
In my years of gastroenterology practice, I have seen the same scenario play out hundreds of times. A patient walks in convinced they have too much stomach acid. They carry a bag full of antacids. But when we actually run the tests, the results tell a completely different story: their stomach is not producing enough acid.
Table of Contents
This clinical paradox quietly affects millions of Americans who end up treating the wrong condition for years. When your digestive system lacks the acidic power it needs, the consequences ripple across your entire body. That burning sensation you blame on excess acid? It could actually be caused by a lack of gastric juice, which triggers a chain of digestive failures that closely mimic acid overproduction.
Modern medicine needs a shift in perspective here. Suppressing acid is rarely the right answer for chronic gut problems. The real path to healing starts with restoring your body’s natural digestive fire.
What Is Hypochlorhydria?
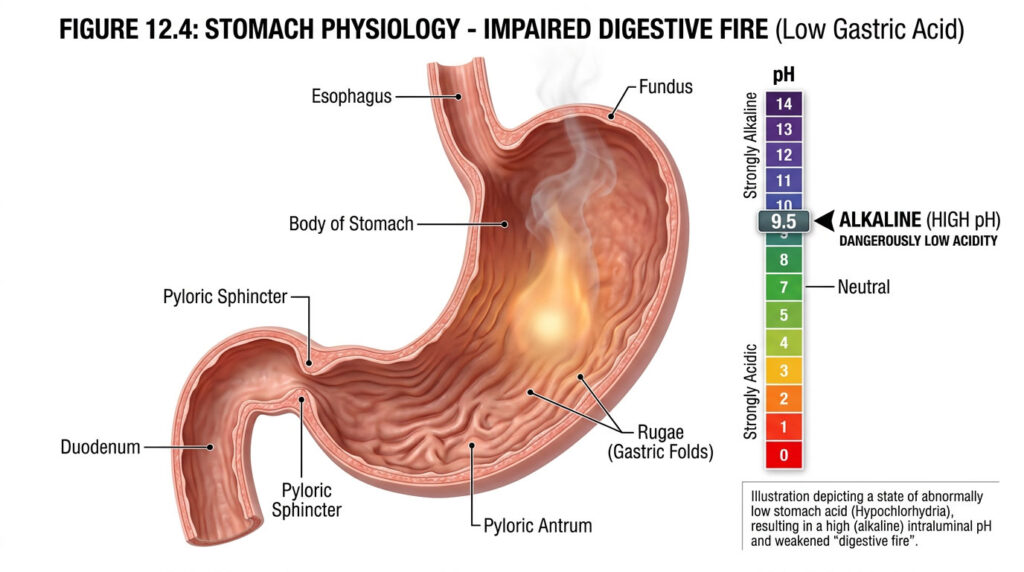
Hypochlorhydria is a clinical condition in which the stomach’s parietal cells fail to produce adequate hydrochloric acid (HCl). This stomach acid deficiency disrupts protein digestion, blocks essential mineral absorption, and allows harmful bacteria to survive. Over time, it leads to significant gastrointestinal distress and systemic malnutrition.
Key Statistics on Gastric Health
- Over 30% of adults above 60 develop atrophic gastritis, per the National Institutes of Health.
- Healthy fasting gastric pH sits between 1.5 and 3.5 for proper digestion.
- An estimated 20% of long-term acid-blocking medication users develop unrecognized stomach acid deficiency.
- More than 50% of patients with unexplained iron deficiency improve after correcting their gastric pH.
- Undiagnosed hypochlorhydria is a leading root cause in over 60% of persistent SIBO cases.
- Around 40% of patients with autoimmune thyroid conditions also carry antibodies that attack their stomach cells.
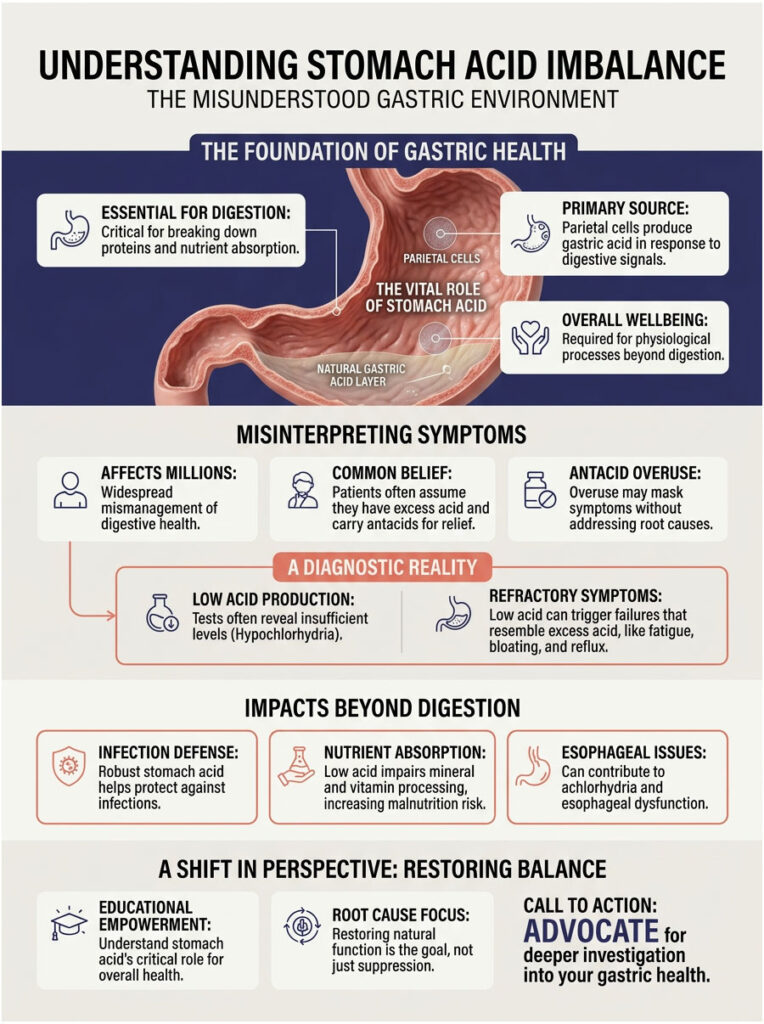
The Misunderstood Gastric Environment
As a Board-Certified Gastroenterologist, I witness the downstream effects of suppressed stomach acid every single day. Restoring the gastric pH barrier is foundational to overall health. True wellness is impossible when your primary digestive fire has been extinguished.
Many patients spend years bouncing between diagnoses for their bloating, fatigue, and reflux. They go through endless scans and elimination diets. More often than not, the missing link is hypochlorhydria.
Here is the uncomfortable truth. When we fail to recognize a stomach struggling to produce acid, we miss the root cause entirely. The conventional medical system runs on 15-minute appointments, and that is barely enough time to write a prescription for an acid blocker, let alone investigate underlying glandular failure.
The stomach relies on specialized structures called parietal cells. These microscopic cells pump out hydrochloric acid around the clock. When they start to fail, you develop a dangerous stomach acid deficiency. Over time, this can progress to achlorhydria, which is the complete absence of stomach acid. It also triggers lower esophageal sphincter dysfunction, and that exact dysfunction causes the reflux patients desperately try to medicate away.
Think about it this way. If your stomach cannot break down food, that food simply sits there. It ferments, produces gas, and creates immense upward pressure. This pressure forces whatever weak acid remains straight into your esophagus.
We have been conditioned to fear stomach acid. Pharmaceutical ads paint acid as the enemy of a comfortable life. In clinical reality, robust stomach acid is your best friend and your primary defender against disease. Without it, you are leaving your front door wide open to infections and malnutrition.
How Your Stomach Actually Produces Acid
The Role of Parietal Cells and Hydrochloric Acid
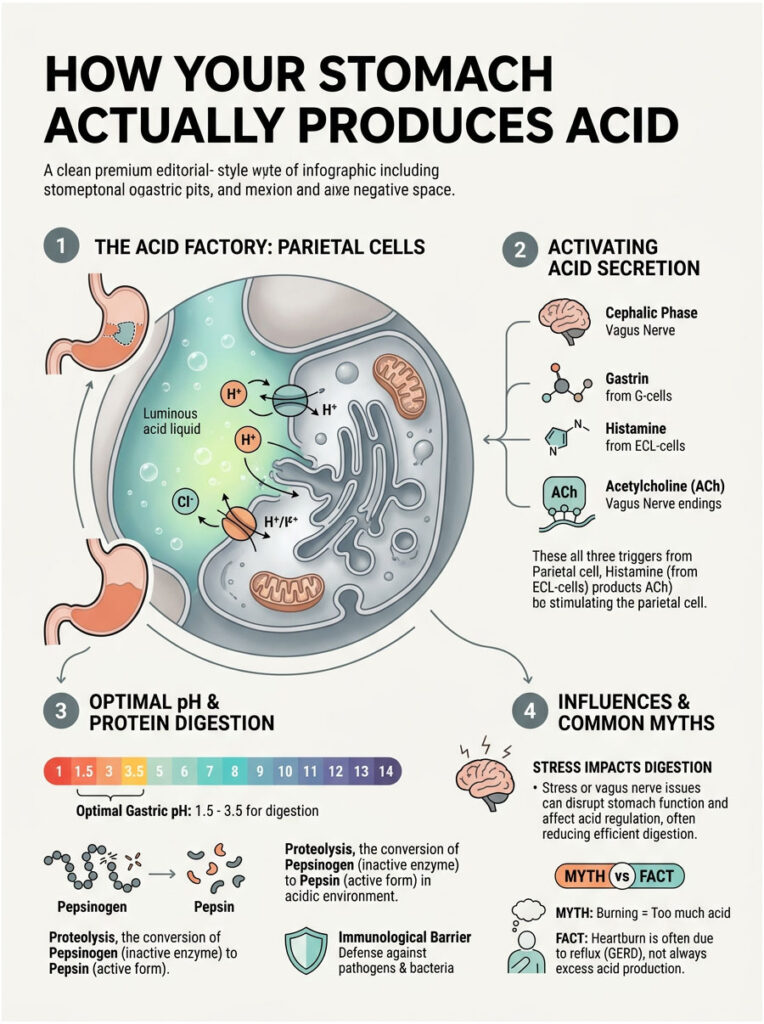
To understand what goes wrong, you first need to know how a healthy stomach works. The stomach lining is packed with millions of microscopic gastric glands, and deep within those glands live the parietal cells. These are the biochemical powerhouses of your entire digestive tract.
Parietal cells rely on three chemical triggers to release acid: gastrin, histamine, and acetylcholine. When you eat, these chemicals signal the parietal cells to activate their proton pumps. The pumps push hydrogen ions into the stomach cavity against a massive concentration gradient, creating potent hydrochloric acid.
Clinical textbooks confirm that the optimal fasting gastric pH range is 1.5 to 3.5. That level of acidity is roughly comparable to battery acid. When the stomach fails to maintain this range and the pH rises above 4.0, the entire digestive system breaks down. Your body simply cannot perform its most basic metabolic duties.
Proteolysis and Pepsinogen Conversion
Why does the stomach need to be so intensely acidic? The answer lies in protein digestion, a process known medically as proteolysis.
When you eat chicken, steak, or any protein source, your body cannot absorb it whole. It must be broken down into individual amino acids. Your stomach secretes an inactive enzyme called pepsinogen to begin this process, but pepsinogen does nothing on its own. It requires a highly acidic environment to activate.
Hydrochloric acid acts as the catalyst that converts inactive pepsinogen into active pepsin, the primary enzyme responsible for slicing up dietary proteins. If you have hypochlorhydria, this critical conversion never happens. The protein sits in your stomach and begins to putrefy. This putrefaction is one of the primary drivers behind the severe symptoms of low stomach acid.
The Vagus Nerve and the Cephalic Phase of Digestion
Digestion actually begins in your brain, not your stomach. This initial stage is called the cephalic phase of digestion, and the brain-gut connection involved is powerful and immediate.
Picture your absolute favorite meal. Just the sight, smell, and anticipation of that food trigger your vagus nerve, which sends a rapid signal directly to your stomach lining. This initiates acid secretion long before food ever enters your mouth. The cephalic phase accounts for up to 30% of your total daily gastric acid output.
Now consider what happens when you eat while stressed, driving, or working. You completely suppress this vagus nerve response, forcing your stomach to digest food without any chemical preparation. This modern habit leads to a temporary stomach acid deficiency every single time you eat under stress.
The Immunological Barrier
Stomach acid does far more than digest lunch. It serves as your body’s first line of defense against ingested pathogens. We unknowingly consume thousands of bacteria, viruses, and fungal spores with every meal.
Highly acidic gastric juice neutralizes these harmful invaders on contact. It prevents yeast overgrowth and keeps the delicate environment of the small intestine sterile. When your stomach struggles to produce acid, this vital immunological barrier disappears, allowing pathogens to survive the transit and colonize the intestines. That is exactly why hypochlorhydria is so closely linked to persistent food poisoning and chronic gut infections.
Expert Insight: Many patients believe their stomach is too acidic because they feel a sharp burning sensation. However, even weak acid will burn the highly sensitive lining of the esophagus. The burning does not mean you have excess acid. It simply means acid is in the wrong place.
The Symptom Paradox: Recognizing Low Stomach Acid
Immediate Gastrointestinal Symptoms
Recognizing the symptoms of low stomach acid requires close attention to the timing of your discomfort. The physical sensations of low acid are distinct but incredibly often misinterpreted by both patients and doctors.
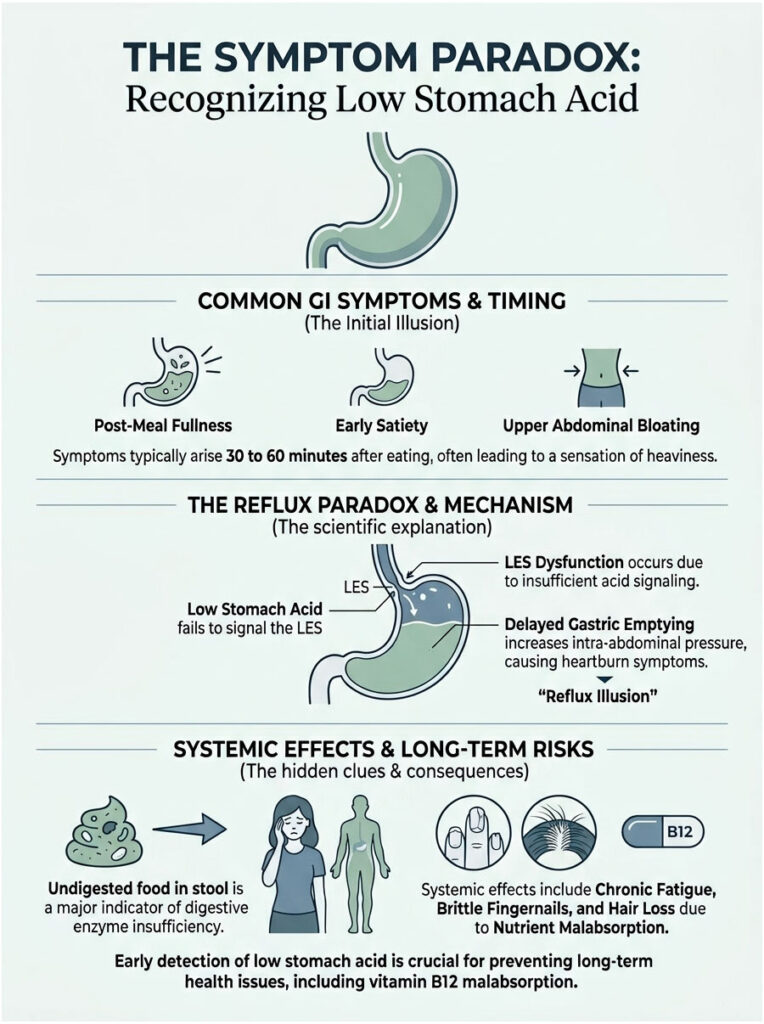
The most common symptoms include post-meal fullness, early satiety, and severe upper abdominal bloating. These typically appear 30 to 60 minutes after eating. You might feel like a heavy brick is sitting in your upper abdomen.
Because food is not breaking down properly, patients frequently notice undigested food in their stool. Finding recognizable food fragments in the toilet is a major red flag for digestive enzyme insufficiency. It proves that the mechanical and chemical breakdown in the stomach has failed, and your body is passing food straight through without extracting the necessary fuel.
The Reflux Illusion: How Low Acid Causes GERD Symptoms
Here is the most confusing part for the average patient. A severe lack of acid actually causes acid reflux. Gastroenterologists sometimes call this the reflux illusion, and it all comes down to lower esophageal sphincter dysfunction.
The lower esophageal sphincter (LES) is the muscular valve between your esophagus and stomach. This valve is highly sensitive to local pH levels. A strong surge of stomach acid signals the LES to close tightly. If your stomach is not producing enough acid, the LES never receives that chemical signal to shut, leaving the door wide open.
On top of that, delayed gastric emptying increases intra-abdominal pressure. The fermenting food creates trapped gas, which forces whatever weak acid is present upward into the unprotected esophagus. This upward pressure causes the burning pain associated with heartburn. It is exactly why treating lower esophageal sphincter dysfunction requires restoring acid levels, not suppressing them further.
Systemic and Neurological Symptoms
The symptoms of low stomach acid extend far beyond the gut. When you cannot break down food, you slowly starve at a cellular level. This starvation leads to profound systemic issues over time.
Patients frequently report crushing chronic fatigue, brittle fingernails, and diffuse hair loss. These are direct downstream effects of long-term protein and mineral starvation. A persistent stomach acid deficiency means your body cannot extract the building blocks it needs for basic tissue repair.
Over time, chronic malabsorption severely impacts the nervous system. We frequently see patients developing the neurological symptoms of vitamin B12 malabsorption, which is exactly why catching hypochlorhydria early is vital for long-term health.
High Acid vs. Low Acid: A Clinical Comparison
Patients are often confused about whether they are dealing with high acid or low acid. The symptoms overlap in surprisingly deceptive ways. The following clinical comparison helps differentiate the two distinct states.
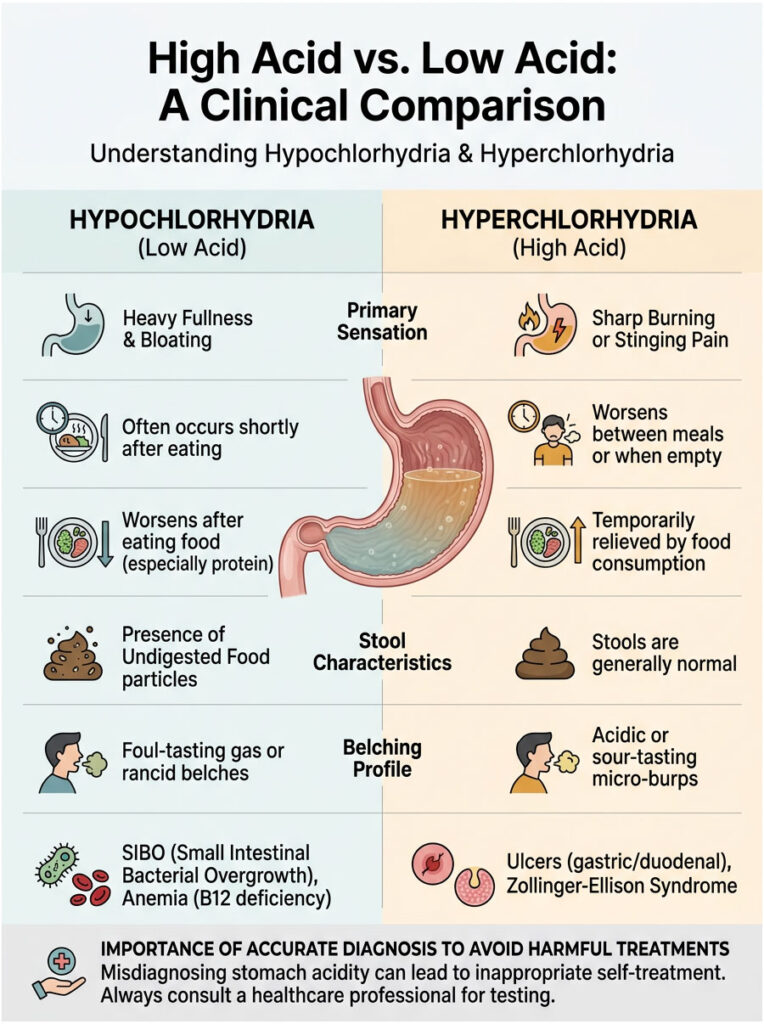
| Clinical Feature | Hypochlorhydria (Low Acid) | Hyperchlorhydria (High Acid) |
| Primary Sensation | Heavy fullness, severe bloating, pressure | Sharp burning, gnawing pain, hot sensation |
| Timing of Symptoms | 30 to 60 minutes after eating | Between meals or on an empty stomach |
| Response to Food | Symptoms worsen after eating heavy protein | Eating temporarily relieves the sharp pain |
| Stool Characteristics | Undigested food clearly visible | Generally normal, occasionally loose |
| Belching Profile | Foul-tasting gas, frequent deep burping | Acidic micro-burps, sour water brash |
| Associated Conditions | SIBO, Pernicious Anemia, Rosacea | Peptic Ulcers, Zollinger-Ellison Syndrome |
As you can see, the symptoms of low stomach acid involve stagnation and bacterial fermentation, while high acid symptoms involve active tissue erosion and ulceration. Differentiating between these two states is the first step toward effective treatment. Giving an acid blocker to someone with fermentation symptoms will make them significantly worse. Conversely, giving acid supplements to someone with an active ulcer can cause severe bleeding. Accurate symptom tracking and professional medical diagnosis are absolutely essential.
The Nutrient Malabsorption Problem
Vitamin B12 and Pernicious Anemia
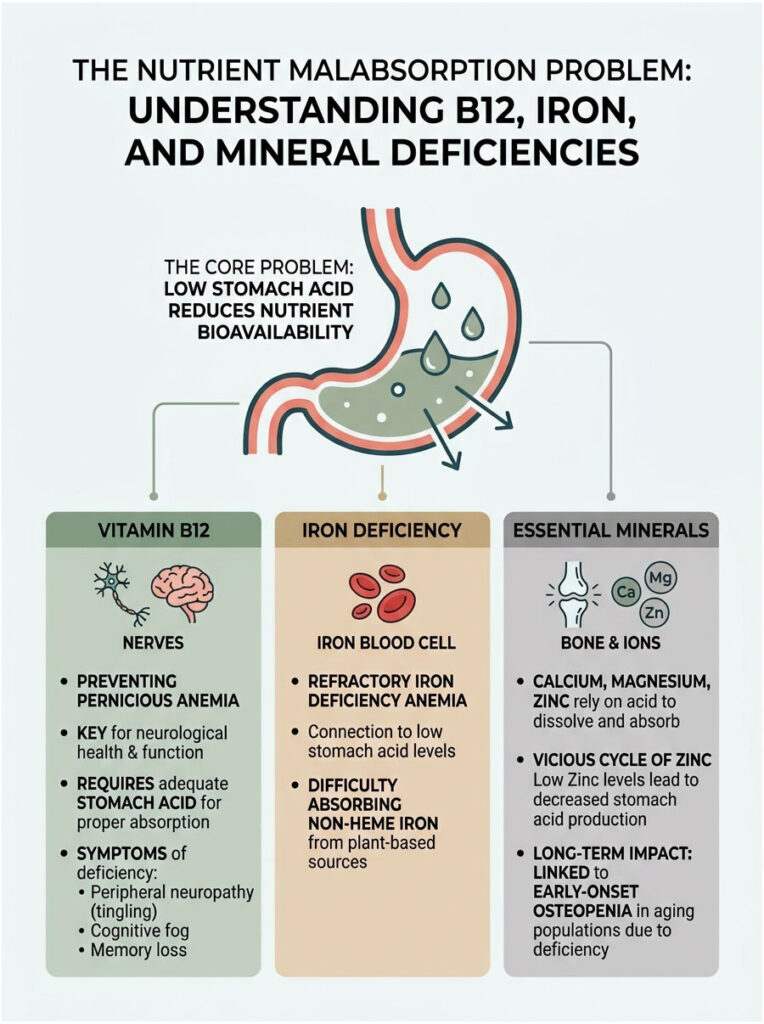
One of the most dangerous and silent consequences of low stomach acid is severe Vitamin B12 deficiency. Stomach acid is required to cleave Vitamin B12 away from dietary animal proteins. Without adequate acid, the B12 remains locked inside the meat you consume.
Your parietal cells also secrete a substance called intrinsic factor, which binds to the freed B12 so it can be absorbed in the small intestine. When parietal cells deteriorate, you lose both the acid and the intrinsic factor. This dual failure leads directly to pernicious anemia.
The neurological symptoms of vitamin B12 malabsorption are severe and sometimes irreversible if caught too late. Patients experience peripheral neuropathy, described as painful pins and needles in the hands and feet, along with cognitive fog, short-term memory loss, and balance disturbances.
I have seen patients misdiagnosed with early-onset dementia when they were simply lacking the stomach acid needed to absorb B12 for brain health. Once we restored their nutrient levels, their cognitive function returned entirely.
Refractory Iron Deficiency Anemia
Iron deficiency is incredibly common worldwide, yet doctors rarely investigate the stomach as the root cause. Hydrochloric acid is required to convert non-heme plant iron into an absorbable form. If you have a stomach acid deficiency, you simply cannot absorb iron from spinach, lentils, or even expensive supplements.
This frustrating condition is known as refractory iron deficiency anemia. Patients diligently take high-dose iron pills for months with zero improvement in their blood work. Clinical data from the American Journal of Hematology shows a clear pattern: patients with unexplained iron deficiency only recovered after doctors addressed their underlying atrophic gastritis.
When we fix the hypochlorhydria, ferritin levels naturally begin to rise. The body simply needed the highly acidic environment to ionize minerals properly. Before blaming your diet, consider whether your stomach chemistry might actually be the culprit.
Calcium, Magnesium, and Zinc Depletion
Iron and B12 are not the only nutrients that suffer in an alkaline stomach. Calcium, magnesium, and zinc all share a deep biochemical dependency on an acidic environment for ionization and intestinal absorption.
A stomach failing to produce acid leaves these crucial minerals in an unusable, solid state. Zinc is particularly important because the stomach actually needs zinc to produce more acid. This creates a vicious cycle: low acid leads to low zinc absorption, which leads to even lower acid production. We constantly see undigested food in stool in these patients because they lack the zinc required to manufacture pancreatic digestive enzymes.
There is also a strong clinical link between long-term stomach acid deficiency and early-onset osteopenia. Without acid to ionize dietary calcium, the bones slowly weaken. This is a major, unaddressed concern for aging populations taking daily antacids.
Primary Causes of Stomach Acid Deficiency
Aging and Atrophic Gastritis
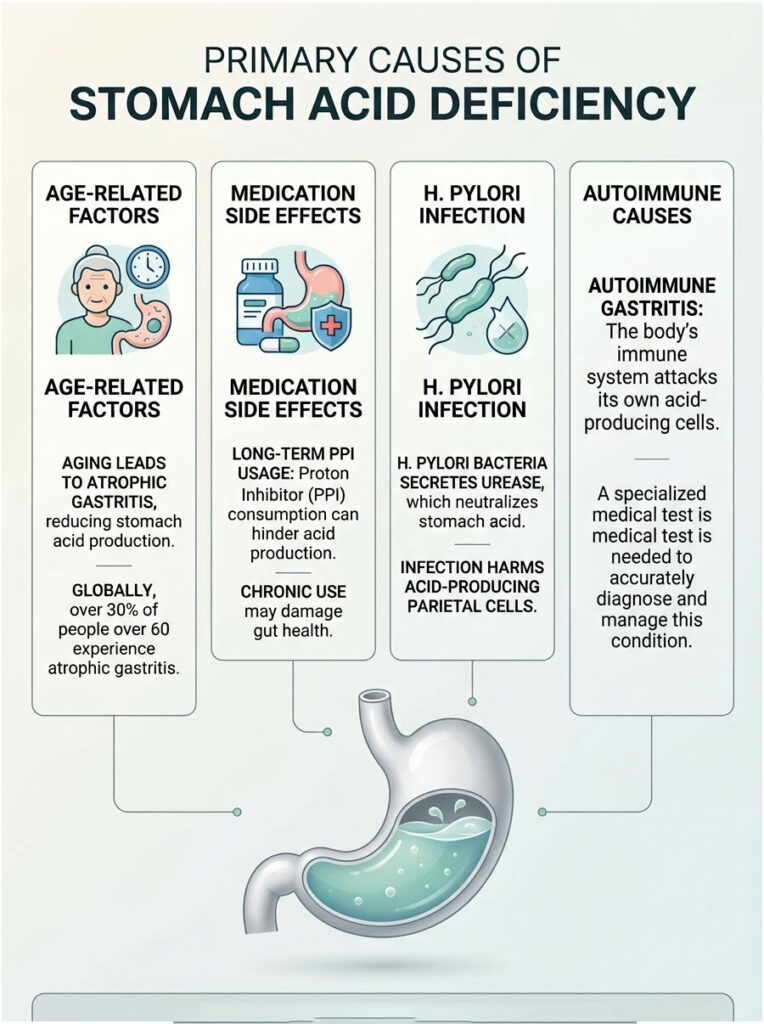
Why does the stomach stop doing its most basic job? Aging plays a major, unavoidable role. As we get older, the cellular lining of the stomach naturally degrades. This degradation is known clinically as atrophic gastritis, a condition where the stomach lining thins out and loses its glandular cells. As the parietal cells disappear, acid production drops dramatically.
Data from the National Institutes of Health confirms that atrophic gastritis affects over 30% of global populations above age 60. This age-related decline explains why older adults frequently experience early satiety, develop an unexplained distaste for heavy meats, and experience rapid weight loss. Their atrophic gastritis has silently destroyed their ability to digest complex proteins.
Long-Term Proton Pump Inhibitor (PPI) Usage
Sometimes, the medical system itself creates the problem. Medications like Omeprazole and Pantoprazole are specifically designed to halt the proton pumps entirely. While useful for short-term ulcer healing, long-term use is damaging to gut health. Proton pump inhibitor side effects include severe rebound reflux and drug-induced hypochlorhydria.
By artificially shutting down the parietal cells for years, the stomach essentially forgets how to function. Patients trying to stop these medications experience terrible withdrawal symptoms as the stomach hyper-secretes acid to compensate. Tapering off these powerful drugs requires careful medical supervision.
Helicobacter Pylori Infection
H. pylori is a highly adaptive, stealthy bacterium that colonizes the deep stomach lining. To survive the harsh acidic environment, it secretes an enzyme called urease, which creates a localized cloud of ammonia. This ammonia neutralizes the surrounding stomach acid, creating a safe haven for the bacteria while slowly destroying the host’s parietal cells.
Over time, an untreated H. pylori infection guarantees a stomach incapable of producing acid. Eradicating H. pylori with targeted antibiotics is essential. However, even after the bacteria is gone, patients often need prolonged support to rebuild their acid production capabilities. The physical damage to the gastric mucosa can be extensive, and it takes months of dedicated nutritional support to regenerate lost parietal cells.
Chronic Stress and Vagal Inhibition
We cannot overlook how modern lifestyles affect digestion. Chronic stress physically alters how your gastrointestinal tract operates. When you are stressed, your body enters sympathetic nervous system dominance, the fight-or-flight response. High cortisol levels shut down the digestive cascade, diverting blood away from the stomach toward the skeletal muscles.
If you eat while stressed, your stomach will not produce acid. This stress-induced stomach acid deficiency is temporary at first. But chronic daily stress can lead to long-term glandular dysfunction and persistent symptoms.
Autoimmune Gastritis
Autoimmune gastritis is a specific, underdiagnosed disease where the immune system produces rogue antibodies against its own parietal cells. The body literally attacks and destroys its own acid-producing factories. This condition rapidly accelerates atrophic gastritis and destroys the cells that produce intrinsic factor, directly leading to the neurological symptoms of vitamin B12 malabsorption.
Autoimmune gastritis requires specialized blood testing and lifelong management. If you have a family history of autoimmune disease, this should be on your radar.
Expert Insight: If you have been diagnosed with an autoimmune condition like Hashimoto’s thyroiditis or Celiac disease, your risk of developing autoimmune gastritis is significantly higher. Always ask your gastroenterologist to check your anti-parietal cell antibodies if you experience chronic bloating.
Clinical Diagnosis: Moving Beyond Guesswork
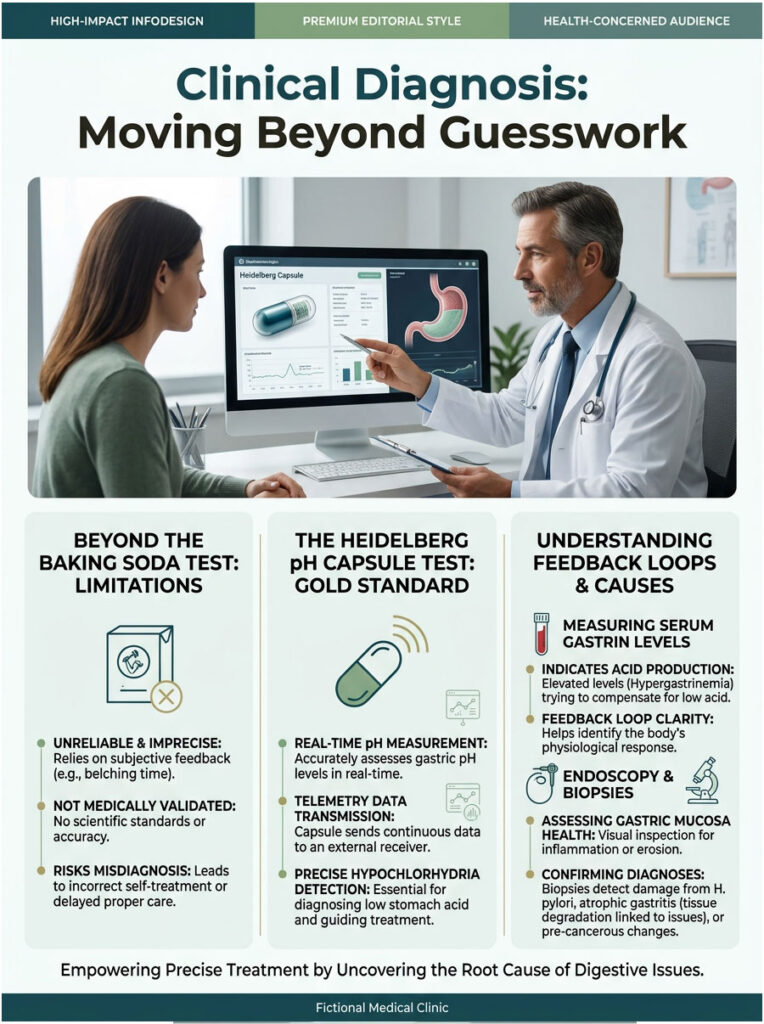
Why the Baking Soda Test Falls Short
When patients suspect low acid, they often turn to the internet for quick answers. The most popular at-home method is the baking soda test: drink a mixture of baking soda and water on an empty stomach, then time how long it takes to burp.
Let me be clear, this test is highly flawed and medically unreliable. The theory relies on a basic acid-base chemical reaction producing carbon dioxide gas, but the timing of the burp lacks true clinical sensitivity and specificity. Swallowing air while drinking, esophageal spasms, and delayed gastric motility can all mimic or delay a burp. Relying on this test to diagnose hypochlorhydria is dangerous and can lead patients to self-prescribe acid supplements inappropriately.
The Heidelberg pH Capsule Test (Gold Standard)
In clinical practice, we do not guess. We measure. The gold standard for diagnosing a stomach not producing enough acid is the Heidelberg Test. During this procedure, the patient swallows a specialized, medical-grade telemetry capsule containing a micro-transmitter.
As it sits in the stomach, the capsule transmits real-time pH data to a clinical monitor. We then give the patient a baking soda solution to neutralize their stomach acid and measure exactly how long it takes for the parietal cells to re-acidify the environment. If the stomach cannot return to a pH of 1.5 to 3.0 quickly, we have a definitive diagnosis of hypochlorhydria.
Serum Gastrin Levels and Hypergastrinemia
Routine blood work also provides valuable diagnostic clues. We frequently measure fasting serum gastrin levels. Gastrin is the primary hormone that tells the stomach to manufacture acid.
When acid levels stay chronically low, the body’s feedback loop kicks into overdrive. The brain pumps out massive amounts of excess gastrin in a desperate attempt to stimulate unresponsive parietal cells. This state, known as a hypergastrinemia feedback loop, strongly indicates that the stomach is failing to produce acid despite being told to do so. Detecting this loop helps us differentiate between temporary stress-induced low acid and permanent glandular failure.
Endoscopy and Gastric Mucosa Biopsy
Direct visual inspection remains a cornerstone of gastroenterology. An upper endoscopy lets the physician look directly at the health of the gastric mucosa. We can see immediately whether the tissue looks healthy and pink or thin, pale, and degraded.
During the procedure, we take tiny tissue samples called biopsies. The pathologist examines these under a high-powered microscope, which is the only way to definitively confirm atrophic gastritis, H. pylori damage, or autoimmune destruction. If we see severe microscopic tissue degradation, we know exactly why the patient has lower esophageal sphincter dysfunction and why they are finding undigested food in their stool.
Comparison of Diagnostic Methods
To help you understand the clinical landscape of digestive testing, here is an overview of the available diagnostic methods and why professional evaluation is vastly superior to at-home guessing.
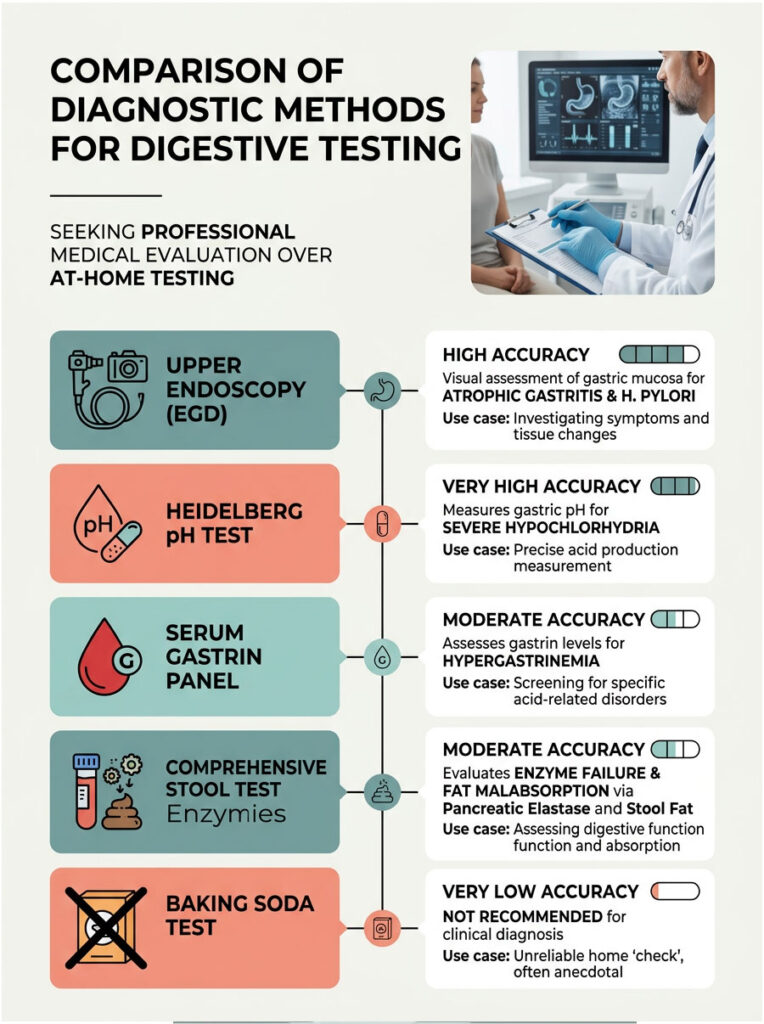
| Diagnostic Method | Accuracy | What It Measures | Best Use Case |
| Heidelberg pH Test | Very High | Real-time gastric pH and re-acidification rate | Definitive diagnosis of severe hypochlorhydria |
| Serum Gastrin Panel | Moderate | Gastrin hormone levels in the blood | Detecting hypergastrinemia feedback loops |
| Comprehensive Stool Test | Moderate | Pancreatic elastase, fat malabsorption, fibers | Assessing downstream enzyme failure |
| Upper Endoscopy (EGD) | High | Visual and microscopic state of gastric mucosa | Diagnosing atrophic gastritis and H. pylori |
| Baking Soda Test | Very Low | Gas from a crude acid-base reaction | Not recommended for clinical diagnosis |
Secondary Complications: SIBO and Gut Dysbiosis
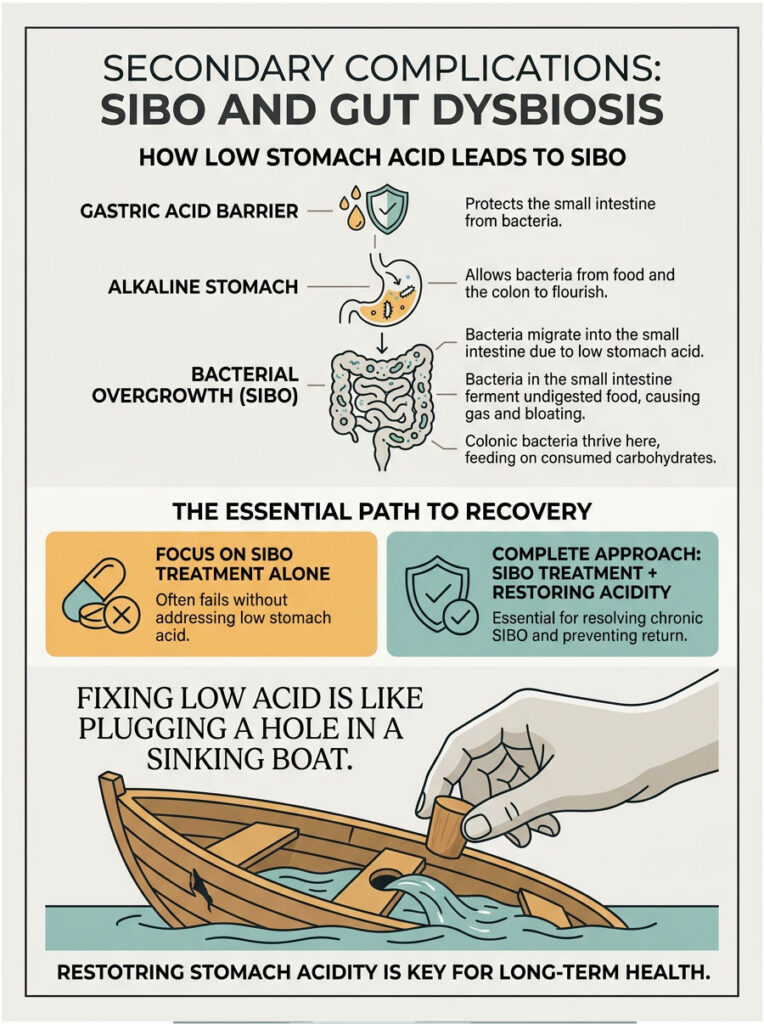
When the Gastric Acid Barrier Fails
What happens when the stomach stays alkaline for too long? You get a severe, cascading downstream effect. The small intestine is supposed to be relatively sterile compared to the heavily populated colon. Strong stomach acid ensures this by aggressively killing incoming microbes.
When your stomach stops producing acid, that protection vanishes. Bacteria from food and bacteria migrating upward from the colon suddenly find a safe, alkaline haven. They survive the stomach transit and set up camp in the small intestine. The overgrown bacteria then ferment undigested food before your body can absorb the nutrients, causing immense gas, painful bloating, and erratic bowel movements.
Small Intestinal Bacterial Overgrowth (SIBO)
This bacterial migration leads directly to Small Intestinal Bacterial Overgrowth, commonly known as SIBO. Colonic bacteria migrate upward through the ileocecal valve into the sterile small intestine when the acid barrier is missing. They thrive there and aggressively feed on the carbohydrates you consume.
SIBO is notoriously difficult to treat. Many doctors prescribe rounds of expensive antibiotics, only for the SIBO to return weeks later. Why? Because the root cause was never addressed. Treating low acid is fundamentally required to resolve chronic SIBO permanently. Once we restore the acidic firewall, bacteria can no longer survive the downward transit, and the small intestine can finally heal.
I tell my patients that treating SIBO without fixing stomach acid is like bailing water out of a sinking boat without plugging the hole. You have to plug the hole first.
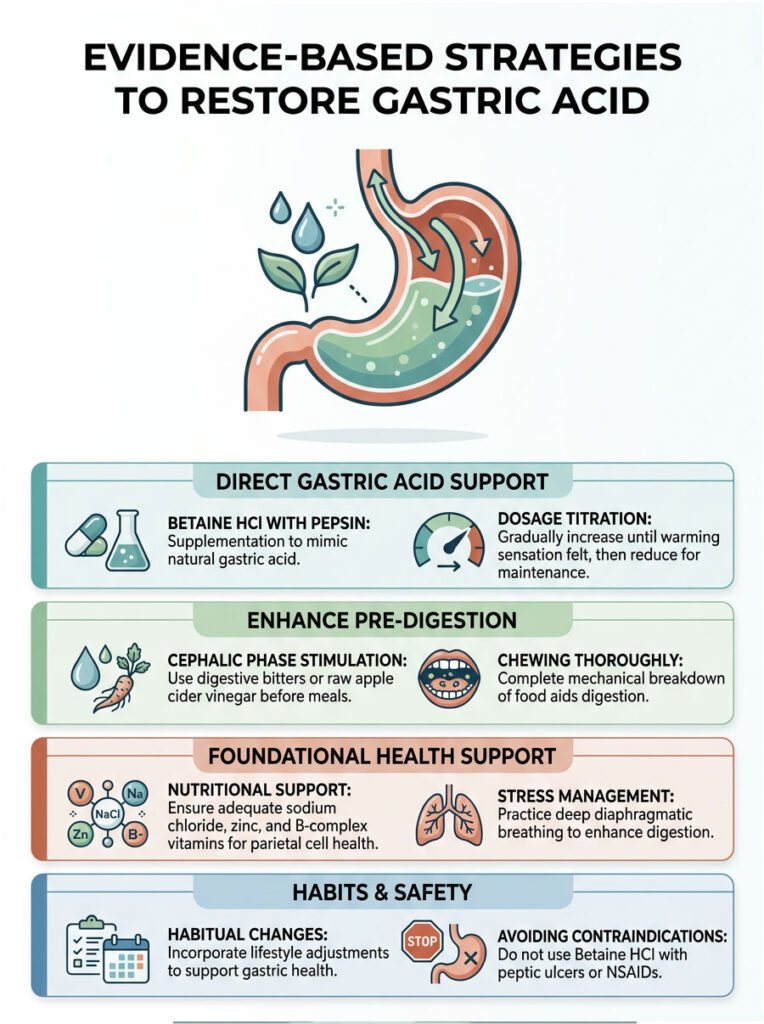
Evidence-Based Strategies to Restore Gastric Acid
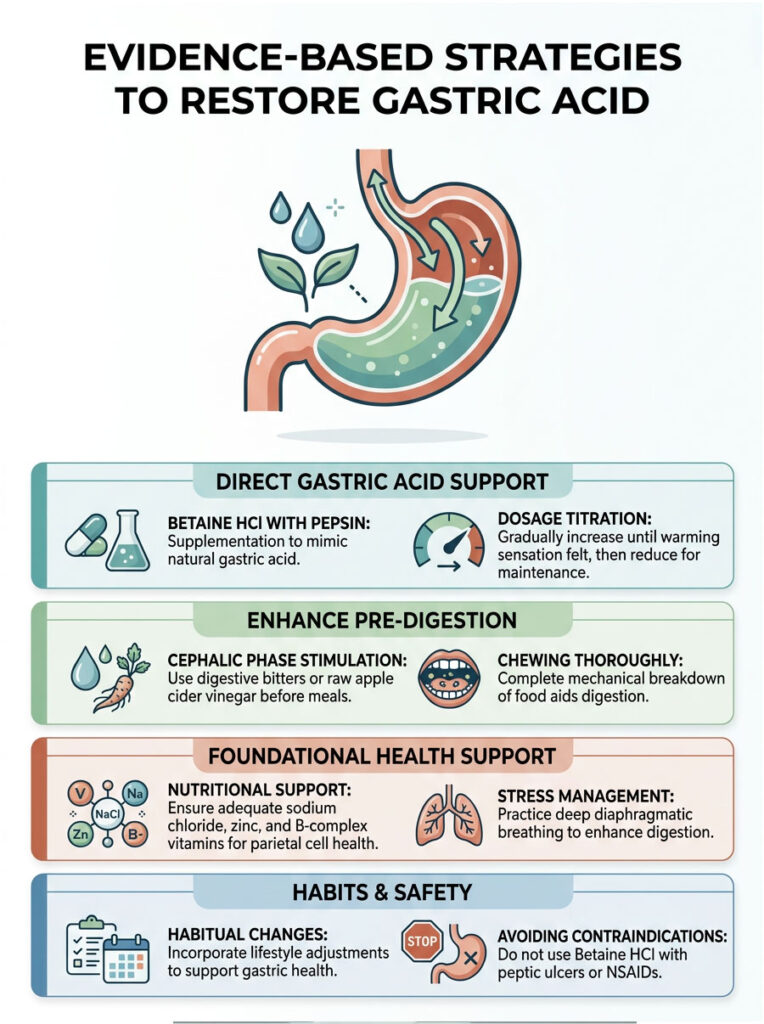
Betaine HCl with Pepsin Supplementation
When a patient has a medically confirmed stomach acid deficiency, therapeutic intervention becomes necessary. Gastroenterologists often use Betaine HCl supplements to artificially lower gastric pH during meals. This supplement provides the exact hydrochloric acid the parietal cells are failing to produce, and it is usually paired with pepsin to jumpstart protein digestion immediately.
Patients take the capsules right before eating. The goal is to mimic the natural acid surge that should occur. This exogenous acid immediately resolves lower esophageal sphincter dysfunction for many severe reflux patients.
Finding the right dose requires careful titration. Patients slowly increase their dosage by one capsule per meal until they feel a slight warming sensation in the stomach, then back down by one capsule for their maintenance dose.
Medical Disclaimer: Betaine HCl should never be used by individuals with active peptic ulcers, gastritis, or those taking NSAIDs, as it can cause severe gastric bleeding.
Stimulating the Cephalic Phase of Digestion
While supplements are helpful, encouraging the body to produce its own acid is equally important. Stimulating the cephalic phase of digestion is highly effective for mild cases of hypochlorhydria.
Digestive bitters such as gentian root, globe artichoke, or dandelion extract are excellent clinical tools. Placing a few drops of bitter herbs on the tongue 15 minutes before a meal sends a strong signal to the brain, which then tells the parietal cells to prepare for incoming food.
Raw apple cider vinegar is another accessible tool. While not as potent as Betaine HCl, it introduces a mild acetic acid that can temporarily lower gastric pH. This mild acidification assists pepsin activation and helps signal the LES valve to close, mitigating the daily symptoms of low stomach acid naturally.
Stress Management and Vagal Nerve Toning
Because chronic stress completely halts the cephalic phase of digestion, dedicated lifestyle changes are mandatory. You simply cannot digest food while your body is locked in a state of panic. The goal is to shift back into a parasympathetic “rest and digest” state.
Deep diaphragmatic breathing before meals is a practical, non-negotiable habit. Taking five slow, deep breaths into the belly signals profound safety to the nervous system. This simple act massively increases blood flow to the digestive organs, allowing the parietal cells to receive the oxygen and nutrients they need to manufacture hydrochloric acid. Managing daily stress is just as important as taking any supplement for correcting a stomach acid deficiency.
Dietary Modifications to Support Parietal Cell Health
Finally, the body needs the right raw materials to produce acid. Parietal cells require specific, high-quality nutrients to manufacture HCl daily.
Adequate sodium chloride from high-quality sea salt provides the literal chloride molecules required for hydrochloric acid creation. Zinc is another essential mineral, as it drives the complex enzymatic reactions within the parietal cells. B-complex vitamins, particularly B6, are also required for healthy gastric secretions.
We often see patients with undigested food in stool recover simply by optimizing their daily zinc intake. Chewing food thoroughly is another vital, often overlooked habit. Mechanical breakdown in the mouth drastically reduces the chemical burden on the stomach and makes digestion significantly easier even when acid levels are slightly low.
Key Takeaways
A stomach not producing enough acid is a widespread, critically underdiagnosed root cause of chronic digestive and systemic health problems. Millions of people suffer needlessly every day because they treat surface symptoms rather than the underlying physiology.
The symptoms of low stomach acid closely mimic high acid conditions. Severe bloating, massive reflux, and early fullness are clear signs of bacterial fermentation, not acid overproduction. Failing to recognize this difference leads to dangerous long-term consequences, including severe proton pump inhibitor side effects, early-onset osteoporosis, and the debilitating neurological symptoms of vitamin B12 malabsorption.
Clinical testing such as the Heidelberg Test is essential for an accurate, safe diagnosis. If you suspect hypochlorhydria, seek out a Board-Certified Gastroenterologist. Stop relying on over-the-counter antacids that may be making your condition exponentially worse.
Frequently Asked Questions
What exactly is hypochlorhydria, and how does it disrupt my digestion?
Hypochlorhydria is a clinical condition where the stomach’s parietal cells fail to secrete adequate hydrochloric acid (HCl). This deficiency raises the gastric pH above the optimal range of 1.5 to 3.5, which halts the conversion of pepsinogen into pepsin. Without this activation, your body cannot effectively perform proteolysis (protein breakdown), leading to food putrefaction, systemic malnutrition, and severe gastrointestinal distress.
If I have frequent heartburn, doesn’t that mean I have too much stomach acid?
Not necessarily. This is known as the ‘reflux illusion.’ The lower esophageal sphincter (LES) is a pH-sensitive valve that requires a strong acidic signal to close tightly. When you have a stomach not producing enough acid, the LES remains dysfunctional or open, allowing even weak gastric juices and fermentation gases to escape into the esophagus, causing the burning sensation commonly mistaken for hyperchlorhydria.
Why do I see undigested food in my stool when my acid levels are low?
Undigested food in the stool is a hallmark sign of gastric acid and digestive enzyme insufficiency. Without sufficient HCl to initiate the chemical breakdown of fibers and proteins, the mechanical churning of the stomach is ineffective. This results in recognizable food fragments passing through the entire GI tract without the extraction of essential nutrients.
How does low stomach acid lead to Small Intestinal Bacterial Overgrowth (SIBO)?
Your stomach acid serves as a primary immunological barrier, neutralizing ingested pathogens and keeping the small intestine relatively sterile. When gastric pH rises, this ‘acidic firewall’ is lost, allowing bacteria to survive the stomach transit and migrate upward from the colon. These microbes then colonize the small intestine, leading to the chronic bloating and fermentation associated with SIBO.
What are the neurological symptoms of vitamin B12 malabsorption caused by low acid?
A stomach acid deficiency prevents Vitamin B12 from being cleaved from animal proteins and often coincides with a lack of intrinsic factor. This leads to neurological issues such as peripheral neuropathy (pins and needles in extremities), cognitive fog, memory loss, and balance disturbances. In severe cases, this can be misdiagnosed as early-onset dementia when the root cause is actually pernicious anemia.
Is there a gold-standard clinical test to definitively diagnose low stomach acid?
Yes, the Heidelberg pH Capsule Test is the clinical gold standard. Unlike the unreliable at-home baking soda test, the Heidelberg Test uses a swallowed telemetry capsule to provide real-time data on your gastric pH and your parietal cells’ ability to re-acidify the stomach after a challenge. This allows gastroenterologists to move beyond guesswork and confirm a diagnosis of hypochlorhydria or achlorhydria.
Why is my iron deficiency not improving despite taking high-dose supplements?
This is often referred to as refractory iron deficiency anemia. Hydrochloric acid is strictly required to ionize and convert non-heme iron into a bioavailable form that the intestines can absorb. If your stomach is not producing enough acid, the iron remains in an unusable solid state, meaning supplements will simply pass through your system without increasing your ferritin levels.
Can chronic stress actually stop my stomach from producing acid?
Absolutely. Digestion begins in the brain via the cephalic phase. Chronic stress triggers sympathetic nervous system dominance (fight or flight), which inhibits the vagus nerve. Since the vagus nerve is responsible for signaling parietal cells to release acid before and during a meal, high cortisol levels can effectively extinguish your ‘digestive fire,’ leading to temporary or chronic hypochlorhydria.
What is atrophic gastritis, and how does it relate to aging?
Atrophic gastritis is a condition where the stomach lining thins and loses its functional glandular cells due to age or chronic inflammation. According to the NIH, over 30% of adults over 60 experience this, which leads to a permanent decline in parietal cell count. This is why many seniors experience early satiety, weight loss, and a sudden distaste for protein-heavy meals.
How do H. pylori infections contribute to a lack of gastric juice?
Helicobacter pylori is a stealth pathogen that secretes an enzyme called urease. This enzyme creates an ammonia cloud that neutralizes stomach acid to ensure the bacteria’s survival. Over time, the resulting chronic inflammation destroys the parietal cells, leading to a permanent state of low acid production even after the infection has been eradicated.
Are there risks to using Betaine HCl supplements to restore acidity?
While Betaine HCl with pepsin is an effective therapeutic tool for restoring gastric pH, it must be used with caution. It should never be taken by individuals with active peptic ulcers or gastritis, nor by those taking NSAIDs or corticosteroids, as the supplemental acid can erode the weakened gastric mucosa and cause severe internal bleeding.
What are ‘digestive bitters,’ and how do they help with low acid?
Digestive bitters are herbal secretagogues, such as gentian or dandelion, that stimulate the bitter receptors on the tongue. This triggers a reflex via the vagus nerve that primes the cephalic phase of digestion, encouraging the stomach to naturally increase acid secretion and the pancreas to release digestive enzymes before food arrives.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. The condition of a Stomach Not Producing Enough Acid requires professional clinical diagnosis. Always consult a Board-Certified Gastroenterologist before starting supplements like Betaine HCl, especially if you have a history of ulcers or are taking anti-inflammatory medications.
References
- National Institutes of Health (NIH) – https://www.ncbi.nlm.nih.gov/ – Epidemiological data on the prevalence of atrophic gastritis in aging populations.
- American Journal of Hematology – https://onlinelibrary.wiley.com/journal/10968652 – Clinical studies linking refractory iron deficiency to gastric pH imbalances.
- American College of Gastroenterology – https://gi.org/ – Guidelines on the diagnosis and management of H. pylori and chronic gastritis.
- Journal of Neurogastroenterology and Motility – https://www.jnmjournal.org/ – Research on the cephalic phase of digestion and vagal nerve influence on gastric secretions.
- Cleveland Clinic – https://my.clevelandclinic.org/ – Detailed clinical overview of hypochlorhydria, achlorhydria, and parietal cell function.
- The Lancet Gastroenterology & Hepatology – https://www.thelancet.com/journals/langas/home – Statistical data on the long-term effects of proton pump inhibitor (PPI) usage.





