

As a board-certified gastroenterologist with over fifteen years of clinical experience, I meet patients every week who are genuinely afraid to eat outside their homes. They describe a disruptive, embarrassing symptom that controls their entire daily routine. If you are dealing with explosive diarrhea after eating, know that you are not alone, and this is not something you are imagining.
Table of Contents
Doctors call this condition postprandial diarrhea. It is a complex physiological response, not a random event or a simple upset stomach. Many people assume they just ate something bad or have a weak gut.
The real underlying causes usually involve rapid gastric emptying, severe bile acid malabsorption, or an overactive nervous system response. In this clinical guide, we will walk through the exact biomechanical and biochemical drivers behind sudden bowel urgency after meals, along with diagnostic criteria from leading medical institutions to help you identify your specific triggers.
Once you understand the root cause of your digestive urgency, you can move beyond temporary symptom management and into targeted, evidence-based treatments that actually work.
Quick Answer: Explosive diarrhea after eating is primarily caused by an exaggerated gastrocolic reflex, Bile Acid Malabsorption (BAM), Dumping Syndrome, or specific food intolerances. When food enters the stomach, hormonal signals tell the colon to empty. In healthy individuals, this is a gentle process. In patients with underlying gut dysfunction, however, this reflex triggers violent, rapid contractions that lead to immediate, watery bowel movements.
Key Statistics on Postprandial Diarrhea
- Prevalence: Up to 1 in 5 Americans suffer from some form of Irritable Bowel Syndrome, with diarrhea being a primary symptom for many.
- Misdiagnosis Rate: Research from the American College of Gastroenterology shows that up to 30 percent of patients diagnosed with IBS-D actually have Bile Acid Malabsorption.
- Surgical Impact: Roughly 20 percent of patients who undergo gallbladder removal surgery develop chronic postprandial diarrhea.
- Transit Time Acceleration: In patients with an overactive gastrocolic reflex, colonic contractions can increase by up to 50 percent within just 15 minutes of eating.
- Enzyme Deficiency: Exocrine Pancreatic Insufficiency affects up to 10 percent of patients with chronic, unexplained gastrointestinal distress.
- Dietary Triggers: Over 70 percent of patients with functional gut disorders experience significant relief after adopting a Low FODMAP dietary protocol.
Understanding Postprandial Diarrhea: The Core Concept
In clinical practice, the timing of a bowel movement provides the most important diagnostic clue. When a patient reports sudden diarrhea after meals, my immediate focus shifts to the mechanical and neural pathways of the upper digestive tract. Postprandial diarrhea involves the urgent passing of loose, watery stool within a very short window after eating.
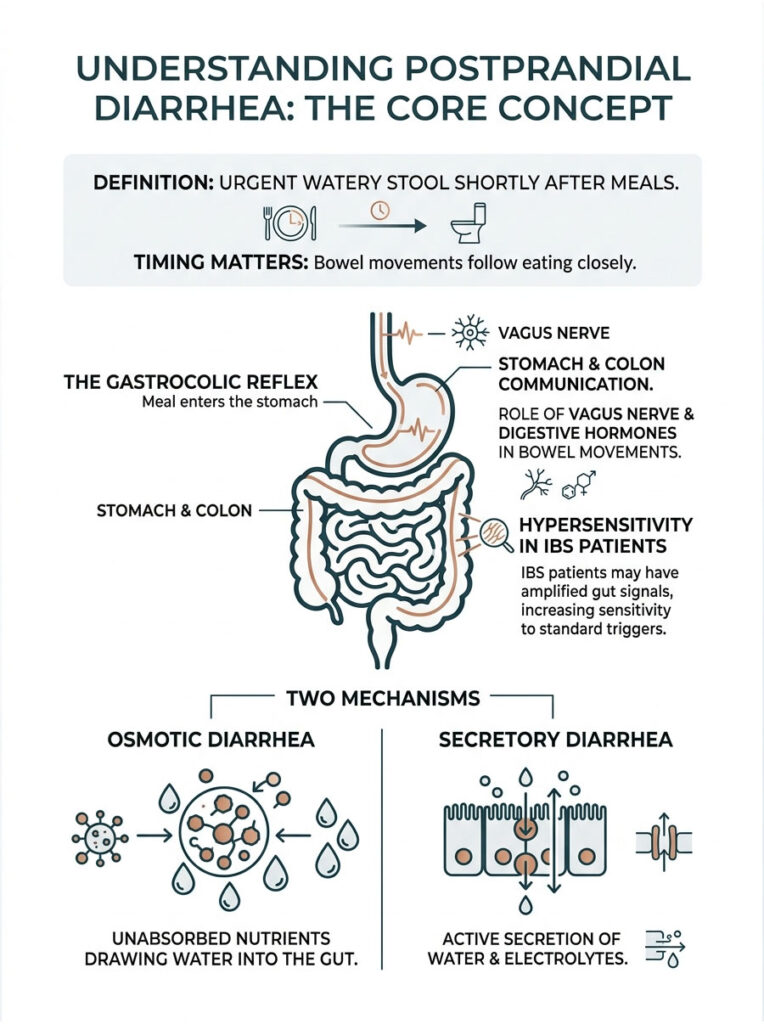
This reaction window can range from a few minutes to a couple of hours. To understand what goes wrong, we first need to understand what the body is supposed to do. The human digestive tract is a highly coordinated muscular tube that relies on a delicate balance of chemical messengers and physical stretch receptors. When this system falls out of sync, the results are rapid and severe.
How the Gastrocolic Reflex Works
Your stomach and colon are in constant communication. The moment you take a bite of food, your stomach physically expands. This stretching stimulates receptors embedded deep within the stomach wall.
Those receptors send immediate electrical signals through the vagus nerve to your brain. The brain then relays a message down to the lower digestive tract, triggering the release of digestive hormones like cholecystokinin and gastrin.
These hormones travel through the bloodstream and bind to receptors in the colon. Their message is simple: contract and push existing waste out to make room for the new food being digested. Medical textbooks call this the gastrocolic reflex.
In a healthy person, this reflex produces a mild, barely noticeable wave of muscle contractions. You might feel a slight urge to use the restroom an hour after a big meal, but it is rarely urgent.
Patients with irritable bowel syndrome, however, have a hypersensitive nervous system. Their gut-brain axis misinterprets normal stomach stretching as a severe threat. The body drastically amplifies the gastrocolic reflex, turning a gentle wave into a violent spasm. The colon squeezes aggressively, forcing out contents before water can be properly absorbed. This is exactly why some patients experience explosive diarrhea after eating before they even finish their plate.
Secretory vs. Osmotic Diarrhea: Two Distinct Mechanisms
When investigating sudden diarrhea after meals, gastroenterologists classify the symptom into two primary mechanical failures: secretory and osmotic.
Osmotic diarrhea occurs when unabsorbed nutrients pull excess water into the intestinal lumen. Think of it like pouring salt onto a snail; water rushes out to balance the concentration. A very similar process happens inside your gut. If you eat highly fermentable sugars that your body cannot absorb, those sugars travel into the colon intact, act like a biological sponge, and draw massive amounts of fluid from your bloodstream directly into your bowels. The hallmark of osmotic diarrhea is that it completely stops when you stop eating the offending foods.
Secretory diarrhea, on the other hand, involves a completely different mechanism. The intestinal wall actively secretes water and electrolytes into the gut cavity, often driven by severe irritation, bacterial toxins, or unabsorbed bile acids. This type is typically more severe and can occur regardless of food intake. You might even wake up at night to use the restroom. However, eating can certainly make the fluid secretion worse, leading to an immediate rush to the toilet.
Biochemical and Mechanical Drivers of Explosive Diarrhea After Eating
To break the cycle of urgent bathroom trips, we need to look closely at specific physiological failures. Many patients spend years trying different restrictive diets without success because they are fighting a mechanical problem, not a simple food allergy. Based on extensive clinical testing, these three conditions are the most frequent culprits.
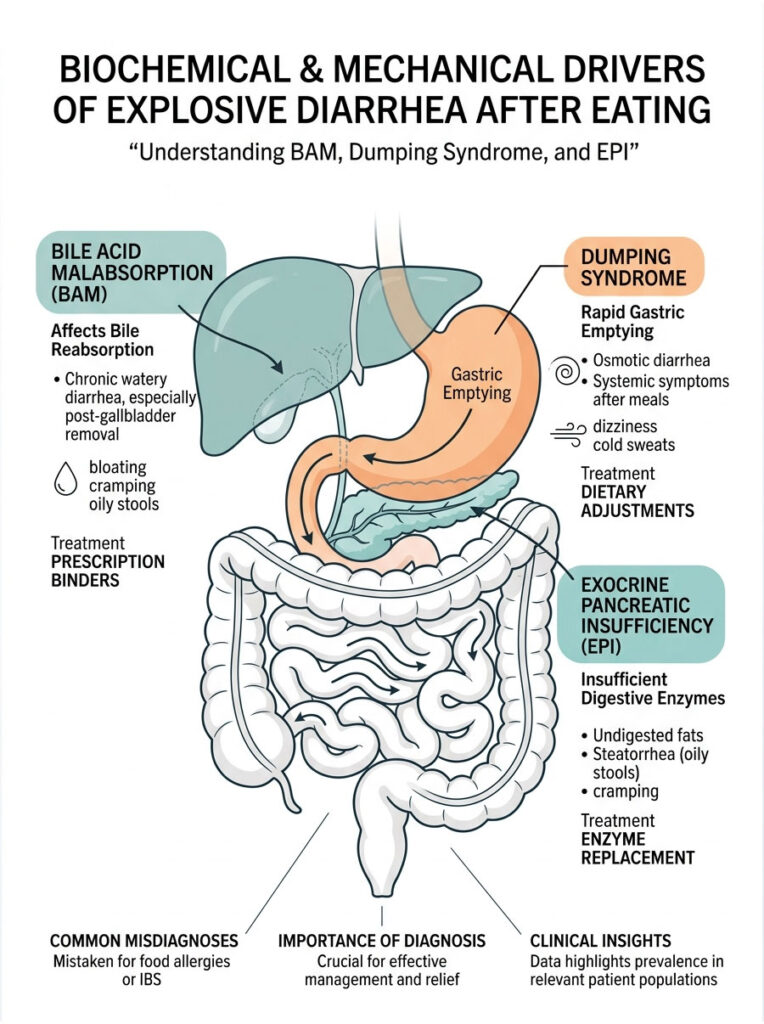
Bile Acid Malabsorption (BAM) and Gallbladder Removal
If you regularly suffer from explosive diarrhea after eating greasy food, you may be dealing with a bile processing error. Your liver produces bile acids, which are essential biological detergents that break down dietary fats. Normally, your gallbladder stores this concentrated bile and releases it into the small intestine when you eat a fatty meal.
Once the bile acids have done their job, they travel to the terminal ileum at the very end of the small intestine. In a healthy digestive tract, this area reabsorbs about 95 percent of bile acids and sends them back to the liver. Doctors call this efficient recycling system enterohepatic circulation.
In patients with Bile Acid Malabsorption, this recycling system breaks down. The terminal ileum fails to reabsorb the bile, and these highly acidic chemicals spill directly into the large intestine. Bile acids are toxic to the sensitive lining of the colon. They act as a potent stimulant laxative, causing the colon to aggressively secrete water and contract violently to expel the irritant.
This condition is incredibly common in patients who have had their gallbladder removed. Without a storage organ, bile continuously drips into the intestines and overwhelms the absorption capacity. Data from the American College of Gastroenterology notes that up to 30 percent of patients diagnosed with diarrhea-predominant IBS actually suffer from BAM. If you have had gallbladder surgery, this is a highly probable cause of your daily symptoms. The good news is that it is also highly treatable with specific prescription binders.
Dumping Syndrome and Rapid Gastric Emptying
Another major structural cause of sudden diarrhea after meals is Dumping Syndrome. Instead of slowly grinding food and releasing it into the small intestine in controlled batches, the stomach dumps large amounts of undigested food into the small bowel all at once.
This rapid transit creates a massive osmotic shift. When a large volume of simple carbohydrates enters the small intestine prematurely, the resulting chyme is far too concentrated for the intestines to handle. To dilute this dense mixture, the body rapidly pulls massive amounts of fluid from surrounding blood vessels into the intestinal cavity, causing extreme bloating, painful cramping, and severe osmotic diarrhea.
Patients with Dumping Syndrome often experience systemic symptoms alongside their digestive distress. The rapid fluid loss can cause sudden drops in blood pressure, intense dizziness, cold sweating, and a racing heart rate within minutes of eating.
This condition is divided into two phases. Early dumping occurs within 15 to 30 minutes of eating and is driven by fluid shifts. Late dumping occurs one to three hours later and is caused by a massive spike and subsequent crash in blood sugar levels. It is especially common after bariatric surgery, but it can also occur in people with altered vagus nerve function or damage from severe viral gastroenteritis.
Exocrine Pancreatic Insufficiency (EPI) and Steatorrhea
Sometimes, the root problem originates directly in the pancreas. Your pancreas produces specialized digestive enzymes, including amylase, protease, and lipase, all essential for breaking down carbohydrates, proteins, and fats.
When the pancreas fails to produce enough of these enzymes, the resulting condition is Exocrine Pancreatic Insufficiency. Without adequate lipase, your body simply cannot digest dietary fats. These undigested lipids travel through your entire digestive tract, causing massive irritation and drastically speeding up intestinal transit times.
This leads to steatorrhea, a specific type of bowel movement characterized by stools that are pale yellow, excessively oily, bulky, and foul-smelling. Patients often notice their stool floats stubbornly in the toilet bowl and is difficult to flush.
If you experience explosive diarrhea after eating greasy food and notice these visual characteristics, investigating pancreatic enzyme failure is essential. Chronic pancreatitis, cystic fibrosis, and severe celiac disease can all permanently damage the pancreas and trigger EPI.
Dietary Triggers and Complex Intolerances
While mechanical and biochemical failures are common, we cannot ignore the profound impact of specific dietary components. Many patients unknowingly trigger their own severe symptoms by consuming foods their bodies lack the tools to process. Generic advice like “eat more fiber” is often unhelpful. In fact, adding bulky fiber to an inflamed gut can make symptoms exponentially worse.
The Role of FODMAPs, Fructose, and Sugar Alcohols
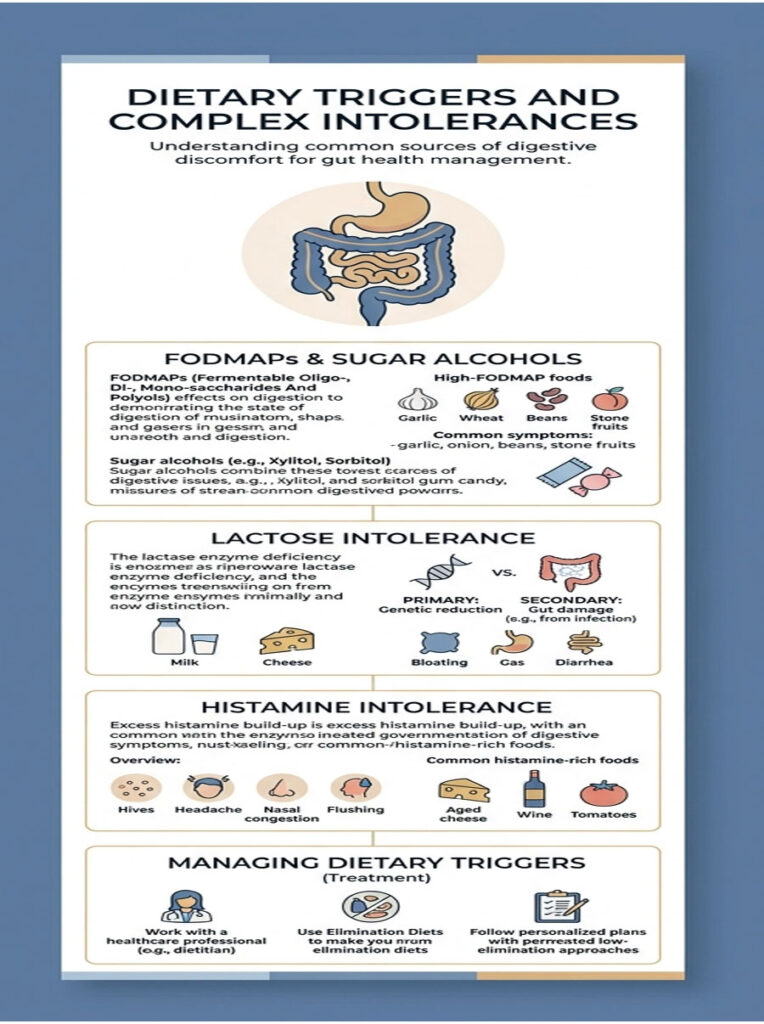
Modern gastroenterology has shifted its focus toward fermentable carbohydrates, collectively known as FODMAPs (Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols). These are short-chain carbohydrates that are notoriously difficult for the human small intestine to absorb.
Foods high in FODMAPs include garlic, onions, apples, wheat, and certain dairy products. When you consume high-FODMAP foods, these sugars travel undigested into the large intestine, where trillions of gut bacteria rapidly ferment them. This produces massive amounts of hydrogen and methane gas, aggressively stretching the intestinal walls and triggering a hypersensitive gastrocolic reflex.
Sugar alcohols are particularly problematic. Ingredients like sorbitol, xylitol, and erythritol are widely used in sugar-free gums, protein bars, and diet drinks. The human body cannot digest these artificial polyols. They bypass early digestion entirely and act as powerful osmotic agents in the colon, drawing in excess water and reliably causing explosive diarrhea after eating.
Many patients completely resolve their daily symptoms simply by eliminating artificial sweeteners from their diet. If you chew sugar-free gum or drink diet sodas regularly, you might be triggering osmotic diarrhea without realizing it.
Lactose Intolerance and Enzyme Deficiency
Lactose intolerance is the most well-known dietary trigger globally, but its severity is often underestimated. Lactose is a complex sugar found in milk and dairy products. To absorb it, the microvilli of your small intestine must produce an enzyme called lactase.
If you have a lactase deficiency, intact lactose molecules reach the colon unbroken. The resulting bacterial fermentation is often explosive and painful, causing severe trapped gas, abdominal bloating, and urgent watery stool within 30 to 120 minutes of dairy consumption. The speed of this reaction often leads patients to believe they have food poisoning, when it is actually a genetic enzyme deficit.
Primary lactase deficiency is genetic and develops naturally with age. Secondary lactase deficiency occurs when an illness like the stomach flu or severe celiac disease temporarily damages the intestinal lining and halts enzyme production.
Histamine Intolerance and Mast Cell Activation
Beyond sugars and fats, we must also consider the role of histamine. Histamine is a chemical naturally present in aged, fermented, and cured foods like aged cheeses, red wine, cured meats, and sauerkraut.
Normally, an enzyme called Diamine Oxidase (DAO) breaks down dietary histamine before it enters your bloodstream. Some patients, however, have a genetic deficiency in DAO production. When they eat high-histamine foods, the chemical floods their system.
Histamine binds to H1 and H2 receptors in the gut lining, triggering immediate fluid secretion and intense smooth muscle contractions. The result is a sudden, urgent need to use the restroom, often accompanied by skin flushing, headaches, or a runny nose. If your diarrhea comes with allergy-like symptoms after eating aged or fermented foods, histamine intolerance is a strong possibility. Treatment requires a strict low-histamine diet and DAO enzyme supplementation.
Comparison: Osmotic vs. Secretory Diarrhea Triggers
The following table breaks down the core differences between the primary mechanisms of postprandial urgency.
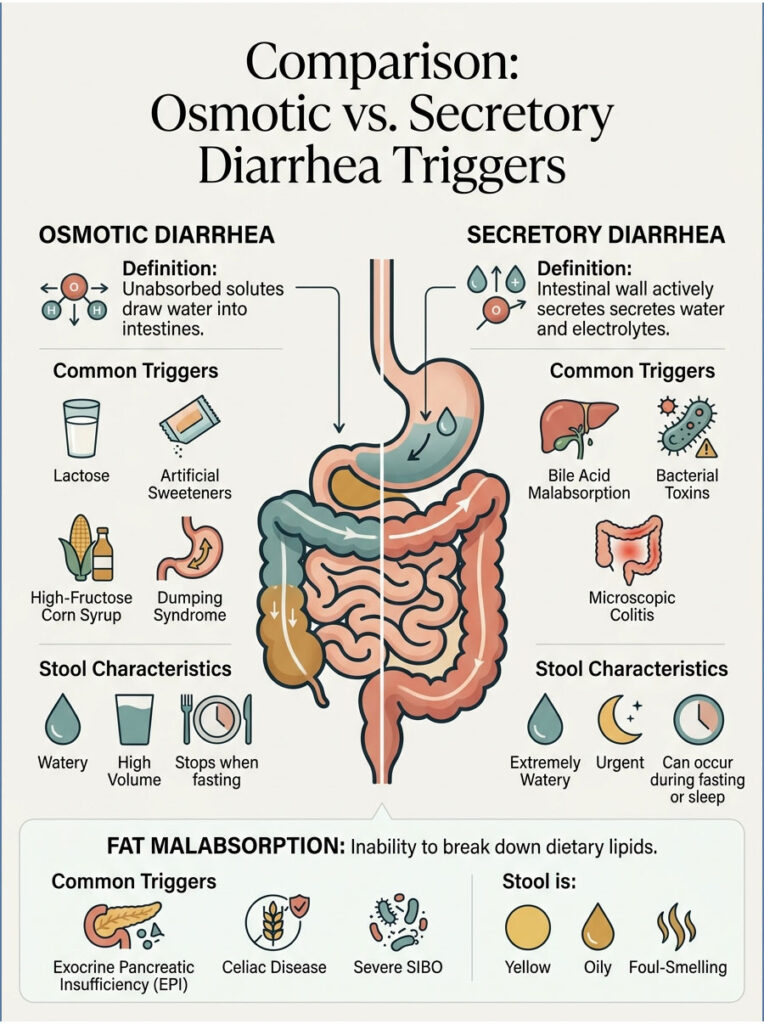
| Classification | Primary Mechanism | Common Triggers | Stool Characteristics |
| Osmotic Diarrhea | Unabsorbed solutes draw water into the intestines. | Lactose, artificial sweeteners, high-fructose corn syrup, Dumping Syndrome. | Watery, high volume. Stops when patient fasts. |
| Secretory Diarrhea | Intestinal wall actively secretes water and electrolytes. | Bile Acid Malabsorption, bacterial toxins, microscopic colitis. | Extremely watery, urgent. Can occur during fasting or sleep. |
| Fat Malabsorption | Inability to break down dietary lipids. | Exocrine Pancreatic Insufficiency (EPI), celiac disease, severe SIBO. | Yellow, oily, floating, foul-smelling (steatorrhea). |
Chronic Conditions and Inflammatory Pathways
Beyond mechanical failures and dietary triggers, we must evaluate underlying chronic diseases. Many severe inflammatory conditions initially present as simple postprandial urgency. If your symptoms persist despite strict dietary changes, a deeper pathological issue is likely at play.
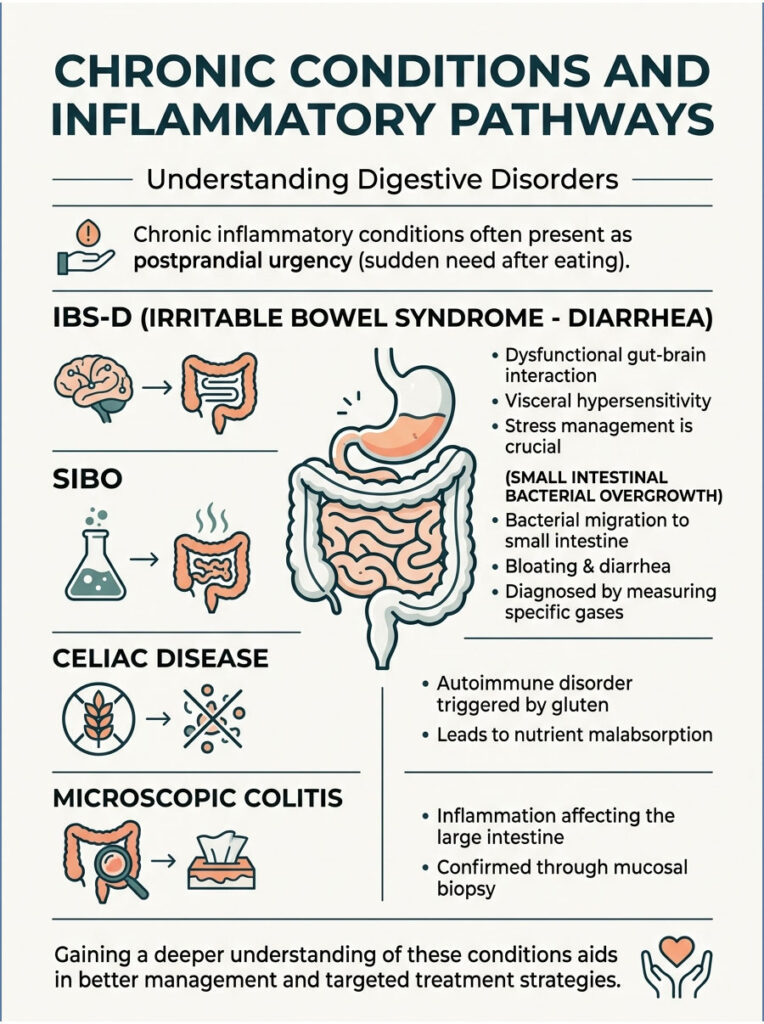
Irritable Bowel Syndrome (IBS-D) and Visceral Hypersensitivity
IBS with diarrhea (IBS-D) is officially classified as a disorder of gut-brain interaction. The physical structures of the intestines appear perfectly normal on a colonoscopy, but the nerves governing those structures are highly dysfunctional. Patients with IBS-D suffer from visceral hypersensitivity, meaning their internal pain receptors are constantly dialed up.
The gut and brain are intimately connected through the vagus nerve and a complex network of serotonin receptors. The human gut produces about 95 percent of the body’s total serotonin supply. When you experience stress or anxiety, your brain floods the digestive tract with neurochemicals that amplify the gastrocolic reflex. The intestines become hyper-reactive to normal food volumes, resulting in sudden diarrhea after meals.
For these patients, managing psychological stress is just as important as managing diet. Cognitive behavioral therapy and gut-directed hypnotherapy have shown remarkable success in calming this hyperactive neural pathway.
Small Intestinal Bacterial Overgrowth (SIBO)
The large intestine is designed to house trillions of beneficial bacteria, but the small intestine should remain relatively sterile. SIBO occurs when colonic bacteria migrate upward and colonize the small bowel. This usually happens because of a failure in the migrating motor complex, your gut’s internal cleansing wave that sweeps debris downward between meals.
When this wave fails, bacteria settle in the small intestine and intercept food before you can absorb the nutrients. They ferment carbohydrates prematurely in the upper digestive tract, creating rapid gas expansion. The sudden bloating puts immense pressure on the intestinal walls, triggering a rapid transit response.
This is why SIBO patients often report looking visibly bloated immediately after a meal, followed quickly by explosive diarrhea after eating. Diagnosis involves measuring specific gases (hydrogen, methane, or hydrogen sulfide) produced during digestion.
Celiac Disease and Microscopic Colitis
Celiac disease is a severe autoimmune condition where ingesting gluten causes the immune system to attack the small intestine. It systematically destroys the villi responsible for nutrient absorption, leading to chronic malabsorption, systemic inflammation, and frequent osmotic diarrhea. Even a tiny crumb of cross-contaminated bread can trigger a massive immune response. Blood tests checking for tTG-IgA antibodies are the first step in identifying this disease.
Microscopic Colitis, on the other hand, exclusively affects the large intestine. Unlike ulcerative colitis or Crohn’s disease, the colon looks perfectly normal during a routine colonoscopy. The inflammation is only visible under a microscope. It causes relentless secretory diarrhea that resists standard over-the-counter medications. A mucosal biopsy during colonoscopy is the only way to confirm this hidden diagnosis.
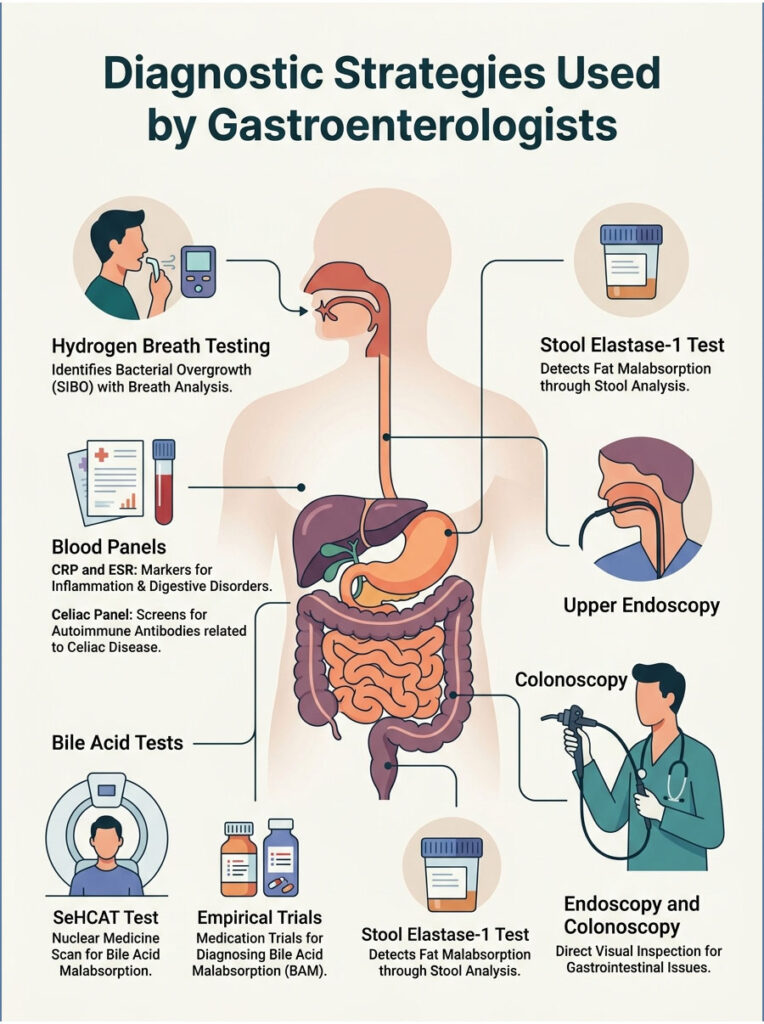
Diagnostic Strategies Used by Gastroenterologists
When a patient asks in desperation, “Why do I get diarrhea 20 minutes after eating?”, I do not guess at the cause. We follow a structured, evidence-based diagnostic pathway to rule out dangerous pathologies and zero in on the exact mechanical or chemical failure causing the distress.
Expert Tip: Never start multiple treatments at once. If you change your diet, begin a probiotic, and start a new prescription simultaneously, you will never know which intervention actually helped. Introduce changes one at a time, spaced about two weeks apart.
Hydrogen Breath Testing and Stool Elastase
To identify hidden bacterial and enzymatic issues, we use specific non-invasive tests. If SIBO is suspected, a comprehensive Hydrogen and Methane Breath Test is ordered. The patient drinks a specialized solution of lactulose or glucose. As bacteria ferment the sugar, they release specific gases that are absorbed into the blood and exhaled through the lungs.
By measuring gas levels in the breath every 15 minutes over a three-hour period, we can pinpoint where the bacterial overgrowth is located. This guides our antibiotic selection.
For patients showing signs of fat malabsorption (greasy steatorrhea), we use a Fecal Elastase-1 test. This painless stool test measures the amount of elastase passing through the digestive tract. Because elastase is extremely stable and is not degraded during digestion, low levels provide definitive proof of Exocrine Pancreatic Insufficiency.
Blood Panels and Inflammatory Markers
Before moving to invasive procedures, we draw a comprehensive series of blood labs. We check C-Reactive Protein (CRP) and Erythrocyte Sedimentation Rate (ESR), which are broad markers of systemic inflammation. Elevated levels point away from functional disorders like IBS and toward Inflammatory Bowel Disease.
We also run a full celiac panel for specific autoimmune antibodies. A complete blood count (CBC) helps identify anemia, which is a major red flag for hidden internal bleeding or severe malabsorption.
SeHCAT Testing and Empirical Trials for BAM
In Europe, doctors use a highly accurate nuclear medicine scan called the SeHCAT test to diagnose Bile Acid Malabsorption. It measures the retention rate of bile acids over seven days using a swallowed radioactive capsule.
However, this test is not FDA-approved or widely available in the United States. American gastroenterologists rely on an empirical medication trial instead. If a patient presents with classic symptoms, especially explosive diarrhea after eating greasy food following a gallbladder removal, we prescribe a short two-week course of bile acid sequestrants. These medications bind tightly to excess bile in the gut. If the patient’s symptoms resolve within a few days, the diagnosis is clinically confirmed without needing a scan.
Endoscopy and Colonoscopy Evaluations
When non-invasive tests do not provide a clear answer, we move to direct visual inspection. An upper endoscopy involves passing a tiny camera down the throat to examine the stomach and small intestine. We can take biopsies to check for celiac disease or severe ulcers.
A colonoscopy examines the entire length of the large intestine. While the preparation is notoriously unpleasant, the procedure itself is painless and potentially life-saving. We look for visible inflammation, bleeding polyps, or signs of Crohn’s disease.
Critically, we take random tissue biopsies throughout the colon even when the tissue looks perfectly healthy. This is the only way to catch Microscopic Colitis, which is a leading cause of sudden diarrhea after meals in older adults.
Differential Diagnosis of Postprandial Diarrhea

| Suspected Condition | Key Symptoms | Gold Standard Test | First-Line Treatment |
| Bile Acid Malabsorption | Yellow stool, worse after greasy foods, prior gallbladder surgery. | Empirical trial of bile acid binders, fecal bile acid test. | Bile acid sequestrants (Cholestyramine, Colesevelam). |
| SIBO | Severe bloating after eating, excessive belching. | Lactulose or Glucose Hydrogen Breath Test. | Gut-specific antibiotics (Rifaximin, Neomycin). |
| Exocrine Pancreatic Insufficiency | Oily, floating stools, weight loss, foul smell. | Fecal Elastase-1 Stool Test. | Pancreatic Enzyme Replacement Therapy (PERT). |
| Dumping Syndrome | Sweating, rapid heart rate, dizziness after high-carb meals. | Gastric Emptying Study, Oral Glucose Tolerance Test. | Dietary modification, smaller low-carb meals. |
Actionable Treatment Strategies and Clinical Protocols
Once the root cause of postprandial diarrhea is identified, we can implement targeted interventions. Generic advice like “drink more water” or “eat plain toast” is woefully insufficient for complex gastrointestinal disorders. The goal is not just surviving your meals, but actually enjoying eating again without fear.
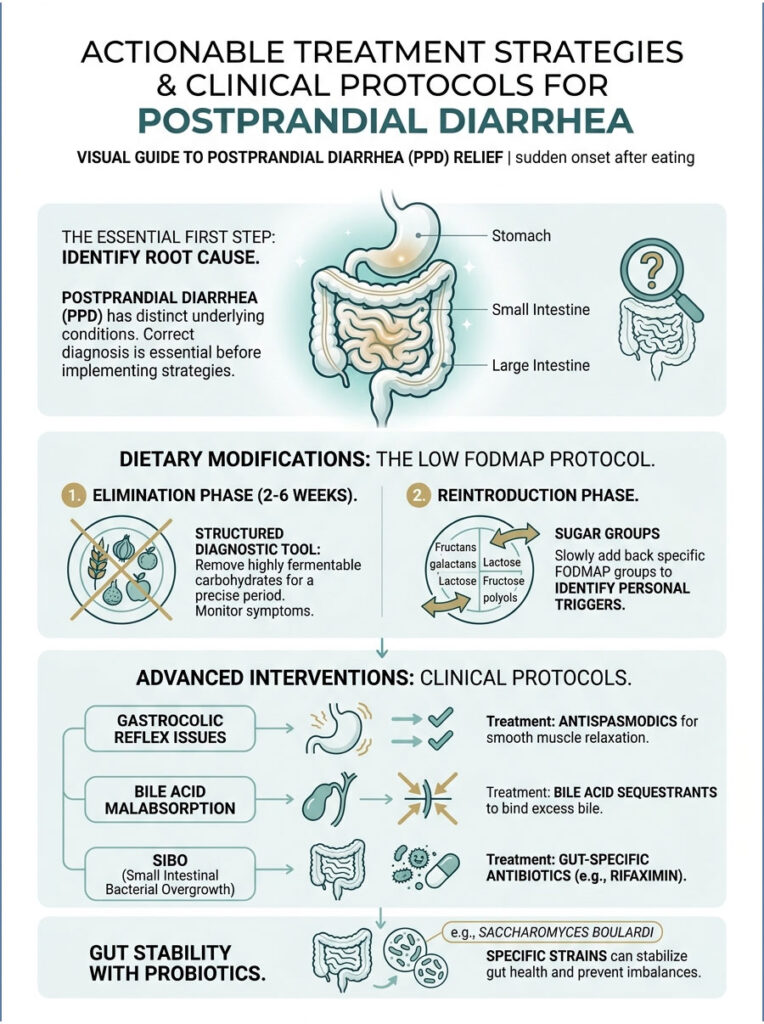
Dietary Modifications and the Low FODMAP Protocol
If osmotic diarrhea driven by carbohydrate fermentation is suspected, the Low FODMAP diet is the clinical gold standard. Developed by researchers at Monash University, this protocol is not a lifelong diet. It is a temporary, structured diagnostic tool.
The process starts with a strict elimination phase lasting two to six weeks, during which all highly fermentable carbohydrates are removed. If symptoms improve, patients move to a reintroduction phase where specific sugar groups (fructose, lactose, etc.) are added back one at a time over several days. This identifies your exact personal triggers.
By the end of the protocol, you will have a highly customized diet that prevents explosive diarrhea after eating while maintaining maximum nutritional variety.
Advanced Pharmacological Interventions
For patients with severe structural or neural issues, dietary changes alone may not be enough. If an overactive gastrocolic reflex is the main problem, antispasmodics like dicyclomine or hyoscyamine can relax the smooth muscles of the intestines and prevent violent contractions. We often advise taking these 30 minutes before a meal.
For Bile Acid Malabsorption, bile acid sequestrants like cholestyramine or colesevelam are truly life-changing. They bind to toxic bile acids in the gut, rendering them harmless. This effectively stops explosive diarrhea after eating greasy food.
Gut-specific antibiotics like Rifaximin are used to eradicate SIBO. Unlike standard antibiotics, Rifaximin stays entirely within the digestive tract, killing overgrown bacteria without causing systemic side effects.
Probiotics and Microbiome Modulation
The gut microbiome plays a massive role in regulating transit times, gas production, and immune responses. However, not all probiotics are created equal. A random multi-strain probiotic from the grocery store can sometimes worsen SIBO or osmotic diarrhea.
Clinical evidence supports using specific strains for specific problems. Saccharomyces boulardii, for instance, is a beneficial non-colonizing yeast with remarkable clinical efficacy. It stabilizes gut transit times, improves intestinal barrier function, and neutralizes certain bacterial toxins. Because it is a yeast, it survives antibiotic treatments, making it ideal for SIBO recovery.
Real-World Case Studies from Clinical Practice
Medical theory is helpful, but seeing how these diagnoses apply to real people makes the science easier to understand. These generalized case studies represent patient journeys I see in my clinic regularly.
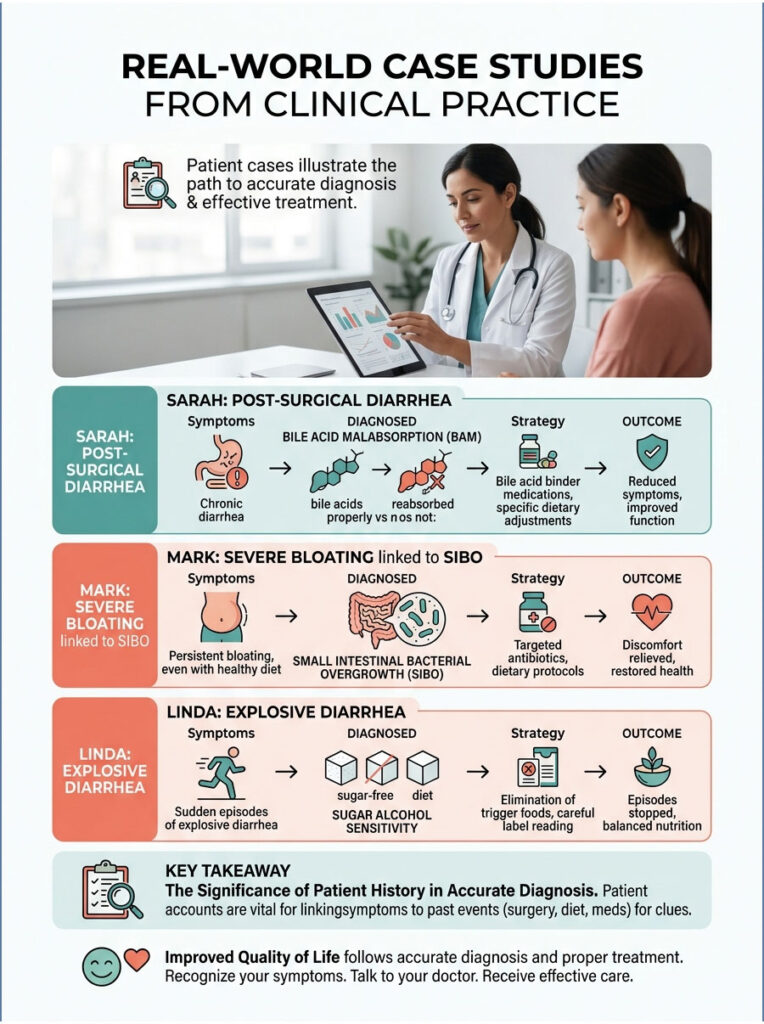
Case Study 1: The Post-Surgical Surprise
Sarah, a 42-year-old woman, had her gallbladder removed three years ago due to painful gallstones. Shortly after surgery, she began experiencing a terrifying new symptom. Every time she went out to dinner, she would barely finish her meal before needing to rush to the restroom.
Her previous doctor diagnosed standard IBS-D and told her to eat more fiber and manage stress. The extra fiber only worsened her bloating. When Sarah came to my clinic, the timeline was the golden key. Postprandial diarrhea starting immediately after cholecystectomy strongly suggested Bile Acid Malabsorption.
We started her on a daily trial of colesevelam. Within 48 hours, her sudden diarrhea after meals completely stopped. She could eat at restaurants again without fear.
Case Study 2: The Hidden Bacterial Hijacker
Mark, a 35-year-old marathon runner, ate an exceptionally healthy diet. Despite eating mostly organic vegetables and lean proteins, he developed severe bloating after every meal, followed within an hour by urgent, watery diarrhea.
He tried cutting out gluten, dairy, and soy, but nothing helped. A lactulose breath test revealed a massive hydrogen spike within the first 60 minutes, confirming severe SIBO. The healthy, fibrous vegetables Mark was eating were actually feeding the misplaced bacteria.
We treated him with a two-week course of Rifaximin and a temporary Low FODMAP diet. Once the bacterial overgrowth was eradicated, his gut normalized completely.
Case Study 3: The Sugar Alcohol Sabotage
Linda, a 55-year-old woman trying to lose weight, switched to “keto-friendly” protein bars and sugar-free iced coffees. Almost immediately, she developed severe watery diarrhea every afternoon. She was terrified she had colon cancer.
A colonoscopy showed a perfectly healthy colon with zero inflammation. The clue was in her dietary history. Linda was consuming massive amounts of erythritol and sorbitol hidden in her diet foods. These sugar alcohols were acting as powerful osmotic laxatives. By simply swapping artificial sweeteners for natural stevia and eating whole foods, her explosive diarrhea after eating vanished within 24 hours.
Red Flag Symptoms: When to Seek Immediate Medical Attention
While sudden diarrhea after meals is often caused by manageable functional disorders, it can sometimes indicate a severe, life-threatening condition requiring emergency care. If you experience any of the following warning signs, stop assuming it is a simple food intolerance and seek immediate medical evaluation.
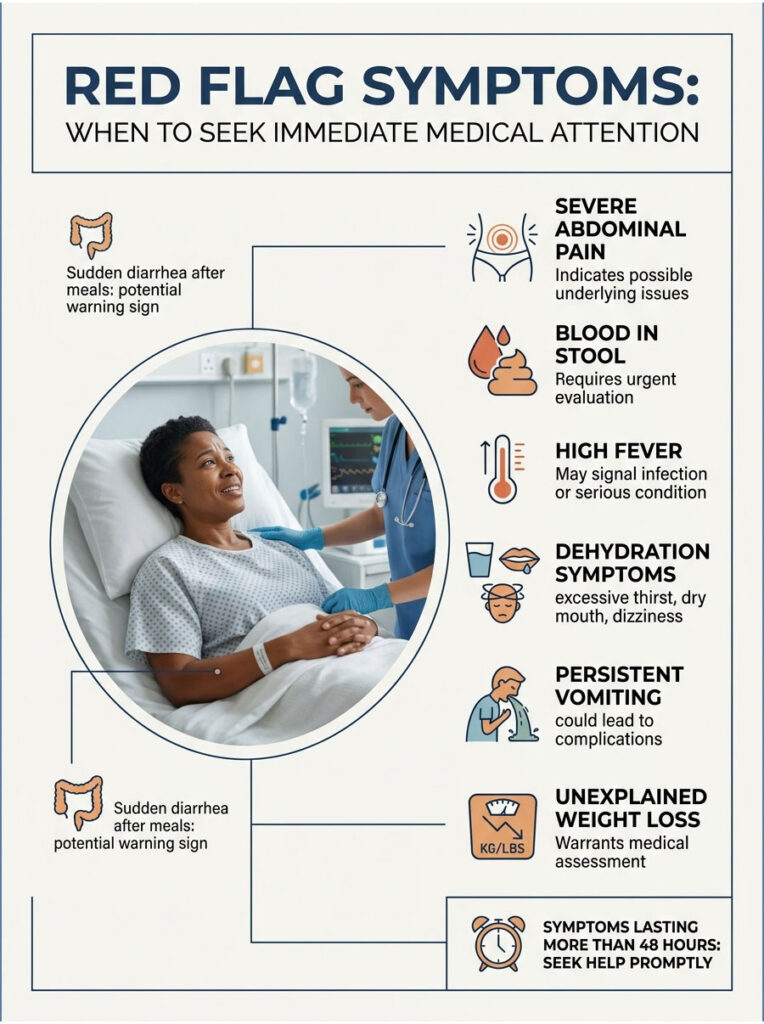
- Unintentional weight loss: Dropping significant weight without trying suggests your body is failing to absorb nutrients, or it may indicate a severe inflammatory disease or malignancy.
- Nocturnal diarrhea: Waking up from sleep to pass watery stool is a major red flag. Functional disorders like IBS-D generally calm down during sleep. Nighttime symptoms point to secretory diarrhea, hidden infections, or inflammatory bowel disease.
- Blood in stool: Visible bright red blood in the toilet, or black tarry stools, strongly indicate internal bleeding. This requires urgent endoscopy to locate and stop the bleed.
- Severe dehydration: Symptoms like extreme thirst, dizziness upon standing, dark urine, or a racing heart indicate dangerous electrolyte imbalances. Rapid fluid loss can cause acute kidney injury if untreated.
- Fever and chills: A high fever alongside bowel urgency suggests an active infection, possibly from a severe pathogen like Salmonella, C. diff, or Campylobacter that requires specific antibiotic therapy.
Key Takeaways and Final Thoughts
Living with chronic digestive urgency is physically exhausting and emotionally draining. It shrinks your world and turns basic social interactions into a minefield. But as we have explored throughout this guide, explosive diarrhea after eating is a solvable mechanical or biochemical issue. It is not a lifelong sentence you simply have to accept.
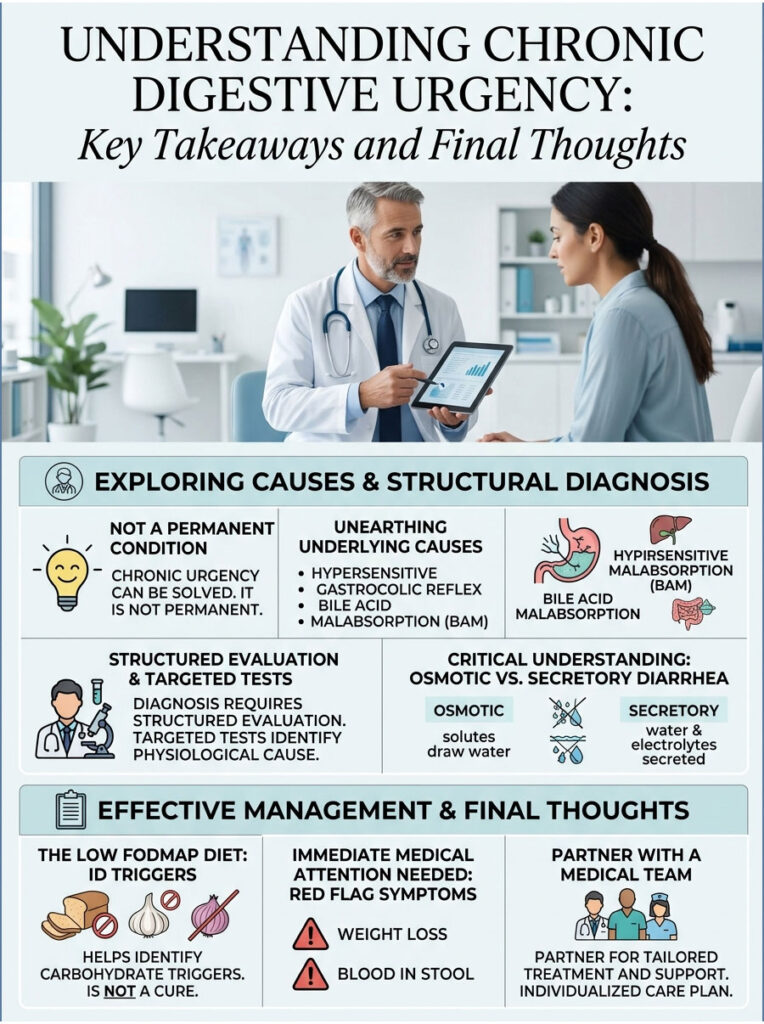
Whether your symptoms are driven by a hypersensitive gastrocolic reflex, Bile Acid Malabsorption, Dumping Syndrome, or specific carbohydrate intolerances, there is a clear physiological explanation for your distress.
The key to lasting relief is moving away from generic internet advice and seeking a proper, structured gastroenterological evaluation. Through targeted breath tests, specific stool analyses, and empirical medication trials, your doctor can pinpoint the exact failure in your digestive cascade.
With the right diagnosis and a dedicated medical team, you can stop the cycle of sudden bowel urgency and finally reclaim full control over your digestive health and daily life.
Frequently Asked Questions
Why do I experience explosive diarrhea within minutes of finishing a meal?
This rapid onset is typically caused by an exaggerated gastrocolic reflex. In a healthy digestive system, this reflex sends mild hormonal and neural signals to the colon to make room for new food. However, in patients with visceral hypersensitivity—often seen in IBS-D—the body overreacts, triggering violent colonic contractions that force out watery stool before the intestines can absorb excess fluid.
Is there a connection between gallbladder removal and sudden postprandial diarrhea?
Yes, approximately 20% of cholecystectomy patients develop Bile Acid Malabsorption (BAM). Without a gallbladder to store bile, these digestive acids drip constantly into the small intestine, eventually overwhelming the terminal ileum’s ability to reabsorb them. When these caustic acids enter the colon, they act as a potent stimulant laxative, causing immediate, urgent, and often yellow-colored diarrhea.
What is Dumping Syndrome, and could it be causing my symptoms?
Dumping Syndrome occurs when the stomach empties its contents into the small intestine too quickly, a condition known as rapid gastric emptying. This is common after bariatric surgery. The undigested food is ‘hyperosmolar,’ meaning it pulls massive amounts of water from your bloodstream into your gut. This leads to a rapid fluid shift causing bloating, cramping, and explosive osmotic diarrhea, often accompanied by dizziness or a racing heart.
Why does greasy or fatty food specifically trigger urgent bowel movements?
This is often a hallmark of either Bile Acid Malabsorption (BAM) or Exocrine Pancreatic Insufficiency (EPI). If your pancreas doesn’t produce enough lipase enzymes, or if your bile flow is dysfunctional, your body cannot break down fats. These undigested lipids travel through the tract, irritating the mucosal lining and accelerating transit time, which results in oily, foul-smelling stools called steatorrhea.
Can Small Intestinal Bacterial Overgrowth (SIBO) cause diarrhea immediately after eating?
Yes. When colonic bacteria migrate into the small intestine, they ferment carbohydrates prematurely. This fermentation produces rapid gas expansion (hydrogen or methane) within 15 to 60 minutes of eating. The resulting pressure on the intestinal walls can trigger a ‘cleansing’ response, leading to severe bloating followed by an urgent need to use the restroom.
What is the difference between osmotic and secretory diarrhea after meals?
Osmotic diarrhea occurs when unabsorbed solutes, like lactose or sugar alcohols, draw water into the bowel; it typically stops when you fast. Secretory diarrhea happens when the intestinal wall actively pumps electrolytes and water into the gut, often due to bile acids or toxins. Secretory diarrhea is generally more severe and can occur even if you haven’t eaten recently or are trying to sleep.
How do sugar-free foods and diet sodas contribute to bowel urgency?
Many diet products contain sugar alcohols like sorbitol, xylitol, or erythritol. These polyols are poorly absorbed by the human gut and act as osmotic agents. They travel to the colon intact, drawing in water and providing a feast for bacteria, which leads to rapid fermentation, gas, and explosive osmotic diarrhea shortly after consumption.
Why does my stool float and look oily after I eat certain foods?
Floating, oily, and exceptionally foul-smelling stool is known as steatorrhea, a clinical sign of fat malabsorption. This frequently points to Exocrine Pancreatic Insufficiency (EPI), where the pancreas fails to secrete enough digestive enzymes. It can also be seen in severe Celiac disease or cases where the ‘enterohepatic circulation’ of bile is disrupted.
Could my post-meal diarrhea actually be a histamine intolerance?
It is possible. If you lack the Diamine Oxidase (DAO) enzyme, eating high-histamine foods like aged cheese, red wine, or cured meats can cause histamine to bind to receptors in your gut. This triggers immediate fluid secretion and smooth muscle contractions, often resulting in diarrhea accompanied by systemic symptoms like skin flushing or headaches.
How do gastroenterologists definitively diagnose the cause of postprandial urgency?
We utilize a structured diagnostic workup including Hydrogen Breath Testing for SIBO, Fecal Elastase-1 tests for pancreatic function, and blood panels for Celiac disease. In the US, because SeHCAT scans aren’t widely available, we often use an empirical trial of bile acid sequestrants to confirm Bile Acid Malabsorption if symptoms improve within a few days.
Will a Low FODMAP diet stop my explosive diarrhea?
The Low FODMAP diet is an effective diagnostic tool for identifying specific carbohydrate triggers that cause osmotic shifts and fermentation. While it provides relief for about 70% of patients with functional gut disorders, it is not a ‘cure.’ It is a three-phase process designed to help you identify your personal threshold for fermentable sugars like fructose and lactose.
What are the ‘red flag’ symptoms that require immediate medical attention?
As a gastroenterologist, I advise immediate evaluation if you experience ‘alarm features’ such as unintentional weight loss, nocturnal diarrhea (waking up at night to go), visible blood in the stool (hematochezia), fever, or signs of severe dehydration like dizziness and a racing heart. These symptoms may indicate inflammatory bowel disease, infection, or malignancy.
Disclaimer
This article is for informational and educational purposes only and does not constitute formal medical advice, diagnosis, or treatment. The content is authored by a medical professional but does not establish a doctor-patient relationship. Always seek the advice of a board-certified gastroenterologist or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
References
- American College of Gastroenterology (ACG) – gi.org – Clinical guidelines on the management of Irritable Bowel Syndrome and functional chronic diarrhea in adults.
- American Gastroenterological Association (AGA) – gastro.org – Clinical practice updates on the diagnosis and management of Bile Acid Malabsorption and SIBO.
- Monash University – monashfodmap.com – Peer-reviewed research and clinical data regarding the Low FODMAP diet for functional gastrointestinal disorders.
- National Institutes of Health (NIH) – niddk.nih.gov – Comprehensive pathophysiology of the gastrocolic reflex and enterohepatic circulation.
- Mayo Clinic Proceedings – mayoclinicproceedings.org – Clinical review of Exocrine Pancreatic Insufficiency (EPI) recognition and enzyme replacement therapy.
- Journal of Clinical Medicine – mdpi.com/journal/jcm – Research study on the prevalence of Microscopic Colitis in patients with chronic watery diarrhea.






