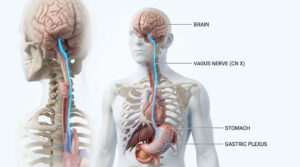
Understanding Adrenal Gland
A pyramidal/semi lunar shaped gland located on top of each kidney which measures 5cm by 2cm. It
secretes several classes of hormones vital for various functions like metabolism, regulation of immune
system, salt and water balance, maintaining pregnancy, aids in the time of stress, among others.
Also called suprarenal glands, these are composed of 2 distinct parts called outer cortex and inner medulla. Adrenal cortex tends to be much more fattier and is larger than the medulla. Further, cortex produces more than 30 hormones (steroids) and is divided into 3 distinct zones, namely; zona glomerulosa, zona fasciculata and zona reticularis which synthesizes aldosterone (regulates salt balance), cortisol (regulates blood glucose levels) and adrenal androgens (for development of sexual characteristics) respectively. Whereas, medulla synthesizes catecholamines; adrenaline and noradrenaline.
Adrenal-Cortex (Adrenal Steroidogenesis)
Adrenal Steroidogenesis is a dynamic process which involves de novo synthesis of hormones. cholesterol
acts as a common precursor for all the steroids conversion. Initially, for adrenal steroidogenesis, cholesterol
is mobilized in the outer mitochondrial membrane which is then transferred to inner mitochondrial membrane
(IMM) with the help of steroidogenic acute regulatory (StAR) protein. In IMM, side-chain cleavage enzyme
(CYP11A1, P450scc) ne from which all other hormones like Corticosterone, Aldosterone, Cortisol, Dehydroepiandrosterone
(DHEA-S), testosterone and others are produced.
Aldosterone Biosynthesis
- It is a mineralocorticoid, synthesized in the zona glomerulosa.
- Its main function includes sodium and water retention by the kidneys causing rise in blood pressure; and excretion of potassium and hydrogen ions by the kidneys.
- Aldosterone is produced because of reninangiotensin-aldosterone system. This involves release of renin enzyme by kidneys in response to low blood pressure. Which then cleaves angiotensinogen circulating in blood, out of which one is called angiotensin I. Then, Angiotensin Converting Enzyme (ACE) results in the formation of angiotensin II in the lungs from angiotensin I. Angiotensin II increases the blood pressure by constricting muscular walls of small arteries. It also stimulates adrenal cortex to release aldosterone, which also increases blood pressure due to salt retention by kidneys.
Cortisol Biosynthesis
- It is a glucocorticoid and is synthesized in zona fasciculata.
- Among sundry of effects on tissues and organs; it is essential for gluconeogenesis, modulation of immune system, it also acts like aldosterone to raise blood pressure but, to a limited extent.
- It also plays a role in increased acid production by stomach, increased appetite and in mental state like euphoria, much of which is poorly understood.
- Cortisol synthesis is controlled by HypothalamusPituitary-Adrenal (HPA) Axis. This axis is one of the four major neuroendocrine systems. It involves complex set of feedback interactions between three organs; hypothalamus, pituitary gland and adrenal gland.
- This glucocorticoid is released in stress which can be emotional (anxiety) or physiological like (injury). Hypothalamus releases Corticotropin Releasing Hormone (CRH) during stress, which travels to the anterior pituitary, where, it stimulates the cleavage of Proopiomelanocortin (POMC). This leads to the release of Melanocyte Stimulating Hormone (MSH) and Adrenocorticotropic Hormone (ACTH). ACTH travels to the cortex of adrenal gland stimulating the production and release of cortisol.
- Once cortisol is released it travels to the tissue to exerts its effects and inhibits hypothalamus and pituitary gland to release CRH and ACTH respectively via, negative feedback mechanism to prevent cortisol release. Cortisol is then inactivated in the liver to inactive cortisone.
Adrenal Androgens Biosynthesis
- These are sex steroids responsible for producing primary and secondary sexual characteristics of male and female.
- It is synthesized in zona reticularis; dehydroepiandrosterone (DHEA) and its sulphate are two most abundant adrenal steroids.
- ACTH is a primary stimulus for Androgens biosynthesis and is required for development of zona reticularis.
- Other growth factors are also believed to regulate the androgen synthesis but, remains poorly understood.
Adrenal-Medulla
Catecholamines Biosynthesis
- Chromaffin cells having chromaffin granules which stores catecholamines are found in clusters or nests.
- Adrenaline and Noradrenaline are catecholamines which are secreted in 4:1 ratio respectively by the medulla.
- Sympathetic Nervous System controls the release of these catecholamines from the chromaffin cells. This part of nervous system is activated during sudden stress, such as conflict or fear (also known as fight, flight or fright response).
- Adrenaline and Noradrenaline acts on a wide range of tissues such as heart, lungs, gut and eyes producing different effects when released in the blood stream.
Effects of Adrenaline
- Increases heart rate and systolic B.P.
- Decreases gut movement and closure of the sphincters
- Dilates the airways and pupils
- Increases blood glucose levels
- Increases B.P.
- Decreases heart rate
- Minimal increase in gut movement
- Minimal dilation of airways
- Dilation of pupils
Effects of Noradrenaline
Other hormones like leu-enkephalin and met enkephalin are also produced but their function is not clear.
Clinical Abnormalities
Primary Hyperaldosteronism
It is observed in 2% of patient suffering from hypertension. Most common cause of this hormonal disorder is
an aldosterone-producing adenoma also known as Conn’s syndrome. While, other causes includes idiopathic
hyperaldosteronism, primary adrenal hyperplasia, dexamethasone suppressible hyperaldosteronism and adrenal
cortical carcinoma.
Primary hyperaldosteronism can be distinguished from other causes of hyperaldosteronism by high levels of plasma aldosterone (PA) and low plasma renin activity (PRA). As in secondary hyperaldosteronism, high PRA and PA is observed, whereas, low PRA and PA is observed in patients with real or apparent mineralocorticoid excess which is not caused by aldosterone.
Diagnosis
For screening, PA:PRA ratio is used, and screening procedure is performed ideally when the patient is not taking
any medications for 2 to 4 hours before testing, along with 2 hours of standing. Once primary hyperaldosteronism
is suspected based on the PA:PRA ratio then confirmatory testing is performed, wherein, 2 liters of saline for over
4 hours is given to the individual to check possible aldosterone suppression (saline suppression test) or 24 hr
urinary aldosterone test is done.
Adrenal Insufficiency (AI)
Al also known as hypocortisolism is a condition in which either, adrenal gland produces insufficient amount of
cortisol (primary Al) or, there is a lack of CRH or corticotropin secondary or tertiary Al). In primary Al called Addison’s
disease, there is cortisol or aldosterone deficiency and in secondary or tertiary Al, Adrenal glands can synthesize
aldosterone but, not cortisol.
Autoimmune diseases, adrenal hemorrhage, HIV, infiltration of the adrenals by Tuberculosis, sarcoidosis or amyloidosis can cause primary Al; and infiltration of anterior pituitary, hypothalamus by craniopharyngioma, pituitary adenoma, metastasis, sarcoidosis, tuberculosis or suppression of corticotropin by steroid use can cause secondary or tertiary Al.
Weakness, fatigue, anorexia, nausea, abdominal pain and diarrhea are the manifestations of chronic Al. Hyponatremia can be seen with all the form of Al but, hyperkalemia is seen only in primary Al due to lack of aldosterone. In acute Al, decreased cardiac output and relative hypovolemia can be observed. If, Al is left untreated, it can lead to coma and even death.
Diagnosis
Diagnosis of Al involves measurement of serum cortisol preferably in moming or corticotropin-stimulation test.
For corticotropin-stimulation test, synthetic cosyntropin is given intravenously to measure the cortisol level at
baseline, at 30 minutes and at 60 minutes. Several other methods are also developed for measuring serum free
cortisol but, they are technically demanding and expensive.
Cushing’s Syndrome
This syndrome is caused due to persistent and inappropriate excess of cortisol caused due to excess glucocorticoids
production by adrenal glands, excess corticotropin (CRH) production or exogenous glucocorticoids. Excess production
by adrenal glands is observed due to adrenal adenoma, carcinoma or nodular hyperplasia. Likewise, corticotropin
can be produced by anterior pituitary gland or by paraneoplastic syndrome like bronchial carcinoid or lung cancer.
Also, ectopic production of CRH can be produced by bronchiali
carcinoid, medullary thyroid cancer or metastatic prostate cancer.
Hypertension, Diabetes mellitus, irregular menses, weight gain, androgen-type hirsutism, ecchymoses, myopathy, osteopenia, truncal obesity, neuropsychological disturbances and purple striae are all the clinical manifestations of Cushing’s Syndrome.
Diagnosis
Initially, screening tests are done for diagnostic evaluation of this abnormality. Among others, the major difficulty
observed in screening process is high falsepositive rates. Initial screening test like 24 hrs urinary measurement
of free cortisol (95-100% sensitive and 98% specific) are done. Alternately, test like 1-mg overnight dexamethasone
suppression is often done for screening Cushing’s Syndrome. A newer technique was made available for
evaluating Cushing’s Syndrome which involves measurement of salivary cortisol levels.
Congenital Adrenal Hyperplasia (CAH)
It is a group of inherited diseases which affects the levels of steroid hormones produced by adrenal cortex.
CAH results in defective activity of one of five enzymes in the adrenal cortex causing decreased production
of corticotropin, excess production of hormones proximal to the defective enzyme and glandular enlargement.
21-hydroxylase deficiency (defect in the P450c21enzyme) and 11-3-hydroxylase deficiency (defect in the P450c11 enzyme) are the two most common types of CAH. With 90% of cases causing by 21 hydroxylase deficiency, it is further classified into classic and non classic forms.
Salt-wasting and simple virilizing agents constitutes the classic forms of 21-hydroxylase deficiency CAH. In saltwasting 21-hydroxylase deficiency CAH, girls and boys may have Addisonian crisis and hypotension along with ambiguous genitalia in girls since birth. While, in simple virilizing 21-hydroxylase CAH, girls have ambiguous genitalia but do not experience Addisonian crisis. The non classic form of 21-hydroxylase deficiency is more common than the classic form.
Diagnosis
21-hydroxylase deficiency increases the hormone 17 Oh Progesterone along with excess testosterone and
DHEA-S helping in its diagnosis by looking for an increase in 17-hydroxyprogesterone from baseline to 60
minutes during a corticotropin-stimulation test.
Adrenal Tumor
Uncontrolled growth in the healthy cells can leads to the formation of a tumor. It can either be benign or
malignant. Further, these tumors can be functional (secreting excessive hormones) or non functional.
Among many, Adenomas are the most common form of adrenal gland tumor. Most of them are non functional while some are functioning with majority of them secreting cortisol. It is also called adrenocorticol adenoma.
Adrenocortical carcinoma is rare and can be functional or non functional. If it is functional, it may produce more than one hormones. Its location is deep in the retroperitoneum making it difficult for detection until they become large.
Incidentalomas are the term used to refer all those tumors found unexpectedly during diagnosis of some other conditions requiring PET-CT Scan or MRI scans of the abdomen. Most of these are benign but some can be malignant or functioning and needs to get removed.
Among others, pheochromocytoma, myelolipomas, paragangliomas, aldosteronomas and others are all capable of affecting adrenal gland or its functions.
Diagnosis
Several biochemical tests are done in order to determine the type of adrenal tumors especially if it is functioning
or non functioning. These test helps in determining catecholamines, ACTH, DHEAS, aldosterone, vanillylmandelic
acid levels along with assessing creatinine, plasma renin activity and others. Additionally, imaging techniques like
computed tomography (CT) or magnetic resonance imaging (MRI) can also be done for evaluating adrenal lesions
with primary goal of distinguishing benign from malignant.
Pheochromocytoma
These are paraganglionic chromaffin cell tumors which are relatively uncommon. Pheochromocytoma are found in
the adrenal medulla and the extra-adrenal paraganglia cells. Microscopic studies reveal whirls or sheets like
arrangement of these tumor cells having granular basophilic or eosinophilic cytoplasm with nuclear pleomorphism.
It is capable of producing, storing and secreting catecholamines. In some cases, it also secretes dopamine, Vasoactive intestinal peptide (VIP), Bendorphines and variety of other substances which can complicate the clinical manifestations.
Its symptoms are non-specific and are similar to other conditions, ultimately, referred as ‘great mimic’ by the professionals. Headache, hypertension, palpitations, tachycardia, anxiety, nausea are the few clinical features among others.
Diagnosis
Several biochemical tests like plasma catecholamines, and 24 hrs urine for catecholamines, noremetanephrines
and metanephrines are required for confirming the diagnosis. Once the clinical evidences are compelling about
its presence then only tumor localization by different imaging techniques should be considered, Techniques like
computed tomography (CT) or magnetic resonance imaging (MRI) are the recommended ones.
Adrenal Fatigue-Is it real?
it is often used by some doctors and healthcare practitioners to describe ‘overuse’ of adrenal glands due to
chronic stress; eventually resulting in functional failure of adrenal glands. According to a review on adrenal
fatigue, there were 6,40,000 results showing on Google when the term ‘adrenal fatigue’ was searched, despite
this, endocrinology societies has not recognized it due to the lack of evidences for its existence.
Conversely, some medical societies claims that adrenal fatigue is real. Additionally, certain tests like estimation of serum basal cortisol levels and salivary cortisol rhythms have been ordered for the patients suspected of this condition by some practitioners. And, if patient is found to have impaired results then they are treated with corticosteroids regardless of its cause.
The use of corticosteroid for the treatment of adrenal fatigue leads to considerable debate among medical professionals. Some stated the fact that use of corticosteroids showed significant improvement in patients. Others claim that several adrenal fatigue sufferer never received the adequate treatment due to strict diagnostic criteria set by endocrinologists for prescribing corticosteroids. In contrast to this, counterarguments were more focused on the risks involved in the use of corticosteroids. As, even in low doses, these steroids increases the risks of osteoporosis, myopathy, cardiovascular disease, psychiatric disorders and others.
Several theories on how adrenal failure could be the genesis for fatigue may be tempting for some along with its widespread use of the term but, the studies completely focused on this subject still remains few, that too only descriptive. Therefore, several questions still lingers to the mind of a fervid reader, questions like; Adrenal fatigue is actually a condition or not? Does it cause adrenal failure? What could be the useful Diagnostic Test for this conditions? And above all, whether ‘Adrenal Fatigue’ is real or not?