After 15 years of practicing gastroenterology, one question comes up in my clinic more than almost any other: what exactly does stomach acid do, and why does it matter so much? Most patients walk in wanting to get rid of their acid entirely, usually because of persistent heartburn. But here is the thing – your stomach acid is not the enemy. It is one of the most important fluids your body produces.
Table of Contents
This guide breaks down how stomach acid works in plain, practical terms. We will cover how it digests protein, kills harmful bacteria, and helps your body absorb essential nutrients like iron, calcium, and Vitamin B12. We will also look at what happens when acid levels are too high or too low, and what you can do about it.
Whether you are dealing with chronic reflux, unexplained bloating, or just want to understand your gut better, this article gives you the expert-backed knowledge to make informed decisions about your digestive health.
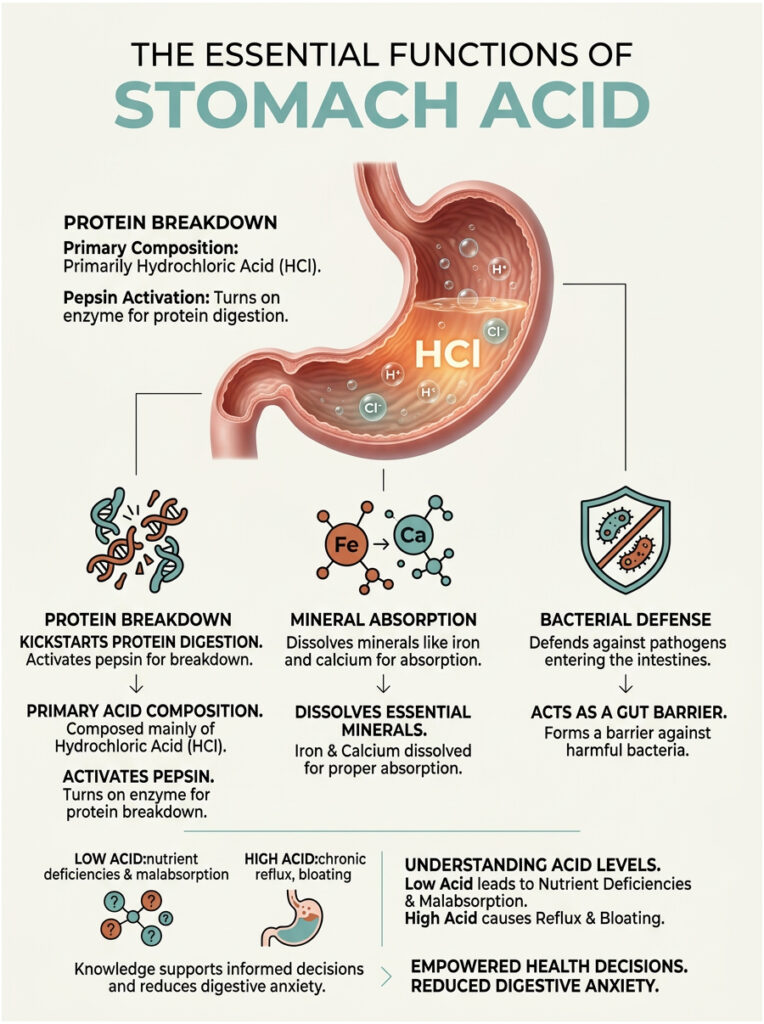
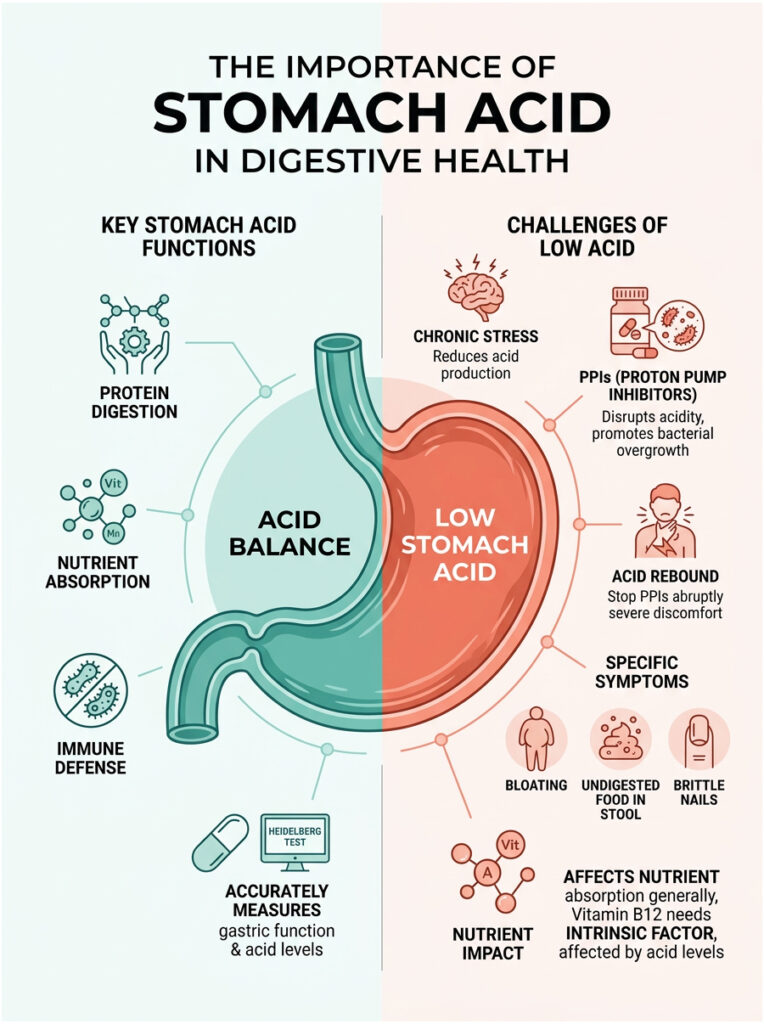
Quick Answer: Stomach acid, primarily made of hydrochloric acid (HCl), plays three essential roles. It kickstarts protein digestion by activating the enzyme pepsin. It dissolves minerals like iron and calcium so your body can absorb them. And it acts as a biological barrier, killing harmful bacteria before they reach your intestines. Without enough stomach acid, you risk malabsorption, nutrient deficiencies, and conditions like Small Intestinal Bacterial Overgrowth (SIBO).
Key Statistics on Gastric Health
- Daily Volume: Your stomach produces roughly 1.5 to 2 liters of gastric juice per day (National Institutes of Health, 2022).
- Resting pH: A healthy fasting stomach maintains a pH between 1.5 and 3.5, making it extremely acidic.
- Low Acid Prevalence: Up to 30% of adults over 60 experience hypochlorhydria (low stomach acid).
- SIBO Connection: Between 50% and 70% of patients with chronic low acidity develop SIBO (American College of Gastroenterology, 2021).
- PPI Usage: Over 15 million Americans are prescribed proton pump inhibitors every year.
- Gut Immunity: About 80% of your immune system resides in the gut, relying heavily on the stomach’s initial sterilizing function.
How Your Stomach Produces Acid
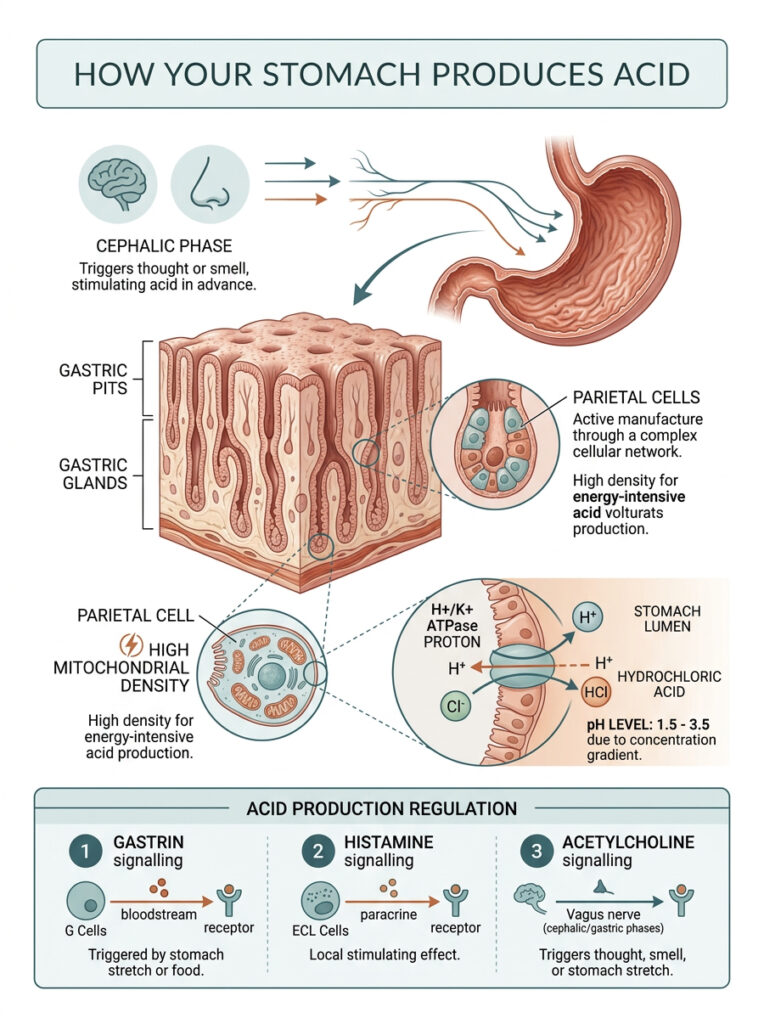
Your stomach does not just sit around filled with a static pool of acid. It actively manufactures hydrochloric acid on demand through a remarkably complex cellular network. The inner lining of your stomach, called the gastric mucosa, is covered in millions of tiny indentations known as gastric pits. These pits house the glands responsible for secreting your digestive fluids.
Parietal Cells: The Acid-Producing Factories
Deep within the gastric glands sit specialized cells called parietal cells. These are the microscopic factories that actually produce your stomach acid. They are packed with mitochondria – in fact, parietal cells have among the highest mitochondrial density of any cell in your body. That is because creating such a powerful acid requires enormous amounts of energy.
When you eat, these cells spring into action. They pump hydrogen and chloride ions into the stomach cavity, where they combine to form hydrochloric acid. The same parietal cells also produce a protein called Intrinsic Factor, a glycoprotein that is absolutely essential for absorbing Vitamin B12. Without it, B12 deficiency is inevitable.
The Proton Pump: How Acid Gets So Strong
The actual mechanism behind acid production is an enzyme called the H+/K+ ATPase proton pump. This molecular engine sits on the surface of each parietal cell. Its job is to push hydrogen ions out of the cell and into the stomach, exchanging them for potassium ions.
What makes this remarkable is the sheer scale of the concentration gradient involved. The hydrogen ion concentration outside the cell is roughly one million times higher than inside. This massive gradient is what drops the pH to a corrosive 1.5 to 3.5.
This is also the exact mechanism that acid-blocking medications target. Proton pump inhibitors (PPIs) chemically disable this enzyme, which stops acid production entirely. While this provides rapid heartburn relief, it also shuts down your primary digestive and defensive functions.
Hormonal Control: Gastrin, Histamine, and Acetylcholine
Acid production is not random. It is tightly regulated by three chemical messengers: gastrin, histamine, and acetylcholine. Together, they tell your parietal cells exactly when to ramp up and when to slow down.
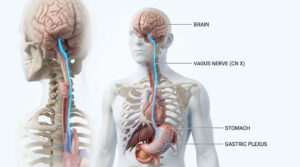
Gastrin is released by specialized G-cells when protein enters your stomach. Histamine amplifies the signal locally, further stimulating nearby acid-producing cells. Acetylcholine, a neurotransmitter released by the vagus nerve, connects your brain directly to your digestive tract.
Expert Insight: Simply smelling or thinking about food triggers acetylcholine release from your brain. This primes your stomach for digestion before food even reaches your mouth. Doctors call this the cephalic phase of digestion.
The Three Core Functions of Stomach Acid
Many people assume the stomach is where most nutrient absorption happens. In reality, it functions primarily as a preparation chamber, getting food ready for the small intestine. Stomach acid serves three major purposes: breaking down protein, preparing minerals for absorption, and killing harmful bacteria.
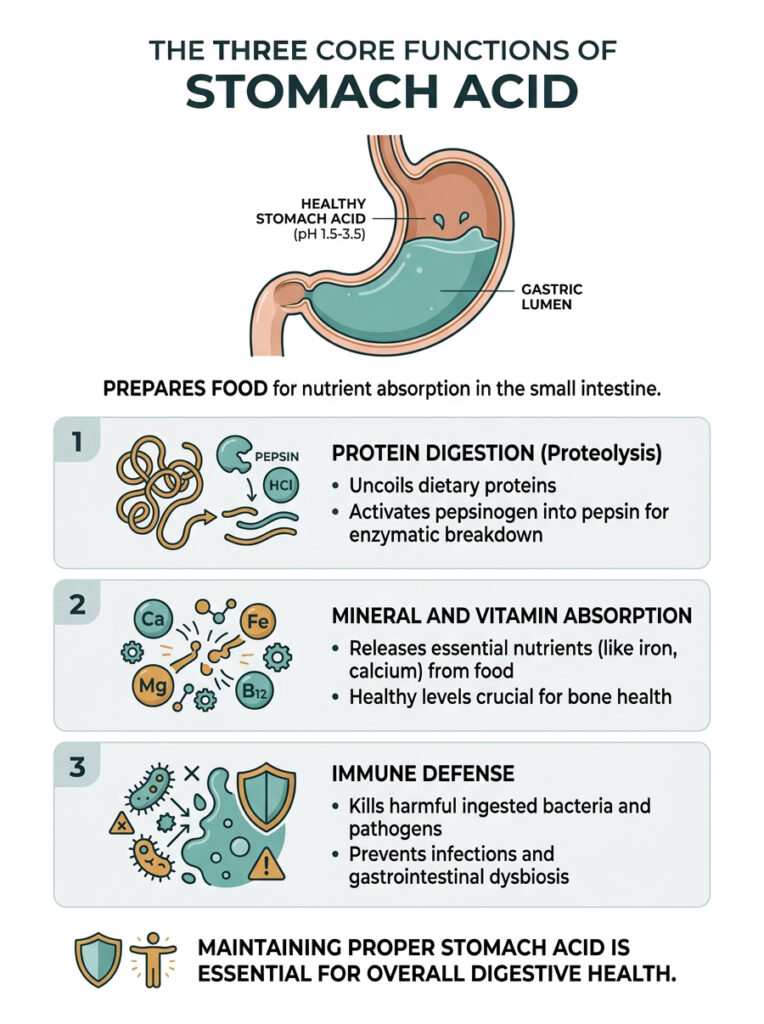
1. Protein Digestion (Proteolysis)
When you eat protein, whether from chicken, eggs, beans, or tofu, it arrives in your stomach as long, tightly folded molecular chains. The highly acidic environment causes these chains to uncoil and unfold, exposing them to enzymatic breakdown.
Your stomach also secretes an inactive enzyme called pepsinogen. In a neutral environment, pepsinogen does nothing. But when it meets hydrochloric acid, it transforms into pepsin, a powerful enzyme that acts like molecular scissors. Pepsin snips uncoiled proteins into smaller fragments called peptides, which then move to the small intestine for further digestion.
If your stomach acid is too low, this conversion never fully happens. Undigested proteins pass into the intestines, often causing bloating, discomfort, and poor nutrient absorption.
2. Mineral and Vitamin Absorption
Many essential vitamins and minerals are locked inside the structural matrix of your food. Stomach acid is required to separate them from their carrier proteins so they can be absorbed further down the digestive tract.
Non-heme iron, the type found in plant foods and supplements, is a good example. Your gastric acid converts it from an unusable ferric form into a highly absorbable ferrous form. Without this conversion, iron absorption drops dramatically.
Calcium absorption follows a similar pattern. Patients on long-term acid-suppressing medications frequently develop poor calcium absorption, which increases the risk of osteoporosis and bone fractures over time. Maintaining healthy acid levels is directly tied to skeletal health.
3. Immune Defense: Killing Harmful Bacteria
Every time you eat or drink, you swallow thousands of microscopic organisms. Your stomach acts as a powerful biological filter. The intense acidity destroys most known pathogens by denaturing the proteins and enzymes within their cell walls, essentially dissolving them from the outside in.
When acid levels drop, this filter stops working properly. Bacteria that would normally be killed survive the journey and reach the small intestine. This opens the door to gastrointestinal infections, food poisoning, and long-term gut dysbiosis. The stomach’s role as an immune defender is hard to overstate.
The Gastric Mucosal Barrier: Why Your Stomach Does Not Digest Itself
If stomach acid can dissolve meat and kill bacteria, why does it not eat through the stomach lining? This is one of the most common questions patients ask, and the answer is genuinely fascinating.
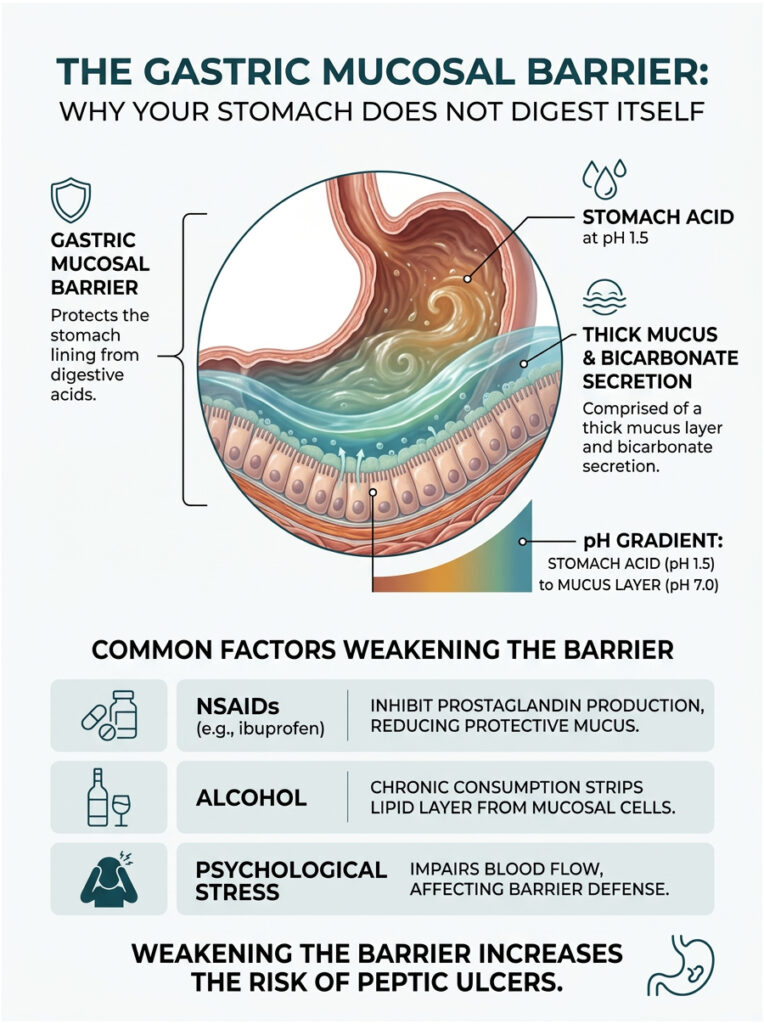
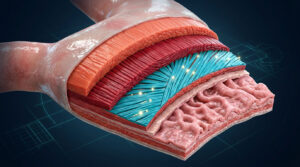
Your stomach is protected by a specialized defense system called the gastric mucosal barrier. This multilayered shield lines the entire inner surface of the organ, allowing it to safely contain an extremely corrosive fluid.
Bicarbonate and the Neutral Zone
The surface cells of your stomach lining secrete a thick, viscous mucus that coats the vulnerable tissue beneath. But mucus alone would not be enough. These cells also continuously release bicarbonate directly into the mucus layer.
This creates a remarkable chemical gradient. While the center of the stomach maintains a harsh pH of about 1.5, the layer right against the stomach wall sits at a near-neutral pH of approximately 7.0. The acid never actually contacts your living cells. Digestion stays safely confined to the center of the organ.
What Damages the Barrier
Despite its sophistication, this barrier is surprisingly fragile. Several common factors can weaken it quickly. The most frequent culprit I see in clinical practice is regular use of non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or aspirin.
These medications block prostaglandin production. Prostaglandins are chemical messengers that signal your body to produce protective mucus and bicarbonate. Without them, the barrier thins rapidly. I regularly treat patients who develop severe gastritis after heavy, unbuffered painkiller use.
Chronic alcohol consumption can also strip the protective lipid layer from mucosal cells. Severe psychological stress impairs blood flow to the stomach lining, further reducing its ability to maintain defenses. Both factors significantly increase the risk of painful peptic ulcers.
When Stomach Acid Levels Go Wrong
Healthy digestion depends on a precise acid balance. When production is disrupted, whether too high or too low, health problems follow quickly. In gastroenterology, we classify these imbalances into two main conditions: hyperchlorhydria (excess acid) and hypochlorhydria (low acid).
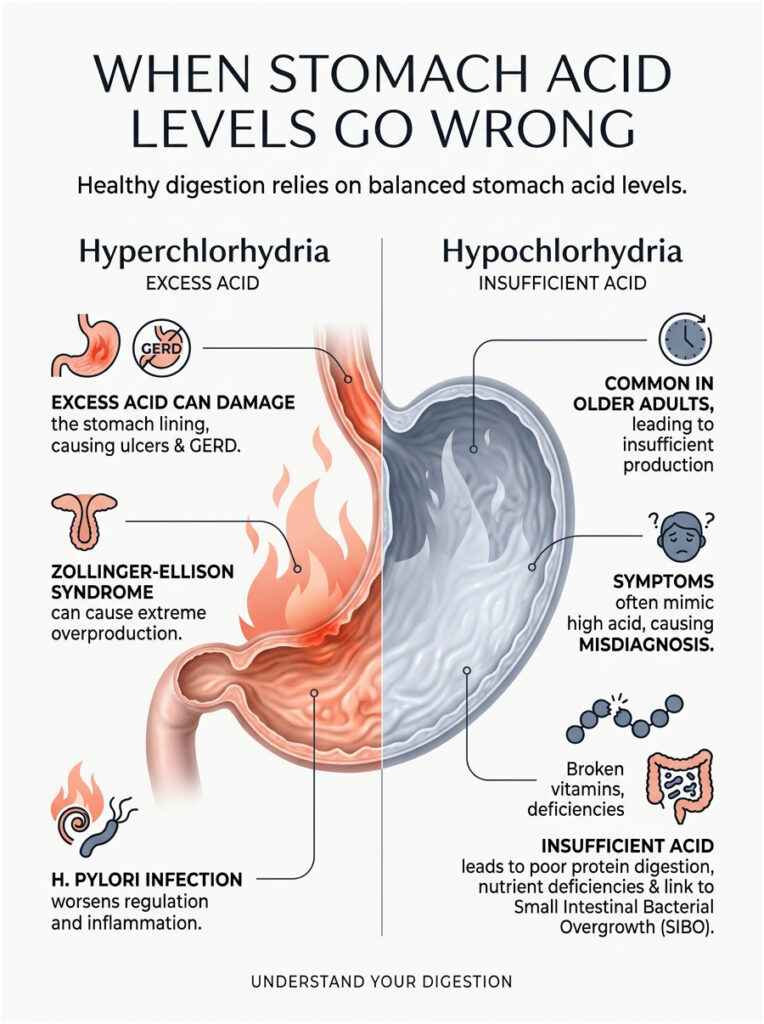
Hyperchlorhydria: Excess Acid Production
Hyperchlorhydria means the stomach produces more acid than the mucosal barrier can handle. While it is less common than most people assume, it is a serious condition. The excess fluid overwhelms the protective lining, causing tissue damage.
This overproduction is a primary driver of peptic ulcer disease and severe gastroesophageal reflux disease (GERD). In rare cases, a condition called Zollinger-Ellison Syndrome causes tumors in the pancreas to release massive amounts of gastrin, forcing dangerously high acid output.
H. pylori infection can further complicate the picture. This bacterium burrows into the mucosal barrier, creating chronic localized inflammation that disrupts normal acid regulation.
Hypochlorhydria: The Often-Missed Low Acid Problem
Hypochlorhydria, or insufficient acid production, is far more common than most people realize, especially in older adults. As we age, parietal cells naturally become less efficient. Achlorhydria, the complete absence of acid production, is the most extreme form.
The tricky part is that low acid symptoms often mimic high acid symptoms. Patients typically feel extreme fullness after meals, chronic bloating, frequent belching, and sometimes find undigested food in their stool. Because these symptoms look so much like GERD, many patients self-treat with antacids, which only makes the underlying problem worse.
Without enough acid, protein digestion stalls, mineral absorption drops, and bacterial defenses fail. Over time, this leads to cascading nutrient deficiencies that affect the entire body.
The Link Between Low Acid and SIBO
When the stomach’s sterilizing function fails, bacteria that should have been killed pass safely into the small intestine. The small intestine is meant to be a relatively clean environment. When oral or colonic bacteria colonize it, the result is Small Intestinal Bacterial Overgrowth (SIBO).
SIBO causes severe daily bloating, trapped gas, and painful abdominal cramping. Clinical data shows a clear connection between long-term acid-suppressing medications and SIBO development. The bacteria ferment food prematurely, producing large amounts of internal gas. Restoring natural acid levels is usually the first step in effective SIBO treatment.
Comparison: Hyperchlorhydria vs. Hypochlorhydria
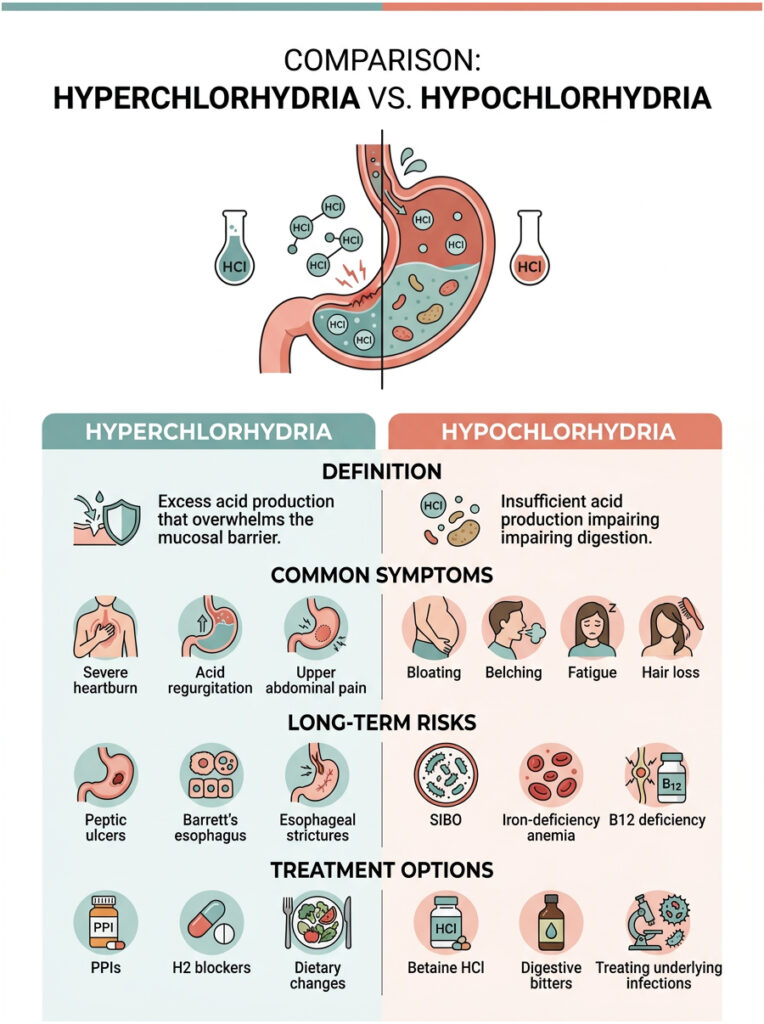
| Condition | Definition | Common Symptoms | Long-Term Risks | Treatment |
| Hyperchlorhydria | Excess acid production that overwhelms the mucosal barrier. | Severe heartburn, acid regurgitation, upper abdominal pain. | Peptic ulcers, Barrett’s esophagus, esophageal strictures. | PPIs, H2 blockers, dietary changes. |
| Hypochlorhydria | Insufficient acid production impairing digestion. | Bloating, belching, fatigue, hair loss. | SIBO, iron-deficiency anemia, B12 deficiency. | Betaine HCl, digestive bitters, treating underlying infections. |
How to Test Your Stomach Acid Levels
If you suspect low acid production, proper medical testing is essential. Guessing your internal pH can lead to treatments that make things worse. In modern gastroenterology, we rely on specific, validated diagnostic tools.
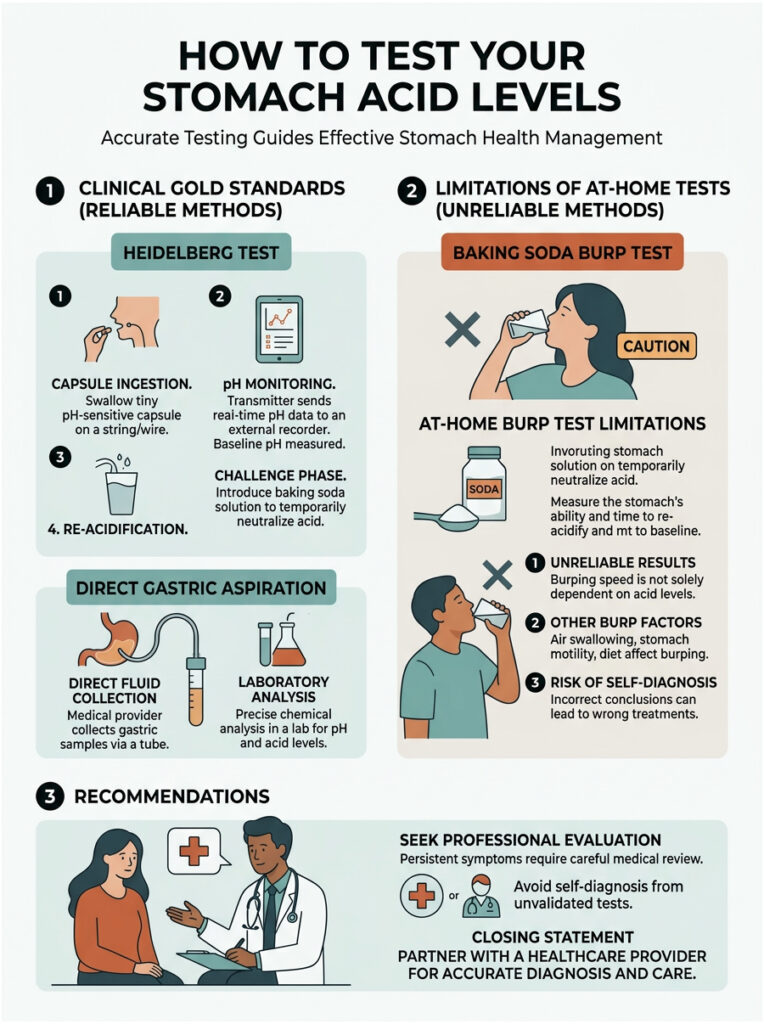
Clinical Gold Standards
The most accurate test available is the Heidelberg Test. During this procedure, you swallow a small capsule equipped with a micro-radio transmitter. This capsule measures the exact pH inside your stomach in real time and sends the data to a computer.
During the test, we challenge your system by having you drink a baking soda solution to neutralize the stomach environment. We then measure how long it takes for your stomach to re-acidify. This timing tells us precisely how well your parietal cells and proton pumps are functioning.
Another reliable method is direct gastric aspiration during an endoscopy. A small tube is passed down the esophagus to extract stomach fluid, which is then analyzed in a laboratory for acid concentration.
Why At-Home Tests Fall Short
Many patients try the popular “baking soda burp test” they found online. The idea is that drinking baking soda mixed with water should cause a burp within three minutes if acid levels are normal. If you do not burp, supposedly you have low acid.
In reality, this test has no clinical validity. How quickly you burp depends on swallowed air, esophageal sphincter tone, and the volume of water used – not actual acid levels. Patients report wildly inconsistent results, and relying on them can lead to incorrect self-diagnosis and potentially dangerous supplementation. For persistent symptoms, always seek a professional evaluation.
Practical Tips for Healthy Stomach Acid Levels
Whether you deal with occasional reflux or suspect low acid production, practical strategies can support your digestive health. Here are evidence-based approaches that I recommend to my patients.
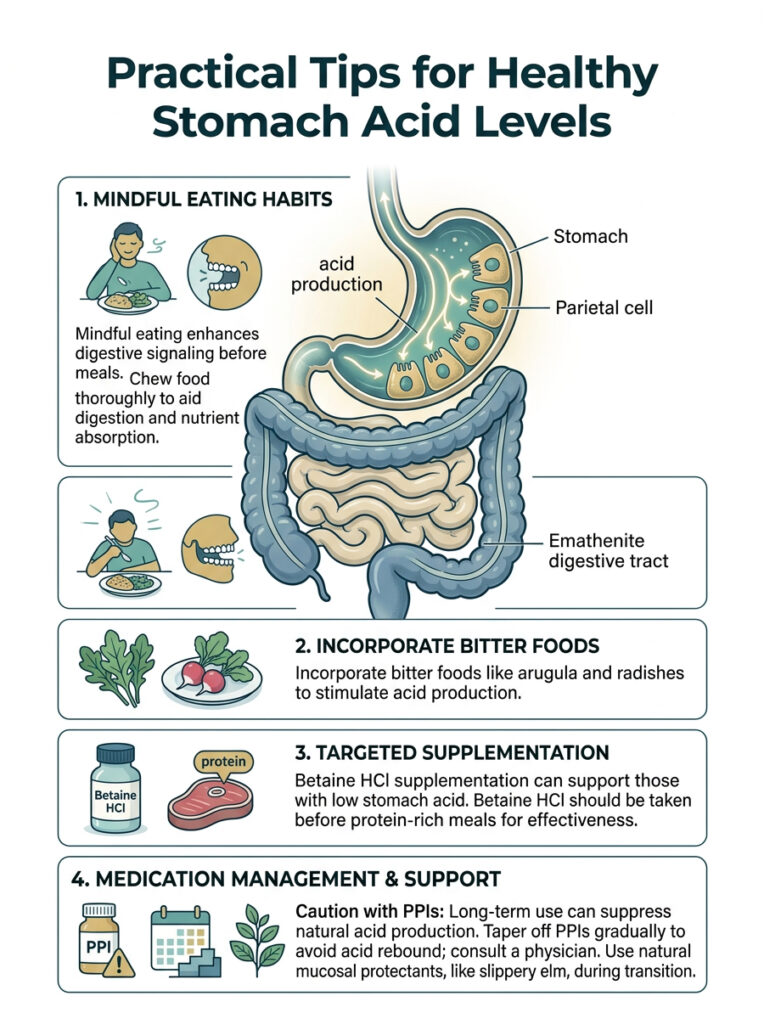
Dietary Changes That Support Acid Production
Digestion actually begins in the brain. Practicing mindful eating, sitting down in a calm environment, and taking a few deep breaths before meals, sends neurological signals through the vagus nerve to your parietal cells. This primes them to produce acid before food even arrives.
Chewing food thoroughly until it is nearly liquid reduces the workload on your stomach and allows acid to penetrate food particles more effectively. This is especially important for absorbing non-heme iron from plant foods.
Eating naturally bitter foods before a meal can also stimulate acid secretion. Fresh arugula, dandelion greens, and radishes are simple additions that help if you have sluggish digestion.
Supplements: Betaine HCl and Digestive Bitters
For patients diagnosed with hypochlorhydria, supplementation is often necessary. Betaine HCl delivers a supplemental form of hydrochloric acid directly to the stomach. It is usually combined with pepsin to closely replicate natural digestive juices.
Taken before a protein-heavy meal, Betaine HCl can restore the acidic environment needed for proper protein breakdown. It reduces post-meal bloating and helps prevent SIBO by sterilizing incoming food.
However, this supplement must be used under medical supervision. If you have an active ulcer or compromised mucosal barrier, adding more acid can cause severe pain. Liquid digestive bitters are a gentler alternative that stimulates your body’s own acid production naturally.
Managing Proton Pump Inhibitors (PPIs) Safely
PPIs are effective medications for healing ulcers and severe reflux. But long-term daily use completely suppresses natural acid production, leading to downstream consequences including nutrient malabsorption and altered gut bacteria.
If you have been taking a daily PPI for months or years, do not stop abruptly. Sudden discontinuation causes a painful phenomenon called acid rebound, where the body drastically overproduces acid to compensate for prolonged suppression.
Tapering off requires a structured plan guided by a physician. We typically reduce the dose gradually over several weeks or months, often bridging the transition with milder H2 receptor blockers or natural mucosal protectants like slippery elm.
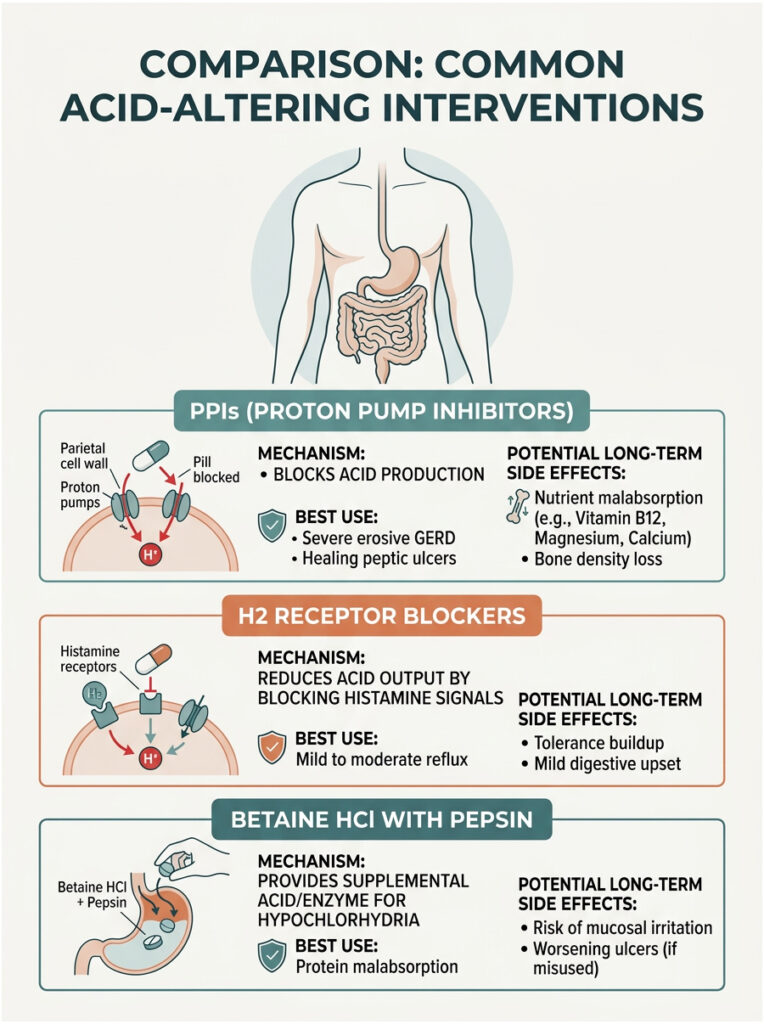
Comparison: Common Acid-Altering Interventions
| Intervention | Mechanism | Best Use | Potential Long-Term Side Effects |
| Proton Pump Inhibitors (PPIs) | Blocks the H+/K+ ATPase enzyme, stopping acid production. | Severe erosive GERD, healing active peptic ulcers. | Nutrient malabsorption, altered gut microbiome, bone density loss. |
| H2 Receptor Blockers | Blocks histamine signals to parietal cells, reducing acid output. | Mild to moderate reflux, occasional heartburn. | Tolerance buildup (tachyphylaxis), mild digestive upset. |
| Betaine HCl with Pepsin | Delivers supplemental acid and enzymes directly to the stomach. | Diagnosed hypochlorhydria, protein malabsorption. | Mucosal irritation, ulcer worsening if used improperly. |
Recent Research: The Gut-Brain Connection and Microbiome Impact
Gastroenterology is constantly evolving, and recent research has deepened our understanding of how stomach acid affects the entire body. Two areas stand out as particularly significant.
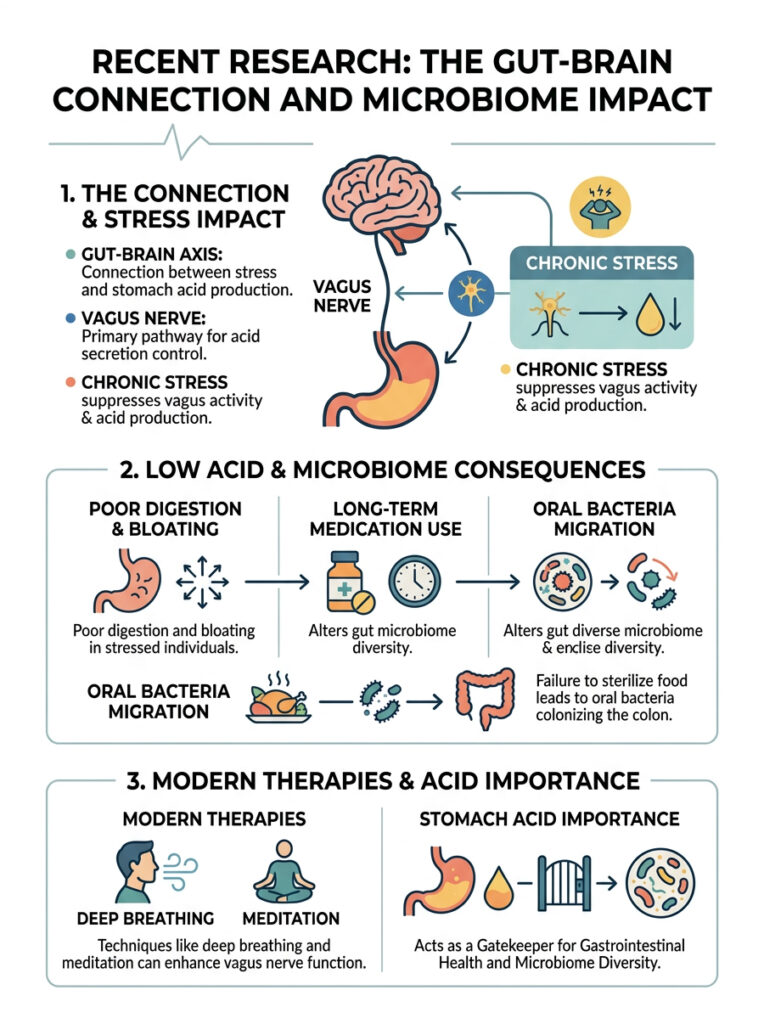
The Gut-Brain Axis and Vagus Nerve
Peer-reviewed studies from major medical journals confirm that chronic psychological stress directly reduces stomach acid production. When you are under constant stress, your body shifts into a sympathetic “fight or flight” state. This suppresses vagus nerve activity, which is the primary neural pathway controlling acid secretion.
When the vagus nerve is chronically suppressed, it stops sending acetylcholine signals to the stomach. Acid production drops, explaining why highly stressed patients often report poor digestion and persistent bloating.
Modern therapies aimed at stimulating the vagus nerve, including deep diaphragmatic breathing, meditation, and cold exposure, show measurable improvements in gastric function. The connection between the brain and the gut is physical and well documented.
Acid Suppression and the Intestinal Microbiome
Emerging research shows that long-term use of acid-suppressing medications significantly alters the microbial diversity of the large intestine. When the stomach fails to sterilize incoming food, oral bacteria migrate downstream and colonize the colon.
Studies from the National Institutes of Health found that patients on long-term PPIs have notably higher levels of oral bacterial strains living in their colonic microbiome. This unnatural shift is linked to increased intestinal inflammation.
This research reinforces the idea that stomach acid is not just a digestive tool. It is the primary gatekeeper for your entire gastrointestinal ecosystem. Protecting natural acid levels physically protects the diversity and health of your gut microbiome.
Final Thoughts
Your stomach acid is far more than a simple digestive fluid. It is a powerful protein-digesting catalyst, an aggressive immune barrier, and an essential nutrient extractor. Without it functioning properly, your body cannot operate at its best.
We have covered how excess acid damages tissue and requires careful medical management. We have also explored how low acid silently leads to nutrient deficiencies, SIBO, and systemic health problems. Recognizing the true symptoms of both conditions is the critical first step toward getting proper treatment.
If you are dealing with chronic digestive issues, avoid prolonged self-medication with over-the-counter antacids. Seek a professional gastroenterological evaluation. Understanding the role of acid in the stomach gives you the foundation to take real control of your gut health, starting today.
Frequently Asked Questions
What are the three primary roles of hydrochloric acid in the digestive process?
As a gastroenterologist, I categorize the functions of gastric acid into three essential pillars: initiating proteolysis by activating the enzyme pepsin for protein breakdown, facilitating the ionization and absorption of critical micronutrients like iron and calcium, and serving as a potent biological filter that sterilizes ingested pathogens to prevent intestinal dysbiosis.
How do parietal cells manage to produce such high levels of acidity without dying?
Parietal cells are biological marvels equipped with a high density of mitochondria to power the H+/K+ ATPase proton pump. This enzyme actively exchanges potassium for hydrogen ions against a massive concentration gradient. The cells remain protected because the corrosive fluid is only fully formed once the ions are secreted into the gastric pits and move toward the stomach cavity.
What is the clinical significance of Intrinsic Factor in gastric health?
Intrinsic Factor is a specialized glycoprotein secreted by the same parietal cells that produce stomach acid. It is absolutely mandatory for the terminal ileum to absorb Vitamin B12. In clinical practice, we often find that patients with suppressed acid production or damaged gastric mucosa also suffer from severe B12 deficiencies because Intrinsic Factor production is concurrently compromised.
Why doesn’t the stomach’s corrosive fluid dissolve the organ itself?
The stomach is protected by the gastric mucosal barrier, a thick layer of viscous mucus. Crucially, the underlying epithelial cells secrete bicarbonate into this mucus, creating a localized neutral pH zone of approximately 7.0. This chemical gradient prevents the highly acidic gastric juice (pH 1.5–3.5) from ever making physical contact with the living stomach lining.
What are the hallmark symptoms of hypochlorhydria (low stomach acid)?
In my clinical experience, hypochlorhydria often presents as severe postprandial fullness, chronic bloating, and frequent belching shortly after meals. Patients may also notice visible undigested food in their stool or suffer from brittle nails and hair loss, which are secondary signs of the chronic malabsorption caused by insufficient gastric acidity.
How does chronic stress lead to digestive issues like bloating and indigestion?
The gut-brain axis plays a decisive role here. Chronic stress shifts the body into a sympathetic state, which downregulates the vagus nerve. This reduction in vagal tone inhibits the release of acetylcholine, the neurotransmitter responsible for signaling parietal cells to produce acid. Without this signal, acid levels drop, leading to sluggish digestion and gas-producing fermentation.
Can long-term use of Proton Pump Inhibitors (PPIs) lead to SIBO?
Yes, there is a strong clinical correlation. By disabling the proton pumps, PPIs significantly raise the stomach’s pH, neutralizing the biological filter. This allows oral and environmental bacteria to survive the passage through the stomach and colonize the small intestine, frequently resulting in Small Intestinal Bacterial Overgrowth (SIBO).
Is the ‘baking soda burp test’ an accurate way to diagnose acid levels?
No, the baking soda test lacks clinical validity and is not a substitute for professional diagnostics. The timing of a burp is influenced by factors like esophageal sphincter tone and how much air was swallowed during the test. For an accurate assessment, I recommend gold-standard medical testing such as the Heidelberg Test or gastric aspiration.
What is the Heidelberg Test and how does it measure gastric function?
The Heidelberg Test is a sophisticated diagnostic procedure where a patient swallows a small electronic capsule containing a pH sensor and radio transmitter. This allows us to monitor the stomach’s pH in real-time and observe how quickly the parietal cells can re-acidify the environment after being challenged with a neutralizing alkaline solution.
How does stomach acid affect the absorption of plant-based (non-heme) iron?
Non-heme iron found in plants is naturally in a ferric state, which the body cannot easily absorb. A highly acidic gastric environment is required to chemically reduce this into a ferrous state. Patients with low acidity or those on acid-suppressants often develop iron-deficiency anemia because this essential chemical conversion is impaired.
What are the risks of hyperchlorhydria if left untreated?
Hyperchlorhydria, or the overproduction of gastric acid, can overwhelm the protective mucosal barrier. This leads to the development of peptic ulcers, chronic gastritis, and Gastroesophageal Reflux Disease (GERD). In severe cases, chronic acid exposure can lead to Barrett’s esophagus, a precancerous change in the lining of the esophagus.
What is ‘acid rebound’ and why is it dangerous to stop PPIs abruptly?
Acid rebound occurs when the body, having been suppressed by medication, attempts to compensate by overproducing gastrin. When the medication is suddenly stopped, the parietal cells overreact, creating a massive surge of acid that can cause severe pain and mucosal damage. We always recommend a gradual, physician-guided taper to safely transition off these medications.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. The biological processes and clinical conditions described should be discussed with a board-certified gastroenterologist. Always consult a qualified healthcare professional before starting supplements like Betaine HCl or changing prescribed medications such as Proton Pump Inhibitors.
References
- National Institutes of Health (NIH) – 2022 Gastric Juice Secretion Data – Statistical source for daily gastric juice volume and pH levels.
- American College of Gastroenterology (ACG) – 2021 Clinical Guidelines – Research regarding the link between hypochlorhydria and SIBO development.
- Journal of Clinical Medicine – “The Role of Parietal Cells in Micronutrient Extraction” – Detailed study on the absorption of Iron and B12.
- American Gastroenterological Association (AGA) – The Gut-Brain Axis in Functional Dyspepsia – Insight into how the vagus nerve regulates gastric acid.
- National Library of Medicine – “The Gastric Mucosal Barrier: Mechanisms of Protection” – Research on bicarbonate secretion and mucosal integrity.
- Harvard Health Publishing – “The Dangers of Long-term PPI Use” – Clinical overview of nutrient malabsorption and bone density risks.