

If you have ever stood at a pharmacy counter holding three or four different prescription bottles and wondering which pill is wrecking your stomach, you are not alone. As a clinical pharmacist with over 15 years of experience, this is one of the most common questions I hear every single day.
Table of Contents
Just last week, a patient dropped a heavy bag of medications on my consultation desk and looked at me with total exhaustion. Constant trips to the bathroom had drained every ounce of energy. When someone takes multiple prescriptions at once, pinpointing the exact culprit can feel like solving a mystery with too many suspects.
Here is the short answer: yes, amoxicillin, magnesium, prednisone, and metformin can all cause diarrhea. But the reasons behind each one are completely different. An antibiotic disrupts your gut bacteria. A mineral supplement pulls water into your colon. A diabetes drug interferes with bile acid absorption. And a steroid strips away the protective lining of your stomach.
In this guide, I will break down exactly what happens inside your digestive system when you take each of these medications. More importantly, I will share evidence-based strategies to reduce or eliminate the discomfort, so you can stay on your treatment plan without living in the bathroom.
Quick Answer: Can These Four Medications Cause Diarrhea?
Yes. All four of these medications are well-known for causing diarrhea, but through entirely different biological mechanisms:
- Amoxicillin kills beneficial gut bacteria, leading to antibiotic-associated diarrhea (AAD).
- Magnesium acts as an osmotic laxative by drawing water into the colon.
- Metformin disrupts bile acid reabsorption and speeds up gut motility.
- Prednisone irritates the stomach lining by reducing its protective mucus layer.
In many cases, you can manage these side effects by switching formulations, adjusting dose timing, or adding a targeted probiotic. Let me walk you through the details.
Key Clinical Statistics on Medication-Induced Diarrhea
- Up to 25% of patients develop antibiotic-associated diarrhea after taking broad-spectrum penicillin drugs (American Journal of Gastroenterology, 2021).
- 20% to 30% of patients experience GI issues during the initial weeks of metformin therapy.
- 350 mg per day is the tolerable upper intake level for supplemental magnesium before osmotic effects kick in.
- Switching from immediate-release to extended-release metformin reduces stomach complaints by up to 70%.
- About 7% of all reported adverse drug reactions are directly tied to medication-induced diarrhea.
- Targeted probiotic therapy typically begins normalizing stool consistency within 48 to 72 hours.
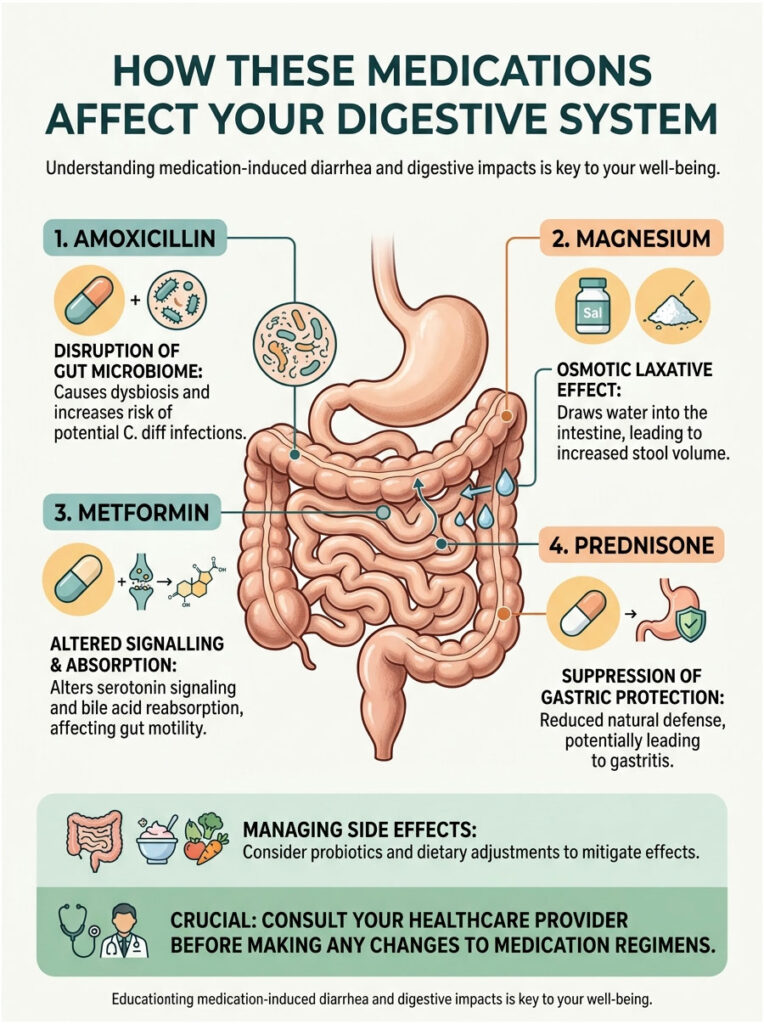
How These Medications Affect Your Digestive System
Medication-induced diarrhea is not a one-size-fits-all problem. Each of these four drugs interacts with your gut in a distinct, chemically specific way. Understanding these pathways is the first step toward taking control of your symptoms.
Your digestive tract is a complex ecosystem that depends on a delicate balance of water, bacteria, and acid. When a synthetic chemical enters this natural environment, the disruption can be immediate. Some drugs speed up muscle contractions, while others destroy protective barriers in your tissues.
Amoxicillin and Gut Microbiome Disruption
Amoxicillin is a widely prescribed broad-spectrum antibiotic used for everything from sinus infections to dental abscesses. The problem? It cannot distinguish between the harmful bacteria causing your infection and the beneficial bacteria living in your intestines.
When you take amoxicillin, it wipes out large populations of healthy intestinal flora. This creates a condition known as gut microbiome dysbiosis, which simply means your internal bacterial ecosystem has fallen out of balance.
Without enough good bacteria, your colon struggles to ferment complex carbohydrates properly. Those unfermented carbs sit in the lower intestine and draw in excess water, which leads directly to antibiotic-associated diarrhea. Medical literature confirms that up to 25% of patients experience this side effect.
Most cases are mild and clear up on their own. However, dysbiosis opens the door for dangerous opportunistic pathogens, particularly Clostridioides difficile (C. diff). When amoxicillin clears out protective bacteria, C. diff can multiply rapidly and release harmful toxins.
Symptoms of a C. diff infection include severe watery stools, intense abdominal cramping, and fever. If you develop these symptoms, contact your doctor right away. Do not take over-the-counter anti-diarrheal medications like Imodium, because they can trap bacterial toxins inside your colon.
To combat this bacterial destruction, many gastroenterologists now recommend Saccharomyces boulardii, a beneficial yeast-based probiotic with strong clinical evidence for preventing AAD. We will cover exactly how to use it later in this guide.
Magnesium and the Osmotic Laxative Effect
Magnesium is an essential mineral involved in over 300 biochemical reactions in the body. People take it daily for muscle cramps, sleep support, and heart health. However, taking the wrong type or dose will send you straight to the bathroom.
The issue comes down to something called an osmotic gradient. Your body can only absorb a certain amount of magnesium at one time. The unabsorbed portion travels into the intestinal lumen, where it acts like a sponge, pulling water from surrounding tissues into the bowel.
This sudden influx of water increases stool volume and triggers rapid peristalsis, the involuntary muscle contractions that move waste through your digestive tract. According to the National Institutes of Health, the tolerable upper intake level for supplemental magnesium is 350 mg per day. Anything above that threshold is likely to cause loose, watery stools.
Many patients accidentally double their magnesium intake by combining a daily multivitamin with a standalone supplement. The resulting fluid loss can ironically worsen the very deficiency symptoms you are trying to fix, including muscle twitching, fatigue, and irregular heartbeat.
The type of magnesium supplement you choose matters enormously. I will cover the best gut-friendly options in a dedicated section below.
Metformin, Bile Acid Malabsorption, and Gut Motility
Metformin is the gold-standard first-line treatment for Type 2 diabetes worldwide. It is highly effective at lowering blood sugar, but it is also notorious for causing gastrointestinal distress. Up to 30% of patients experience nausea, bloating, and loose stools during their first few weeks of therapy.
The mechanism behind this discomfort involves two main pathways. First, metformin alters serotonin signaling in the gut lining. Your gut produces a large share of your body’s serotonin, which regulates bowel motility. When metformin speeds up this signaling, food moves through your system faster than normal.
Second, metformin interferes with bile acid reabsorption. Your liver produces bile acids to help digest dietary fats. Normally, these are neatly reabsorbed at the end of the small intestine. Metformin blocks this process in a significant number of patients, allowing raw bile acids to dump into the large intestine, where they irritate the colon lining and trigger urgent bowel movements.
The formulation of the drug plays a huge role here. The immediate-release (IR) version dissolves rapidly, hitting your stomach all at once and overwhelming the gut. The extended-release (ER) version slowly delivers the medication over a full 24-hour period.
Switching from IR to ER metformin successfully resolves up to 70% of diarrhea cases in diabetic patients. It is one of the simplest and most effective interventions I perform daily as a pharmacist.
Prednisone and Corticosteroid-Induced Gastritis
Prednisone is a powerful systemic corticosteroid used to treat severe inflammation, acute asthma, and autoimmune diseases. While remarkably effective, it is incredibly harsh on the digestive system.
Your stomach lining is protected by a thick layer of mucus, which is maintained by chemical messengers called prostaglandins. Prednisone works by shutting down prostaglandin production throughout the body. This is what reduces inflammation in your joints or lungs, but it also strips away your stomach’s natural protective barrier.
Without that barrier, normal stomach acid begins to burn the exposed tissue. This leads to corticosteroid-induced gastritis, which causes stomach pain, cramping, and accelerated digestion as your body tries to expel the irritating acid quickly.
Prednisone also suppresses your immune system, which is its intended therapeutic effect for autoimmune conditions. But this lower immune defense makes you more vulnerable to opportunistic gut infections that can trigger additional diarrhea.
Doctors typically recommend taking prednisone with a substantial meal or a glass of milk. Enteric-coated formulations, which feature a hardened shell that prevents the drug from dissolving in the stomach, can also eliminate upper GI burning and lower bowel urgency.
When Multiple Medications Collide: The Polypharmacy Problem
Dealing with side effects from one drug is manageable. But what happens when you take two, three, or all four of these medications at the same time? In the medical community, this overlap is called polypharmacy, and it is extremely common in older adults managing multiple chronic conditions.
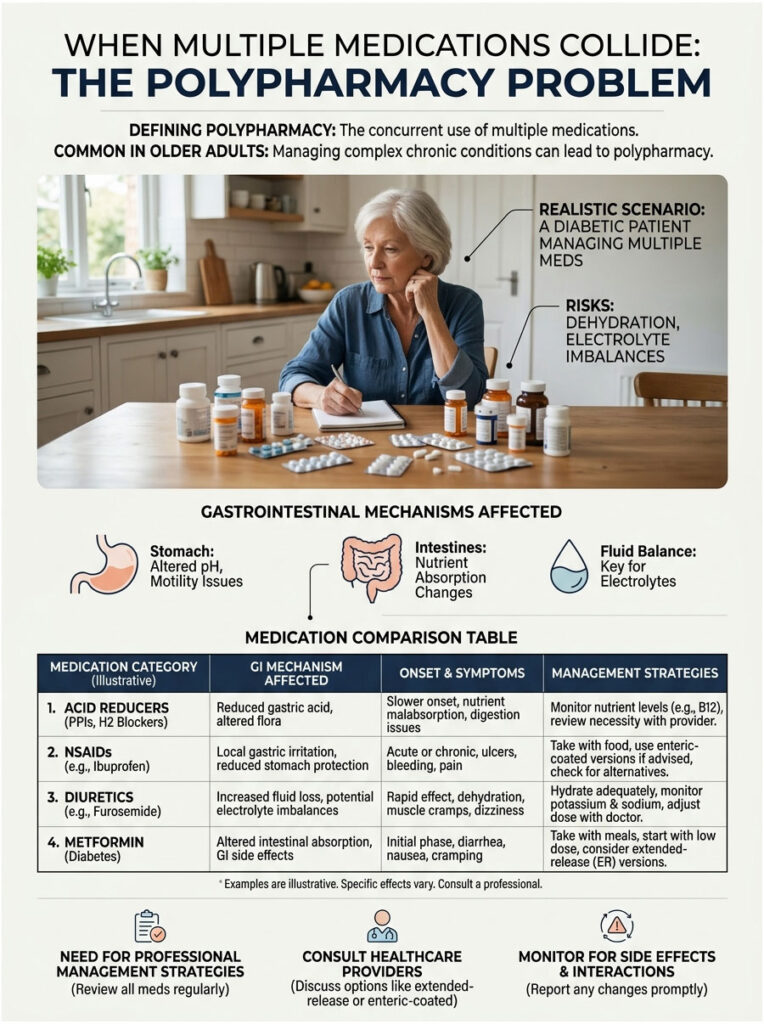
Consider this realistic scenario. A diabetic patient takes daily metformin for blood sugar control. They catch a sinus infection and receive prescriptions for amoxicillin and prednisone from urgent care. To help with sleep, they take a magnesium supplement at bedtime.
This creates a perfect storm. The amoxicillin causes dysbiosis by killing protective gut flora. The metformin speeds up motility through bile acid malabsorption. The magnesium pulls water into the already irritated colon. And the prednisone causes gastritis, making the entire digestive tract hypersensitive.
When these medications collide, the risk of severe dehydration and dangerous electrolyte imbalances rises sharply. This is exactly why a professionally guided management strategy is essential. You cannot guess your way through a polypharmacy interaction.
Medication Comparison: GI Mechanisms and Management Strategies
| Medication | Primary GI Mechanism | Typical Onset | Clinical Management Strategy |
| Amoxicillin | Microbiome dysbiosis and flora depletion | 2 to 5 days | Co-administer targeted probiotics; monitor for C. diff |
| Magnesium | Osmotic fluid shift into the colon | 2 to 6 hours | Reduce dose; switch to high-bioavailability form |
| Metformin | Bile acid malabsorption and altered motility | 1 to 3 weeks | Take with meals; switch to ER formulation |
| Prednisone | Gastric mucosal irritation | Varies by dose | Take with food or milk; consider enteric-coated version |
Always ask your doctor or pharmacist whether an extended-release or enteric-coated version of your medication is available. It can make a significant difference.
Choosing the Right Magnesium Supplement for Your Gut
The most easily correctable cause of supplement-related diarrhea is a poorly chosen magnesium formulation. Walk into any pharmacy, and you will find a dozen different types of magnesium on the shelf. Picking the wrong one almost guarantees a rough night.
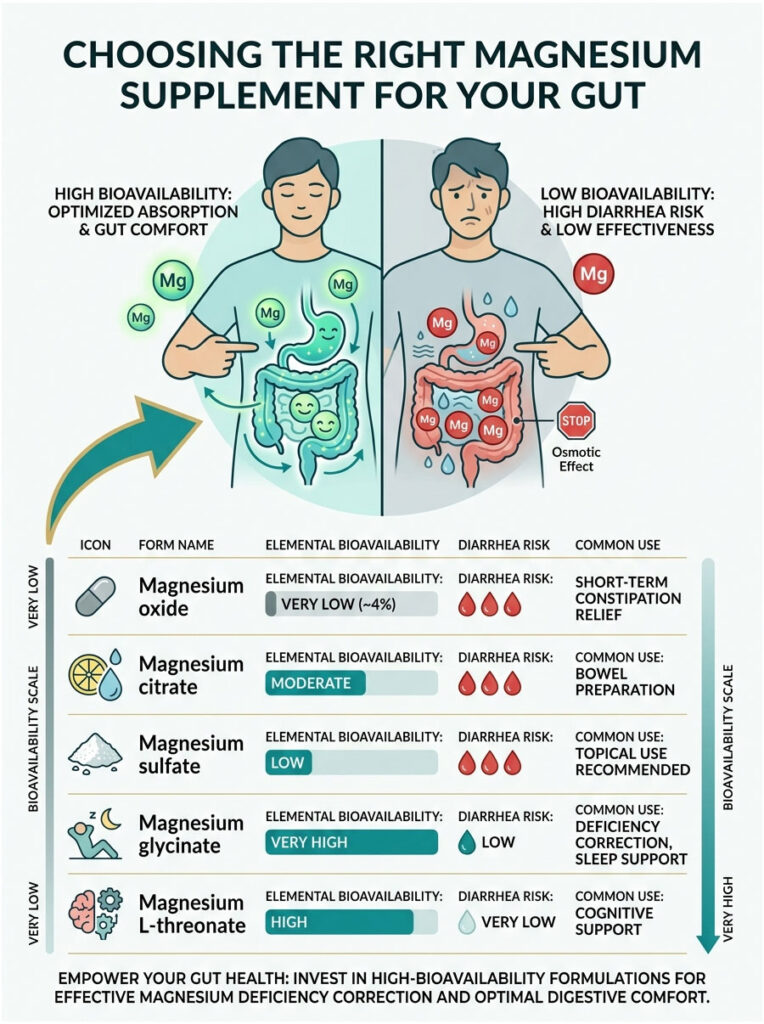
The key concept here is elemental bioavailability, which refers to how efficiently your body absorbs the mineral through the intestinal wall. Cheap supplements have very low bioavailability, while premium formulations are absorbed much more efficiently.
A generic bottle of magnesium oxide, for example, only delivers about 4% of the active ingredient to your bloodstream. The remaining 96% stays in your gut and acts as an osmotic laxative. This is actually why hospitals use it to treat stubborn constipation.
Magnesium glycinate, on the other hand, is created by binding the mineral to the amino acid glycine. This stable chemical bond allows the mineral to bypass the normal digestive absorption pathways that cause irritation. Very little residue is left in the colon to draw in water, making stomach upset rare compared to other forms.
If you are dealing with deficiency symptoms like leg cramps or eye twitches, you need an effective supplement. But you cannot fix those symptoms if the pill gives you diarrhea, because the fluid loss will just dehydrate you further.
Magnesium Formulation Comparison
| Formulation | Bioavailability | Diarrhea Risk | Best Use |
| Magnesium Oxide | Very Low (~4%) | Very High | Short-term constipation relief |
| Magnesium Citrate | Moderate | High | Bowel preparation procedures |
| Magnesium Sulfate | Low | High | Topical use (Epsom salts) or IV |
| Magnesium Glycinate | Very High | Low | Deficiency correction and sleep support |
| Magnesium L-Threonate | High | Very Low | Cognitive and neurological support |
Spending a few extra dollars on a high-bioavailability formulation can spare your digestive system a lot of grief.
Recent Research on Gut Health and Medication Side Effects
Gastroenterology has shifted significantly in recent years when it comes to managing medication-induced diarrhea. Doctors no longer just tell patients to wait it out. Instead, the focus is now on targeted therapies that actively protect the gut microbiome.
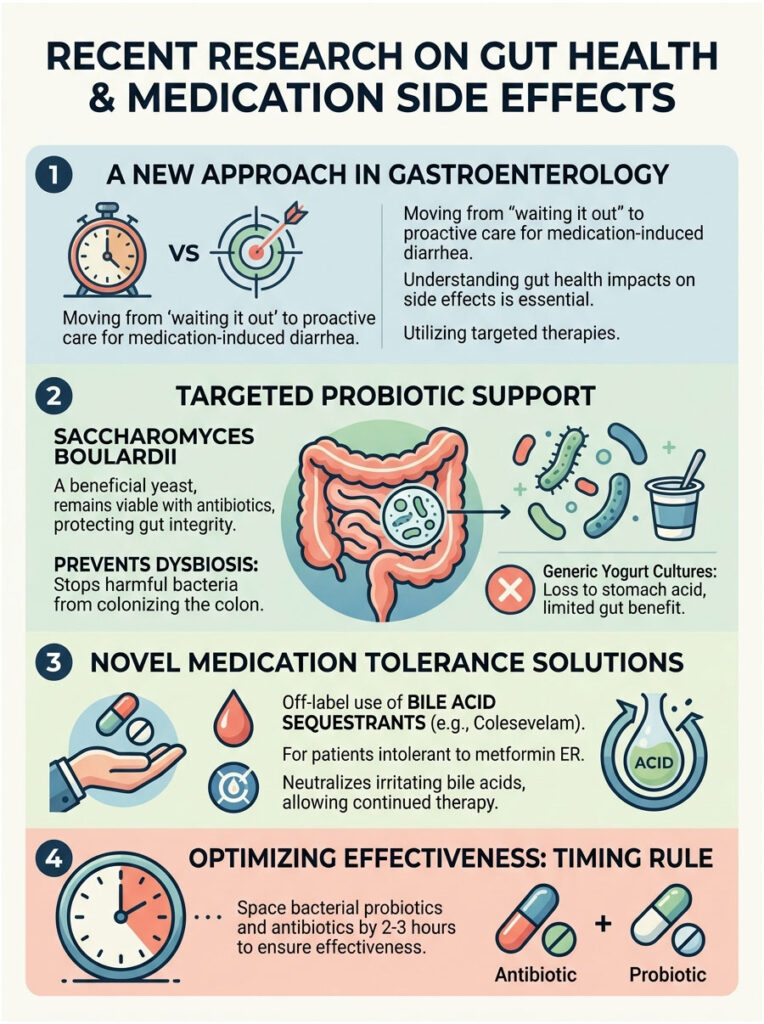
For decades, the standard advice was to eat yogurt while taking antibiotics. We now know that generic yogurt cultures are largely destroyed by stomach acid before reaching the colon. They do very little to prevent dysbiosis.
Modern clinical research strongly supports Saccharomyces boulardii, a beneficial, non-pathogenic yeast. Because it is a yeast and not a bacterium, amoxicillin cannot kill it. You can take it at the same time as your antibiotic, and it helps maintain the integrity of your intestinal lining while preventing harmful bacteria from colonizing your vulnerable colon.
Another major clinical development involves the off-label use of bile acid sequestrants for patients who cannot tolerate metformin ER. Drugs like colesevelam physically bind to irritating bile acids in the gut, neutralizing them. This allows sensitive patients to continue their diabetes therapy without severe GI side effects.
Expert Insight: The Probiotic Timing Rule
If you are using a standard bacterial probiotic like Lactobacillus instead of a yeast-based option, timing matters enormously. Never take a bacterial probiotic at the same time as amoxicillin, because the antibiotic will kill it on contact. Space them at least two to three hours apart so the beneficial bacteria can survive the journey to your colon.
How a Pharmacist Evaluates Medication-Induced Diarrhea
When a patient asks me about diarrhea from their medications, I treat it as a diagnostic opportunity. I never just hand over a box of anti-diarrheal pills. Instead, I sit down with the patient and map out their entire daily routine.
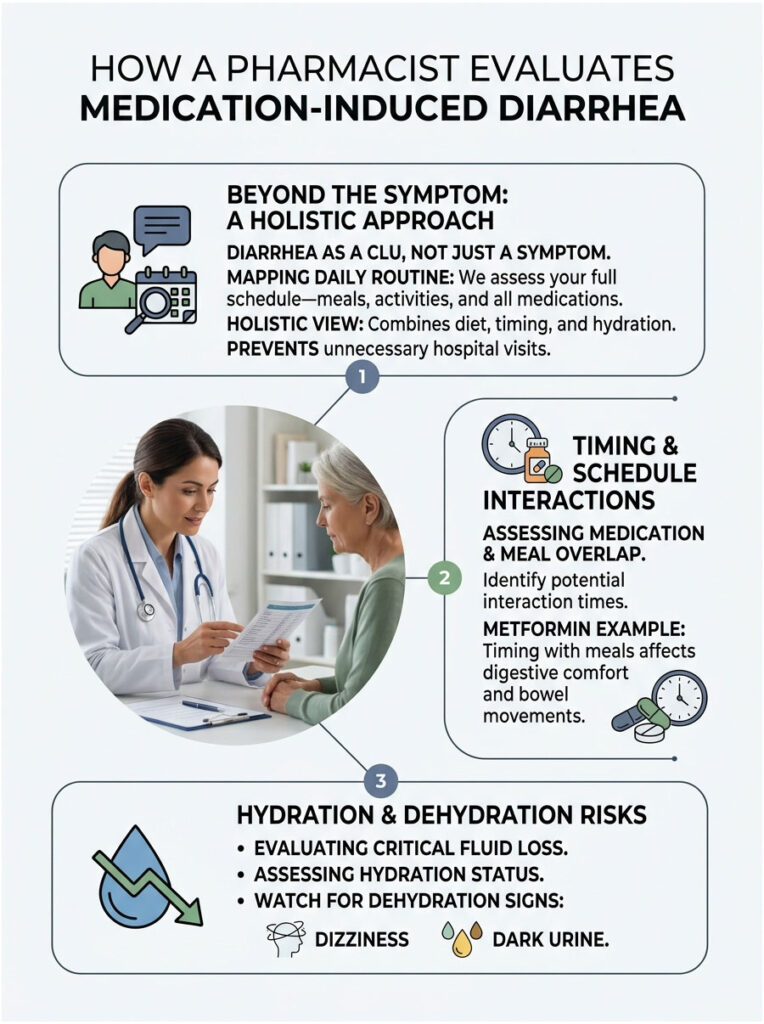
We look at what time they wake up, what they eat, and exactly when they take each pill. Often, the fix is surprisingly simple once we put the schedule on paper. A patient might be taking metformin on an empty stomach with black coffee, which naturally stimulates bowel movements. By moving that one pill to the middle of dinner, the diarrhea stops completely.
I also assess baseline hydration status. Chronic diarrhea aggressively depletes your body of essential water. If a patient reports dizziness or dark urine along with stomach issues, I immediately shift the conversation to hydration protocols.
This holistic approach, looking at diet, pill timing, and fluid intake together, is what separates a good outcome from a preventable hospital visit.
Practical Strategies to Manage Medication-Related Diarrhea
Strategic Medication Timing
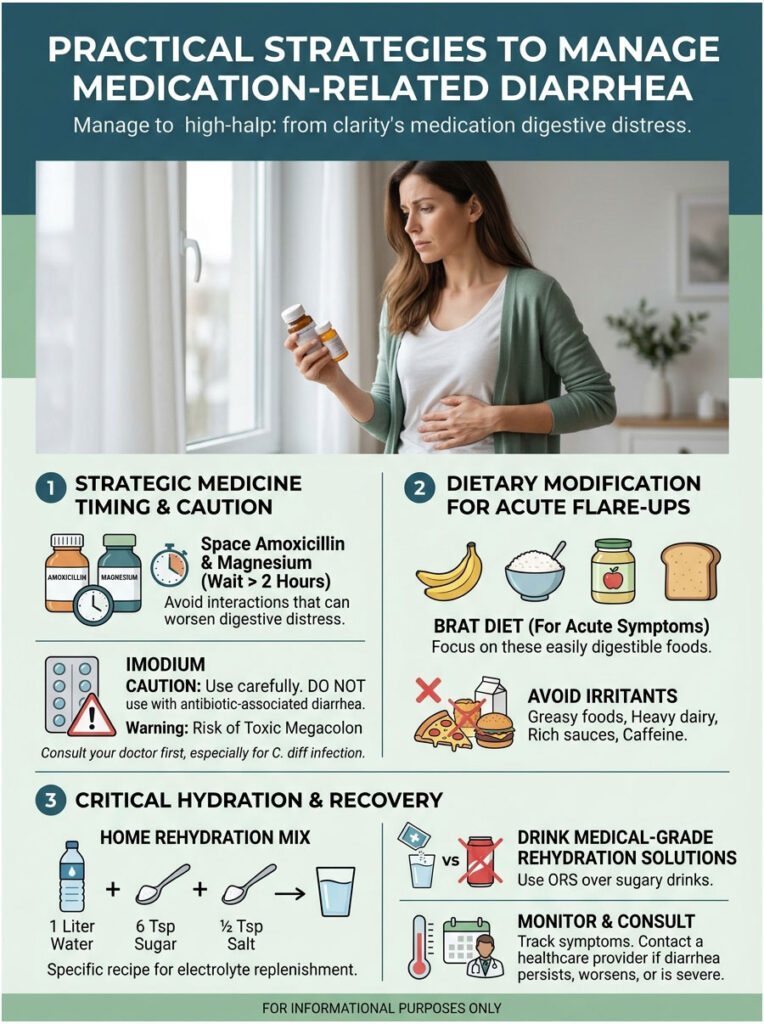
How you schedule your pills has a direct impact on your gut health. Never take amoxicillin and magnesium at the same time, because the mineral can bind to the antibiotic molecules and prevent proper absorption. This leaves both chemicals sitting in your gut, creating ideal conditions for diarrhea.
Space them at least two hours apart. Always take supplements after your prescription drugs have had time to digest. And always take prednisone with a heavy, fat-containing meal, which acts as a physical buffer against gastritis. Never take a steroid on an empty stomach.
The BRAT Diet for Acute Flare-Ups
When your stomach is actively upset, switch to the BRAT diet: bananas, rice, applesauce, and toast. These foods are bland, easy to digest, and rich in soluble fiber, which absorbs excess fluid in the bowel and adds bulk to watery stools.
Avoid greasy, fried foods and heavy dairy completely until your stomach settles. These require large amounts of bile to digest. If you are already dealing with metformin-related bile acid issues, eating heavy foods will make things worse.
Hydration Protocols for Severe Fluid Loss
Medication-induced diarrhea rapidly drains your body of water and electrolytes. Do not rely on sugary sports drinks to rehydrate. High sugar content actually worsens osmotic diarrhea by pulling more water into the gut.
Instead, use a medical-grade oral rehydration solution (ORS), available at any pharmacy. You can also make an effective version at home: mix one liter of clean water, six level teaspoons of sugar, and half a teaspoon of table salt. Sip it slowly throughout the day.
An Important Warning About Imodium
Patients frequently ask whether they can take loperamide (Imodium) to stop the bathroom trips. If your diarrhea is caused strictly by metformin or magnesium, Imodium is generally safe for a day or two.
However, if you have antibiotic-associated diarrhea, Imodium can be dangerous. If you have unknowingly developed a C. diff infection, your body is using diarrhea to flush out bacterial toxins. Taking an anti-diarrheal paralyzes the bowel and traps those toxins inside, which can lead to a life-threatening condition called toxic megacolon.
Advanced Dietary Management During Medication Therapy
Soluble Fiber vs. Insoluble Fiber
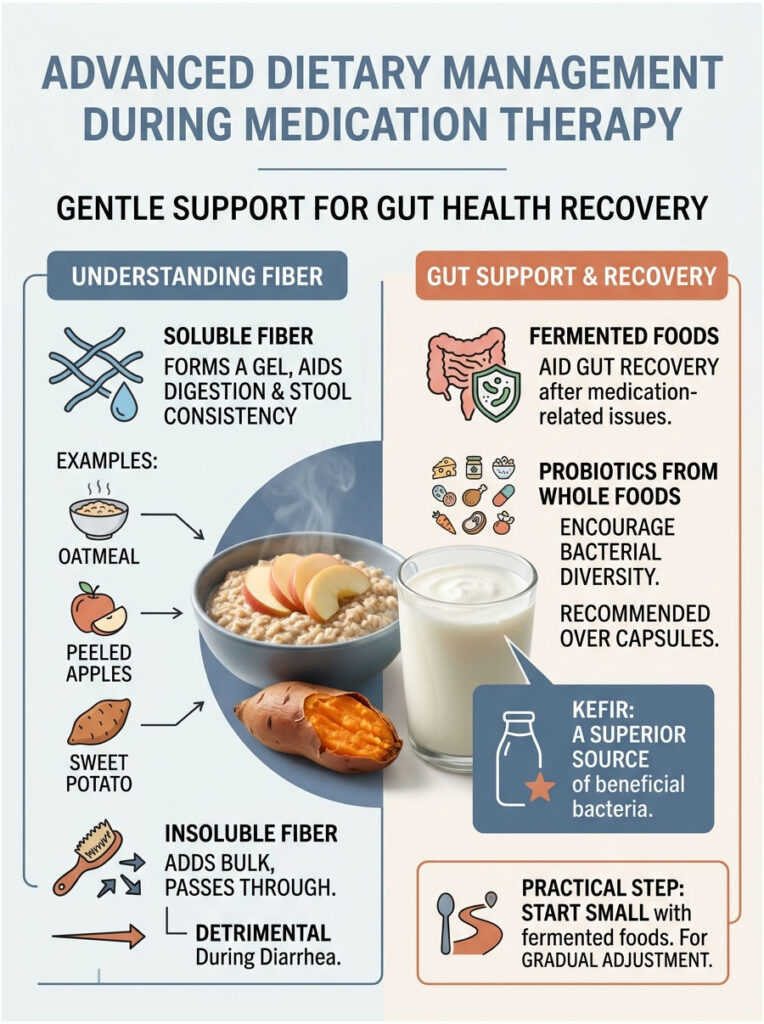
Not all fiber is helpful when you have diarrhea. Insoluble fiber, found in raw vegetables and wheat bran, acts like a stiff broom that sweeps through your intestines and speeds up digestion, making diarrhea worse.
Soluble fiber is what you need. It dissolves in water to form a thick, soothing gel that slows rapid digestion and binds loose stools together. Excellent sources include warm oatmeal, peeled apples, and sweet potatoes. Eating a bowl of plain oatmeal 30 minutes before taking metformin can significantly reduce bile acid-related symptoms.
Fermented Foods for Gut Recovery
Once the acute diarrhea phase has passed, focus on rebuilding your gut bacteria. While probiotic capsules are effective, real food provides a broader spectrum of bacterial diversity.
Kefir, a fermented milk drink, contains up to 60 different strains of beneficial bacteria and yeasts, making it far superior to standard grocery store yogurt. Other strong options include unpasteurized sauerkraut, kimchi, and traditional miso soup. Start with small portions, about one tablespoon a day, and let your stomach adjust gradually.
When to Seek Emergency Medical Care
Most cases of medication-induced diarrhea are an inconvenience, not a crisis. But some situations require immediate medical attention. Knowing the warning signs could prevent serious harm.
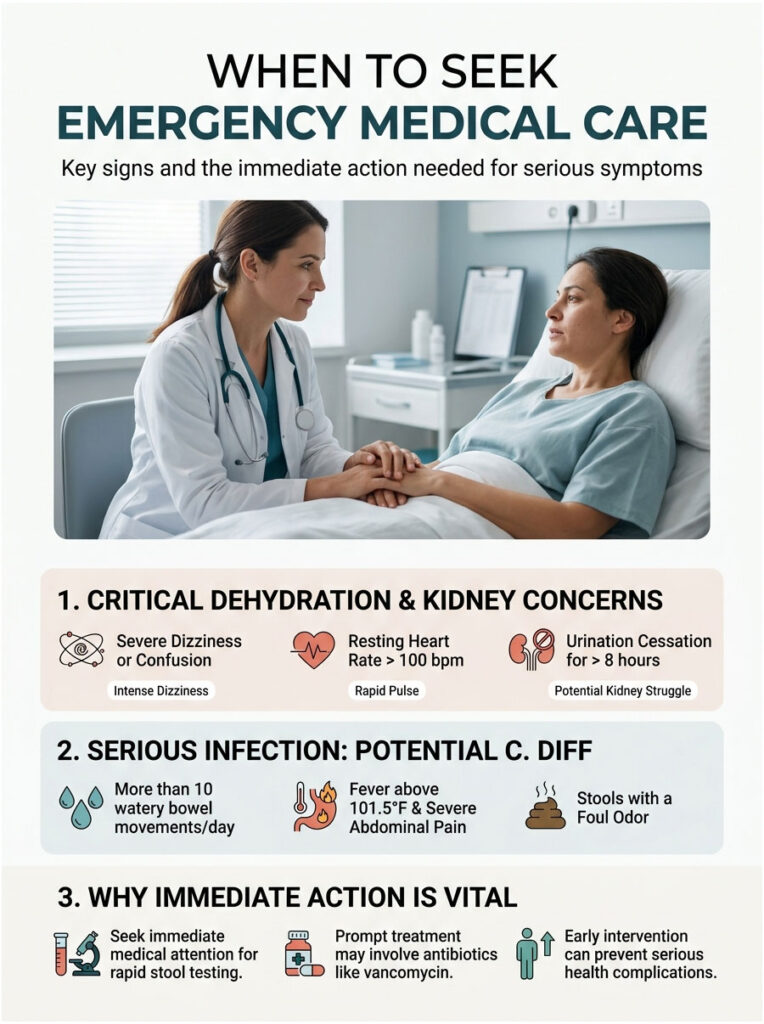
Signs of Severe Dehydration
When you lose large amounts of fluid through diarrhea, your blood volume drops and your heart works harder to compensate. Watch for a resting heart rate above 100 beats per minute, intense dizziness when standing, and dark-colored urine. If you have not urinated in over eight hours, your kidneys may be struggling. These are signs of clinical dehydration that require intravenous fluids at a hospital.
Signs of a C. diff Infection
If your antibiotic-associated diarrhea escalates to more than ten watery bowel movements per day, suspect C. diff immediately. Other red flags include fever above 101.5 degrees Fahrenheit, severe abdominal pain, and an abnormally foul odor.
Do not wait for your doctor to return your call. Go to an urgent care clinic or emergency room for a rapid stool test. Prompt treatment with targeted antibiotics like vancomycin is critical.
Long-Term Gut Rehabilitation After Medication Damage
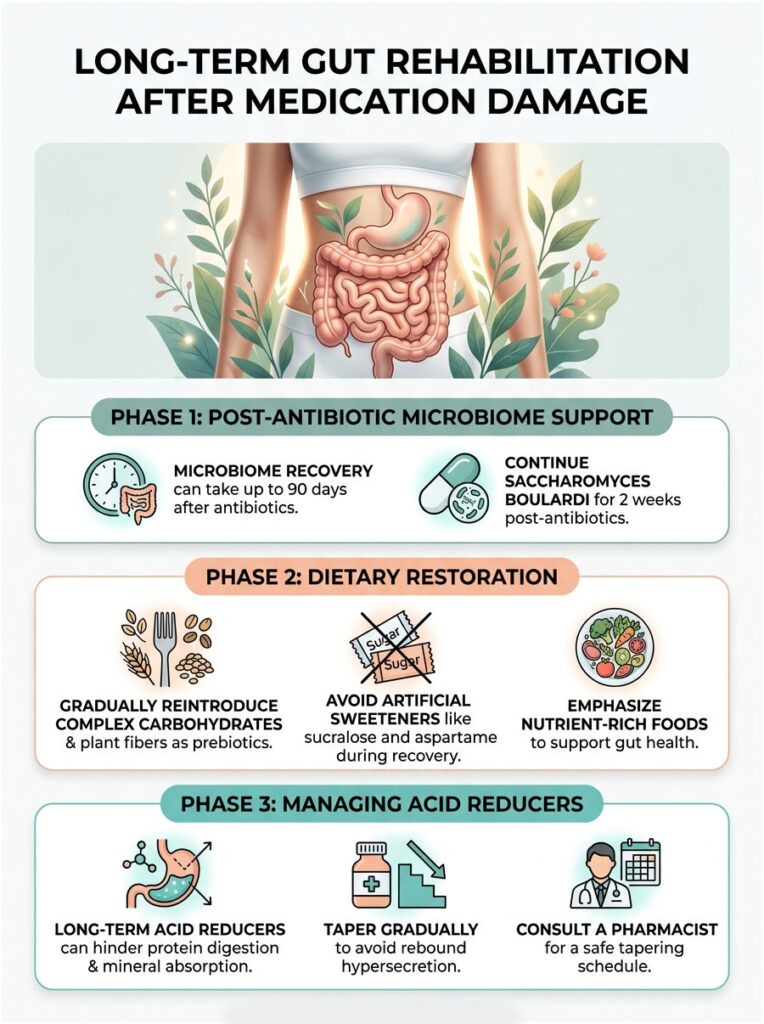
Rebuilding Your Microbiome After Antibiotics
Clinical studies show it can take up to 90 days for gut bacteria to fully normalize after a course of antibiotics. Continue taking Saccharomyces boulardii for at least two weeks after your final antibiotic dose. Gradually reintroduce complex carbohydrates and diverse plant fibers, which serve as prebiotics that feed your good bacteria.
Avoid artificial sweeteners like sucralose and aspartame during this recovery window. Emerging research suggests these chemicals can disrupt the repopulation of healthy gut flora.
Weaning Off Acid-Suppressing Medications Safely
If you took prednisone, your doctor may have prescribed an acid reducer like omeprazole to prevent gastritis. While helpful short-term, long-term use of acid reducers creates its own problems, including reduced protein digestion and poor mineral absorption.
Do not stop taking an acid reducer abruptly. Your stomach will overproduce acid in a painful process called rebound hypersecretion. Instead, work with your pharmacist to taper off gradually, typically by cutting the dose in half for a week, then switching to every other day.
Real-World Case Studies
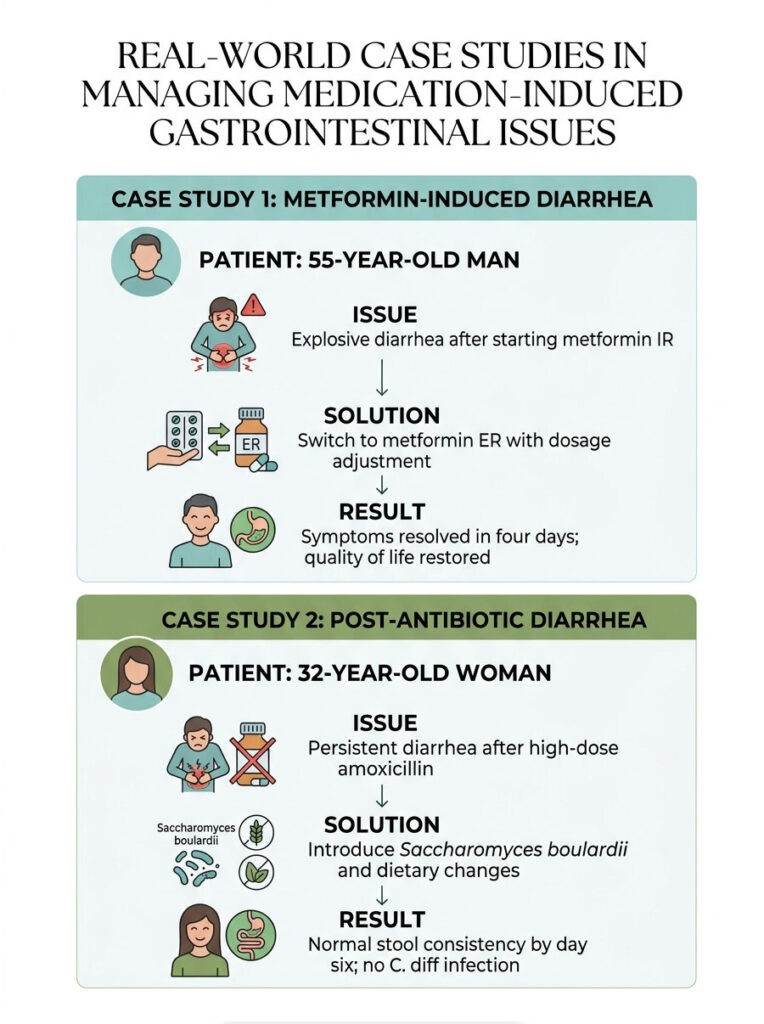
Case Study 1: Resolving Metformin-Induced Diarrhea
David, age 55, was recently diagnosed with Type 2 diabetes and started on 1000 mg of metformin immediate-release twice daily. Within a week, he experienced explosive diarrhea after every meal and was ready to quit the medication entirely.
During our consultation, I explained the difference between the immediate-release and extended-release formulations. The rapid drug dump from the IR version was overwhelming his gut and triggering bile acid malabsorption. I contacted his physician, and we switched David to 500 mg of metformin ER taken in the middle of his largest meal.
Within four days, his symptoms resolved completely. His blood sugar stayed well controlled, and he got his quality of life back.
Case Study 2: Managing Post-Antibiotic Diarrhea
Sarah, a 32-year-old teacher, was prescribed a 10-day course of high-dose amoxicillin for a severe sinus infection. By day four, she developed persistent diarrhea and was terrified she had contracted C. diff.
After reviewing her symptoms carefully, there was no fever, no severe cramping, and no blood present. It was a straightforward case of microbiome dysbiosis. I started her on Saccharomyces boulardii twice daily alongside her antibiotic and advised her to increase soluble fiber intake with oatmeal and ripe bananas. By day six, her stool consistency was back to normal.
These cases illustrate why understanding the root cause matters. FDA adverse event data shows that over 60% of GI-related drug complaints can be resolved without stopping the primary medication.
Key Takeaways
Amoxicillin, magnesium, prednisone, and metformin can all cause diarrhea, but through entirely different biological pathways:
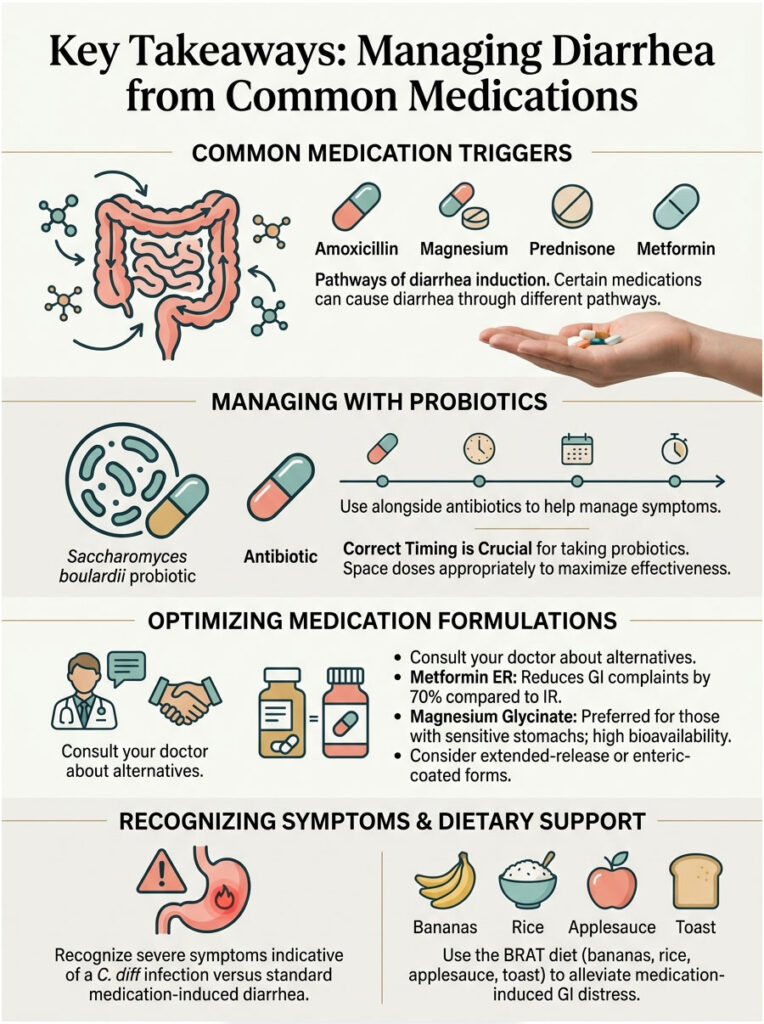
- Amoxicillin disrupts your gut microbiome by killing healthy bacteria.
- Magnesium acts as an osmotic laxative that pulls water into the bowel.
- Metformin blocks bile acid reabsorption and accelerates gut motility.
- Prednisone damages the stomach’s protective mucus layer, causing gastritis.
You do not have to suffer in silence. Ask your doctor about switching to an extended-release or enteric-coated version of your medication. Consider adding Saccharomyces boulardii when taking antibiotics. Use the dietary strategies, hydration protocols, and timing adjustments outlined in this guide to manage your symptoms safely.
Never stop your prescribed medications abruptly without talking to your healthcare provider first. With the right knowledge and a proactive approach, you can control these side effects and stay on the treatment plan that keeps you healthy.
Frequently Asked Questions
Why do Amoxicillin, Magnesium, Prednisone, and Metformin all cause diarrhea if they are different types of drugs?
As a pharmacist, I explain to patients that while these drugs differ, they each disrupt the GI tract via unique biological pathways. Amoxicillin causes gut microbiome dysbiosis by killing good bacteria; Magnesium creates an osmotic gradient that pulls water into the colon; Metformin triggers bile acid malabsorption; and Prednisone causes corticosteroid-induced gastritis by stripping the stomach’s protective mucus layer.
Can I take a probiotic at the same time as my Amoxicillin prescription?
Yes, but timing is critical. If using a bacterial probiotic like Lactobacillus, space it at least 2 to 3 hours away from your Amoxicillin dose so the antibiotic doesn’t kill the supplement. Alternatively, I recommend Saccharomyces boulardii for AAD (antibiotic-associated diarrhea) because it is a yeast-based probiotic that Amoxicillin cannot destroy, allowing you to take it simultaneously.
Is Metformin ER better than Metformin IR for preventing diarrhea?
Absolutely. Clinical data shows a 70 percent reduction in gastrointestinal complaints when patients switch from the Immediate Release (IR) to the Extended Release (ER) formulation. The ER version prevents the sudden chemical spike that overwhelms the gut, significantly reducing the risk of bile acid malabsorption and urgent bowel movements.
Which form of magnesium is least likely to cause an osmotic laxative effect?
Magnesium Glycinate is the preferred choice for those with sensitive stomachs. Because it is bound to the amino acid glycine, it has very high bioavailability and is absorbed efficiently through the intestinal wall. This leaves very little mineral residue behind to pull water into the colon, unlike Magnesium Oxide, which has low absorption and a high diarrhea risk profile.
Why does Prednisone cause stomach pain and rapid digestion?
Prednisone inhibits prostaglandins, which are the chemical messengers responsible for maintaining your stomach’s protective mucus lining. Without this barrier, your gastric mucosa becomes irritated by stomach acid—a condition known as corticosteroid-induced gastritis. This irritation can speed up motility as your body attempts to expel the acid, leading to cramping and loose stools.
How do I know if my diarrhea is a side effect or a dangerous C. diff infection?
Standard medication-induced diarrhea is usually mild and manageable. However, if you experience more than 10 watery stools a day, a fever over 101.5°F, severe abdominal cramping, or a distinct foul odor, you may have a Clostridioides difficile (C. diff) infection. If these red flags appear after taking Amoxicillin, seek emergency medical care immediately.
What is the maximum dose of supplemental magnesium I can take safely?
The National Institutes of Health sets the tolerable upper intake level for supplemental magnesium at 350mg per day for adults. Exceeding this dose frequently triggers an osmotic fluid shift, where the excess mineral acts like a sponge in your intestines, leading to medication-induced diarrhea and potential electrolyte imbalances.
Is it safe to take Imodium (Loperamide) for antibiotic-associated diarrhea?
I generally advise against using Imodium for diarrhea caused by antibiotics like Amoxicillin. If the diarrhea is actually caused by a C. diff infection, Imodium can paralyze the bowel and trap dangerous toxins inside your colon, potentially leading to a life-threatening condition called toxic megacolon. It is safer to use Imodium only for Metformin or Magnesium-related issues.
How does the BRAT diet help with medication-induced GI distress?
The BRAT diet (Bananas, Rice, Applesauce, Toast) focuses on foods high in soluble fiber. Soluble fiber absorbs excess water in the intestinal tract and turns into a soothing gel, which adds bulk to watery stools and slows down rapid digestion. This is especially helpful for counteracting the effects of Metformin and Magnesium.
What is the ‘perfect storm’ of polypharmacy in relation to diarrhea?
A perfect storm occurs when a patient takes multiple GI-irritating drugs at once, such as Amoxicillin (killing flora), Metformin (speeding motility), and Magnesium (pulling in water). This combination multiplies the risk of severe dehydration and hypomagnesemia symptoms, making it vital to coordinate dose timing and use protective strategies like probiotics and meal-time administration.
How long does it take for the gut to recover after finishing Amoxicillin?
It can take up to 90 days for your gut microbiome to fully normalize after a course of broad-spectrum antibiotics. To aid this recovery, I recommend continuing targeted probiotics for at least two weeks post-treatment and gradually increasing prebiotic fibers and fermented foods like kefir to rebuild bacterial diversity.
Can taking Metformin with food really stop the diarrhea?
Yes, taking Metformin—especially the ER version—in the middle of a large, heavy meal provides a physical buffer for the stomach lining. Food slows the absorption rate and helps mitigate bile acid malabsorption metformin issues, allowing the drug to be processed more gently by the small intestine and colon.
Disclaimer
This article is for educational and informational purposes only and does not constitute official medical advice. While written by a licensed clinical pharmacist, you should never alter, start, or stop any prescribed medication regimen without directly consulting your primary care physician or local pharmacist. Every patient’s medical history is unique, and complex polypharmacy interactions require personalized, professional clinical oversight.
References
- American Journal of Gastroenterology – https://journals.lww.com/ajg/ – Provided clinical statistics on the prevalence of antibiotic-associated diarrhea in outpatient settings (2021).
- National Institutes of Health (NIH) – https://ods.od.nih.gov/ – Provided the tolerable upper intake levels for supplemental magnesium and osmotic fluid shift data.
- U.S. Food and Drug Administration (FDA) – https://www.fda.gov/ – Reference for FAERS data regarding the tolerability of Metformin ER versus IR formulations.
- Journal of Clinical Gastroenterology – https://journals.lww.com/jcge/ – Peer-reviewed study on the efficacy of Saccharomyces boulardii in the prevention of AAD.
- Gastroenterology & Hepatology Journal – https://www.ncbi.nlm.nih.gov/pmc/journals/471/ – Source for the pathophysiology of bile acid malabsorption and its interaction with Metformin.
- Mayo Clinic Proceedings – https://www.mayoclinicproceedings.org/ – Provided clinical guidelines for managing corticosteroid-induced gastritis and mucosal protection.






