
A board-certified endocrinologist explains the proven link between hypothyroidism and chronic head pain, and what you can do about it.
Table of Contents
Every week, patients walk into my clinic with the same story. They have been popping ibuprofen for months, sometimes years, trying to manage a dull, heavy headache that just will not quit. Most of them have already seen a neurologist. Some have had MRIs. Almost none of them suspect that their thyroid could be behind the pain.
So, can underactive thyroid cause headaches? Yes, absolutely. As an endocrinologist, I see this connection on a regular basis. When your thyroid gland fails to produce enough hormone, it throws off your metabolism, stiffens your blood vessels, and starves your brain of the energy it needs. The result is a persistent, bilateral pressure that no amount of over-the-counter painkillers can fix.
In this guide, I will walk you through the exact science behind thyroid-related headaches. You will learn how to tell this type of pain apart from a migraine, what blood tests to request, and how hormone replacement therapy can bring lasting relief. If you have been struggling with unexplained head pain, this article was written for you.
Quick Answer: The Thyroid-Headache Link
An underactive thyroid is a clinically established cause of chronic headaches. Low thyroid hormone levels reduce vascular elasticity in the brain, causing a constant heavy pressure on both sides of the head. This type of pain typically resolves once hormone levels are restored through proper medication.
Key Statistics Worth Knowing
- 30% of patients with hypothyroidism experience chronic daily headaches (Journal of Headache and Pain, 2021).
- Normal TSH range: 0.4 to 4.0 mIU/L according to the American Thyroid Association.
- Up to 70% reduction in headache burden after three months of stable hormone therapy.
- Women are four times more likely than men to develop hypothyroidism and related neurological symptoms.
- 6 to 8 weeks: typical time to reach stable thyroid hormone levels after starting medication.
- Over 60% of thyroid-related headaches are initially misdiagnosed as primary tension headaches.
The Neurological Connection Between Your Thyroid and Your Head
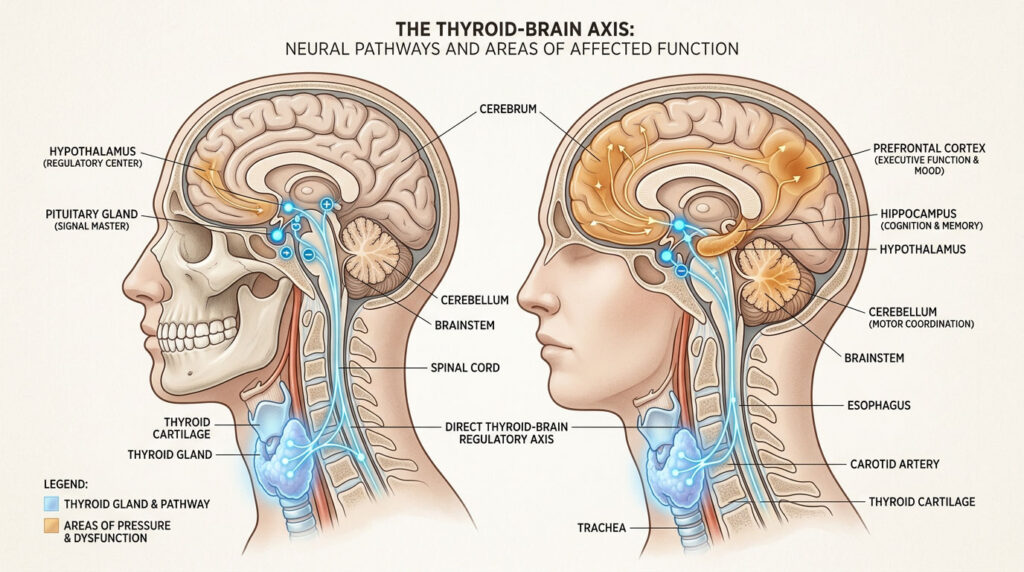
To understand why your head hurts, we need to look at your neck first. Your thyroid is a small, butterfly-shaped gland sitting at the base of your throat. Think of it as the control center for your cellular metabolism. Every organ, every tissue, and especially your brain depends on it to keep things running.
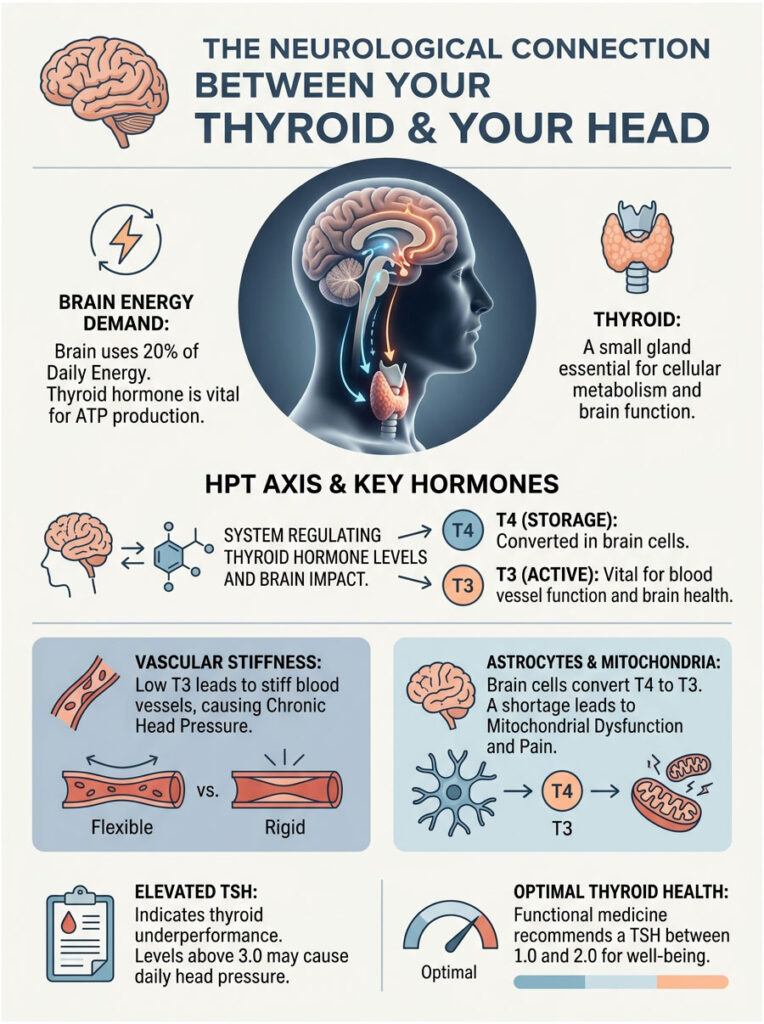
When this gland slows down, your brain is one of the first organs to feel it. The brain consumes roughly 20% of your total energy supply each day. Without enough thyroid hormone, your brain cells cannot generate the adenosine triphosphate (ATP) they need to function properly. That energy deficit shows up as pain.
The system governing this process is called the Hypothalamus-Pituitary-Thyroid (HPT) axis. Your hypothalamus monitors thyroid hormone levels in the blood. When those levels dip, it signals the pituitary gland to release more Thyroid Stimulating Hormone (TSH). TSH then pushes the thyroid to produce more hormones. When the thyroid cannot keep up, the whole system falls out of balance.
The Role of T3 and T4 in Brain Health
Your thyroid produces two key hormones: Thyroxine (T4) and Triiodothyronine (T3). T4 is mostly a storage form. Your body has to convert it into T3, which is the active hormone that actually drives cellular metabolism.
T3 directly regulates the smooth muscle cells lining your blood vessels. When T3 is at healthy levels, your brain’s blood vessels expand and contract smoothly to deliver oxygen where it is needed. When T3 drops, those vessels become stiff and unresponsive. They lose the ability to adapt to changes in blood pressure or oxygen demand.
This vascular stiffness is exactly where the pain begins. It creates a physical environment inside your skull that is ripe for chronic, daily pressure.
Astrocytes: The Brain’s Local Hormone Converters
Inside your brain, specialized star-shaped cells called astrocytes handle the conversion of T4 into T3 locally. They use an enzyme called deiodinase type 2 to do this.
When systemic thyroid levels fall, these astrocytes struggle to keep up. The localized T3 shortage leads to mitochondrial dysfunction in your brain tissue. Mitochondria are your cells’ power generators, and they need active thyroid hormone to work. When they fail, your brain enters a state of low-grade energy starvation.
This energy crisis activates pain receptors called nociceptors, which start sending constant pain signals to the brain. This is a key reason why patients with perfectly clean MRIs still suffer from severe, daily head pain.
Why Elevated TSH Matters
As your active hormones decline, your pituitary gland responds by flooding the bloodstream with TSH. According to the American Thyroid Association, normal TSH falls between 0.4 and 4.0 mIU/L. Anything above that strongly suggests your thyroid is underperforming.
TSH itself does not cause brain pain directly. But elevated TSH is the clearest alarm bell telling you that your brain is running on empty. When patients come in with a TSH of 10.0 or higher, they almost always describe a heavy, dull ache across their entire skull.
It is like trying to run a high-powered computer on a dying battery. Everything lags, overheats, and eventually starts sending distress signals.
Expert Insight: When “Normal” Labs Are Not Normal Enough
Many patients are told their thyroid is fine because their TSH reads 4.5. But in functional medicine, optimal TSH is usually between 1.0 and 2.0. If you are experiencing daily head pressure with a TSH above 3.0, your brain may already be feeling the deficit. Always ask for a full thyroid panel, not just a basic TSH screen.
How Hypothyroidism Triggers Chronic Head Pain
Let me break down what actually happens inside your head when your metabolism slows. The core issue is altered vascular homeostasis. Your blood vessels are not rigid pipes. They are dynamic, muscular tubes that constantly adjust their diameter to regulate blood flow.
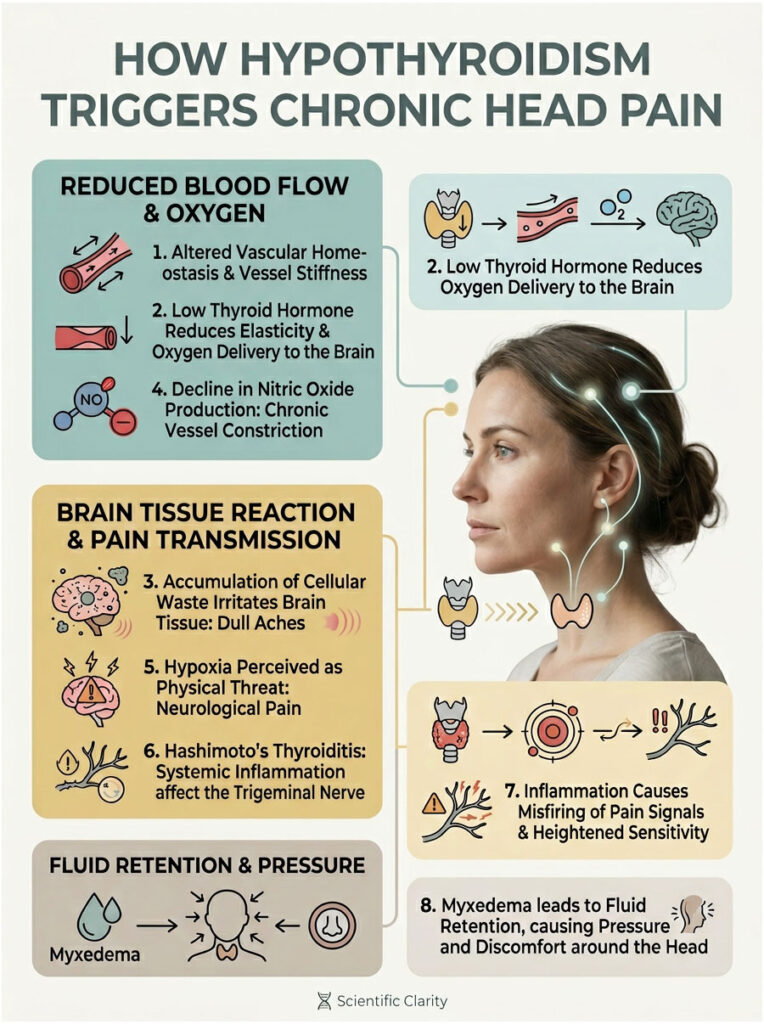
When thyroid hormone is low, these vessels lose their elasticity. They become sluggish and fail to dilate when your brain needs more oxygen. The result is a slow, suffocating pressure rather than a sharp, stabbing pain. It is a deep ache rooted in vascular stiffness.
On top of that, a slow metabolism means your body struggles to clear normal cellular waste products. These toxins build up around delicate brain tissue, irritating sensitive nerves and feeding into that persistent, dull ache.
Endothelial Dysfunction and Nitric Oxide
The inner lining of your blood vessels, called the endothelium, produces a molecule called nitric oxide. Nitric oxide tells blood vessels to relax. Active thyroid hormone is required for the endothelium to produce enough of it.
When T3 drops, nitric oxide production drops with it. Without enough nitric oxide, blood vessels stay chronically constricted. Less oxygen-rich blood reaches your brain, creating a state of mild hypoxia. Your brain interprets that oxygen shortage as a physical threat, and the result is neurological pain.
This is exactly why standard painkillers rarely touch this kind of headache. Ibuprofen and acetaminophen do not increase nitric oxide production. They do not relax stiffened blood vessels. They just temporarily mask the pain while the underlying problem continues.
Hashimoto’s Thyroiditis and Systemic Inflammation
In the United States, the most common cause of hypothyroidism is Hashimoto’s Thyroiditis, an autoimmune condition where the immune system attacks the thyroid gland. This creates widespread inflammation that does not stay in the neck.
That inflammation travels through the bloodstream and sensitizes the trigeminal nerve, which is the primary pain pathway for migraines and facial pain. When the trigeminal nerve becomes inflamed, it misfires constantly, sending pain signals to the brain.
This is why a Hashimoto’s flare is so hard to treat with regular painkillers. The immune system keeps the trigeminal nerve in a state of hyper-excitability. Every minor stressor can trigger a disproportionate pain response.
Myxedema and That “Balloon” Feeling
Many of my patients describe their head feeling like a balloon about to burst. This sensation usually comes from myxedema, a clinical condition caused by severe fluid retention in the body’s tissues.
Poor thyroid function leads to a buildup of complex sugars called mucopolysaccharides. These molecules act like tiny sponges, drawing in water and causing swelling in the face, neck, and sinus cavities. It mimics a severe sinus infection, but there is no actual infection present.
The fluid simply presses against nerve endings in the face and skull. The pressure stays constant until the metabolic rate is restored through proper treatment.
How to Identify a Thyroid Headache
So how do you know if your pain is coming from your thyroid? In clinical practice, we look for a specific set of symptoms that we call the thyroid headache profile. It looks and feels different from a classic migraine or a standard tension headache.
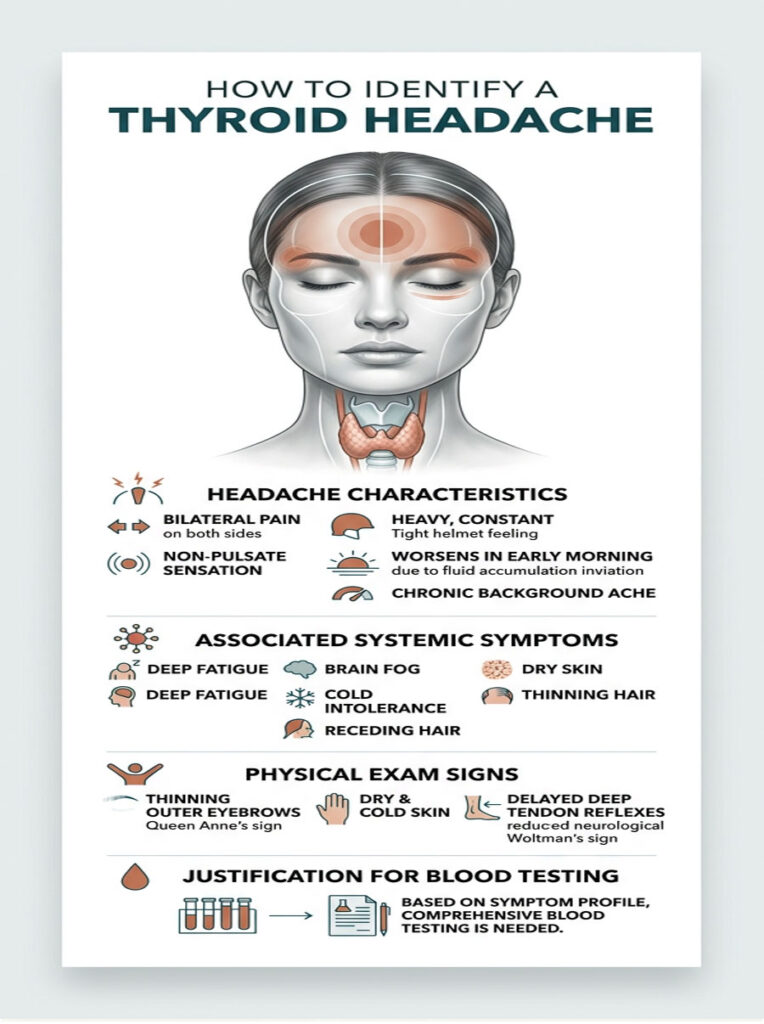
Bilateral, Non-Pulsatile Pain
The most telling feature is bilateral distribution. Thyroid-related headaches are almost always felt on both sides of the head at the same time. Classic migraines, by contrast, typically affect one side only.
The pain quality is another major clue. Migraines often throb in rhythm with your heartbeat. Thyroid headaches do not pulse. They feel like a constant, heavy weight pressing down on the top of the skull. Many patients compare it to wearing a motorcycle helmet that is two sizes too small.
This heavy sensation usually gets worse in the early morning. When you lie flat overnight, excess fluid accumulates in the head and neck. Because your metabolism is too slow to process that fluid, you wake up in significant pain. Waking up daily with a heavy head is a classic sign of metabolic dysfunction.
Chronic Nature and Associated Symptoms
Unlike migraines, which come and go in episodes, thyroid headaches are profoundly chronic. They show up every day as a persistent background ache that wears you down over time.
This pain almost never occurs alone. We always look for accompanying symptoms: deep fatigue that does not improve with sleep, brain fog that makes it hard to find words or remember simple tasks, cold intolerance, dry skin, and thinning hair, especially the outer third of the eyebrows.
Physical Exam Clues
During a physical examination, we look for thinning of the outer third of the eyebrows (called Queen Anne’s sign), skin that feels dry and unusually cold, and delayed deep tendon reflexes, particularly at the ankle. That delayed reflex, known as Woltman’s sign, confirms the neurological system is running at reduced speed.
The combination of these physical signs alongside bilateral head pressure defines the clinical thyroid headache profile and justifies comprehensive blood testing.
Thyroid Headache vs. Migraine vs. Tension Headache
Getting the right diagnosis early is one of the biggest challenges. Hypothyroid symptoms overlap with many neurological conditions, which is why misdiagnosis is so common. Over 60% of patients with thyroid-induced head pain are initially told they have tension headaches.
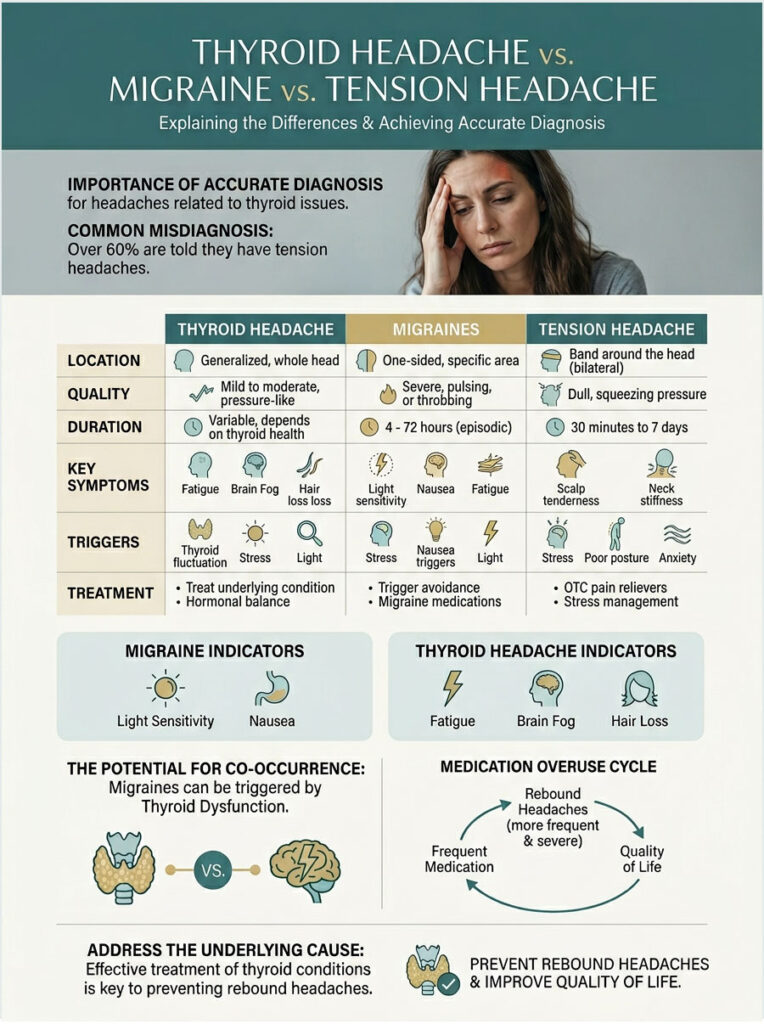
| Feature | Thyroid Headache | Classic Migraine | Tension Headache |
| Location | Both sides of the head | Usually one side | Band-like, both sides |
| Quality | Heavy, dull, non-pulsatile | Throbbing, pulsatile | Tight, squeezing |
| Duration | Daily, chronic | 4 to 72 hours, episodic | Variable |
| Key Symptoms | Brain fog, fatigue, cold intolerance, hair loss | Nausea, light/sound sensitivity | Neck/shoulder stiffness |
| Trigger | Low T3/T4, high TSH | Environment, hormones, diet | Stress, poor posture |
| Treatment | Levothyroxine (HRT) | Triptans, NSAIDs | NSAIDs, physical therapy |
The associated symptoms are the real tiebreaker. If you have light sensitivity and crippling nausea, you are likely dealing with a migraine. If you are losing the outer third of your eyebrows and feeling constant head pressure alongside fatigue and brain fog, your thyroid is the prime suspect.
It is also entirely possible to have both. Some patients have a genetic predisposition to migraines that are triggered more frequently by failing thyroid function. In those cases, treating the thyroid first usually cuts migraine frequency by more than half.
The Medication Overuse Trap
When patients do not know their thyroid is behind the pain, they naturally reach for painkillers every day. Over time, the brain becomes dependent on those medications. When the drug wears off, a rebound headache kicks in on top of the existing thyroid pain.
This creates a vicious cycle that destroys quality of life. The only way to break it is to stop the painkillers and fix the underlying metabolic problem. Early, accurate diagnosis prevents patients from falling into this trap.
What Recent Research Tells Us
The medical community has made significant progress in understanding this connection. Studies published in leading endocrine journals now confirm that hormonal deficits directly alter brain chemistry and pain signaling.
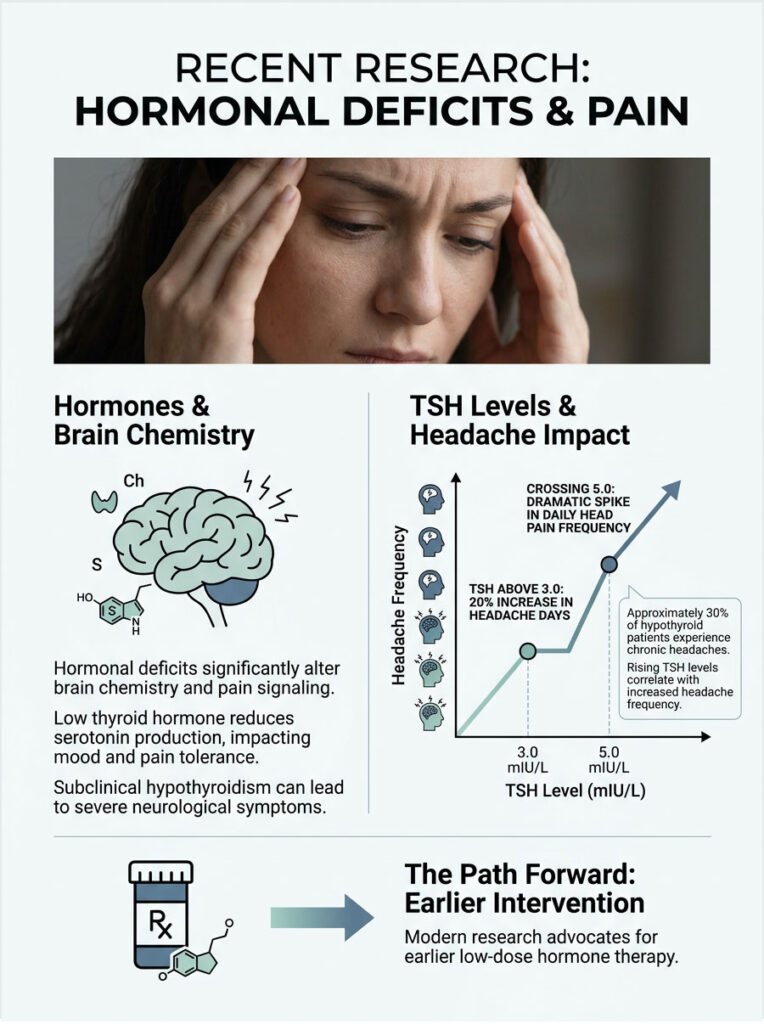
Roughly 30% of hypothyroid patients suffer from chronic headaches, a staggering number considering millions of Americans have diagnosed thyroid disease. Researchers have also found that low thyroid hormone decreases serotonin production in the brain. Serotonin regulates mood and central pain pathways, so when it drops, your natural pain tolerance drops with it.
Subclinical Cases Are Not Harmless
One of the most eye-opening areas of recent research involves subclinical hypothyroidism, where TSH is mildly elevated but T4 still sits in the normal range. In the past, doctors told these patients to wait and watch.
Modern studies from the Journal of Headache and Pain tell a different story. Even mild subclinical cases carry a significant headache burden. The brain is remarkably sensitive to minor metabolic shifts. You do not need a completely non-functioning thyroid to experience severe neurological symptoms. This finding is now a recognized reason to start low-dose hormone therapy earlier.
TSH Levels and Pain Frequency
Data from the Journal of Clinical Endocrinology & Metabolism tracked thousands of symptomatic patients over five years and mapped the correlation between rising TSH and headache frequency.
When TSH climbed above 3.0 mIU/L, patients reported a 20% increase in headache days per month. Once TSH crossed 5.0 mIU/L, daily head pain frequency spiked dramatically. This research supports early, proactive intervention to protect neurological function and improve quality of life.
Treatment: Restoring Thyroid Balance for Headache Relief
Once we have a confirmed diagnosis, the goal is not to mask the pain. The goal is to fix the root cause through Hormone Replacement Therapy (HRT).
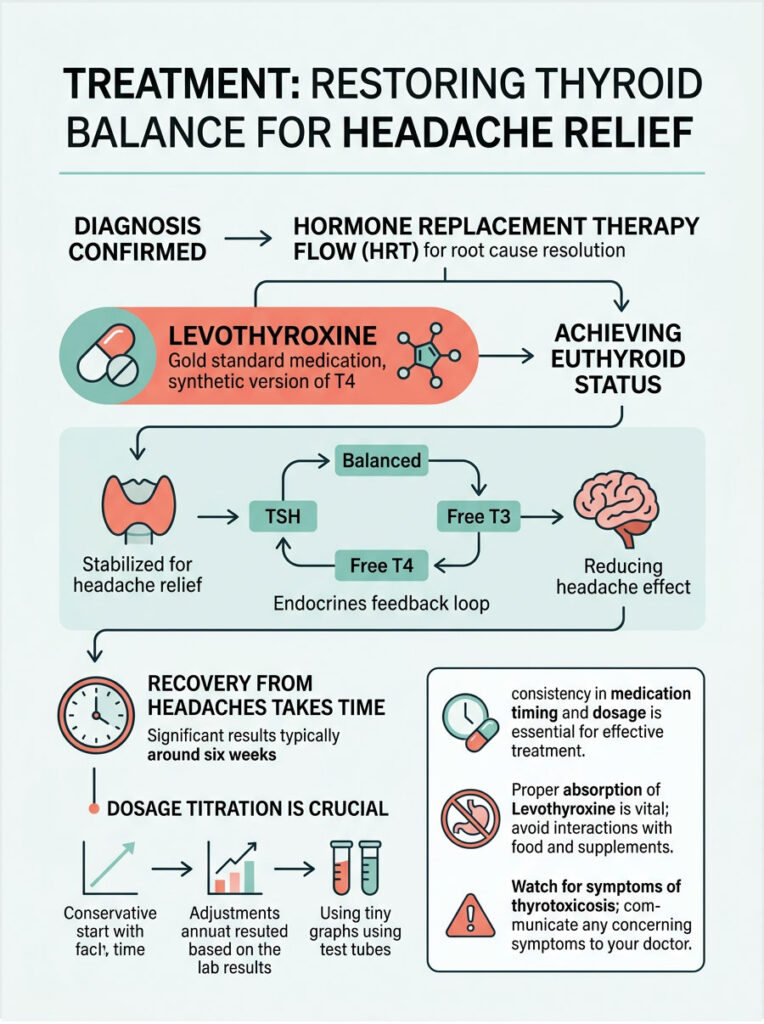
The gold standard medication is Levothyroxine, sold under brand names like Synthroid and Tirosint. It is a synthetic version of T4. When you take it daily, your body absorbs the T4 and converts it into active T3. Finding the right dose takes time, careful lab work, and patience.
What Euthyroid Status Means
Our clinical target is euthyroid status, meaning your TSH, Free T4, and Free T3 are all stabilized within optimal ranges. True relief comes when this balance is maintained consistently over several months.
As the body reaches this state, blood vessels regain elasticity. Myxedema fluid drains from facial tissues. Trigeminal nerve inflammation subsides. But it is not an overnight fix. Hormones work slowly at the cellular level. Recovery takes time, especially if you have been undertreated for months or years.
Safe Dosage Adjustment
Doctors always start with a conservative dose and increase it every six weeks based on lab results. This careful process, called dosage titration, is critical. Rushing it can cause thyrotoxicosis, where the dose is too high and mimics hyperthyroidism.
Thyrotoxicosis forces the heart to race and spikes blood pressure. Ironically, it can trigger a completely different type of vascular headache, a sharp, throbbing pain at the temples. If you notice heart palpitations or sudden anxiety after a dose increase, tell your doctor immediately.
Treatment Timeline: What to Expect
| Phase | Timeline | What You Can Expect |
| Starting HRT | Weeks 1-2 | Minimal headache change. Body begins slow metabolic adjustment. |
| Early Stabilization | Weeks 3-4 | Brain fog and fatigue start improving. Subtle decrease in head pressure. |
| Reaching Euthyroid | Weeks 6-8 | Significant reduction in bilateral head pain. Vascular tone normalizes. |
| Long-Term Maintenance | 3+ Months | Up to 70% drop in headache burden. Systemic inflammation decreases. |
True, lasting relief typically begins around the six-week mark. Consistency matters. Take your medication every single morning on an empty stomach, and do not skip doses.
Expert Tip: Absorption Matters
Take Levothyroxine with a full glass of water at least 60 minutes before eating or drinking coffee. Coffee, iron supplements, and calcium all block absorption in the gut. Poor gut absorption is the single most common reason patients fail to reach euthyroid status.
Practical Steps You Can Take Right Now
Medication is only half the picture. As a patient, you play a critical role in your own recovery. Managing thyroid-related headaches takes a proactive approach to both medical care and daily habits.
Ask for the Right Blood Tests
Do not settle for a basic TSH test. Request a full thyroid panel that includes TSH, Free T4, Free T3, and Reverse T3. Most importantly, ask for Thyroid Peroxidase (TPO) and Thyroglobulin (TgAb) antibodies. These antibody tests are the only way to confirm or rule out Hashimoto’s disease.
Keep a Headache Diary
Track the type of pain, duration, severity on a 1-to-10 scale, and whether it is bilateral or one-sided. Note the timing relative to your medication. If you notice that the pain spikes about an hour after taking your pill, the inactive fillers in generic levothyroxine might be causing an allergic reaction. Your doctor may switch you to a cleaner formulation like Tirosint.
Bring this diary to every appointment. Real-world data helps your doctor fine-tune your dose far more effectively than blood tests alone.
Adjust Your Diet
If your labs show high TPO antibodies, systemic inflammation is a major factor. Many patients find significant relief by adopting an anti-inflammatory, gluten-free diet. The molecular structure of gluten closely resembles thyroid tissue, and in susceptible patients, eating gluten can trigger an autoimmune flare.
Also focus on nutrient density. Your thyroid needs selenium and zinc to convert T4 into active T3. Brazil nuts, pumpkin seeds, and high-quality proteins provide the raw materials your body needs.
Manage Stress and Cortisol
Chronic stress drives your adrenal glands to pump out cortisol. High cortisol directly blocks the conversion of T4 into active T3 and instead creates Reverse T3, an inactive form. That metabolic slowdown brings on more head pain.
Stress management is not optional. Deep breathing, meditation, and consistent sleep are medical necessities when you are managing hypothyroidism. Lowering your cortisol is just as important as taking your daily medication.
Summary and Key Takeaways
If you have been wondering whether an underactive thyroid can cause headaches, the medical evidence is clear: it absolutely can, and it does more often than most people realize.
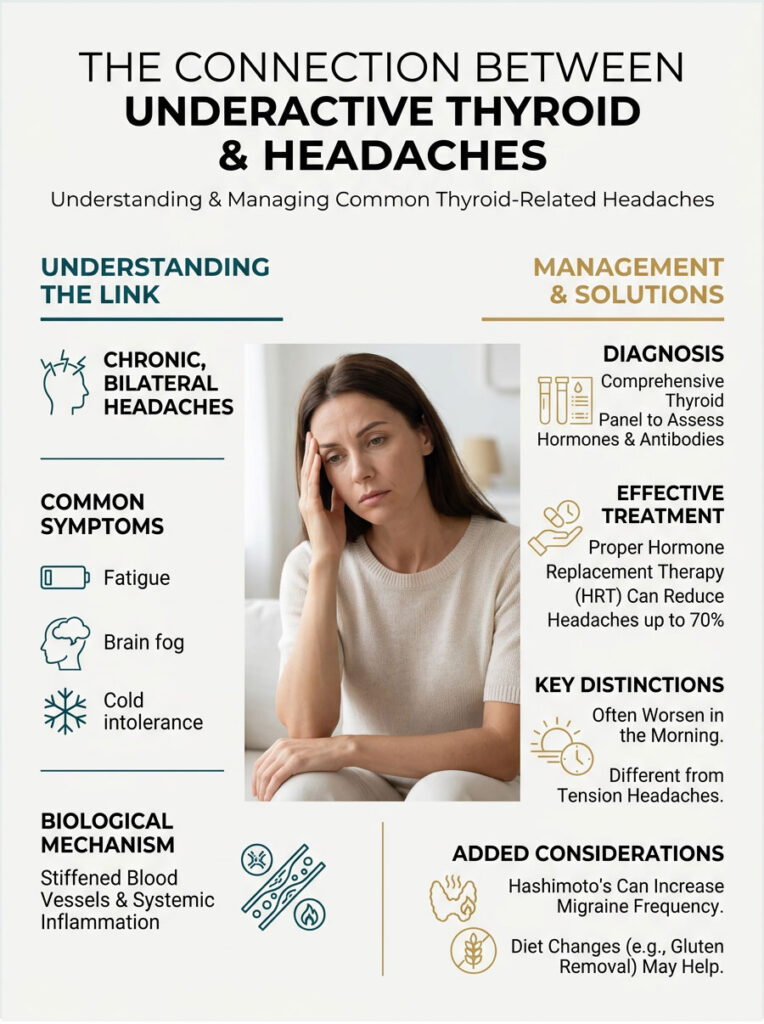
Low thyroid hormones stiffen blood vessels, starve the brain of energy, trigger systemic inflammation, and cause fluid retention. All of these pathways converge on chronic, bilateral head pain that does not respond to standard painkillers.
The good news is that this is a treatable condition. Proper hormone replacement therapy, combined with proactive lifestyle changes, can reduce your headache burden by up to 70% within a few months.
If you suffer from unresponsive daily headaches alongside fatigue, brain fog, and cold intolerance, ask your doctor for a comprehensive thyroid panel. Do not settle for endless prescriptions of over-the-counter painkillers. Track your symptoms, work with a specialist, and address the root cause. With the right clinical approach, you can get your life back.
Frequently Asked Questions
Can an underactive thyroid cause daily headaches?
Yes, chronic daily headaches are a clinically recognized symptom of hypothyroidism. When thyroid hormone levels drop, it disrupts vascular homeostasis and lowers your metabolic rate, leading to persistent, bilateral head pain. Approximately 30% of patients with thyroid insufficiency report chronic headaches as a primary symptom.
What does a typical thyroid-induced headache feel like?
A thyroid headache profile is usually characterized by non-pulsatile, heavy, and dull pressure felt on both sides of the head (bilateral). Unlike migraines, which are often throbbing and one-sided, endocrine-related head pain feels like a constant weight or a tight band around the skull, frequently worsening in the morning due to fluid retention.
Why does low thyroid hormone lead to head pressure and pain?
The pathophysiology involves endothelial dysfunction. Without adequate active T3 hormone, blood vessels lose their elasticity and fail to produce enough nitric oxide to relax. This leads to chronic vascular constriction and mild hypoxia in brain tissues, which triggers pain receptors (nociceptors) to signal metabolic distress.
Can subclinical hypothyroidism cause migraines even if my T4 levels are normal?
Absolutely. Recent clinical data suggests that even subclinical cases—where TSH is mildly elevated but T4 remains in the ‘normal’ range—can cause a significant headache burden. The brain is highly sensitive to minor metabolic shifts, and many patients experience relief only once they achieve optimal TSH levels between 1.0 and 2.0 mIU/L.
How long does it take for headaches to stop after starting Levothyroxine?
The average euthyroid status recovery time is typically 6 to 8 weeks. While some patients notice a reduction in brain fog within the first month, it takes several weeks of stable hormone replacement therapy for vascular tone to normalize and for systemic inflammation to subside enough to eliminate chronic head pain.
Is there a link between Hashimoto’s Thyroiditis and chronic migraines?
Yes, Hashimoto’s is an autoimmune condition that creates systemic inflammation. This inflammation can sensitize the trigeminal nerve, the primary pathway for migraine pain. Patients with Hashimoto’s often experience a higher frequency of migraines during ‘flares’ when thyroid peroxidase (TPO) antibodies are elevated.
Can my thyroid medication actually cause more headaches?
It is possible. If your levothyroxine dosage is too high, you may enter a state called thyrotoxicosis (mimicking hyperthyroidism), which causes rapid heart rate and vascular throbbing. Additionally, some patients react to inactive fillers or dyes in generic tablets; switching to a cleaner formulation like Tirosint often resolves these medication-linked headaches.
What is the relationship between high TSH levels and head pressure?
High TSH serves as a metabolic alarm bell. While TSH doesn’t cause pain directly, its elevation correlates with a state of cellular energy starvation and myxedema. Myxedema causes fluid retention in the interstitial tissues of the face and skull, creating a physical sensation of intense intracranial pressure.
Why do thyroid headaches often feel worse when waking up in the morning?
This is primarily due to the metabolic slowdown and fluid dynamics. When you lie flat overnight, the lack of metabolic efficiency leads to increased fluid accumulation (myxedema) in the head and neck tissues. This extra fluid presses against sensitive nerves, causing many hypothyroid patients to wake up with a heavy, aching head.
What blood tests should I request to investigate thyroid-related head pain?
A basic TSH screening is often insufficient. You should request a full thyroid panel including TSH, Free T4, Free T3, and Reverse T3. Furthermore, ensure your doctor tests for TPO and TgAb antibodies to rule out Hashimoto’s, as autoimmune inflammation is a major trigger for neurological pain.
Can a gluten-free diet help reduce thyroid-induced headaches?
In cases of autoimmune Hashimoto’s, yes. Gluten proteins can trigger molecular mimicry, causing the immune system to attack the thyroid and increase systemic inflammation. Many patients find that removing gluten reduces their antibody count and significantly lowers the frequency of their subclinical hypothyroidism migraines.
How can I tell the difference between a tension headache and a thyroid headache?
While both are bilateral and dull, a thyroid headache is almost always accompanied by other metabolic symptoms like profound fatigue, cold intolerance, brain fog, and physical signs like Queen Anne’s sign (thinning eyebrows). If your ‘tension’ headache doesn’t respond to NSAIDs but correlates with low energy, an endocrine origin is likely.
Disclaimer
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The link between endocrine function and neurological pain is complex; always consult with a board-certified endocrinologist or qualified healthcare professional before starting hormone replacement therapy or changing your medication regimen.
References
- Journal of Headache and Pain (2021) – “The Prevalence of Chronic Daily Headache in Patients with Hypothyroidism” – Statistical data on the 30% prevalence of headaches in thyroid patients.
- American Thyroid Association – thyroid.org – Standard reference ranges for TSH and guidelines for diagnosing hypothyroidism.
- Journal of Clinical Endocrinology & Metabolism – “TSH Dynamics and Neurological Stress” – Research correlating elevated TSH levels with increased migraine frequency.
- National Institutes of Health (NIH) – “Neurological Manifestations of Hypothyroidism” – Deep dive into the HPT axis and its effect on central nervous system function.
- Endocrine Society – endocrine.org – Clinical resources regarding the metabolic impact of T3 and T4 on vascular smooth muscle cells.





