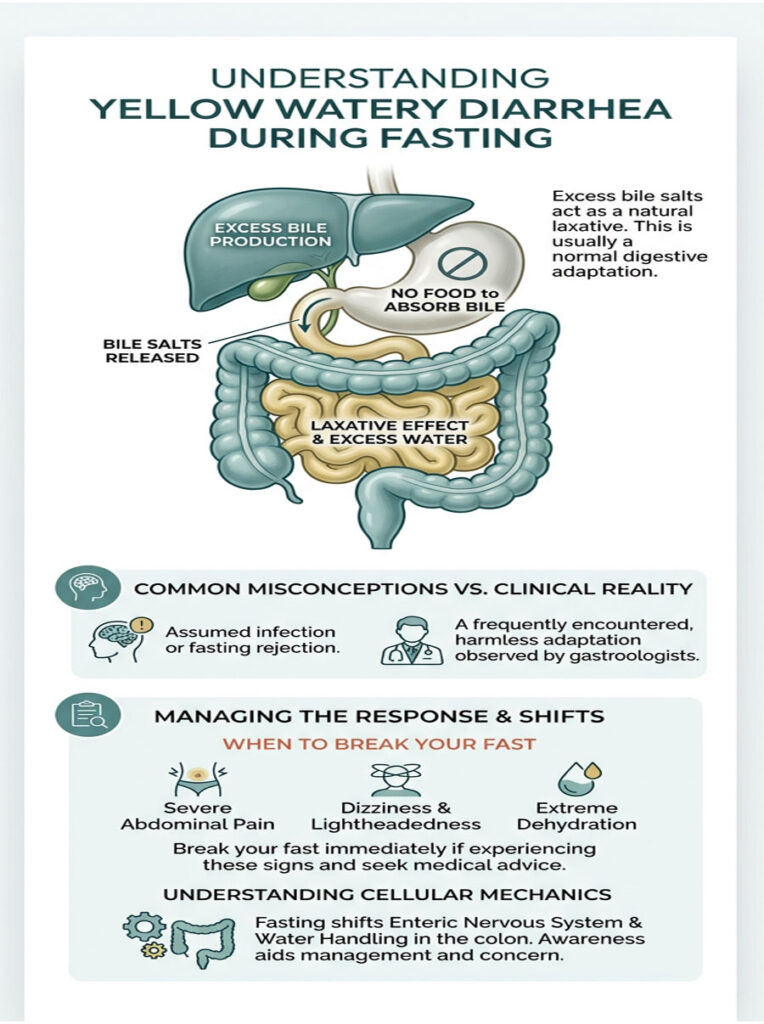
Yellow watery diarrhea while fasting is typically caused by bile dumping, glycogen water release, and electrolyte imbalances. Without food to absorb digestive juices, excess bile salts reach the colon and act as a natural laxative. This is usually a harmless adaptation, but you should break your fast immediately if you experience severe abdominal pain, dizziness, or signs of extreme dehydration.
Table of Contents
A patient recently sat across from me in my gastroenterology clinic, visibly anxious and clutching a water bottle. She told me her 72-hour water fast had been interrupted by a terrifying trip to the bathroom. This is not unusual. Yellow watery diarrhea while fasting is one of the most common, yet deeply misunderstood, digestive events that sends people to my office every year. Most assume their body is rejecting the fast or that they have caught a stomach bug.
Here is the truth. This symptom is rarely a sign of infection or organ failure. It is almost always a predictable mechanical response from a digestive tract adapting to a sudden lack of calories. When you shift from a fed state to a fasted state, your entire gastrointestinal system undergoes a major metabolic transition.
The absence of incoming food drastically changes your enteric nervous system, your biliary tree, and the way the colon handles water. As a board-certified gastroenterologist with over 15 years of clinical experience, I see this exact panic weekly. Patients are blindsided because popular fasting guides rarely discuss the messy, uncomfortable reality of digestive adaptation.
In this article, we are going to break down the exact cellular mechanics behind why your liver and gallbladder react this way when deprived of calories. You will learn the role of electrolytes, the specific warning signs that demand immediate medical attention, and the clinical protocols you can use to manage these symptoms safely.
Key Clinical Statistics on Fasting and Digestion
- Daily Bile Production: The liver continuously produces 800ml to 1,000ml of bile every day, according to the National Institutes of Health (NIH).
- Glycogen Water Weight: Every 1 gram of stored glycogen binds approximately 3 grams of water.
- Gallbladder Volume: During a 72-hour fast, resting gallbladder volume can increase by up to 40% due to biliary retention.
- Transit Time: Liquid bile can travel from the duodenum to the rectum in as little as 45 minutes during an active fasting flush.
- Electrolyte Absorption: The human colon can absorb up to 5 liters of fluid per day.
- Osmotic Overload: Sudden osmotic shifts from salt supplements can overwhelm colonic absorption within 20 minutes.
- Bile Acid Malabsorption: Up to 30% of unexplained functional diarrhea cases are linked to unabsorbed bile acids, per the American College of Gastroenterology.
The Physiology Behind Yellow Watery Diarrhea While Fasting
To understand why the body reacts so aggressively during a fast, you need to look at the microscopic mechanics of your digestive organs. The gastrointestinal tract is not a passive tube sitting idle. It is a highly active, hormone-driven system that expects a regular delivery of macronutrients. When food stops arriving, the system has to adapt quickly to survive.
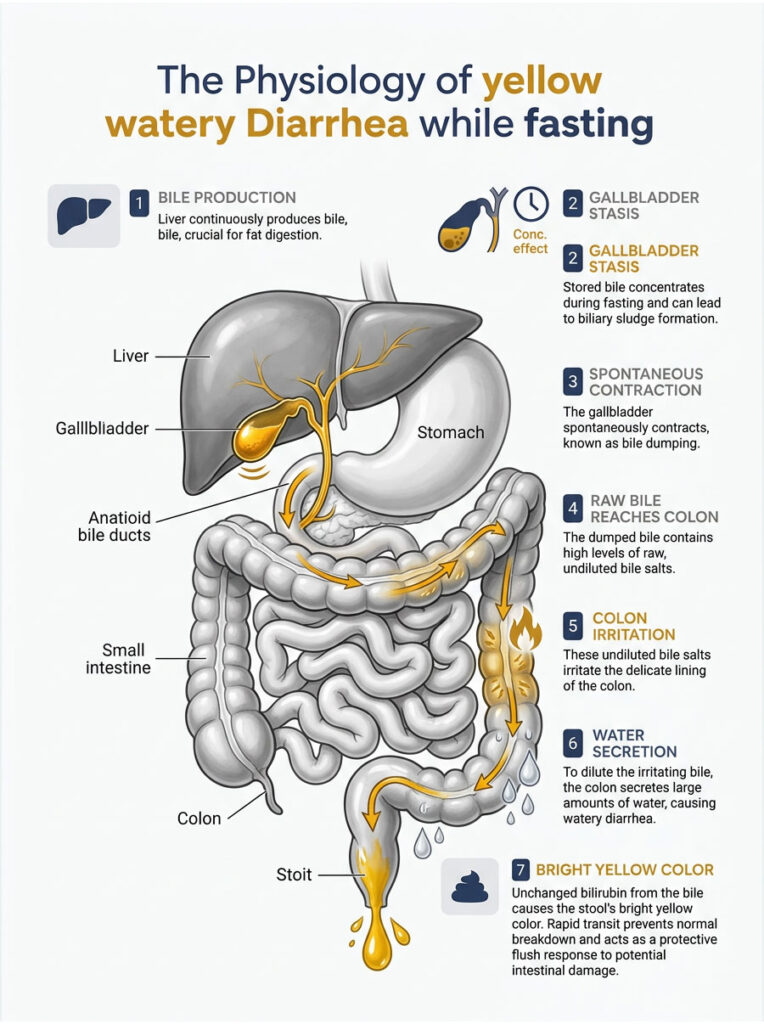
The Liver Never Stops Making Bile
Your liver is a chemical factory that never shuts down. One of its primary jobs is the continuous production of bile, a greenish-yellow, alkaline fluid essential for breaking down dietary fats and absorbing fat-soluble vitamins.
Under normal feeding conditions, bile flows down the hepatic duct and gets stored in the gallbladder. The gallbladder acts as a specialized storage balloon, concentrating the bile by pulling water and electrolytes out while you wait for your next meal.
During a fast, you are not consuming any dietary fats. Without fat to trigger hormonal signals, the gallbladder does not receive the cue to empty. This leads to a well-documented clinical state known as gallbladder stasis.
Gallbladder Stasis and Biliary Sludge
As the fast progresses, bile simply sits in the gallbladder, becoming thicker and more concentrated by the hour. On abdominal ultrasounds, we frequently see this as biliary sludge, an incredibly common finding in patients who practice prolonged water fasting.
Gallbladder stasis is usually temporary, but it sets the stage for digestive trouble. The liver keeps producing fresh bile, the gallbladder keeps storing it, and internal pressure within the biliary tree builds steadily. Eventually, this concentrated, pressurized fluid has to go somewhere.
Picture a water balloon attached to a slowly dripping faucet. The balloon stretches to hold the water for a while, but once it reaches capacity, pressure forces the fluid out through the path of least resistance.
Bile Dumping: The Spontaneous Gallbladder Squeeze
Normally, eating a fat-containing meal triggers the release of Cholecystokinin (CCK), a hormone that tells the gallbladder to contract and squirt bile into the small intestine. The chewed food acts like a sponge, soaking up bile salts so they can do their job and eventually get recycled back to the liver.
During a fast, the enteric nervous system sometimes misfires. It triggers a spontaneous gallbladder contraction even without CCK or food present. In the medical community, we call this sudden, inappropriate release bile dumping.
When bile dumping happens on an empty stomach, a concentrated wave of acidic bile salts floods the small intestine. With no food to bind to, those salts stay in their raw, caustic form and travel rapidly toward the large intestine.
What Bile Does to the Colon
When raw, unabsorbed bile salts reach the colon, they cause immediate disruption. The delicate mucosal lining treats excess bile salts as a dangerous chemical irritant, a toxin that must be flushed out as quickly as possible.
In response, the colon actively secretes large volumes of water and electrolytes into its lumen to dilute and expel the irritant. Normal water absorption stops completely. This creates a temporary, localized form of bile acid malabsorption.
The result is sudden, urgent, and often painful. This mechanism produces a violent bout of fasting diarrhea that can wake you from sleep. It is an active defense system your body deploys to protect the intestinal lining from chemical damage.
Why the Stool Is Bright Yellow
The neon yellow color alarms most of my fasting patients. People call my emergency line thinking their liver is failing. The explanation is actually straightforward chemistry.
The color comes from bilirubin, a natural byproduct of red blood cell breakdown that your body excretes through bile. Bilirubin carries a bright yellowish-green pigment.
When you eat normally, bile moves slowly through the 20 feet of digestive tract. Gut bacteria have time to break down yellow bilirubin into stercobilin, the chemical responsible for the typical brown color of healthy stool.
During bile dumping, transit is so fast that bacteria never get the chance to oxidize the pigment. The bright yellow fluid you see is proof that raw bile has passed through your system completely unchanged.
Primary Triggers for Fasting Bowel Issues
Now that we understand the role of bile, we need to look at the specific triggers behind sudden bowel movements during a fast. This rarely comes down to one isolated factor. It is usually a perfect storm of metabolic switching, massive water release, and supplementation errors.
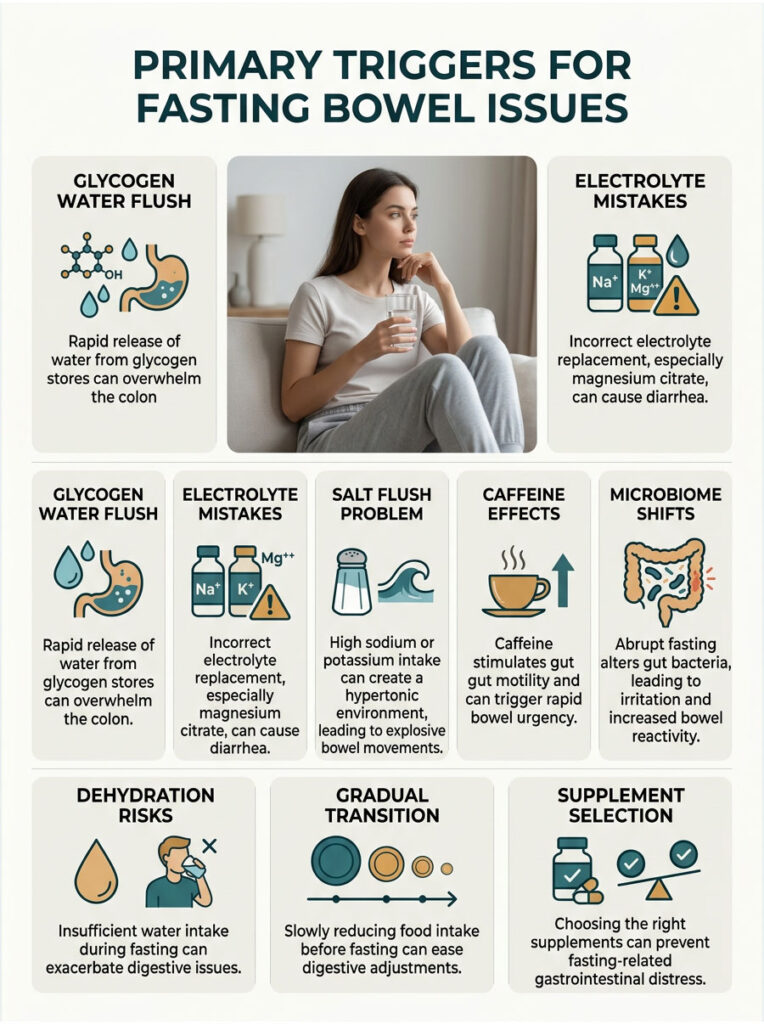
The Glycogen Water Flush
When you stop eating carbohydrates, the body starts burning stored glycogen for fuel. These reserves sit primarily in the liver and skeletal muscles.
Here is the key metabolic detail: glycogen is an extremely hydrophilic molecule. For every gram of glycogen stored, the body holds onto roughly three grams of water. The average adult stores about 500 grams of glycogen.
As you enter ketosis and burn through these stores during the first 24 to 48 hours, your body releases up to 1.5 liters of previously bound water directly into the bloodstream. A large portion of this fluid gets dumped into the gastrointestinal tract, easily overwhelming the colon’s absorption capacity and producing highly liquid stool.
This is why the first few days of a fast are notorious for rapid weight loss. You are not burning pure fat yet. You are shedding pounds of water as glycogen stores deplete.
Electrolyte Mistakes and Osmotic Overload
Fasting aggressively depletes sodium, potassium, and magnesium. To fight fatigue and cramps, many people turn to electrolyte powders or concentrated salt water. Replacing electrolytes is vital for heart health during a fast, but taking them incorrectly is one of the biggest triggers for digestive distress.
The type of magnesium matters enormously. Magnesium citrate is a highly osmotic compound that pulls massive amounts of water from the bloodstream into the intestines. This is exactly why magnesium citrate is used as a prescription laxative before colonoscopies. Taking it on an empty fasting stomach makes diarrhea almost guaranteed.
Magnesium glycinate, on the other hand, is bound to an amino acid and absorbs much more efficiently through cellular walls without creating the same osmotic gradient. Switching your supplement is often the simplest fix for fasting bowel problems.
The Salt Flush Problem
Drinking too much sodium or potassium at once creates a hypertonic environment in the stomach. The fluid in your gut becomes denser than the fluid in your bloodstream. To restore balance, water passively flows across the intestinal wall into the gut to dilute the salt load.
This leads to a sudden, explosive bowel movement. Fasting communities commonly call this a salt flush. It is entirely preventable if you understand the basic physics of osmosis and spread your intake throughout the day.
Caffeine and the Gastrocolic Reflex
Many fasting protocols allow black coffee or plain green tea. While these drinks will not break a fast metabolically, they have a powerful impact on gut motility. Caffeine directly stimulates the smooth muscles of the digestive tract.
Black coffee on an empty stomach triggers the rapid release of gastrin and motilin, hormones that promote intestinal peristalsis. This initiates the gastrocolic reflex, a biological signal telling the colon to clear out existing waste to make room for incoming food. Even though no calories are coming, the gut reacts as if a large meal is on the way.
When caffeine-induced peristalsis combines with a pocket of unabsorbed bile sitting in the duodenum, the result is rapid, uncontrollable bile dumping. If a patient reports severe bowel urgency while fasting, my first clinical recommendation is to temporarily stop all caffeine. This simple change often resolves the problem within 24 hours.
Microbiome Shifts During Fasting
Your gut microbiome relies on the fiber, complex carbohydrates, and sugars you eat every day. When you abruptly stop feeding those bacteria during a prolonged water fast, the microbial landscape shifts dramatically.
Certain bacterial strains that depend on regular sugar intake begin to die off. This die-off phase temporarily irritates the intestinal mucosal lining. The remaining bacteria start feeding on the mucin layer of the gut wall to survive, causing mild degradation of the protective mucus barrier.
This temporary state of dysbiosis makes the colon highly reactive to any fluid passing through it, amplifying the severity of any fasting-related diarrhea.
Secretory vs. Osmotic Diarrhea: Identifying Your Type
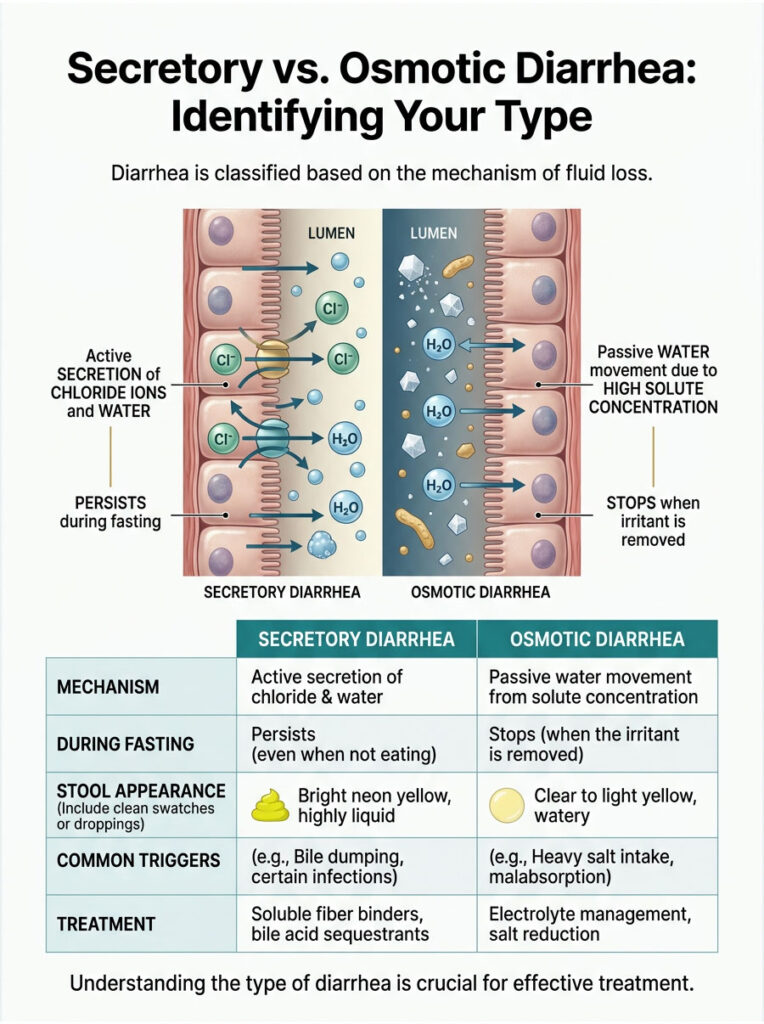
In gastroenterology, we classify diarrhea based on the cellular mechanism driving the fluid loss. Knowing the difference between secretory and osmotic diarrhea is critical for choosing the right fix. The treatment for one will not work for the other.
| Feature | Secretory (Bile Acid Induced) | Osmotic (Electrolyte Induced) |
| Mechanism | Active secretion of chloride ions and water into the gut lumen. | Passive drawing of water into the gut due to high solute concentration. |
| Fasting Trigger | Gallbladder stasis and spontaneous bile dumping. | Glycogen water release or heavy salt supplementation. |
| Stool Appearance | Bright neon yellow, highly liquid, acidic burning sensation. | Watery, clear to light yellow, high volume, little burning. |
| Fasting Response | Persists or worsens even if you stop drinking fluids temporarily. | Stops completely once the offending supplement is removed. |
| Management | Soluble fiber binders, dietary titration, or prescription bile acid sequestrants. | Sipping electrolytes slowly, switching magnesium forms, reducing salt load. |
Secretory diarrhea is an active biological process. The colon pumps chloride ions and water into the gut lumen through CFTR protein channels because it detects a dangerous irritant. During extended fasting, that irritant is raw, unbuffered bile. This type is aggressive and can wake you from sleep.
Osmotic diarrhea is entirely passive. It happens purely because of physics. If you drink a concentrated glass of salt water, water flows across the intestinal wall to dilute the minerals.
If your stool burns intensely and is neon yellow, you are dealing with secretory bile acid malabsorption. If it is clear, high volume, and happens about 20 minutes after drinking supplements, it is an osmotic flush.
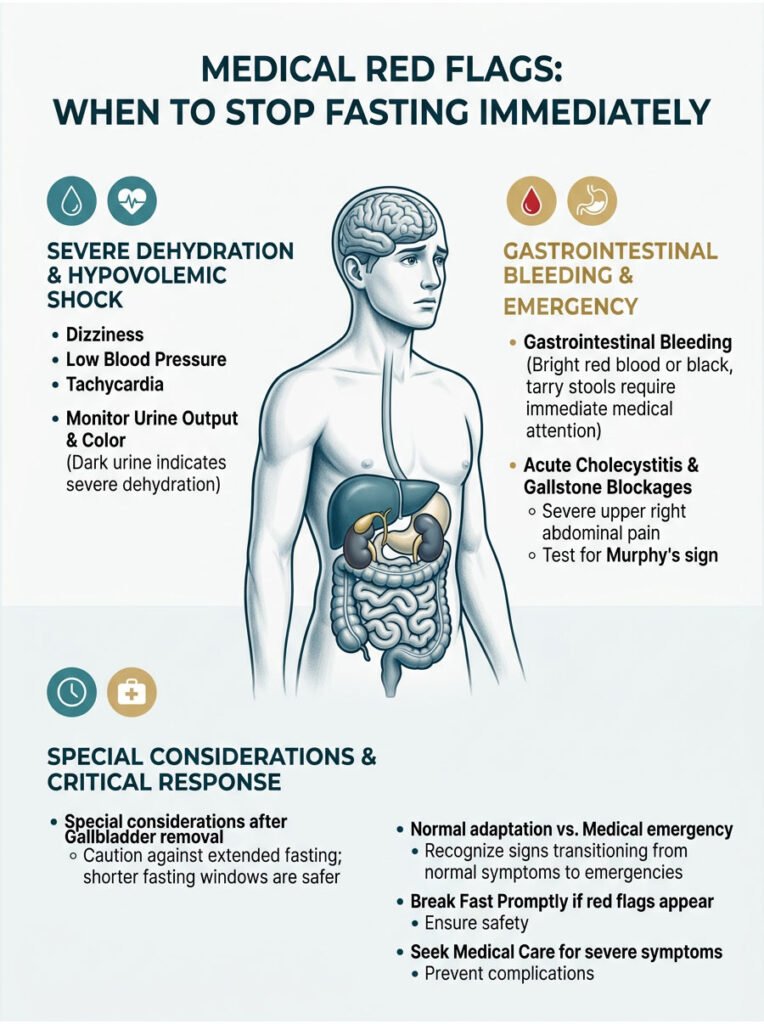
Medical Red Flags: When to Stop Fasting Immediately
Loose stools during a fast are usually a harmless metabolic adaptation. But fasting is a significant physiological stressor, and normal symptoms can cross the line into a genuine medical emergency. Patient safety is always my primary concern.
You need to know the clinical red flags that indicate severe distress. Pushing through dangerous symptoms to complete a fast is reckless. Here are the warning signs that mean you stop immediately.
Severe Dehydration and Hypovolemic Shock
The most immediate danger of fasting diarrhea is rapid dehydration. Without solid food, you are already missing the 20% to 30% of daily water intake that typically comes from meals. Adding liquid bowel movements to this deficit drains your blood volume quickly.
Watch for orthostatic hypotension. If you stand up and experience severe dizziness, tunnel vision, or feel like you are about to faint, your blood pressure has dropped dangerously low. A systolic drop of more than 20 mmHg upon standing is a major red flag.
Tachycardia is another warning. If your resting heart rate stays above 100 beats per minute while sitting still, your heart is compensating for a severe lack of blood volume. Break the fast and start oral rehydration immediately.
Monitoring Kidney Function
Pay close attention to urine output. If you stop urinating for more than 8 hours, your kidneys are conserving every drop of water they can. If urine becomes dark and concentrated like apple juice, plain water alone may no longer be sufficient.
At this stage, blood urea nitrogen and creatinine levels are likely elevated. In severe cases of complete urine absence, intravenous fluids at an emergency department may be necessary to protect the kidneys from acute injury.
Never ignore extreme thirst combined with a dry, sticky mouth and sunken eyes. These are late-stage signs of severe volume depletion. The benefits of autophagy are completely negated if you put yourself into hypovolemic shock.
Gastrointestinal Bleeding
Fasting does not cause internal bleeding or gastrointestinal infections. If you see bright red blood in your stool (hematochezia), this is never a normal fasting symptom.
If the stool looks black, sticky, and tarry like wet coffee grounds, you are experiencing melena. This indicates active bleeding in the upper GI tract, likely from a stomach ulcer or severe gastritis. Both require immediate endoscopic evaluation.
Severe dehydration can also reduce blood flow to the colon, causing ischemic colitis. This presents with intense cramping abdominal pain followed by bloody diarrhea. If this happens, go to the nearest emergency room.
Acute Cholecystitis and Gallstone Blockages
Learn to tell the difference between mild cramping from normal bile dumping and the severe, unrelenting pain of an inflamed organ. A sharp, stabbing pain in the upper right abdomen just below the rib cage that radiates to the right shoulder blade is a classic presentation of biliary colic.
This pattern could indicate cholecystitis (an inflamed gallbladder) or a gallstone blocking the common bile duct. Fasting actually raises gallstone risk because of the prolonged stasis we discussed earlier.
Clinically, we test for this using Murphy’s sign. If taking a deep breath while pressing under the right rib cage causes you to gasp in sharp pain, the test is positive. Break the fast, seek medical imaging, and avoid heavy fats until a doctor clears you.
Special Considerations After Gallbladder Removal
Patients who have had a cholecystectomy face a unique set of digestive challenges during fasting. Without the gallbladder’s storage function, the liver continuously drips raw bile directly into the duodenum around the clock.
For these patients, extended multi-day water fasting is often medically contraindicated. The constant bile drip can cause severe gastritis, duodenal ulcers, and chronic secretory diarrhea. If you do not have a gallbladder, sticking to shorter intermittent fasting windows of 12 to 14 hours is a much safer approach, ensuring food is regularly present to bind the bile.
Normal Adaptation vs. Medical Emergency
| Category | Normal Fasting Adaptation | Red Flag – Seek Care |
| Duration | Lasts 1 to 3 days during initial metabolic switch into ketosis. | Persists beyond 48 hours despite stopping all supplements. |
| Appearance | Bright neon yellow, clear liquid, or light green fluid. | Black, tarry, or containing streaks of bright red blood. |
| Pain | Mild, transient cramping before a bowel movement. | Severe, localized, stabbing pain in upper right or lower left abdomen. |
| Systemic Signs | Mild fatigue, slight headache, standard keto flu aches. | High fever, extreme dizziness upon standing, rapid resting heart rate. |
If your symptoms fall into the red flag category, the therapeutic benefit of the fast has ended. Breaking the fast with a small, gentle meal is the safest decision you can make.
How to Stop Fasting Diarrhea: Actionable Clinical Protocols
If you are experiencing normal, non-emergency fasting diarrhea, there are specific clinical protocols to calm the gut. These strategies focus on managing osmotic pressure, physically binding excess bile, and reintroducing food without triggering a massive gastrocolic reflex.
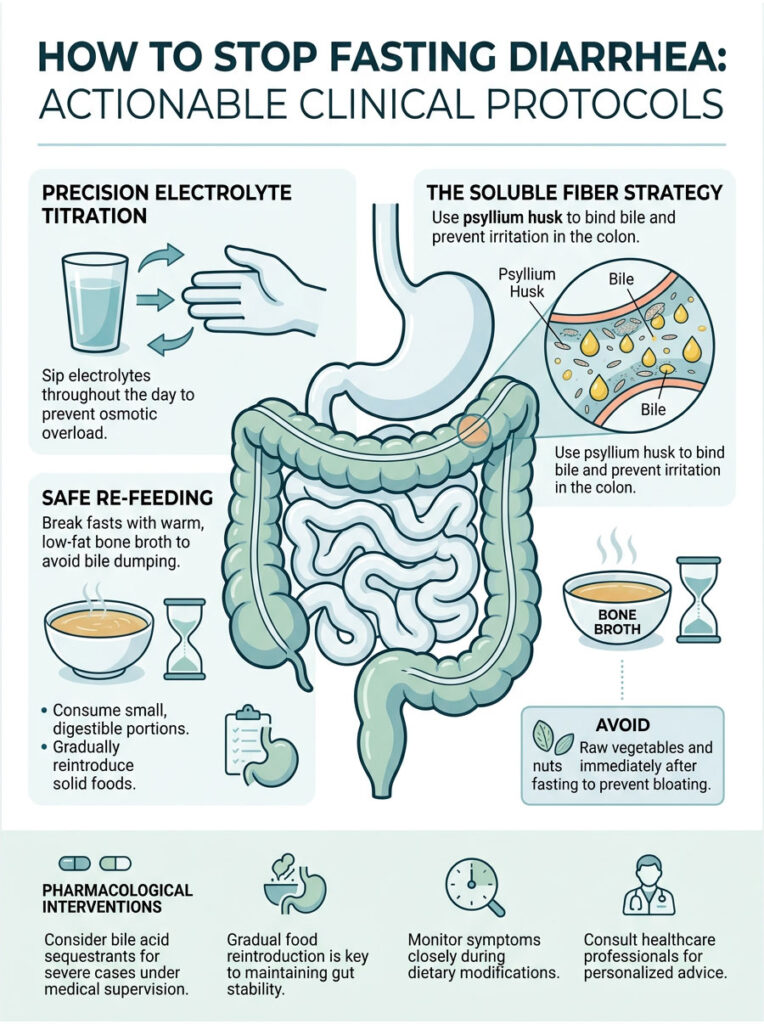
Precision Electrolyte Titration
The single biggest mistake people make is chugging electrolyte water all at once. Drinking 16 ounces of heavily salted water in five minutes creates an instant osmotic gradient. The heavy fluid flushes straight through the stomach, bypasses absorption, and floods the colon.
Instead, mix your total daily sodium chloride and potassium chloride into a large jug of water, ideally two to three liters. Take small, continuous sips throughout the entire day. This slow-drip method lets the intestinal villi absorb electrolytes gradually and prevents sudden pooling of heavy fluid in the colon.
For magnesium, drop oral citrate capsules entirely. Switch to a transdermal magnesium spray applied after a shower, or take a high-quality magnesium glycinate capsule before bed with a small sip of water. This bypasses the severe osmotic laxative effect in the lower intestine.
The Soluble Fiber Strategy
For patients struggling with chronic loose stools during feeding windows or shorter fasts, I frequently recommend pure psyllium husk. It is a highly effective, natural soluble fiber that contains no digestible carbohydrates, meaning a small dose will not spike insulin.
A single teaspoon of pure psyllium husk powder mixed in eight ounces of water forms a thick, viscous gel in the stomach. As this gel moves into the small intestine, it acts as a physical sponge, binding to the raw bile salts released by spontaneous bile dumping.
The psyllium traps caustic bile salts inside its gel matrix, preventing them from touching and irritating the colon lining. It effectively stops bile acid malabsorption without breaking the metabolic benefits of the fast.
Safe Re-feeding After Prolonged Fasts
How you break your fast is just as important as the fast itself. After prolonged gallbladder stasis, the biliary tree is loaded with concentrated, pressurized bile. If you break the fast with a massive, high-fat meal like a cheeseburger, you will trigger a disaster.
The sudden fat influx triggers a massive release of CCK. The gallbladder contracts violently, dumping all stored bile at once. This produces explosive, painful diarrhea within an hour.
The safest approach is a small cup of warm, low-fat bone broth. The gentle amino acids slowly stimulate the gut lining without provoking a massive bile dump. Wait at least 60 to 90 minutes after the broth before attempting solid food.
Expert Tip: Never break an extended fast with raw vegetables, nuts, or large salads. The fasting gut temporarily lacks the enzymatic capacity and microbiome diversity to handle heavy cellulose. Eating raw veggies immediately leads to severe bloating, painful cramping, and mechanical irritation.
Pharmacological Interventions
In severe, medically supervised cases, we may prescribe bile acid sequestrants. Medications like cholestyramine or colesevelam specifically bind to bile acids in the gut, forming an insoluble complex that neutralizes their laxative effect.
These prescriptions are usually reserved for chronic conditions like Crohn’s disease, but they work extremely well for severe fasting responders. I only use pharmacological interventions when dietary modifications and fiber supplements completely fail.
Recent Clinical Research and Gastroenterology Data
Gastroenterology is a strictly evidence-based field. The advice I give patients is rooted in clinical data, peer-reviewed observations, and physiological facts. Reviewing the research helps remove fear and replace it with scientific understanding.
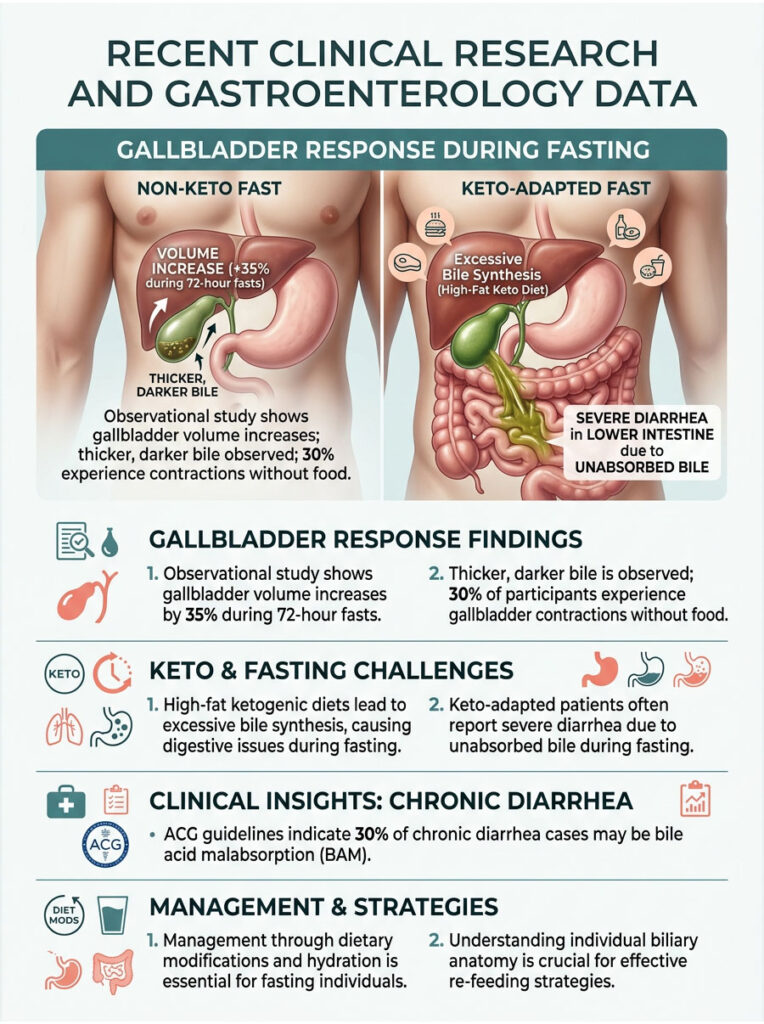
Gallbladder Imaging During 72-Hour Fasts
A landmark observational study used advanced ultrasound imaging to monitor the biliary tracts of healthy adults undergoing a 72-hour water fast. Researchers measured resting gallbladder volume every 12 hours.
By hour 48, the average gallbladder volume had increased by 35%. The bile inside became visibly thicker and darker on the monitor. Roughly 30% of participants experienced spontaneous, partial gallbladder contractions without any food stimulus. This directly confirms the mechanical reality of fasting bile dumping.
Keto-Adaptation and Bile Synthesis
Research on patients transitioning to high-fat ketogenic diets paired with intermittent fasting shows a significant metabolic mismatch. When dietary fat intake increases drastically, the liver upregulates bile acid synthesis to handle the new macronutrient ratio.
When these keto-adapted patients enter a fasting window, the liver continues producing high volumes of bile, expecting a high-fat meal based on recent patterns. The liver makes maximum bile, but the stomach stays empty.
These patients report the highest incidence of severe diarrhea during fasting windows. Over four to six weeks, the liver typically downregulates its baseline bile production, and the severe symptoms naturally subside.
Insights from the American College of Gastroenterology
The ACG publishes peer-reviewed guidelines on chronic diarrheal conditions. According to recent ACG data, up to 30% of patients with unexplained functional diarrhea actually suffer from undiagnosed bile acid malabsorption. The ACG recommends therapeutic trials of bile acid binders or strict dietary modifications.
For the fasting community, this reinforces a critical reality. Unabsorbed bile is a potent, medically recognized laxative. It must be managed through careful re-feeding strategies, proper hydration, and an understanding of your own biliary anatomy.
Key Takeaways: Managing Yellow Watery Diarrhea While Fasting
Sudden bowel urgency during a fast can be alarming and uncomfortable, but as we have covered thoroughly, it is rarely a sign of serious illness. It is the logical, mechanical result of your digestive system adapting to a sudden lack of incoming food.

The core mechanism is a perfect storm of predictable biological reactions. The liver continues making bile relentlessly, causing temporary gallbladder stasis. Spontaneous nerve contractions trigger bile dumping into an empty intestine. Without food to absorb these caustic fluids, bile acid malabsorption occurs in the colon.
Layer on the glycogen water flush, add poorly timed electrolyte supplements, and the result is rapid expulsion of liquid stool.
Remember the primary safety rules: sip electrolytes slowly throughout the day, avoid osmotic laxatives like magnesium citrate, and temporarily cut black coffee to calm the gastrocolic reflex.
If your symptoms include severe abdominal pain, bright red blood, or signs of extreme dehydration like a racing heart and dark urine, break the fast immediately. Fasting is a powerful, evidence-based tool for metabolic health, but practicing it safely requires understanding why you might experience yellow watery diarrhea while fasting.
Frequently Asked Questions
Why is my diarrhea bright neon yellow during a water fast?
The neon yellow color is caused by bilirubin, a natural pigment found in your bile. Under normal circumstances, gut bacteria have time to convert yellow bilirubin into brown stercobilin. However, during a fast, the rapid transit time caused by ‘bile dumping’ means the fluid moves through your system too quickly for this chemical conversion to occur, leaving the stool its original yellowish hue.
Is yellow watery diarrhea a sign of a stomach infection or the ‘keto flu’?
While it can be mistaken for an infection, yellow watery diarrhea while fasting is typically a physiological adaptation known as secretory diarrhea. Without food to buffer digestive juices, raw bile salts irritate the colonic mucosa. The body responds by secreting massive amounts of water into the colon to flush out the irritant, which is a mechanical response rather than a viral or bacterial infection.
How does glycogen depletion contribute to bowel urgency?
As a gastroenterologist, I often point to the 3:1 water-to-glycogen ratio. For every gram of stored glycogen your body burns for fuel during the first 48 hours of a fast, it releases approximately three grams of water. This systemic ‘glycogen water flush’ can overwhelm the colon’s absorption capacity, leading to high-volume, liquid bowel movements.
Should I stop drinking black coffee if I experience fasting diarrhea?
I strongly recommend pausing caffeine intake if you experience urgency. Caffeine is a central nervous system stimulant that triggers the gastrocolic reflex and the release of gastrin and motilin. These hormones increase intestinal peristalsis, which can accelerate the movement of unbuffered bile through your empty digestive tract, worsening diarrhea.
Which magnesium supplement is safest for preventing digestive upset while fasting?
You should strictly avoid magnesium citrate, as it is a potent osmotic laxative used clinically for colonoscopy preps. Instead, utilize magnesium glycinate or transdermal magnesium sprays. Glycinate is bound to an amino acid and is absorbed much more efficiently by the intestinal walls, preventing the osmotic gradient that draws water into the gut.
What is ‘bile dumping’ and why does it happen on an empty stomach?
Bile dumping is the spontaneous contraction of the gallbladder without the presence of food. Normally, the hormone Cholecystokinin (CCK) triggers bile release after you eat fat. During a fast, the gallbladder can reach maximum capacity—a state called gallbladder stasis—causing the enteric nervous system to trigger an inappropriate squeeze to relieve internal pressure, flooding the empty small intestine with caustic bile salts.
Can I perform extended fasts if I have had a cholecystectomy (gallbladder removal)?
Patients without a gallbladder are at a significantly higher risk for chronic bile acid malabsorption during fasts. Because the liver drips bile continuously into the duodenum without a storage balloon, the fasting gut is subjected to a constant, irritating trickle of acidic salts. I generally advise post-cholecystectomy patients to stick to shorter intermittent fasting windows, such as 12 to 14 hours.
What are the clinical red flags that indicate I should break my fast immediately?
You must break your fast if you experience signs of hypovolemic shock or severe dehydration. These include orthostatic hypotension (severe dizziness when standing), a resting heart rate over 100 bpm (tachycardia), dark ‘apple juice’ colored urine, or severe, stabbing pain in the upper right quadrant which could indicate acute cholecystitis or a gallstone blockage.
How can I supplement sodium and potassium without causing a ‘salt flush’?
The key is precision titration. Avoid ‘slugging’ concentrated electrolyte shots. Instead, mix your total daily requirement of sodium and potassium chloride into 2 to 3 liters of water and sip it slowly throughout the day. This ‘slow-drip’ method allows the intestinal villi to absorb the minerals gradually, preventing an osmotic overload in the colon.
Will taking psyllium husk break my fast or help stop the diarrhea?
A small amount of pure, unflavored psyllium husk (1 teaspoon) is often a clinical ‘game changer’ for fasting diarrhea. As a soluble fiber, it forms a viscous gel that acts as a physical sponge, binding to raw bile salts and preventing them from irritating the colon. Since it contains no digestible carbohydrates, it typically does not spike insulin or break the metabolic state of autophagy.
Why does diarrhea sometimes occur immediately after my first meal post-fast?
This is often due to an exaggerated gastrocolic reflex combined with gallbladder stasis. After days of inactivity, your gallbladder is full of highly concentrated bile. If you break your fast with a high-fat meal, the massive surge of CCK causes a violent contraction, dumping a large volume of bile that the dormant gut cannot process, resulting in immediate ‘re-feeding’ diarrhea.
What is the safest protocol for re-feeding after a prolonged fast?
To wake up the dormant digestive tract safely, start with a small cup of warm, low-fat bone broth. The gentle amino acids stimulate the gut lining without provoking a massive bile dump. Wait at least 60 to 90 minutes before consuming solid food, and avoid raw vegetables, nuts, or heavy fats for the first 24 hours to prevent mechanical irritation and osmotic shifts.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. Fasting can be a significant physiological stressor. Always consult a qualified healthcare professional or gastroenterologist before beginning an extended fast, especially if you have pre-existing conditions or experience severe symptoms like yellow watery diarrhea while fasting.
References
- National Institutes of Health (NIH) – https://www.ncbi.nlm.nih.gov/books/NBK470209/ – Clinical data on daily bile production and liver function.
- American College of Gastroenterology (ACG) – https://gi.org/topics/diarrhea/ – Guidelines on bile acid malabsorption and functional diarrheal triggers.
- Journal of Clinical Gastroenterology – “Gallbladder Volume and Emptying during Fasting and Re-feeding” – Study detailing the 35-40% increase in gallbladder volume during prolonged fasts.
- American Journal of Physiology – “Mechanics of Osmotic Water Shift in the Human Colon” – Research supporting the 3:1 ratio of water to glycogen storage and release.
- The Lancet Gastroenterology & Hepatology – “Bile Acid Diarrhea: Pathophysiology and Management” – Clinical review of secretory diarrhea mechanisms and bile acid sequestrants.
- World Journal of Gastroenterology – “The Enteric Nervous System and Fasting Motility” – Insights into the gastrocolic reflex and hormonal triggers like CCK and motilin.