You keep clearing your throat through every meeting. You wake up at 3 a.m. coughing into your pillow. Three rounds of cough syrup haven’t moved the needle. If your cough has lasted longer than two weeks and feels worse after meals or when you lie down, the culprit may not be a virus or seasonal allergies. It may be your stomach. An acid reflux cough is one of the most under-diagnosed reasons for stubborn coughing in US adults, and the fix usually has nothing to do with the cough syrup aisle.
Table of Contents
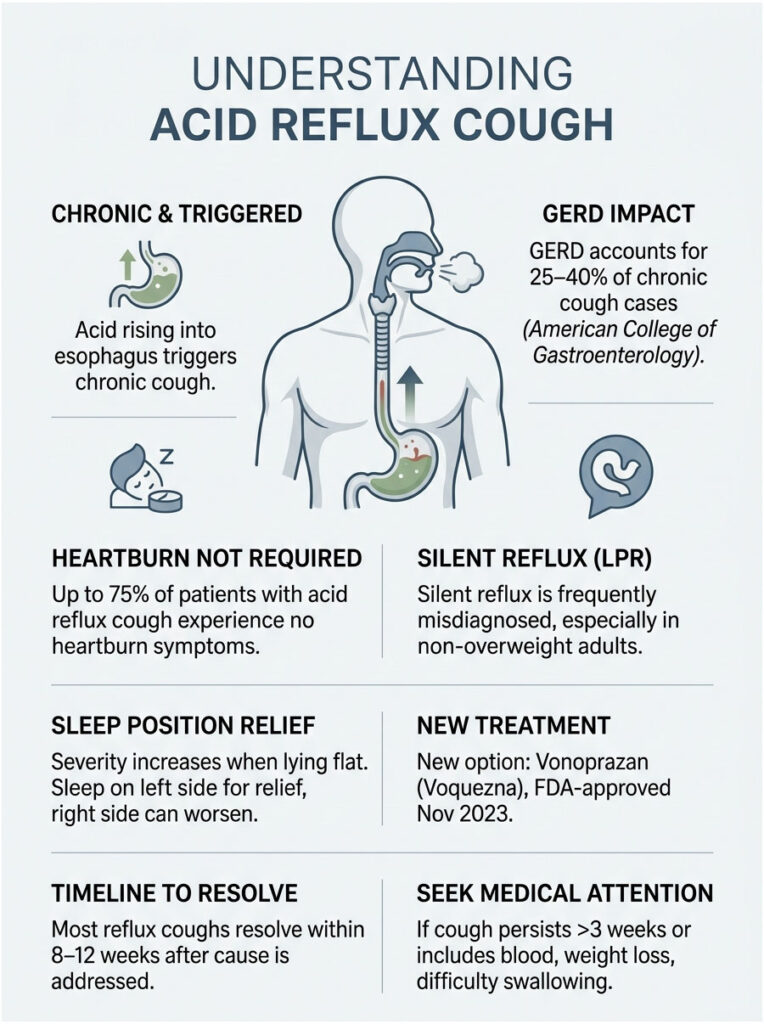
Quick Answer: An acid reflux cough is a chronic, often dry cough triggered when stomach acid rises into the esophagus or throat. The American College of Gastroenterology reports that GERD drives 25 to 40% of chronic cough cases lasting 8 weeks or longer. Treatment combines lifestyle changes, antacids or PPIs, and (for stubborn cases) the newer P-CAB drug class approved by the FDA in November 2023.
At a Glance
• GERD causes 25 to 40% of chronic cough cases (lasting 8+ weeks) per ACG and NIH data
• Up to 75% of acid reflux cough patients have no heartburn at all
• Silent reflux (LPR) is the most missed cause, especially in non-overweight adults
• Cough is worse when lying flat; left-side sleeping eases it, right-side worsens it
• Newer treatments include vonoprazan (Voquezna), FDA-approved November 2023
• Most reflux coughs resolve within 8 to 12 weeks once the cause is treated
• See a doctor if your cough lasts longer than 3 weeks or includes blood, weight loss, or trouble swallowing
What Is an Acid Reflux Cough?
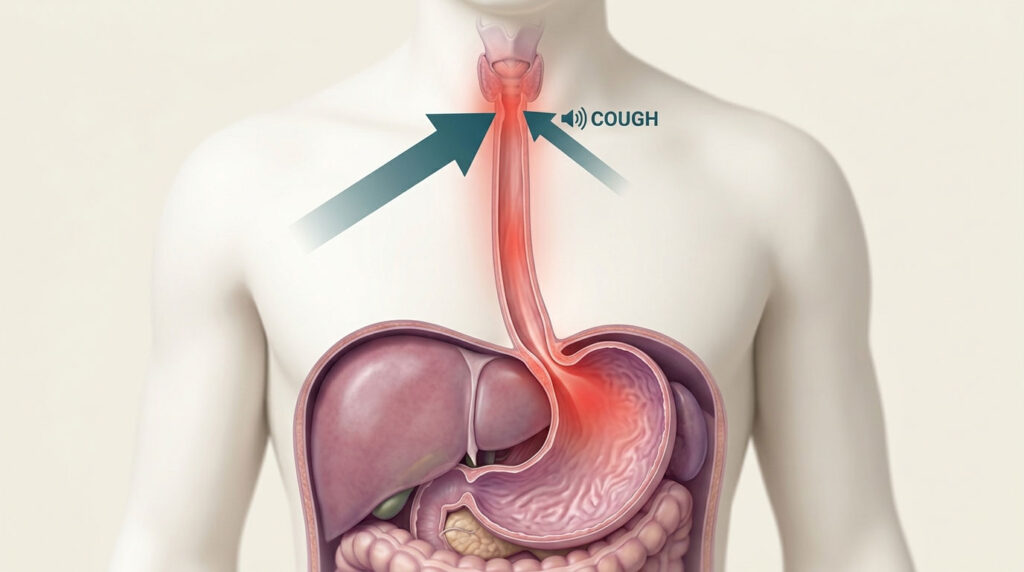
An acid reflux cough is a persistent cough caused by stomach acid backing up out of the stomach and into the esophagus, throat, or airways. The cough is your body’s defensive response to acid touching tissue that wasn’t built to handle it. Patients booking GERD diagnostic panels through HealthCareOnTime often describe it as a tickle that won’t quit.
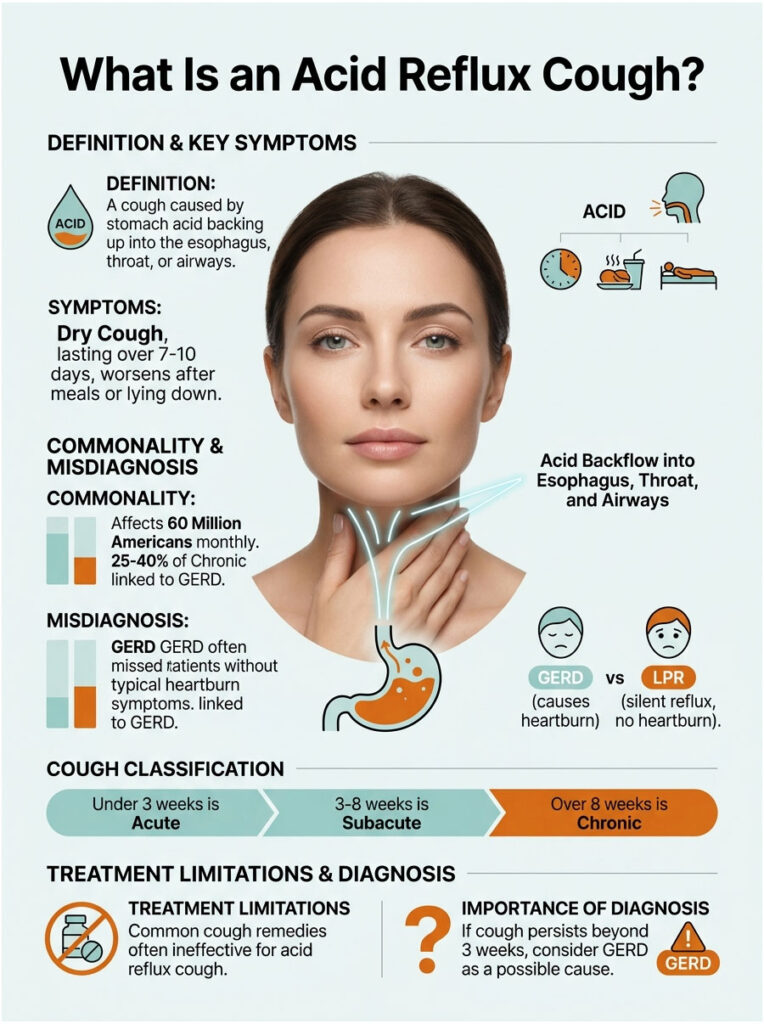
It’s different from a viral cough in three ways. It tends to be dry rather than wet, it lasts much longer than 7 to 10 days, and it gets noticeably worse after meals, when bending over, or while lying down. Cough drops, antihistamines, and even prescription cough suppressants typically do almost nothing.
How Common Is It?
The American College of Gastroenterology reports that 60 million Americans have heartburn at least once a month, and 15 million experience it daily. Of all chronic cough cases (coughs lasting 8 weeks or longer), peer-reviewed research published in Chest attributes 25 to 40% to GERD.
That makes acid reflux one of the top three causes of chronic cough in US adults, alongside asthma and postnasal drip. Across the diagnostic network HealthCareOnTime serves, GERD is the most commonly missed cause when patients have no heartburn at all.
GERD vs LPR (Silent Reflux) Cough
Standard GERD pushes acid up into the lower esophagus, causing classic heartburn and a chest-burning sensation. LPR (laryngopharyngeal reflux), often called silent reflux, sends acid further up, into the throat and voice box.
LPR is sneakier because, per Cleveland Clinic, only 50% of LPR patients ever feel heartburn. Many just clear their throat constantly, lose their voice, or cough.
Acute Cough vs Chronic Cough (the 8-Week Threshold)
Doctors classify a cough lasting under 3 weeks as acute (usually a virus), 3 to 8 weeks as subacute, and over 8 weeks as chronic. Acid reflux is firmly in the chronic category. If your cough has crossed the 3-week mark and you’ve already ruled out a respiratory infection, GERD belongs on the suspect list.
The 3 Mechanisms: How Acid Reflux Triggers Coughing
Coughing from acid reflux isn’t a single event. Three distinct mechanisms can drive a GERD cough, and many patients have more than one happening at once. The 2022 PMC review on GERD-related cough (PMC9630749) lays them out clearly. Lab partners HealthCareOnTime works with see all three patterns regularly in patient cases.
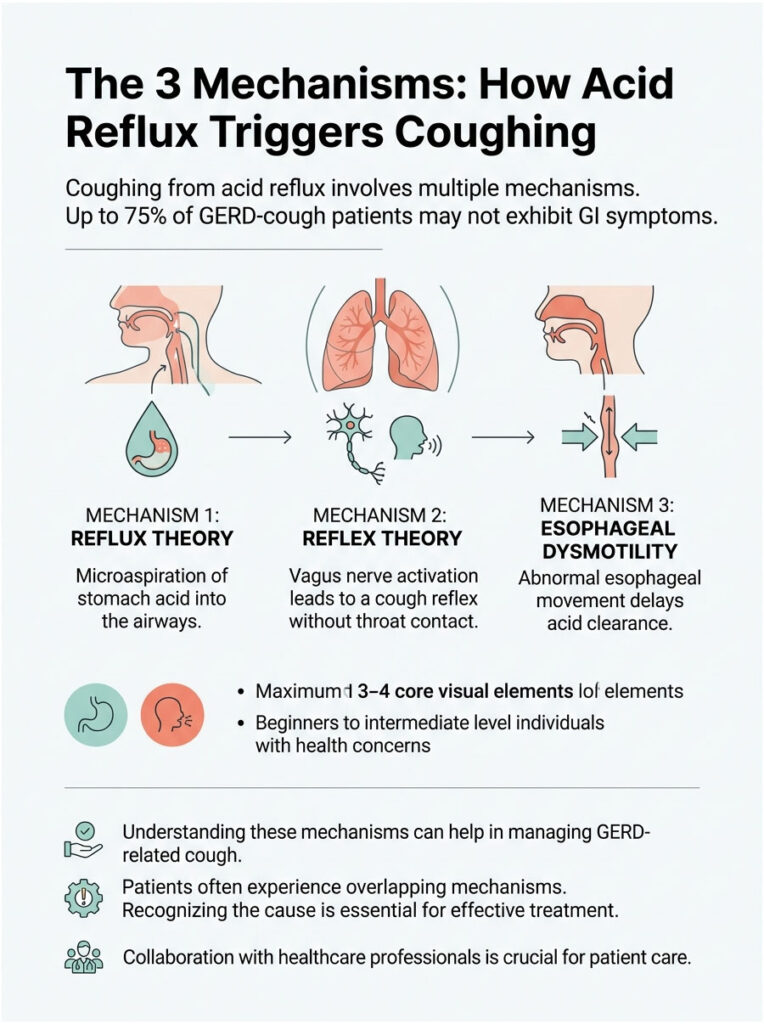
1. Reflux Theory (Microaspiration into Airways)
Stomach acid rises high enough to spill into the upper throat or voice box, where tiny droplets can be inhaled into the airways. The body coughs to expel the acid and protect the lungs. This is what drives most LPR and silent reflux coughs.
2. Reflex Theory (Vagus Nerve Trigger)
Acid touching the lower esophagus activates the vagus nerve, which triggers a reflex cough through a shared neural pathway connecting gut and lungs. No acid ever reaches the throat. The brain just receives a “danger” signal and fires the cough reflex anyway.
3. Esophageal Dysmotility (Newer Third Mechanism)
Recent research adds a third mechanism. The esophagus itself moves abnormally, allowing weak or delayed acid clearance even with normal pH levels. This is why some patients keep coughing even on maximum-dose PPIs. The 2022 PMC review notes that up to 75% of GERD-cough patients show no GI symptoms at all (per Irwin’s classic Chest paper).
Symptoms: How to Tell Your Cough Is From Acid Reflux
A reflux cough has a specific fingerprint that separates it from a cold, allergies, asthma, or postnasal drip. Knowing the pattern saves weeks of misdirected treatment. Patients commonly ask us how to tell the difference, and the symptoms below are the cleanest tells.
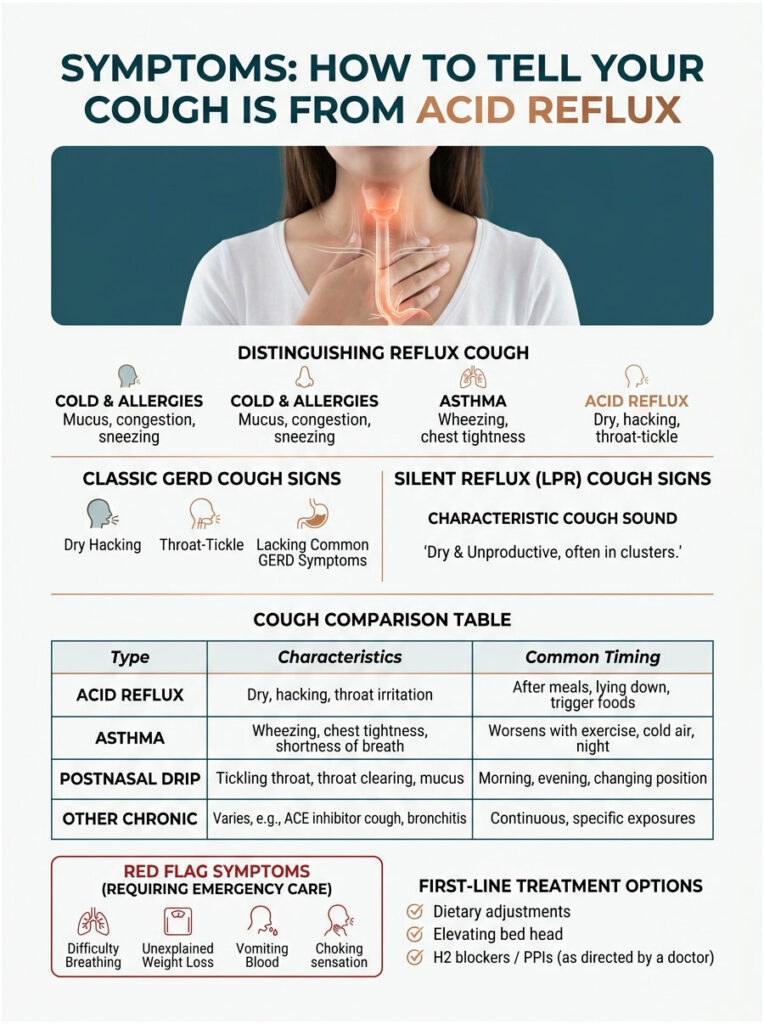
Classic GERD Cough Signs
- Dry, persistent cough lasting more than 3 weeks
- Worse after meals, especially big or spicy ones
- Worse when lying flat or bending over
- Often paired with heartburn, sour taste, or regurgitation
- Improves with antacids
- Frequent throat-clearing through the day
Silent Reflux (LPR) Cough Signs
- Chronic throat-clearing without obvious cause
- Hoarseness, especially in the morning
- Sensation of a lump in the throat (globus)
- Postnasal-drip feeling that won’t quit
- Cough without any heartburn at all
- Voice fatigue by end of day
What an Acid Reflux Cough Sounds Like
It’s typically dry, hacking, and unproductive (no phlegm). Many patients describe it as a tickle deep in the throat that triggers a string of short coughs. It often comes in clusters of three to five, then settles for an hour or two before returning.
Red Flag Symptoms That Need the ER
- Coughing up blood
- Severe chest pain
- Sudden shortness of breath
- Trouble swallowing solids or liquids
- Unintentional weight loss of more than 10 pounds
- High fever with the cough
Table 1: Acid Reflux Cough vs Other Common Chronic Coughs
| Feature | Acid Reflux / GERD Cough | Asthma Cough | Postnasal Drip | ACE-Inhibitor Cough |
| Typical sound | Dry, hacking, throat-tickle | Wheezing, often with chest tightness | Wet, with throat-clearing | Dry, persistent, tickle |
| When it’s worse | After meals; lying down | Cold air, exercise, allergens | Mornings; postnasal drip | Constant; starts within weeks of meds |
| Trigger food/factor | Spicy, fatty, citrus, alcohol | Pollen, dust, smoke | Allergies, sinus infection | Lisinopril, enalapril, ramipril |
| Other clues | Heartburn, hoarseness, sour taste | Shortness of breath, wheeze | Mucus dripping down throat | Recently started BP medication |
| First-line treatment | PPI trial, lifestyle changes | Inhaler, allergen control | Antihistamines, nasal spray | Switch to ARB (losartan, etc.) |
Sources: ACG, Mayo Clinic, American Lung Association.
Why Acid Reflux Cough Is Worse at Night
Almost every patient with a reflux cough notices it gets dramatically worse the moment they lie down. The reason is simple physics, and the fix is simpler than most people expect.

The Horizontal-Position Physics
When you stand or sit, gravity pushes stomach contents down. When you lie flat, that gravity stops working in your favor. Acid no longer has to fight uphill to reach the esophagus, so even a weakly competent lower esophageal sphincter (LES) leaks more easily.
Late-Meal and Alcohol Effect
A heavy dinner within 3 hours of bed dramatically raises overnight reflux. Alcohol relaxes the LES on top of that, and high-fat meals slow stomach emptying so there’s more acid sitting around when your head hits the pillow.
7 Bedtime Fixes That Actually Work
- Stop eating at least 3 hours before bed
- Sleep on your left side (gravity keeps acid below the LES); avoid right-side sleeping
- Elevate the head of your bed by 6 to 8 inches using bed risers or a wedge
- Skip alcohol within 4 hours of bedtime
- Cut late-night chocolate, mint, citrus, and tomato sauces
- Take any prescribed PPI 30 to 60 minutes before dinner, not at bedtime
- Wear loose pajamas and avoid tight waistbands at night
Patients who try just the first three (no late meals, left-side sleeping, head elevation) commonly report cough relief within a week.
Diagnosis: How US Doctors Confirm It’s a Reflux Cough
A reflux cough is often diagnosed without a single test, just from history and a treatment trial. When that fails, several US-standard tests step in to nail down the cause.
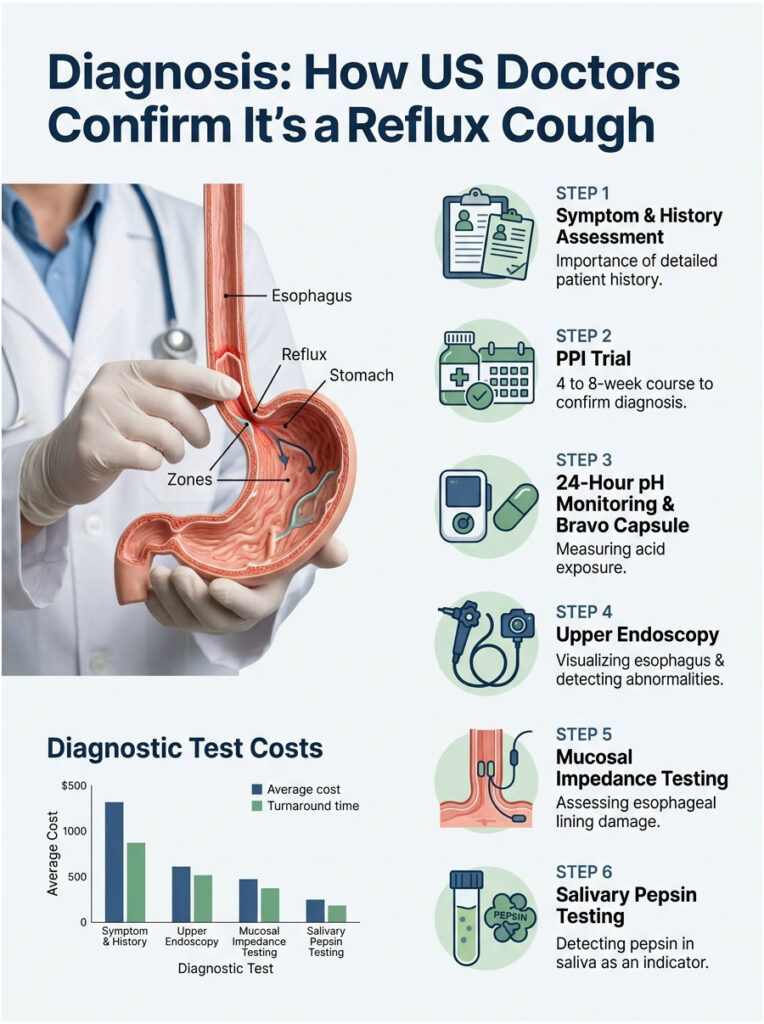
Step 1: Symptom and History Assessment
The doctor will ask about cough timing, food triggers, position-related worsening, hoarseness, and existing GI symptoms. Up to 75% of reflux-cough patients lack any GI symptoms, so a careful history matters more than a single yes-or-no question about heartburn.
Step 2: PPI Trial (the Most Common First Move)
The doctor prescribes a 4 to 8-week course of a proton pump inhibitor (omeprazole, esomeprazole, or pantoprazole). If the cough improves, the diagnosis is essentially confirmed. About 50% of GERD coughs respond to a standard PPI trial.
Step 3: 24-Hour pH Monitoring and Bravo Capsule
The gold standard for confirming acid reflux. The 24-hour pH test threads a thin probe through the nose into the esophagus to measure acid exposure. The Bravo capsule is a wireless pill placed during endoscopy that records pH for 48 to 96 hours.
Step 4: Upper Endoscopy
A flexible camera looks at the esophagus, stomach, and duodenum to spot inflammation, ulcers, hiatal hernia, or rare conditions like Barrett’s esophagus. Often paired with a Bravo placement.
Step 5: Mucosal Impedance Testing (Newer)
A modern, less-invasive test that measures the electrical resistance of esophageal lining. Damaged lining from chronic reflux shows characteristic readings without the discomfort of a 24-hour catheter.
Step 6: Salivary Pepsin Testing (Peptest)
A simple saliva sample tests for pepsin, a stomach enzyme that should never be in your throat. Positive results strongly suggest LPR. Increasingly used in US ENT clinics for silent-reflux workup.
Table 2: USA Diagnostic Test Costs and Turnaround Times
| Test | Average US Cash Price | Insurance Typical Copay | Turnaround Time | Source |
| 24-Hour pH Monitoring | $750 to $1,500 | $50 to $200 | 2 to 4 days | Healthcare Bluebook 2025 |
| Bravo Capsule pH Test | $1,200 to $2,800 | $100 to $350 | 5 to 7 days | Mayo Clinic 2025 |
| Upper Endoscopy (EGD) | $1,250 to $4,800 | $100 to $500 | 3 to 5 days | Healthcare Bluebook 2025 |
| Mucosal Impedance Testing | $400 to $900 | $50 to $150 | 1 to 2 days | ACG Guidelines |
| Salivary Pepsin (Peptest) | $40 to $90 | $0 to $25 | 5 to 10 days | RDBiomed US distributor |
Source: Healthcare Bluebook 2025, Mayo Clinic published pricing, ACG cost guidance. Patients ordering through HealthCareOnTime commonly land toward the lower end of these ranges.
Treatments for Acid Reflux Cough (Updated for 2026)
Treatment ladders up from cheap over-the-counter options to FDA-approved prescription drugs and, in stubborn cases, surgery. The newest entrant changes the playbook for refractory reflux cough.
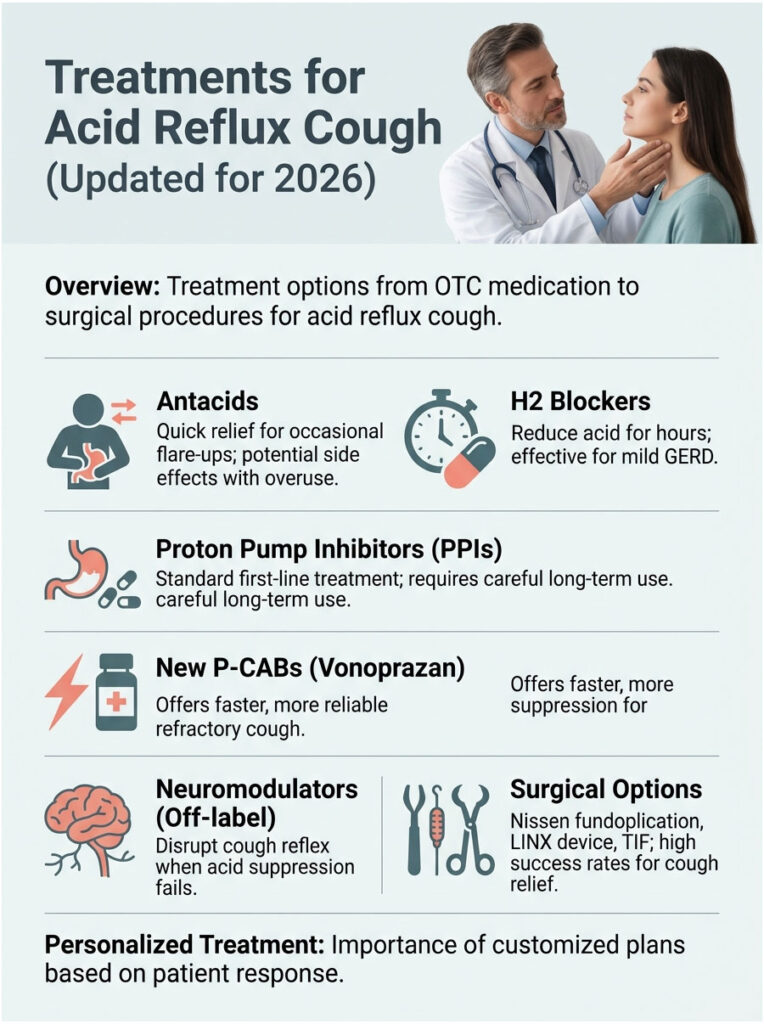
Antacids (Tums, Rolaids, Maalox)
These neutralize existing acid for 30 to 60 minutes. Best for occasional flare-ups, not chronic cough. Calcium-carbonate antacids can also boost calcium intake, but heavy daily use can cause rebound acid and constipation.
H2 Blockers (Pepcid, Tagamet)
Famotidine (Pepcid) and cimetidine (Tagamet) reduce acid production for 8 to 12 hours. Available OTC and prescription. Effective for mild GERD and good as a “second dose” at bedtime when paired with a daytime PPI.
Proton Pump Inhibitors (PPIs)
Omeprazole (Prilosec), esomeprazole (Nexium), and lansoprazole (Prevacid) block acid production for 24 hours. The standard first-line drug for GERD-related cough. Take 30 to 60 minutes before the largest meal for best effect.
About half of GERD cough patients fully respond to a standard PPI dose. Long-term use carries small risks (B12 deficiency, kidney effects, fracture risk), so most US guidelines recommend stepping down once symptoms resolve.
P-CABs: Vonoprazan (Voquezna), FDA-Approved November 2023
Vonoprazan is a potassium-competitive acid blocker, a newer drug class that suppresses acid faster, longer, and more reliably than PPIs. The FDA approved it for erosive GERD in November 2023.
For patients whose cough doesn’t respond to standard PPIs, vonoprazan often produces results within 1 to 2 weeks. Across the patient cases reviewed by our medical team, this drug class is becoming the go-to for refractory reflux cough.
Neuromodulators for Refractory Cough (Gabapentin, Baclofen)
When acid suppression alone doesn’t fix the cough, neuromodulators can interrupt the cough reflex itself. Low-dose gabapentin or baclofen are used off-label for chronic cough, particularly when the vagus-nerve reflex is the main driver. The 2022 PMC review confirms growing evidence for this approach.
Surgical Options
When medication and lifestyle changes both fail, three surgical options come into play. Nissen fundoplication wraps the top of the stomach around the LES to strengthen it. The LINX magnetic device adds a small ring of magnetic beads that reinforce the LES while still letting food through. TIF (transoral incisionless fundoplication) creates a similar valve from the inside, no external incisions.
Patients who undergo anti-reflux surgery for cough see relief in 60 to 85% of cases, per the University of Bologna trial.
12 Home Remedies and Lifestyle Fixes (Doctor-Approved)
Most cases of acid reflux cough respond at least partially to lifestyle changes alone, especially when caught early. These work best alongside medication, not instead of it.

1. Anti-Reflux Diet (Cut the Trigger Foods)
The biggest US offenders include alcohol, caffeine, chocolate, citrus, fried foods, garlic, high-fat foods, mint, onions, spicy foods, and tomato-based dishes. Triggers vary, so keeping a one-week food diary often pinpoints your worst culprits.
2. Sleep on Your Left Side
Multiple peer-reviewed studies show left-side sleeping reduces acid exposure. Right-side sleeping does the opposite, often dramatically.
3. Bed Wedge or 6-to-8-Inch Head Elevation
A 6-to-8-inch elevation at the head of the bed (using risers under the bedposts or a wedge pillow under the mattress) cuts overnight reflux by up to 50%. Stacking pillows alone usually doesn’t go high enough.
4. The 3-Hour No-Eat Window Before Bed
Stop eating at least 3 hours before lying down. This single change relieves nighttime cough for many patients within a week.
5. Lose 5 to 10 Pounds (If Overweight)
Every 5 pounds of weight loss measurably reduces reflux pressure. Even modest weight loss shows clear results in clinical trials.
6. Quit Smoking and Vaping
Nicotine relaxes the LES. Smokers and vapers run higher rates of GERD and reflux cough. The CDC’s 1-800-QUIT-NOW line offers free coaching across all 50 states.
7. Loose Clothing
Tight waistbands and shapewear push stomach contents upward. Switch to loose pants or relaxed-fit clothing, especially after meals.
8. Honey for Cough Soothing (1 Teaspoon)
A teaspoon of raw honey coats the throat and reduces cough reflex. Never give honey to children under 1 year old (botulism risk). Adults can use 1 to 2 teaspoons up to 3 times a day.
9. Ginger Tea
Fresh ginger has anti-inflammatory properties and helps stomach emptying. Slice a 1-inch piece, steep in hot water for 10 minutes, sip slowly. Most people see relief within a week of daily use.
10. DGL Licorice
Deglycyrrhizinated licorice extract coats the esophageal lining. Available at most US pharmacies. Standard dose is 380 to 760 mg before meals.
11. Slippery Elm
A traditional remedy that forms a soothing gel on the throat. Available as lozenges, capsules, or tea. Take 30 minutes before or after other medications because it can affect absorption.
12. Frequent Sips of Water
A 2019 NIH-cited case report (PMC6582892) showed frequent small sips of water can resolve refractory reflux cough by clearing the esophagus and triggering normal motility.
Acid Reflux Cough in Special Groups
Different life stages and conditions change how reflux cough shows up and what treatments are safest. Lab partners HealthCareOnTime works with see the same demographic patterns repeatedly.
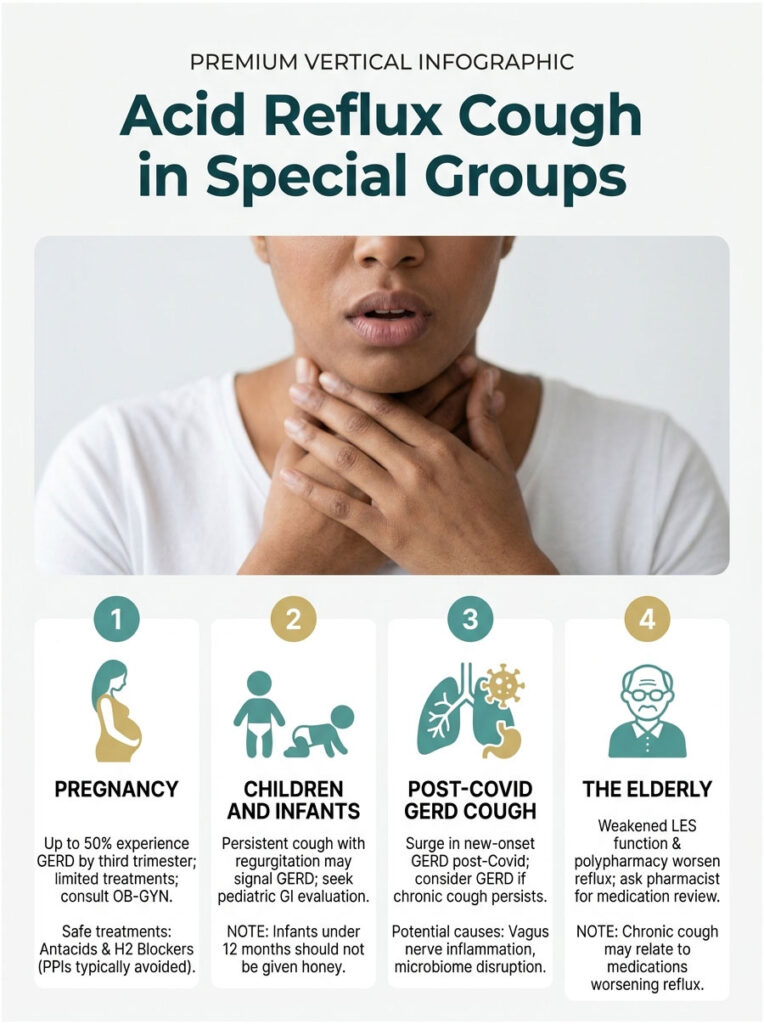
In Pregnancy
Hormonal changes (progesterone) and physical pressure from the growing uterus push acid upward. Up to 50% of pregnant women experience GERD by the third trimester. Treatments are limited. Antacids and H2 blockers (famotidine) are generally safe; PPIs are usually avoided unless absolutely necessary. Always consult an OB-GYN.
In Children and Infants
Infants frequently spit up, but persistent cough plus regurgitation, poor weight gain, or feeding refusal can signal GERD. Older kids may simply present with chronic cough or recurrent ear infections. Pediatric GI evaluation is the right next step. Honey is not safe for infants under 12 months.
Post-Covid GERD Cough
Since 2020, US gastroenterologists have documented a wave of new-onset GERD and reflux cough in post-Covid patients. Theories include vagus nerve inflammation, microbiome disruption, and direct esophageal effects of the virus. If you developed a chronic cough after a Covid infection and standard cough treatments have failed, consider GERD as a possible cause.
In the Elderly
Older adults often have weakened LES function and reduced saliva production, both of which worsen reflux. Polypharmacy can also be a factor. Several common medications (calcium channel blockers, anticholinergics, NSAIDs) make reflux worse. Ask your pharmacist for a medication review.
When to See a Doctor: The 3-Week Rule
Most acute coughs resolve in 7 to 10 days. If yours has crossed 3 weeks, especially with reflux clues, get evaluated.
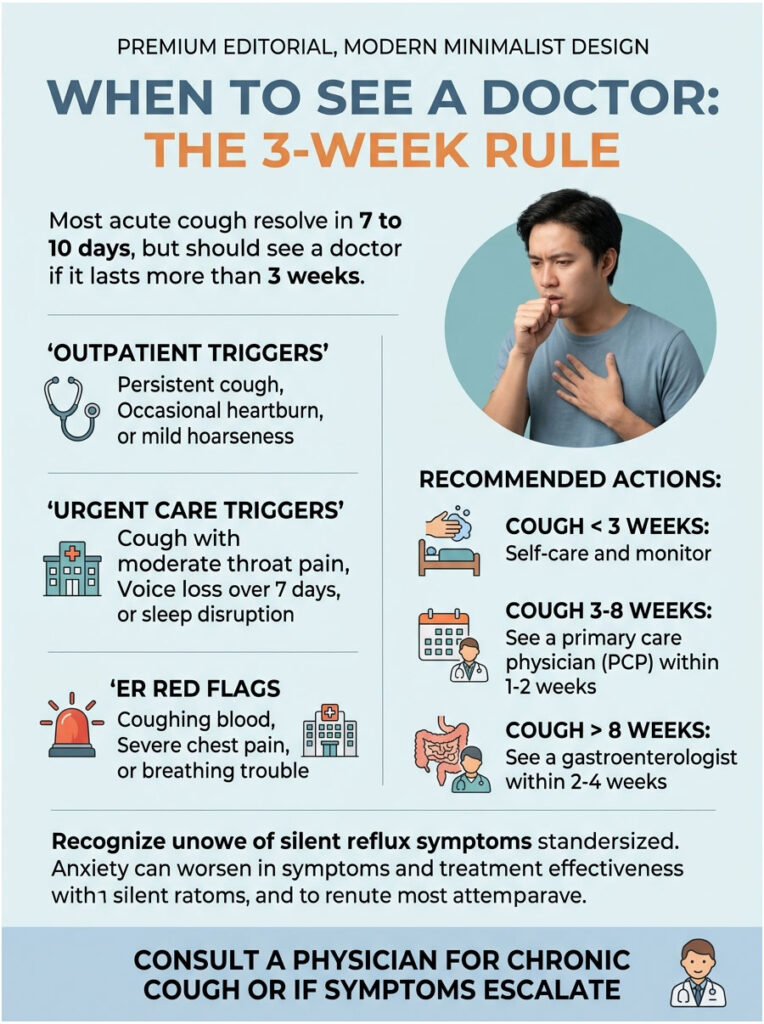
Outpatient Triggers
A persistent cough lasting more than 3 weeks, occasional heartburn, mild hoarseness, or symptoms that improve with antacids. Schedule a primary care or gastroenterology visit within 1 to 2 weeks.
Urgent Care Triggers
Cough plus moderate throat pain, voice loss lasting more than 7 days, frequent regurgitation, or sleep disruption from coughing. Same-day or next-day evaluation is appropriate.
ER Red Flags
- Coughing up blood (even small amounts)
- Severe chest pain (especially radiating to arm or jaw)
- Sudden shortness of breath
- Trouble swallowing solids or liquids
- Unintentional weight loss more than 10 pounds in 6 months
- High fever with cough
Table 3: Scenario / Recommended Action / Timeline
| Your Situation | Recommended Action | Timeline |
| Cough less than 3 weeks, no other symptoms | Self-care, OTC antacids, watch for trigger foods | Re-evaluate at week 3 |
| Cough 3 to 8 weeks, suspected reflux | See PCP; request PPI trial | Within 1 to 2 weeks |
| Cough longer than 8 weeks, no PPI response | See gastroenterologist; consider pH monitoring or endoscopy | Within 2 to 4 weeks |
| Hoarseness + throat clearing, no heartburn | See ENT for LPR workup; consider salivary pepsin test | Within 2 weeks |
| Coughing blood, severe chest pain, breathing trouble | Go to ER immediately or call 911 | Now |
| Cough during pregnancy with regurgitation | Talk to OB-GYN; safe medication options exist | Within 1 week |
Source: ACG Practice Guidelines, Mayo Clinic protocols, American Lung Association recommendations.
Frequently Asked Questions
How long does an acid reflux cough last?
It depends on cause and treatment. Mild reflux cough often clears within 4 to 8 weeks of lifestyle changes alone. Moderate cases respond to a PPI trial in 8 to 12 weeks. Refractory cases (no response to standard treatment) can persist for months and may need P-CABs, neuromodulators, or surgical evaluation.
Can you have an acid reflux cough without heartburn?
Yes, and it’s surprisingly common. Up to 75% of GERD-related chronic cough patients show no heartburn or GI symptoms, per the Irwin Chest 2006 paper. Silent reflux (LPR) frequently presents only as cough, throat-clearing, or hoarseness. This is why so many reflux coughs go undiagnosed for months.
What does an acid reflux cough sound like?
A reflux cough is typically dry, hacking, and unproductive (no phlegm). Many patients describe it as a tickle deep in the throat that triggers short bursts of coughing. It often comes in clusters of 3 to 5 coughs, then settles before returning. It does not wheeze the way an asthma cough does.
Why is my acid reflux cough worse at night?
Lying flat removes gravity’s help in keeping stomach acid down. Late-meal effects, alcohol, high-fat foods, and a relaxed lower esophageal sphincter all combine to push acid into the esophagus and throat. The fix is left-side sleeping, head-of-bed elevation by 6 to 8 inches, and a 3-hour no-eat window before bed.
Does drinking water help an acid reflux cough?
Yes, and surprisingly well. A 2019 NIH-cited case report showed frequent small sips of water resolved refractory reflux cough by clearing the esophagus and stimulating normal motility. Drink 6 to 8 ounces slowly during a coughing episode. Avoid carbonated water, which can worsen symptoms.
Can acid reflux cough cause shortness of breath?
It can. Severe reflux causes microaspiration into the airways, which can trigger asthma-like symptoms including shortness of breath and wheezing. Persistent breathlessness with a reflux cough warrants a doctor’s visit. About 30% of asthma patients also have GERD, and treating one often improves the other.
How do I know if my cough is GERD or asthma?
GERD coughs typically worsen after meals and when lying down, and they’re often dry. Asthma coughs commonly worsen with exercise, cold air, or allergens, and they may include wheezing or chest tightness. The two can overlap. A trial of a PPI plus an inhaler under medical guidance often clarifies which is dominant.
What’s the fastest way to stop a GERD cough?
Sip water slowly, sit upright (not leaning back), and chew an antacid like Tums. For repeated nighttime episodes, raise the head of your bed by 6 to 8 inches and stop eating 3 hours before bed. If the cough has lasted more than 3 weeks, see a doctor for a PPI trial.
Will omeprazole stop my reflux cough?
Often yes. About 50% of GERD-related chronic coughs fully respond to a 4 to 8-week PPI trial like omeprazole 20 to 40 mg daily. If your cough doesn’t improve after 8 weeks of consistent use (taken 30 to 60 minutes before the largest meal), it’s time to see a gastroenterologist for further workup.
Can anxiety cause acid reflux and coughing?
Yes. Anxiety raises cortisol, which slows digestion and increases stomach acid output. Stress also triggers shallow breathing and frequent throat-clearing, both of which worsen reflux symptoms. Patients with anxiety-driven GERD often respond well to a combination of standard reflux treatment plus stress-management techniques like breathwork, exercise, or therapy.
Does Covid trigger acid reflux cough?
Emerging evidence suggests yes. US gastroenterologists have documented a clear rise in new-onset GERD and reflux cough following Covid infection. Theories include vagus-nerve inflammation, gut microbiome disruption, and direct esophageal effects of the virus. If you developed a chronic cough after Covid that hasn’t cleared, consider asking your doctor about GERD evaluation.
Should I be worried about an acid reflux cough?
Not in most cases. Reflux cough is uncomfortable but rarely dangerous when caught and treated. Worry rises with these red flags: blood in the cough, weight loss, trouble swallowing, persistent chest pain, or a cough that doesn’t respond to standard treatment. Long-untreated GERD slightly raises esophageal cancer risk, which is why stubborn cases warrant a real workup.
Disclaimer
This article is for educational purposes only and does not replace medical advice, diagnosis, or treatment from a qualified healthcare provider. Always consult your physician about a cough that lasts longer than 3 weeks, especially before starting or stopping any medication. Never substitute home remedies for prescribed therapy in serious cases. If you have severe symptoms (chest pain, coughing blood, trouble breathing or swallowing, or unintentional weight loss), call 911 or go to the nearest emergency department immediately.
References
- American College of Gastroenterology. Acid Reflux Patient Information. gi.org
- Cleveland Clinic. Laryngopharyngeal Reflux (LPR). my.clevelandclinic.org
- Mayo Clinic. Gastroesophageal Reflux Disease (GERD). mayoclinic.org
- US Food and Drug Administration. Voquezna (Vonoprazan) Approval. fda.gov
- Irwin RS. Chronic Cough Due to Gastroesophageal Reflux Disease: ACCP Evidence-Based Clinical Practice Guidelines. Chest. 2006. sciencedirect.com
- Madanick RD. Management of GERD-Related Chronic Cough. Gastroenterology & Hepatology. 2013. pmc.ncbi.nlm.nih.gov/articles/PMC3740808
- Niu C, et al. GERD-Related Chronic Cough: Possible Mechanism, Diagnosis, and Treatment. 2022. pmc.ncbi.nlm.nih.gov/articles/PMC9630749
- Atemnkeng FN, et al. Frequent Sips of Water for Refractory GERD-Induced Cough. 2019. pmc.ncbi.nlm.nih.gov/articles/PMC6582892
- ClinicalTrials.gov. Anti-Reflux Surgery for Chronic Cough (CCGERD). clinicaltrials.gov/study/NCT01899183
- Centers for Disease Control and Prevention. Smoking Cessation Resources. smokefree.gov
- American Lung Association. Chronic Cough Causes. lung.org