As a board-certified pediatrician with more than 15 years of neonatal experience, one of the questions I hear most from anxious parents is simple but loaded: what does diarrhea look like in newborns? It is completely understandable to feel overwhelmed trying to decode every diaper change. A baby’s gut health is one of the clearest windows into their overall well-being, and learning to tell normal infant digestion apart from true clinical diarrhea is your first line of defense against dehydration.
Table of Contents
Spotting these early warning signs can protect your child from serious complications. Newborns have incredibly sensitive digestive tracts that respond fast to changes in diet, environment, or illness. You will quickly notice that infant stool changes almost daily during the first few weeks. Let me walk you through exactly how to monitor these changes safely at home and know when it is time to call the doctor.
Quick Answer: What Does Diarrhea Look Like in Newborns?
Newborn diarrhea shows up as a sudden shift to purely liquid, watery stools that soak completely into the diaper. Unlike normal loose baby poop, clinical diarrhea leaves a clear “ring of water” or damp halo around the solid matter. It usually happens far more often than the baby’s normal pattern and may explode forcefully out of the body. If you spot these signs, especially alongside a fever or poor feeding, contact your pediatrician right away.
Why does this distinction matter so much? It comes down to fluid loss and how quickly a small infant can become medically compromised. A newborn’s body is mostly water, which makes them highly vulnerable to rapid dehydration. Let’s look at the data behind this.
Key Statistics on Neonatal Gastrointestinal Health
- Prevalence: According to the CDC, acute gastroenteritis affects over 3 million infants each year.
- Rotavirus impact: Before the vaccine launched in 2006, rotavirus caused over 400,000 doctor visits for U.S. infants annually.
- Dehydration timeline: Infants under three months can reach critical dehydration within just 12 to 24 hours of diarrhea onset.
- Normal frequency: The American Academy of Pediatrics notes that breastfed newborns can have up to 12 normal bowel movements a day.
- Allergy rates: Cow’s Milk Protein Allergy (CMPA) affects about 2% to 3% of all infants globally.
- Hospitalization drops: Routine vaccinations have cut infant hospitalizations for severe diarrhea by over 80% in the last two decades.
- Water content: A healthy newborn’s body is roughly 75% water, compared to 60% in adults.
How the Newborn Digestive System Actually Works
Before we get into diagnosing sick diapers, you need to understand how a baby’s gut actually functions. The neonatal digestive system is not just a smaller version of an adult’s. It is still developing, highly permeable, and learning to process nutrients for the very first time. That immaturity is exactly why newborns have so many digestive quirks.
When your baby is born, their intestinal lining is incredibly porous. This “open gut” lets beneficial antibodies from breast milk pass straight into the bloodstream. The downside is that the same permeability also lets in irritating proteins and pathogens. Over the first six months, the gut lining gradually closes and strengthens.
Newborns also lack the diverse microbiome that older children have. They are born with a nearly sterile gut that slowly populates with bacteria through feeding and environmental exposure. This delicate bacterial balance is easy to throw off. When the flora gets disrupted, digestion speeds up, and stools turn loose and watery.
The Role of Gastric Emptying
Gastric emptying is how fast food leaves the stomach and enters the intestines. In newborns, this process is remarkably quick. Breast milk digests in about 90 minutes, and formula takes a little longer. This rapid transit naturally produces softer, more frequent stools.
When a virus or allergy irritates the stomach, gastric emptying speeds up even more. The intestines simply do not have time to absorb water from the digested milk. The result is purely liquid output that bypasses normal absorption.
The Gastrocolic Reflex
Ever noticed your baby pooping mid-feeding? That is the gastrocolic reflex at work. When a newborn’s stomach stretches with incoming milk, it sends a strong nerve signal to the colon. The colon contracts to make room for the new meal.
This reflex is especially powerful during the first three months. Pooping after every feeding is actually a sign of a healthy, active nervous system. It does not automatically mean your baby has diarrhea.
What “Normal” Newborn Stool Actually Looks Like
You cannot tell baby diarrhea from normal stool if you do not know what a healthy diaper looks like in the first place. Newborn poop changes dramatically over the first weeks of life. Knowing this progression helps parents skip the late-night panic searches.

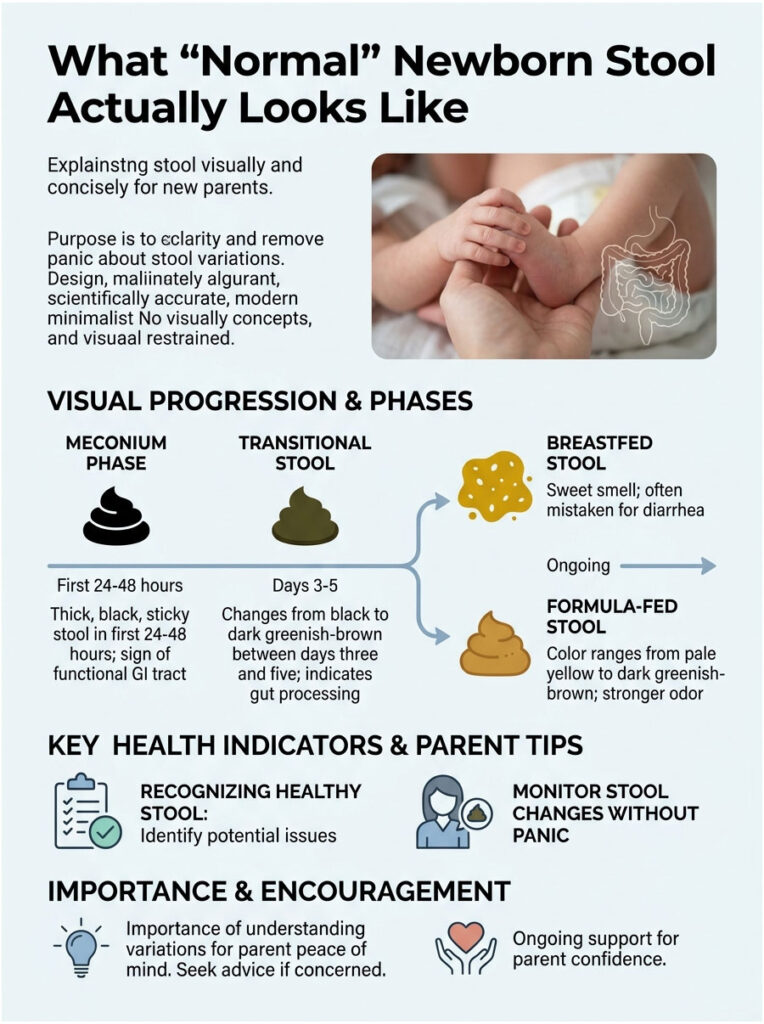
The Meconium Phase
During the first 24 to 48 hours, your baby will pass meconium. This stuff is thick, black, and incredibly sticky, almost like roofing tar or motor oil. Meconium is not made of digested milk. It contains everything the baby ingested in the womb, including amniotic fluid, skin cells, and fine body hair called lanugo.
Passing meconium is a big positive sign for your pediatrician. It proves the baby’s lower GI tract is open, connected, and working properly.
Transitional Stool
Between days three and five, the baby’s gut starts processing early breast milk or formula. The stool enters a transitional phase. The color shifts from black to dark greenish-brown, and the texture becomes less sticky and noticeably looser. This early loosening is normal. It just means the gut is clearing the last of the meconium and waking up.
Breastfed Stool Characteristics
Once mature breast milk comes in, the baby’s diet drives diaper contents. Breastfed stool is typically bright mustard-yellow, loose, runny, and full of small white flecks that look like sesame seeds. That seedy texture is the hallmark of healthy breast milk digestion.
The smell is distinct too, often described as sweet, popcorn-like, or yeasty. Because it is naturally so runny, parents frequently mistake healthy breastfed poop for diarrhea.
Formula-Fed Stool Characteristics
Formula-fed babies produce slightly firmer stool that often looks like peanut butter, hummus, or thick paste. The color ranges from pale yellow to tan or dark greenish-brown. The smell is generally stronger and more pungent than breastfed stool. Formula takes longer to digest, so these babies usually poop less often.
Knowing these healthy textures is essential before you can spot real warning signs.
What Does Diarrhea Look Like in Newborns? The Core Signs
Here is the tricky part. Because normal infant stool is already so soft, identifying a real medical problem can be hard for tired parents. So what does diarrhea actually look like in newborns? In clinical practice, we look for very specific changes in appearance and texture.
True diarrhea is a sudden, significant departure from your baby’s normal baseline. It involves dramatic shifts in water content, frequency, and how forcefully it comes out. Here is what to look for at the changing table.
The “Ring of Water” Test
The single best at-home diagnostic tool is the ring of water test. Normal newborn stool, even when runny, has enough substance to sit on top of the diaper’s inner lining. Diarrhea has no such substance.
Because diarrhea is purely liquid, the water separates rapidly from the solid particles. That liquid soaks deep into the diaper fabric almost instantly, leaving a visible damp halo spreading outward from the stool. If you keep seeing that halo, the test is positive. It means the intestines are failing to absorb fluid properly.
Texture and Consistency Changes
When checking for diarrhea, focus on consistency more than color. Clinical diarrhea loses the normal seedy or pasty texture you are used to seeing. It becomes entirely watery, stringy, or frothy.
You may also notice a sudden jump in mucus. Mucus in stool looks slimy, shiny, or jelly-like. A tiny bit is normal, but large strings suggest active inflammation in the gut lining.
Explosive Bowel Movements
Newborns are famous for grunting, straining, and turning red while pooping. That effort is normal because they are still learning to coordinate their abdominal muscles. Diarrhea, though, is often forceful, sudden, and explosive. It may shoot out with excess gas, sounding loud and sputtering. Sometimes the stool escapes the diaper entirely, creating the legendary “blowout” up the back.
Watching for Frequency Spikes
Comparing baby diarrhea to normal stool always means looking at your child’s specific patterns. Frequency is relative. If a baby who normally has three dirty diapers a day suddenly has eight liquid ones, that is a major red flag. On the other hand, a breastfed baby who normally poops eight times a day is fine, as long as the texture stays seedy. It is the sudden change in pattern that warrants medical attention.
| Characteristic | Normal Newborn Stool | Clinical Newborn Diarrhea |
|---|---|---|
| Diaper Absorption | Sits mostly on top of the diaper | Soaks rapidly into the diaper core |
| Water Ring | No wet halo | Distinct damp halo (positive test) |
| Texture | Seedy, pasty, slightly curd-like | Purely liquid, watery, slimy, frothy |
| Mucus | Rarely visible | Often contains strings of mucus |
| Frequency | Predictable daily pattern | Sudden, drastic increase |
| Expulsion | Mild grunting and effort | Often explosive and forceful |
Stool Colors: A Pediatrician’s Guide
Parents spend enormous amounts of time analyzing poop color. While consistency is the main indicator of diarrhea, color gives excellent secondary clues about gut health. Different colors tell us how fast food is moving through the digestive tract.
Bile is a digestive fluid produced by the liver that starts out bright green. As it mixes with food and travels through the intestines, it turns yellow and then brown.
What Green Stool Means
Green watery poop in breastfed babies is one of the most common things I see in clinic. When stool moves through the intestines too quickly, the green bile does not have time to break down. It exits the body still bright green. This rapid transit is a sign of intestinal irritation, often from a mild stomach bug, food sensitivity, or foremilk imbalance. Green stool alone is not dangerous, but watery green stool is worth watching closely.
Yellow and Brown
Yellow is the gold standard for breastfed babies. It signals perfect digestion and ideal transit time. Brown or tan is the standard for formula-fed infants, reflecting added iron and different protein structures.
If a baby with diarrhea produces yellow or brown watery stool, it usually points to a viral cause. The body is flushing out the virus, but bile is still breaking down normally. The focus shifts to keeping the baby hydrated until the virus passes.
Warning Colors: Red, Black, and White
Some colors require immediate medical attention.
- Red streaks mean active bleeding in the lower GI tract, often from severe milk protein allergies.
- Black stool (after meconium has cleared) means digested blood from higher up in the stomach.
- White or chalky gray stool is rare but critical. It means the liver is not producing bile, pointing to a serious biliary problem.
If you ever see red, black, or white stool, call your pediatrician right away.
Clinical Causes of Newborn Diarrhea
Knowing what diarrhea looks like is only half the job. You also need to figure out why it is happening. The neonatal gut reacts to a wide range of triggers, and the cause shapes the treatment plan.
Viral Gastroenteritis
Viral infections are the leading cause of acute intestinal trouble in infants. Commonly called the stomach bug, these viruses attack the gut lining and stop the intestines from absorbing water properly. Recognizing rotavirus in infants is especially important during winter months. Symptoms include foul-smelling stool, vomiting, and a low-grade fever. Other common viruses like norovirus and adenovirus look very similar.
Bacterial Infections
Bacterial infections are less common but generally more severe. Bacteria like Salmonella, E. coli, or Campylobacter can enter through contaminated food, water, or unwashed hands. They cause heavy inflammation in the gut lining.
Bacterial diarrhea often comes with higher fevers and visible blood or mucus. Babies with bacterial infections usually look much sicker and more lethargic than those with viral bugs. These cases often need lab testing and sometimes specialized antibiotics.
Cow’s Milk Protein Allergy (CMPA)
Food proteins can really irritate a baby’s gut lining. Cow’s Milk Protein Allergy is a common culprit in the first few months. The infant’s immune system mistakenly identifies dairy proteins as a threat and launches an attack, causing intestinal inflammation.
The result is often bloody or very mucousy diarrhea. Babies with CMPA are usually extremely fussy, have terrible gas, and may develop skin rashes like eczema.
Lactose Overload vs. True Intolerance
Parents often confuse these two. True lactose intolerance is incredibly rare in babies under one year old. Babies are biologically built to produce lactase, the enzyme needed to digest lactose in breast milk.
What is common is lactose overload. It happens when a mother has an oversupply of milk. The baby fills up on watery, high-lactose foremilk and never reaches the fatty hindmilk. That heavy lactose load ferments in the gut, causing severe gas and green watery poop. It looks like diarrhea, but it is really just a temporary digestive overload. Adjusting nursing posture usually resolves it completely.
Antibiotic-Associated Diarrhea
Sometimes the medications meant to heal cause secondary issues. Newborn diarrhea after antibiotics is well documented. Antibiotics do not discriminate between good and bad bacteria. They wipe out the harmful infection but also strip the beneficial bacteria from the developing microbiome. Without healthy flora, stools turn loose and watery. This can happen whether the baby takes antibiotics directly or the nursing mother does.
Expert Insight: If you notice diarrhea after antibiotics, do not stop the medication without talking to your doctor first. Stopping early can let the original infection come back stronger. We often manage this by adjusting the dose or recommending infant-safe probiotics.
How Maternal Diet Affects Breastfed Babies
Breast milk is the perfect food for infants, but it reflects what the mother eats. Trace amounts of dietary proteins pass into breast milk within hours of a meal. For most babies this is harmless and actually helps build immune tolerance. But for babies with sensitive guts, those same trace proteins can trigger diarrhea.
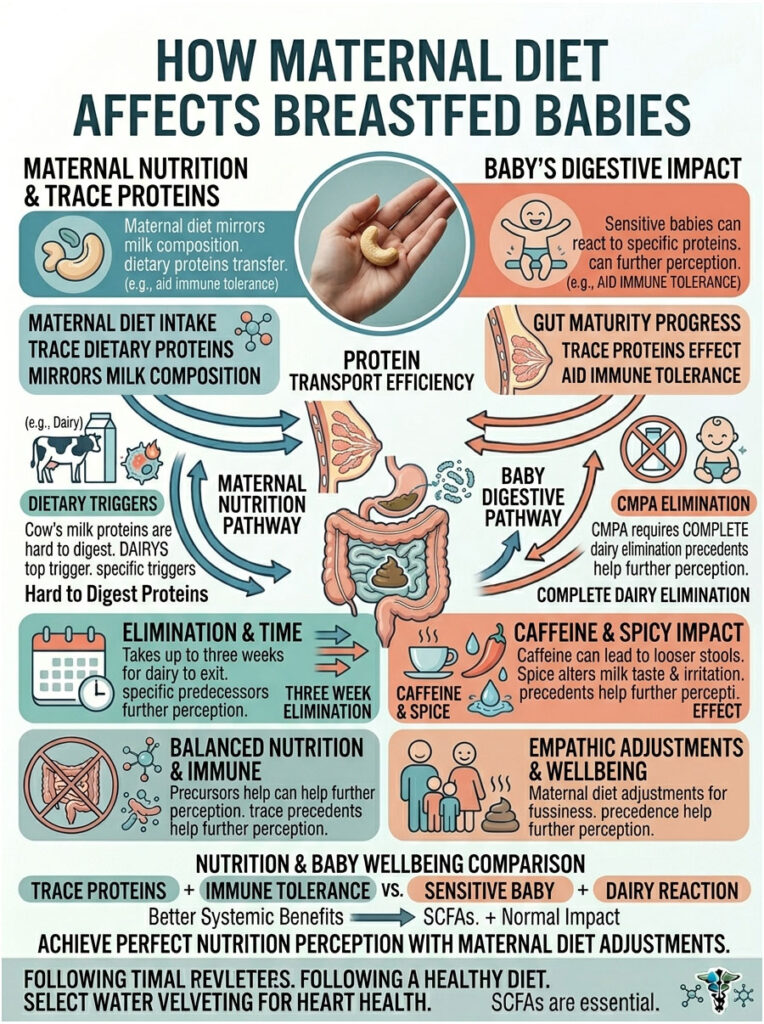
The Dairy Connection
Dairy is the number one dietary trigger for breastfed babies. The proteins in cow’s milk, cheese, and yogurt are large and hard for a newborn to break down. If a baby has CMPA, they will react to maternal dairy intake.
If your pediatrician suspects a dairy allergy, they will ask you to eliminate all dairy from your diet. It can take up to three weeks for dairy proteins to clear your milk completely. Read food labels carefully, since whey and casein hide in many processed foods.
Caffeine and Spicy Foods
Caffeine and spicy foods are less likely to cause true allergic diarrhea, but they can still cause GI upset. High caffeine intake can speed up the baby’s digestive tract, leading to looser stools and a jittery, fussy baby. Spicy foods can occasionally alter milk taste and mildly irritate the baby’s stomach. If you notice a clear pattern between your morning coffee and explosive diapers, try cutting back. Moderation usually keeps the baby’s gut happy.
The Real Danger: Spotting Dehydration in Infants
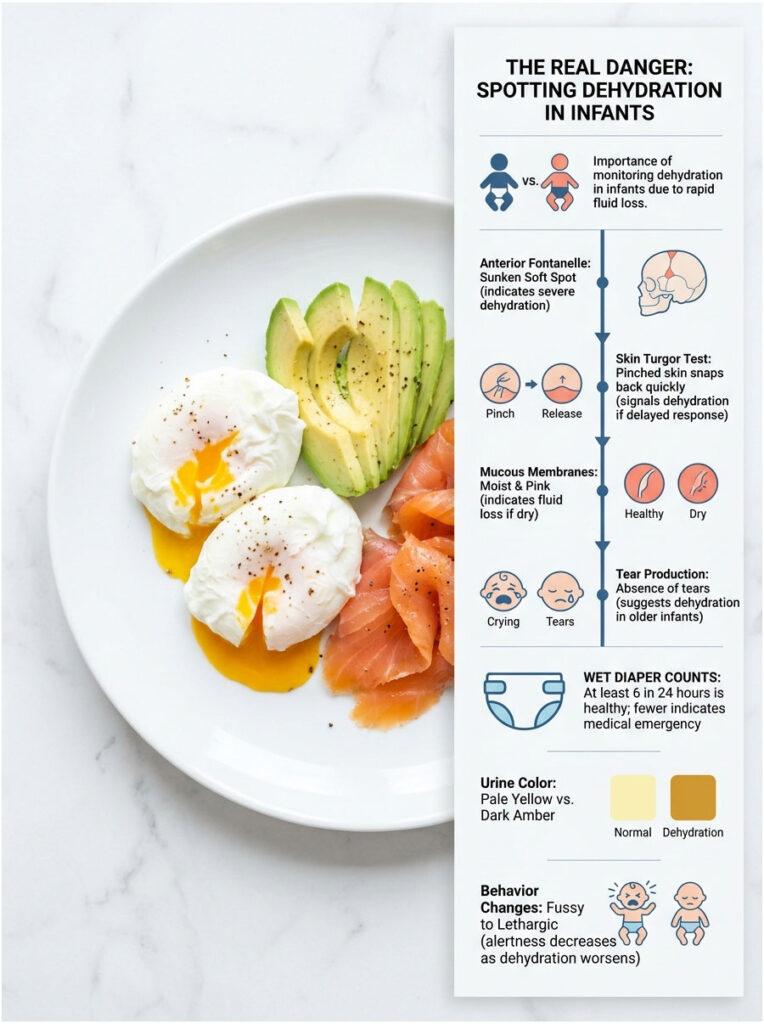
Why do pediatricians take newborn diarrhea so seriously? One word: dehydration. When infants lose fluids fast through the GI tract, their tiny bodies cannot compensate quickly enough. Dehydration can escalate from mild to a medical emergency in just hours. Your job at home is to monitor for specific clinical markers.
Checking the Anterior Fontanelle
The soft spot on top of your baby’s head is called the anterior fontanelle. It is a natural gap between skull bones that have not yet fused. In a well-hydrated baby, this spot feels relatively flat or slightly curved inward.
A sunken soft spot is a major warning sign. When fluid volume drops dangerously low, the fluid around the brain decreases too. The fontanelle dips noticeably, feeling like a shallow bowl or crater. If you see this, seek medical evaluation immediately. Do not wait for your next appointment.
The Skin Turgor Test
Doctors use the skin turgor test to measure skin elasticity, which tracks closely with cellular hydration. It is quick, painless, and easy to do at home.
Gently pinch a small fold of skin on your baby’s bare abdomen and release it immediately. In a healthy infant, the skin snaps right back. In a dehydrated baby, the skin loses its natural elasticity. It may stay “tented” in a pinched shape or take several seconds to fall back. A delayed response means it is time to call the doctor.
Mucous Membranes and Tear Production
Check inside your baby’s mouth with a clean finger. The membranes inside the cheeks should be bright pink, moist, and glistening. Dehydration shows up as dry or cracked lips and a tacky, sticky mouth.
Pay attention to crying habits too. Very young newborns may not produce tears for the first few weeks, but older infants do. An older baby who normally cries with tears but suddenly stops is showing signs of severe fluid loss.
Wet Diaper Counts
Tracking urine output is non-negotiable when dealing with possible diarrhea. A healthy newborn should produce at least six heavily wet diapers in 24 hours. Urine should be pale yellow and mostly odorless.
If your baby goes more than six hours without a wet diaper, the kidneys are conserving water. If urine becomes dark amber and smells strong, it is highly concentrated. Fewer than four wet diapers in 24 hours is a strict medical emergency.
| Clinical Sign | Mild | Moderate | Severe (Emergency) |
|---|---|---|---|
| Anterior Fontanelle | Flat or slightly soft | Noticeably sunken | Deeply sunken, crater-like |
| Skin Turgor | Snaps back instantly | Slightly delayed | Tented for over 2 seconds |
| Mucous Membranes | Moist, pink | Tacky, slightly dry | Dry, parched, cracked lips |
| Urine Output | Normal, pale | 4 to 5 wet diapers/24 hrs | Fewer than 4 wet diapers/24 hrs |
| Behavior | Alert and responsive | Fussy, irritable | Lethargic, floppy, hard to wake |
Practical Strategies and Clinical Management
When you spot the first signs of newborn diarrhea, your instinct may be to panic. Take a breath. With careful observation, mild cases can often be managed at home with proper guidance. The medical goal is simple: replace lost fluids faster than the gut loses them, and support the baby’s body while it heals.
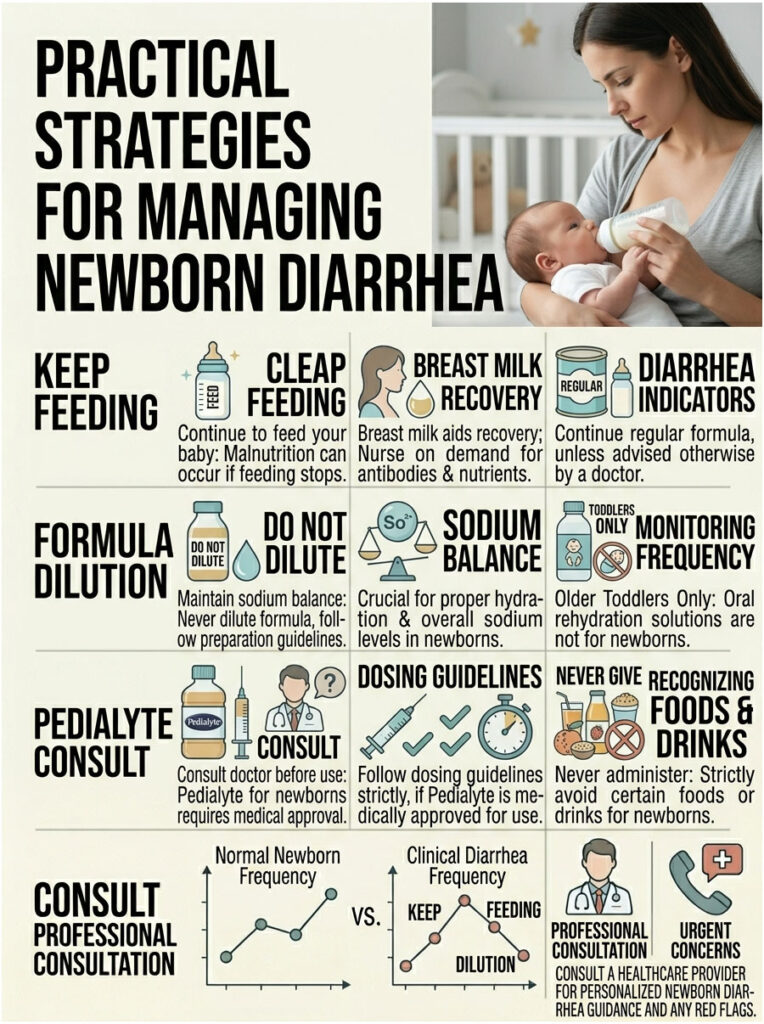
Why You Should Keep Feeding
The single most important step is to keep feeding your baby. Years ago, doctors told parents to withhold food to “rest” the gut. We now know that advice was wrong and led to rapid malnutrition.
If you are breastfeeding, nurse on demand as often as the baby will accept it. Breast milk is therapeutic for a sick gut. It contains antibodies, easily digestible hydration, and natural prebiotics that help repair the intestinal lining. If you are formula feeding, keep offering the regular formula unless your pediatrician suspects an allergy. Do not dilute the formula with extra water, since that disrupts sodium balance. Smaller, more frequent feeds are often easier for a sick baby to tolerate.
Oral Rehydration Solutions and Pedialyte
Parents often ask about Pedialyte and other oral rehydration solutions. These contain a precise mix of water, salts, and sugars designed to maximize cellular absorption. They work great for older toddlers.
But using Pedialyte for a 1-month-old requires strict medical caution. Never give Pedialyte or any ORS to a newborn without direct authorization from your doctor. The electrolyte balance in a neonate is delicate and easily disrupted. If your pediatrician does approve it, they will calculate the dose based on your baby’s weight in kilograms. Follow those measurements exactly.
What You Should Never Give a Newborn
Some rules are non-negotiable when treating infant diarrhea:
- Never give plain water to a baby under six months. It lacks the sodium needed to balance the blood and can cause water intoxication, which can be fatal.
- Never give fruit juice, sports drinks, or sugar water. The high sugar load pulls more water into the intestines and makes diarrhea worse.
- Never give over-the-counter anti-diarrheal medications. These are strictly banned for infants because they can paralyze the bowel.
Managing Diaper Rash from Diarrhea
Frequent watery stools are highly acidic and packed with digestive enzymes. They break down the delicate skin barrier almost instantly. Severe chemical burns and rashes can develop in just hours, so being proactive matters.
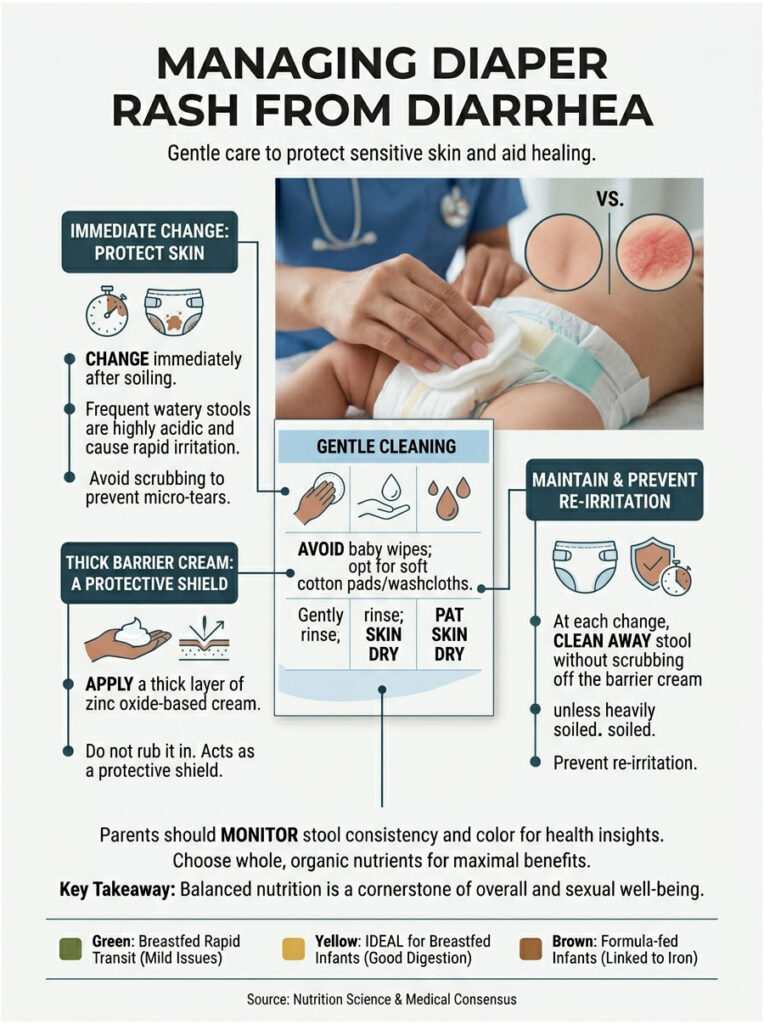
Gentle Cleaning
Change the diaper the moment it gets soiled. Do not let acidic stool sit on the skin. Avoid commercial baby wipes, even those labeled “sensitive,” because they often contain hidden alcohols, preservatives, or fragrances that sting irritated skin.
Use soft cotton pads or a washcloth soaked in warm water. Gently squeeze the water over the area to rinse the stool away. Pat the skin dry with a soft towel. Never scrub, since that creates micro-tears. If the skin is extremely raw, a hairdryer on the cool setting can help dry the area completely.
Applying Barrier Creams
Once the skin is bone dry, apply a thick layer of zinc oxide-based barrier cream. Zinc oxide physically blocks acidic stool from touching the skin and provides anti-inflammatory relief. Think of it like frosting a cake. You want a thick, opaque layer that completely covers the area. Do not rub it in like lotion. It needs to sit on top as a shield.
At the next change, do not scrub the cream off unless it is heavily soiled. Wiping it off removes the healing top layer of skin. Just clean away the stool and apply a fresh layer over the old one.
Real Clinical Scenarios
Let me share a few real-world cases that show why careful observation matters so much.
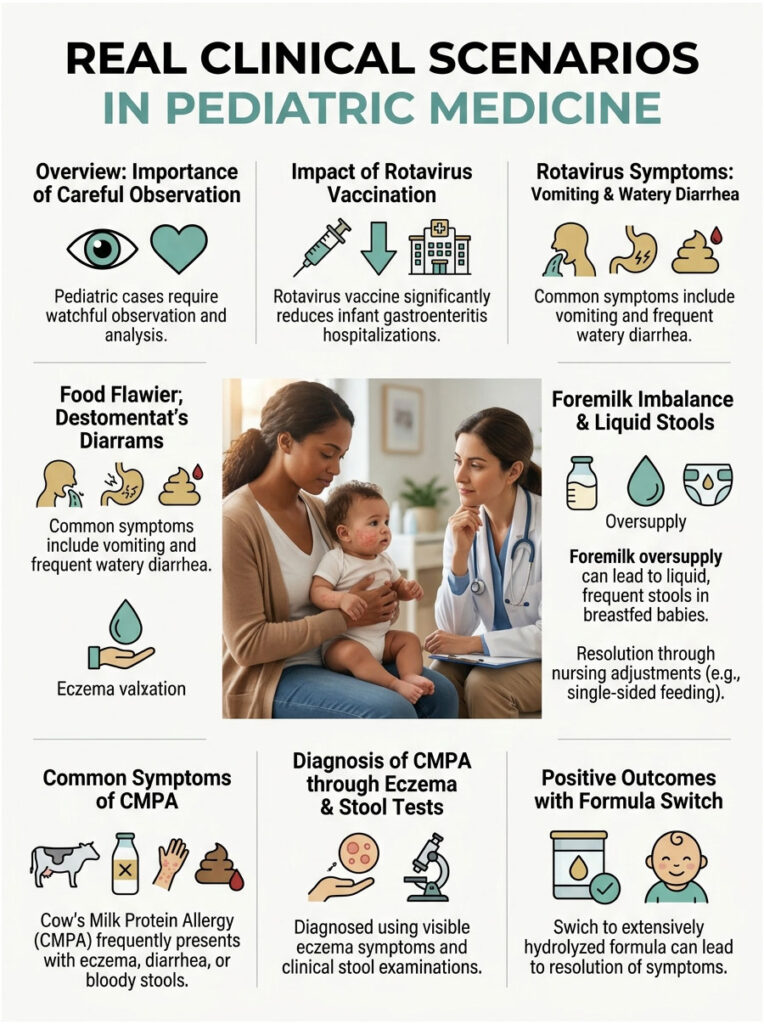
The Power of Rotavirus Vaccination
Picture pediatric medicine before 2006. Hospital wards were filled with infants suffering severe dehydration every winter. The culprit was almost always rotavirus. Symptoms included sudden vomiting followed by explosive, foul-smelling watery diarrhea. Babies deteriorated rapidly and needed IV fluids to survive.
Once the oral rotavirus vaccine joined the standard immunization schedule, things changed dramatically. Hospitalizations for infant gastroenteritis dropped by over 80% nationwide. That data alone shows why preventive care is the most powerful weapon against severe diarrhea.
The Foremilk Imbalance Misdiagnosis
A mother brought in her three-week-old recently, very distressed about the baby’s diapers. She described frequent, explosive, completely liquid stools. The diaper showed classic green watery poop.
Mom assumed it was a virus or that she needed to switch to a hypoallergenic formula. But the baby had no fever and passed the skin turgor test perfectly. After talking through her feeding habits, we figured out she had a massive milk oversupply. The baby was filling up on watery foremilk before reaching the fat-rich hindmilk. By adjusting her nursing posture and letting the baby fully drain one breast, the issue resolved within 48 hours, no medication needed.
A Case of Cow’s Milk Protein Allergy
Another common one: a two-month-old formula-fed baby with chronic loose stools. The parents said the baby was extremely colicky, crying for hours after every bottle. The diapers consistently failed the ring of water test.
During the exam, I noticed severe eczema on the baby’s cheeks and chest. A stool test revealed microscopic blood. Together, these pointed clearly to CMPA. We switched to an extensively hydrolyzed formula, where the milk proteins are pre-broken into fragments the immune system cannot detect. Within a week, the diarrhea stopped, the rash cleared, and the baby was finally sleeping peacefully.
When to Call the Pediatrician Right Away
Some mild loose stools can be handled at home, but other situations demand immediate medical care. Newborns under 28 days old have very immature immune systems and can go from stable to critical fast. When in doubt, always call. Trust your parental instincts.
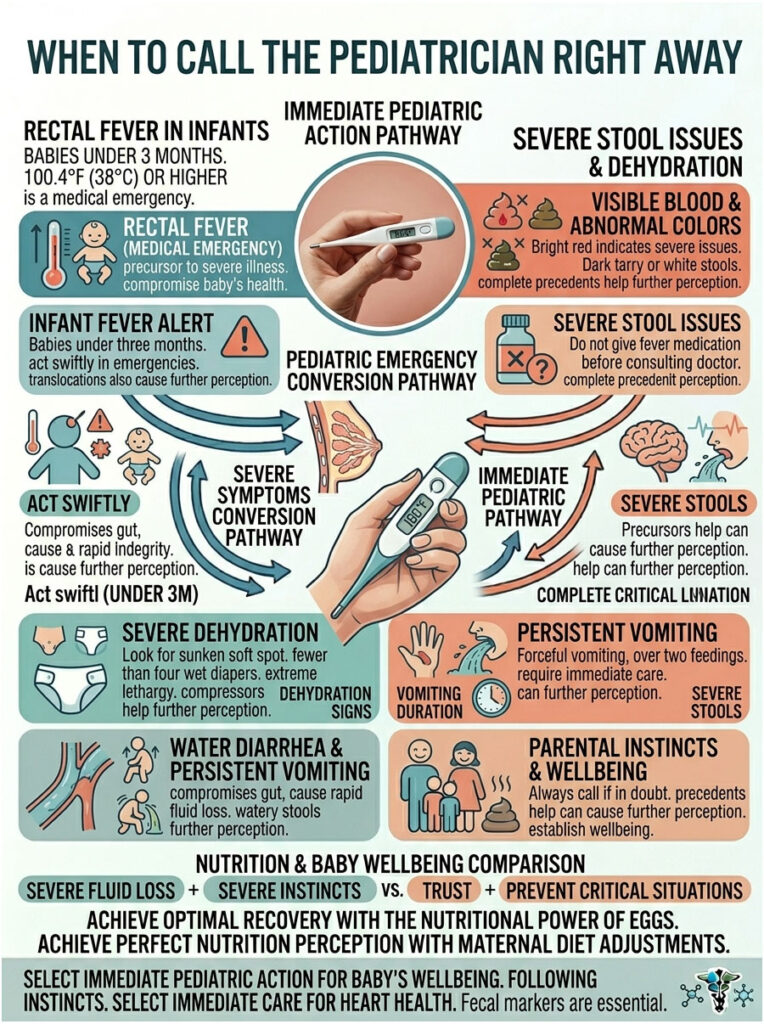
Fever in Infants
Fever is the body’s natural response to infection, but in young infants it is dangerous. A rectal temperature of 100.4°F (38°C) or higher in a baby under three months old is a strict medical emergency, with or without diarrhea.
Do not give Tylenol to a baby under three months to lower a fever before seeing a doctor. Masking the fever can hide a serious bacterial infection. Go straight to the emergency room.
Visible Blood or Abnormal Colors
Stools with bright red streaks indicate severe inflammation, tearing, or an allergic reaction. Dark, tarry stool means bleeding higher up in the digestive tract. Both need immediate testing. White or chalky gray stool indicates a liver or bile duct problem. Do not wait for the next diaper. Call right away.
Severe Dehydration
Act fast if your baby shows late-stage dehydration signs: a sunken soft spot, failed skin turgor, or fewer than four wet diapers in 24 hours. Watch for extreme lethargy too. If your baby is unusually floppy, hard to wake, or too weak to cry normally, they are in real danger. A baby too weak to eat cannot rehydrate themselves and will need IV fluids.
Persistent Vomiting
Spitting up small amounts is normal. Forceful, projectile vomiting is not. If your baby is vomiting forcefully and cannot keep milk or formula down for more than two feedings in a row, dehydration will hit fast. Vomiting plus diarrhea means fluid loss from both ends, which dramatically shortens the safe window. Get medical care to stop the vomiting and restore fluid balance.
Key Takeaways
Decoding diaper contents is a stressful rite of passage for every new parent. Answering the question of what diarrhea looks like in newborns really comes down to careful observation and knowing your baby’s baseline. Frequent, seedy, loose stools are completely normal, especially for breastfed babies.
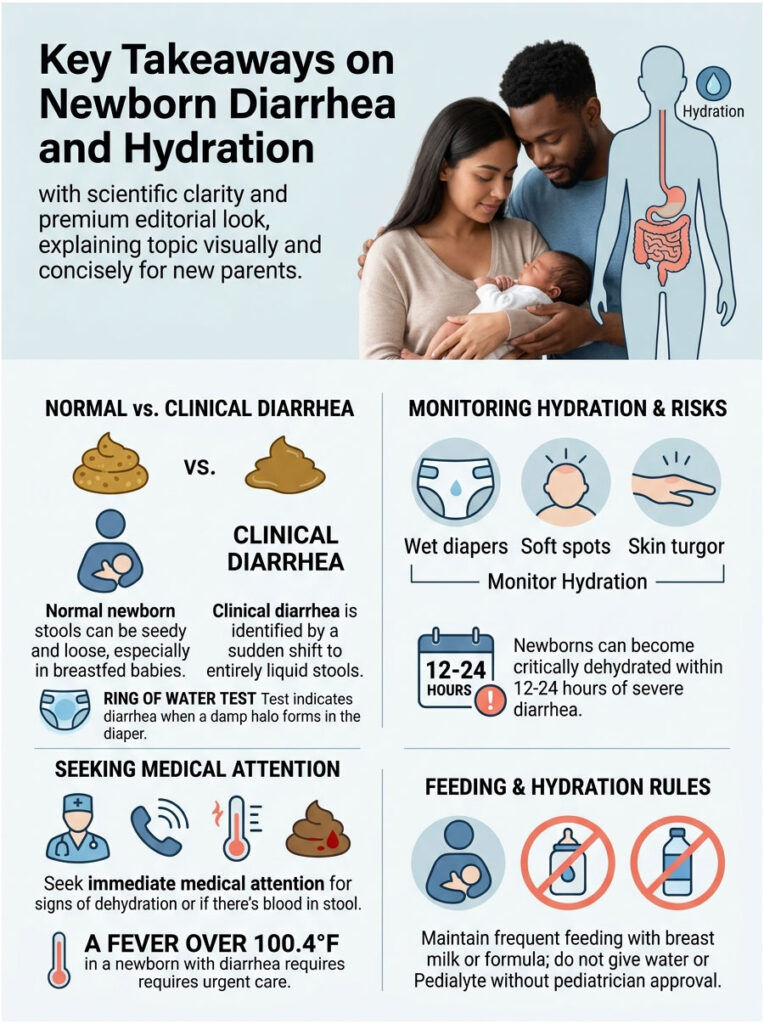
What you are watching for is a sudden, dramatic shift to purely liquid output. The most reliable home test is the ring of water test. If the stool separates and leaves a clear damp halo soaked into the diaper, you are likely dealing with clinical diarrhea.
Always prioritize hydration by offering breast milk or formula on demand. Monitor relentlessly for dehydration by checking the soft spot, doing the skin turgor test, and counting wet diapers. Most importantly, trust your gut. If your baby’s behavior changes or something feels off, your pediatrician is there to help you navigate it safely. You know your baby better than anyone, and acting early is always the right call.
Frequently Asked Questions
How can I tell the difference between normal loose newborn stool and clinical diarrhea?
As a pediatrician, I advise parents to look for a sudden deviation from their baby’s baseline. While breastfed stool is naturally runny and seedy, clinical diarrhea is purely liquid and fails the ‘ring of water’ test, where a damp halo of fluid soaks deeply into the diaper fabric, leaving no solid matter behind. If the stool is explosive, lacks its usual ‘seedy’ texture, and occurs with significantly higher frequency, it is likely diarrhea.
What is the ‘ring of water’ test for infant diarrhea?
The ring of water test is a diagnostic observation where you check the diaper’s inner lining. Normal newborn stool, even when runny, typically sits on top of the fabric. In cases of true diarrhea, the water content separates from the stool particles and absorbs rapidly into the diaper core, creating a visible, wet ring or halo around the solid components. This indicates that the intestines are not properly absorbing fluids.
Is it normal for a breastfed baby to have green, watery bowel movements?
Green watery poop in a breastfed baby is often caused by a ‘foremilk/hindmilk imbalance’ or lactose overload. If a baby receives too much of the watery, high-lactose foremilk and not enough fatty hindmilk, the lactose ferments in the gut, leading to rapid transit and green, gassy stools. However, if the green stool is accompanied by a fever or signs of dehydration, it may indicate a viral infection like rotavirus.
What are the most common clinical causes of diarrhea in newborns?
The most frequent triggers include viral gastroenteritis (such as rotavirus or norovirus), bacterial infections from contaminated sources, and Cow’s Milk Protein Allergy (CMPA). Additionally, we often see antibiotic-associated diarrhea, which occurs when medications disrupt the baby’s developing microbiome, or mechanical issues like lactose overload due to oversupply during breastfeeding.
How quickly can a newborn become dehydrated from diarrhea?
Because a newborn’s body weight is composed of approximately 75% water, they are exceptionally vulnerable to fluid loss. An infant under three months old can reach critical, life-threatening dehydration levels within just 12 to 24 hours of the onset of severe diarrhea. This is why monitoring urine output and physical signs of fluid loss is a medical priority.
What are the physical signs of dehydration I should look for in my baby?
You must monitor four key areas: the anterior fontanelle (the soft spot on the head), which may appear sunken; the skin turgor, which is tested by pinching the abdominal skin to see if it ‘tents’; the mucous membranes, checking for a dry or tacky mouth; and tear production. If the soft spot is dipped like a crater or the skin does not snap back instantly, seek emergency care immediately.
How many wet diapers should a newborn have if they are suffering from diarrhea?
A healthy, well-hydrated newborn should produce at least six heavily wet diapers in a 24-hour period. If your baby’s output drops to fewer than four wet diapers in 24 hours, or if they go more than six hours without urinating, they are entering a dangerous state of dehydration and require immediate pediatric evaluation.
Can I give my one-month-old Pedialyte or water to treat diarrhea?
No, you should never give plain water to a newborn, as it can cause fatal water intoxication by diluting their sodium levels. Regarding oral rehydration solutions like Pedialyte, they should only be administered to infants under three months of age with a specific dosage and direct authorization from your pediatrician. The primary treatment remains frequent, on-demand breastfeeding or formula feeding.
Why does my baby have diarrhea after taking antibiotics?
Antibiotics are non-discriminatory; they kill the targeted infection but also wipe out the beneficial ‘good’ bacteria in the infant’s gut flora. This disruption to the microbiome prevents proper digestion and water absorption, leading to loose, watery stools. If this occurs, do not stop the medication; instead, consult your doctor about adjusting the dose or introducing infant-safe probiotics.
What does it mean if there is mucus or blood in my baby’s diaper?
Visible strings of slimy mucus or red streaks of blood usually indicate significant inflammation in the intestinal lining. This is a hallmark sign of Cow’s Milk Protein Allergy (CMPA) or a bacterial infection. If you see blood, black tarry stools, or white/chalky stools, these are considered ‘red flags’ that require an immediate call to your pediatrician or a visit to the emergency room.
How should I treat a diaper rash caused by frequent diarrhea?
Diarrhea is highly acidic and can cause chemical burns on delicate skin. Avoid commercial wipes, which contain irritating fragrances; instead, use warm water and cotton pads. Pat the skin bone-dry—never rub—and apply a thick, opaque layer of zinc oxide-based barrier cream. Think of it like frosting a cake; the cream should act as a physical shield between the skin and the stool.
When is a fever in a newborn with diarrhea considered an emergency?
For any infant under three months of age, a rectal temperature of 100.4°F (38°C) or higher is a strict medical emergency. In a neonate, a fever combined with diarrhea can indicate a systemic infection or severe dehydration. Do not administer infant Tylenol to mask the fever; take the baby to the nearest emergency department for a full clinical workup.
Disclaimer
This article is for informational and educational purposes only and does not constitute professional medical advice, diagnosis, or treatment. The neonatal digestive system is highly sensitive, and symptoms can escalate rapidly. Always seek the advice of a board-certified pediatrician or other qualified health provider with any questions you may have regarding a medical condition or your infant’s gastrointestinal health. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
References
- American Academy of Pediatrics (AAP) – healthychildren.org – Comprehensive guidelines on normal infant bowel movements and identifying illness in newborns.
- Centers for Disease Control and Prevention (CDC) – cdc.gov – Data on rotavirus prevalence and the clinical impact of infant vaccinations on gastrointestinal health.
- World Health Organization (WHO) – who.int – Global statistics and management protocols for diarrheal disease and dehydration in infants.
- Mayo Clinic – mayoclinic.org – Clinical descriptions of dehydration signs in infants, including skin turgor and fontanelle assessments.
- Journal of Pediatric Gastroenterology and Nutrition – journals.lww.com – Research on Cow’s Milk Protein Allergy (CMPA) and its effects on the neonatal gut lining.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – niddk.nih.gov – Technical resources on the physiology of the infant digestive system and gastric emptying.