Seeing bright green in the toilet bowl is alarming. It is one of the most common questions patients bring to my gastroenterology clinic: what does green diarrhea mean? The sudden change causes immediate anxiety, which is completely understandable.
Table of Contents
As a board-certified gastroenterologist, I can tell you that stool color is a direct reflection of your digestive efficiency and gut health. While the appearance is visually startling, it is often just a harmless dietary byproduct. Sometimes, though, this color shift serves as a clinical signal for underlying transit issues or gut infections that need attention.
This guide covers the exact physiological mechanisms behind green stool, from dietary triggers and infections to specific medical red flags. By the end, you will know exactly how to evaluate your own situation and when you need professional care.
Quick Answer: Green diarrhea typically means food is moving through your intestines too quickly for bile to break down completely. This rapid transit leaves the bright green pigment of raw bile intact. While it is often caused by leafy greens or artificial dyes, it can also signal viral infections, food poisoning, or bile acid malabsorption requiring medical attention.
Key Digestive Statistics
- Normal Transit Time: Healthy digestion takes 24 to 72 hours from eating to excretion.
- Rapid Transit: Watery output often indicates a transit time under 10 hours.
- Antibiotic Impact: Up to 25% of patients experience microbiota disruption after broad-spectrum antibiotics, per the American College of Gastroenterology.
- Foodborne Illness: The CDC estimates 48 million Americans get sick from foodborne diseases annually.
- Gallbladder Removal: Up to 20% of patients experience chronic digestive changes after cholecystectomy.
- Bile Recycling: A healthy system recycles 95% of bile acids back to the liver.
- Dehydration Risk: Severe fluid loss can become a systemic threat within 24 hours.
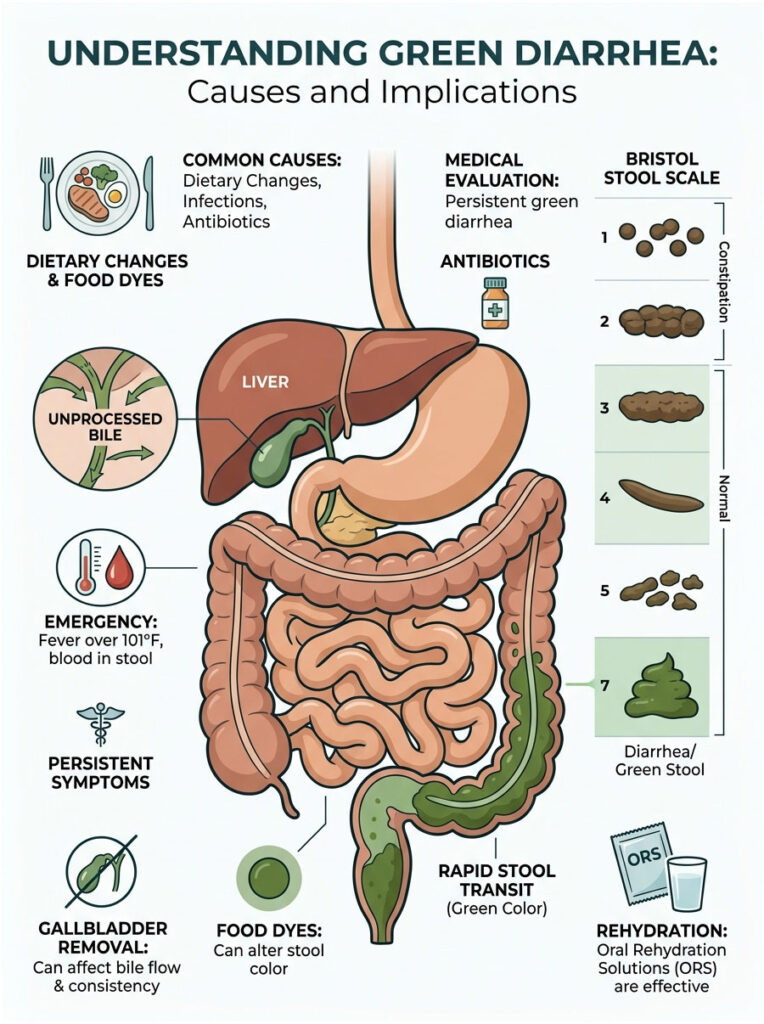
The Physiology of Stool Color: Why It Turns Green
The Role of Bile and the Liver
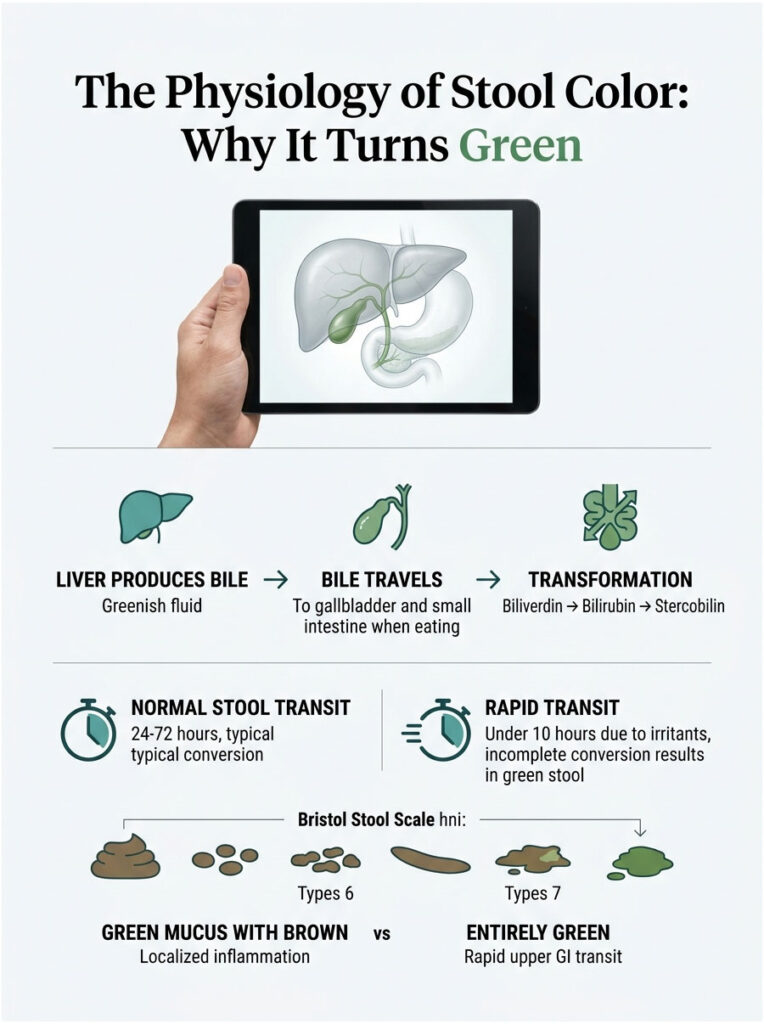
Your liver produces bile, a thick, alkaline fluid that is naturally bright green or yellowish-green. After manufacture, bile travels through the hepatic duct and gets stored in the gallbladder. When you eat, especially fats, the gallbladder contracts and squirts bile into the small intestine.
Bile’s primary job is to emulsify dietary fats, much like dish soap breaking up grease in a pan. Without it, your body cannot absorb essential fatty acids or fat-soluble vitamins like A, D, E, and K.
Because bile starts out bright green, the initial mixture in your upper GI tract is also green. The color only changes as food moves further through the system.
The Chemical Breakdown: Biliverdin to Stercobilin
The green color of bile comes from a pigment called biliverdin. As food moves slowly through the twenty feet of small intestine, gut bacteria facilitate a complex chemical transformation. They convert green biliverdin into a yellow-orange compound called bilirubin.
As waste continues into the colon, bacteria break bilirubin down further into stercobilin, the molecule responsible for the typical brown color of healthy stool.
This entire conversion requires significant time. If the biological clock runs out too quickly, the reaction stops halfway, and you are left with the original green starting color.
The Rapid Transit Mechanism
In gastroenterology, rapid stool transit time describes waste moving abnormally fast through the intestines. A healthy cycle takes 24 to 72 hours, providing plenty of time for the biliverdin-to-stercobilin conversion.
When the gut is irritated by a virus, spicy food, or psychological stress, the intestines essentially panic. They secrete extra water and contract forcefully to flush the irritant out. Processing time can drop from 48 hours to under 10.
At that speed, gut bacteria simply do not have enough time to convert the green biliverdin into brown stercobilin. The green color you see is literally raw, unprocessed bile exiting your body, a direct visual indicator of digestive speed.
The Bristol Stool Scale Connection
The Bristol Stool Scale is a clinical tool that classifies stool into seven categories based on shape and consistency. Types 1 and 2 indicate constipation. Types 3 and 4 are healthy and well-formed.
Rapid transit issues show up at the other end: Type 6 is fluffy and mushy with ragged edges, and Type 7 is entirely liquid. If your output matches Type 6 or 7, your gut lining is inflamed and secreting excess fluid rather than absorbing it. This is why dehydration becomes critical so quickly.
Clinical Tip: Green mucus mixed with brown stool often points to localized colon inflammation. Entirely green liquid, on the other hand, points to an upper GI rapid transit issue.
Dietary Causes of Green Diarrhea
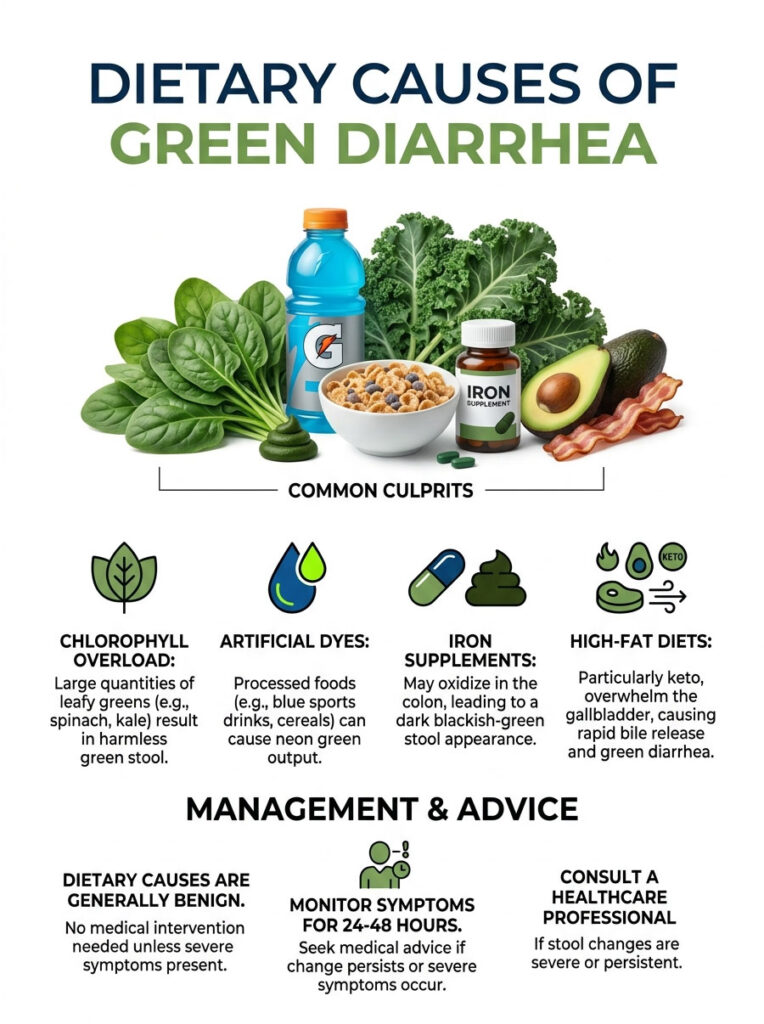
Chlorophyll Overload and Green Juicing
Health enthusiasts frequently experience this completely harmless phenomenon. Chlorophyll is the pigment that gives plants their green color. If you consume large quantities of spinach, kale, broccoli, or bok choy, especially as concentrated juices without the binding fiber, the excess pigment passes straight through the colon.
This is one of the most common benign causes of green stool and requires no medical intervention.
Artificial Dyes and Processed Foods
The artificial dye does not even need to be green. Blue, purple, and black synthetic dyes mix with yellow stomach acids and green bile to create neon green output. Common offenders include blue sports drinks, grape-flavored sodas, dark frosting, and colorful breakfast cereals.
Because sugary liquids pass through the stomach quickly, they often cause mild rapid transit. If you notice strange colors after a party or celebration, artificial dyes are almost certainly the cause.
Iron Supplements and Anemia Treatments
Iron supplements are notorious for changing stool color. While iron typically turns waste dark and tarry, unabsorbed iron salts can oxidize in the colon, creating a dark blackish-green appearance.
This is a completely standard side effect of oral iron therapy. Unless accompanied by severe stomach cramps, there is no need to stop the medication.
High-Fat Diets and the Keto Effect
The ketogenic diet, which relies on very high fat intake, can overwhelm the gallbladder. Your body signals for massive bile release to handle the sudden fat load. If your system is not adapted, the excess bile acts as a natural laxative, causing a rush of liquid carrying raw green bile through the colon.
This usually resolves within a week as the liver and gallbladder adjust.
Dietary Causes at a Glance
| Category | Common Culprits | Transit Effect | Symptoms | Action |
| Dietary/Benign | Spinach, kale, blue/purple dyes, juices | Normal to slightly elevated | None (usually painless) | Monitor 24-48 hours |
| Supplements | Iron sulfate, prenatal vitamins | Normal to accelerated | Mild nausea, dark color | Continue; consult if painful |
| High-Fat/Keto | MCT oil, heavy cream, butter | Highly accelerated | Sudden urgency, mild bloating | Reduce fat intake temporarily |
| Medications | Certain NSAIDs, birth control, antacids | Slightly accelerated | Mild stomach upset | Review with pharmacist |
Infections and Microbiota Disruption
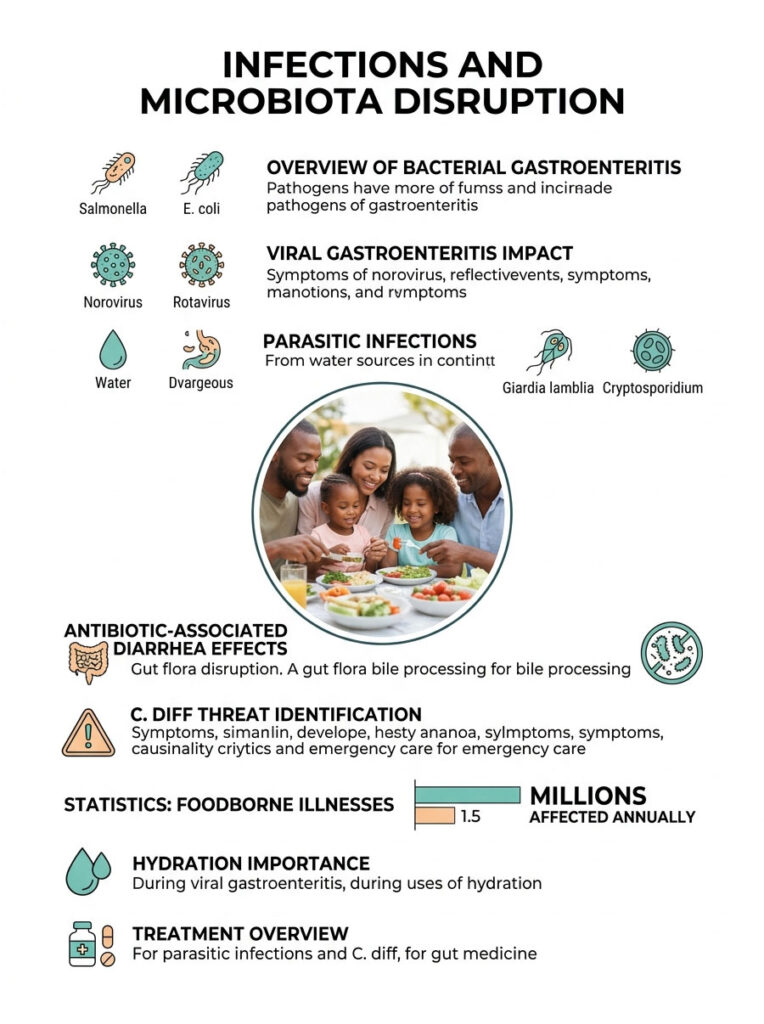
Bacterial Gastroenteritis and Food Poisoning
Pathogens like Salmonella, Campylobacter, and E. coli are commonly found in undercooked poultry, contaminated ground beef, or unwashed produce. Once ingested, they multiply rapidly and severely inflame the intestinal lining, physically stopping the intestines from absorbing water.
The CDC reports that foodborne illnesses affect tens of millions of Americans every year. In all these cases, the body prioritizes expelling the pathogen, entirely bypassing the normal biliverdin-to-stercobilin conversion.
Viral Gastroenteritis
Norovirus is a highly contagious virus that sweeps through cruise ships, schools, and nursing homes. It causes violent cramping, nausea, and explosive liquid output. In young children, Rotavirus is a frequent cause of green, watery stool.
These viruses attack the mature cells lining the small intestinal villi, preventing fluid absorption. Viral gastroenteritis hits suddenly, peaks within 48 hours, and causes such rapid transit that raw bile pours straight through. Hydration is the most critical factor during viral infections.
Parasitic Infections from Water Sources
Giardia lamblia is a parasite commonly found in contaminated streams, lakes, and untreated well water. Hikers and campers frequently contract it after drinking unfiltered water. Once inside the body, Giardia coats the small intestine, blocking fat absorption and causing foul-smelling, bright green liquid stool. Patients often report sulfur-smelling burps alongside bathroom symptoms.
Cryptosporidium is another waterborne parasite with similar effects. Unlike viral infections, parasitic infections rarely resolve on their own and usually require prescription anti-parasitic medication.
Antibiotic-Associated Diarrhea
Broad-spectrum antibiotics cannot distinguish between harmful bacteria and the beneficial ones in your gut. When antibiotics wipe out your healthy flora, the bacteria responsible for breaking down bile are destroyed. Bile stays green as it travels to the colon. Clinical data shows up to 25% of patients develop this side effect.
The C. diff Threat
Clostridioides difficile (C. diff) is a dangerous opportunistic bacterium that can take over when healthy gut bacteria are eliminated by antibiotics. It produces powerful toxins that severely damage the intestinal wall. Patients present with extremely frequent, urgent liquid stool with a distinct, sickly-sweet odor.
If you are passing liquid stool more than six times daily after antibiotics, accompanied by fever and severe abdominal pain, you need emergency medical testing. C. diff requires specific, targeted antibiotic therapy to prevent life-threatening colon damage.
Chronic Conditions and Malabsorption Syndromes
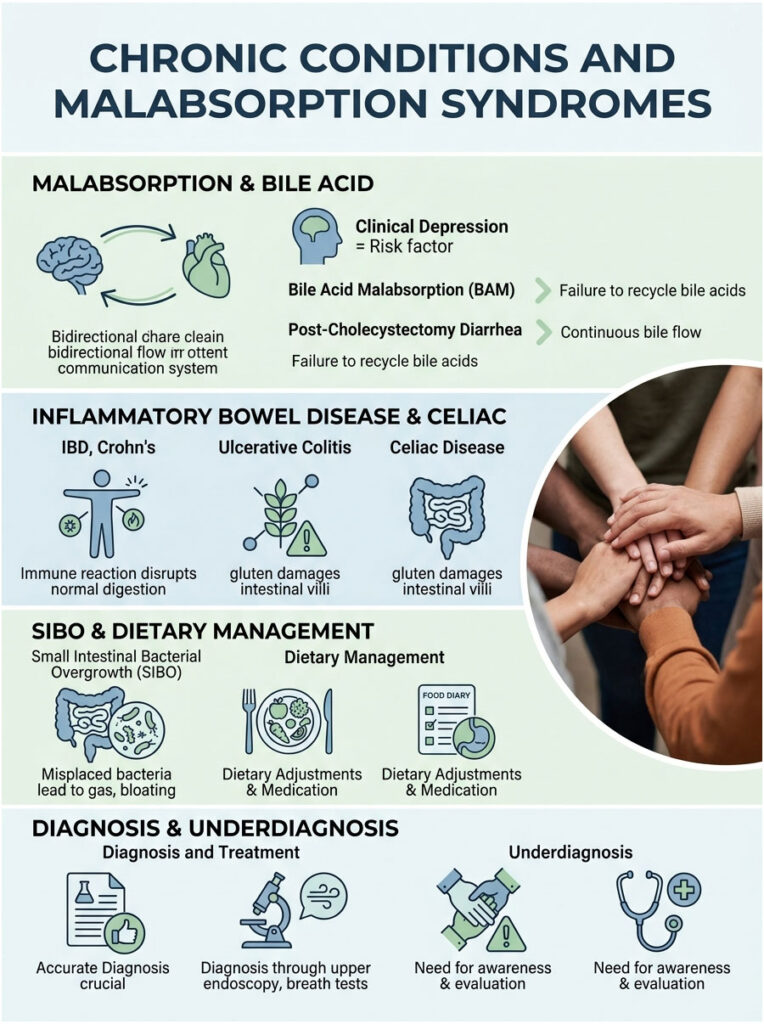
Bile Acid Malabsorption (BAM)
Normally, about 95% of bile acids are reabsorbed in the terminal ileum and recycled back to the liver. In bile acid malabsorption, this recycling mechanism fails. Massive amounts of harsh bile spill directly into the colon, irritating the lining, drawing in water, and triggering chronic rapid transit.
Patients with BAM often experience explosive urgency immediately after fatty meals. This condition is significantly underdiagnosed and can be treated with prescription bile acid sequestrants.
Post-Cholecystectomy Diarrhea
After gallbladder removal, the liver loses its storage facility for bile. Raw bile drips continuously into the small intestine around the clock. This unregulated flow can overwhelm the digestive tract, leading to chronic loose stools. Up to 20% of cholecystectomy patients experience this. Long-term management often requires dietary adjustments and binding medications.
Inflammatory Bowel Disease (IBD)
Crohn’s disease and Ulcerative Colitis both fall under Inflammatory Bowel Disease. In Crohn’s, inflammation can damage the terminal ileum, preventing normal bile reabsorption. In Ulcerative Colitis, the colon lining is too damaged to absorb water properly. Both lead to rapid transit and prevent the normal color conversion.
IBD patients also deal with severe cramping, weight loss, and fatigue. Management requires specialized immunosuppressant medications.
Celiac Disease
Celiac disease causes an extreme immune reaction to gluten. When a Celiac patient eats wheat, barley, or rye, the immune system attacks and destroys the villi lining the small intestine. Without healthy villi, the body cannot absorb fats or nutrients. Unabsorbed fats mix with raw bile, producing pale or brightly colored, foul-smelling stool.
Diagnosis requires an upper endoscopy. A strict, lifelong gluten-free diet is the only effective treatment.
Small Intestinal Bacterial Overgrowth (SIBO)
SIBO occurs when colon bacteria migrate into the small intestine where they do not belong. These misplaced bacteria prematurely ferment carbohydrates, producing excessive gas and bloating. They also break apart bile acids prematurely, rendering them useless for fat digestion.
This causes unabsorbed fats to rush into the colon, triggering rapid transit and green output. SIBO is diagnosed with a specialized breath test and usually treated with Rifaximin, a localized antibiotic.
When to Worry: Clinical Red Flags
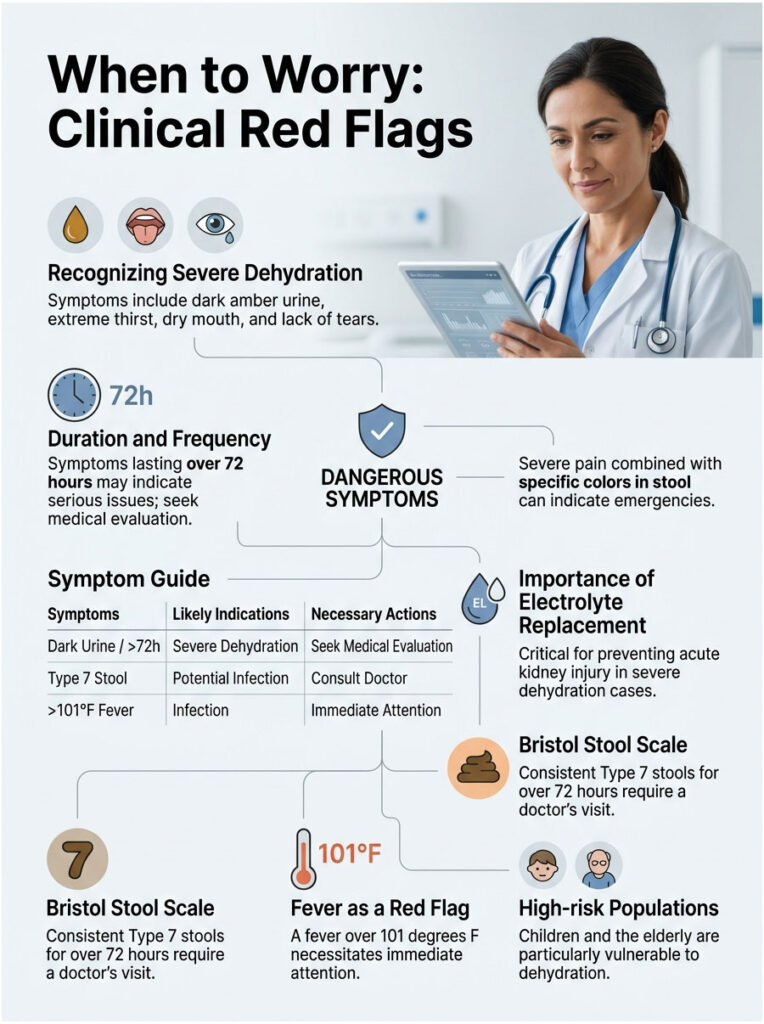
Recognizing Severe Dehydration
The most immediate threat from rapid transit is dehydration. When waste moves too fast, the colon cannot extract water for your organs. Dehydration can become systemic within 24 hours, especially in children and the elderly.
Watch for dark amber urine, extreme thirst, dry sticky mouth, and lack of tears when crying. In severe cases, orthostatic hypotension (dizziness when standing) develops. Aggressive electrolyte replacement is mandatory to prevent acute kidney injury.
Duration and Frequency of Symptoms
If symptoms clear within 48 to 72 hours, you likely had a mild viral bug or dietary reaction. However, liquid output lasting more than three consecutive days requires medical evaluation. Chronic fluid loss depletes potassium and sodium to dangerous levels.
If you are consistently at Type 7 on the Bristol Stool Scale for over 72 hours, call your doctor and request a stool culture.
Dangerous Accompanying Symptoms
Color alone is rarely an emergency. Color combined with severe pain is a major red flag. Mild cramping without fever usually points to a viral bug or food intolerance.
However, fever over 101 degrees F (38.3 degrees C) demands attention. Extreme localized abdominal pain that makes it hard to stand straight is another serious warning. Bright red blood or black tarry textures mixed with liquid suggest severe IBD, dangerous bacterial infections, or ischemic colitis, all of which require emergency care.
Symptom Guide: When to Seek Care
| Symptom Profile | Likely Indication | Setting | Action |
| Green stool, mild cramping, no fever | Dietary or mild viral | Home care | Oral rehydration, BRAT diet, rest |
| Lasting 3-4 days, mild dehydration | Persistent infection or microbiota imbalance | Primary care | Schedule appointment, request stool culture |
| High fever, cannot keep liquids down | Severe gastroenteritis or C. diff | Urgent care | IV fluids, targeted antibiotics |
| Severe pain, bloody stool, confusion | Potential sepsis, IBD flare, or ischemia | Emergency room | Immediate medical intervention |
A Gastroenterologist’s Recovery Protocol

Mastering Hydration and Electrolytes
Plain water is not enough when you are losing massive amounts of fluid. It lacks the essential salts and sugars your cells need to absorb moisture. Use Oral Rehydration Solutions (ORS) formulated to WHO standards, which use a precise glucose-to-sodium ratio that activates the SGLT1 transporter in your intestines.
Standard sports drinks are generally too high in sugar, which can worsen symptoms by drawing more water into the colon via osmosis.
Dietary Modifications for Slowing Transit
The classic BRAT diet (Bananas, Rice, Applesauce, Toast) works well for slowing transit. These foods are bland, gentle on the stomach, and high in soluble fiber. Soluble fiber absorbs excess liquid and adds bulk, helping move output from liquid Type 7 back toward a healthy Type 4.
Avoid dairy, greasy foods, and spicy meals, as these trigger further bile release and worsen symptoms.
Targeted Probiotics for Recovery
To restore the broken biliverdin-to-stercobilin conversion, you need to replenish gut bacteria. Not all probiotics are equal. Look for clinically researched strains that survive stomach acid.
Saccharomyces boulardii, a beneficial non-pathogenic yeast, actively binds to harmful pathogens and carries them out of the tract. It is especially effective for antibiotic-associated issues. Lactobacillus rhamnosus GG stabilizes the gut mucosal barrier and reduces the duration of viral symptoms.
Medications to Approach with Caution
Anti-motility drugs like loperamide (Imodium) are tempting, but if symptoms are caused by infection, these drugs can be dangerous. They paralyze colon muscles, trapping harmful bacteria and toxins inside the body. This can lead to toxic megacolon, a life-threatening condition.
Only use anti-motility drugs if you are certain your symptoms are diet-related, or if explicitly directed by a physician. When in doubt, let the infection run its course and focus entirely on hydration.
Stress Management and the Gut-Brain Axis
The gut-brain axis connects your emotional state directly to your digestive tract. Severe anxiety triggers the fight-or-flight response, which overstimulates the vagus nerve and forces the intestines to contract rapidly, causing fast transit even without infection.
Practice diaphragmatic breathing to calm the vagus nerve. Prioritize sleep, as sleep deprivation weakens the intestinal barrier. Sometimes, simply knowing this condition is temporary helps slow things down.
Clinical Case Studies

Case 1: Post-Surgical Struggle
A 45-year-old woman presented with explosive morning episodes that started three months prior. Her history showed a cholecystectomy four months earlier. Without a gallbladder, raw bile was leaking continuously into her intestines overnight.
I prescribed cholestyramine, a bile acid sequestrant. Within 48 hours, her transit normalized and output returned to a healthy brown Type 4.
Case 2: Antibiotic Aftermath
A 32-year-old man presented with urgent, brightly colored output and mild cramping after a 10-day course of amoxicillin. He feared a severe parasite. Since he had no fever, I ruled out C. diff and placed him on Saccharomyces boulardii with a BRAT diet. His symptoms resolved completely in four days.
Case 3: The Marathon Runner’s Mistake
A 28-year-old runner was terrified by neon-colored stool two days before her race. She had no pain, fever, or nausea. Her recent intake revealed nearly a gallon of bright blue sports drink. The Blue 1 dye mixed with stomach acid to create the color. Switching to plain water with natural electrolytes resolved everything by the next morning.
Case 4: The Camper’s Regret
A 55-year-old man arrived pale, exhausted, and severely dehydrated. He reported foul-smelling green liquid up to ten times daily for a week, plus sulfur burps and deep cramps. He had recently drunk from an unfiltered mountain stream. Stool culture confirmed Giardia lamblia. A course of metronidazole restored normal function over two weeks.
Summary and Key Takeaways
So, what does green diarrhea mean for your health? It is a clear visual indicator that your digestive system is moving too fast. Whether triggered by a big spinach salad, a viral infection, or antibiotics, the green pigment is simply unprocessed raw bile. Your gut bacteria did not have enough time to complete their color-changing chemistry.
- Diet is often to blame. Artificial dyes and large amounts of leafy greens are the most common, entirely harmless causes.
- Speed is the mechanism. Lack of time in the colon prevents the biliverdin-to-stercobilin conversion, leaving bile in its raw state.
- Hydration is critical. Prioritize medical-grade oral rehydration solutions to prevent systemic dehydration.
- Monitor the timeline. Symptoms lasting longer than 72 hours require a doctor’s evaluation and possible stool testing.
- Know the red flags. High fevers, severe pain, and bloody output are medical emergencies requiring immediate care.
While usually benign and self-limiting, persistent watery green stool always warrants medical evaluation. By understanding the Bristol Stool Scale and your body’s signals, you can manage these changes confidently and protect your digestive health.
Frequently Asked Questions
What does green diarrhea mean in terms of digestive physiology?
As a gastroenterologist, I explain to patients that green diarrhea is a direct visual indicator of rapid stool transit time. It means waste is moving through your intestines so quickly that your gut bacteria do not have enough time to chemically convert green biliverdin (raw bile) into brown stercobilin. The green color you see is literally unprocessed bile exiting the body.
Can eating large amounts of leafy greens cause green liquid stool?
Yes. This is known as chlorophyll overload. When you consume high concentrations of dark leafy greens like spinach, kale, or bok choy—especially in juiced form—the excess pigment can bypass normal digestive breakdown. This is a benign dietary byproduct and typically requires no medical intervention if it is painless.
Why did my stool turn green after taking a course of antibiotics?
Antibiotics often cause microbiota disruption, killing the beneficial bacteria responsible for breaking down bile pigments. Without these microbes, the biliverdin-to-bilirubin conversion process halts. Clinical data shows up to 25% of patients experience this. However, if this is accompanied by a foul odor and high fever, we must test for a C. diff infection.
What are the clinical red flags that indicate green diarrhea is a medical emergency?
You should seek immediate care if the diarrhea is accompanied by a fever over 101°F, hematochezia (bright red blood), or severe localized abdominal pain. Additionally, systemic signs of dehydration—such as dark amber urine, extreme dizziness (orthostatic hypotension), and a lack of tears—require urgent medical evaluation.
How does gallbladder removal affect stool color and consistency?
After a cholecystectomy, the liver lacks a storage tank for bile, causing it to drip continuously into the small intestine. This can lead to Bile Acid Malabsorption (BAM), where excess caustic bile irritates the colon and triggers chronic rapid transit. This often results in urgent, brightly colored liquid output after fatty meals.
Can artificial food dyes like blue or purple make diarrhea look green?
Surprisingly, yes. Synthetic dyes such as Blue 1, often found in sports drinks and sodas, do not break down during digestion. When these blue pigments mix with yellow stomach acids and green bile in the upper GI tract, the resulting mixture turns a neon green color by the time it reaches the toilet bowl.
How do doctors use the Bristol Stool Scale to diagnose this issue?
The Bristol Stool Scale is a diagnostic tool used to classify waste consistency. Green diarrhea typically falls into Type 6 (mushy pieces) or Type 7 (entirely liquid). These scores indicate that the gut lining is inflamed and secreting excess fluid rather than absorbing it, confirming a rapid transit mechanism.
What is the ‘Keto Dump’ and why does it cause green stool?
The ‘Keto Dump’ occurs when a sudden increase in high-fat dietary intake overwhelms the gallbladder. The body releases a massive surge of bile to emulsify the fats, which acts as a natural laxative. This rush of liquid carries raw green bile through the colon before it can be reabsorbed or chemically altered.
Why is plain water insufficient for rehydration during severe diarrhea?
Plain water lacks the essential salts and glucose needed to trigger the sodium-glucose linked transporter (SGLT1) in the intestines. For effective rehydration when the gut is inflamed, I recommend Oral Rehydration Solutions (ORS) that follow World Health Organization standards to force water across the intestinal wall.
Could a parasitic infection like Giardia be the cause of green diarrhea?
Yes. Parasites like Giardia lamblia, often contracted from untreated water sources, physically coat the small intestine. This creates a barrier that blocks fat absorption and causes foul-smelling, brightly colored liquid waste. Unlike viral bugs, parasitic infections usually require targeted prescription anti-parasitic medications.
Is it normal for iron supplements to cause greenish-black stool?
While iron supplements typically turn stool a tarry black, unabsorbed iron salts can also oxidize within the colon. This chemical reaction frequently creates a dark, forest-green or blackish-green appearance. As long as there is no severe cramping, this is a standard and expected side effect of anemia treatment.
How long should I wait before seeing a doctor for altered bowel habits?
In healthy adults, most viral or dietary issues resolve within a 48 to 72-hour window. If you are passing purely liquid waste for more than three consecutive days, you should schedule a primary care appointment for a comprehensive stool culture to check for pathogens or underlying malabsorption syndromes.
Disclaimer
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional or board-certified gastroenterologist before making health decisions or if you are experiencing severe symptoms like high fever, dehydration, or intense abdominal pain.
References
- Centers for Disease Control and Prevention (CDC) – https://www.cdc.gov/foodsafety/foodborne-germs.html – Data regarding the prevalence and impact of foodborne illnesses in the United States.
- American College of Gastroenterology (ACG) – https://gi.org/topics/antibiotic-associated-diarrhea/ – Clinical insights into microbiota disruption and antibiotic-associated digestive issues.
- University of Bristol – Bristol Stool Chart – The official diagnostic tool used to evaluate human waste consistency and transit time.
- World Health Organization (WHO) – Oral Rehydration Salts – Standards for electrolyte replacement and the physiological mechanisms of the SGLT1 transporter.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – https://www.niddk.nih.gov/health-information/digestive-diseases/ – Information on chronic malabsorption syndromes and bile acid issues.
- Journal of Clinical Gastroenterology – Research Study – Clinical efficacy of Saccharomyces boulardii in treating antibiotic-associated diarrhea.