Healing
A 35-year-old man came in with chronic, unexplained hives and sudden food sensitivities to foods he had eaten his whole life. He was taking multiple antihistamines daily just to function.
We found extremely low stomach acid. Because he could not break down proteins properly, large undigested protein molecules were entering his intestines. His immune system flagged these oversized proteins as threats and launched histamine responses. We started a Betaine Hydrochloride titration protocol. Within two months, the hives vanished. His immune system calmed down because proteins were finally broken into harmless amino acids before reaching the gut immune tissue.
Key Takeaways and Next Steps
Your overall health depends heavily on the health of your stomach. Ignoring low stomach acid symptoms sets the stage for bacterial overgrowth, severe nutrient deficiencies, and systemic inflammation.
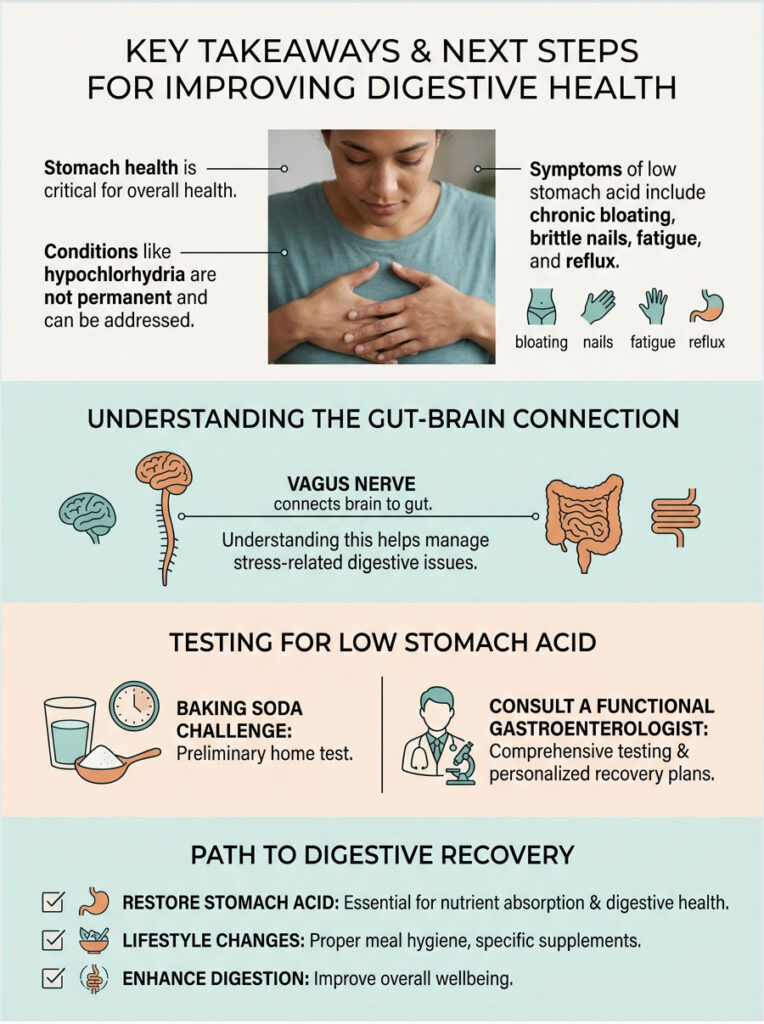
The good news is that hypochlorhydria and achlorhydria are not permanent conditions. By understanding how the vagus nerve and gut-brain axis work, you can start addressing stress-related digestive failure. By carefully supplementing with Betaine Hydrochloride and practicing proper meal hygiene, you can immediately improve protein breakdown and nutrient absorption.
If you are dealing with chronic bloating, brittle nails, persistent fatigue, or stubborn reflux, stop reaching for the antacids. You may be putting out the very fire your body needs. I strongly recommend consulting with a functional gastroenterologist for proper testing.
Ask for a comprehensive stool analysis, check your serum gastrin levels, and build a targeted recovery plan. Restoring stomach acid is the single most important step you can take toward reclaiming your digestive health. Treat the root cause, respect your gastric physiology, and your body will do the rest.
Frequently Asked Questions
What exactly is hypochlorhydria and how does it affect the digestive cascade?
Hypochlorhydria is a clinical condition characterized by a deficiency in hydrochloric acid (HCl) production within the stomach. As a functional gastroenterologist, I view this as a failure of the parietal cells to maintain a target gastric pH of 1.5 to 3.0. This disruption halts the conversion of pepsinogen into pepsin, preventing protein breakdown and allowing food to ferment rather than digest, which triggers a systemic cascade of nutrient malabsorption and gastrointestinal distress.
How can low stomach acid cause acid reflux and heartburn symptoms?
This is a common clinical paradox. The lower esophageal sphincter (LES), the valve separating the stomach from the esophagus, is pH-sensitive and requires high acidity to signal it to close tightly. In cases of hypochlorhydria, the lack of acid prevents this closure. Consequently, fermenting food and weak gastric juices splash into the unprotected esophagus, causing the burning sensation typically mistaken for acid overproduction.
What are the most common visible symptoms of a stomach acid deficiency?
Beyond internal distress, low stomach acid often manifests dermatologically and structurally. Patients frequently present with brittle, weak fingernails featuring deep vertical ridges, as well as unexplained hair thinning. These are classic markers of protein, iron, and zinc malabsorption. Additionally, seeing undigested food particles in your stool is a definitive sign that the chemical digestion phase in the stomach has failed.
Why does chronic stress lead to a decrease in hydrochloric acid production?
The gut-brain axis plays a critical role in gastric secretion via the vagus nerve. Digestion is a parasympathetic process (rest and digest). When you are under chronic stress, the sympathetic nervous system (fight or flight) takes over, diverting blood flow away from the digestive tract and signaling the parietal cells to halt acid production. This neurological shift effectively shuts down the stomach’s chemical factory.
What is the clinical link between low stomach acid and SIBO?
Gastric acid acts as a primary sterilizing barrier for the digestive tract. When acid levels are insufficient, this ‘acid wash’ fails to kill rogue bacteria ingested with food. This allows bacteria from the large intestine to migrate upward into the small intestine, leading to Small Intestinal Bacterial Overgrowth (SIBO). Statistics show that approximately 78% of patients with chronic hypochlorhydria eventually develop this painful bacterial imbalance.
How do Proton Pump Inhibitors (PPIs) contribute to long-term acid deficiency?
PPIs are designed to irreversibly block the enzyme system in parietal cells to stop acid production. While useful for acute conditions like bleeding ulcers, long-term use can force the stomach into a state of artificial hypochlorhydria or achlorhydria. Over time, the parietal cells can lose their functional capacity, and patients often experience ‘acid rebound’ when attempting to stop the medication, making recovery complex.
What is the ‘Gold Standard’ diagnostic test for measuring stomach acid levels?
The Heidelberg pH Test is considered the gold standard in functional gastroenterology. This test involves the patient swallowing a small electronic capsule containing a pH sensor. We then introduce a sodium bicarbonate challenge to observe how quickly the parietal cells can re-acidify the stomach. This provides a precise, real-time mathematical graph of the patient’s gastric secretory capacity.
Can I perform a preliminary low stomach acid test at home?
Yes, the baking soda challenge is a helpful, though not definitive, screening tool. By mixing 1/4 teaspoon of baking soda in 4 ounces of water and drinking it on an empty stomach, you trigger a chemical reaction. If your stomach has adequate acid, the bicarbonate should produce carbon dioxide gas (a burp) within two to three minutes. If no burp occurs within five minutes, it strongly suggests a state of hypochlorhydria.
What is Betaine Hydrochloride and how is it used in clinical protocols?
Betaine Hydrochloride (HCl) is an exogenous supplement used to replace missing stomach acid. In a clinical setting, we use a titration protocol where the patient gradually increases the dosage with protein-rich meals until a mild warming sensation is felt in the stomach. This helps identify the optimal maintenance dose required to activate digestive enzymes and restore the gastric barrier.
Why is the ‘cephalic phase’ of digestion vital for patients with low acid?
The cephalic phase occurs before food hits the stomach; it is triggered by smelling, seeing, or thinking about food. This phase accounts for up to 30% of total acid production. To stimulate this, I recommend using liquid digestive bitters on the tongue 15 minutes before meals. The bitter taste signals the brain to activate the vagus nerve, which commands the parietal cells to begin pumping acid in preparation for the meal.
How does an H. pylori infection suppress gastric acid secretion?
Helicobacter pylori is a resilient bacterium that survives by secreting an enzyme called urease. Urease produces ammonia, which neutralizes the acid in the immediate vicinity of the bacteria. Chronic infection leads to atrophic gastritis—the inflammation and eventual shrinking of the stomach lining—which permanently destroys the parietal cells’ ability to manufacture hydrochloric acid if left untreated.
Can untreated low stomach acid lead to osteoporosis or bone fractures?
Absolutely. Essential bone-building minerals like calcium and magnesium require a highly acidic environment to become ‘ionized’ or water-soluble for absorption. In a state of hypochlorhydria, these minerals pass through the gut unabsorbed. To maintain blood calcium levels, the body will leach calcium from the bones, significantly increasing the risk of osteoporosis and hip fractures, especially in older adults.
Disclaimer
This article is for informational and educational purposes only and does not constitute medical advice. The clinical protocols discussed, including acid supplementation, should only be performed under the direct supervision of a qualified healthcare professional. Always consult a doctor before changing medications or starting new supplements, especially if you have a history of ulcers or gastritis.
References
- American Gastroenterological Association (AGA) – gastro.org – Clinical guidelines on the management and long-term impact of Helicobacter pylori infections.
- Journal of the American Medical Association (JAMA) – jamanetwork.com – Research documenting the correlation between long-term PPI use and increased hip fracture risk.
- National Institutes of Health (NIH) – nih.gov – Clinical data regarding the prevalence of Vitamin B12 deficiency in patients with reduced gastric acidity.
- World Journal of Gastroenterology – wjgnet.com – Peer-reviewed study on the role of gastric acid as a barrier against Small Intestinal Bacterial Overgrowth (SIBO).
- Harvard Health Publishing – health.harvard.edu – Expert insights on the “Rest and Digest” state and the Vagus nerve’s role in gastric secretion.
- The Lancet Gastroenterology & Hepatology – thelancet.com – Statistical analysis of age-related decline in parietal cell function among adults over 60.