After more than 15 years of treating patients as a board-certified gastroenterologist, there is one question I hear almost every single day: when should I actually worry about diarrhea?
Table of Contents
Patients walk into my office exhausted, anxious, and unsure whether they are dealing with a passing stomach bug or something far more serious. Gastrointestinal distress affects millions of Americans every year, and most episodes resolve on their own with rest and fluids.
But here is the truth that matters: knowing the exact point where a common stomach illness crosses into a clinical emergency can genuinely save your life. I have watched firsthand as untreated, persistent cases spiraled into life-threatening situations, sometimes within hours.
A viral infection that seems harmless can quickly trigger severe dehydration, dangerous drops in blood volume, or even mask a hidden gastrointestinal hemorrhage. In this article, I will walk you through the exact clinical benchmarks we rely on in the hospital, including the 48-hour rule, the 6-stool benchmark, and the critical red flags that demand immediate medical attention.
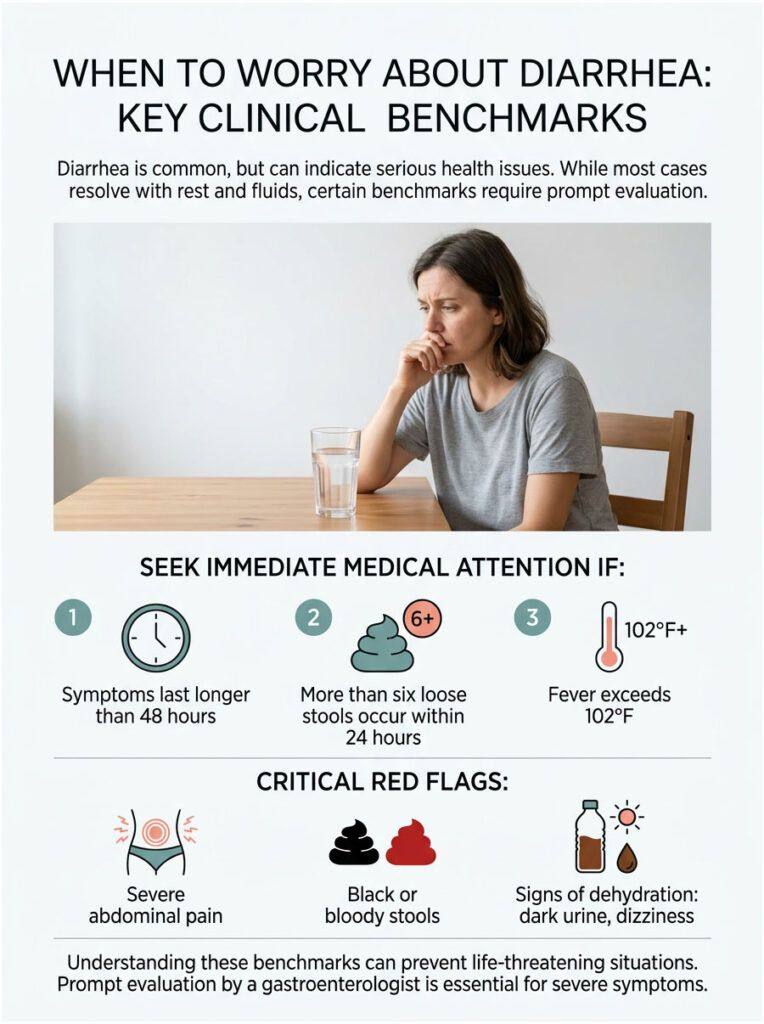
| Quick Answer: Seek immediate medical attention for diarrhea if it lasts longer than two days, you pass more than six loose stools within 24 hours, or you develop a fever above 102°F. Other red flags include severe abdominal pain, black or bloody stools, and signs of significant fluid loss such as dark urine or dizziness. A prompt gastroenterologist evaluation is necessary if any of these symptoms appear. |
Key Statistics on Adult Gastrointestinal Health
Before diving into warning signs, consider these numbers that highlight just how common, and how dangerous, gastrointestinal illness can be in adults.
Outpatient visits: According to the CDC, acute diarrheal infections cause over 1.5 million outpatient visits in the United States each year.
Fluid loss rate: Adults lose roughly 1 liter of fluid for every 3 to 4 watery bowel movements.
Kidney injury risk: The risk of acute kidney injury jumps by 40% when severe dehydration goes untreated for more than 48 hours.
C. diff infections: Clostridioides difficile causes nearly 500,000 infections in the United States annually.
Post-infectious IBS: Up to 10% of patients with acute infectious enteritis go on to develop symptoms that require post-infectious IBS recovery protocols.
Viral dominance: Over 80% of acute gastrointestinal infections are viral, which means antibiotics are completely ineffective against them.
Normal Versus Abnormal Bowel Function: What Healthy Digestion Looks Like
To recognize when something is genuinely wrong, you first need to understand how healthy digestion works. Your digestive tract is essentially a finely tuned processing plant. Each day, your stomach and small intestine handle gallons of food, water, and digestive secretions.
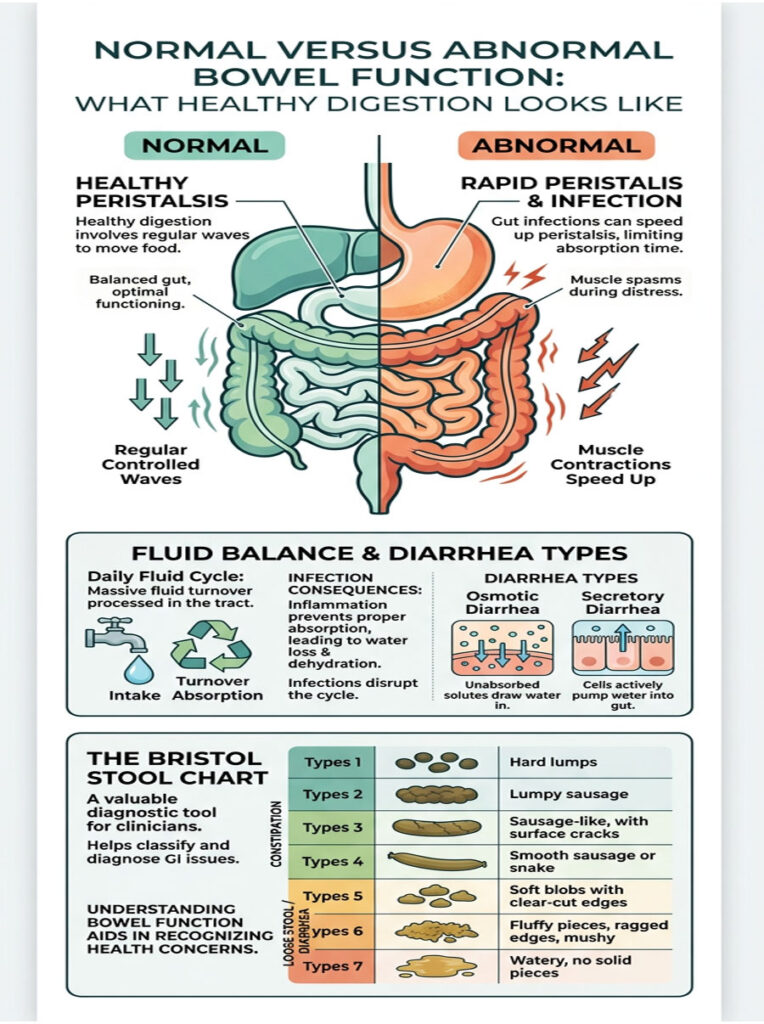
By the time that mixture reaches your colon, it is mostly liquid. The colon’s primary job is straightforward: absorb water and form solid waste. When a virus or bacteria inflames the intestinal lining, that entire process breaks down. The colon stops absorbing water and, in severe cases, actually secretes extra fluid directly into the bowel. The result is liquid waste rushing through your system with little control.
How Peristalsis and Intestinal Motility Work
Food moves through your digestive tract via peristalsis, a series of rhythmic muscle contractions that push contents from your stomach all the way to your rectum. Under normal conditions, these contractions are slow, steady, and coordinated, allowing plenty of time for nutrient absorption and fluid retention.
When infection strikes, your body shifts into emergency mode. It deliberately speeds up peristalsis to flush out the invading pathogen as quickly as possible. Clinically, this rapid flushing falls into two main categories. Osmotic diarrhea occurs when unabsorbed substances pull water into the bowel, often triggered by certain foods. Secretory diarrhea happens when the body actively pumps water and electrolytes into the intestinal space because of infection.
The 9-Liter Daily Fluid Cycle Inside Your Gut
Most people have no idea how much fluid their digestive system processes every day. Even if you only drink about two liters of water, your gut handles roughly nine liters of fluid, including saliva, gastric acid, bile, and pancreatic juices.
Your small intestine absorbs around seven liters, and your large intestine handles roughly two more, leaving just a small amount of water in your stool. During a severe stomach illness, this entire fluid cycle collapses. Instead of absorbing those nine liters, your body expels them. That is exactly why dehydration sets in so rapidly during a gut infection. You are not just losing the water you drink. You are losing your body’s own internal digestive fluids.
Using the Bristol Stool Chart for Accurate Self-Assessment
Patients frequently struggle to describe their bowel movements in a way that gives doctors useful information. That is why gastroenterologists worldwide rely on the Bristol Stool Chart, a standardized visual guide that eliminates guesswork.
The chart ranges from Type 1, which represents hard lumps indicating constipation, to Type 7, which is entirely liquid and signals severe, rapid-transit diarrhea. Types 3 and 4 are considered optimal, healthy stool. Types 6 and 7 point to significant inflammation and rapid intestinal transit. When a patient consistently reports passing Type 7 stools, I immediately begin evaluating for severe dehydration and electrolyte imbalance.
| Stool Type | Visual Description | Clinical Significance | Recommended Action |
| Type 4 | Smooth, soft sausage shape | Optimal, healthy bowel movement | Maintain current diet and hydration |
| Type 5 | Soft blobs with clear edges | Mild urgency or dietary distress | Monitor symptoms; add dietary fiber |
| Type 6 | Fluffy pieces, ragged edges | Early-stage diarrhea or mild enteritis | Start oral rehydration; track frequency |
| Type 7 | Entirely liquid, no solid pieces | Severe diarrhea with rapid transit | Follow the 48-hour rule; watch for dehydration |
Clinical Benchmarks: When Home Care Is No Longer Enough
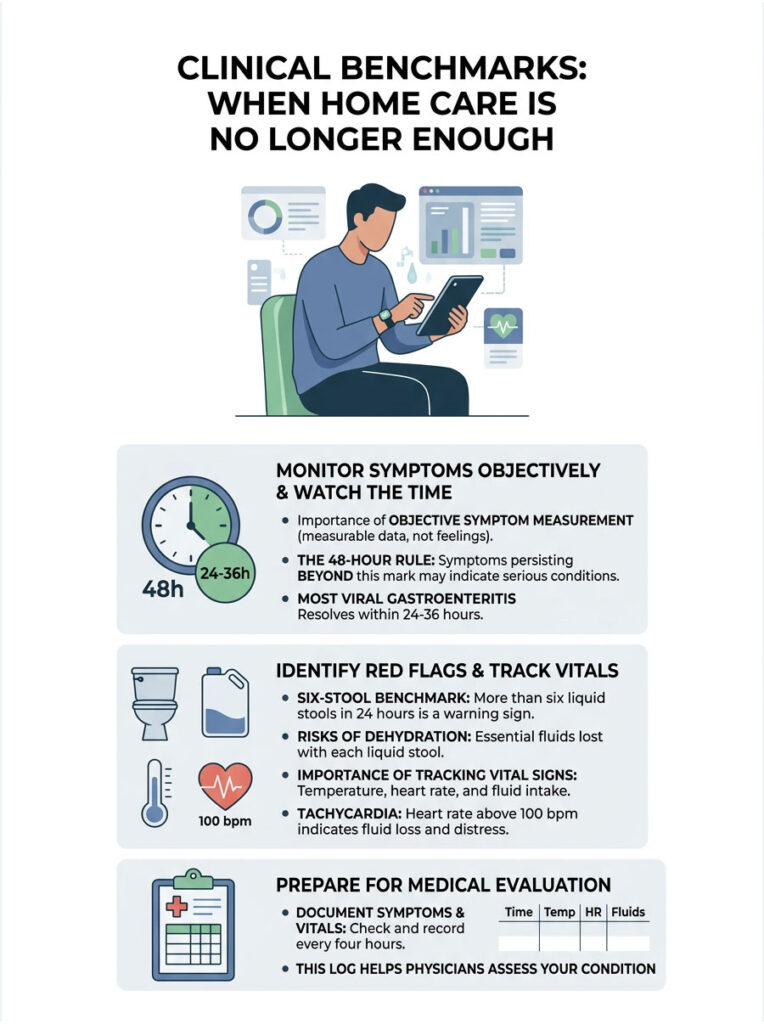
One of the most important parts of my job is teaching patients how to measure their symptoms objectively, rather than relying on fear or guesswork. Panic tends to set in during the first few hours of a stomach bug, but there is a specific, evidence-based timeline worth following before heading to the clinic.
Two primary rules guide our decision-making in the emergency room, and understanding them will tell you exactly when to worry about diarrhea in adults.
The 48-Hour Rule for Diarrhea
The most important clinical timeline is the 48-hour rule. If your symptoms persist beyond two full days, the situation changes significantly. Most viral gastroenteritis cases peak and start resolving within 24 to 36 hours.
When symptoms stretch past 48 hours, we start considering more serious possibilities: bacterial infections, parasitic illness, or underlying inflammatory conditions. I always encourage patients to write down the exact time their symptoms begin. Timestamping gives your healthcare team critical data. If you reach the 48-hour mark and are still passing liquid stools, a professional medical assessment is necessary. Ignoring this rule significantly raises your risk of hospitalization.
The 6-Stool Benchmark and Output Volume
Duration is only half the picture. Output volume matters just as much. Passing more than six unformed, liquid stools in a single 24-hour period is a major warning sign.
At that volume, home rehydration efforts almost never keep pace with fluid loss. Every liquid bowel movement drains essential water, sodium, and potassium from your body. Once you exceed six episodes in a day, cellular hydration drops rapidly and dangerously. That is the point where a formal gastroenterologist evaluation becomes necessary.
Monitoring Your Vital Signs at Home
Counting bathroom trips alone is not enough. You need to track your vital signs to understand the full scope of your illness. I recommend keeping a simple log of your temperature, heart rate, and fluid intake.
If your resting heart rate jumps above 100 beats per minute, your body is struggling. This condition, called tachycardia, is a direct response to falling blood volume. Your heart has to beat faster to compensate for having less fluid to circulate. Documenting these changes helps medical professionals evaluate your condition quickly. Write down your vitals every four hours to establish a clear clinical timeline.
Immediate Red Flags: When to Go to the Emergency Room
While duration and frequency are helpful guides, certain symptoms override every timeline. These warning signs demand immediate emergency care, regardless of whether you have been sick for two hours or two days.
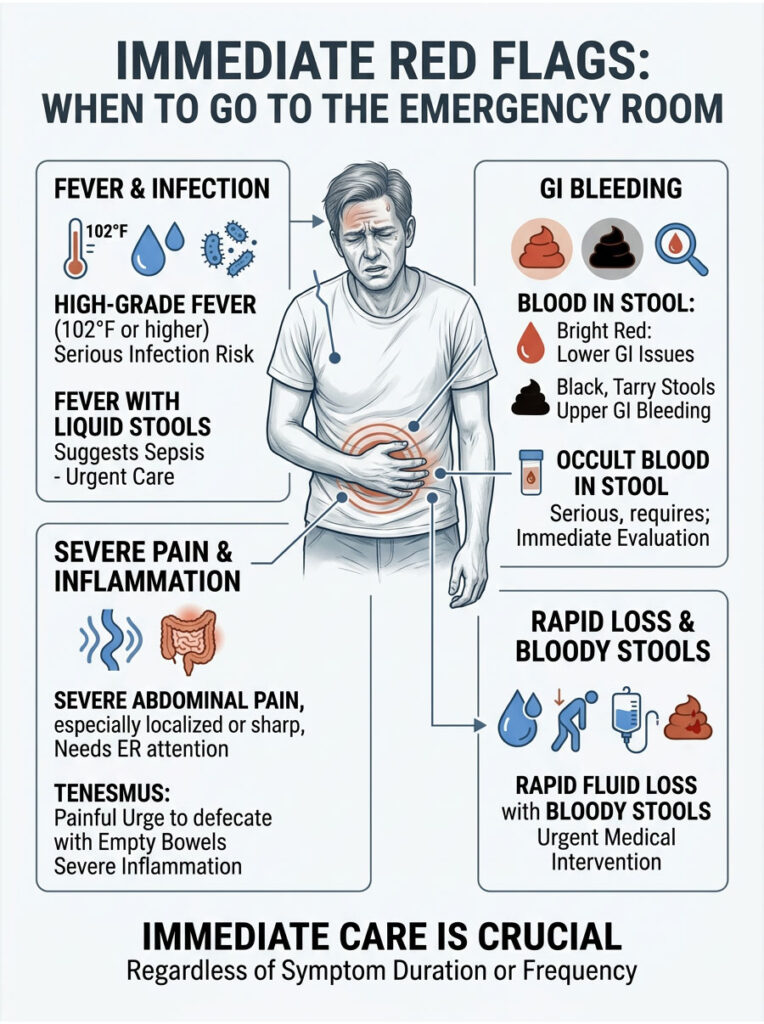
High-Grade Fever and the Risk of Systemic Infection
A mild temperature elevation is a perfectly normal immune response to a virus. However, a body temperature of 102°F or higher points to something much more serious. High fevers strongly suggest an invasive bacterial infection from pathogens like Salmonella, Campylobacter, or Shigella.
A high fever can also signal an acute flare of Inflammatory Bowel Disease. When fever accompanies liquid stools, the risk of sepsis increases substantially. The intestinal barrier can become compromised, allowing gut bacteria to enter the sterile bloodstream. If you record a temperature above 102°F, stop home management immediately. This is a definitive indicator of when to worry about diarrhea in adults.
Blood in Stool: Recognizing Gastrointestinal Hemorrhage
Seeing blood in the toilet is understandably alarming. In gastroenterology, we differentiate between two main types of GI bleeding. Bright red blood typically points to lower GI tract issues, such as severe colitis, acute rectal fissures, or bleeding hemorrhoids worsened by frequent wiping.
Black, tarry stools, on the other hand, indicate upper GI bleeding from the stomach or upper intestines. We call this dark, foul-smelling stool melena, and it is always a serious red flag. Sometimes bleeding is entirely invisible to the naked eye, a condition known as occult blood in stool. Bloody stools paired with rapid fluid loss require urgent medical intervention and usually an immediate colonoscopy.
Tenesmus and Severe Abdominal Pain
Mild, generalized cramping is expected with most stomach bugs. Severe pain that doubles you over is not. If your pain is localized to one area, sharp, or prevents you from standing upright, go to the ER immediately.
This kind of pain could indicate an intestinal obstruction, a bowel perforation, or even appendicitis hiding behind what seems like a simple gut infection. You should also watch for a distressing symptom called tenesmus, which is the constant, painful urge to pass a bowel movement even when your bowels are completely empty. Tenesmus indicates severe rectal inflammation and requires a thorough gastroenterologist evaluation.
The Silent Danger: Dehydration, Hypovolemia, and Electrolyte Loss
The most common reason for hospitalization and death related to gastrointestinal illness is not the infection itself. It is the resulting fluid loss. When you lose water faster than you can replace it, your total blood volume drops, a condition called hypovolemia. This causes your circulatory system to falter because there simply is not enough fluid to maintain normal blood pressure.
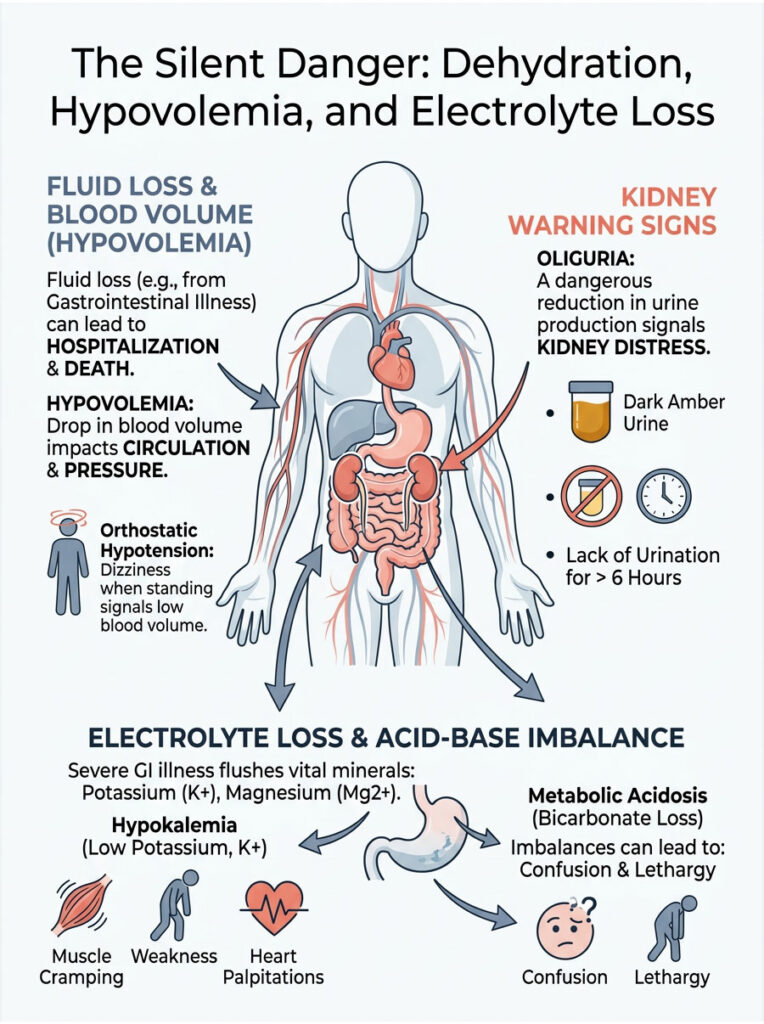
Oliguria and Orthostatic Hypotension
One of the first organ systems to fail during severe fluid loss is the kidneys. When blood volume drops, the kidneys intentionally reduce urine production to conserve remaining water. This dangerous reduction is called oliguria.
If you have not urinated in over six hours, you are already in trouble. If your urine is dark amber and strong-smelling, your kidneys are struggling to filter toxins. Another critical warning sign is orthostatic hypotension, which causes dizziness, lightheadedness, or faintness when you stand up from a seated or lying position. It means your blood volume is too low to pump adequate oxygen to your brain against gravity.
Hypokalemia: Dangerous Potassium Loss
During a severe bout of enteritis, you are not just losing water. You are flushing vital minerals out of your system rapidly. Potassium and magnesium take a particularly heavy hit during severe gastrointestinal illness.
Symptoms of hypokalemia include severe muscle cramping, profound weakness, and a heavy feeling in your limbs. Potassium is essential for muscle function, particularly the electrical signals that keep your heart beating properly. When potassium drops too low, you may experience tachycardia and frightening heart palpitations. If you feel your heart fluttering or racing while resting, you need immediate medical help. A sports drink will not fix severe hypokalemia. You need medical-grade intravenous replacement.
Metabolic Acidosis: A Hidden Complication
There is a biochemical complication that many people are unaware of. Your lower intestines contain bicarbonate, a base that helps regulate your blood’s pH balance. Rapid fluid loss flushes this bicarbonate out of your body.
As a result, your blood becomes too acidic, a dangerous state known as metabolic acidosis. This causes rapid, shallow breathing and extreme fatigue. In advanced stages, it leads to severe mental confusion and lethargy. If a loved one becomes confused, difficult to wake, or disoriented during a stomach illness, call 911 immediately. It means their brain is no longer receiving properly oxygenated blood.
| Expert Tip: Never try to fix severe dehydration by forcing down plain water alone. Drinking large amounts of water without adequate sodium and potassium will actually dilute your remaining blood minerals further, worsening electrolyte imbalance and potentially leading to a fatal condition called hyponatremia. Always use a scientifically formulated oral rehydration solution. |
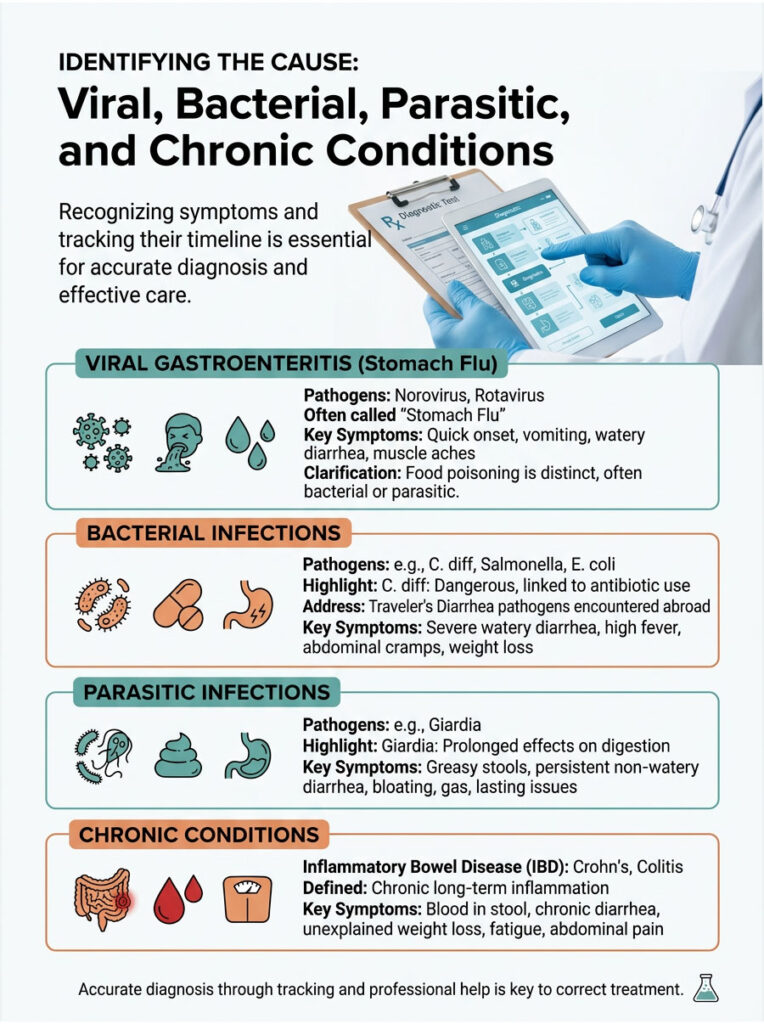
Identifying the Cause: Viral, Bacterial, Parasitic, and Chronic Conditions
Not all gastrointestinal illness behaves the same way. Knowing when to worry about diarrhea in adults often depends entirely on identifying the root cause. A standard viral infection is a completely different clinical picture from a chronic autoimmune flare-up.
As a specialist, my job is to play detective: examine recent history, look for patterns, and isolate the exact pathogen or mechanism behind the problem. Have you recently completed a course of antibiotics? Traveled internationally? Have a family history of autoimmune disease? These details point us toward the right diagnosis.
C. diff: One of the Most Dangerous Bacterial Infections
Clostridioides difficile is one of the most dangerous bacterial infections we encounter in the hospital. The rise of C. diff is directly linked to the widespread overuse of broad-spectrum antibiotics, which wipe out the protective bacteria in your gut and allow dormant C. diff spores to multiply and release destructive toxins.
Classic C. diff symptoms in adults include an unmistakable, foul-smelling odor, severe watery output, and intense abdominal cramping. If you develop liquid stools during or shortly after finishing antibiotics, contact your doctor immediately. C. diff requires highly targeted antibiotic therapy, and standard anti-diarrheal medications will make the infection significantly worse.
Viral Gastroenteritis: Norovirus and Rotavirus
Viral gastroenteritis is the leading cause of acute digestive illness in adults. Norovirus is notoriously contagious and spreads rapidly through cruise ships, nursing homes, and households. It typically causes explosive, sudden-onset symptoms.
The reassuring news is that norovirus is generally self-limiting, striking hard but clearing your system within 24 to 48 hours. Rotavirus is another common pathogen, though it affects children more frequently. Adults can still contract rotavirus, but symptoms tend to be milder due to partial immunity. With any viral infection, antibiotics are entirely useless. Your only priority is maintaining aggressive hydration until your immune system clears the virus.
Inflammatory Bowel Disease: Colitis Versus Enteritis
Sometimes the problem is not an external infection at all. Sometimes, your own immune system is attacking your digestive tract. Inflammatory Bowel Disease includes conditions like Crohn’s disease and Ulcerative Colitis.
Understanding the difference between colitis and enteritis matters for proper diagnosis. Enteritis is usually a temporary infection affecting the small intestine. Colitis involves chronic, long-term inflammation and ulceration of the large intestine. An IBD flare-up often presents with visible mucus in the stool, persistent fatigue, and unexplained weight loss. If your symptoms come and go over several weeks or months, this is not a simple virus. Chronic patterns require a thorough gastroenterologist evaluation to prevent permanent intestinal damage.
| Condition | Typical Duration | Key Symptoms | Clinical Urgency |
| Viral Gastroenteritis | 24 to 48 hours | Watery stool, mild nausea, low-grade fever | Low. Usually resolves with home hydration. |
| Bacterial Infection | 3 to 7 days | High fever, severe cramping, possible blood | Moderate to High. May need antibiotics. |
| C. diff Infection | Persistent | Extreme foul odor, watery stool, recent antibiotic use | High. Requires targeted medical treatment. |
| IBD Flare (Colitis) | Chronic or recurring | Mucus in stool, occult blood, weight loss, tenesmus | High. Requires gastroenterologist evaluation. |
Traveler’s Diarrhea and International Pathogens
Millions of adults experience severe gastrointestinal illness while traveling internationally. Traveler’s diarrhea occurs when you consume food or water contaminated with bacteria your body has never encountered, most commonly enterotoxigenic Escherichia coli.
Your immune system does not recognize these foreign strains, triggering a massive inflammatory response. If you are in a developing nation and develop a high fever or bloody stools, seek local medical care immediately. Do not attempt to fly home while actively experiencing severe dehydration.
Giardia and Parasitic Infections
Parasites are incredibly resilient and cause prolonged, miserable digestive problems. Giardia is a microscopic parasite commonly found in contaminated streams, lakes, and untreated drinking water. Campers, hikers, and international travelers carry the highest risk.
Symptoms are distinctly unpleasant: explosive, greasy, foul-smelling stools, severe bloating, and sulfur-tasting burps. Unlike a viral bug, giardia will not resolve in 48 hours. It can persist for weeks, causing significant weight loss and nutrient malabsorption. If your symptoms continue for more than a week after a camping or hiking trip, ask your doctor for a specialized stool parasite panel.
Food Poisoning Versus the Stomach Flu
Patients frequently ask how to tell the difference between food poisoning and a stomach bug. The primary distinction is the onset timeline. Food poisoning from bacterial toxins hits fast, typically causing vomiting and liquid stools within two to six hours of eating contaminated food. A viral stomach flu usually has an incubation period of 24 to 48 hours.
Food poisoning is violent but tends to burn out within a single day. Regardless of the cause, the initial treatment approach remains the same: focus on fluid replacement and monitor your vital signs closely. If you suspect food poisoning from a restaurant, report it to your local health department to help prevent wider outbreaks.
High-Risk Populations: The Elderly, Immunocompromised, and Pregnant Women
The clinical rules change dramatically depending on who is getting sick. A healthy 25-year-old can generally recover from a stomach bug with minimal intervention. But certain groups face a much steeper, more dangerous battle.
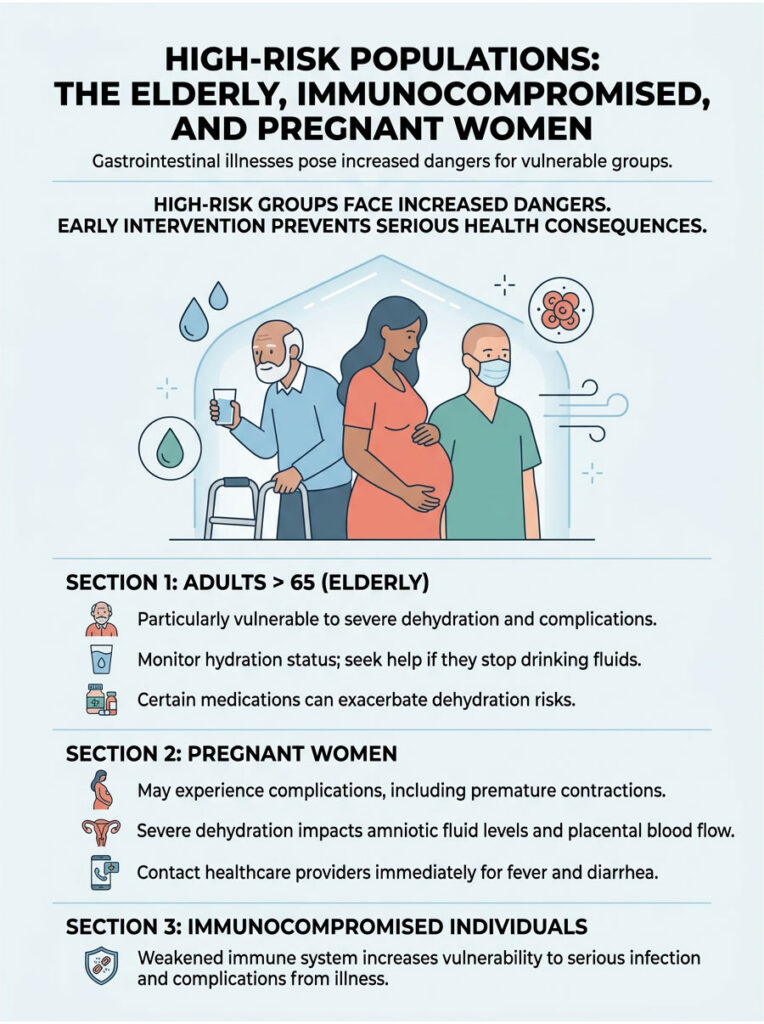
For high-risk populations, the window for seeking professional help shrinks considerably. We do not wait for the 48-hour rule to expire in vulnerable patients. Early intervention in these groups prevents organ failure and prolonged hospitalization.
Why Age Raises the Stakes
Adults over 65 have a much smaller physiological buffer against dehydration. As we age, our bodies naturally hold a lower percentage of water, and the brain’s thirst mechanism becomes less sensitive. Older adults often do not feel thirsty even when they are already significantly dehydrated.
CDC data shows that older adults face a threefold higher risk for rapid dehydration complications. Persistent watery stools can lead to acute kidney failure within hours in this age group. If an elderly family member is sick, monitor their urine output and mental clarity constantly. Do not hesitate to go to the ER if they stop drinking fluids.
Medication Interactions and Kidney Risks
Many adults take daily medications that amplify the dangers of rapid fluid loss. Blood pressure drugs, particularly ACE inhibitors and diuretics, are designed to remove fluid from the body. Combining prescription diuretics with a severe stomach illness creates an extremely dangerous situation.
This combination drastically increases the risk of acute kidney injury. If you take heart medications, blood thinners, or immunosuppressants, consult your doctor at the first sign of gastrointestinal distress. You may need to temporarily pause certain medications. However, never stop heart medication without speaking to a doctor first.
Pregnancy and Gastrointestinal Illness
Pregnant women face unique challenges during acute enteritis. The physical stress of severe cramping can sometimes trigger premature uterine contractions. Severe dehydration reduces amniotic fluid levels and compromises blood flow to the placenta.
Pregnant women are also more vulnerable to certain dangerous bacteria, including Listeria, which can cross the placental barrier and cause serious complications for the baby. If you are pregnant and develop a fever with liquid stools, contact your obstetrician immediately. You will likely need intravenous fluids to protect both you and your baby.
What to Expect During a Gastroenterologist Evaluation
When you make the decision to seek help, here is what happens next. A professional evaluation is a structured, evidence-based process. We do not guess. We run specific tests to identify the exact cause of your illness.
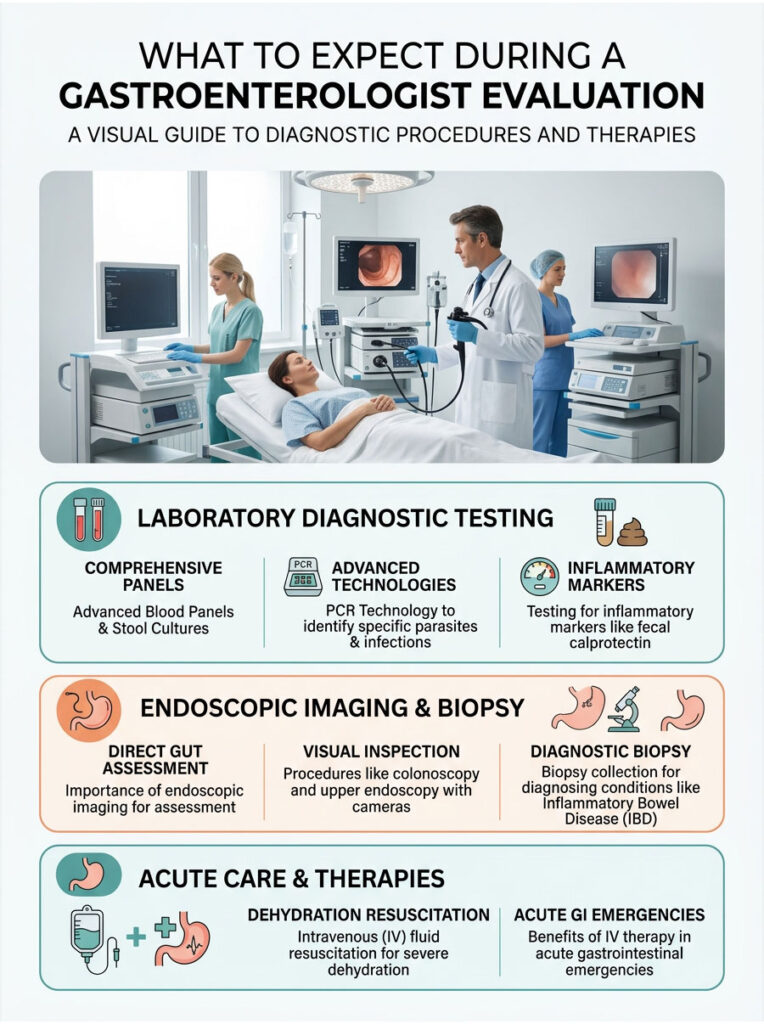
Stool Cultures and Advanced Blood Panels
The first step is comprehensive laboratory testing. We order stool panels using advanced PCR technology to identify the exact DNA of specific parasites, bacterial toxins, and viruses. This is the fastest, most accurate way to confirm C. diff or identify a Salmonella infection.
We also test for inflammatory markers like fecal calprotectin. Elevated calprotectin levels indicate active, severe inflammation in the gut lining and help us distinguish between colitis and enteritis. Blood tests check kidney function, white blood cell count, and screen for systemic infection.
Endoscopic Imaging and Direct Gut Assessment
If symptoms are chronic or we detect occult blood in the stool, we need to look directly inside the digestive tract. A colonoscopy or upper endoscopy allows us to visually inspect the intestinal lining for ulcers, precancerous polyps, or areas of active bleeding.
During these procedures, we take tiny tissue samples called biopsies, which are essential for diagnosing Inflammatory Bowel Disease or microscopic colitis. While endoscopy might sound intimidating, it is a routine, painless procedure done under sedation. It provides definitive answers and is the gold standard for ruling out colon cancer.
Intravenous Fluid Resuscitation
If you arrive at the clinic or emergency room with severe dehydration, our immediate priority is fluid resuscitation. When your gut is highly inflamed, drinking water often proves ineffective because the intestinal lining cannot absorb it due to rapid transit.
IV therapy delivers a precise, medically balanced mixture of saline, potassium, and magnesium directly into your bloodstream, bypassing the compromised digestive tract entirely. Within about an hour of IV therapy, most patients experience a dramatic improvement. Heart rate stabilizes, mental clarity returns, and electrolyte imbalance symptoms begin to resolve. IV fluids are genuinely lifesaving in acute gastrointestinal emergencies.
Safe Home Management Strategies for Mild Symptoms
If you have not reached the clinical benchmarks for an emergency visit, you can manage mild symptoms at home. However, effective home care requires a structured, evidence-based approach, not just sipping ginger ale and hoping for the best.
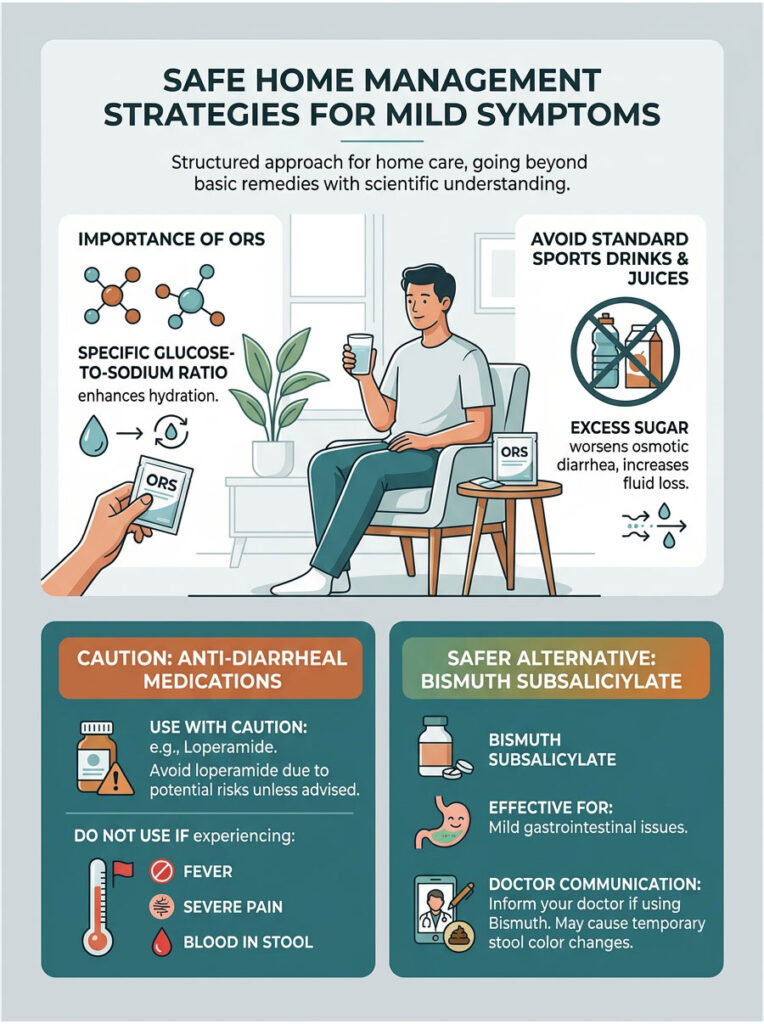
Oral Rehydration: The Right Way to Replace Fluids
The single most important tool in your home care kit is a proper Oral Rehydration Solution (ORS). Standard sports drinks, sodas, and fruit juices are poor choices. They contain too much refined sugar and far too little sodium.
Excess sugar in the gut actually pulls more water out of your tissues, actively worsening osmotic diarrhea and increasing fluid loss. A proper ORS uses a specific glucose-to-sodium ratio developed by the World Health Organization. This ratio activates the sodium-glucose cotransporter protein in your intestines, forcing your cells to absorb water even during active inflammation. Starting these solutions early is the best way to prevent dangerous potassium loss.
When to Avoid Anti-Diarrheal Medications
Over-the-counter drugs like loperamide are widely used, but they can be dangerous if taken at the wrong time. These medications work by slowing peristalsis, essentially paralyzing the gut to reduce bowel movements.
The danger is this: if you have an invasive bacterial infection or C. diff, slowing the gut traps toxic bacteria inside your body. This can lead to a life-threatening surgical emergency called toxic megacolon. Do not use motility-slowing drugs if you have a fever over 101°F, severe abdominal pain, or suspect any blood in your stool. When in doubt, let your body flush the infection naturally and focus entirely on aggressive hydration.
Bismuth Subsalicylate: A Safer Alternative for Mild Cases
Bismuth subsalicylate, the active ingredient in Pepto-Bismol, works differently from loperamide. It has mild antibacterial properties and coats the stomach and intestinal lining, reducing inflammation and slowing the flow of fluids into the bowel.
This makes it a somewhat safer option for mild traveler’s diarrhea. However, be aware that bismuth can turn your stool completely black. This is a harmless chemical reaction, but it can mimic the appearance of melena. Always inform your doctor if you have taken bismuth so they do not misinterpret dark stools as a sign of gastrointestinal hemorrhage.
What to Eat and Avoid During Acute Gastrointestinal Illness
What you put into your body during a gut crisis matters as much as your hydration strategy. Food can either soothe inflamed intestines or make things significantly worse.
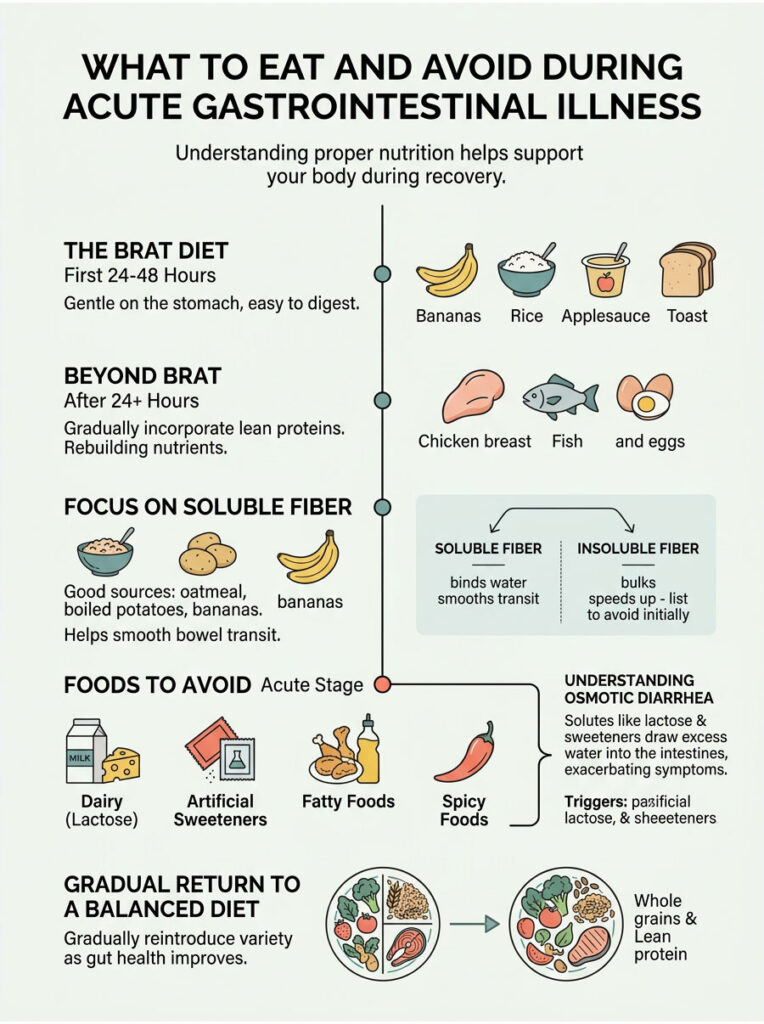
The BRAT Diet: Still Useful, But Not Enough on Its Own
For decades, doctors recommended the strict BRAT diet: Bananas, Rice, Applesauce, and Toast. These foods are bland, low in fiber, and easy for a compromised gut to process. They remain safe choices.
However, modern medicine recognizes that staying exclusively on the BRAT diet for too long deprives your body of essential protein and fat, both of which your immune system needs to fight the underlying infection. The current recommendation is to start with BRAT foods for the first 24 hours. Once nausea subsides, gradually introduce lean proteins like baked chicken or plain scrambled eggs. The goal is returning to a balanced, whole-food diet as quickly as your gut can tolerate it.
Foods That Make Osmotic Diarrhea Worse
While recovering, certain foods are off-limits. Dairy products top the restriction list because acute enteritis temporarily destroys the enzyme lactase in your gut, causing severe temporary lactose intolerance. Consuming milk or cheese during illness will trigger massive bloating and explosive stools.
You should also strictly avoid artificial sweeteners, particularly sugar alcohols like sorbitol and xylitol, which draw large amounts of water into the colon and worsen osmotic diarrhea. Finally, skip fatty, greasy, or heavily spiced foods. Fat delays stomach emptying and requires complex bile processing that your gut cannot handle during illness. Stick to simple carbohydrates and lean proteins until your stool returns to a Type 4 on the Bristol chart.
Why Soluble Fiber Helps Recovery
Not all fiber works the same way during gut distress. Insoluble fiber, found in raw vegetables and fruit skins, speeds up intestinal transit, which is the opposite of what you need. Soluble fiber, on the other hand, absorbs excess water in the colon and forms a soothing, gel-like substance that helps bulk up loose stools and slow rapid transit.
Good sources of soluble fiber include plain oatmeal, peeled boiled potatoes, and bananas. Adding these foods to your recovery diet helps solidify your output safely, providing structure to your bowel movements without irritating the intestinal lining.
Recent Research and Emerging Insights in Gut Health
The field of gastroenterology is evolving rapidly. We no longer view the digestive tract as a simple mechanical system. It is a complex, delicate ecosystem that depends heavily on a balanced population of microscopic bacteria.
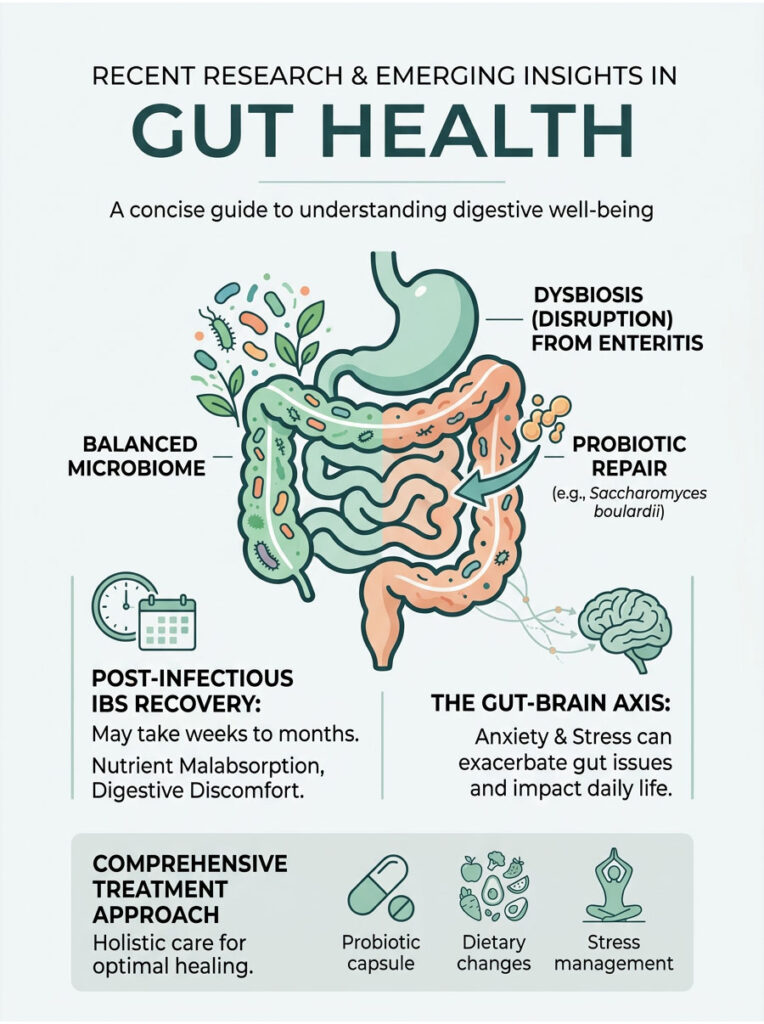
Microbiome Disruption and Recovery After Infection
Every severe bout of enteritis deals a significant blow to your gut microbiome. The violent flushing of liquid stools removes millions of beneficial bacteria. Current gastroenterology consensus emphasizes the importance of active microbiome recovery after infection.
Clinical studies have demonstrated strong results from specific probiotic strains in repairing the intestinal mucosal barrier. Saccharomyces boulardii, a beneficial yeast, has proven particularly effective in clinical trials, helping reduce the duration of acute infections and supporting post-infectious IBS recovery. Rebuilding your microbiome with targeted probiotics and high-fiber prebiotic foods is essential for long-term digestive health.
Post-Infectious IBS and Nutrient Malabsorption
What happens when the infection clears but your stomach still does not feel right? A severe bout of enteritis can damage the microscopic villi lining your intestines, triggering temporary irritable bowel syndrome or sudden food intolerances.
Post-infectious IBS recovery can take several weeks or even months. During this time, your gut may struggle with nutrient malabsorption, causing severe bloating, gas, and loose stools after eating certain trigger foods. Recovery requires a specialized elimination diet, high-quality probiotics, and patience. Rebuilding the intestinal mucosal barrier takes time.
The Gut-Brain Connection and Psychological Impact
The psychological toll of severe gastrointestinal illness deserves attention. Your gut and brain communicate directly through the vagus nerve, a relationship known as the gut-brain axis. Severe anxiety and stress can trigger rapid bowel motility, and chronic, unpredictable bowel habits cause significant psychological distress.
Many patients develop anxiety about leaving their homes or traveling. Treating chronic gut issues increasingly involves addressing this psychological component. Stress management, cognitive behavioral therapy, and gut-directed hypnotherapy are becoming standard parts of comprehensive gastroenterology care.
Summary and Key Takeaways
Knowing exactly when to worry about diarrhea in adults comes down to objectively monitoring three things: duration, volume, and systemic warning signs. Most cases are simple viral infections that resolve quickly on their own. But vigilance matters.
Track your symptoms using proper Bristol Stool Chart assessment to give your doctor accurate, useful data.
Follow the benchmarks: Enforce the 48-hour rule and watch for the 6-stool benchmark.
Never ignore red flags: High fever, severe localized pain, or blood in your stool demand immediate emergency care.
Prioritize proper rehydration: Use scientifically formulated Oral Rehydration Salts to combat electrolyte loss and prevent dangerous potassium depletion.
Seek early help if you are high-risk: If you suspect your medication is worsening symptoms, or if you belong to a vulnerable demographic, do not wait.
Schedule a comprehensive gastroenterologist evaluation immediately if symptoms turn chronic. Proactive hydration, careful dietary management, and early medical intervention are your strongest defenses. Protect your gut, monitor your vitals, and never hesitate to seek professional care when the warning signs appear.
Frequently Asked Questions
What is the 48-hour rule for diarrhea in adults?
As a gastroenterologist, I advise patients that the 48-hour rule is a critical clinical benchmark. Most viral gastroenteritis cases begin to resolve within 36 hours. If your symptoms persist beyond two full days, it suggests the cause may be a bacterial infection, parasite, or an underlying inflammatory condition that requires a professional medical evaluation to prevent systemic complications.
When does the frequency of bowel movements become a medical emergency?
We use the 6-stool benchmark to determine clinical severity. Passing more than six liquid stools in a 24-hour period is a major red flag. At this volume, the body loses water and electrolytes faster than home rehydration can typically replace, significantly increasing the risk of hypovolemia and acute kidney injury.
What are the early signs of severe dehydration or hypovolemia I should watch for?
You should monitor for oliguria, which is a significant reduction in urine output (not urinating for over six hours), and orthostatic hypotension, which manifests as dizziness or lightheadedness when standing up. These symptoms indicate that your blood volume has dropped to a level where your circulatory system and kidneys are struggling to function.
How can the Bristol Stool Chart help me describe my symptoms to a doctor?
The Bristol Stool Chart is the gold standard diagnostic tool we use to categorize transit time. Type 6 stools (fluffy pieces with ragged edges) indicate early-stage enteritis, while Type 7 stools (entirely liquid) signify severe inflammation and rapid transit. Tracking these types helps us assess the severity of your intestinal distress objectively.
Why is a high-grade fever concerning when accompanied by diarrhea?
While a mild temperature is a normal immune response, a fever of 102°F or higher suggests an invasive bacterial infection like Salmonella or Shigella, or a severe flare of Inflammatory Bowel Disease. High fevers increase the risk of sepsis, where the intestinal barrier is compromised and bacteria enter the bloodstream.
What does black or tarry stool indicate during a gastrointestinal illness?
Black, tarry, and foul-smelling stool, known clinically as melena, is a red flag for upper gastrointestinal hemorrhage. This is a medical emergency that requires immediate evaluation. However, be aware that bismuth subsalicylate (Pepto-Bismol) can also turn stool black; if you haven’t taken bismuth, seek emergency care for any dark stools.
Can antibiotics actually cause diarrhea symptoms?
Yes, this is a frequent concern in my clinic. Broad-spectrum antibiotics can disrupt the healthy microbiome, allowing Clostridioides difficile (C. diff) to proliferate. C. diff symptoms in adults include watery output with a distinct, foul odor and intense cramping. If you develop diarrhea during or after an antibiotic course, you need a specific stool PCR test.
What are the symptoms of hypokalemia resulting from fluid loss?
Hypokalemia, or low potassium, is a dangerous complication of prolonged diarrhea. Symptoms include severe muscle cramping, profound weakness, and cardiac issues like tachycardia (rapid heart rate) or palpitations. These imbalances often require intravenous replacement because the inflamed gut cannot absorb oral minerals efficiently enough.
Is it safe to take over-the-counter anti-diarrheal medications like loperamide?
Loperamide should be used with extreme caution. If you have a high fever, bloody stools, or a suspected bacterial infection, slowing down peristalsis with anti-diarrheals can trap toxins in the colon. In severe cases, this can lead to toxic megacolon, a life-threatening surgical emergency. Never use these meds if you have systemic red flags.
How does the BRAT diet fit into modern recovery protocols?
While the BRAT diet (Bananas, Rice, Applesauce, Toast) is helpful for the first 24 hours because these foods are low-fiber and easy to digest, it is nutritionally incomplete. Modern protocols suggest transitioning to lean proteins like baked chicken as soon as nausea subsides to provide the amino acids necessary for the immune system to repair the intestinal mucosal barrier.
What is the difference between Colitis and Enteritis?
Enteritis typically refers to an acute, often temporary infection or inflammation of the small intestine. Colitis involves the large intestine (colon) and is often associated with chronic conditions like Ulcerative Colitis or Crohn’s Disease. We differentiate between them using inflammatory markers like fecal calprotectin and endoscopic imaging.
Why are elderly adults at higher risk for diarrhea complications?
Older adults have a lower physiological water reserve and a less sensitive thirst mechanism. This means they can progress to severe dehydration and acute kidney failure much faster than younger patients. In the elderly, we often bypass the 48-hour rule and recommend medical intervention much earlier to prevent metabolic acidosis and organ stress.
Disclaimer
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Gastrointestinal emergencies can escalate rapidly. Always consult a qualified healthcare professional or seek emergency medical services immediately if you experience severe pain, high fever, or signs of significant dehydration.
References
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov – Provided statistics on acute diarrheal infections and C. diff infection rates in the United States.
- World Health Organization (WHO) – https://www.who.int – Clinical guidelines for the formulation and use of Oral Rehydration Salts (ORS) in managing fluid loss.
- The American Journal of Gastroenterology – https://journals.lww.com/ajg – Source for the Bristol Stool Chart clinical application and diagnostic benchmarks for enteritis.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – https://www.niddk.nih.gov – Supporting data on the physiology of digestion, fluid absorption, and chronic IBD symptoms.
- Mayo Clinic – https://www.mayoclinic.org – Reference for symptoms of hypovolemia, orthostatic hypotension, and electrolyte imbalance complications.
- Journal of Clinical Medicine – Peer-reviewed research regarding post-infectious IBS recovery and the impact of the gut-brain axis on motility.