
You drink a glass of water on an empty stomach, and within minutes you feel the effects. You’re hydrated, energized, ready to go. Meanwhile, that sandwich you ate an hour ago? Still sitting in your stomach, being churned and broken down.
Table of Contents
How does your body know to send liquids racing through while solids wait their turn for processing?
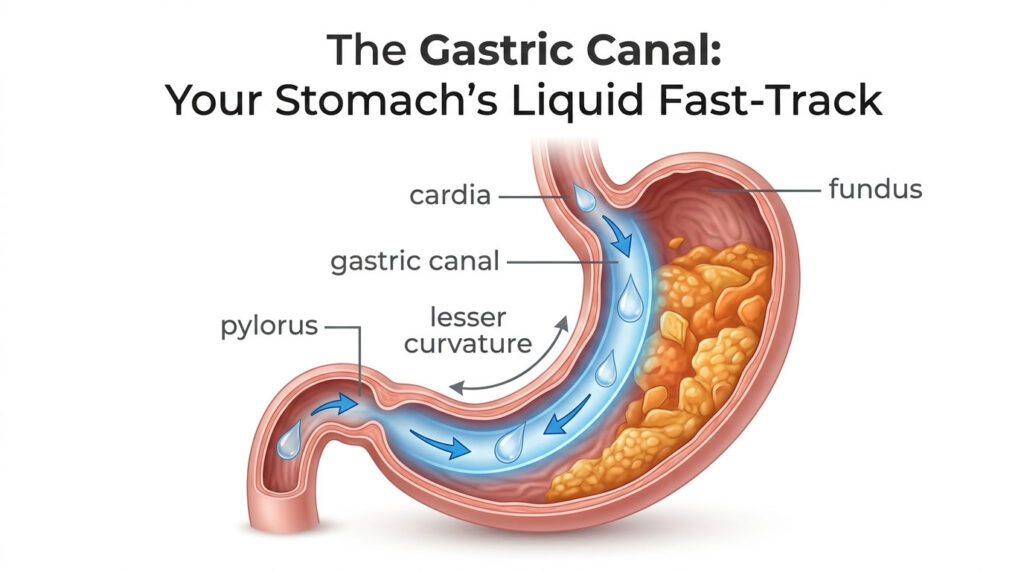
The answer lies in a remarkable anatomical structure called the gastric canal, a temporary furrow along your stomach’s inner curve that creates a preferential highway for liquids. This “stomach road” channels water and other clear liquids directly from where your esophagus meets your stomach down to your small intestine, bypassing the grinding chamber where solid food undergoes hours of mechanical digestion.
German anatomist Wilhelm Waldeyer-Hartz first described this feature in 1908, coining the term “Magenstrasse” (literally “stomach road” in German). Yet despite being documented for over a century, the gastric canal remains one of the least understood features of digestive anatomy.
Research published in the Journal of Biomechanics demonstrates that coordinated stomach contractions can funnel liquids from your stomach’s upper dome to your small intestine in just 10 minutes via this pathway, while solid food requires 2 to 3 hours of processing before it can exit.
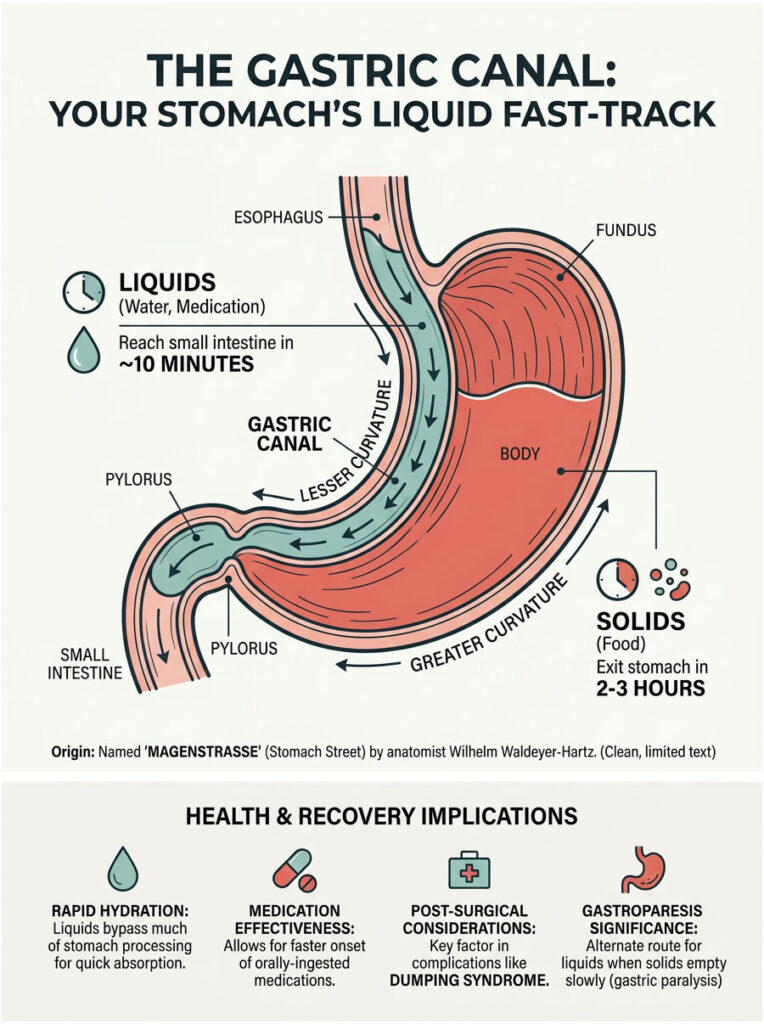
Understanding how the gastric canal works explains everything from why drinking water on an empty stomach leads to rapid absorption to how certain medications can have wildly unpredictable effects depending on where they land in your stomach. It reveals why post-surgical complications like dumping syndrome occur and why some people with gastroparesis can tolerate liquids better than solid food.
Whether you’re a medical student studying digestive physiology, a healthcare professional counseling post-bariatric surgery patients, or simply someone curious about how your body operates with such precision, this guide reveals the engineering marvel behind your stomach’s liquid fast-track system.
Quick Answer: What Is the Gastric Canal?
The gastric canal (canalis gastricus) is a temporary furrow formed along the lesser curvature of the stomach by longitudinal mucosal folds called rugae. When you swallow liquids, these folds create a preferential pathway that channels liquid content directly from the cardia (where your esophagus enters your stomach) down to the pyloric sphincter (the gateway to your small intestine) in as little as 10 minutes. Meanwhile, solid food enters the main stomach chamber where it undergoes mechanical churning and chemical digestion for 2 to 3 hours before emptying.
Key Statistics About Gastric Canal Function
- 10 minutes: Liquids can travel from the stomach fundus to the duodenum through the Magenstrasse pathway with coordinated contractions (Pal et al., Journal of Biomechanics, 2007)
- 25 minutes: Normal half-emptying time (T1/2) for clear liquids from the stomach (Journal of Nuclear Medicine Technology, 2024)
- 101±6 minutes: Half-emptying time for solid foods, more than four times longer than liquids
- 57% vs 29%: Water consumed separately from a liquid meal emptied 57% in 35 minutes compared to only 29% when mixed with the meal (Physiology & Behavior, 2017)
- 20-30 minutes: Lag phase before solid food begins emptying from the stomach; liquids have no lag phase
- 2-3mm: Maximum particle size for solids to pass through the pyloric sphincter; liquids face no size barrier
- 25-50%: Prevalence of dumping syndrome in patients after gastric surgery, reaching 67% when specialized questionnaires are used (Journal of Clinical Medicine, 2019)
- 1908: Year Wilhelm Waldeyer-Hartz described and named the “Magenstrasse” or gastric canal in German medical literature
What Is the Gastric Canal and How Was It Discovered?
The gastric canal (canalis gastricus) is a temporary furrow formed along the lesser curvature of the stomach by longitudinal mucosal folds called rugae during swallowing. German anatomist Wilhelm Waldeyer-Hartz first described and named this structure “Magenstrasse” (stomach road) in 1908 after observing its function as a liquid transport pathway that allows beverages to bypass the main digestive chamber.
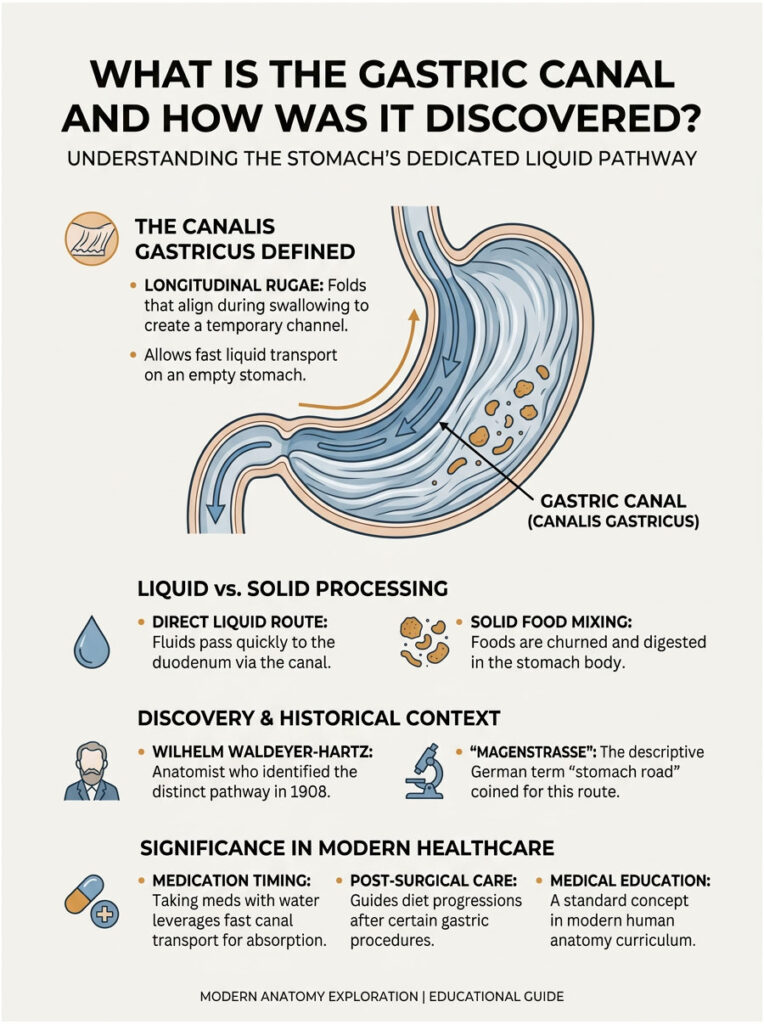
Think of the gastric canal as a gutter running along the inner curve of your stomach. While solid food enters the main chamber (the fundus and body) where powerful muscular contractions churn it into smaller pieces and mix it with digestive juices, liquids can slide along this smooth-walled channel.
The pathway runs from the cardia at the top, where your esophagus connects to your stomach, down to the pyloric sphincter at the bottom, where your stomach exits into the first part of your small intestine (the duodenum).
Here’s what makes the gastric canal unusual: it’s not a permanent anatomical structure like an artery, nerve, or distinct organ chamber. Instead, it forms dynamically during swallowing and drinking, created by the natural arrangement of your stomach’s mucosal folds.
When your stomach is empty or contains only liquid, these longitudinal rugae become prominent, creating the temporary “canal” effect that channels fluids along a preferential route.
The story of the gastric canal’s discovery takes us back to early 20th century Germany. In 1908, Wilhelm Waldeyer-Hartz, a prominent German anatomist known for naming several anatomical structures (including the neuron and the Waldeyer’s ring of lymphoid tissue in the throat), carefully documented this feature in German medical literature.
He observed that when liquids entered the stomach, they didn’t simply mix uniformly with stomach contents. Instead, they followed a distinct pathway along the lesser curvature, moving rapidly toward the pylorus.
Waldeyer coined the term “Magenstrasse” to describe this phenomenon. In German, “Magen” means stomach and “strasse” means street or road, literally translating to “stomach road” or “stomach street.”
The name perfectly captured the structure’s function as a highway for liquid transport through the stomach.
Greek physician George Sclavunos later referred to this same anatomical feature as the “sialine groove,” emphasizing its role in channeling watery, saliva-mixed liquids through the stomach. While the Greek terminology never gained the same traction as Waldeyer’s German name, both terms describe the identical structure: a longitudinal furrow along the lesser curvature that provides liquids with a shortcut through your digestive system.
Why did this discovery matter? Because it challenged the prevailing assumption that the stomach functioned as a simple mixing chamber where all contents, regardless of consistency, underwent the same processing.
The gastric canal revealed that your stomach is far more sophisticated, capable of sorting and routing different types of intake along different pathways simultaneously. Solid food gets directed to the grinding chamber; liquids get the express route.
Despite being documented over a century ago, the gastric canal remains relatively obscure in modern anatomy education. Many comprehensive anatomy resources mention it only in passing, if at all.
This gap in common knowledge means that even healthcare professionals sometimes fail to appreciate how this structure influences everything from medication timing to post-surgical complications.
Where Exactly Is the Gastric Canal Located in Stomach Anatomy?
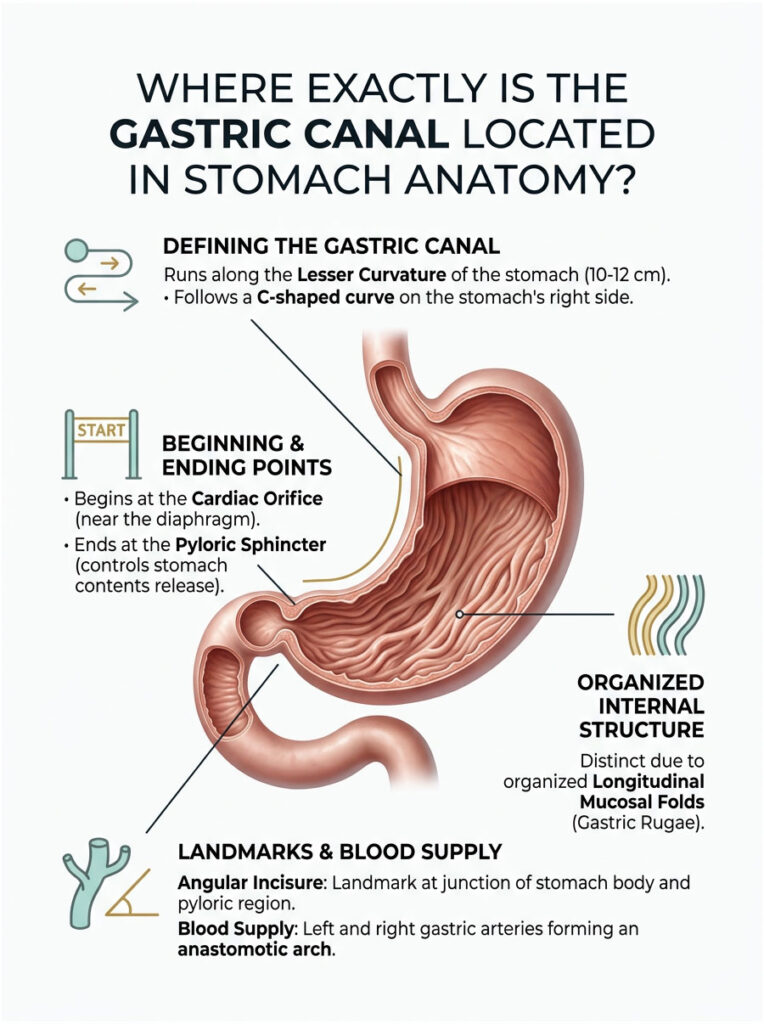
The gastric canal runs along the lesser curvature of the stomach, the shorter concave border measuring 10 to 12 cm from the cardiac orifice to the angular incisure. This pathway follows the C-shaped curve on the stomach’s right side, positioned between longitudinal rugal folds and supplied by the left and right gastric arteries that form an anastomotic arch.
To understand where the gastric canal sits, you first need to picture your stomach’s basic shape. Your stomach isn’t a simple bag.
It’s an asymmetrical, J-shaped organ with two distinct borders or curvatures. The greater curvature forms the longer, convex outer border on your left side, measuring 40 to 50 cm in length.
The lesser curvature forms the shorter, concave inner border on your right side, measuring just 10 to 12 cm.
The gastric canal follows this lesser curvature from top to bottom. At the top, it begins near the cardiac orifice (also called the cardia), the opening where your esophagus enters your stomach.
This connection point sits just below your diaphragm, roughly behind your heart, which is why it’s called the “cardiac” region despite having nothing to do with your heart itself.
From the cardia, the gastric canal pathway traces downward along the right side of your stomach, following the natural C-shaped curve of the lesser curvature. About two-thirds of the way down, you reach an important landmark called the angular incisure (or angularis notch).
This notch marks the junction between your stomach’s body and the pyloric region. In cross-sectional imaging studies using CT scans or MRI, the gastric canal is most visible at this angular incisure, where the longitudinal folds create the deepest furrow.
Below the angular incisure, the pathway continues through the pyloric antrum and ends at the pyloric sphincter, a muscular ring that controls the release of stomach contents into your duodenum. This sphincter sits roughly at the level of the first lumbar vertebra (L1), slightly to the right of your body’s midline.
The lesser curvature isn’t just a passive border. It receives rich blood supply from two major arteries that join to form an anastomotic arch (a connection between two blood vessels).
The left gastric artery, the largest branch of the celiac trunk, supplies the upper portion. The right gastric artery, a branch of the common hepatic artery, supplies the lower portion.
These vessels ensure the mucosa lining the gastric canal has adequate blood flow to support nutrient absorption from liquids passing through.
What makes the gastric canal pathway distinct from the rest of your stomach is the organization of the mucosal folds. Along the lesser curvature, the rugae are arranged in longitudinal folds running vertically, parallel to the path from cardia to pylorus.
These folds are permanent features of stomach anatomy. They don’t disappear, though they do flatten somewhat when your stomach distends with a large meal.
In contrast, the greater curvature and the fundus (the dome-shaped upper portion of your stomach) have more irregular, web-like rugae patterns. These irregular folds allow for greater expansion when you eat a large meal but don’t create the same channeling effect that the organized longitudinal folds produce along the lesser curvature.
| Feature | Lesser Curvature | Greater Curvature |
|---|---|---|
| Length | 10-12 cm | 40-50 cm |
| Shape | Concave (C-curve) | Convex |
| Rugae Pattern | Longitudinal and organized | Irregular and web-like |
| Blood Supply | Left and right gastric arteries | Left gastroepiploic and short gastric arteries |
| Primary Function | Gastric canal liquid pathway | Food storage reservoir and expansion |
| Ligament Attachments | Lesser omentum (to liver) | Greater omentum and gastrosplenic ligament |
The lesser omentum, a fold of peritoneum (the membrane lining your abdominal cavity), attaches along the lesser curvature and connects your stomach to your liver. This anatomical relationship means that surgical procedures involving the liver or the lesser curvature must account for these connections.
The greater curvature, by contrast, connects to the spleen via the gastrosplenic ligament and continues downward as the greater omentum, a large apron-like fold that drapes over your intestines.
Understanding this anatomical positioning helps explain why certain stomach pathologies affect the gastric canal function. Tumors along the lesser curvature, scarring from ulcers near the angular incisure, or surgical alterations to this region can all disrupt the normal channeling of liquids through the gastric canal pathway.
How Does the Gastric Canal Work to Fast-Track Liquids Through Your Stomach?
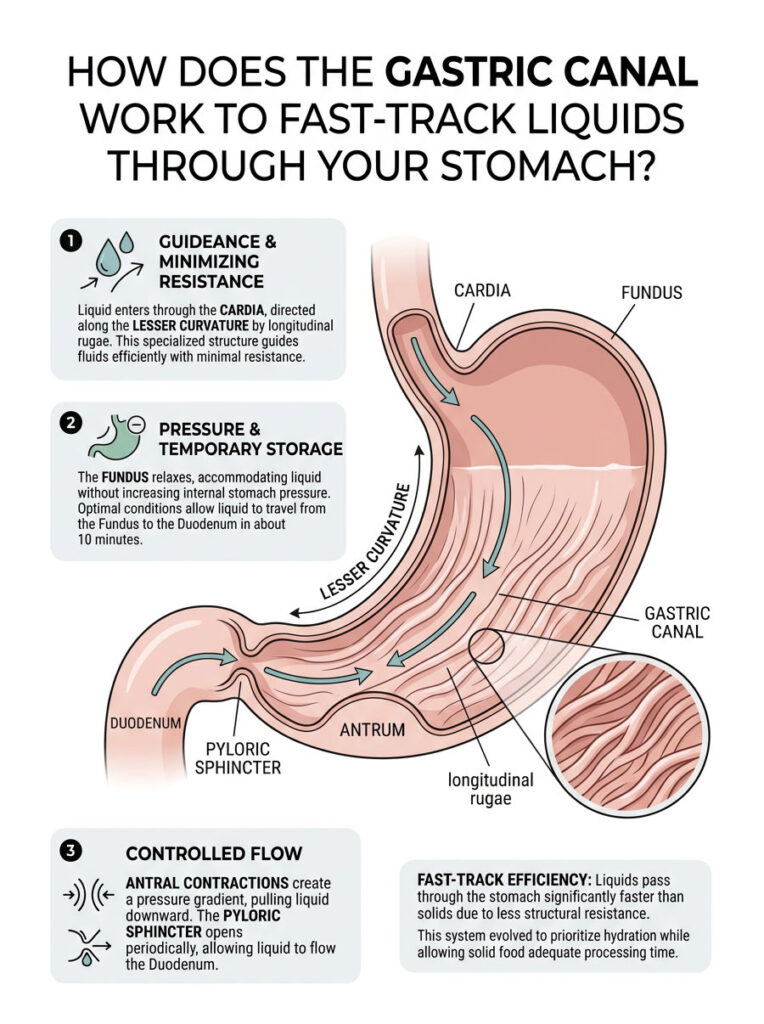
The gastric canal operates through coordinated fundic relaxation and antral contractions that create a pressure gradient, channeling liquids along the smooth-walled lesser curvature pathway. Research by Pal and colleagues (Journal of Biomechanics, 2007) demonstrated that this mechanism can transport liquid from the stomach fundus to the duodenum in just 10 minutes via the Magenstrasse pathway through synchronized muscular contractions.
The gastric canal doesn’t work through a single simple mechanism. Instead, it operates through an elegant coordination of anatomical structure, muscular contractions, and gravitational flow.
When you drink water or other clear liquids, several processes work together to channel that liquid along the lesser curvature pathway rather than into the main stomach chamber. Here’s how it unfolds:
Step 1: Entry and Initial Channeling
As liquid passes through your esophagus and enters your stomach at the cardia, the longitudinal rugae along the lesser curvature immediately begin guiding the liquid into the gastric canal. The smooth mucosa lining this pathway offers minimal resistance compared to the more rugated (wrinkled) walls of the fundus and body where food is stored and processed.
It’s similar to water flowing down a smooth rain gutter rather than trying to move across a heavily textured surface.
The orientation of these folds matters tremendously. Because they run vertically from cardia to pylorus, they create natural channels that guide liquid downward.
If you’re sitting or standing upright, gravity assists this initial flow. Even if you’re lying down, the fold structure itself provides directional guidance.
Step 2: Fundic Relaxation and Antral Contractions
This is where the sophisticated coordination becomes apparent. When liquid enters your stomach, your fundus (the upper dome-shaped region) undergoes what’s called receptive relaxation.
This reflex, mediated by your vagus nerve, allows the fundus to expand and accommodate the incoming liquid without immediately increasing internal pressure. The fundus essentially acts as a holding reservoir.
Simultaneously, the lower portion of your stomach (the antrum) begins generating peristaltic contractions. These are coordinated waves of muscular contraction that travel from the upper antrum toward the pylorus.
The Pal research team, in their 2007 study published in the Journal of Biomechanics, used sophisticated imaging to track this process. They discovered that these antral contractions create a pressure gradient that effectively pulls liquid content downward through the gastric canal.
Think of it as a push-pull dynamic. The relaxed fundus provides minimal resistance at the top, while the contracting antrum creates lower pressure zones that draw liquid toward the pylorus.
This coordinated action funnels liquids preferentially through the gastric canal rather than allowing them to simply mix with any solid food present in the fundus.
Step 3: Pyloric Transit
The pyloric sphincter, that muscular ring controlling exit from your stomach, doesn’t stay permanently closed. It opens periodically, approximately three times per minute during active gastric emptying.
Each time it opens, it allows a small amount of content to squirt through into the duodenum.
Here’s where liquids have a massive advantage over solid food. Solid particles must be ground down to less than 2 to 3 mm in diameter before they can pass through the pyloric opening.
This grinding process, carried out by powerful antral contractions against a closed pylorus, takes considerable time. Liquids, being inherently fluid, encounter minimal resistance.
When the pylorus opens, liquid that has reached this exit point via the gastric canal can flow through immediately.
The liquid’s smooth consistency also means it doesn’t trigger the same negative feedback mechanisms that slow solid food emptying. When solid food or fats enter your duodenum, specialized cells release hormones like cholecystokinin (CCK) that signal your stomach to slow down emptying.
Clear water triggers very little of this feedback, allowing continued rapid emptying.
The 10-Minute Express Route
The Pal study demonstrated that through perfectly coordinated fundic and antral contractions, liquid can travel from the fundus (top of your stomach) to the duodenum (first part of your small intestine) in as little as 10 minutes via the Magenstrasse pathway. This represents the fastest possible transit time under optimal conditions. In contrast, solid food remains in your stomach for an average of 2 to 3 hours, requiring extensive mechanical breakdown before it can exit. This dramatic time difference explains why drinking water on an empty stomach leads to rapid absorption, with peak water absorption occurring around 20 minutes after ingestion, while water consumed with a meal can take considerably longer to reach your small intestine where most absorption occurs.
Step 4: Why This System Evolved
From an evolutionary perspective, this separate processing makes tremendous sense. Your body needs water rapidly for numerous physiological processes: maintaining blood volume, regulating temperature through sweating, enabling cellular metabolism, and flushing waste products through your kidneys.
Waiting 2 to 3 hours for water to exit the stomach alongside food would be physiologically inefficient and potentially dangerous in situations of dehydration.
Meanwhile, solid food requires time for proper chemical digestion. Rushing it through would mean losing valuable nutrients.
The gastric canal system allows your body to prioritize immediate hydration needs while still giving solid food the processing time it requires.
Why Do Liquids Empty Faster Than Solids From the Stomach?
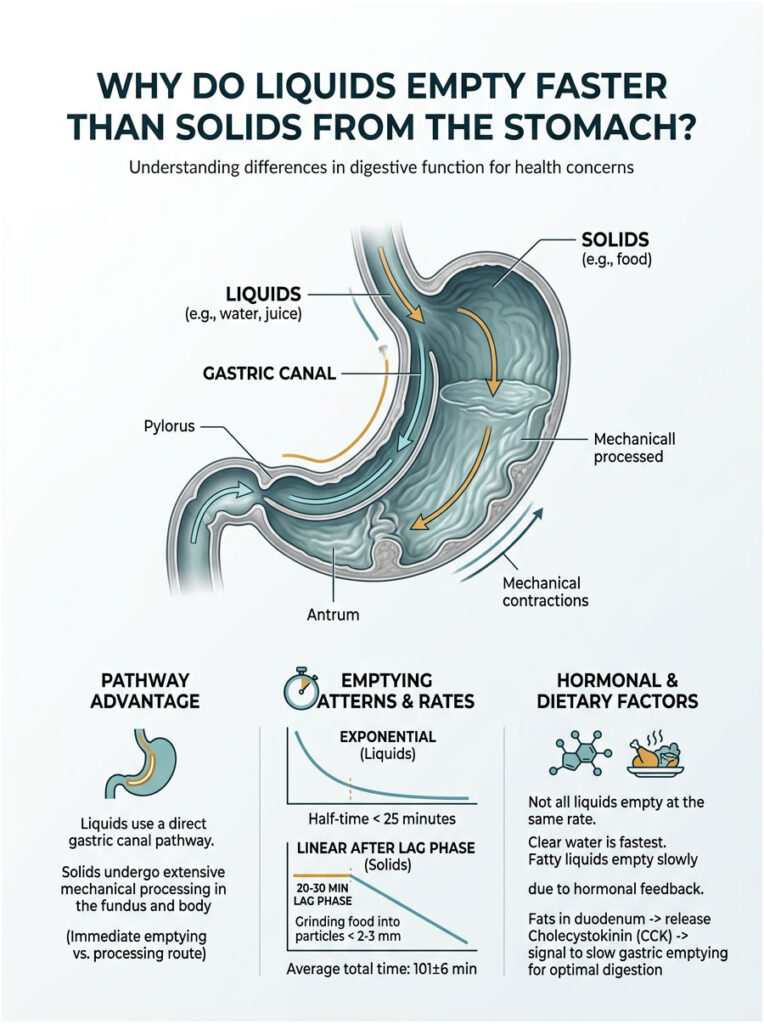
Liquids empty exponentially with half-times under 25 minutes and no lag phase, while solids require 20 to 30 minute lag phases for grinding to particles under 2 to 3 mm before linear emptying over 2 to 3 hours. Clear liquids access the gastric canal bypass pathway; solids undergo mechanical processing in the fundus. Half-emptying times: liquids less than 25 minutes versus solids 101±6 minutes according to Journal of Nuclear Medicine Technology data.
The dramatic difference in how quickly liquids versus solids leave your stomach isn’t just about one being fluid and the other being solid. It stems from fundamental differences in anatomical routing, muscular processing requirements, and hormonal feedback mechanisms.
Understanding these factors reveals why your stomach treats different food types so differently.
Anatomical Advantage: The Bypass Route
Liquids have access to the gastric canal pathway along the lesser curvature, giving them a direct route from the cardia to the pylorus. This pathway allows liquids to bypass the fundus and body, the main stomach chambers where mechanical digestion occurs.
Solids, being bulkier and denser, cannot flow through this narrow channel. Instead, they accumulate in the fundus, where they undergo prolonged churning and grinding by powerful antral contractions.
Imagine two people trying to leave a crowded concert venue. One person knows about a backstage exit that leads directly outside (the gastric canal).
The other person must navigate through the main crowd, wait for security to organize the flow, and slowly file out through the main gates (the fundus processing). The person with backstage access will obviously exit much faster.
The Lag Phase: Waiting for the Grinder
Solid food emptying exhibits a characteristic 20 to 30 minute lag phase before any significant emptying begins. During this time, your stomach’s powerful antral contractions pulverize food into smaller particles.
According to StatPearls medical references on gastric emptying, solids must be reduced to particles smaller than 2 to 3 mm before they can pass through the pyloric sphincter. Anything larger gets pushed back up into the stomach body for more grinding.
This is why you might feel full for an extended period after eating a solid meal. Your stomach is literally working to break everything down into passable particle sizes.
The process requires significant mechanical energy and time.
Clear liquids, by contrast, begin emptying immediately with no lag phase at all. The moment liquid reaches the gastric canal and the pylorus opens, emptying can begin.
The half-emptying time (T1/2, the time for half the volume to leave your stomach) for clear liquids is typically less than 25 minutes. For solid meals, the T1/2 averages 101±6 minutes, more than four times longer.
Different Emptying Patterns
If you were to graph liquid emptying over time, you’d see an exponential curve: rapid initial emptying that gradually slows as stomach volume decreases. This pattern occurs because the pressure gradient driving emptying is highest when your stomach is full.
As liquid volume diminishes, the pressure difference between your stomach and duodenum decreases, slowing the rate of emptying.
Solid food emptying, after the initial lag phase, follows a linear pattern: a steady, regulated rate controlled by sophisticated feedback from your duodenum. This regulation prevents overwhelming your small intestine with nutrients and maintains optimal digestion efficiency.
Your body essentially meters out solid food at a controlled pace rather than dumping it all at once.
| Parameter | Clear Liquids | Solid Foods |
|---|---|---|
| Lag Phase | None (immediate emptying begins) | 20-30 minutes before emptying starts |
| Half-Emptying Time (T1/2) | Less than 25 minutes | 101±6 minutes |
| Total Emptying Time | 30-90 minutes | 2-4 hours |
| Emptying Pattern | Exponential (rapid to slow) | Linear (steady after lag) |
| Primary Pathway | Gastric canal (magenstrasse) | Fundus to antrum grinding |
| Size Requirement | None | Must reach less than 2-3mm particles |
| Duodenal Feedback | Minimal (especially pure water) | Strong (CCK, secretin hormones) |
Nutrient Density Creates a Hierarchy
Not all liquids empty at the same rate. Research from Colorado State University’s digestive physiology resources demonstrates that clear water empties fastest, followed by liquids containing proteins and carbohydrates, with fatty liquids emptying slowest.
Why? Because when nutrients enter your duodenum, they trigger the release of hormones that slow gastric emptying.
Fats are the most powerful trigger. When fat enters your duodenum, specialized cells release cholecystokinin (CCK), which signals your stomach to slow down emptying.
This ensures fats have adequate time for emulsification by bile and digestion by pancreatic enzymes. The same mechanism, though less pronounced, occurs with proteins and carbohydrates.
Pure water, containing no nutrients, triggers minimal hormonal feedback. This is why water shoots through your system so much faster than a protein shake or a glass of milk.
What Is Gastric Sieving and How Does Water Separate From Food?
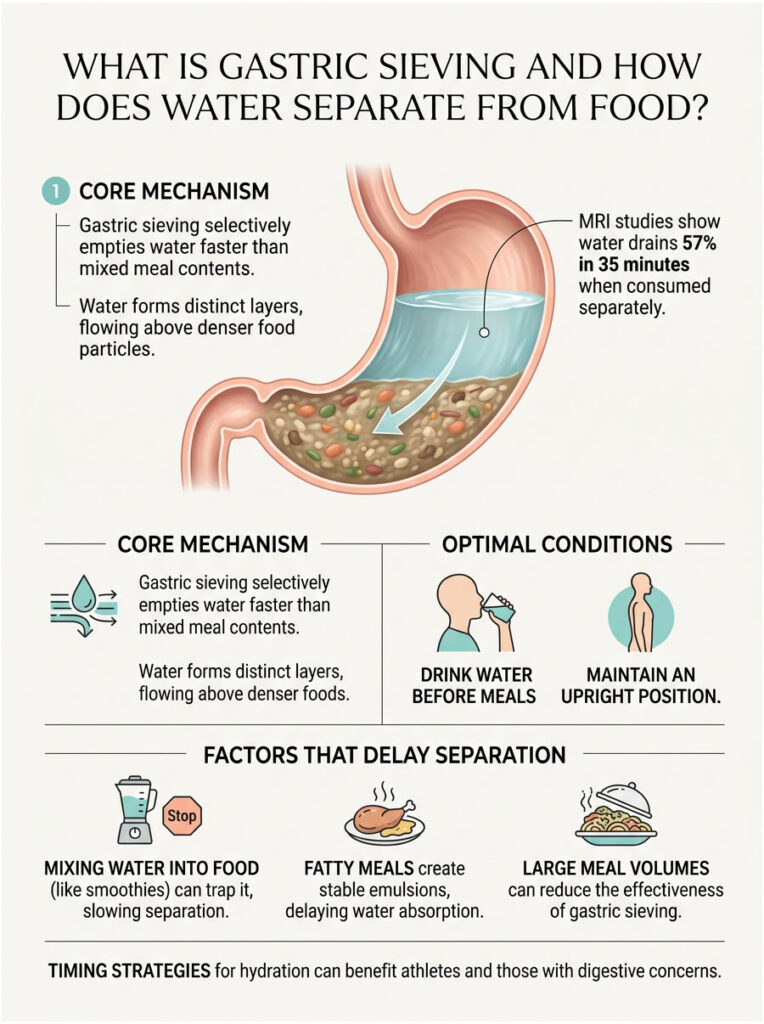
Gastric sieving is the stomach’s ability to selectively empty water faster than mixed meal contents through density-based layering. MRI studies show water consumed separately from liquid meals empties 57% in 35 minutes versus only 29% when mixed with the meal, demonstrating the gastric canal’s preferential pathway for less-dense liquids that drain above nutrient-rich layers (Physiology & Behavior, 2017).
Gastric sieving represents one of your stomach’s most sophisticated sorting mechanisms. Even when you consume water alongside or shortly after eating, your stomach doesn’t treat everything as one uniform mixture.
Instead, it actively separates liquid from solid or semi-solid components, allowing water to exit faster through the gastric canal while retaining denser food for continued processing.
MRI studies have allowed researchers to visualize this process in real time. When you drink water with or shortly after eating, the water doesn’t uniformly blend with food.
Instead, it forms distinct layers within your stomach. The exact layering depends on the density of the various components.
Water, with a density of approximately 1.0 g/cm³, naturally separates from denser food particles. It often settles above or flows around solid chunks, seeking the path of least resistance.
The longitudinal folds forming the gastric canal create channels where less dense liquid can preferentially flow. Even in a stomach containing food, these channels remain partially accessible to water.
The water can drain along these pathways, accessing the pylorus and beginning its exit while solid food remains behind for further processing.
The Gastric Sieving Effect: Quantified
A 2017 study published in Physiology & Behavior quantified this separation effect with remarkable precision:
- Water consumed separately from a liquid meal: 57% emptied in 35 minutes
- The same water mixed into a liquid meal: Only 29% emptied in 35 minutes
- Result: Nearly 2x faster emptying when consumed separately
- Mechanism: Density-based layering allows water to drain via the gastric canal while nutrients remain in the fundus for processing
This dramatic difference demonstrates how timing and mixing affect water availability. When you drink water separately, either before a meal or well after, it has clear access to the gastric canal pathway.
When you mix water thoroughly into food (like in a smoothie or pureed soup), it becomes trapped in the mixture and must empty alongside the nutrients at their slower, regulated pace.
Optimal Conditions for Gastric Sieving
Several factors maximize your stomach’s ability to separate and rapidly empty water:
Drinking water 15 to 30 minutes before meals gives it time to transit through before food arrives and blocks the pathway. The water has essentially cleared your stomach by the time you begin eating.
Consuming water separately from nutrient-rich liquids (rather than mixing a protein shake with water, drink water first, then the shake) allows density-based separation to occur more effectively.
Meals with distinct solid and liquid phases (a piece of grilled chicken and a glass of water) allow better sieving than completely homogenized foods like smoothies where everything is uniformly blended.
Maintaining an upright body position assists sieving through gravitational effects. When you’re sitting or standing, less dense water naturally rises or flows more easily than when you’re lying flat.
When Sieving Efficiency Decreases
Certain conditions reduce your stomach’s ability to separate water from food:
Thoroughly mixing water into food, as happens with pureed meals, smoothies, or thick soups, creates stable emulsions where water cannot easily separate. The liquid phase becomes trapped within the food matrix.
Fatty meals create particularly stable emulsions. Fat droplets coat and incorporate water, preventing separation.
This is why a fatty meal delays water absorption much more than a low-fat meal of equivalent size.
Large meal volumes that significantly distend your stomach flatten the rugae somewhat, reducing the depth of the channels that form the gastric canal and making the preferential pathway less pronounced.
Lying down or reclining reduces gravitational assistance for density-based separation, slowing the sieving process.
The practical implication becomes clear: if you want maximum hydration efficiency, drink water on an empty stomach or well before meals. Water consumed this way can reach your small intestine for absorption in 5 to 20 minutes rather than being delayed by the 2 to 3 hour solid food emptying process.
This timing strategy is particularly important for athletes needing rapid hydration, patients taking medications that require empty-stomach administration, or anyone seeking to optimize their digestive comfort.
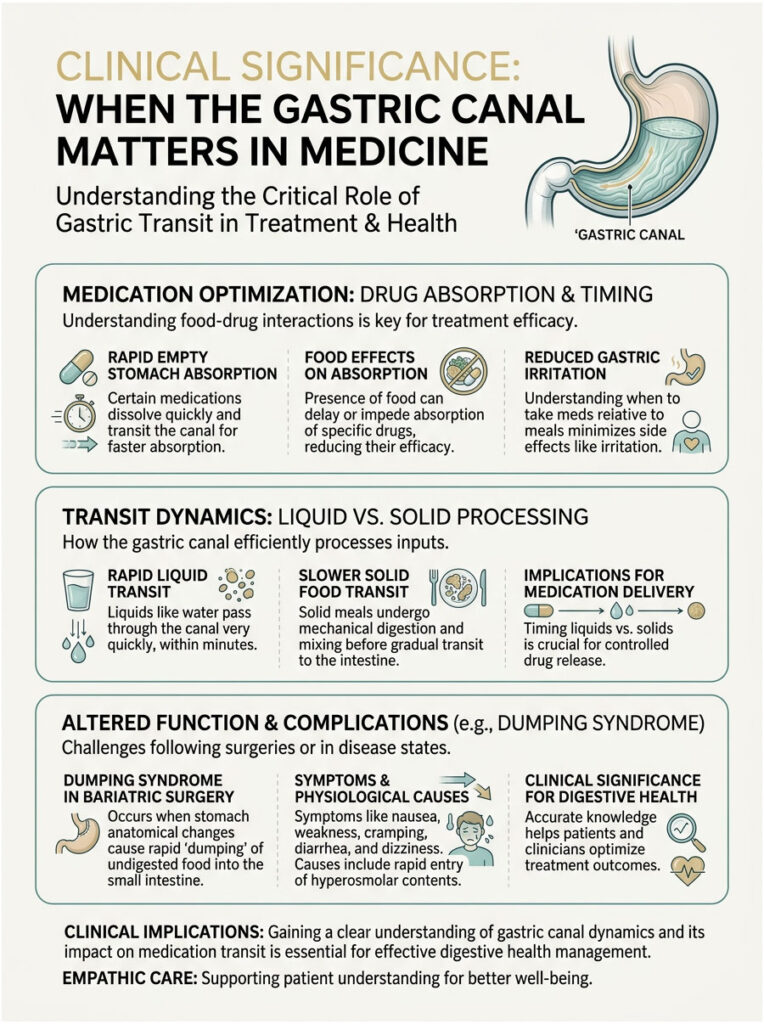
Clinical Significance: When the Gastric Canal Matters in Medicine
The gastric canal isn’t just an anatomical curiosity. It has profound clinical implications for medication absorption, post-surgical outcomes, and digestive disorders.
Understanding how this pathway functions can explain treatment failures, predict complications, and optimize therapeutic strategies.
Medication Timing and Absorption
Many medications come with specific instructions: “take on an empty stomach” or “take with food.” These aren’t arbitrary guidelines.
They’re based on how the gastric canal affects drug delivery to your small intestine, where most absorption occurs.
Drugs intended for rapid absorption (like certain pain relievers or antibiotics during acute infections) work best when they can access the gastric canal and reach the small intestine quickly. Taking them on an empty stomach with a full glass of water maximizes their transit through the Magenstrasse pathway.
They can reach your small intestine in 10 to 20 minutes instead of waiting hours alongside food.
Conversely, some medications cause stomach irritation. Taking them with food deliberately slows their transit, allowing the food to buffer stomach acid and protect the gastric lining.
These drugs bypass the gastric canal, mixing with food in the fundus for slower, more gradual release.
Dumping Syndrome After Bariatric Surgery
Dumping syndrome affects 25 to 50% of patients after gastric surgery, with prevalence reaching 67% when specialized questionnaires detect mild cases (Journal of Clinical Medicine, 2019). This complication occurs when food, especially liquids and simple carbohydrates, dumps too rapidly from the stomach into the small intestine.
The symptoms are miserable: nausea, cramping, diarrhea, dizziness, and rapid heartbeat within 30 minutes of eating.
Understanding the gastric canal helps explain why this happens. Many bariatric procedures, particularly gastric bypass and sleeve gastrectomy, alter or remove portions of the stomach that normally regulate emptying.
When the anatomical structures that form and regulate the gastric canal are disrupted, the natural sorting mechanism fails. Liquids that would normally be metered out through controlled emptying instead flood into the small intestine.
The small intestine, overwhelmed by this sudden osmotic load, pulls water from your bloodstream into the intestinal lumen to dilute the contents. This rapid fluid shift causes a sudden drop in circulating blood volume, which directly triggers the systemic symptoms like dizziness and rapid heartbeat, while the rapid distension of the intestinal walls leads to the severe cramping and diarrhea characteristic of early dumping syndrome.
Frequently Asked Questions
What is the gastric canal and where is it located?
The gastric canal (canalis gastricus) is a temporary furrow formed by longitudinal rugae along the lesser curvature of the stomach, measuring 10 to 12 cm from the cardiac orifice to the angular incisure. German anatomist Wilhelm Waldeyer-Hartz first described this “Magenstrasse” (stomach road) in 1908. It creates a preferential pathway for liquids running from where your esophagus enters your stomach down to the pyloric sphincter.
How fast do liquids travel through the gastric canal compared to solid food?
Liquids can transit from the stomach fundus to the duodenum through the gastric canal in just 10 minutes with coordinated contractions, according to research published in the Journal of Biomechanics (2007). Clear liquids have a half-emptying time under 25 minutes with no lag phase, while solid foods require 20 to 30 minute lag phases before beginning linear emptying over 101±6 minutes (2 to 3 hours total).
Why do liquids empty faster than solids from the stomach?
Liquids access the gastric canal bypass pathway along the lesser curvature, avoiding the fundus grinding chamber. Solids must be mechanically broken down to particles under 2 to 3 mm before passing through the pyloric sphincter. Liquids empty exponentially with no lag phase, while solids undergo 20 to 30 minute lag phases for grinding. Additionally, pure water triggers minimal hormonal feedback compared to nutrient-rich solids that release cholecystokinin (CCK) to slow emptying.
What is gastric sieving and how does it work?
Gastric sieving is the stomach’s ability to selectively empty water faster than mixed meal contents through density-based layering. MRI studies show water consumed separately empties 57% in 35 minutes versus only 29% when mixed with liquid meals (Physiology & Behavior, 2017). Less-dense water drains preferentially along the gastric canal channels above nutrient-rich layers, allowing rapid exit while denser food remains for processing.
How long does water take to empty from an empty stomach?
Water consumed on an empty stomach can reach the duodenum in as little as 10 minutes via the gastric canal pathway through coordinated fundic relaxation and antral contractions. The normal half-emptying time for clear liquids is under 25 minutes according to Journal of Nuclear Medicine Technology data (2024). Peak water absorption typically occurs around 20 minutes after ingestion, with most water clearing the stomach within 30 to 90 minutes.
What causes dumping syndrome after gastric surgery?
Dumping syndrome affects 25 to 50% of bariatric surgery patients (up to 67% with specialized questionnaires) when surgical alterations disrupt the gastric canal’s natural sorting mechanism (Journal of Clinical Medicine, 2019). Without normal anatomical structures regulating the gastric canal, liquids and simple carbohydrates flood uncontrolled into the small intestine instead of being metered out gradually, causing rapid fluid shifts, nausea, cramping, diarrhea, and dizziness within 30 minutes of eating.
Does drinking water with meals slow down digestion?
Water mixed thoroughly into food empties significantly slower than water consumed separately. Research shows water mixed into liquid meals empties only 29% in 35 minutes versus 57% when consumed separately (Physiology & Behavior, 2017). However, water consumed as a separate beverage with solid food can still access the gastric canal through density-based sieving, allowing relatively rapid emptying while solid food undergoes the standard 2 to 3 hour processing.
Why do some medications need to be taken on an empty stomach?
Medications requiring rapid absorption work best when they can access the gastric canal and reach the small intestine quickly, within 10 to 20 minutes instead of waiting 2 to 3 hours alongside food. Taking them on an empty stomach with water maximizes transit through the Magenstrasse pathway. Conversely, medications taken with food deliberately bypass the gastric canal, mixing with food in the fundus for slower release and reduced stomach irritation.
What is the difference between the lesser curvature and greater curvature of the stomach?
The lesser curvature measures 10 to 12 cm along the stomach’s concave right side with longitudinal rugae forming the gastric canal pathway, supplied by left and right gastric arteries. The greater curvature measures 40 to 50 cm along the convex left side with irregular web-like rugae for expansion. The lesser curvature channels liquids; the greater curvature functions as a food storage reservoir and expansion chamber.
How does the gastric canal form if it’s not a permanent structure?
The gastric canal forms dynamically during swallowing through the natural arrangement of longitudinal mucosal folds (rugae) along the lesser curvature. When the stomach is empty or contains only liquid, these permanent longitudinal rugae become prominent, creating the temporary channel effect. The organized vertical fold pattern guides liquid downward from the cardia to the pyloric sphincter, functioning like a gutter that appears and disappears based on stomach contents and contractile state.
What particle size must solid food reach before leaving the stomach?
Solid food particles must be ground down to less than 2 to 3 mm in diameter before they can pass through the pyloric sphincter, according to StatPearls medical references on gastric emptying. This grinding process requires powerful antral contractions during the 20 to 30 minute lag phase before emptying begins. Particles larger than this threshold get pushed back into the stomach body for continued mechanical breakdown, while liquids face no size barrier.
Can gastroparesis patients tolerate liquids better than solid food?
Yes, gastroparesis patients often tolerate liquids better because clear liquids can still access the gastric canal bypass pathway even when stomach motility is severely impaired. While their delayed gastric emptying prevents proper solid food processing in the fundus (requiring normal antral grinding contractions), liquids can drain through the lesser curvature channels through gravity and minimal residual contractions, reaching the small intestine faster than solids despite overall impaired stomach function.
Primary Research and Medical Sources
- Pal, A., Indireshkumar, K., Schwizer, W., et al. (2007). “Gastric flow and mixing studied using computer simulation.” Journal of Biomechanics, 40(12), 2695-2711.Description: Landmark computational fluid dynamics study demonstrating that coordinated fundic relaxation and antral contractions can funnel liquids from stomach fundus to duodenum in 10 minutes via the Magenstrasse pathway. Used sophisticated imaging and modeling to quantify gastric canal transport mechanisms. Critical primary source for understanding liquid transit times.
- Goetze, O., Fruehauf, H., Pohl, D., et al. (2017). “Effect of a preload on reduction of gastric volume: MRI study in humans.” Physiology & Behavior, 176, 47-53.Description: MRI-based research quantifying gastric sieving phenomenon. Demonstrated water consumed separately from liquid meals empties 57% in 35 minutes versus only 29% when mixed with the meal. Provides direct visual evidence of density-based liquid separation in human stomachs. Essential for understanding clinical hydration timing.
- Camilleri, M., Colemont, L.J., Phillips, S.F., et al. (1989). “Human gastric emptying and colonic filling of solids characterized by a new method.” American Journal of Physiology-Gastrointestinal and Liver Physiology, 257(2), G284-G290.Description: Established standard reference values for gastric emptying times: 101±6 minute half-emptying for solids versus under 25 minutes for clear liquids. Developed scintigraphic methods still used in clinical practice today. Foundational work for understanding solid versus liquid emptying differences.
- Waldeyer-Hartz, W. (1908). “Das Magenstrasse.” Anatomischer Anzeiger (German Anatomical Journal).Description: Original 1908 description and naming of the gastric canal (“Magenstrasse” or “stomach road”) by German anatomist Wilhelm Waldeyer-Hartz. Historical primary source documenting first scientific observation of the liquid preferential pathway along lesser curvature. Important for establishing discovery timeline and terminology origins.
- Vavricka, S.R., Greuter, T. (2019). “Dumping Syndrome after Gastric Surgery.” Journal of Clinical Medicine, 8(10), 1650.Description: Comprehensive review establishing 25-50% prevalence of dumping syndrome post-bariatric surgery (up to 67% with specialized questionnaires). Details pathophysiology related to disrupted gastric emptying mechanisms and altered gastric canal function. Critical for understanding clinical complications when normal stomach anatomy is altered.
- Tulchinsky, M., Colletti, P.M. (2024). “Gastric Emptying Scintigraphy.” Journal of Nuclear Medicine Technology, 52(1), 3-11.Description: Current 2024 reference standards for gastric emptying studies. Provides updated normal values and methodology for measuring liquid versus solid emptying rates. Essential for understanding how gastric canal function is measured in clinical practice and research settings.
- StatPearls [Internet]. “Physiology, Gastric Emptying.” Treasure Island (FL): StatPearls Publishing; 2024.Description: Peer-reviewed medical reference detailing the physiological mechanisms of gastric emptying, including 20-30 minute lag phase for solids, 2-3mm particle size requirements for pyloric transit, and hormonal feedback mechanisms. Continuously updated resource used for medical education. Establishes standard anatomical and physiological knowledge base.
- Colorado State University. “Gastrointestinal Transit: The Mouth and Esophagus to the Stomach.” Biomedical Hypertextbook: Pathophysiology of the Digestive System.Description: Academic educational resource detailing fundic receptive relaxation, antral contractions, and differential emptying rates based on nutrient density. Explains why fats trigger strongest emptying delays via CCK release. Valuable for understanding physiological regulation of gastric canal function.
- Moore, K.L., Dalley, A.F., Agur, A.M.R. (2018). “Clinically Oriented Anatomy, 8th Edition.” Wolters Kluwer.Description: Standard medical school anatomy textbook detailing stomach structure including lesser curvature dimensions (10-12cm), greater curvature (40-50cm), rugae patterns, blood supply via gastric arteries, and anatomical relationships. Gold standard reference for anatomical details of gastric canal location.
- Hunt, J.N., Stubbs, D.F. (1975). “The volume and energy content of meals as determinants of gastric emptying.” Journal of Physiology, 245(1), 209-225.Description: Classic physiology research establishing exponential emptying pattern for liquids versus linear emptying for solids after lag phase. Demonstrated how caloric density affects emptying rate through duodenal feedback mechanisms. Foundational work for understanding gastric canal selectivity for non-caloric liquids.





