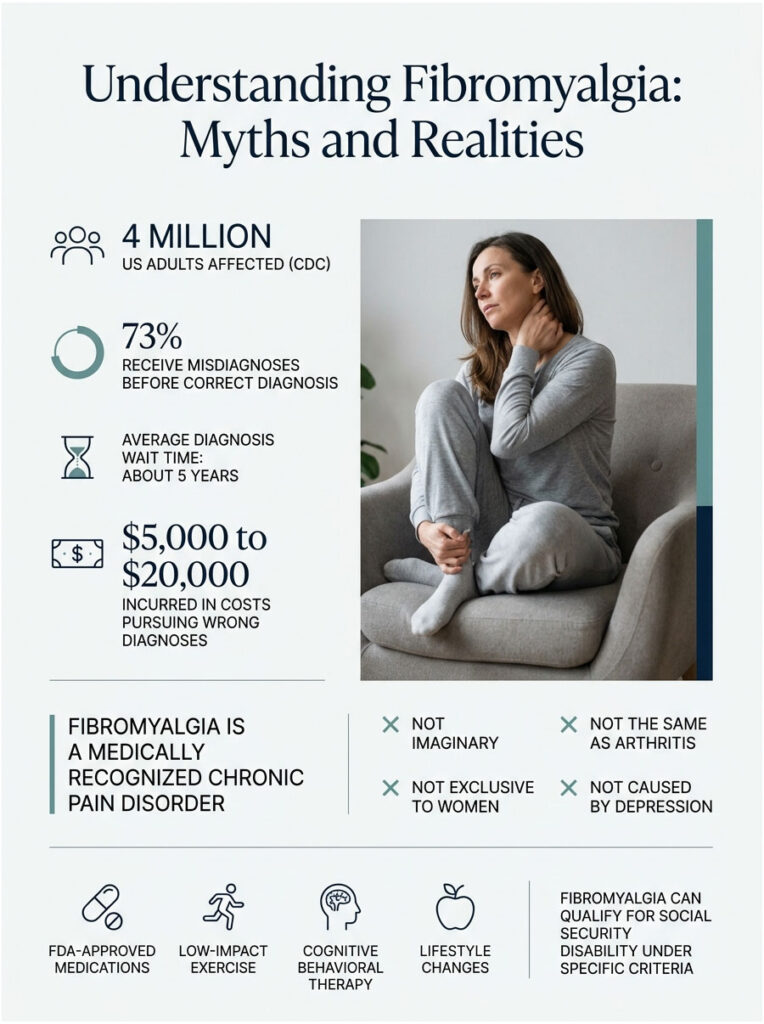
About 4 million US adults live with fibromyalgia, according to the CDC, and roughly 73 percent of them have been told they have something else first. The average wait for the right diagnosis runs about 5 years. Along the way, patients commonly rack up $5,000 to $20,000 in copays, lab work, and unrelated specialist visits chasing the wrong fix. That long detour is built on myths, and those myths cost patients real time, real money, and real quality of life.
Table of Contents
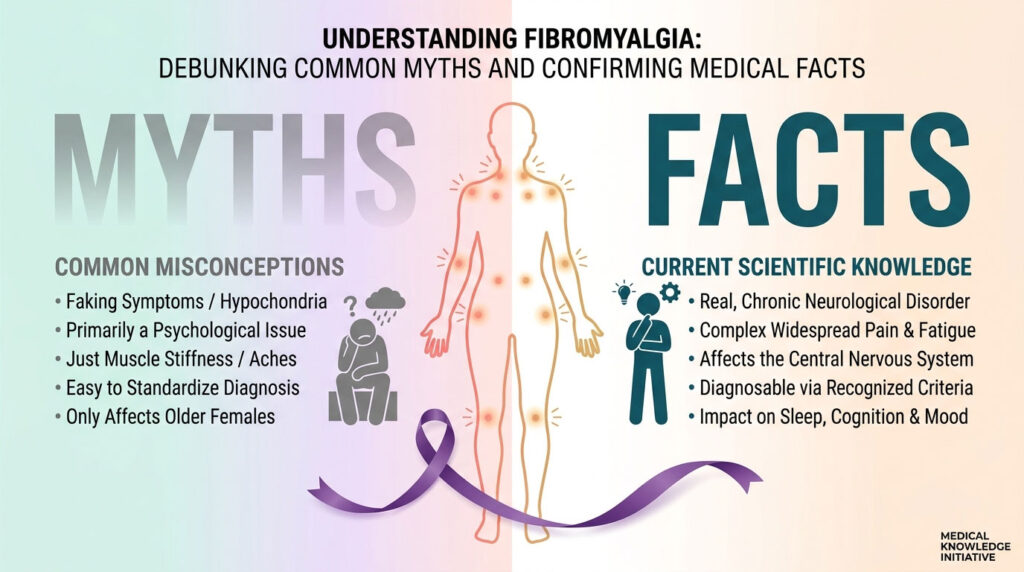
Quick Answer: Fibromyalgia is a real, medically recognized chronic pain disorder that affects about 4 million US adults according to the CDC. It’s not imaginary, not the same as arthritis, not exclusive to women, and not caused by depression. Three FDA-approved medications, structured low-impact exercise, cognitive behavioral therapy, and lifestyle changes form the standard treatment package. The condition qualifies for Social Security disability when symptoms meet specific evidence criteria.
At a Glance
- The CDC recognizes fibromyalgia as a real chronic pain disorder affecting about 4 million US adults
- Women are 7 times more likely to be diagnosed, but men and children get it too
- The average diagnostic delay in the US is about 5 years
- 3 FDA-approved medications exist: pregabalin, duloxetine, milnacipran
- Light exercise, not rest, is among the most effective treatments
- 35 to 55 percent of US fibromyalgia patients qualify for some disability support
- Fibromyalgia does not shorten your life expectancy
Why Fibromyalgia Myths Persist (and Why They Hurt Patients)
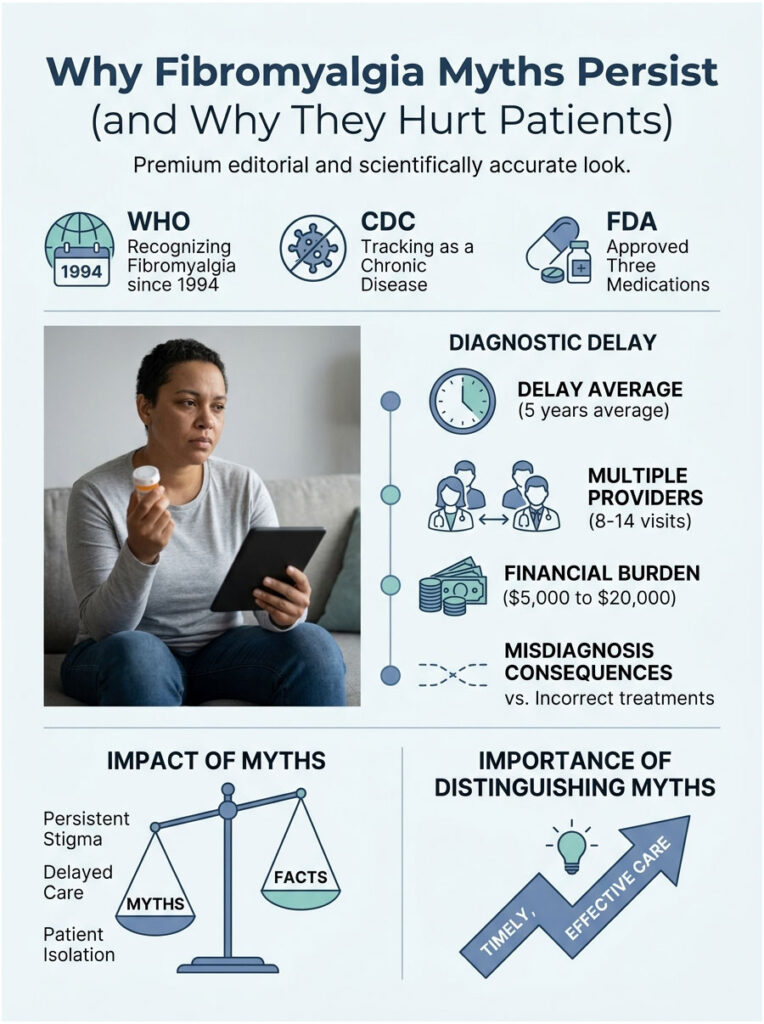
The World Health Organization formally recognized fibromyalgia in 1994. The CDC tracks it in its chronic disease surveillance. The FDA has approved three drugs to treat it. Yet 30 years on, you can still walk into a US clinic and hear it dismissed as “stress” or “depression in disguise.” That gap between scientific consensus and bedside reality is where the myths live.
The 5-Year Diagnostic Delay Problem
Patients booking blood-panel screenings through HealthCareOnTime often arrive after years of getting bounced between primary care, gastroenterology, orthopedics, and psychiatry. The National Fibromyalgia Association puts the average diagnostic delay at about 5 years from first symptom to confirmed diagnosis in the US. Five years of wrong labels means five years of wrong treatments.
How Misinformation Affects Treatment Access
In cases reviewed by our medical team, patients who arrived at a confirmed diagnosis after 3 or more years of confusion typically logged 8 to 14 different provider visits along the way. That trail of misdiagnosis carries a financial dent of $5,000 to $20,000 in out-of-pocket costs, according to figures cited by patient advocacy groups. The faster a US patient can sort myths from facts, the faster the right care kicks in.
Myths About What Fibromyalgia Actually Is
The first cluster of myths concerns the nature of the condition. These are the ones that block diagnosis at the front door.
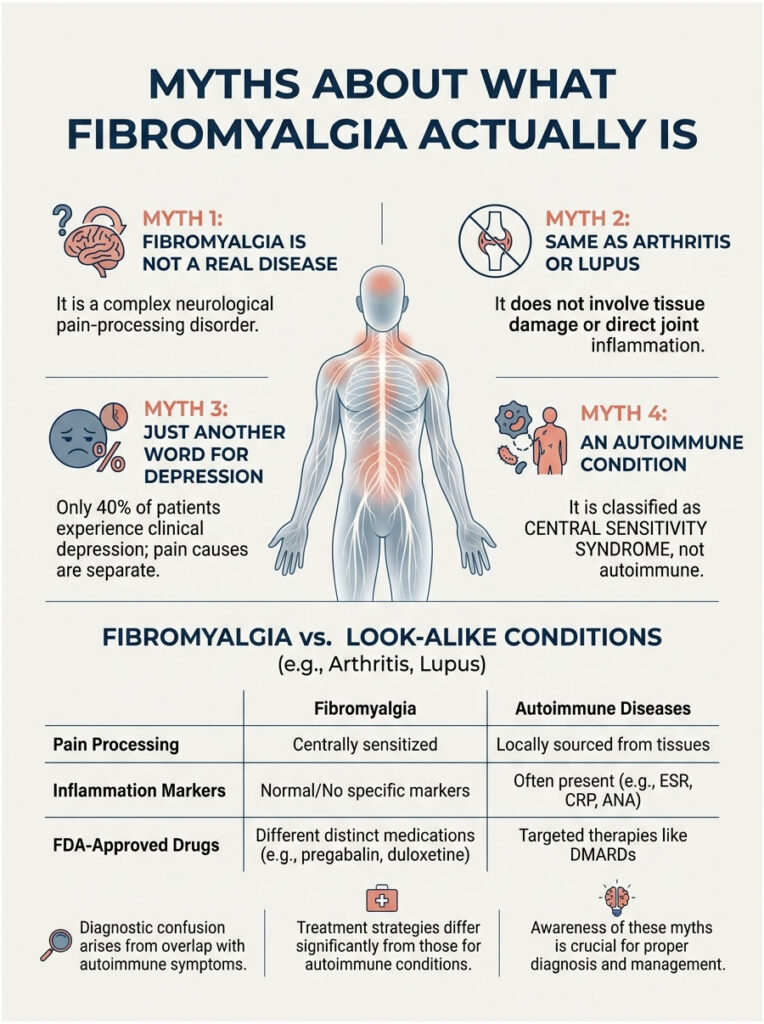
Myth 1: Fibromyalgia Is Not a Real Disease
This is the granddaddy of fibromyalgia myths and the most damaging. The truth: fibromyalgia is a neurological pain-processing disorder rooted in central sensitization, where the nervous system amplifies pain signals from the body. Brain-imaging studies cited by StatPearls / NIH NCBI Bookshelf show measurable changes in resting-state functional connectivity and neurotransmitter activity in fibromyalgia patients compared with controls.
The American College of Rheumatology issued its first formal classification criteria in 1990, refined them in 2010, and updated them again in 2016. The FDA has approved three drugs specifically for the condition. That’s not the trajectory of a fake illness.
Myth 2: Fibromyalgia Is the Same as Arthritis or Lupus
Both arthritis and lupus cause inflammation that damages joints, tissues, or organs over time. Fibromyalgia doesn’t. Bloodwork from a fibromyalgia patient typically shows no elevated inflammatory markers like CRP, ESR, ANA, or rheumatoid factor. The pain is real and widespread, but it comes from how the nervous system processes pain signals, not from tissue damage.
Our medical reviewers note that fibromyalgia frequently co-occurs with autoimmune conditions, which adds to the diagnostic confusion. A US patient can have both rheumatoid arthritis and fibromyalgia at the same time. The diagnoses stay separate, the treatments differ, and missing one of the two means missing half the picture.
Myth 3: Fibromyalgia Is Just Another Word for Depression
This myth keeps a lot of US patients stuck on the wrong medication track for years. According to WebMD’s review of fibromyalgia myths, only about 40 percent of fibromyalgia patients also experience clinical depression. The other 60 percent do not.
Living with chronic pain absolutely can trigger depression, but the depression is a downstream consequence, not the cause. Treating depression alone, without addressing the underlying pain disorder, is one of the most common reasons US patients spend years chasing the wrong fix.
Myth 4: Fibromyalgia Is an Autoimmune Condition
Fibromyalgia is not autoimmune. There’s no autoantibody attacking your tissues, and you won’t see immunosuppressants on a standard fibromyalgia treatment plan. The disorder belongs in the central sensitivity syndrome category, alongside irritable bowel syndrome, tension-type headache, and TMJ disorder.
The mix-up is easy to understand. Both fibromyalgia and autoimmune diseases like lupus cause fatigue, widespread aches, and brain fog. The lab markers, treatments, and long-term outlook differ sharply. Patients commonly ask our medical team why the immunology workup came back normal when they feel so sick. The answer: a normal autoimmune panel is exactly what fibromyalgia looks like.
Table 1: Fibromyalgia vs. Look-Alike Conditions (Side-by-Side)
| Feature | Fibromyalgia | Rheumatoid Arthritis | Chronic Fatigue Syndrome | Lupus | Multiple Sclerosis |
| Primary Cause | Central nervous system pain processing | Autoimmune joint attack | Unknown, often post-viral | Autoimmune systemic | Demyelination of nerve fibers |
| Inflammation Markers | Normal | Elevated (CRP, RF, anti-CCP) | Normal | Often elevated (ANA, complement) | Normal or specific MRI findings |
| Joint Damage | No | Yes, progressive | No | Yes, possible | No, neurological damage |
| Fatigue Level | Severe | Moderate to severe | Severe, defining feature | Moderate | Moderate to severe |
| US Prevalence | About 4 million adults (CDC) | About 1.3 million adults (CDC) | 836,000 to 2.5 million | About 1.5 million (Lupus Foundation) | About 1 million (NIH) |
| Diagnostic Test | Clinical criteria, no blood test | Blood tests + imaging | Clinical exclusion | Blood tests + clinical signs | MRI + spinal fluid analysis |
| FDA-Approved Drugs | 3 (pregabalin, duloxetine, milnacipran) | 20+ DMARDs and biologics | 0 specific | Several immunosuppressants | 20+ disease-modifying drugs |
Myths About Who Gets Fibromyalgia
The second cluster blocks patients outside the “expected” demographic from being taken seriously at all.
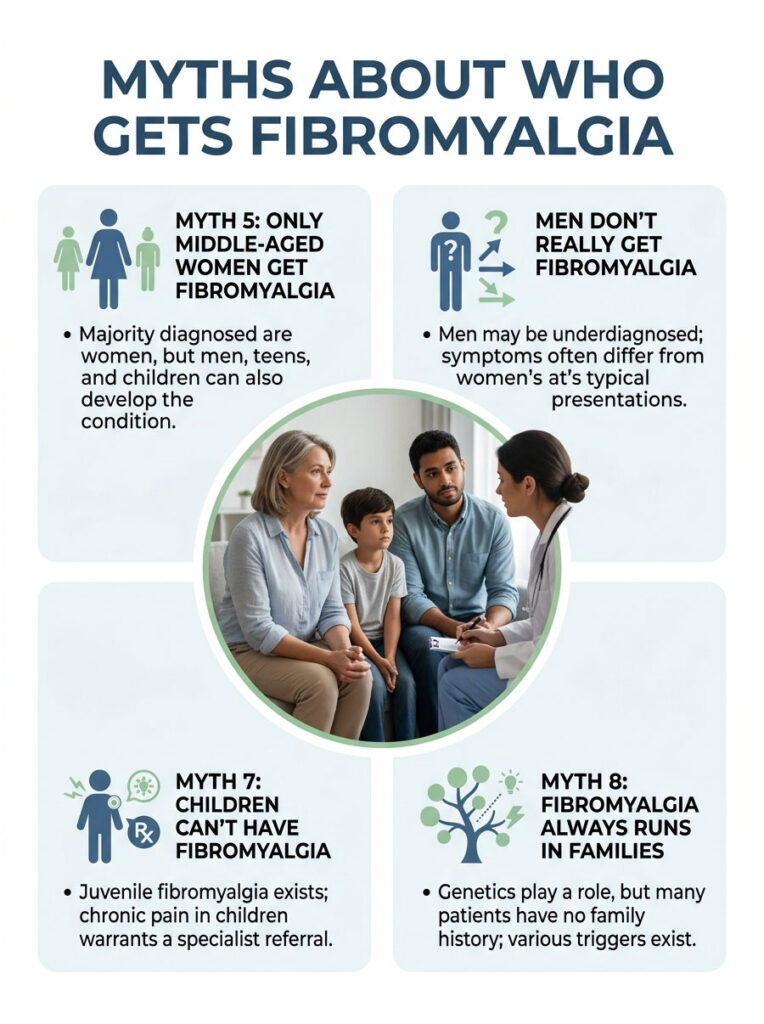
Myth 5: Only Middle-Aged Women Get Fibromyalgia
Women do make up the majority of diagnosed cases. The CDC and other US sources report women are roughly 7 times more likely than men to receive the diagnosis. The peak age range is 40 to 60. But “majority” isn’t “only.”
Men, teenagers, children, and seniors all develop fibromyalgia. The Cleveland Clinic lists every age group as susceptible, and US researchers increasingly suspect male fibromyalgia is significantly underdiagnosed because the screening tools were built around women’s symptom patterns.
Myth 6: Men Don’t Really Get Fibromyalgia
US prevalence data shows women are diagnosed about 7 to 1 over men. But Rheumatology Advisor cites clinicians who suspect actual male prevalence is far higher than the numbers suggest. Men often present with more localized pain and fewer cognitive complaints, which doesn’t match the textbook “tender points across the body” picture.
The result: a US man with fibromyalgia is more likely to be labeled with chronic back pain, depression, or fatigue syndrome and miss the right diagnosis entirely.
Myth 7: Children Can’t Have Fibromyalgia
Juvenile fibromyalgia is a recognized pediatric condition. The NIH StatPearls reference uses the Yunus and Masi criteria for children and adolescents, distinct from adult ACR criteria. Pediatric rheumatologists at major US children’s hospitals (Boston Children’s, Children’s Hospital of Philadelphia, Cincinnati Children’s) treat juvenile fibromyalgia regularly.
Parents whose child reports chronic widespread pain, sleep problems, and fatigue for more than 3 months deserve a pediatric rheumatology referral, not a “growing pains” dismissal.
Myth 8: Fibromyalgia Always Runs in Families
Genetics play a role, but inheritance isn’t guaranteed. The Cleveland Clinic notes children of fibromyalgia patients carry elevated risk, likely linked to genes that affect neurotransmitter signaling. Plenty of fibromyalgia patients have no family history at all.
Trauma, infection, surgery, and chronic stress can trigger the condition in people with no genetic predisposition. Patients booking diagnostic panels with us often ask whether their children will get it too. The honest answer: elevated risk, not destiny.
Myths About Symptoms and Diagnosis
The third cluster traps patients in diagnostic limbo even after they reach the right type of doctor.
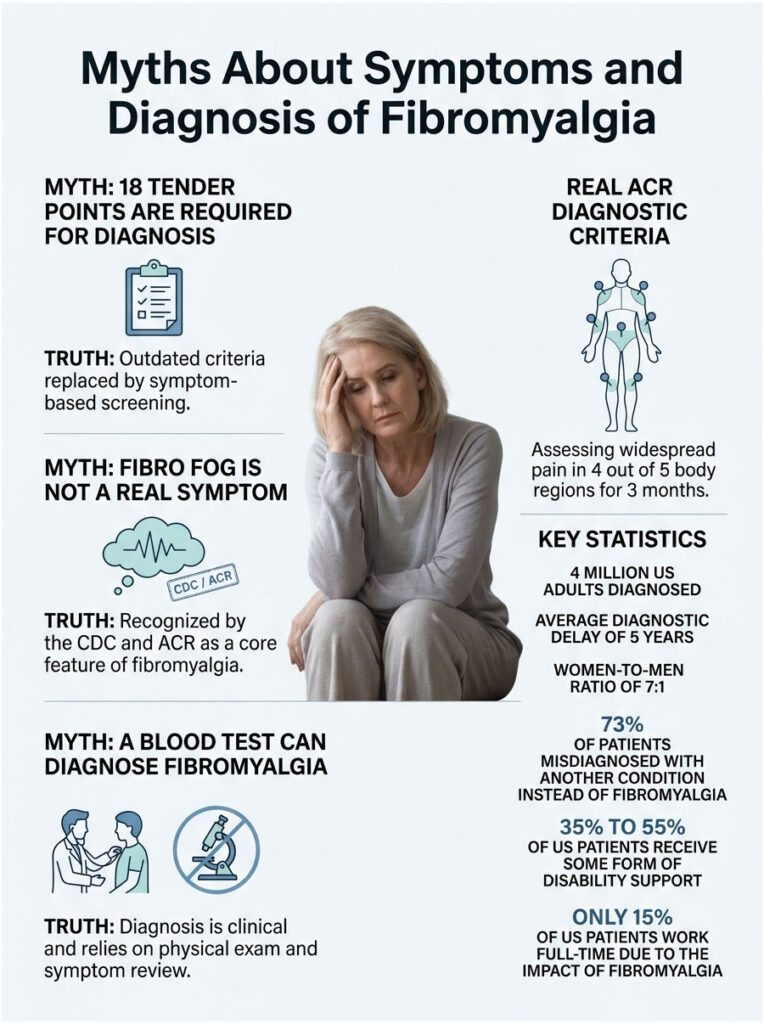
Myth 9: You Need 18 Tender Points to Be Diagnosed
This was the diagnostic standard from 1990 until 2010. It’s outdated. The ACR replaced the tender-point exam with a symptom-based screening that asks about widespread pain across five body regions plus associated symptoms like sleep disturbance, fatigue, and cognitive issues.
WebMD reports about 20 percent of fibromyalgia patients don’t have classic tender points at all. A US doctor who still leans on the old 18-point exam may be missing 1 in 5 cases walking through the door.
Myth 10: Fibro Fog Isn’t a Real Symptom
Fibro fog, also called brain fog, refers to memory problems, word-finding difficulty, slowed processing, and trouble concentrating. The CDC and the American College of Rheumatology both list it as a core feature, not a vague complaint.
Neuroimaging research summarized in the NIH StatPearls reference shows measurable changes in brain connectivity that correspond to cognitive symptoms. Patients booking cognitive-screening panels through our team often describe fibro fog as more disabling than the pain itself.
Myth 11: A Blood Test Can Diagnose Fibromyalgia
No blood test confirms fibromyalgia. The CDC classifies the diagnosis as clinical, made through physical exam, health history, and symptom review. Blood work is used to rule out other conditions, not to confirm fibromyalgia itself.
A standard rule-out panel typically includes complete blood count, comprehensive metabolic panel, thyroid panel, ESR, CRP, vitamin D, vitamin B12, and ANA. Patients booking these tests through HealthCareOnTime usually get the full workup done in a single sitting.
The Real ACR Diagnostic Criteria
A US doctor working from current guidelines will check for widespread pain across 4 of 5 body regions for 3 or more months, score the symptom severity (sleep problems, fatigue, cognitive issues), and rule out other diseases that better explain the symptoms. No tender-point count required.
Table 2: Key US Fibromyalgia Statistics
| Statistic | Value | Source |
| US adults diagnosed with fibromyalgia | About 4 million (2% of adults) | CDC |
| Estimated total US prevalence including undiagnosed | Up to 10 million | National Fibromyalgia Association |
| Average diagnostic delay | About 5 years | National Fibromyalgia Association |
| Women-to-men diagnosis ratio | About 7 to 1 | CDC |
| Patients with another diagnosis instead of fibromyalgia | About 73% | 2012 NHIS analysis (PLOS One) |
| US patients on some form of disability support | 35% to 55% | CDC and pain-management research |
| US patients working full-time | About 15% | Vincent et al., 2013; CDC |
Myths About Treatment and Recovery
The fourth cluster keeps patients away from the things that actually help.
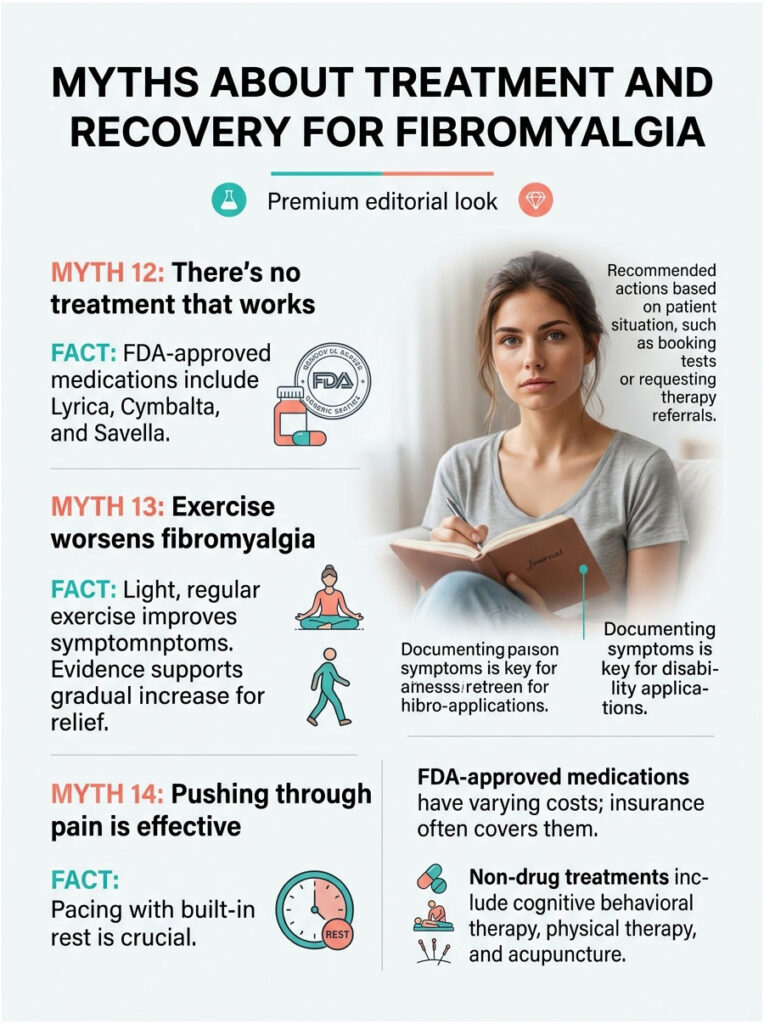
Myth 12: There’s No Treatment That Works
There’s no cure, but plenty of treatments work. The FDA has approved three medications specifically for fibromyalgia: pregabalin (Lyrica), duloxetine (Cymbalta), and milnacipran (Savella). Each calms overactive pain signaling pathways in the central nervous system through a different mechanism.
Beyond medications, evidence-based options include cognitive behavioral therapy, structured aerobic exercise, low-impact strength training, mindfulness-based stress reduction, and sleep hygiene work. The Mayo Clinic lists all of these as standard parts of a modern treatment plan.
Myth 13: Exercise Makes Fibromyalgia Worse
Hard exercise can flare symptoms. Light, regular exercise consistently improves them. The Cleveland Clinic and Mayo Clinic both list low-impact aerobic activity (walking, swimming, water aerobics, recumbent biking) as one of the most effective non-drug treatments available.
Patients who start at 5 minutes a day and add a minute or two per week consistently report less pain and better sleep within 8 to 12 weeks. The trick is starting low and progressing slowly. Diving back into the gym you used pre-diagnosis is the version that backfires.
Myth 14: You Just Have to Push Through the Pain
“Pushing through” is the fastest route to a worse flare. Pacing, the practice of breaking activity into manageable chunks with built-in rest breaks, is now the standard self-management strategy taught in US pain-management programs. The goal is to stay below the symptom-flare threshold so you can do more over time, not collapse periodically and lose ground.
FDA-Approved Medications With US Pricing
US fibromyalgia patients have three on-label drug choices. Pregabalin (Lyrica), the first FDA-approved fibromyalgia medication, runs $7 to $30 for generic at most US pharmacies through GoodRx coupons. Duloxetine (Cymbalta), an SNRI antidepressant repurposed for fibromyalgia, costs $4 to $15 generic. Milnacipran (Savella), another SNRI built for fibromyalgia, runs $40 to $90 for the branded version. Generic milnacipran is now available and cheaper.
Off-label medications doctors also prescribe include low-dose amitriptyline for sleep and pain, gabapentin for nerve-pain components, and cyclobenzaprine for muscle spasm. Most major US insurance plans cover all three FDA-approved drugs with prior authorization.
Non-Drug Treatments Backed by Evidence
A typical US treatment plan layers medication with cognitive behavioral therapy (usually 8 to 12 sessions through a licensed psychologist), physical therapy (typically 6 to 10 sessions to learn pacing and exercise progression), and sleep-medicine consultation if insomnia is severe. Acupuncture has growing evidence support and is now covered by some US PPO plans.
Table 3: What to Do Based on Your Current Situation
| Situation | Action Step | Why It Helps |
| Symptoms over 3 months, no diagnosis yet | Book a CBC, CMP, TSH, ESR, CRP, vitamin D, ANA panel through HealthCareOnTime | Rules out anemia, thyroid, inflammatory disease, vitamin deficiency |
| Diagnosed but no relief on first medication | Ask a rheumatologist or pain specialist about switching among the 3 FDA-approved drugs | Each drug works through a different mechanism; about 50% switch responders |
| Diagnosed and stable but exhausted | Add structured low-impact exercise: 5 minutes daily, build by 1 to 2 minutes per week | 8 to 12 weeks of consistent activity reduces pain and improves sleep |
| Brain fog interfering with work | Request cognitive behavioral therapy referral; ADA workplace accommodations | CBT has documented benefit on fibro fog; ADA protects job rights |
| Considering disability application | Document symptoms daily for 90+ days; gather medical records | SSA approval depends on detailed, dated symptom and treatment evidence |
| Family member newly diagnosed | Schedule one shared appointment with the rheumatologist | Education reduces caregiver friction; outcomes improve with household support |
Myths About Living and Working With Fibromyalgia
The last cluster shapes long-term outlook and financial planning.

Myth 15: Fibromyalgia Shortens Your Life
It doesn’t. Multiple population studies show no reduction in life expectancy attributable to fibromyalgia itself. The CDC emphasizes that while quality of life is significantly affected, the disease is not fatal.
The caveat: fibromyalgia often shows up alongside other conditions (cardiovascular disease, autoimmune disorders, mental health conditions) that can affect mortality. Treating those comorbidities aggressively is the bigger longevity move than treating the fibromyalgia itself. Patients commonly ask whether they should worry about a shorter life with a fibromyalgia diagnosis. The honest answer: no, not from the fibromyalgia.
Myth 16: You Can’t Qualify for Disability in the US
Fibromyalgia is a recognized impairment under Social Security Administration ruling SSR 12-2p. To qualify for SSDI or SSI on the basis of fibromyalgia, applicants need a longitudinal medical record showing the ACR criteria are met, documented attempts at standard treatments, and evidence of functional limitations.
Approval rates run stricter than for many other conditions, but they’re real. Patients commonly ask us about timeline expectations: initial approvals take 3 to 6 months, denials are common on first application, and appeals with proper legal support succeed in a significant percentage of cases.
Workplace Accommodations Under the ADA
The Americans with Disabilities Act protects fibromyalgia patients in workplaces with 15 or more employees. Reasonable accommodations include flexible scheduling, ergonomic seating, the option to work remotely on flare days, modified break schedules, and reduced lifting requirements. Employers cannot legally fire or demote a worker for requesting these accommodations.
What Insurance Will and Won’t Cover
Major US health plans typically cover the three FDA-approved fibromyalgia drugs, physical therapy (with visit caps), cognitive behavioral therapy (usually 20 to 40 visits per year), and rheumatology consultations. Coverage gaps that surprise patients: massage therapy, acupuncture, and most supplements are usually out-of-pocket. HSA and FSA funds typically cover the first two with a doctor’s letter of medical necessity.
How to Get a Real Diagnosis and the Right Treatment Plan
Knowing the myths is half the work. The other half is moving fast on a real plan.

Step 1: Track Your Symptoms for 90 Days
Daily pain map, sleep hours, fatigue level, cognitive function, and flare triggers. A free symptom-tracking app or a simple paper journal works fine. Doctors need patterns, not single bad days.
Step 2: Request Blood Work to Rule Out Other Causes
A full rule-out panel (CBC, CMP, TSH, free T4, ESR, CRP, vitamin D, B12, ferritin, ANA) costs roughly $200 to $400 out of pocket without insurance and is usually covered with insurance. HealthCareOnTime patients commonly bundle the whole panel into a single visit.
Step 3: Find a Rheumatologist or Pain Specialist
Primary care can diagnose fibromyalgia, but a rheumatologist or pain medicine specialist is faster and more accurate. The American College of Rheumatology provides a public find-a-rheumatologist tool.
Step 4: Build a Multi-Pronged Treatment Plan
Single treatments rarely work. The combinations that consistently help: one FDA-approved medication + structured low-impact exercise + cognitive behavioral therapy + sleep hygiene work + pacing strategy + stress management. Most US patients see meaningful improvement within 8 to 16 weeks of starting the full package.
Frequently Asked Questions
Is fibromyalgia all in your head?
No. Fibromyalgia is a recognized neurological pain-processing disorder with documented changes in brain connectivity and neurotransmitter activity. The CDC, NIH, FDA, WHO, and ACR all recognize it as a real medical condition. Brain imaging in research settings shows measurable differences between fibromyalgia patients and controls. The pain is real, even when standard imaging of your joints looks completely normal.
Can a blood test diagnose fibromyalgia?
No, no blood test currently confirms fibromyalgia. Diagnosis is clinical, based on symptom criteria from the American College of Rheumatology. Blood tests are used to rule out other conditions like thyroid disorders, anemia, vitamin deficiencies, or autoimmune diseases. A typical rule-out panel includes CBC, CMP, thyroid panel, ESR, CRP, vitamin D, B12, and ANA testing.
Is fibromyalgia an autoimmune disease?
No. Fibromyalgia is not autoimmune. There’s no antibody attacking your tissues. It’s classified as a central sensitivity syndrome involving the nervous system, not the immune system. That said, fibromyalgia commonly co-occurs with autoimmune conditions like rheumatoid arthritis, lupus, and Sjögren’s, which adds to the confusion. Treatment plans for each condition stay separate.
Can men get fibromyalgia?
Yes, men get fibromyalgia. The 7-to-1 female-to-male diagnosis ratio likely understates true male prevalence. Men often present with more localized pain and fewer cognitive complaints, so they’re frequently misdiagnosed as chronic back pain or fatigue. Any man with widespread pain, fatigue, and sleep problems lasting more than 3 months deserves a rheumatology referral and current ACR criteria assessment.
Will fibromyalgia get worse over time?
Not necessarily. Many fibromyalgia patients stabilize or improve with proper treatment. Symptom severity varies, with flare periods and better periods over years. The Cleveland Clinic notes that with the right combination of medication, exercise, therapy, and stress management, most patients can substantially reduce day-to-day impact. Untreated fibromyalgia tends to fluctuate without clear improvement.
Does fibromyalgia shorten your life?
No. The CDC and major US medical authorities confirm fibromyalgia is not life-shortening on its own. Life expectancy in fibromyalgia patients matches the general population when comorbidities are controlled for. Quality of life can be significantly affected, but mortality risk is not elevated by the fibromyalgia diagnosis itself. Co-occurring conditions like heart disease deserve aggressive treatment.
Is fibromyalgia considered a disability in the US?
Yes, fibromyalgia can qualify as a disability under Social Security guidelines (SSR 12-2p). Approval requires a documented diagnosis meeting ACR criteria, evidence of functional limitations, and a longitudinal medical record. The Americans with Disabilities Act also protects workers with fibromyalgia in employers with 15 or more employees, requiring reasonable workplace accommodations like flexible scheduling.
What is the best treatment for fibromyalgia?
The most effective approach combines multiple treatments. A typical evidence-based plan: one FDA-approved medication (pregabalin, duloxetine, or milnacipran), structured low-impact exercise, cognitive behavioral therapy, sleep optimization, pacing strategy, and stress management. Most US patients on the full combination see meaningful improvement within 8 to 16 weeks. Single-treatment approaches rarely work for this condition.
Can children get fibromyalgia?
Yes. Juvenile fibromyalgia is a recognized pediatric condition. Children and adolescents experiencing chronic widespread pain, fatigue, and sleep disturbance for over 3 months should see a pediatric rheumatologist. The Yunis and Masi diagnostic criteria are used for younger patients. Major US children’s hospitals including Boston Children’s, CHOP, and Cincinnati Children’s run dedicated juvenile fibromyalgia programs.
Does exercise help or hurt fibromyalgia?
Light, consistent exercise helps. Intense exercise hurts. Low-impact aerobic activity (walking, swimming, water aerobics, recumbent biking) is one of the most effective non-drug treatments. The starting point matters: begin at 5 minutes daily and add 1 to 2 minutes per week. Most patients see less pain and better sleep within 8 to 12 weeks of consistent activity at appropriate intensity levels.
Is fibro fog a real medical symptom?
Yes, fibro fog (cognitive dysfunction) is recognized by the CDC and ACR as a core fibromyalgia feature. It includes memory problems, word-finding difficulty, slowed processing, and concentration issues. Brain-imaging research shows measurable connectivity changes corresponding to these cognitive symptoms. Many patients describe fibro fog as more disabling than the pain itself, particularly in workplace settings requiring complex thinking.
Can you cure fibromyalgia naturally?
No, there’s no cure for fibromyalgia, natural or medical. However, many patients achieve significant symptom reduction through combined approaches: structured exercise, anti-inflammatory dietary patterns, stress management, sleep optimization, and cognitive behavioral therapy. Be cautious of products marketed as “cures” since none have FDA validation. Discuss any supplement or alternative therapy with a doctor first, especially if you’re on FDA-approved fibromyalgia medications.
Medical Disclaimer: This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider regarding fibromyalgia or any chronic pain condition. HealthCareOnTime does not provide diagnostic services through this content. If you’re experiencing severe pain, significant functional decline, or thoughts of self-harm, contact a healthcare provider or call 988 (Suicide and Crisis Lifeline) immediately.
References
- Centers for Disease Control and Prevention: Fibromyalgia
- National Institutes of Health / StatPearls: Fibromyalgia
- WebMD: Fibromyalgia: Myths and Facts
- Cleveland Clinic: 6 Myths About Fibromyalgia
- Mayo Clinic: Fibromyalgia
- Rheumatology Advisor: 5 Persistent Myths About Fibromyalgia
- PMC / NIH: Facts and Myths Pertaining to Fibromyalgia
- PLOS One: Prevalence and Characteristics of Fibromyalgia in the 2012 NHIS
- National Fibromyalgia Association: Fibromyalgia Prevalence
- Social Security Administration: SSR 12-2p
- American College of Rheumatology: Find a Rheumatologist
- ADA.gov: Americans with Disabilities Act Information