
When an endoscope passes beyond the lower esophageal sphincter, it enters a cavity that is far more than a simple food pouch. The stomach is one of the most impressive organs in the human body, and the oblique muscle layer is the reason why.
Table of Contents
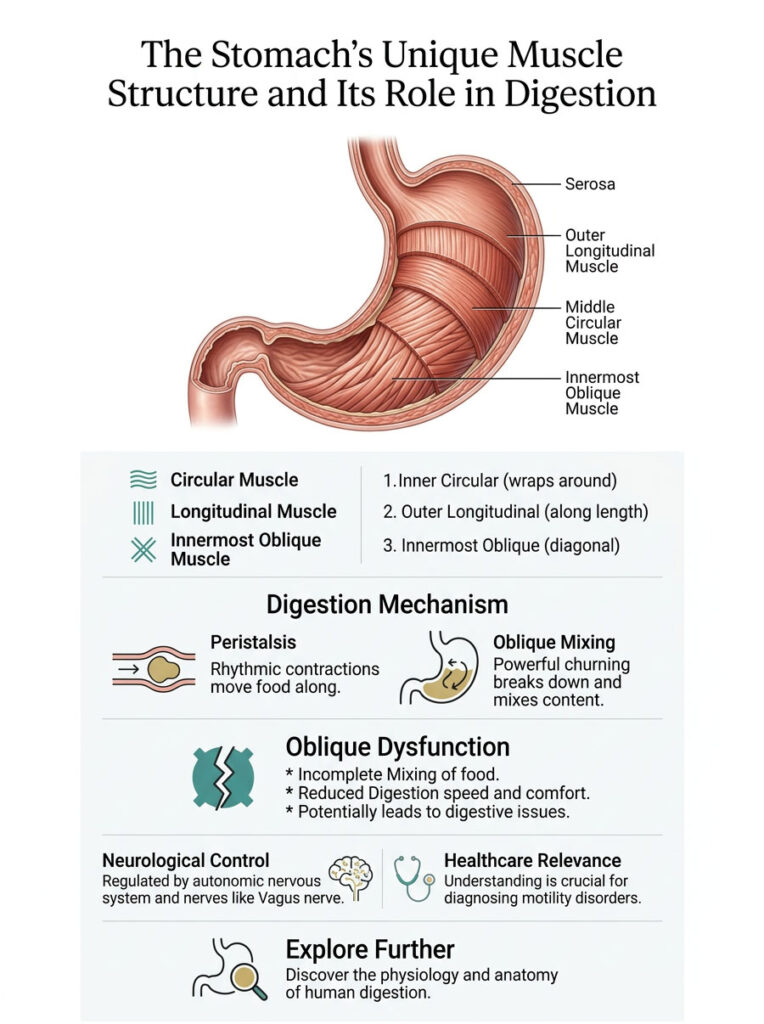
Most of the gastrointestinal tract runs on a basic two-layer muscular system known as the muscularis externa. There is an inner circular layer and an outer longitudinal layer. Together, they push food forward through peristalsis. The stomach, however, breaks this rule entirely. It adds a third, innermost muscle layer, the oblique fibers, and that single addition changes everything about how this organ works.
Without this specialized muscular arrangement, digesting a solid meal would be biologically impossible. The stomach would have no way to grind, twist, or crush food into a form the intestines can absorb.
In this detailed clinical review, we will explore the precise anatomy of the oblique muscle layer, the physics of mechanical digestion, the neurological control systems behind it, and what happens when this critical layer fails. Whether you are a medical student, a clinician, or simply curious about human physiology, understanding this unique gastric structure is essential to making sense of how digestion actually works.
Quick Answer: What Is the Oblique Muscle Layer?
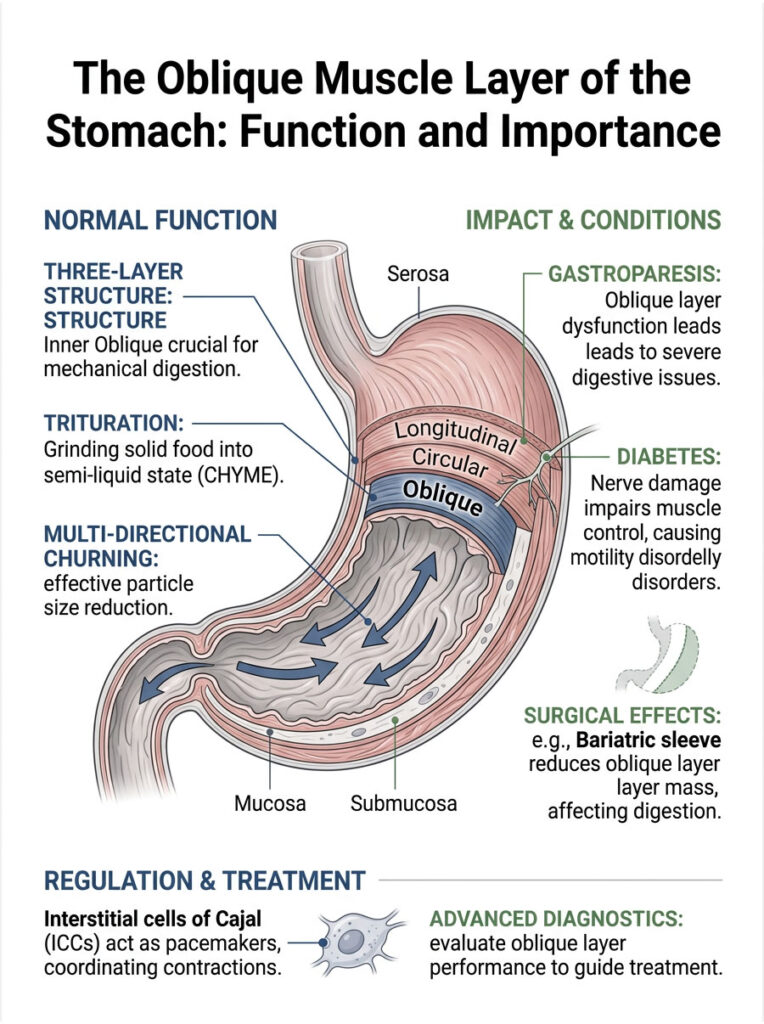
The oblique muscle layer is the innermost third layer of the muscularis externa, found exclusively in the human stomach. It is responsible for multi-directional churning that mechanically grinds solid food into a semi-liquid state called chyme. This layer is most concentrated in the gastric fundus and body, giving the stomach the ability to perform complex digestion that the rest of the two-layer digestive tract simply cannot achieve.
Key Statistics on Gastric Motility
- The stomach generates a basal electrical rhythm of roughly 3 cycles per minute.
- Smooth muscle cells in the gastric wall range from 20 to 500 micrometers in length.
- Solid food particles must be ground down to less than 2 millimeters before they can pass through the pyloric sphincter.
- A standard solid meal takes about 3 to 4 hours to empty from a healthy stomach.
- Bariatric sleeve gastrectomy removes up to 80 percent of stomach volume, drastically reducing the oblique layer.
- Up to 40 percent of patients with functional dyspepsia show impaired gastric accommodation.
- The stomach can expand from a resting volume of 50 milliliters to more than 1,000 milliliters during a large meal.
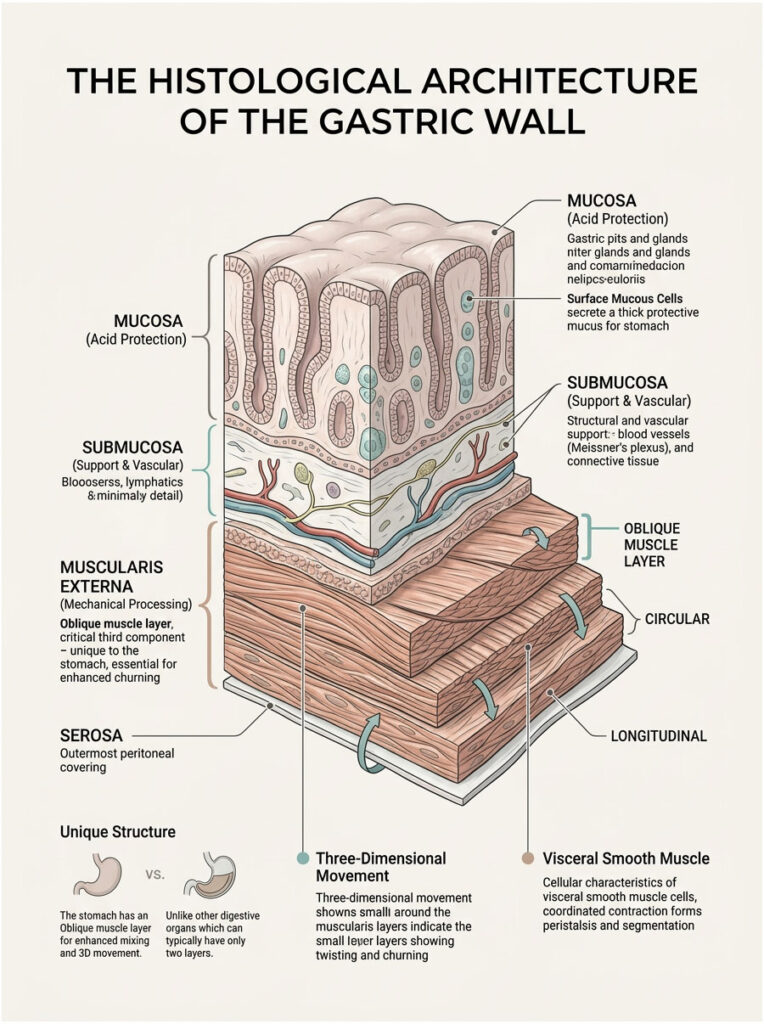
The Histological Architecture of the Gastric Wall
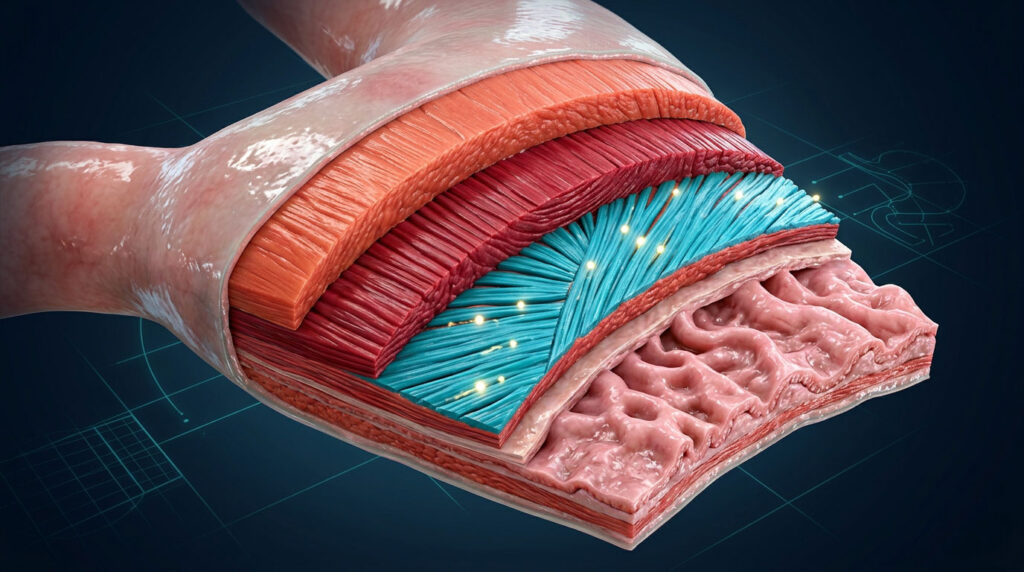
To really understand how the stomach processes a meal, you need to look at it under a microscope. Gastric wall histology reveals a layered system built for both defense and mechanical processing. The mucosal lining shields against acid. The submucosa provides structural and vascular support. But the real mechanical power sits deeper, inside the muscularis externa.
The stomach does not just squeeze food in one direction. It twists, folds, and crushes food with remarkable physical force. That kind of three-dimensional movement demands a physical framework that goes well beyond the standard two-layer design. And that framework is built by the oblique muscle fibers.
Here is the key point: you cannot generate three-dimensional movement using only two layers of muscle. The human body evolved a specific anatomical solution to handle solid, fibrous foods, and that solution was the oblique muscle layer.
Breaking Down the Muscularis Externa Layers
Across the esophagus, small intestine, and large intestine, the muscularis externa follows a strict two-layer rule. An inner circular layer pinches the tube closed, and an outer longitudinal layer shortens it to push contents forward. This setup works perfectly for simple forward propulsion.
The stomach needs something entirely different. It introduces the inner oblique layer as the critical third component. This layer sits closest to the submucosa, directly inside the middle circular layer. By adding diagonal fibers to the horizontal and vertical ones, the stomach creates a complete muscular grid.
This distinct gastric wall histology is what turns the stomach into a biological cement mixer. When all three layers contract in a coordinated sequence, the stomach wall can wring itself out like a wet towel. That extreme mechanical force is exactly what breaks down fibrous meats and dense vegetables.
Cellular Makeup of Visceral Smooth Muscle
The cells that make up the oblique muscle layer are fundamentally different from skeletal muscle. They lack the rigid striations you see in your biceps or quadriceps. Instead, actin and myosin filaments arrange themselves in a loose, lattice-like network. This design allows the muscle to stretch dramatically without losing its ability to contract.
When you eat a large meal, the stomach volume expands significantly. The oblique fibers stretch smoothly to handle that increase. Even at their maximum stretch, these smooth muscle cells still generate powerful contractile force.
These cells also connect through specialized gap junctions, tiny communication tunnels between adjacent cells that let electrical signals pass instantly from one cell to the next. This ensures perfectly synchronized contractions across the entire stomach wall.
Embryological Development of the Third Layer
How does this third layer form in the womb? During human embryogenesis, the primitive gut tube starts as a simple, straight cylinder. Around the fourth week of gestation, the stomach region begins to dilate and rotate, creating the greater and lesser curvatures we recognize in adult anatomy.
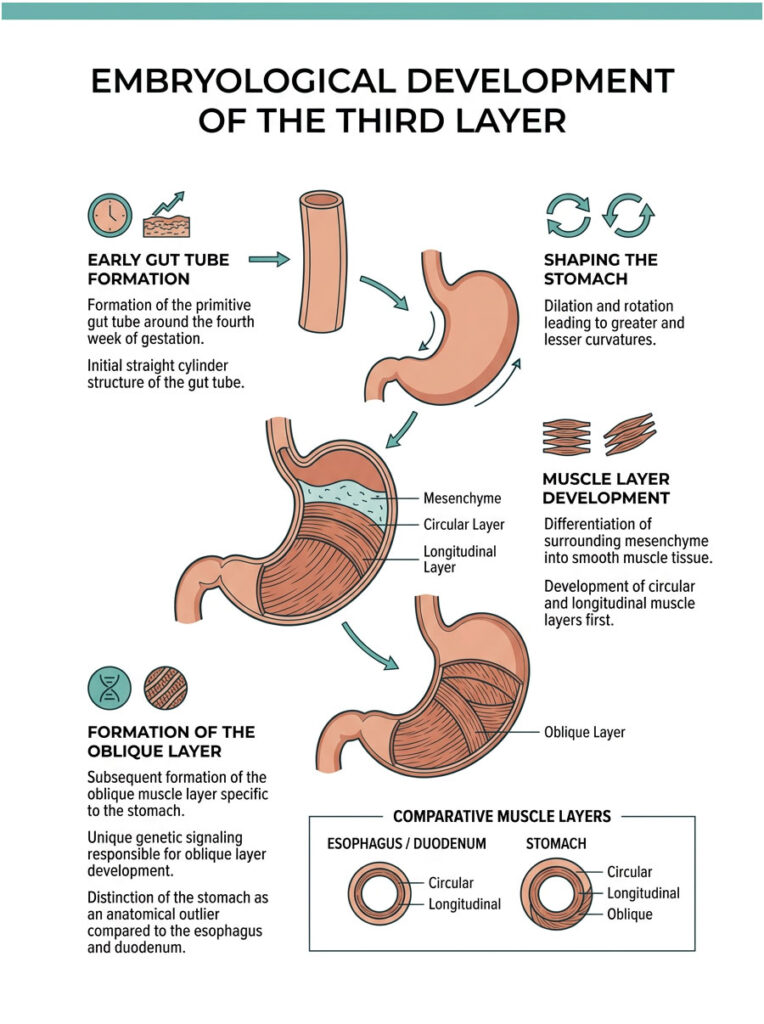
As the stomach rotates, the surrounding mesenchyme differentiates into smooth muscle tissue. The circular and longitudinal layers develop first, mirroring the rest of the gut tube. The oblique muscle layer develops slightly later, forming in response to genetic signaling unique to the gastric region.
This developmental timing is why the oblique layer exists only in the stomach. The genetic markers that trigger its formation are absent in the esophagus and duodenum. It makes the stomach a genuine anatomical outlier within the human body.
Anatomical Origin: The Cardiac Notch and Fundus
The oblique muscle layer does not cover the stomach uniformly. Its positioning is highly strategic. The fibers originate near the cardiac notch, which is the sharp angle where the esophagus meets the greater curvature.
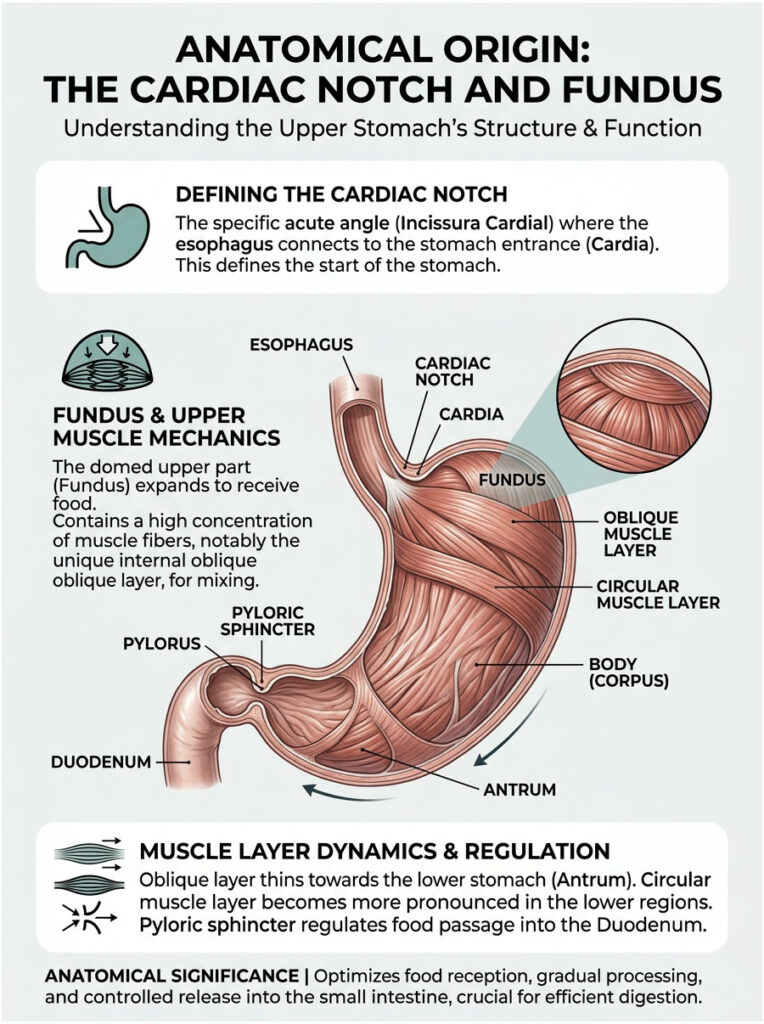
From there, these specialized muscle fibers fan out extensively. They are most heavily concentrated in the fundus and the upper body of the stomach. This concentration makes sense because the upper stomach is responsible for receiving and initially mixing the swallowed food.
As you move lower toward the antrum, the oblique layer begins to thin out. By the time you reach the distal antrum, these oblique fibers have largely disappeared. The heavy lifting in the lower stomach is handled by the massively thickened circular layer, which eventually forms the pyloric sphincter.
Comparative Anatomy: How the Stomach Stands Apart
To understand why the stomach is anatomically unique, it helps to compare it directly against other parts of the digestive tract.
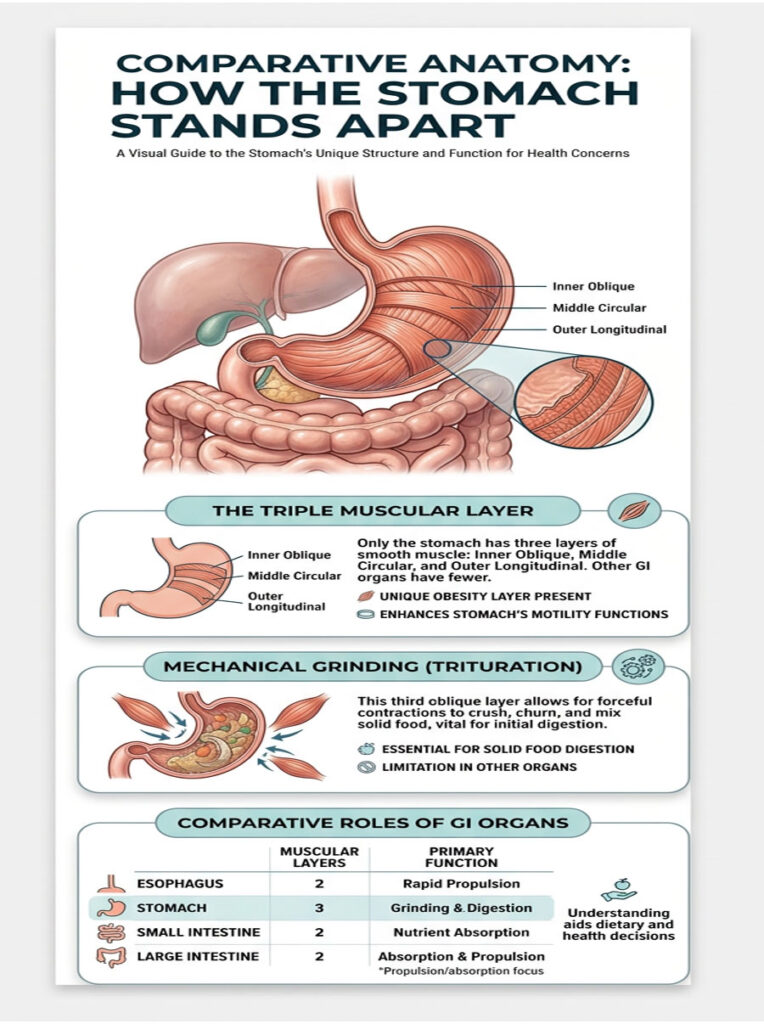
| Organ | Muscularis Externa Layers | Primary Motility Function | Oblique Layer |
| Esophagus | Two (Inner Circular, Outer Longitudinal) | Rapid Propulsion (Peristalsis) | Absent |
| Stomach | Three (Inner Oblique, Middle Circular, Outer Longitudinal) | Mechanical Grinding (Trituration) | Present |
| Small Intestine | Two (Inner Circular, Outer Longitudinal) | Nutrient Absorption (Segmentation) | Absent |
| Large Intestine | Two (Inner Circular, Outer Longitudinal / Teniae Coli) | Water Absorption and Mass Movement | Absent |
The stomach is the only organ in the GI tract with three muscular layers. Without that third layer, humans would be unable to digest solid food and would be limited to liquid diets.
The Physics of Trituration and Mechanical Digestion
We tend to think of digestion as a chemical process driven by stomach acid and enzymes. In reality, the stomach is primarily a mechanical processor. The physical breakdown of food is just as critical as the chemical breakdown. This mechanical grinding is clinically called trituration.
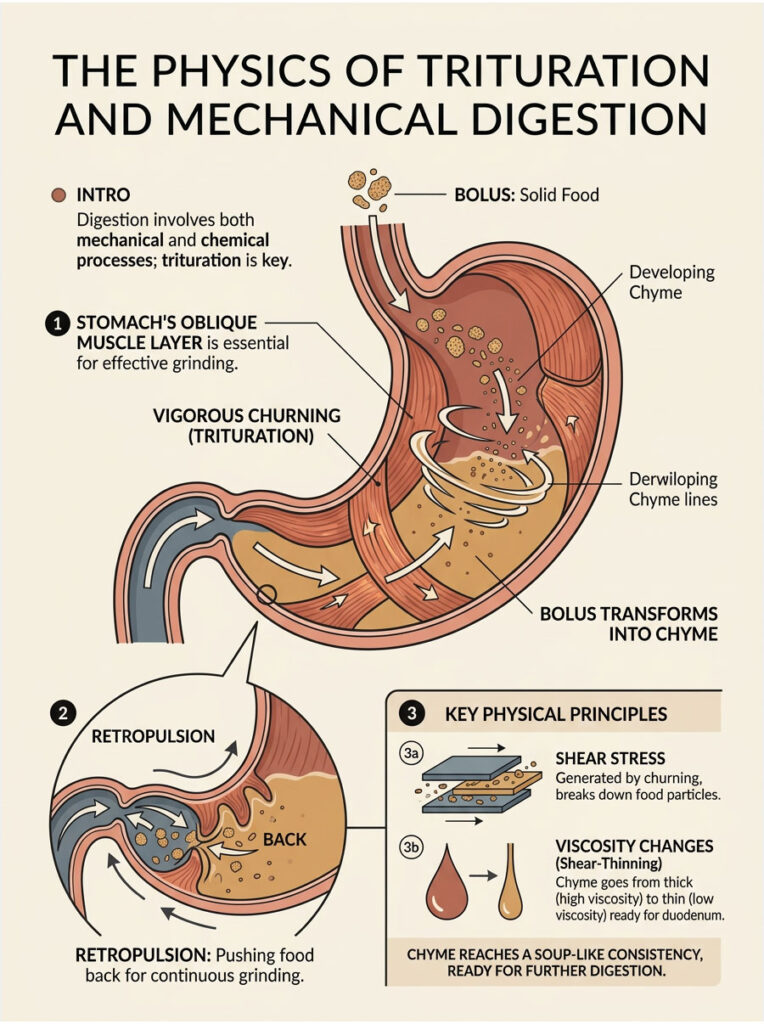
Trituration is the vigorous, multi-directional churning that reduces solid food into a semi-liquid state. Without the oblique muscle layer, this type of grinding would be impossible. The stomach would merely push large, undigested chunks forward, leading to serious intestinal blockages.
Bolus to Chyme: How Grinding Actually Works
When you swallow a piece of steak, it enters the stomach as a solid, cohesive mass. The stomach must apply raw physical force to tear that mass apart. This is where the three-layer architecture proves its worth.
Once food enters the stomach, the inner oblique layer initiates diagonal contractions. These work against the circular and longitudinal layers to produce a multi-dimensional wringing effect. The food is violently thrown against the closed pyloric valve at the bottom of the stomach, an action known in gastroenterology as retropulsion.
Retropulsion forces the food back up into the body of the stomach for more grinding. Through repeated cycles of propulsion and retropulsion, the solid bolus is slowly sheared apart. It mixes with gastric acid and pepsin, eventually becoming the thick, milky fluid known as chyme.
Fluid Dynamics Inside the Gastric Cavity
The creation of chyme involves complex fluid dynamics. As the oblique muscle layer churns the stomach contents, it generates intense shear stress, the physical force that literally rips microscopic food particles away from the main solid mass.
The viscosity of the stomach contents changes dramatically during this process. A meal starts as a thick, highly viscous mass. As trituration continues and gastric juices mix in, the overall viscosity drops. This physical transformation is called shear-thinning.
The oblique fibers constantly adjust their contractile force as the fluid dynamics change inside the cavity. Once the chyme reaches the consistency of a thick soup, it is ready for the next stage of digestion.
Gastric Accommodation and Receptive Relaxation
Before the stomach can grind food, it has to receive it safely. This brings us to a specialized function called gastric accommodation. When you start eating, the upper part of the stomach must actively relax to hold the incoming volume of food.
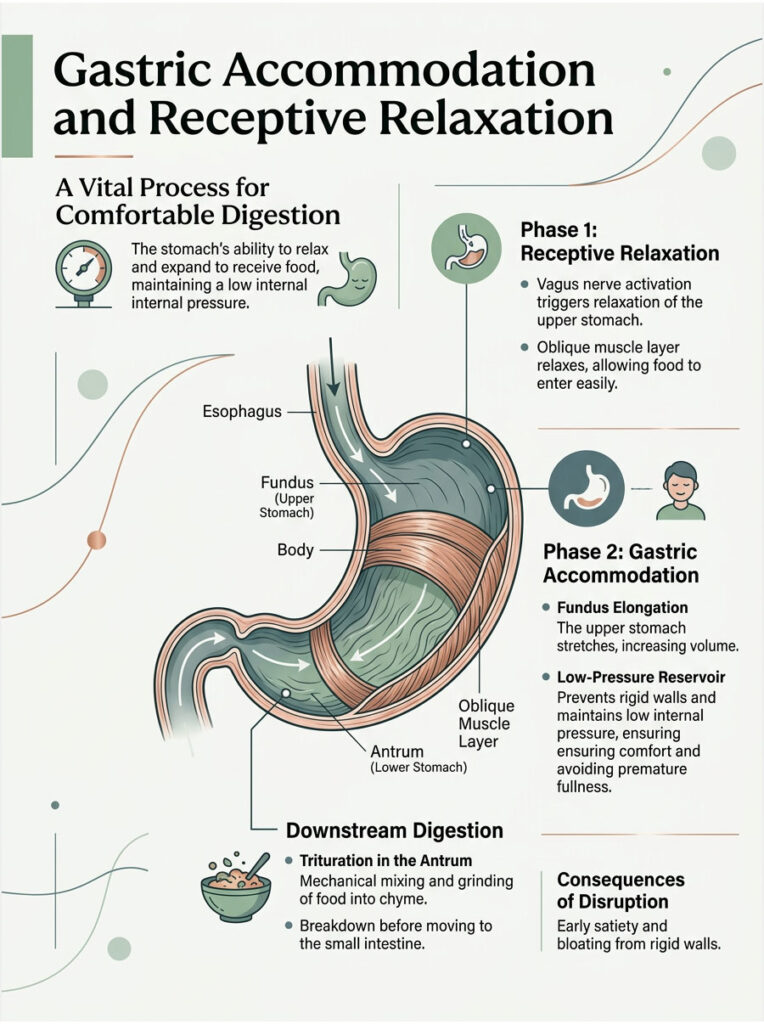
The oblique muscle layer plays a direct role in this receptive relaxation. Because its fibers are concentrated in the fundus, they can actively elongate. This allows the stomach to expand without a dangerous spike in internal pressure.
If the stomach walls were rigid, eating even a small amount of food would cause immediate pain and regurgitation. Gastric accommodation ensures the stomach acts as a low-pressure reservoir while the lower antrum begins the slow process of trituration.
The Pyloric Sphincter: The Stomach’s Particle Filter
The stomach does not dump its contents randomly into the intestines. It acts as a highly selective biological sieve. The gatekeeper is the pyloric sphincter, a thick ring of smooth muscle at the junction of the stomach and the duodenum.

Food particles must be ground to less than 2 millimeters in diameter before they can pass into the small intestine. Anything larger gets rejected by the pyloric sphincter and sent back for more grinding.
The synergy between the oblique layer’s grinding action and the circular layer’s control of the pyloric sphincter is precise. The oblique fibers smash the food down to the required size. Once the chyme reaches the correct consistency, the sphincter relaxes just enough to let a small amount pass through at a time.
Electromechanical Coupling and Neurological Control
Muscles do not contract on their own. They need precise, rhythmic electrical signals. The stomach’s muscularis externa is controlled by a sophisticated neurological network that ensures all three muscle layers fire in the exact sequence needed for effective digestion.
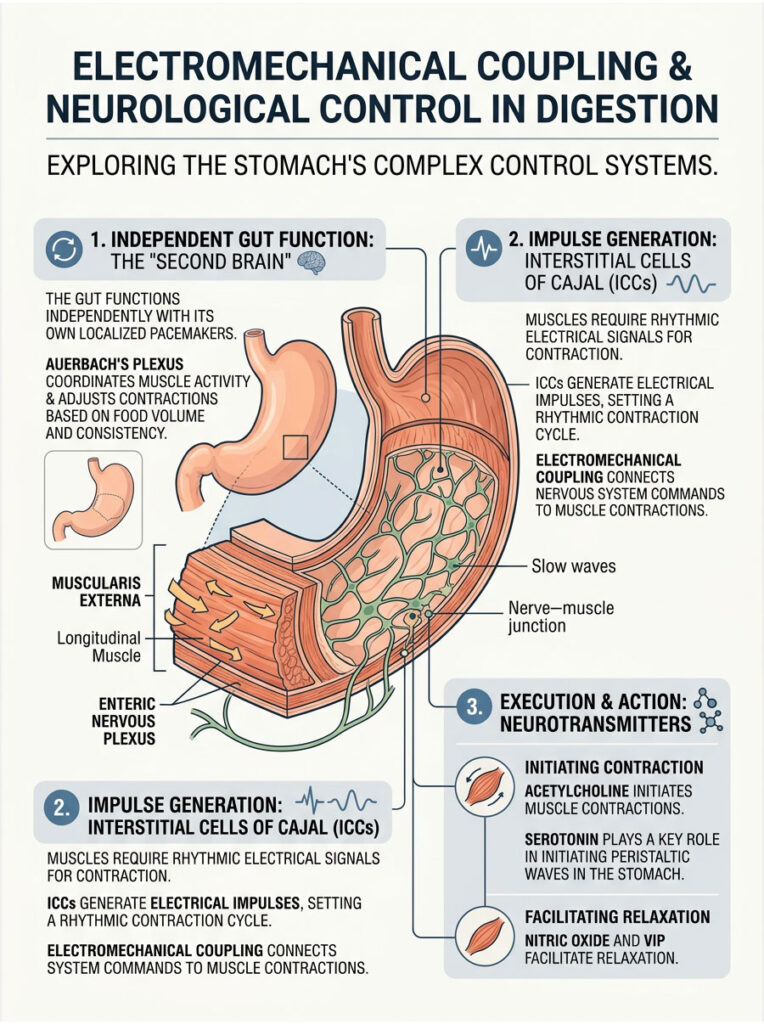
This signaling process is called electromechanical coupling. It bridges the gap between the nervous system’s electrical commands and the physical contraction of the visceral smooth muscle. When the coupling is perfectly synchronized, digestion goes completely unnoticed.
What makes this even more remarkable is that the gut operates largely independently from the central nervous system. It relies on its own localized pacemakers and nerve bundles, a system often called the body’s second brain.
The Myenteric Plexus (Auerbach’s Plexus)
The enteric nervous system is a vast web of neurons embedded directly within the gastrointestinal walls. The most important component for motor function is Auerbach’s plexus, also known as the myenteric plexus. This nerve network sits between the longitudinal and circular muscle layers.
Auerbach’s plexus acts as the master conductor of the stomach’s muscular activity. It sends efferent signals deep into the inner oblique layer to coordinate complex contractions. Without these signals, the oblique fibers would fire randomly, causing painful spasms instead of productive churning.
The myenteric plexus constantly evaluates the volume and consistency of the food inside the stomach. It then adjusts the intensity of muscle contractions accordingly. A heavy, fat-rich meal triggers stronger and longer trituration cycles.
Neurotransmitters That Drive the Oblique Muscle Layer
Communication between Auerbach’s plexus and the oblique muscle layer relies on specific chemical messengers. Acetylcholine is the primary excitatory neurotransmitter. When released, it binds to muscarinic receptors on the smooth muscle cells, triggering a powerful contraction.
The stomach also needs to relax, especially during gastric accommodation. This relaxation is driven by inhibitory neurotransmitters like nitric oxide and vasoactive intestinal peptide (VIP). These chemicals signal the oblique fibers in the fundus to elongate and yield to incoming food.
Serotonin (5-HT) also plays a major role. Over 90 percent of the body’s serotonin is found in the gut, where it helps initiate the peristaltic waves that sweep across the stomach wall.
Interstitial Cells of Cajal: The Gastric Pacemakers
Just as the heart has a pacemaker to regulate its beat, the stomach has its own rhythmic timekeepers. These are the Interstitial cells of Cajal (ICC), located within the gastric pacemaker zone along the greater curvature. The ICCs generate spontaneous electrical impulses.
These impulses create slow-wave electrical potentials that propagate through all three muscle layers. In a healthy stomach, the ICCs produce a basal electrical rhythm of exactly three cycles per minute. This steady rhythm sets the maximum frequency of gastric contractions.
When the slow waves align with signals from Auerbach’s plexus, an action potential fires. That action potential results in a physical muscle contraction. This is a textbook example of electromechanical coupling, and it keeps the oblique muscle layer churning food at a steady, measured pace.
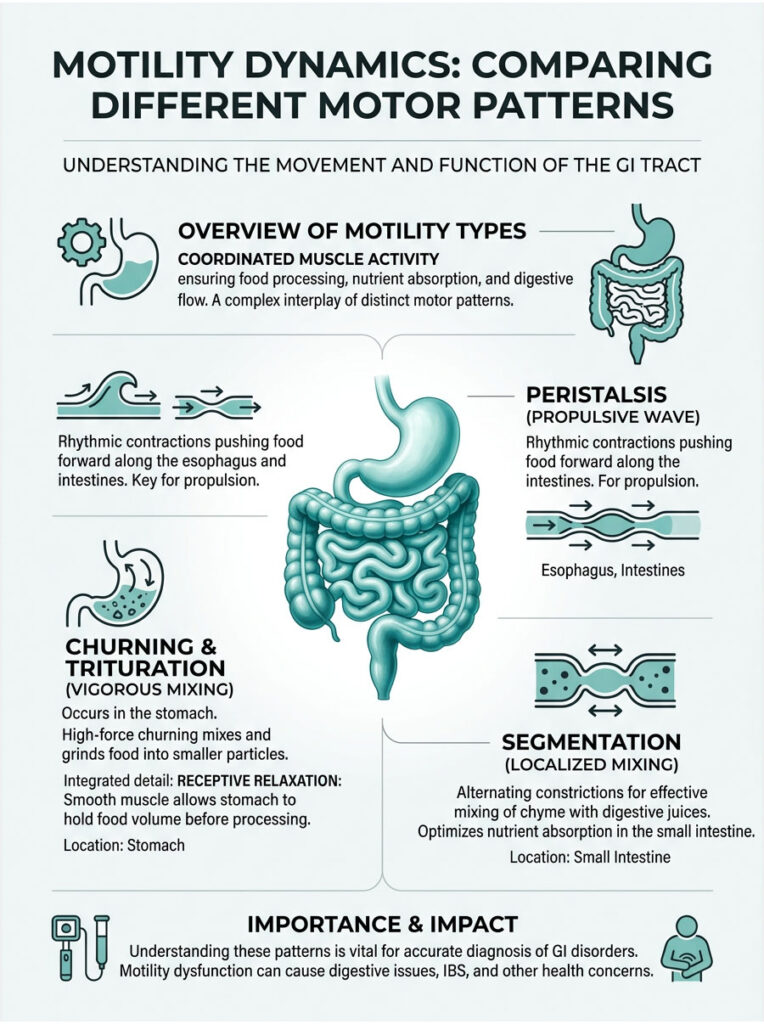
Motility Dynamics: Comparing Different Motor Patterns
| Motility Type | Description | Dominant Muscle Layer | Primary GI Location |
| Peristalsis | Rhythmic, wave-like forward propulsion | Circular and Longitudinal | Esophagus, Intestines |
| Churning / Trituration | Vigorous, multi-directional mixing and grinding | Oblique (with Circular and Longitudinal) | Stomach |
| Segmentation | Localized, oscillatory contractions for mixing | Circular | Small Intestine |
| Receptive Relaxation | Smooth muscle relaxation to hold volume | Oblique and Circular | Gastric Fundus |
Understanding these motor patterns is crucial for any clinician. When a patient presents with digestive symptoms, identifying which motility type is failing leads directly to the correct diagnosis.
Clinical Correlations: When the Oblique Muscle Layer Fails
Understanding normal physiology is only half the picture. Clinicians must also recognize what happens when the system breaks down. When the muscularis externa loses its ability to contract effectively, the entire digestive process stalls.
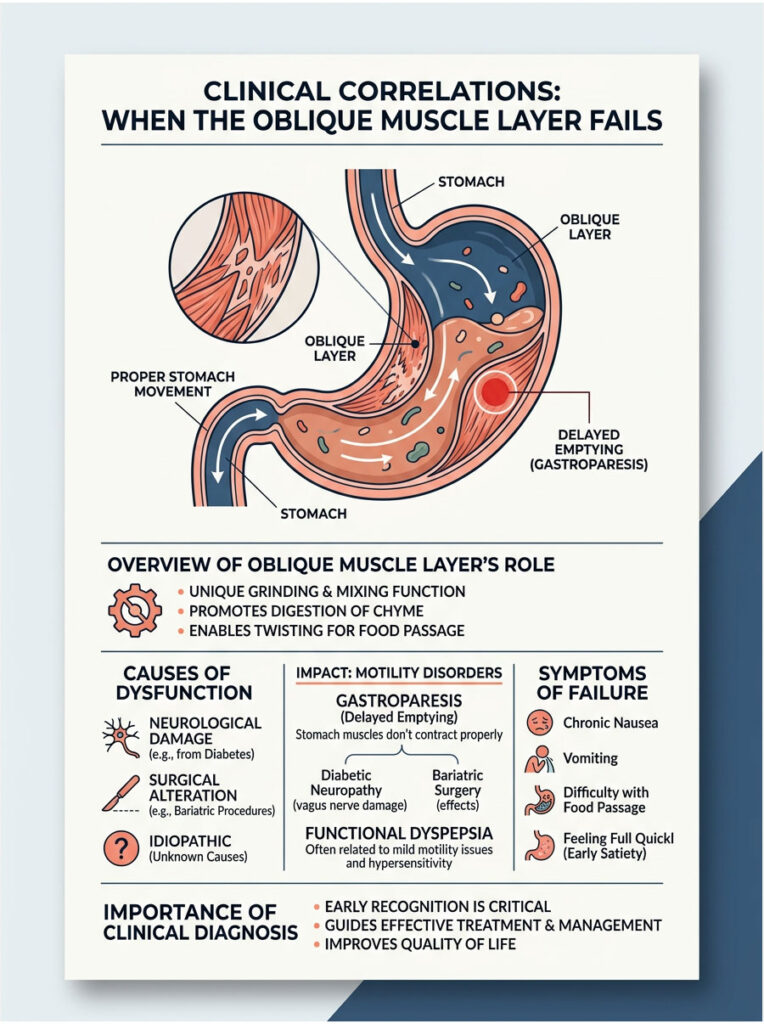
Failure of the stomach’s muscle layers can result from neurological damage, surgical alteration, or idiopathic causes. Regardless of origin, the symptoms are universally debilitating. A stomach with a non-functional oblique muscle layer transforms from a dynamic processor into a stagnant reservoir.
Clinical Insight: When a patient presents with chronic nausea and vomiting of undigested food eaten hours earlier, always suspect a failure of the mechanical grinding phase. If the food is not reduced to under 2 millimeters, the pyloric sphincter will simply refuse to let it pass.
Gastroparesis and Delayed Gastric Emptying
Gastroparesis literally translates to stomach paralysis. It occurs when vagal innervation to the stomach is severely damaged. When the vagus nerve fails, Auerbach’s plexus cannot properly stimulate the muscularis externa.
The inner oblique layer stops churning completely. The bolus-to-chyme conversion process fails. Patients experience severe nausea, vomiting, and early satiety because solid food sits in the stomach, unable to be broken down.
Because the food particles remain too large, the pyloric sphincter stays tightly closed. The stomach essentially becomes a painful trap for undigested meals.
Diabetic Neuropathy and Smooth Muscle Decline
Diabetes is the leading known cause of gastroparesis worldwide. Chronic hyperglycemia causes severe oxidative stress and microvascular damage to the nerves supplying the gut. Over time, uncontrolled high blood sugar physically destroys the vagus nerve endings.
When nerve supply is compromised, the Interstitial cells of Cajal begin to deplete. Biopsies from diabetic patients often reveal a significant reduction in these pacemaker cells. Without the ICCs generating the 3-cycle-per-minute rhythm, the oblique muscle layer loses its coordination.
In advanced diabetic neuropathy, the stomach muscles may atrophy. Smooth muscle cells shrink and lose contractile force. This makes blood glucose management extremely difficult, as food absorption becomes highly unpredictable.
Bariatric Surgery: The Impact of Sleeve Gastrectomy
Modern weight-loss surgeries intentionally alter gastric wall histology to force a reduction in caloric intake. The vertical sleeve gastrectomy is currently the most popular bariatric procedure. However, it drastically changes the stomach’s mechanical capabilities.
During a sleeve gastrectomy, the surgeon removes up to 80 percent of the stomach, including the majority of the fundus and the greater curvature. This directly excises a massive volume of oblique muscle fibers.
The result is that the stomach can no longer perform effective trituration. Post-operative patients must chew food extremely thoroughly before swallowing. Swallowing a large chunk of meat with a surgically reduced stomach often leads to painful blockages, because the remaining organ lacks the muscular power to grind it down.
Functional Dyspepsia and Motility Disorders
Functional dyspepsia is characterized by chronic indigestion without an obvious structural cause. Recent studies point to subtle failures in the visceral smooth muscle as a frequent culprit. Specifically, many of these patients suffer from impaired gastric accommodation.
When the oblique fibers in the fundus fail to relax during a meal, the stomach cannot expand. This causes an immediate, painful spike in intragastric pressure. Patients experience severe bloating and early satiety after just a few bites of food.
Research increasingly links functional dyspepsia to this specific loss of fundic compliance. The oblique muscle layer simply refuses to yield to incoming food, turning every meal into a distressing experience.
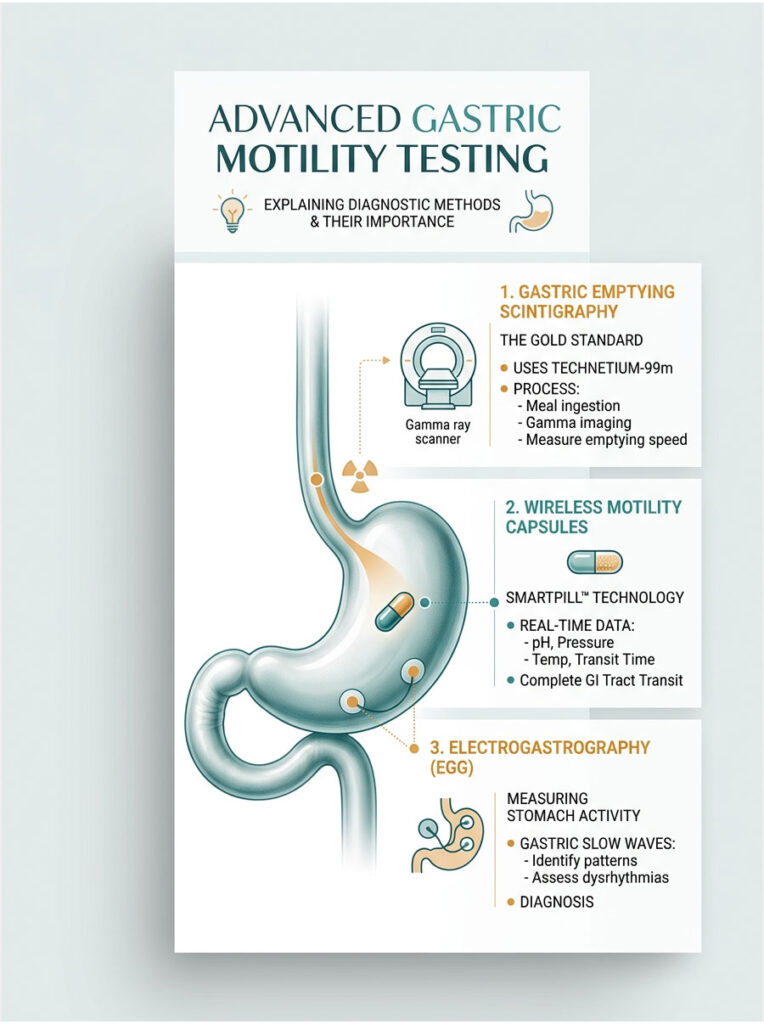
Advanced Diagnostic Testing for Gastric Motility
The field of neurogastroenterology is advancing rapidly. For decades, clinicians relied on crude barium swallows to assess general stomach function. Today, advanced diagnostic tools allow us to measure the exact performance of the muscularis externa in real time.
Accurate testing is the foundation of effective treatment. Treating motility disorders requires pinpoint accuracy. You cannot simply prescribe an antacid for a complex muscle problem. You must address the electromechanical failure directly, and that requires knowing exactly where the breakdown occurs.
Gastric Emptying Scintigraphy
The gold standard for evaluating stomach function is gastric emptying scintigraphy. The patient eats a standardized meal tagged with a small amount of radioactive material, typically technetium-99m sulfur colloid mixed into scrambled eggs.
A gamma camera then tracks the radioactive food over four hours. It monitors how quickly the stomach grinds food into chyme and pushes it through the pyloric sphincter. Clinicians look for specific retention percentages at the one-hour, two-hour, and four-hour marks.
If more than 10 percent of the meal remains after four hours, gastroparesis is confirmed. This delayed emptying time proves that the oblique muscle layer is failing to perform its mechanical duties.
Wireless Motility Capsules and SmartPill Technology
Another major advancement is the wireless motility capsule, commonly known as the SmartPill. The patient swallows this small electronic device in the clinic. As it travels through the gut, it continuously measures pressure, pH, and temperature.
The SmartPill provides a real-time readout of how forcefully the inner oblique layer is contracting. It measures the exact amplitude of the peristaltic waves sweeping across the stomach. This data transmits wirelessly to a receiver worn by the patient.
If the SmartPill shows weak pressure readings in the stomach but normal readings in the intestines, it pinpoints exactly where the mechanical failure lies.
Electrogastrography (EGG) and Waveform Analysis
To evaluate the stomach’s electrical pacemaker system, clinicians use electrogastrography, or EGG. This test is similar to an EKG performed on the heart. Small, non-invasive electrodes are placed on the patient’s abdomen over the stomach area.
The EGG measures the gastric slow waves generated by the Interstitial cells of Cajal. A healthy stomach shows a consistent baseline rhythm peaking at precisely 3 cycles per minute. During active digestion, this rhythm spikes into taller action potentials.
If the EGG shows bradygastria (too slow) or tachygastria (too fast), it indicates severe electromechanical uncoupling. The electrical signals are misfiring, meaning the oblique muscle layer receives chaotic commands. This often explains why a patient experiences severe nausea despite having normal anatomy on endoscopy.
Pharmacological and Dietary Interventions
When the stomach muscles are paralyzed or uncoordinated, aggressive intervention is needed. Treatment involves a combination of prokinetic medications, dietary modifications, and sometimes surgical devices. The goal is either to stimulate the oblique muscle layer or to bypass the need for heavy mechanical grinding.
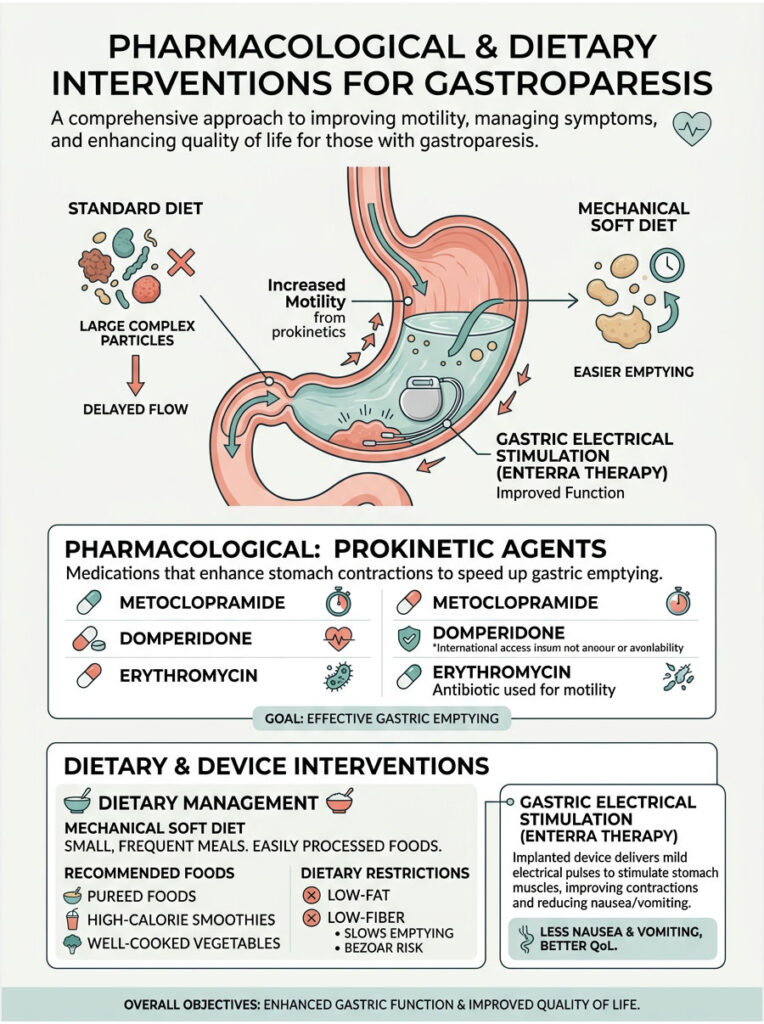
Prokinetic Agents Targeting Smooth Muscle
Prokinetic agents are medications designed to stimulate gastrointestinal motility. They work by forcing the enteric nervous system to fire more frequently, which jumpstarts the muscle layers and forces them to contract.
Drugs like metoclopramide and domperidone target specific dopamine and serotonin receptors within Auerbach’s plexus. By blocking inhibitory dopamine signals, they encourage the inner oblique layer to resume aggressive churning. However, these drugs require close monitoring due to potential neurological side effects.
Another pharmacological approach involves erythromycin. While primarily known as an antibiotic, erythromycin mimics motilin, a naturally occurring gastrointestinal hormone. In low doses, it binds directly to receptors on the smooth muscle, triggering powerful, sweeping contractions that clear the stomach.
Gastric Electrical Stimulation Devices
When medications fail to stimulate the oblique muscle layer, a gastric pacemaker can be implanted. The Enterra Therapy system is a surgically implanted device used for refractory gastroparesis. It consists of a battery pack placed under the skin of the abdomen.
Surgeons implant two small electrical leads directly into the muscularis externa. These leads deliver high-frequency, low-energy electrical pulses to the muscle tissue. While this does not cure the underlying nerve damage, it significantly reduces nausea.
The exact mechanism is still being studied. However, patients report a major improvement in quality of life. The device appears to override chaotic electrical signals in the gut, providing a stabilizing effect on the stomach’s sensory nerves.
Dietary Management for Compromised Trituration
When medical therapies fall short, dietary modification is the single most effective intervention. If a patient’s stomach cannot perform trituration, the work must be done before the food is swallowed.
Clinicians recommend strict mechanical soft diets for patients with compromised oblique muscle function. This includes pureed foods, high-calorie smoothies, and thoroughly cooked vegetables. By replicating the stomach’s churning process with a blender, you completely bypass the need for heavy gastric grinding.
Patients must also adopt a low-fat and low-fiber diet. Fat naturally slows gastric emptying, while raw fiber demands massive mechanical force to break down. Removing these difficult macronutrients gives the weakened stomach a much better chance of emptying successfully.
Case Studies: Real Clinical Data on the Oblique Muscle Layer
Theoretical knowledge is valuable, but real-world application is where clinical expertise truly lives. Observing how the human body adapts to anatomical changes offers powerful insight into gastric physiology.
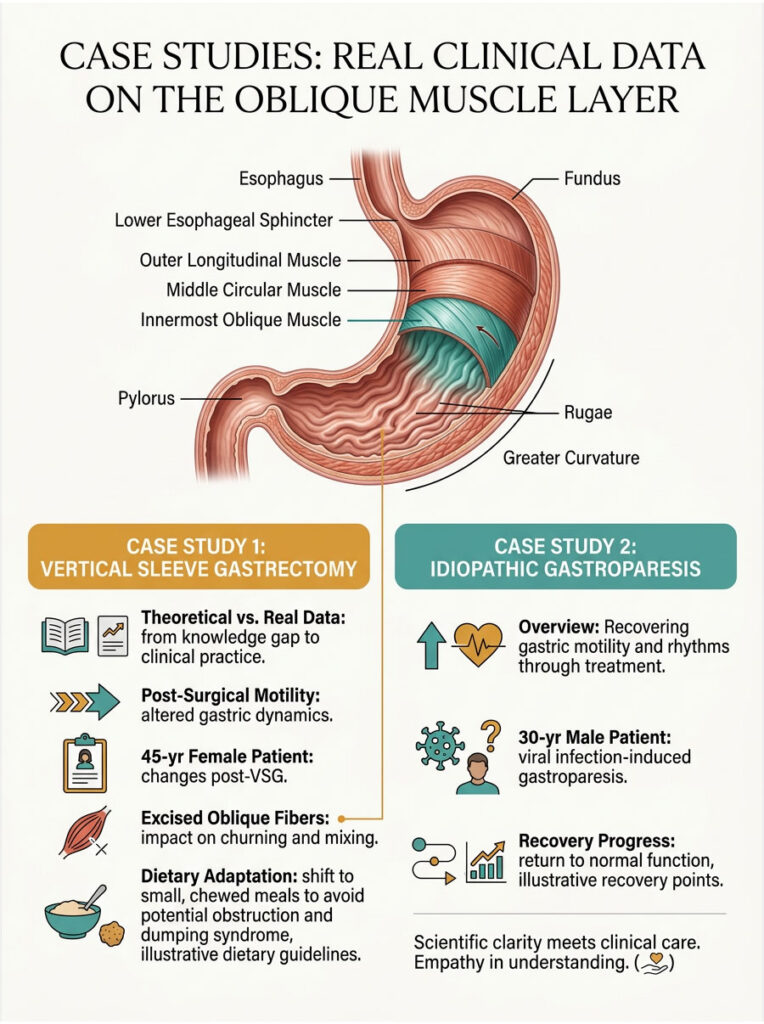
Post-Surgical Motility Changes
Consider a 45-year-old female undergoing a vertical sleeve gastrectomy for severe obesity. Pre-operatively, her gastric emptying scintigraphy showed a perfectly normal half-time of 90 minutes. Her stomach easily accommodated large meals, and her bolus-to-chyme conversion was efficient.
During surgery, the surgeon removed the vast majority of the fundus and greater curvature. This excised the bulk of her oblique muscle fibers, turning her stomach into a narrow tube. Post-operatively, her motility dynamics changed drastically.
Without the muscular power for proper trituration, her GI tract had to compensate. She experienced rapid emptying of liquids but severe delayed emptying of heavy solids. She transitioned to eating six tiny, highly chewed meals a day to prevent painful obstructions.
Idiopathic Gastroparesis Recovery
In another scenario, a 30-year-old male presented with severe, sudden-onset idiopathic gastroparesis following a viral infection. His SmartPill test showed almost zero contractile pressure in the gastric body. The viral infection had temporarily paralyzed his myenteric plexus.
Because his oblique muscle layer was intact but neurologically stunned, treatment focused on temporary support. He was placed on a strict liquid diet and prescribed a short course of liquid erythromycin. This combination bypassed the need for mechanical grinding while artificially stimulating the muscle.
Over six months, his enteric nervous system slowly healed. Follow-up EGG testing confirmed a return of the normal 3-cycle-per-minute pacemaker rhythm. His oblique muscle layer gradually resumed normal churning, proving that visceral smooth muscle can recover when the underlying nerve damage resolves.
Summary and Key Takeaways
The stomach is a biological marvel built to withstand extreme chemical environments and exert massive physical force. At the core of this capability is the oblique muscle layer. By adding a third, diagonal dimension to the standard gastrointestinal blueprint, the stomach transforms from a simple transit tube into a powerful mechanical grinder.
The unique three-layer architecture of the muscularis externa ensures that solid food is churned and reduced to a liquid state. The innermost oblique layer is the engine of mechanical digestion and trituration. Without it, the pyloric sphincter would remain closed, and digestion of solid meals would fail entirely.
Understanding this specific gastric wall histology is not just an academic exercise. It is vital for diagnosing and treating complex motility disorders. Whether you are managing gastroparesis, functional dyspepsia, or post-bariatric complications, recognizing the mechanics of the oblique muscle layer is the key to restoring patient health.
Frequently Asked Questions
What is the oblique muscle layer of the stomach?
The oblique muscle layer is the innermost third layer of the muscularis externa, found exclusively in the human stomach. Unlike the rest of the gastrointestinal tract, which operates on a two-layer system (inner circular and outer longitudinal), the stomach adds this diagonal layer to enable multi-directional churning. It is most concentrated in the gastric fundus and body, and it is the primary reason the stomach can mechanically grind solid food into a semi-liquid state called chyme.
Why does only the stomach have three muscle layers?
During embryological development, specific genetic signals unique to the gastric region trigger the formation of the oblique layer. These genetic markers are not present in the esophagus, small intestine, or large intestine. The stomach needs this third layer because it must perform heavy mechanical grinding (trituration) on solid food, a task that simple two-layer peristalsis cannot accomplish. This makes the stomach a true anatomical outlier in the digestive system.
Where exactly is the oblique muscle layer located within the stomach?
The oblique fibers originate near the cardiac notch, the sharp angle where the esophagus meets the greater curvature of the stomach. From there, the fibers fan out across the fundus and the upper body. As you move toward the lower antrum, the oblique layer gradually thins out and largely disappears. The lower stomach relies on the thickened circular layer, which forms the pyloric sphincter.
What is trituration and why does it matter?
Trituration is the clinical term for the vigorous, multi-directional churning that reduces solid food into a semi-liquid state inside the stomach. It is just as important as the chemical breakdown by stomach acid and enzymes. Without trituration, food particles would remain too large to pass through the pyloric sphincter (which requires particles smaller than 2 millimeters), leading to intestinal blockages and severe digestive failure.
What happens when the oblique muscle layer stops working?
When the oblique layer fails, the stomach loses its ability to grind solid food. This leads to conditions like gastroparesis, where food sits undigested in the stomach for hours, causing severe nausea, vomiting, bloating, and early satiety. The pyloric sphincter refuses to open because the food particles are still too large. In essence, the stomach transforms from a dynamic processing organ into a stagnant holding pouch.
How does diabetes affect the oblique muscle layer?
Diabetes is the most common known cause of gastroparesis. Chronic high blood sugar causes oxidative stress and microvascular damage to the vagus nerve, which controls stomach muscle contractions. Over time, this nerve damage leads to depletion of the Interstitial cells of Cajal (the stomach’s pacemaker cells), loss of the 3-cycle-per-minute electrical rhythm, and eventual atrophy of the smooth muscle itself. This makes the oblique layer progressively weaker and less coordinated.
Does bariatric sleeve gastrectomy remove the oblique muscle layer?
Yes, significantly. During a vertical sleeve gastrectomy, surgeons remove up to 80 percent of the stomach, including most of the fundus and greater curvature where the oblique fibers are most concentrated. This drastically reduces the stomach’s capacity for mechanical grinding. Post-operative patients must chew food extremely thoroughly and follow a modified diet to compensate for the lost muscular power.
What is the role of Interstitial cells of Cajal in the oblique muscle layer?
The Interstitial cells of Cajal (ICC) act as the stomach’s biological pacemakers. They generate spontaneous slow-wave electrical impulses at a rate of 3 cycles per minute. These impulses propagate through all three muscle layers, including the oblique layer, setting the rhythm for coordinated contractions. When the ICCs are damaged or depleted, the oblique fibers lose their timing and the stomach’s grinding action becomes chaotic or stops entirely.
How is oblique muscle layer dysfunction diagnosed?
Clinicians use several advanced tests to evaluate the oblique layer’s performance. Gastric emptying scintigraphy is the gold standard, tracking how quickly the stomach processes a radioactive-tagged meal over four hours. The wireless motility capsule (SmartPill) measures real-time pressure inside the stomach. Electrogastrography (EGG) evaluates the electrical pacemaker rhythm generated by the ICCs. Together, these tools pinpoint exactly where and how the mechanical system is failing.
Can the oblique muscle layer recover after damage?
In some cases, yes. If the underlying cause is temporary, such as a viral infection that stuns the myenteric plexus, the oblique layer can gradually regain normal function as the nerve supply heals. Clinical cases have shown full recovery of the 3-cycle-per-minute pacemaker rhythm and normal churning over a period of several months. However, if the damage is permanent, such as from advanced diabetic neuropathy or surgical removal, the lost function does not return, and patients require lifelong dietary and medical management.
Medical Disclaimer
The information presented in this article is intended for educational and informational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of a qualified healthcare provider with any questions you may have regarding a medical condition or treatment plan.
This article does not establish a doctor-patient relationship between the reader and the author. The clinical data, case studies, and treatment protocols discussed are based on generally accepted medical literature and are meant to provide a broad understanding of gastric anatomy and motility. Individual patient outcomes may vary significantly based on personal health history, underlying conditions, and other factors.
Never disregard professional medical advice or delay seeking treatment because of something you have read in this article. If you suspect you have a gastrointestinal motility disorder such as gastroparesis or functional dyspepsia, consult a board-certified gastroenterologist for proper evaluation and personalized care.
The authors and publishers of this content assume no liability for any injury, loss, or damage resulting from the use or misuse of the information provided. Medication names, dosages, and treatment devices mentioned are for informational context only and should not be interpreted as prescriptions or endorsements.
All efforts have been made to ensure the accuracy of the information at the time of publication. However, medical science evolves continuously, and some details may become outdated as new research emerges. Readers are encouraged to verify clinical information with current peer-reviewed sources and consult their healthcare team before making any medical decisions.
References and Recommended Reading
- Standring S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. Elsevier; 2020. Chapters on abdominal viscera and gastric musculature.
- Hall JE, Hall ME. Guyton and Hall Textbook of Medical Physiology. 14th ed. Elsevier; 2021. Sections on gastrointestinal motility and smooth muscle physiology.
- Barrett KE, Barman SM, Brooks HL, Yuan JX. Ganong’s Review of Medical Physiology. 26th ed. McGraw-Hill Education; 2019. Chapter on gastrointestinal motility.
- Huizinga JD, Lammers WJ. Gut peristalsis is governed by a multitude of cooperating mechanisms. American Journal of Physiology-Gastrointestinal and Liver Physiology. 2009;296(1):G1-G8.
- Camilleri M, Parkman HP, Shafi MA, Abell TL, Gerson L. Clinical guideline: management of gastroparesis. American Journal of Gastroenterology. 2013;108(1):18-37.
- Farrugia G. Interstitial cells of Cajal in health and disease. Neurogastroenterology and Motility. 2008;20(Suppl 1):54-63.
- Tack J, Talley NJ, Camilleri M, et al. Functional gastroduodenal disorders. Gastroenterology. 2006;130(5):1466-1479.
- Rao SS, Camilleri M, Hasler WL, et al. Evaluation of gastrointestinal transit in clinical practice: position paper of the American and European Neurogastroenterology and Motility Societies. Neurogastroenterology and Motility. 2011;23(1):8-23.
- Abell TL, Camilleri M, Donohoe K, et al. Consensus recommendations for gastric emptying scintigraphy: a joint report of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine. American Journal of Gastroenterology. 2008;103(3):753-763.
- Kuo B, McCallum RW, Koch KL, et al. Comparison of gastric emptying of a nondigestible capsule to a radio-labelled meal in healthy and gastroparetic subjects. Alimentary Pharmacology and Therapeutics. 2008;27(2):186-196.
- Sanders KM, Koh SD, Ward SM. Interstitial cells of Cajal as pacemakers in the gastrointestinal tract. Annual Review of Physiology. 2006;68:307-343.
- Grover M, Farrugia G, Lurken MS, et al. Cellular changes in diabetic and idiopathic gastroparesis. Gastroenterology. 2011;140(5):1575-1585.
- Himpens J, Dobbeleir J, Peeters G. Long-term results of laparoscopic sleeve gastrectomy for obesity. Annals of Surgery. 2010;252(2):319-324.
- Tack J, Piessevaux H, Coulie B, Caenepeel P, Janssens J. Role of impaired gastric accommodation to a meal in functional dyspepsia. Gastroenterology. 1998;115(6):1346-1352.
- Sadler TW. Langman’s Medical Embryology. 14th ed. Wolters Kluwer; 2019. Sections on gut tube development and gastric differentiation.
- American Gastroenterological Association. AGA Technical Review on the Diagnosis and Treatment of Gastroparesis. Gastroenterology. 2004;127(5):1592-1622.
- Parkman HP, Hasler WL, Fisher RS. American Gastroenterological Association medical position statement: diagnosis and treatment of gastroparesis. Gastroenterology. 2004;127(5):1589-1591.
- Koch KL. Gastric dysrhythmias: a potential objective measure of nausea. Experimental Brain Research. 2014;232(8):2553-2561.





