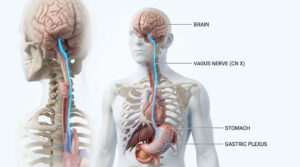
The white death, the great white plague or the graveyard cough, tuberculosis (TB) is known by many names. It is a disease known as the greatest killer of mankind and has inflicted many since its million years old origin. TB, a debilitating lung ailment is also capable of invading and scathing other organs/glands. Organs like brain, spinal cord, lymph nodes, liver, spleen, kidneys, endocrine glands and many others. Yes, it can even affect endocrine glands like thyroid, pancreas and even adrenals. Although, cases of TB affecting endocrine glands directly or indirectly, are not many but majority of them are related to adrenal glands.
Adrenal glands or Suprarenal glands are the part of endocrine system and are present above the kidneys. It is composed of two different parts known as adrenal cortex and adrenal, medulla responsible for secreting aldosterone, cortisol, androgens, catecholamines, adrenaline and noradrenaline. These hormones helps to cope with stress, maintains metabolism, salt and water balance, and have several other functions. The cortical part of adrenal gland is the outer part, which is much larger in size than the inner part called adrenal medulla.
Tuberculosis- King’s evil
Tuberculosis (TB) in humans is a disease caused due to infection by Mycobacterium tuberculosis. Whereas,
Mycobacteria other than tuberculosis (MOTT) are responsible for causing atypical infections. M. tuberculosis
strains are reportedly the most virulent strain due to the aerosol formation. They show increased transmissibility
as well as higher morbidity and mortality in infected individuals. Although, it is primarily a pulmonary disease,
but when involvement of central nervous system, endocrine system or other organ of the body occurs, it is
referred as Extrapulmonary TB. This pathogen is transmitted through droplet nuclei which are dispersed into
air by an infected person during coughing, sneezing or talking .
Types
Tuberculosis can be categorized into 3 types
- Pulmonary Tuberculosis It affects lungs and is the most common form of tuberculosis. It is symptomatic with productive cough, fever and weight loss.
- Extrapulmonary Tuberculosis M. tuberculosis can spread to other organs during silent phase inclusive of lymph nodes, meninges, vertebrae, kidney, genital organs, abdominal cavity, joints and bones.
- postprimary pulmonary tuberculosis It occurs due to reactivation after years following the initial infection.
- Pathogenesis It can be divided into three different but, interrelated stages
Stage 2 (Secondary stage). The emergence of cell-mediated immunity and the formation of granulomas are characteristic features of this stage. M. tuberculosis bacilli that escape from bactericidal effects of the AMS, multiply and result in destruction of AMs. This leads to migration of blood monocytes and other inflammatory cells like neutrophils to the site of infection. The monocytes then mature to become an antigen presenting AMs and ingest the bacteria, but does not effectively kill them. By 6-8 weeks post-infection, antigen presenting dendritic cells travel to lymph nodes where I lymphocytes are activated and recruited. These activated T lymphocytes migrate to the site of infection and proliferate forming an early stage granuloma, where macrophages become activated to kill intracellular M. tuberculosis. However, continuous T cell activation leads to the formation of granulomas that mark persistent stage of the infection (latency), where the growth and spread of bacteria into additional tissue sites are restricted. At this stage more than 90% of infected people remain asymptomatic, but the bacteria may survive within AMS.
Stage 3 (Final stage) In this stage, the latent and controlled M. tuberculosis infection is reactivated. There are two important reasons described for a reactivation event to occur, decline in the host’s immunity due to genetic or environmental cause; and failure to develop and maintain immune signals. Under these circumstances, the granuloma structure disrupts and results in lung cavitation, pulmonary disease and spread of bacteria to other sites.
TB Affecting Adrenal gland
M. tuberculosis enters via airway into the lungs and then may disseminate to extrapulmonary sites such as
spleen, bone marrow, kidneys, and adrenal glands by lymphohematogenous route. This dissemination may
occur during initial pulmonary infection or later, due to the activation of the bacteria. Among other endocrine
glands, adrenal is the most commonly affected gland. Majority of the cases are seen to be affected after 10-15
years of the initial infection and, consequently, it is often associated with extra-adrenal infection. Pulmonary
or gastrointestinal tuberculosis are the common manifestations in such cases where infection is not restricted
only to the adrenals.
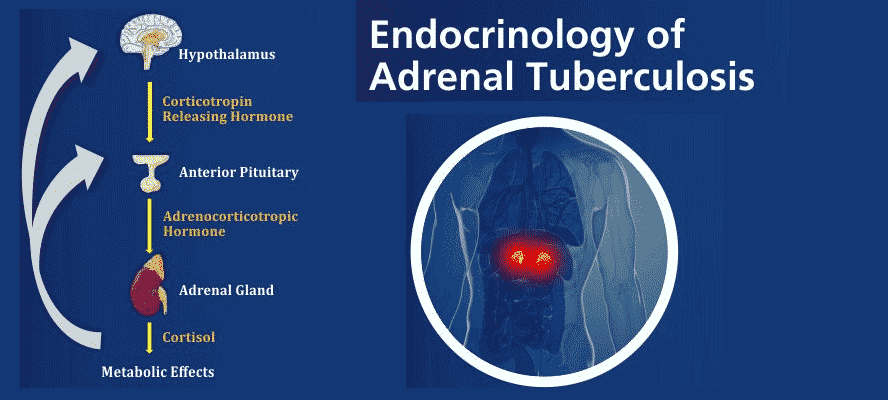
M. tuberculosis can cause adrenal insufficiency through direct glandular involvement, extra-adrenal infection or due to anti tuberculous therapy. When adrenal insufficiency is because of direct glandular involvement, of M. tuberculosis, signs and symptoms may not appear till 90% of the gland has been destroyed. This destruction that occurred in the mean time leads to the deficiency of glucocorticoids, mineralocorticoids and androgens production.
There are generally four histopathological patterns seen, in adrenal tuberculosis. These includes caseating or non caseating granulomas, mass lesions secondary to the development of cold abscesses, glandular enlargement with adrenal destruction by inflammatory granulomas or adrenal atrophy from fibrosis related to chronic infection. Epithelioid granulomas occur less frequently in the adrenals than in extra-adrenal foci and calcification of the gland is common but not specific Although, majority of the studies more often focuses on cortical involvement, in some cases, medulla may also be involved.
After extensive research, adrenal tuberculosis causing adrenal insufficiency has been characterized as enlarged or atrophied adrenal glands; compatible with the time passed since the onset of the infection. This enlargement of gland is not only due to direct involvement of tuberculosis on adrenals but also due to stress created by M. tuberculosis for increased requirement of cortisol. Here, larger glands mean recent and probably active infection while, small calcified glands indicate inactive infection.
Due to the stress, exogenous ACTH (Adrenocorticotropic hormone) stimulates adrenals in order to maintain high plasma cortisol level. However, this can further result in failure of ACTH inhibiting cortisol, release.
M. tuberculosis Affecting Immunological Response
Most of the biological effects like cell mediated immunity and allergic responses of the immune system are mediated
by cytokines. For these responses, Th1 and Th2 plays an essential roles. Th1-type cytokine produces pro inflammatory
responses for killing the pathogen and for perpetuating the immune response. As, excess pro inflammatory responses
can cause tissue damage, so to counteract this, Th2 type cytokines are present which has more anti-inflammatory
response.
In adrenal tuberculosis, responses of Th1 and Th2-type cytokines are compromised as both Th1 and Th2 responses need to be balanced. Stress induced by M. tuberculosis, shifts this balance more towards Th2 because of increased levels of glucocorticoids which is known to enhance Th2 activity. In contrast, DHEA S enhances Th1 type cell activity and also has anti glucocorticoid effect but, in patients with TB, DHEA-S levels were found to be decreased. This high glucocorticoids and low DHEA S level leads to immunologically-mediated tissue damage in tuberculosis.
Symptoms
The possibility of adrenal TB is considered when patient’s with a history of tuberculosis (either active infection or
positive tuberculin skin test) have classical manifestations like
- Malaise
- Anorexia
- Orthostatic hypotension
- Hyperpigmentation
- Anemia
- Hyponatremia
- Hyperkalemia
In rare cases, patients may have acute onset of life threatening adrenal insufficiency.
Diagnosis and Management
Both invasive methods and non invasive methods can be used for diagnosis purposes. Non invasive
or radiographic methods includes computed tomography PET-CT Scan, magnetic resonance imaging (MRI)
or positron emission tomography (PET). Whereas, invasive methods like obtaining of tissue by biopsy,
CT guided fine needle aspiration, PCR and culturing of Mycobacterium can also be done to achieve a
diagnostic conclusion.
In the initial years or stage of infection, CT findings reveals non calcified, enlarged adrenal glands with an area of lucency reflecting caseous necrosis. While, in chronic infections, CT scan discloses shrunken adrenal glands often associated with calcifications. MRI scans are also useful in finding the clues for a diagnosis but, calcifications are more clearly visible on CT Scans.
For microbiological and pathological analysis, tissue specimen should be obtained, especially, in cases wherein, adrenal involvement is the only evidence of tuberculosis. Even, CT-guided fine needle aspiration of the adrenal gland can be done to obtain adequate amount of tissue specimen for diagnosis. Not necessarily, culturing and PCR of these tissue affected by M. tuberculosis consistently show positive results, so a combination of tests like culturing, PCR and histopathology can be used to confirm the diagnosis.
With the exception of children having miliary tuberculosis, treatment for adrenal tuberculosis with drug-susceptible isolates are generally same as of pulmonary tuberculosis. Commonly, rifampin is use which induces the hepatic enzymes responsible for steroids metabolism to boost the glucocorticoid synthesis. Hardly, there are any cases of adrenal crisis precipitated by rifampin administrations. In several instances, adrenal recovery of patients were also reported after receiving anti tuberculosis therapy in the initial stages, i.e. prior to the adrenal gland’s destruction,
TB affecting other endocrine glands
- Thyroid Gland Tuberculosis affecting thyroid gland without the involvement of other organs is extremely rare. It can result from hematogenous dissemination or by direct extension from an active laryngeal or lymph node infection. Solitary cold abscess, acute abscess, diffuse goiter, multiple lesions due to dessimination and chronic fibrosing tuberculosis are the described presentations of thyroid tuberculosis with miliary disease being the most common presentation.
- Pituitary Gland It is rarely seen and can arise from hematogenous seeding either in presence or absence of miliary disease. Also, it can occur due to direct extension from sphenoid sinus, meninges or brain. Depending on the pathogenesis,tuberculosis can affect only pituitary gland or can also be associated with other sites.
- Pancreas Although, tuberculosis affecting gastrointestinal tract is more common, it can also affect pancreas in some cases. Pancreatic tuberculosis may present with abdominal mass. Its diagnosis is confirmed through biopsy or aspiration. Some patients also presents obstructive jaundice, pain or gastrointestinal bleeding.
TB alone being such a pestilence, imagine the affects of adrenal TB on its sufferer, who not only faces the emotional and economical burden but also the strings of stigmas that comes with it. Nothing describes it better than the lines said by H James Harrington, “Measurement is the 1st step that leads to control and eventually to improvement. If you can’t measure something, you can’t understand it. If you can’t understand it, you can’t control it. If you can’t control it, you can’t improve it”.