
Roughly 20 million American adults live with eczema. Another 7.4 million have psoriasis. The two skin conditions share a stunning amount of overlap, including red patches, scales, itching, and the same emotional drain when nothing seems to work. Yet they’re driven by completely different biology, and treating the wrong one wastes money and sometimes makes the rash worse.
Table of Contents
| Quick Answer: Psoriasis usually shows thick, well-defined plaques topped with silvery scales, often on elbows, knees, scalp, and lower back, and tends to burn or sting. Eczema usually looks redder or pinker, less defined, very itchy, and prefers skin folds (inner elbows, behind knees) plus hands and face. Eczema typically starts in childhood; psoriasis often appears in young adulthood. Both are non-contagious chronic conditions that need different treatments. |
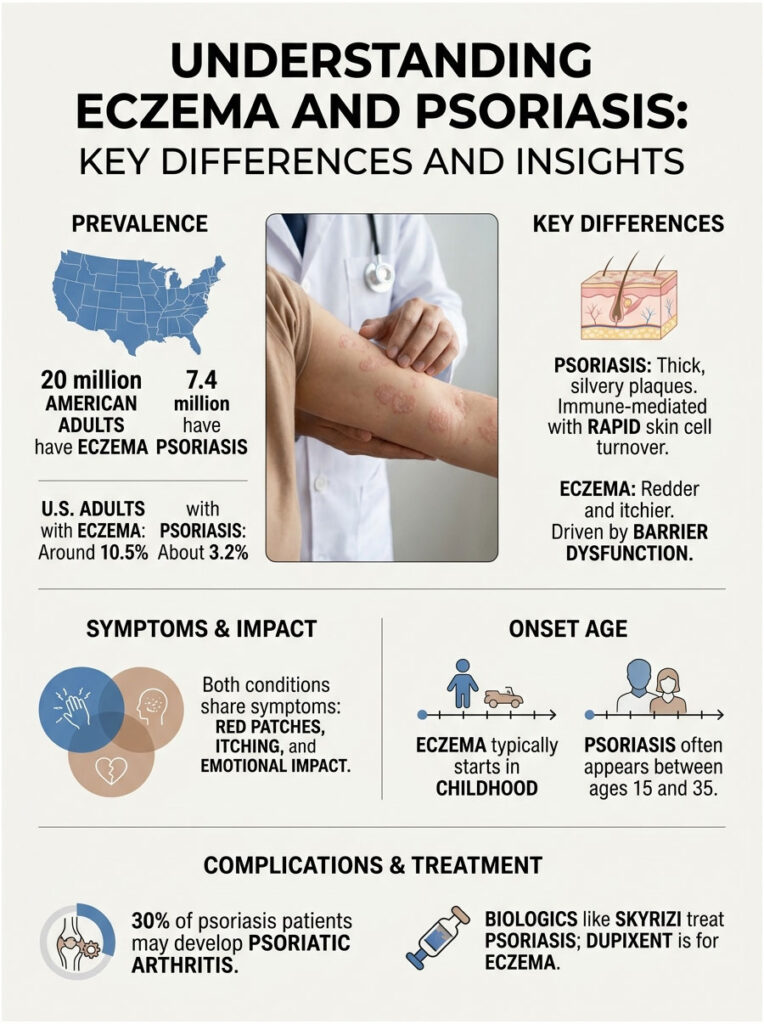
| At a Glance • Psoriasis is an immune-mediated condition with fast skin cell turnover; eczema is a barrier-dysfunction condition with allergic-type triggers. • Intensely itchy and sometimes weeping skin suggests eczema; thick silvery plaques suggest psoriasis. • Eczema usually starts in babyhood; psoriasis often appears between ages 15 and 35. • About 3.2% of US adults have psoriasis; about 10.5% of US adults have eczema in recent estimates. • About 30% of people with psoriasis go on to develop psoriatic arthritis. • Treatments differ; biologics like Skyrizi target psoriasis, while Dupixent targets eczema. • Neither condition is contagious, and neither can be caught from another person. |
The Fast Way to Tell Psoriasis From Eczema
Psoriasis vs eczema looks like the same problem at first glance, but the underlying biology and the visible patterns are different enough to identify with patience and the right clues. In cases reviewed by our medical team, getting this distinction right at the start typically cuts months off a patient’s treatment journey.
What Psoriasis Actually Is
Psoriasis is a chronic immune-mediated skin disease where the immune system tells skin cells to grow too fast. Normal skin cycles in about 28 days. In psoriasis, cycles drop to 3 to 5 days, which causes immature cells to pile up and form thick plaques with silvery or whitish scales.
The most common form is plaque psoriasis, which accounts for about 80 to 90% of cases. Less common types include guttate, inverse, pustular, and erythrodermic psoriasis. Around 30% of psoriasis patients also develop psoriatic arthritis over time, which affects joints and tendons.
What Eczema Actually Is
Eczema is an umbrella term, with atopic dermatitis being the most common type. It’s driven by a damaged skin barrier and an overactive immune response, often genetically inherited through filaggrin gene variants that weaken the skin’s outer layer.
Eczema patches lose moisture quickly, react to soaps and fragrances, and itch intensely. Other forms include contact dermatitis, dyshidrotic eczema, nummular eczema, seborrheic dermatitis (scalp), and stasis dermatitis (legs). Our medical reviewers at HealthCareOnTime see all of these labeled simply as “rash” in patient charts when proper typing would change the treatment plan entirely.
60-Second Self-Check
Three quick questions usually settle the psoriasis vs eczema debate before you spend money on the wrong cream.
- Are the patches thick and silvery, or thin and oozing? Thick and silvery leans psoriasis; thin, raw, or weeping leans eczema.
- Where on the body? Outsides of elbows and knees, scalp, and lower back point to psoriasis. Insides of elbows, behind knees, hands, face, and skin folds point to eczema.
- How old were you when it started? Infancy or early childhood points to eczema. Teens, twenties, or thirties points more often to psoriasis.
Two of three matching answers gives you a strong working diagnosis. Three out of three is close to certain, though a dermatologist still needs to confirm with examination and sometimes a biopsy.
| Feature | Psoriasis | Eczema (Atopic Dermatitis) | Why It Matters |
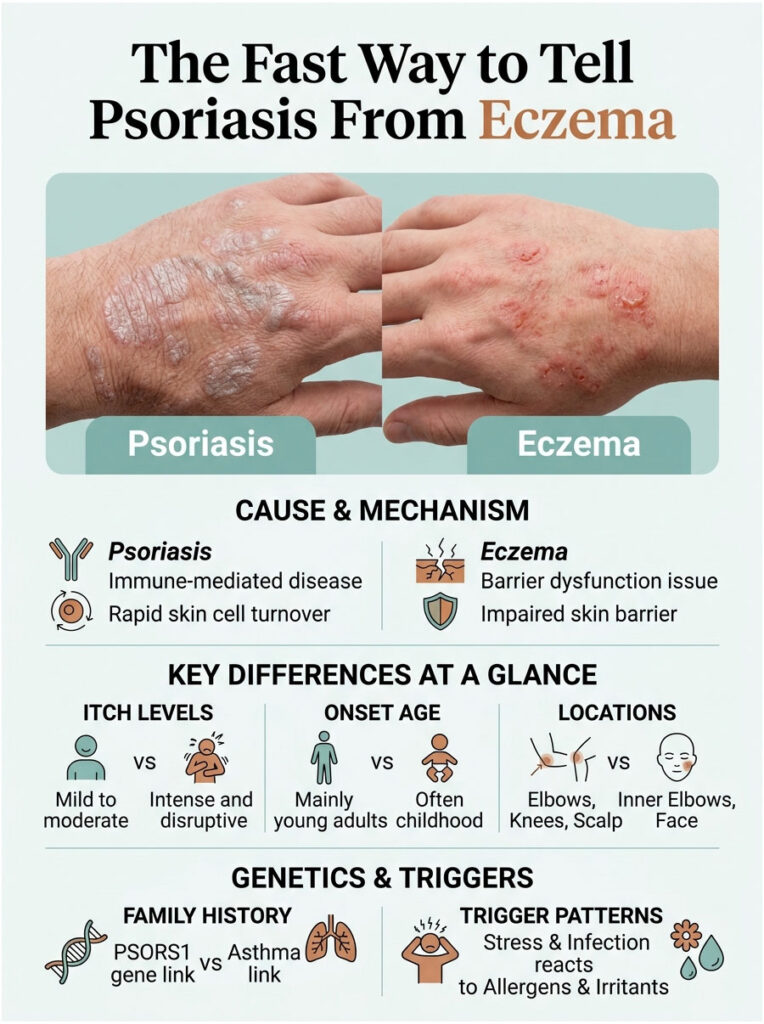
| Underlying cause | Immune-mediated; rapid skin cell turnover | Barrier dysfunction + immune sensitivity | Drives different treatments |
| Appearance | Thick, well-defined plaques with silvery scales | Red or pink patches, less defined, often oozing | Visual identification clue |
| Itch level | Mild to moderate; often burns or stings | Intense, often disrupts sleep | Sleep-stealing itch is a key flag |
| Typical onset age | 15 to 35 years (peak); also 50 to 60 | Infancy or early childhood | Age narrows the diagnosis fast |
| Body locations | Elbows, knees, scalp, lower back, nails | Inner elbows, behind knees, hands, face | Pattern is a strong tell |
| Family history | Genetic link, PSORS1 gene cluster | Strong link to asthma, hay fever (atopic triad) | Family asthma points to eczema |
| Trigger pattern | Stress, infection, cold weather, certain meds | Allergens, irritants, dry air, fragrances | Different triggers, different avoidance |
| Skin texture | Silvery scale, may bleed if scraped (Auspitz sign) | Cracked, weepy, sometimes crusted | Helps narrow workup |
| Contagious? | No | No | Neither spreads person to person |
Table 1: Psoriasis vs eczema side-by-side comparison. Sources: Rush University Medical Center, Medical News Today, NIAID.
Why It Matters: US Numbers You Should Know
The financial and quality-of-life weight of getting psoriasis vs eczema wrong is bigger than most patients realize.
How Common Are Psoriasis and Eczema in America?
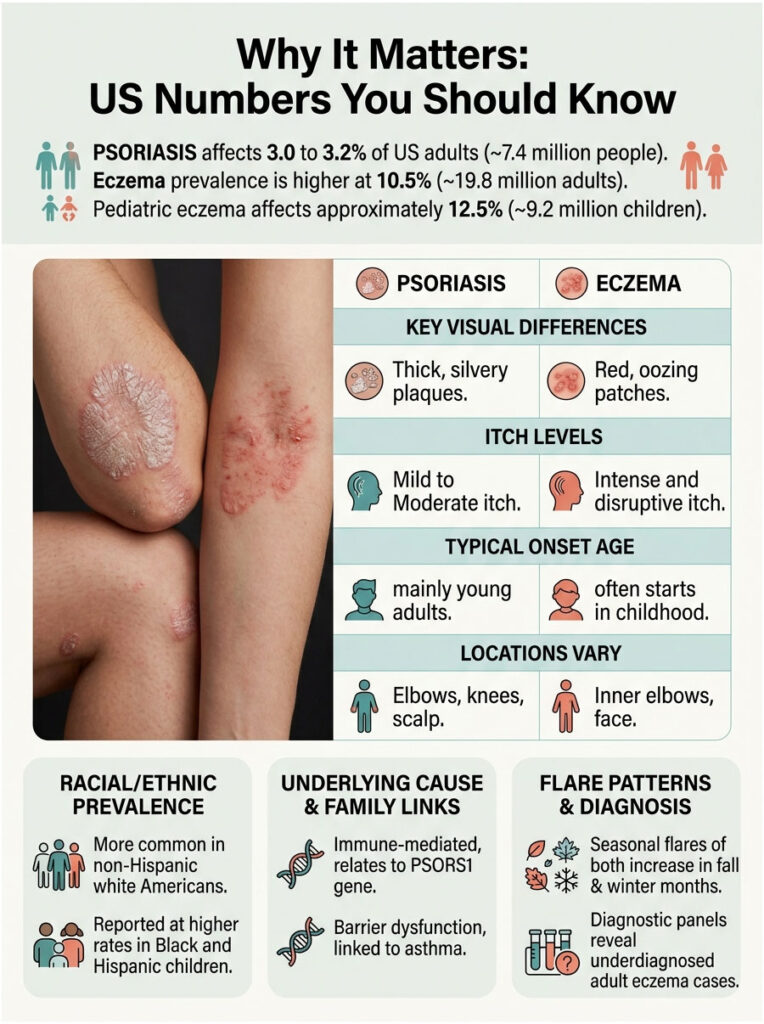
Psoriasis affects roughly 3.0 to 3.2% of US adults, which translates to about 7.4 million people, according to NHANES data published in JAAD. The rate has been stable for the past 15 years.
Eczema is more common. The latest JAAD analysis using 2024 National Health Interview Survey data put US adult atopic dermatitis prevalence at 10.5%, or roughly 19.8 million adults. About 9.2 million US children carried the diagnosis, with the strongest growth among kids.
The NIAID puts the overall pediatric range at 10 to 30%, with 2 to 10% in adults. The disparity reflects how many adults outgrow childhood eczema or stop seeking care once symptoms get milder. Patients booking inflammatory panels with us frequently turn out to have low-grade adult eczema that flew under the radar for decades.
Who Gets Each Condition
Psoriasis is more common in non-Hispanic white Americans. Eczema affects all races but is reported at higher rates in Black and Hispanic children, and tends to be underdiagnosed in skin of color because the classic “redness” is harder to spot.
Both conditions cluster in families. Patients arriving with a known parent or sibling diagnosis usually speed up the workup considerably, since family pattern alone often points strongly toward one diagnosis.
| Condition | US Prevalence / Volume | Annual Impact | Source |
| Psoriasis (adults) | 3.2% (~7.4 million US adults) | ~150,000 new cases/year | JAAD / NHANES |
| Atopic dermatitis (adults) | 10.5% (~19.8M in 2024) | Up from 7.3% in 2021 | JAAD 2026 |
| Atopic dermatitis (children 0-17) | ~12.5% (~9.2M in 2024) | Significant increase since 2021 | JAAD 2026 |
| Psoriatic arthritis (PsA) | ~30% of psoriasis patients | ~2.2 million US adults | National Psoriasis Foundation |
| Multi-type eczema | 1 in 5 adult eczema patients | Most common pair: AD + seborrheic | NEA / JID 2025 |
| Pediatric eczema (highest states) | Up to 18.1% (East Coast) | Higher in metro, Black children | NCBI / NSCH |
Table 2: USA prevalence and impact of psoriasis vs eczema.
Across the diagnostic network our lab partners support, skin condition inflammatory panel orders climb noticeably in fall and winter, which fits the well-documented seasonality of both psoriasis and eczema flares in cold, dry US climates.
Symptom Decoder: 9 Clues Your Skin Is Giving You
Skip the guessing. Run your symptoms through these nine signals and the psoriasis vs eczema question usually answers itself.

Clue 1: Where the Patches Show Up
Psoriasis loves extensor surfaces: the outer elbows, the front of knees, the scalp, the lower back, and the nails. Plaques there are a near-classic giveaway.
Eczema favors the flexures: the inner elbows, the back of the knees, the wrists, the neck, the hands, and the face, especially around the eyes. Distribution alone resolves about 60% of cases in dermatology practice.
Clue 2: Color and Scale Texture
Psoriasis plaques are typically thick, raised, and topped with loose silvery-white scales that flake when scratched. Beneath the scale, the skin is bright red or salmon-colored in light skin, and darker, sometimes purplish, in darker skin tones.
Eczema patches are usually thinner, redder, sometimes pink or grayish, and often weep clear fluid or crust over when irritated. Scales, when present, are finer and less silvery. A telltale eczema feature: tiny clear fluid blisters that pop with scratching.
Clue 3: Itch vs Burn vs Sting
If the itch is so intense it wakes you up at night or has you scratching until you bleed, eczema is the more likely culprit. The “sleep-stealing itch” is a well-known atopic dermatitis flag.
Psoriasis can itch, but it more often burns, stings, or feels sore. In tests booked through HealthCareOnTime, patients describing the sensation as “itchy plus burning” are usually working with psoriasis rather than eczema.
Clue 4: Age You First Noticed It
Most eczema starts in babyhood or early childhood. By age 5, the majority of children who will ever develop atopic dermatitis already have it. Adult-onset eczema does happen, but it’s less common.
Psoriasis can appear at any age but most often begins between 15 and 35, with a second smaller peak between ages 50 and 60. Adult-onset rash with no childhood history leans toward psoriasis. New-onset rash after a strep throat infection in a teen is especially suspicious for guttate psoriasis.
Clue 5: Family History Pattern
Eczema tracks closely with the atopic triad: eczema, asthma, and hay fever. Family members often have one or more of these together, and many eczema patients personally have at least one of the other two.
Psoriasis is more strongly linked to other psoriasis or psoriatic arthritis cases in the family, plus higher rates of inflammatory bowel disease and cardiovascular disease. A father or grandparent with “thick scaly elbows” is a strong family clue.
Clue 6: Nail and Joint Involvement
Nail pitting (tiny depressions in the nail surface), separated nail beds, or yellow-brown “oil drop” spots strongly suggest psoriasis. About half of psoriasis patients have nail changes at some point.
Joint pain, morning stiffness, or sausage-shaped fingers and toes (dactylitis) are major red flags for psoriatic arthritis. Eczema does not cause nail pitting or joint inflammation, which makes these features useful tiebreakers.
Clue 7: How It Reacts to Moisturizer
Eczema usually responds well to a thick, fragrance-free moisturizer applied right after a bath. Patches calm down within a day or two, especially with CeraVe, Cetaphil, Vanicream, or plain petrolatum.
Psoriasis plaques may feel softer with moisturizer, but the silvery scale and thickness rarely budge without something more targeted, like a vitamin D analog or topical steroid. Moisturizer alone never clears true plaque psoriasis.
Clue 8: Triggers That Set It Off
Eczema flares from soap residue, wool, perfume, dust mites, pet dander, sweating, stress, hot showers, and sometimes specific foods in children. Hard water in many US regions also worsens it.
Psoriasis flares from cold weather, sunburn, strep throat infections, stress, smoking, alcohol, skin injuries (the Koebner phenomenon), and certain medications including lithium, beta blockers, and antimalarials. Cases reviewed by our clinical team show that pinpointing the right trigger pattern often shortens the path to control.
Clue 9: What Skin Tone Changes the Picture
On darker skin, psoriasis can look violet, dark brown, or even gray rather than red. The silvery scale stays, but the underlying color shifts. After healing, patches often leave dark or light marks (post-inflammatory hyperpigmentation or hypopigmentation) that can persist for 6 to 12 months.
Eczema on Black, brown, or Asian skin can look ashen, gray, or hyperpigmented rather than red. Lichenified patches (thickened from chronic scratching) often appear darker than surrounding skin. This is a real reason for underdiagnosis in skin of color, and a strong argument for in-person dermatology evaluation when the visual picture is unclear.
When You Should Get Tested (Not Guess)
For most patients, the nine clues above will resolve the psoriasis vs eczema question. There’s still a meaningful category of cases where biopsy or lab work is genuinely needed.
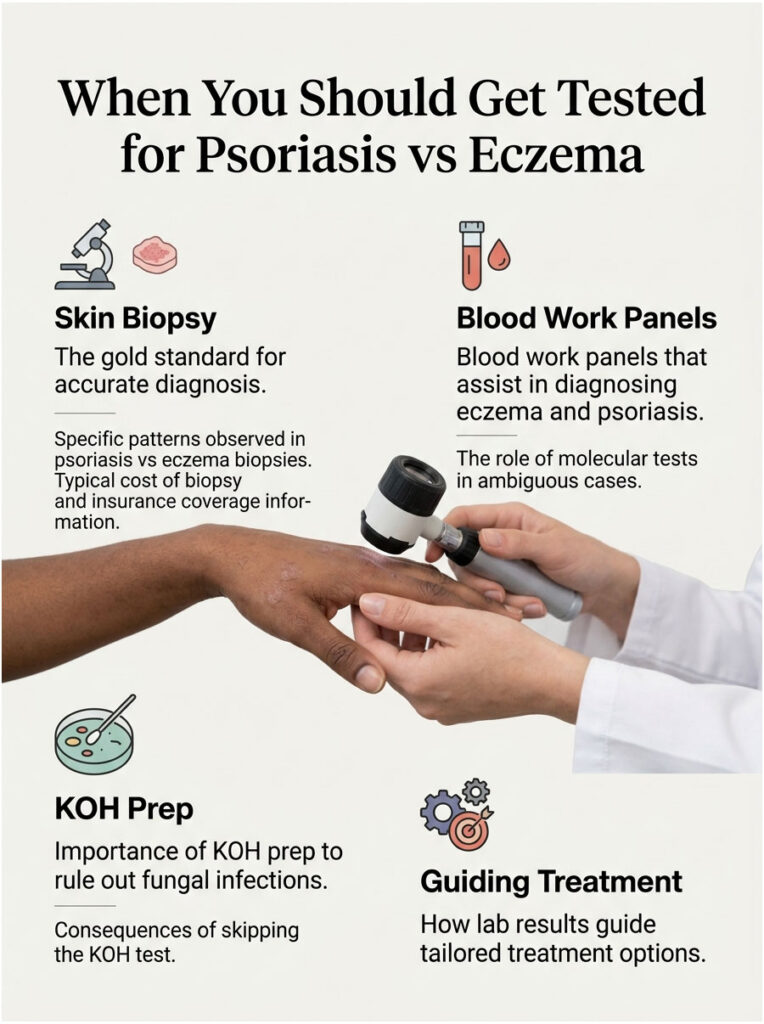
Skin Biopsy: The Gold Standard
A 4 mm punch biopsy taken from an active patch is the most reliable test. The dermatologist sends it to a pathologist who looks at the cells under a microscope.
Psoriasis biopsy shows specific patterns including parakeratosis, neutrophil collections (Munro microabscesses), and thinning of the upper skin layer above the dermal papillae. Eczema biopsy shows spongiosis (fluid between skin cells) and a different inflammatory cell mix. The US cost typically ranges from $150 to $400 in private practice, with insurance usually covering it.
Blood Work That Helps
There’s no single blood test that diagnoses either condition, but a few panels are helpful. A specific IgE blood panel can confirm atopic tendency in suspected eczema and identify environmental allergens.
For severe or unclear psoriasis, doctors may check inflammatory markers (CRP, ESR), HLA-Cw6 genetic testing in research settings, and screen for comorbidities including high cholesterol, diabetes, and fatty liver disease. Our lab partners report a steady rise in integrated panels that include vitamin D, lipid profile, and fasting glucose alongside skin condition workups.
KOH Prep and Why It’s Worth Asking About
A potassium hydroxide (KOH) skin scraping test rules out fungal infections that often mimic both psoriasis and eczema, including tinea corporis (ringworm) and tinea capitis (scalp fungus). It takes 5 minutes in the office and is inexpensive.
Skipping the KOH prep is one of the most common diagnostic shortcuts that leads to months of wrong treatment. Patients commonly ask us why their “eczema” hasn’t improved on steroid cream, and the answer is sometimes that it was never eczema at all.
What Lab Results Actually Tell You
A clear biopsy diagnosis lets your dermatologist match treatment to mechanism. Newer molecular tools, like a molecular PCR test using NOS2 and CCL27 gene expression, can distinguish psoriasis from eczema in cases where standard pathology is ambiguous.
Biopsy reports with immunohistochemistry markers are increasingly common when the clinical picture overlaps. That extra step usually pays for itself in faster treatment success.
Treatment That Actually Works
Treatment is where the cost of confusing psoriasis vs eczema hits hardest. The medications target different biology and rarely cross over fully.

Treating Psoriasis
The goal is to slow skin cell turnover and calm the immune signals driving it.
Topicals
For mild to moderate plaque psoriasis, daily topical care is the first step. Common picks include high-potency steroids (clobetasol, betamethasone), vitamin D analogs (calcipotriene as Dovonex or Vectical), topical retinoids (tazarotene as Tazorac), and combination products like Taclonex or Duobrii. Coal tar shampoo helps scalp psoriasis.
Phototherapy
Narrowband UVB light therapy, delivered in a dermatology office 2 to 3 times per week, can clear large areas of plaque psoriasis. Excimer laser targets smaller stubborn patches. US sessions typically cost $50 to $150 each, often partially covered by insurance.
Systemics
Oral methotrexate, cyclosporine, acitretin, apremilast (Otezla), and deucravacitinib (Sotyktu) are pill-based options for moderate to severe psoriasis. Otezla is generally well tolerated; Sotyktu is the newest oral TYK2 inhibitor and reaches clearer skin scores than Otezla in head-to-head studies.
Biologics for Psoriasis
For moderate to severe disease that fails topicals and systemics, biologics deliver dramatic results. The main classes are TNF inhibitors (Humira, Enbrel), IL-17 inhibitors (Cosentyx, Taltz, Bimzelx), IL-23 inhibitors (Skyrizi, Tremfya, Ilumya), and IL-12/23 inhibitors (Stelara).
Skyrizi is currently the most-prescribed first-line biologic by US dermatologists for psoriasis as of 2025, given as 4 doses per year after 2 starter doses. US list price runs about $20,000 to $25,000 per dose without insurance, though manufacturer savings programs can bring monthly out-of-pocket cost to $5 to $35 for eligible commercially insured patients.
Treating Eczema
The goal is to repair the skin barrier and calm the immune over-reaction.
Topicals
Daily thick moisturizers (CeraVe, Cetaphil, Vanicream, Aveeno, Aquaphor) are the foundation. Topical steroids (hydrocortisone OTC, triamcinolone or fluocinonide by prescription) treat flares. Calcineurin inhibitors (tacrolimus as Protopic, pimecrolimus as Elidel) are safe for face and skin folds. PDE4 inhibitors (crisaborole as Eucrisa, roflumilast as Zoryve) are non-steroid options.
Eczema Biologics
For moderate to severe atopic dermatitis, biologics have changed the picture in the last few years. The first was dupilumab (Dupixent), FDA-approved in 2017 for adults and now approved down to age 6 months. Tralokinumab (Adbry) followed. The newest is lebrikizumab (Ebglyss), approved by the FDA in September 2024 for adolescents and adults 12 and older.
These are injectable IL-4, IL-13, or IL-13 blockers. Dupixent costs about $3,500 per month without insurance; commercial copay programs bring most US patients to $0 to $25 per month with insurance.
JAK Inhibitors
Ruxolitinib (Opzelura) is a topical JAK inhibitor approved for mild to moderate eczema. Oral JAK inhibitors abrocitinib (Cibinqo) and upadacitinib (Rinvoq) are approved for moderate to severe atopic dermatitis in adults and adolescents. They work fast but carry boxed warnings, so US dermatologists monitor labs closely during treatment.
Moisturizers and Daily Skin Care
For both conditions, daily moisturizer is non-negotiable. Apply within 3 minutes of getting out of the bath or shower to lock in water.
Best US drugstore picks include CeraVe Moisturizing Cream, Vanicream Moisturizing Cream, Cetaphil Restoraderm, Aveeno Eczema Therapy, and Eucerin Advanced Repair. Avoid heavily fragranced products, alcohol-based lotions, and anything with essential oils on active patches.
OTC Costs Compared (USD Pricing)
| Product | Type | Use For | Approx US Cost | Where to Buy |
| CeraVe Moisturizing Cream (19 oz) | Ceramide moisturizer | Both, daily | $18 to $22 | CVS, Walgreens, Target |
| Vanicream Moisturizing Cream (16 oz) | Fragrance-free moisturizer | Both, sensitive skin | $14 to $18 | Walmart, Amazon |
| Cortizone 10 Hydrocortisone (1 oz) | OTC steroid | Eczema flare | $7 to $10 | All drugstores |
| Eucerin Eczema Relief (8 oz) | Colloidal oatmeal | Eczema flare | $15 to $20 | CVS, Walgreens |
| MG217 Coal Tar Cream | OTC psoriasis | Psoriasis plaques | $14 to $20 | Walmart, Amazon |
| Neutrogena T/Gel Shampoo | Coal tar shampoo | Scalp psoriasis | $8 to $12 | All drugstores |
| Sarna Sensitive Anti-Itch | Pramoxine | Itch relief, both | $10 to $14 | CVS, Walgreens |
| Aveeno Eczema Therapy Balm | Oatmeal balm | Eczema flare | $16 to $20 | Target, Walmart |
| Aquaphor Healing Ointment (14 oz) | Petrolatum | Barrier repair | $15 to $20 | All drugstores |
Reading the label matters. Adding multiple steroid products at once (a 1% hydrocortisone plus a prescription steroid) can thin the skin if used long term, especially on the face. Our clinical reviewers see this stacking pattern often in patients self-managing without dermatology guidance.
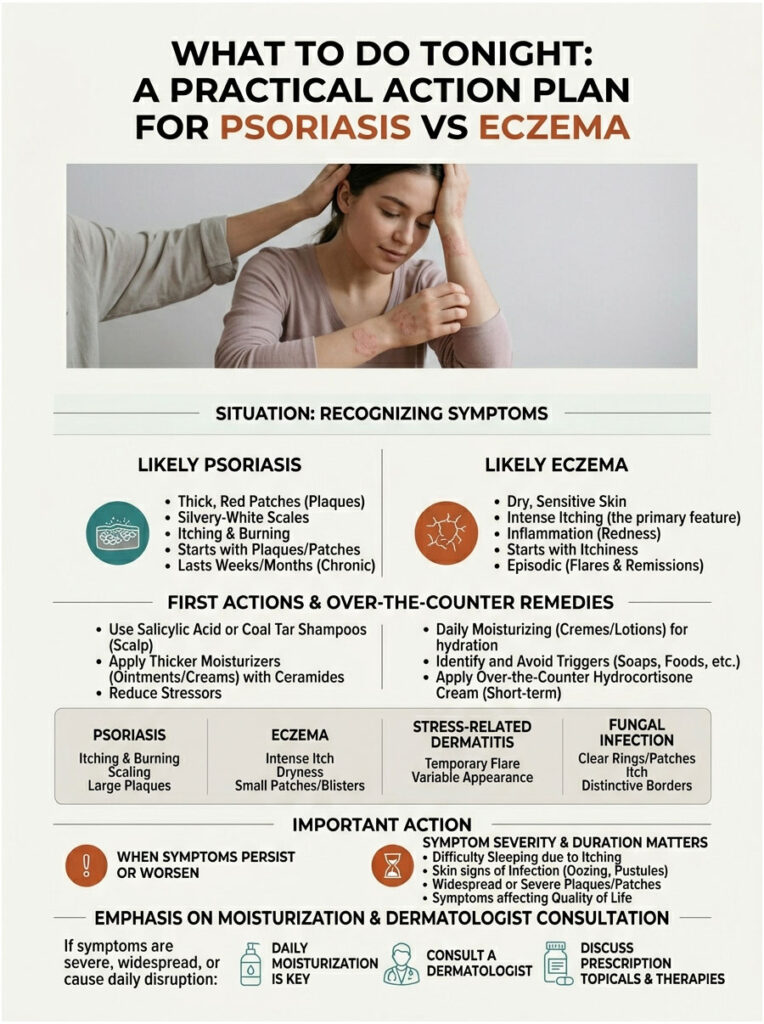
What to Do Tonight: A Practical Action Plan
The decision matrix below covers the psoriasis vs eczema situations our team gets asked about most often.
| Your Situation | Most Likely Cause | What to Do First | When to Escalate |
| Thick silvery patches on elbows, knees, or scalp | Plaque psoriasis | OTC coal tar shampoo or cream; thick moisturizer | If covers >10% of body, see dermatologist |
| Intensely itchy red patches in inner elbows or behind knees | Atopic dermatitis (eczema) | Thick fragrance-free moisturizer + OTC hydrocortisone | If oozing, infected, or sleep-disrupting |
| Dry, scaly scalp with flakes | Could be either; often seborrheic dermatitis | Try anti-dandruff shampoo (Nizoral, T/Gel) | If thick silvery scale, see dermatologist |
| Patches plus joint pain or morning stiffness | Likely psoriatic arthritis | See rheumatologist or dermatologist promptly | Any swelling of fingers or toes (dactylitis) |
| Red, itchy rash in baby or toddler | Almost certainly eczema | Thick emollient + bathing in lukewarm water | If face, eye, or genital area is heavily involved |
| Patches that won’t budge after 8+ weeks of OTC care | Either, undertreated | Book a dermatology visit; ask about biopsy | If new patches keep appearing |
| Sudden widespread small red drops after a sore throat | Guttate psoriasis | See doctor within a week | If fever or systemic symptoms |
| Cracked, painful hands from work exposure | Likely hand eczema or palmoplantar psoriasis | Heavy moisturizer + cotton gloves overnight | If unable to use hands daily |
Table 3: Decision matrix for psoriasis or eczema situations.
Special Situations
Some patient groups need a different playbook for psoriasis vs eczema.
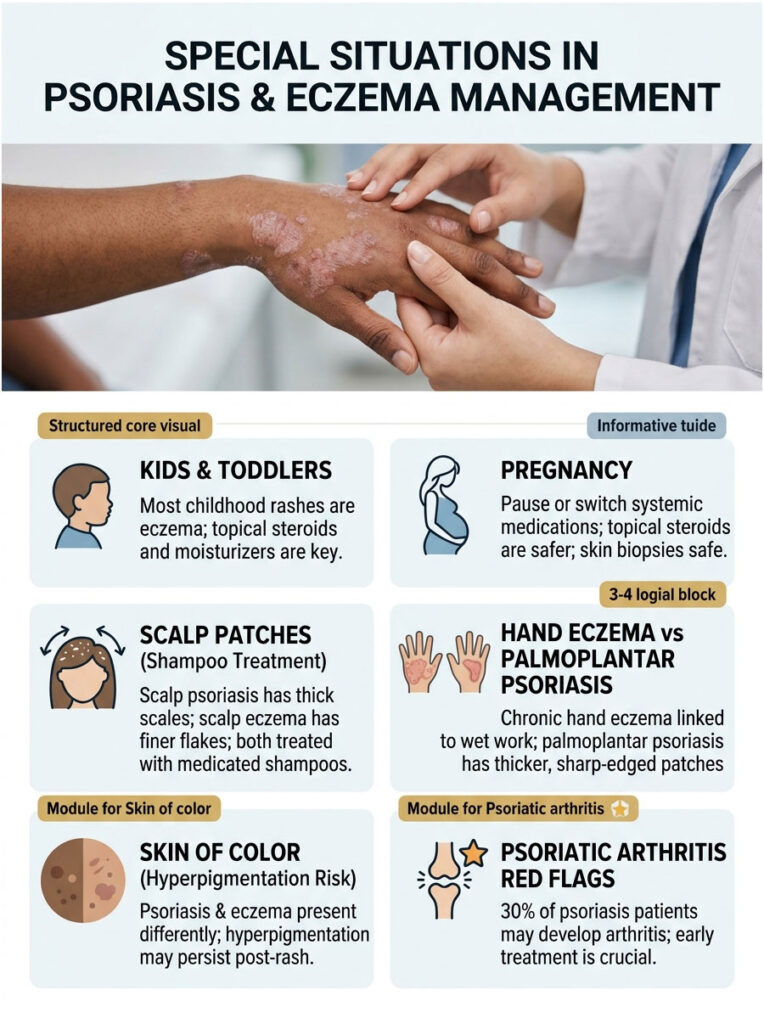
Kids and Toddlers
Most childhood rashes are eczema, not psoriasis. About 60% of children outgrow eczema by adolescence, though sensitivity often remains. Topical steroids in pediatric strengths, plus generous moisturizer, are the foundation. Severe pediatric eczema may now qualify for Dupixent starting at 6 months old.
Pediatric psoriasis is less common but real. It often shows up as guttate psoriasis after a strep infection. Treatment relies more on topicals and phototherapy than systemics, given long-term safety considerations in growing children.
Pregnancy
Many systemic and biologic medications need to be paused or switched during pregnancy. Topical steroids in low to moderate strength, calcineurin inhibitors, and moisturizers are generally considered safer choices.
Most US OB-GYNs and dermatologists co-manage these cases. Patients commonly ask whether skin biopsies are safe in pregnancy. They are, since they’re a simple local procedure with no fetal exposure risk.
Scalp Patches and Hair Concerns
Scalp psoriasis tends to extend past the hairline onto the forehead, ears, and neck, with thick silvery scales. Scalp eczema (often seborrheic dermatitis) usually stays in oily areas like the scalp, eyebrows, and sides of the nose, with finer yellow-white flakes.
Both can be managed with medicated shampoos. Ketoconazole 1% (Nizoral) helps seborrheic dermatitis. Coal tar (T/Gel) and salicylic acid (T/Sal) help psoriasis. Prescription clobetasol foam or solution is the standard for moderate scalp psoriasis.
Hand Eczema vs Palmoplantar Psoriasis
Hands are a common battleground where psoriasis vs eczema overlap most. Chronic hand eczema is usually linked to wet work, soaps, and contact allergens.
Palmoplantar psoriasis (palms and soles) tends to be thicker, sharply edged, and may include cracks deep enough to bleed. Both need a biopsy when stubborn. Our medical reviewers note that hand cases get the most frequent diagnostic switches, sometimes years into the wrong treatment.
Skin of Color: What’s Different
Psoriasis and eczema both look different on Black, brown, and Asian skin. Patches may appear violet, dark brown, or gray instead of pink or red, and post-inflammatory hyperpigmentation can linger for months after the rash clears.
The American Academy of Dermatology has expanded its image libraries to address historic underrepresentation. If your dermatologist relies only on classic “red, scaly” descriptions, it’s worth asking whether they’re factoring in your skin tone.
When Joints Hurt (Psoriatic Arthritis Red Flags)
About 30% of psoriasis patients develop psoriatic arthritis at some point, often years after skin symptoms start. Red flags include:
- Morning joint stiffness lasting more than 30 minutes
- A swollen finger or toe that looks like a sausage (dactylitis)
- Heel pain or Achilles tendon pain (enthesitis)
- Lower back pain that improves with movement
- Eye redness or pain (uveitis)
Treating psoriatic arthritis early protects joints from permanent damage, which is why catching psoriasis symptoms early matters even more.
When to See a Doctor
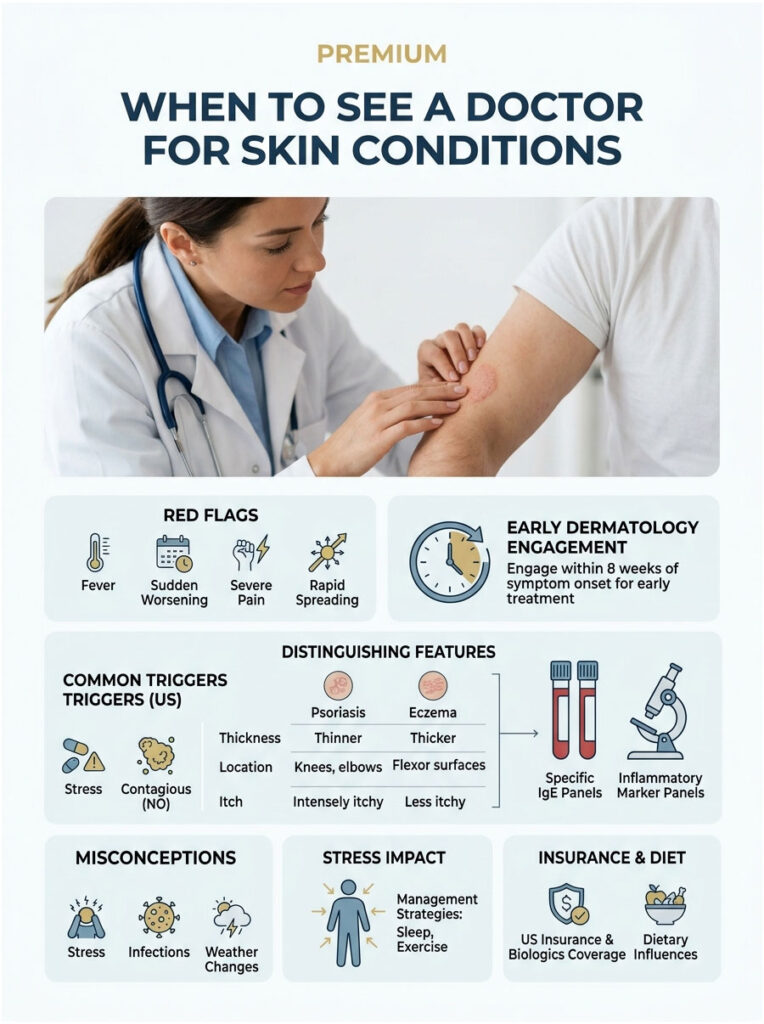
Red flags that mean it’s time to be evaluated in person:
- Rash covering more than 10% of your body
- Rash that won’t improve after 4 to 8 weeks of OTC treatment
- Patches that look infected (yellow crust, fever, spreading redness)
- Joint pain or swelling along with skin symptoms
- Rash that wakes you up at night for multiple weeks
- Severe scalp involvement causing hair loss
- New widespread eruption after a sore throat (possible guttate psoriasis)
- Rash on the face or genital area that doesn’t respond to gentle care
A telehealth visit can often start the workup, but biopsy and severe-disease treatment require in-person dermatology. Cases reviewed by our clinical team show that early dermatology engagement, often within 8 weeks of symptom onset, leads to faster and cheaper resolution.
For US patients trying to settle the psoriasis vs eczema question with hard data, specific IgE blood panels can confirm atopic tendency, while inflammatory marker panels (CRP, ESR, vitamin D, fasting glucose, lipid profile) help screen for the metabolic and cardiovascular comorbidities that often travel with psoriasis.
Frequently Asked Questions
What’s the easiest way to tell psoriasis from eczema?
Look at three things: thickness, location, and itch. Psoriasis plaques tend to be thick, well-defined, and silvery, often on elbows, knees, scalp, and lower back, with burning more than itching. Eczema patches are typically thinner, redder, intensely itchy, and prefer inner elbows, behind knees, hands, and face. Childhood onset leans eczema; teen or adult onset leans psoriasis.
Can a dermatologist diagnose by sight alone?
Often yes, especially with classic plaque psoriasis or longstanding atopic dermatitis. Experienced dermatologists correctly identify the condition in the office about 80 to 85% of the time. For ambiguous cases, doctors order a 4 mm punch biopsy, sometimes with immunohistochemistry, to confirm. Newer molecular tests now help in cases where standard pathology is unclear. Our medical reviewers recommend biopsy whenever treatment for 6 to 8 weeks hasn’t worked.
Is psoriasis an autoimmune disease?
Yes. Psoriasis is widely classified as an immune-mediated, autoimmune-related disease. The immune system, especially T-cells and the IL-17 and IL-23 signaling pathways, mistakenly drives skin cells to grow far too fast. This is why biologics targeting these specific pathways (Skyrizi, Cosentyx, Tremfya, Taltz) work so well. Some researchers prefer the term “autoinflammatory” because antibody involvement is less prominent than in classic autoimmune diseases like lupus.
Can you have both psoriasis and eczema?
Yes, although it’s uncommon. Studies suggest only a small percentage of people carry both diagnoses simultaneously, but it does happen, and the two conditions can flare independently. About 1 in 5 adult eczema patients have more than one eczema type, which adds another layer of complexity. If you suspect overlap, ask your dermatologist about biopsy and possibly molecular testing to distinguish patches.
Is psoriasis or eczema contagious?
Neither is contagious. You cannot catch psoriasis or eczema from another person, even through direct skin contact, sharing towels, or swimming pools. Both are driven by your own immune system and genetics, not by bacteria or viruses you can pass on. This is one of the most common myths our patient education team has to correct. Public misunderstanding still drives social stigma, which adds emotional weight to an already difficult condition.
What triggers a psoriasis flare in the US?
Common US triggers include cold dry winter weather (especially in the Northeast and Midwest), stress, smoking, alcohol, strep throat infections, sunburn, skin injuries (the Koebner phenomenon), and certain medications including lithium, beta blockers, and antimalarials. Stopping smoking and moderating alcohol intake produce measurable improvement in many patients. A trigger diary kept for 4 to 6 weeks often reveals patterns that change treatment decisions.
Does stress make eczema worse?
Yes, and the evidence is consistent. Stress raises cortisol and shifts the immune balance, which weakens the skin barrier and increases itch perception. Most eczema patients can name specific stressors that precede flares, including work deadlines, sleep loss, and family conflict. Cognitive behavioral therapy, mindfulness, and structured sleep routines reduce flare frequency in clinical studies. Treatments work better when stress management runs alongside topical or systemic care.
What is the strongest OTC cream for psoriasis?
The strongest OTC topical specifically for psoriasis is coal tar (in MG217, T/Gel shampoo, or generic versions). Salicylic acid 3% products help remove scale. OTC hydrocortisone 1% is the strongest steroid available without a prescription and is too mild for thick plaques. Stronger topical steroids (clobetasol, betamethasone) and prescription vitamin D analogs (calcipotriene) require a doctor visit and deliver much better results.
Can children outgrow psoriasis like they outgrow eczema?
Childhood psoriasis is less likely to resolve completely. About 60% of children with eczema see significant improvement by adolescence, and many appear to outgrow it (though sensitive skin often remains). Psoriasis tends to be lifelong, though severity can wax and wane dramatically over decades. Long remissions of years are possible, particularly with successful biologic treatment. Genetic factors and early flare patterns help predict the long-term course.
Are biologics covered by US insurance?
Most commercial US insurance plans, Medicare Part D, and many Medicaid programs cover biologics for moderate to severe psoriasis or eczema after step therapy. Patients typically need to fail one or two cheaper treatments first. Manufacturer copay programs can bring monthly out-of-pocket costs to $5 to $35 for commercially insured patients on Skyrizi, Cosentyx, Dupixent, and Ebglyss. Patient assistance programs offer free medication for uninsured patients meeting income criteria.
Does diet affect psoriasis or eczema?
Diet plays a meaningful role in psoriasis, especially in the form of weight management (obesity worsens psoriasis severity and biologic response), reduced alcohol intake, and an anti-inflammatory eating pattern (Mediterranean-style). For eczema, food allergens (cow’s milk, eggs, peanuts, soy, wheat) can trigger flares in some children, though this is less common in adults. Elimination diets should be done under medical supervision to avoid nutritional gaps.
What does psoriasis look like on Black skin?
Psoriasis on Black skin often appears violet, dark brown, or grayish rather than pink or red, but retains the same silvery or whitish scale on top. Patches commonly leave hyperpigmented or hypopigmented marks after they heal, sometimes for 6 to 12 months. Diagnosis can be delayed because clinical descriptions in older textbooks focused on light skin. The American Academy of Dermatology and major dermatology programs now teach skin-of-color recognition explicitly.
| Disclaimer: This article is general health education and is not medical advice. Skin symptoms can look alike across many conditions, and only a licensed US dermatologist can confirm a diagnosis of psoriasis or eczema. If you have a rash that is rapidly spreading, infected, painful, accompanied by fever, or affecting more than 10% of your body, contact a healthcare provider promptly. If you have signs of a severe allergic reaction (swelling of lips, tongue, or throat, or trouble breathing), call 911 or go to your nearest emergency room. |
References
- National Institute of Allergy and Infectious Diseases (NIAID). Eczema (Atopic Dermatitis).
- Rabin J, et al. Psoriasis prevalence among adults in the United States. JAAD.
- Mahmoud O, et al. Prevalence of atopic dermatitis in the United States from 2021 to 2024: NHIS data. JAAD, 2026.
- National Eczema Association. Multi-type eczema research letter (JID, 2025).
- Rush University Medical Center. Eczema or Psoriasis: How to Tell Which One You May Have.
- Medical News Today. Psoriasis vs. eczema: Symptoms, causes, and treatment.
- WebMD. Psoriasis or Eczema: How to Tell the Difference.
- American Academy of Dermatology Association (AAD).
- National Psoriasis Foundation. Current Biologics on the Market.
- GoodRx. Skyrizi vs Stelara for Psoriasis.
- Eczema Prevalence in the United States: Data from the 2003 NSCH.





