Waking up and sprinting to the bathroom is a rough way to start any day. If you keep asking yourself, “Why do I have diarrhea every morning?”, trust me, you’re far from alone. As a board-certified gastroenterologist with more than 15 years of clinical experience, I see patients every single week who feel like prisoners to their own bathrooms.
Table of Contents
Morning urgency is rarely just a reaction to something you ate last night. More often, it’s a tangled interaction between your gut microbiome, your nervous system, and the small habits you repeat each day. Plenty of people try the usual fixes, cutting back on coffee, eating bland food, drinking more water, only to find nothing really changes.
In clinic, we dig deeper. We look at how your body wakes up, how it handles hormones, and how your colon responds to that first sip or bite of the day. This guide walks you through exactly what’s happening inside your gut each morning and what you can actually do about it.
What Causes Morning Diarrhea?
Morning urgency is usually driven by an exaggerated gastrocolic reflex or the cortisol awakening response. When it becomes a daily pattern, though, it often points to deeper issues like Irritable Bowel Syndrome with Diarrhea (IBS-D), bile acid malabsorption, or overnight bacterial fermentation.
Key Clinical Statistics
- Prevalence: Roughly 10 to 15 percent of adults in the USA live with Irritable Bowel Syndrome with Diarrhea.
- Misdiagnosis: Research from the American Gastroenterological Association suggests up to 30 percent of patients labeled with functional diarrhea actually have bile acid malabsorption.
- Hormonal impact: The cortisol awakening response can boost colonic motility by as much as 50 percent within the first hour after waking.
- Transit time: A normal colonic transit takes 30 to 40 hours, but patients with morning urgency often clear their gut in under 15 hours.
- Diagnostic accuracy: The fecal calprotectin test offers about 93 percent sensitivity for detecting active Inflammatory Bowel Disease.
- Dietary success: The low-FODMAP diet improves morning symptoms in up to 75 percent of compliant patients.
The Physiology of Morning Digestion
To understand why your stomach goes haywire at dawn, it helps to know how a healthy gut actually operates. Your digestive tract isn’t just a passive tube. It’s a sensitive organ system with its own dedicated nervous network, called the enteric nervous system.
While you sleep, your gut slows down and shifts into a maintenance phase. It absorbs water, tidies up leftover debris, and quietly moves things along. When you wake up, this slow mode ends almost instantly. Your body flips from rest to high alert in minutes.
Understanding this baseline helps us figure out exactly where things are going wrong in your digestion. Here’s what’s really happening in those first few hours of the morning.
The Cortisol Awakening Response and Gut Motility
Every morning, your body releases a big surge of cortisol, the main stress hormone. This is known as the cortisol awakening response, and it usually peaks within 30 to 45 minutes of opening your eyes.
That hormone spike is meant to make you alert and ready for the day. But cortisol also acts directly on your enteric nervous system, stimulating the smooth muscles in your colon and triggering bowel contractions.
For most people, this simply leads to a normal morning bowel movement. For those with a sensitive gut, though, the cortisol surge sparks violent spasms. Stool gets pushed through too fast, water never gets properly absorbed, and the result is loose, urgent stools.
Expert insight: If you wake up feeling anxious or on edge, your cortisol response is probably amplified. A few minutes of slow, deep breathing before you even get out of bed can genuinely reduce colonic spasms.
Understanding the Gastrocolic Reflex
Another big player is the gastrocolic reflex. This is an involuntary signal that tells your colon to make room whenever new food enters your stomach. When your stomach stretches, a neural message travels down to your lower intestines, telling them to empty.
This reflex is completely normal. The problem starts when someone develops visceral hypersensitivity, where the gut nerves overreact to even mild stretching.
In that case, the gastrocolic reflex goes into overdrive. A sip of coffee or a bite of toast can trigger massive colonic contractions, leaving you racing to the bathroom seconds after breakfast.
Circadian Rhythm and the Microbiome
Your gut bacteria also follow a strict 24-hour clock. This internal rhythm controls how your microbiome ferments food. Overnight, bacteria in your large intestine feed on leftover carbohydrates from dinner.
When this balance tips the wrong way, we call it microbiome dysbiosis. Dysbiosis leads to excessive overnight fermentation, producing large amounts of gas and short-chain fatty acids while you sleep.
By morning, your colon is stuffed with irritating byproducts and trapped gas. Your body responds with a rapid purge. This is why fixing your evening meals often matters more than changing breakfast.
The Vagus Nerve Connection
The vagus nerve is the biological highway between your brain and your digestive tract. It controls your “rest and digest” functions, and when its tone is poor, digestion becomes erratic.
Stress hits this nerve hard. If you go to bed wound up, your vagus nerve can’t regulate overnight digestion properly, and your colon is already jittery by morning.
Improving vagal tone is a major focus in modern gastroenterology. Simple habits like humming, gargling water, or slow diaphragmatic breathing can all stimulate this nerve. A calmer vagus nerve means a calmer gut.
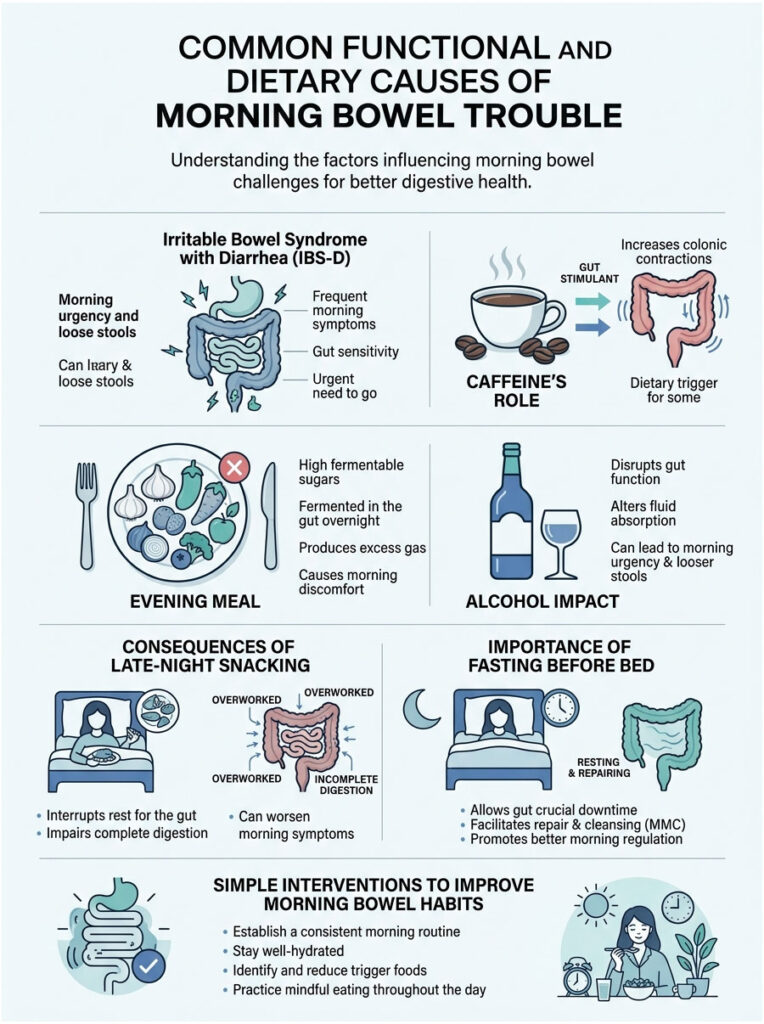
Common Functional and Dietary Causes
When investigating morning bowel trouble, we usually start with functional and dietary factors. They’re the most common culprits, and while they aren’t life-threatening, they can seriously drag down your quality of life.
Many patients spend years chasing a specific food allergy when the real problem is how the gut behaves as a whole. Functional disorders mean your gut looks normal on a scan but doesn’t work normally. The nerves and muscles simply don’t coordinate the way they should.
Irritable Bowel Syndrome with Diarrhea (IBS-D)
IBS-D is one of the most common functional gut disorders in the USA. We diagnose it using the Rome IV clinical criteria, which require recurrent abdominal pain linked to changes in stool frequency or form.
These patients almost always feel worst in the morning. They often pass Bristol Stool Scale Type 6 or 7 stools (fluffy with ragged edges, or completely watery).
A hallmark sign is that cramping tends to improve right after going. Once the morning storm passes, many patients feel fine for the rest of the day, until the whole cycle restarts tomorrow.
Dietary Triggers, Caffeine, and Osmotic Shifts
What you eat and drink plays a huge role in your morning routine. Caffeine is a notorious trigger for sensitive stomachs. It stimulates the release of gastrin, a hormone that cranks up colonic activity.
Your evening meals matter just as much. Foods loaded with fermentable sugars pull extra water into the intestines overnight, creating what we call osmotic diarrhea.
Artificial sweeteners like sorbitol are powerful osmotic laxatives. If you snack on diet sodas or sugar-free candies before bed, you’re practically setting an alarm for an urgent bathroom visit.
The Impact of Alcohol on Morning Bowel Habits
Alcohol is highly disruptive to normal gut function. Evening drinking blocks anti-diuretic hormone, which prevents your colon from properly absorbing water from stool.
Alcohol also breaks down into toxic byproducts like acetaldehyde, which directly irritate the gut lining. Your body treats these as threats and tries to flush them out fast.
That’s the mechanism behind the infamous morning-after urgency. Even a single glass of wine before bed can shift your gut motility enough to cause diarrhea the next morning.
The Role of Late-Night Snacking
Eating right before bed is rough on your digestive health. Your gut needs a solid fasting window to run the migrating motor complex, a sweeping wave that cleans out the small intestine.
Late-night eating interrupts that cleanup. Food sits stagnant, ferments, and produces excess gas. By morning, your colon is overwhelmed with partly digested, overly fermented material.
The gastrocolic reflex then kicks in the moment you wake up, and the result can be explosive. Stopping all food at least three hours before bed is a simple but highly effective intervention.
Overlooked Clinical Causes Beyond IBS
Here’s the truth most patients don’t hear: not all morning urgency is IBS. Plenty of people are labeled with a functional disorder when they actually have a treatable organic condition. I always look for these hidden causes.
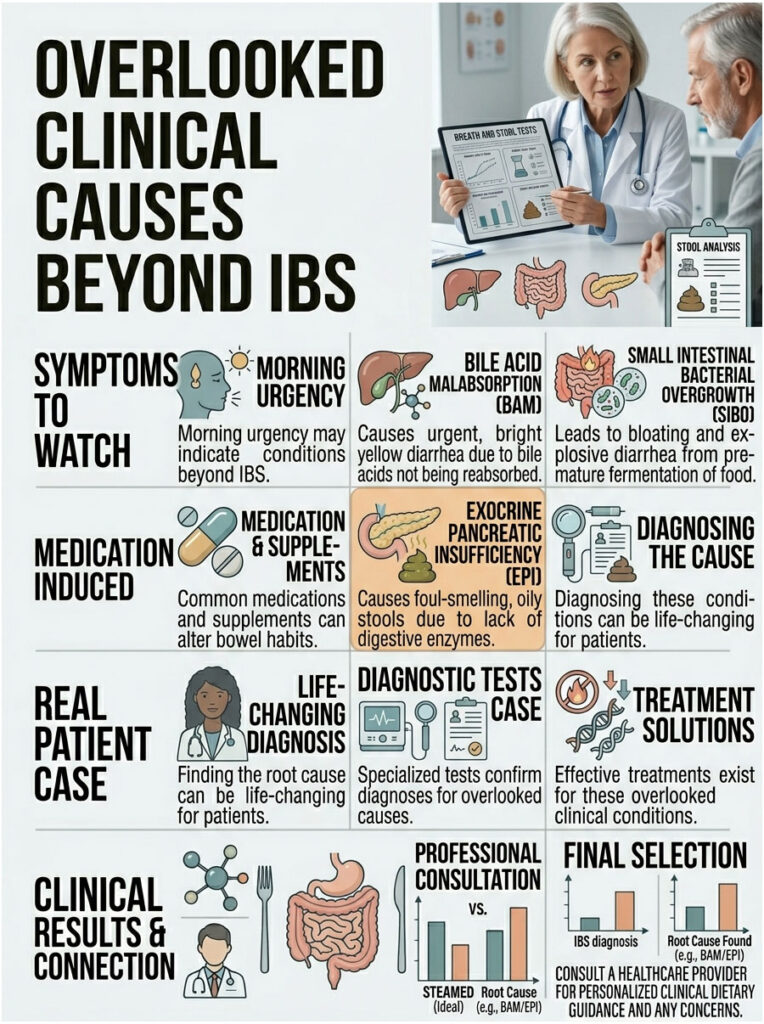
If diet and stress management haven’t worked, we need to look further. The following conditions are often missed in general practice, and diagnosing them can be life-changing.
Bile Acid Malabsorption (BAM)
Bile acid malabsorption is remarkably common yet frequently missed. Your liver makes bile acids to help digest fats. Normally, these acids do their job in the small intestine and get reabsorbed in the terminal ileum for reuse.
In BAM, that reabsorption fails. Harsh, acidic bile spills into the large intestine, which isn’t built to handle it. The acids act like a potent laxative.
The giveaway is bright yellow, greasy, urgent morning diarrhea. Because bile is produced overnight, the highest concentration hits the colon right when you wake up. Thankfully, BAM responds well to specific binding medications.
Small Intestinal Bacterial Overgrowth (SIBO)
SIBO happens when bacteria from the large intestine migrate upward into the small intestine, which is meant to stay relatively sterile. Once there, they ferment your food early.
That premature fermentation creates large amounts of hydrogen and hydrogen sulfide gas, which build up overnight. The pressure stimulates the gastrocolic reflex aggressively when you wake up.
Patients with SIBO often wake up badly bloated and only feel relief after explosive morning diarrhea. A specialized breath test confirms the diagnosis, and targeted antibiotic therapy usually resolves it.
Medication and Supplement-Induced Diarrhea
Sometimes the cause is sitting right in your medicine cabinet. Plenty of over-the-counter supplements and prescription drugs alter bowel habits, especially when taken at bedtime.
Magnesium-induced diarrhea is a classic example. Many people take magnesium at night for sleep or muscle cramps, but forms like magnesium citrate or oxide draw water into the bowel overnight.
Other common offenders include some antidepressants, which raise serotonin in the gut, and metformin, a diabetes medication known for morning GI distress. Always review your medication list with your doctor.
Exocrine Pancreatic Insufficiency (EPI)
EPI is a condition where the pancreas doesn’t produce enough digestive enzymes. Without them, your body can’t break down fats, proteins, or carbohydrates properly. Undigested food rushes into the colon.
When undigested fat reaches the colon, it causes steatorrhea: foul-smelling, pale, oily stools that often float and are hard to flush.
Because dinner is usually the heaviest meal, undigested fat sits in the gut overnight. By morning, the colon forcefully expels it. A simple stool test called fecal elastase helps confirm the diagnosis.
Diagnostic Differentiation: Functional vs. Organic Disease
When a patient asks me, “Why do I have diarrhea every morning?”, my first job is separating functional disorders from organic diseases. Functional means the gut looks normal but works abnormally. Organic means there’s actual, visible tissue damage.
This distinction matters enormously. Treating an organic disease as if it were functional can lead to serious complications. Think of it like troubleshooting a car: a functional issue is a software glitch, an organic issue is a broken engine part.
Recognizing Inflammatory Bowel Disease (IBD)
Inflammatory Bowel Disease mainly includes Crohn’s Disease and Ulcerative Colitis. These are serious autoimmune conditions where the body attacks its own intestinal lining, causing ulcers and chronic bleeding.
When the gut lining is inflamed, it loses its ability to absorb fluids properly. The result is persistent watery output no matter what you eat. Unlike functional issues, this involves real tissue destruction and needs aggressive medical treatment.
IBD patients often have other symptoms too, like severe joint pain, chronic fatigue, and unexplained weight loss. If these show up alongside morning urgency, you need a full medical workup.
Morning Urgency vs. Nocturnal Diarrhea
One of the first questions I ask every new patient is whether their symptoms ever wake them up from deep sleep. This is a major dividing line in gastroenterology.
Functional disorders like IBS almost never interrupt sleep. If you’re waking up at 3:00 AM to rush to the bathroom, that’s a serious red flag. It means the drive to empty your colon is overriding the normal circadian rhythm that should keep you asleep.
This pattern usually points to organic disease rather than a functional issue. It warrants immediate investigation to rule out infection, microscopic colitis, or IBD.
Comparison Table 1: Functional vs. Organic Bowel Disorders
| Clinical Feature | Functional Disorder (e.g., IBS-D) | Organic Disease (e.g., Crohn’s) |
|---|---|---|
| Primary symptom timing | Waking hours, especially early mornings | Anytime, including deep sleep |
| Nocturnal symptoms | Extremely rare | Common and highly indicative of damage |
| Stool characteristics | Loose, watery, sometimes clear mucus | Bloody, purulent, chronic watery output |
| Pain profile | Cramping that eases after defecation | Severe localized pain, joint pain, systemic issues |
| Unintended weight loss | Highly unlikely | Common and concerning |
| Fecal calprotectin | Normal range (no inflammation) | Elevated (active inflammation) |
If you have organic warning signs, don’t assume your symptoms are just an annoyance. Delaying diagnosis for something like Crohn’s disease can cause irreversible bowel damage. Be honest with your doctor about what you’re actually seeing in the toilet.
When to Worry: Red Flags That Need Immediate Evaluation
Passing Type 6 or 7 stools every morning is frustrating, but it isn’t always dangerous. Many people live with functional bowel issues for decades without it shortening their lifespan. That said, certain symptoms change the picture entirely.
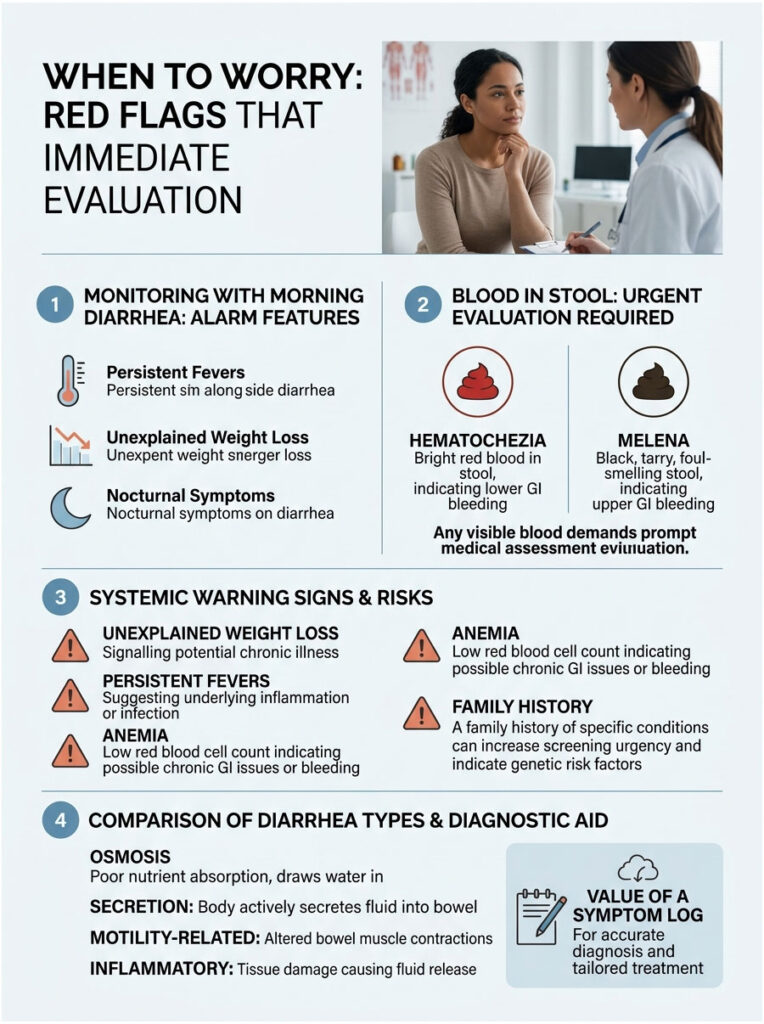
We call these alarm features. If you notice any of them alongside your morning diarrhea, stop self-treating and get evaluated. Ignoring them can turn a manageable issue into an emergency.
Identifying Hematochezia and Melena
Blood in your stool is never normal. Hematochezia is bright red blood visible in the toilet bowl or on toilet paper, usually from bleeding in the lower GI tract (colon or rectum).
Melena looks different: black, tarry, and incredibly foul-smelling. It indicates bleeding higher up, such as a stomach ulcer. The blood turns black as it’s digested on its way through the intestines.
Both require urgent investigation. They can signal severe IBD, bleeding polyps, or even colorectal cancer. Never ignore visible changes in stool color.
Systemic Warning Signs and Unexplained Weight Loss
You should also pay attention to symptoms affecting your whole body. Losing more than ten pounds without trying is a major warning sign, suggesting either malabsorption or a serious disease process.
Persistent low-grade fevers can point to ongoing infection or inflammation. Anemia picked up on routine bloodwork is another big flag, hinting that you might be losing blood microscopically through your GI tract every day.
A strong family history of colon cancer or celiac disease also raises your risk significantly. If close relatives have these conditions, your morning symptoms deserve more aggressive screening and earlier investigation.
Comparison Table 2: Types of Diarrhea and Their Mechanisms
| Classification | Mechanism | Common Morning Triggers |
|---|---|---|
| Osmotic diarrhea | Unabsorbed substances pull water into the colon | Sorbitol, excess lactose, nighttime magnesium supplements |
| Secretory diarrhea | Gut actively secretes electrolytes and water | Bile acid malabsorption, bacterial toxins from food poisoning |
| Motility-related | Rapid transit prevents water absorption | Hyperactive gastrocolic reflex, morning anxiety, hyperthyroidism |
| Inflammatory | Damage to mucosal lining impairs absorption | Ulcerative Colitis, Crohn’s Disease, severe infections |
Identifying which category fits your symptoms lets us tailor treatment. Osmotic diarrhea responds beautifully to dietary changes. Secretory diarrhea, on the other hand, won’t budge with diet alone.
This is why keeping a symptom log is so valuable. Tracking food, stool consistency, and timing gives us the clues needed to categorize your condition quickly and accurately.
How Gastroenterologists Investigate Morning Diarrhea
When you walk into my clinic with morning diarrhea, we don’t guess. We follow a structured, evidence-based diagnostic roadmap to rule out dangerous conditions before settling on a functional diagnosis.
Modern medicine offers excellent tools for testing gut function. Most workups start with simple, non-invasive tests and only escalate if needed. The good news is that much of the initial testing can be done without leaving home.
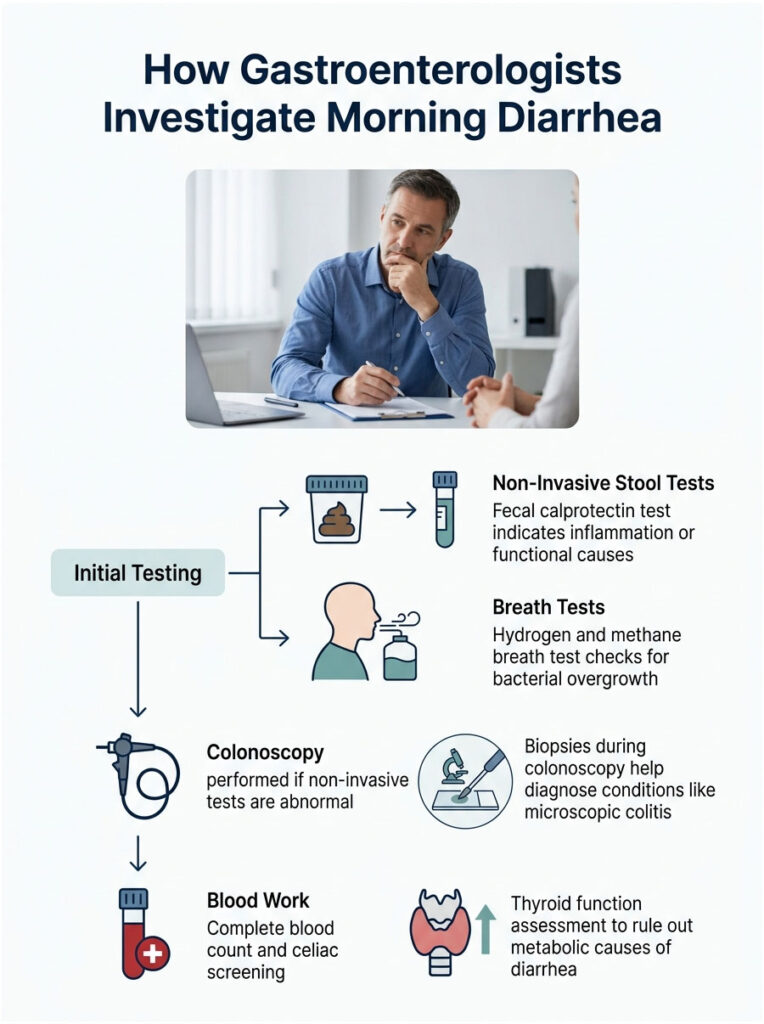
Non-Invasive Stool and Breath Testing
Step one is almost always the fecal calprotectin test. Calprotectin is a protein released by white blood cells called neutrophils. When the gut is inflamed, these cells shed the protein into your stool.
A negative result strongly suggests a functional cause. A positive result points toward IBD and active inflammation. This simple test saves thousands of patients from unnecessary invasive procedures.
If we suspect bacterial overgrowth, we order a hydrogen and methane breath test. You drink a specific sugar solution and we measure the gases you exhale over three hours. Early gas spikes confirm that bacteria are fermenting food prematurely in the small intestine.
The Role of Endoscopy and Colonoscopy
If non-invasive tests are abnormal or red flags are present, colonoscopy becomes necessary. Current guidelines for chronic diarrhea often require direct mucosal biopsy. Sometimes we simply need to see the tissue ourselves.
Colonoscopy lets us check for ulcers, bleeding polyps, or tumors. Just as importantly, we take painless tissue samples during the procedure. These biopsies catch microscopic colitis, which causes severe watery diarrhea despite a normal-looking colon.
An upper endoscopy may also be done to examine the stomach and small intestine. Biopsies of the small intestine check whether the villi have flattened, a classic sign of celiac disease.
Blood Work and Celiac Screening
A thorough blood panel gives us a full-body view. We check your complete blood count for hidden anemia or elevated white cells, and your metabolic panel to make sure electrolytes aren’t depleted from chronic diarrhea.
Celiac screening is a must for anyone with chronic diarrhea. A blood test looks for tissue transglutaminase antibodies. If these are elevated, your immune system is attacking your gut whenever you eat gluten.
We also check thyroid stimulating hormone. An overactive thyroid accelerates metabolism, including bowel transit time. Treating a thyroid problem alone often resolves morning bowel urgency without any gut-specific therapy.
Evidence-Based Treatments and Practical Strategies
Once we have a clear diagnosis, treatment becomes targeted. The goal is to calm the nervous system, regulate motility, and restore normal stool form. Popping anti-diarrheal pills every morning is a band-aid, not a real solution.
A multi-layered approach works best: dietary changes, strategic supplementation, and specific medications, all working together. Here are the protocols I use with my own patients.
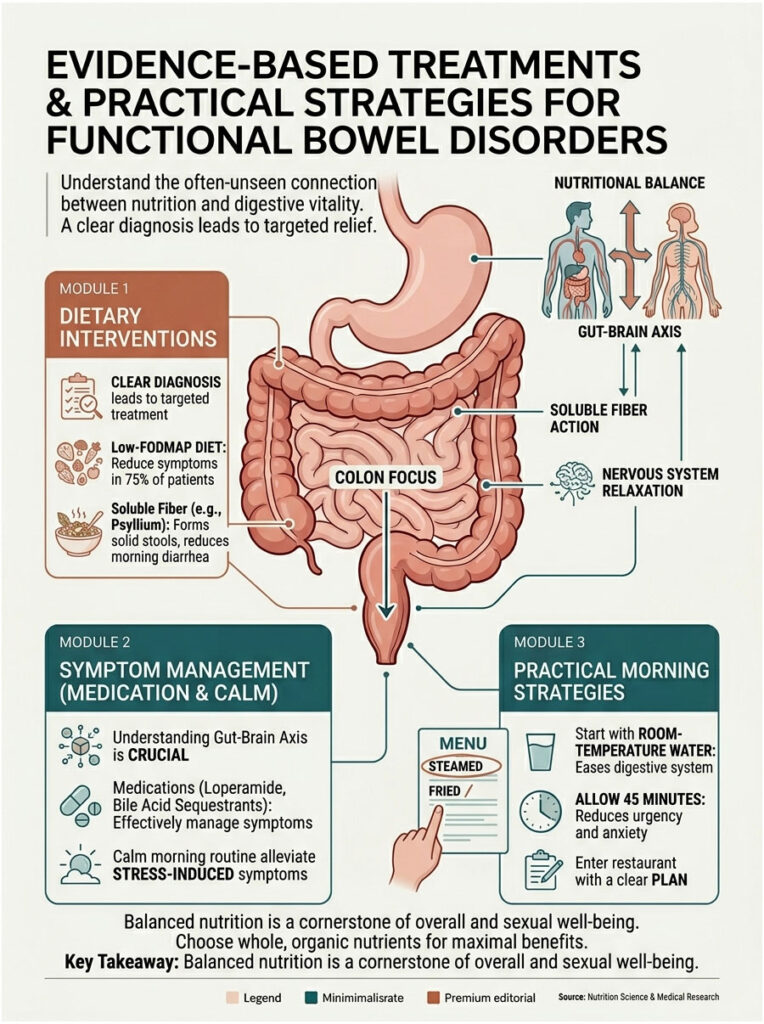
Dietary Interventions and the Low-FODMAP Diet
Dietary modification is the cornerstone of managing functional bowel disorders. The low-FODMAP diet reduces symptoms in up to 75 percent of compliant patients. It temporarily eliminates short-chain carbohydrates that ferment easily in the gut.
By removing these sugars from your evening meals, you prevent overnight dysbiosis. You wake up with less trapped gas, and the gastrocolic reflex loses much of its punch. After a strict elimination phase, foods are slowly reintroduced to pinpoint personal triggers.
For post-meal urgency, I recommend a low-residue, gut-friendly breakfast. Plain oatmeal, a ripe banana, or a slice of sourdough toast are gentle on the stomach and far less likely to trigger colonic spasms.
Strategic Fiber Titration
Fiber is tricky when you’re dealing with morning diarrhea. Many people eat tons of roughage hoping it’ll bulk their stool, but insoluble fiber acts like a scrub brush, irritating a sensitive colon and making things worse.
The better option is soluble fiber, which dissolves in water to form a soothing gel. That gel slows transit and absorbs excess fluid, helping form solid stools.
A soluble fiber supplement like pure psyllium husk taken at night can work wonders. It quietly absorbs excess water while you sleep and often prevents watery morning outputs altogether.
Pharmacological and Medical Interventions
When diet and fiber aren’t enough, targeted medications step in. For hyperactive guts, over-the-counter Loperamide can safely slow motility. It binds to opioid receptors in the gut wall, giving the colon more time to absorb water.
For confirmed bile acid malabsorption, we prescribe bile acid sequestrants like cholestyramine. These bind the irritating bile acids tightly, rendering them harmless. The yellow, urgent morning diarrhea often resolves almost overnight.
For SIBO, we use gut-specific antibiotics like Rifaximin. Unlike broad antibiotics, Rifaximin stays inside the digestive tract. It clears the overgrown bacteria and stops the overnight fermentation at its source.
Managing the Gut-Brain Axis
You can’t ignore the link between your brain and your gut. The vagus nerve is a direct line between your emotional center and your digestive tract. Calming visceral hypersensitivity means actively calming that pathway.
To blunt an exaggerated cortisol response, build a slower, calmer morning routine. Skip the phone and the stressful news the instant you wake up. Gentle stretching or a few minutes of meditation can prevent that big hormone spike.
For severe cases, I often recommend gut-directed hypnotherapy or cognitive behavioral therapy. Both are clinically proven to retrain the brain to ignore normal digestive signals, which dramatically reduces morning urgency.
Creating a Gut-Friendly Morning Routine
Your morning routine sets the tone for the entire day. Jumping out of bed and chugging hot coffee is a recipe for disaster. Wake up gently, and give your nervous system time to adjust.
Start with a glass of room-temperature water. Cold water can shock the stomach and trigger aggressive spasms. Room-temperature water gently wakes the digestive tract and eases in the gastrocolic reflex.
Give yourself at least 45 minutes between waking up and leaving the house. That buffer lets you use the bathroom without rushing, and knowing you have time actually reduces the stress that’s triggering the diarrhea in the first place.
Key Takeaways
Occasional loose stools are just part of life. But constantly asking, “Why do I have diarrhea every morning?” means there’s a chronic pattern worth addressing. Your body is telling you something in its daily rhythm is off.
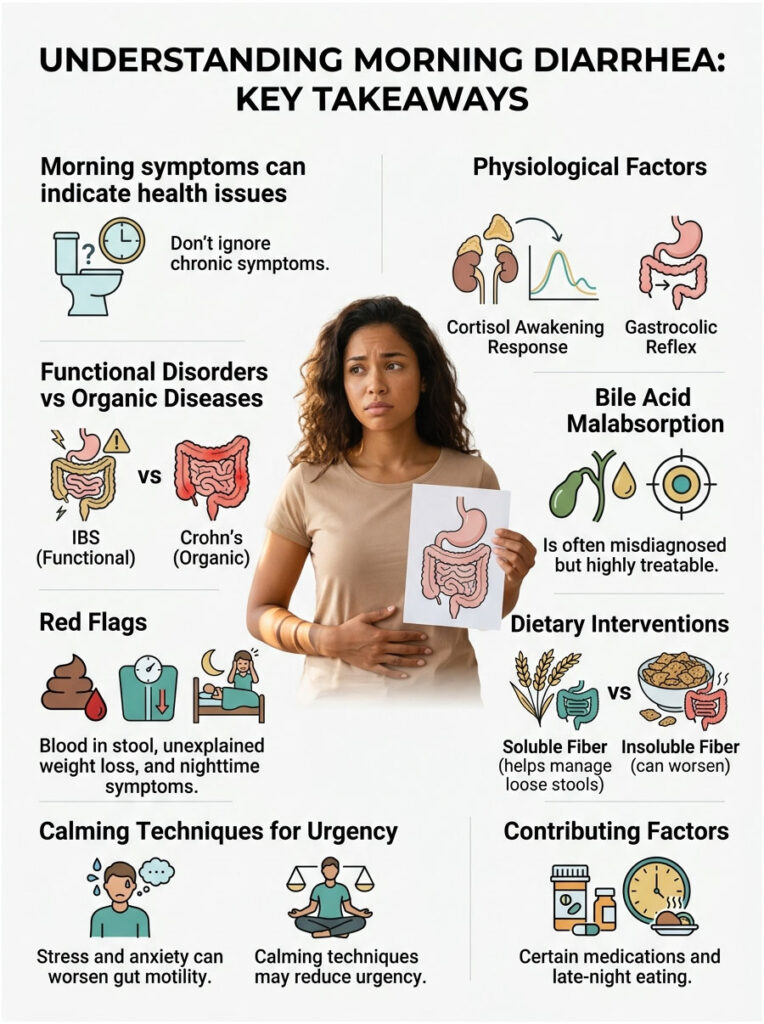
We’ve covered how the cortisol awakening response and an amplified gastrocolic reflex can wreck your mornings. We’ve also separated functional issues like IBS from serious organic conditions like Crohn’s disease. Knowing your own biology is the first real step toward feeling better.
Hidden conditions like bile acid malabsorption are frequently missed but highly treatable. If you notice red flags like nighttime symptoms, blood in your stool, or unexplained weight loss, get medical care right away. You don’t have to spend your life tied to the bathroom.
Frequently Asked Questions
Why do I experience a sudden urge to use the bathroom specifically in the morning?
This phenomenon is primarily driven by two physiological events: the cortisol awakening response and the gastrocolic reflex. Upon waking, your body releases a surge of cortisol that stimulates colonic motility. When you subsequently eat or drink, the gastrocolic reflex triggers contractions to clear the lower intestines. In patients with visceral hypersensitivity, these normal processes become exaggerated, leading to urgent, loose stools.
Can bile acid malabsorption (BAM) be mistaken for Irritable Bowel Syndrome (IBS-D)?
Yes, clinical research indicates that up to 30 percent of patients diagnosed with functional diarrhea actually suffer from bile acid malabsorption. The hallmark of BAM is urgent, bright yellow, or greasy morning diarrhea caused by the liver’s bile acids spilling into the colon rather than being reabsorbed. Unlike IBS-D, this condition typically requires specific bile acid sequestrant medications for resolution.
What are the clinical ‘red flags’ that indicate morning diarrhea requires urgent evaluation?
As a gastroenterologist, I look for ‘alarm features’ such as hematochezia (bright red blood), melena (black, tarry stools), unexplained weight loss, or persistent low-grade fevers. Most importantly, if your diarrhea symptoms wake you up from a deep sleep—known as nocturnal diarrhea—it strongly suggests an organic disease like Inflammatory Bowel Disease (IBD) rather than a functional disorder like IBS.
How does the cortisol awakening response affect my gut motility?
The cortisol awakening response is a hormonal surge that occurs within the first 30 to 45 minutes of waking. Cortisol acts directly on the enteric nervous system, stimulating the smooth muscles of the colon to contract. For those with a sensitive gut, this hormonal peak can cause violent spasms that push stool through the colon too quickly for proper water absorption, resulting in diarrhea.
Why is the distinction between functional and organic bowel disorders so important?
Functional disorders, like IBS-D, mean the gut’s ‘software’ is glitching but the tissue looks healthy. Organic diseases, such as Crohn’s or Ulcerative Colitis, involve physical damage, ulcers, and inflammation of the intestinal lining. Treating an organic disease with only lifestyle changes can lead to irreversible bowel damage, which is why we use tools like the fecal calprotectin test to differentiate between the two.
Can Small Intestinal Bacterial Overgrowth (SIBO) cause explosive morning diarrhea?
Absolutely. In SIBO, bacteria from the large intestine migrate into the small intestine and ferment food prematurely. This process produces excessive hydrogen and methane gases overnight. By morning, the physical pressure from this trapped gas aggressively stimulates the gastrocolic reflex, leading to severe bloating followed by an urgent morning purge.
Does my morning coffee contribute to gastrointestinal urgency?
Caffeine is a potent pharmacological trigger for the gut. It stimulates the release of gastrin, a hormone that increases motor activity throughout the colon. For individuals with a hyperactive gastrocolic reflex, the combination of morning cortisol and the gastrin surge from coffee often creates a ‘perfect storm’ for immediate post-prandial diarrhea.
How does late-night snacking impact my digestion the following morning?
Eating late at night interrupts the Migrating Motor Complex (MMC), a vital ‘sweeping’ wave that cleans the small intestine during fasting. When you eat before bed, food sits stagnant and ferments overnight. By morning, the colon is overwhelmed with irritants and partially digested matter, which triggers an aggressive evacuation response as soon as you wake up.
What is the role of the fecal calprotectin test in diagnosing chronic diarrhea?
Fecal calprotectin is a protein marker for intestinal inflammation. With a 93 percent sensitivity rate, it is an essential non-invasive tool for detecting active Inflammatory Bowel Disease. If your levels are normal, we can be more confident that your morning diarrhea is functional (like IBS) rather than caused by autoimmune damage or infection.
Is it better to use soluble or insoluble fiber to manage morning loose stools?
For morning diarrhea, you should focus on soluble fiber, such as psyllium husk. Unlike insoluble fiber, which can act as a mechanical irritant, soluble fiber dissolves into a soothing gel that absorbs excess water and slows down colonic transit time. Taking a soluble fiber supplement at night can help ‘bulk’ the stool while you sleep, leading to more formed movements in the morning.
How can managing the ‘gut-brain axis’ reduce morning bathroom trips?
The vagus nerve serves as the primary communication highway between your brain and gut. Stress and morning anxiety impair vagal tone, making the gut highly reactive to cortisol. Implementing a calming morning routine and diaphragmatic breathing can stimulate the parasympathetic nervous system, which helps blunt the spasms responsible for morning urgency.
Can common medications or supplements cause diarrhea upon waking?
Yes, several substances can trigger osmotic diarrhea. Magnesium supplements taken at night for sleep are a frequent culprit, as they draw water into the bowel overnight. Other medications, including Metformin for diabetes and certain SSRI antidepressants, are clinically known to alter gut motility and contribute to chronic morning gastrointestinal distress.
Disclaimer
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The “Why Do I Have Diarrhea Every Morning?” clinical roadmap is intended to provide educational context regarding gastrointestinal physiology. Always consult a qualified healthcare professional or board-certified gastroenterologist before making changes to your medication, diet, or health regimen, especially if you experience “red flag” symptoms.
References
- American College of Gastroenterology (ACG) – Clinical Guidelines for the Management of Irritable Bowel Syndrome – Provides the evidence-based framework for IBS-D diagnosis and treatment.
- American Gastroenterological Association (AGA) – Research on Bile Acid Malabsorption – Cited regarding the 30% misdiagnosis rate in functional diarrhea patients.
- Journal of Clinical Medicine – “The Cortisol Awakening Response and its Impact on Colonic Motility” – Supports the hormonal link to morning bowel urgency.
- Rome Foundation – Rome IV Criteria for Functional Gastrointestinal Disorders – The gold standard for categorizing and diagnosing functional gut issues.
- Monash University – Low-FODMAP Diet Research – Supports the 75% success rate for dietary intervention in IBS-D patients.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – Chronic Diarrhea in Adults – Provides statistical data on prevalence and common organic causes.