
Somewhere in the United States, a person has a heart attack about every 40 seconds, and many never saw it coming. Behind a large share of those events sits a single emergency: acute coronary syndrome.
Knowing what it is, how it shows up, and what to do in the first minutes can change how the story ends.
Table of Contents
Quick Answer: Acute coronary syndrome (ACS) is an umbrella term for a sudden, serious drop in blood flow to the heart muscle. It covers three conditions: unstable angina, NSTEMI, and STEMI. ACS is a medical emergency. If you or someone near you has sudden chest pain or pressure, especially with shortness of breath, sweating, or pain spreading to the arm or jaw, call 911 right away. Every minute matters.
At a Glance
- ACS is a group of emergencies, not a single disease, caused by suddenly blocked blood flow to the heart.
- The three types are unstable angina, NSTEMI, and STEMI, in rising order of severity.
- A heart attack (NSTEMI or STEMI) involves heart muscle death; unstable angina is a warning that often comes first.
- Classic signs are chest pressure and pain spreading to the arm, jaw, neck, or back, with shortness of breath, sweating, or nausea.
- Women, older adults, and people with diabetes often have quieter, atypical symptoms.
- Treatment is time-sensitive: opening the blocked artery fast saves heart muscle and lives.
- When in doubt, call 911. Don’t drive yourself, and don’t wait to see if it passes.
What Acute Coronary Syndrome Actually Is
ACS is not one illness. It’s the label doctors use for a sudden, dangerous reduction in blood flow to the heart muscle. The American Heart Association describes it as an umbrella term that covers heart attack and unstable angina.
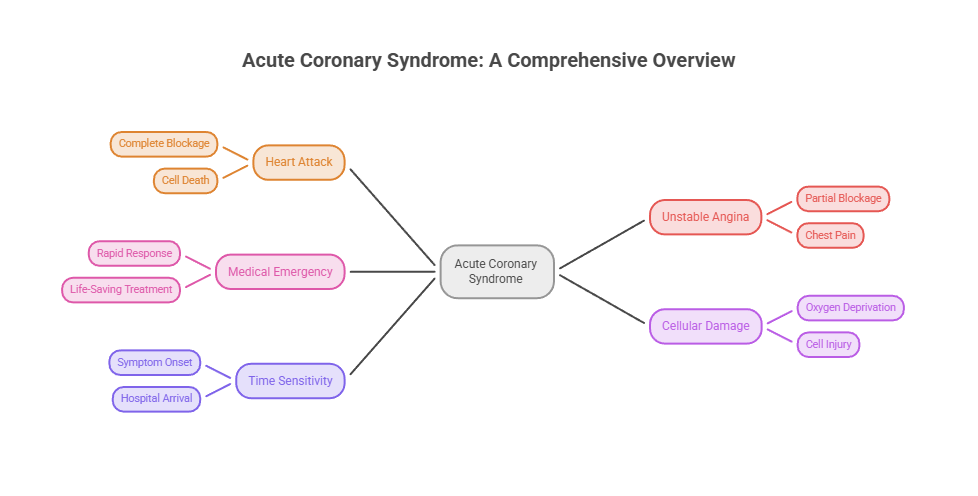
When blood can’t reach part of the heart, that muscle starts to suffer within minutes. Starved of oxygen, the cells become injured, and if the blockage holds, they begin to die.
That’s why ACS is treated as an emergency from the very first symptom. Our medical reviewers stress that the clock starts the moment blood flow drops, not when you finally reach the hospital.
The Plaque-and-Clot Mechanism
Most ACS begins with atherosclerosis, a slow buildup of fatty plaque inside the coronary arteries. Plaque is made of cholesterol, fat, and other cells layered along the artery wall.
Trouble hits when a plaque ruptures. A blood clot forms over the tear, and that clot can quickly narrow or fully block the artery feeding the heart.
Less often, a spasm in a coronary artery squeezes off blood flow on its own. Either way, the heart muscle downstream pays the price almost immediately.
ACS vs Heart Attack vs Angina
These terms overlap, which is where the confusion creeps in. ACS is the big umbrella. A heart attack, known medically as a myocardial infarction, is one possible outcome under that umbrella.
Angina is chest pain caused by reduced blood flow. Stable angina is predictable, shows up with exertion, and eases with rest. Unstable angina is the dangerous kind that strikes at rest or worsens quickly.
Patients who book cardiac risk tests with HealthCareOnTime often ask whether a chest twinge is “just angina.” The honest answer is that new, changing, or at-rest chest pain needs urgent evaluation, not a guess.
The 3 Types of Acute Coronary Syndrome
Doctors sort ACS into three types based on how blocked the artery is, whether heart muscle is dying, and what the tests reveal. Those differences decide how fast and how aggressively treatment happens.
The table below lines them up side by side.
| Feature | Unstable Angina | NSTEMI | STEMI |
| Artery blockage | Partial, temporary | Partial or severe | Complete |
| Heart muscle damage | None yet | Yes, some | Yes, often extensive |
| ECG finding | Normal or ST depression / T-wave changes | ST depression or T-wave changes, no ST elevation | ST-segment elevation |
| Troponin (blood marker) | Normal | Elevated | Elevated |
| Severity | Warning sign | Serious | Most severe |
| Treatment urgency | Urgent evaluation | Urgent, often angiography | Emergency, fastest possible |
Unstable Angina
Unstable angina is the least severe of the three, but it’s a loud warning. Blood flow is reduced enough to cause symptoms, often at rest, yet not long enough to kill heart muscle.
Because there’s no significant muscle damage, the blood marker troponin usually stays normal. That single feature is what separates it from a heart attack.
It can escalate fast, though. Cleveland Clinic notes that unstable angina can quickly turn into a heart attack, which is why it’s never something to ride out at home.
NSTEMI (Non-ST-Elevation Myocardial Infarction)
An NSTEMI is a heart attack. A partial blockage cuts blood flow enough to damage heart muscle, so troponin rises in the blood and confirms the injury.
On the EKG, an NSTEMI does not show the telltale ST-segment elevation of the most severe type. It may show ST depression, T-wave changes, or look subtle to an untrained eye.
NSTEMI still demands hospital care and, often, a procedure to open the artery. It’s serious, even when the EKG looks less dramatic than a STEMI.
STEMI (ST-Elevation Myocardial Infarction)
A STEMI is the most severe form of ACS. A coronary artery is completely blocked, the heart muscle starts to die, and a person could die without quick treatment.
The EKG shows clear ST-segment elevation, which tells the medical team to act immediately. Troponin is elevated as well, reflecting the damage underway.
A STEMI is a race against the clock. Reopening the artery within a tight window is what protects the heart and saves the person’s life.
Warning Signs and Symptoms
ACS symptoms can appear suddenly, sometimes at rest, and they don’t always look like the movies. Recognizing them early is the part that matters most.
Across the readers we serve, the most common mistake is assuming a heart problem always means dramatic, crushing chest pain. It often doesn’t.
Classic Symptoms
The hallmark is chest discomfort: pressure, tightness, squeezing, burning, or aching, usually in the center or left side of the chest. It may come and go or settle in and stay.
Pain often spreads to the left arm, shoulder, neck, jaw, or back. Other signs include shortness of breath, a cold sweat, nausea, lightheadedness, and a sense that something is badly wrong.
Cleveland Clinic advises always seeking care for sudden chest pain rather than guessing the cause, because if it turns out to be ACS, every minute counts.
Symptoms in Women and Other Atypical Presentations
Women, older adults, and people with diabetes are more likely to have quieter symptoms. The classic chest-clutch may be mild, brief, or absent altogether.
Instead, the warning may be unusual fatigue, shortness of breath, nausea, indigestion-like discomfort, or pain in the jaw, neck, or back. These are easy to brush off, and that’s exactly the danger.
Our medical reviewers stress that “atypical” does not mean “less serious.” A woman with sudden fatigue, nausea, and jaw pain deserves the same urgent 911 response as anyone with crushing chest pain.
Silent and Gray-Zone Symptoms
Some heart attacks cause so few symptoms that people miss them entirely. About 1 in 5 heart attacks are silent, often discovered later on a routine test.
When symptoms are vague, lean toward caution. It’s far better to be checked and cleared than to sit at home through a true emergency.
Is It a Heart Attack, Heartburn, or a Panic Attack?
Chest discomfort doesn’t always mean ACS. Heartburn can burn behind the breastbone, and a panic attack can bring chest tightness, a racing heart, and shortness of breath that feel frighteningly similar.
The catch is that you often can’t tell them apart in the moment, and neither can many doctors without tests. If chest pain is new, severe, lasts more than a few minutes, or comes with sweating, nausea, or pain spreading to the arm or jaw, treat it as a possible heart attack and call 911.
What Causes ACS and Who’s at Risk
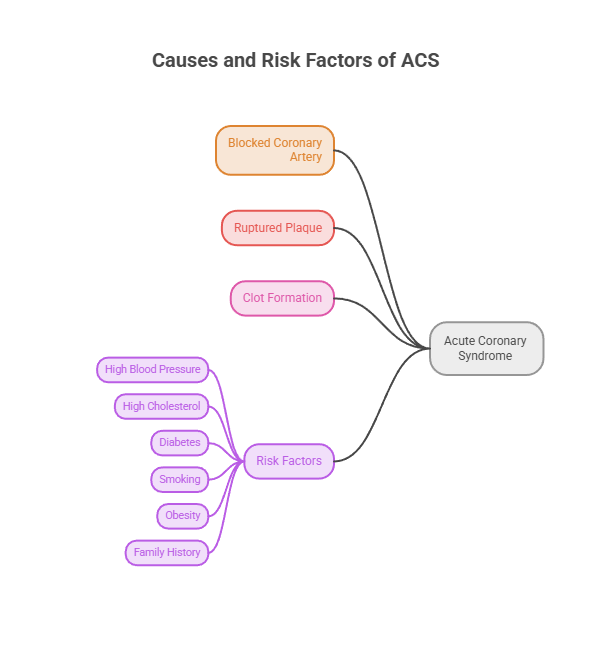
At its core, ACS comes from a blocked coronary artery, almost always from a ruptured plaque and the clot that forms over it. Understanding the risk factors helps you lower the odds.
Root Causes
The usual sequence is plaque buildup, then a sudden rupture, then a clot that chokes off blood flow. Coronary artery spasm is a less common trigger.
Anything that damages artery walls or thickens the blood over time raises the risk of that chain reaction firing. That includes years of high blood pressure, high cholesterol, and the inflammation that comes with smoking or diabetes.
Risk Factors
The big modifiable risk factors are high blood pressure, high LDL cholesterol, smoking, diabetes, obesity, an unhealthy diet, and physical inactivity. Chronic stress and poor sleep add to the load.
Non-modifiable factors include older age, a family history of early heart disease, and being male, though a woman’s risk climbs after menopause.
Coronary artery disease, the problem behind most ACS, is common. About 1 in 20 adults age 20 and older in the US have it, and many don’t know until symptoms strike.
How Doctors Diagnose ACS
Diagnosis moves fast and usually combines a few tools. The goal is to confirm ACS, sort out which type it is, and start treatment without delay.
Our lab partners note that the same markers checked in emergencies, like troponin and a lipid profile, also appear in routine cardiac risk screening, which is why prevention and diagnosis share a toolkit.
EKG/ECG
An electrocardiogram records the heart’s electrical activity in seconds. It’s the fastest way to spot a STEMI and to flag other dangerous patterns.
Because timing is everything, an EKG is often the first test done, and paramedics may run one in the ambulance on the way in. The result helps the hospital prepare before you even arrive.
Cardiac Troponin and Blood Tests
Troponin is a protein released when heart muscle is damaged. A rise in troponin separates a heart attack, whether NSTEMI or STEMI, from unstable angina.
Doctors usually draw blood more than once over a few hours to watch the trend, since troponin levels change as an event unfolds. A single normal result early on isn’t always the full picture.
Imaging and Angiography
An echocardiogram uses ultrasound to show how well the heart pumps and whether one section is struggling. A CT angiogram can map the coronary arteries without surgery.
A coronary angiogram, where dye and X-ray reveal blockages directly, is often the definitive look. It can lead straight into treatment in the same session, since the cardiologist can open a blockage on the spot.
What Happens at the Hospital
Walking into an emergency room with chest pain triggers a fast, well-rehearsed routine. Knowing the steps can take some of the fear out of the moment.
Staff move quickly because protocols are built around speed. The faster a blocked artery is found and opened, the more heart muscle survives.
The First Few Minutes
Expect an EKG almost immediately, often within minutes of arrival, plus blood drawn for troponin. A nurse will place an IV and attach monitors to track your heart rhythm.
You’ll be asked about your symptoms, your medical history, and any medications. Honest, quick answers help the team rule conditions in or out without losing time.
Moving to Treatment
If the team confirms a STEMI, you may go straight to the cardiac catheterization lab to reopen the artery. For an NSTEMI or unstable angina, doctors weigh your risk to decide how soon to do an angiogram.
Throughout, the staff explains each step as they go. Patients commonly ask us how long this takes, and the answer is that the highest-risk cases are handled fastest, sometimes within an hour of arrival.
Treatment and What to Expect
ACS treatment has two jobs: restore blood flow quickly and protect the heart from further harm. What happens depends on the type and severity.
The phrase cardiologists use is “time is muscle.” Every minute an artery stays blocked, more heart muscle is lost, so speed shapes the entire plan.
Immediate Emergency Treatment
Early steps often include aspirin to slow clotting, nitroglycerin to ease chest pain, and oxygen if blood levels are low. Treatment usually starts the moment ACS is suspected.
From there, doctors add stronger medicines, including a second antiplatelet drug, a blood thinner like heparin, and often a beta-blocker and a statin, tailored to the person.
Restoring Blood Flow
For a STEMI, reopening the blocked artery fast is the priority. The usual route is angioplasty, where a tiny balloon opens the artery and a stent holds it open.
If angioplasty isn’t available quickly, clot-dissolving drugs called thrombolytics may be used instead. For certain complex blockages, bypass surgery (CABG) is the better fix.
NSTEMI and unstable angina are risk-stratified first. Many people still go to angiography and stenting, though the timing may be less immediate than for a STEMI.
Ongoing Medications and Cardiac Rehab
After the emergency passes, most people stay on a mix of medications: dual antiplatelet therapy, a statin, a beta-blocker, and often an ACE inhibitor. Together they cut the risk of another event.
Cardiac rehab, a supervised program of exercise, education, and support, is one of the most effective steps for recovery. Patients commonly ask us how to “get back to normal,” and rehab is usually a big part of that answer.
Possible Complications
ACS can strain the heart in ways that show up during the event or in the weeks after. Knowing them helps you spot trouble early and ask the right questions.
Most complications are more likely when treatment is delayed, which is one more reason speed matters so much.
Short-Term Risks
During or soon after a heart attack, the heart can develop dangerous rhythm problems called arrhythmias. Severe damage can weaken the heart’s pumping enough to cause heart failure or, rarely, cardiogenic shock.
These risks are exactly why people are monitored closely in the hospital. Continuous heart-rhythm tracking lets the team act the instant something shifts.
Longer-Term Effects
After significant muscle damage, some people develop ongoing heart failure, where the heart pumps less efficiently than before. Others face a higher risk of a future event.
The encouraging part is that medications, cardiac rehab, and risk-factor control meaningfully lower these odds. Recovery is rarely passive; the steps you take afterward shape the outcome.
Recovery and Life After ACS
Surviving ACS is the beginning of a new chapter, not just the end of an emergency. Most people can rebuild a full, active life with the right plan.
Across patients we serve, the ones who recover best tend to treat aftercare as seriously as the emergency itself. The habits built in the first months tend to stick.
The First Weeks Home
Early on, expect to take several medications on a strict schedule and to ease back into activity gradually. Your care team will set limits on lifting, driving, and returning to work based on your case.
Watch for warning signs like returning chest pain, new shortness of breath, or swelling, and report them promptly. When in doubt about chest pain, treat it as an emergency again.
Building a Heart-Strong Routine
Cardiac rehab, a heart-healthy diet, regular movement, and quitting smoking form the backbone of long-term recovery. Managing stress and sleep matters more than many people expect.
Follow-up visits and repeat lab work keep the plan on track. Patients who stay engaged with monitoring often catch small problems before they grow, which is the whole point of consistent aftercare.
Support matters too. Leaning on family, a cardiac-rehab group, or a counselor helps many people stick with the changes, especially in the first hard months after an event.
When to Call 911 (Don’t Wait)
This is the section to remember. If ACS is even possible, calling 911 is the safest move, every single time.
Don’t drive yourself to the hospital, and don’t ask someone to drive you when an ambulance is available. Paramedics can start treatment and monitoring on the way.
Symptoms That Mean Call Now
Call 911 for sudden chest pain or pressure, especially with pain spreading to the arm, jaw, neck, or back, shortness of breath, a cold sweat, nausea, or feeling faint.
If a 911 dispatcher advises chewing an aspirin and it’s safe for you, do it. Then stay still and wait for help to arrive.
Why Waiting Is Dangerous
People often wait, hoping the symptoms pass or worrying about a false alarm. That delay is exactly what leads to preventable heart damage and death.
Treatment works best in the first minutes and hours. Getting evaluated early, even if it turns out to be nothing, is always the right call.
Studies of heart attack care consistently show better survival when the blocked artery is opened sooner. That single fact is why emergency teams move so fast, and why your speed at home matters just as much.
| Your Situation | What It Might Mean | What To Do |
| Sudden chest pressure or pain spreading to the arm or jaw | Possible heart attack (ACS) | Call 911 now; don’t drive yourself |
| Chest pain that comes with exertion and eases with rest | Possibly stable angina | See a doctor promptly; get it evaluated, don’t ignore it |
| New, worsening, or at-rest chest pain if you have heart disease | Possible unstable angina or heart attack | Call 911 now |
| Unusual fatigue, nausea, or jaw or back pain, especially in women | Possible atypical ACS | Call 911 now; treat it as serious |
| Chest pain returning after a recent stent or procedure | Possible re-blockage | Call 911 or seek urgent care immediately |
| Symptoms ease but you’re unsure | Could still be ACS | Call 911 or get checked; don’t wait it out |
Lowering Your Risk
Most risk factors for ACS are within your influence. Small, steady changes add up to a meaningfully lower risk over the years.
Heart-Healthy Habits
The American Heart Association sums up heart health in eight habits it calls Life’s Essential 8: not smoking, staying active, eating well, keeping a healthy weight, sleeping well, and managing cholesterol, blood pressure, and blood sugar.
None of these require perfection. Quitting smoking, walking most days, and cooking more meals at home each move the needle on their own.
Managing the Numbers That Matter
Three numbers deserve regular attention: blood pressure, cholesterol, and blood sugar. Each one, left unchecked, quietly damages arteries over time.
Patients who book routine panels with HealthCareOnTime often catch a rising cholesterol or blood sugar early, while it’s still easy to act on. Knowing your numbers is a simple, powerful habit.
Questions to Ask Your Doctor
A short list of questions turns a checkup into a plan. Consider asking about your blood pressure, cholesterol, and blood sugar numbers, your personal heart-attack risk, and whether a statin or daily aspirin makes sense for you.
It’s also worth asking which symptoms should send you to the ER given your history, and which single lifestyle change would help you most. People who come in with questions tend to leave with clearer next steps.
By the Numbers: ACS and Heart Disease in the US
The scale of heart disease in America is sobering, and it explains why ACS is treated with such urgency. The figures below come from the CDC and the American Heart Association.
| Metric | Figure | Source |
| How often a heart attack occurs in the US | About every 40 seconds | CDC |
| Heart attacks per year in the US | About 805,000 | CDC |
| First-time vs recurrent heart attacks | 605,000 first, 200,000 recurrent | CDC |
| Heart attacks that are “silent” | About 1 in 5 | CDC |
| US adults age 20+ with coronary artery disease | About 1 in 20 (5%) | CDC |
| How often someone dies of cardiovascular disease in the US | About every 34 seconds | CDC / AHA |
Two numbers stand out. A heart attack hits someone in the US about every 40 seconds, and about 805,000 Americans have one each year. Heart disease also remains the nation’s leading cause of death.
These statistics aren’t meant to scare you. They’re a reminder that knowing the signs, and acting fast, genuinely saves lives.
Frequently Asked Questions
Is acute coronary syndrome the same as a heart attack?
Not exactly. ACS is an umbrella term for a sudden drop in blood flow to the heart. A heart attack (NSTEMI or STEMI) is one type of ACS. Unstable angina is another, where flow drops but heart muscle isn’t yet dying. All are emergencies needing immediate care.
What are the three types of acute coronary syndrome?
The three types are unstable angina, NSTEMI (non-ST-elevation heart attack), and STEMI (ST-elevation heart attack). They differ by how blocked the artery is, whether heart muscle is dying, and what the EKG and troponin test show. STEMI is the most severe and needs the fastest treatment.
What are the first warning signs of ACS?
The earliest sign is often chest pressure, tightness, or pain, sometimes spreading to the arm, jaw, neck, or back. Shortness of breath, a cold sweat, nausea, and lightheadedness can come with it. Symptoms may begin at rest. Any sudden, unexplained chest discomfort deserves a 911 call.
What’s the difference between STEMI and NSTEMI?
Both are heart attacks. A STEMI involves a complete artery blockage and shows ST-segment elevation on the EKG, putting a large area of heart muscle at risk. An NSTEMI is usually a partial blockage without that pattern. Both raise troponin and both need urgent hospital treatment.
Can acute coronary syndrome be cured?
ACS can be treated effectively, especially when caught early, but the underlying coronary artery disease is managed rather than cured. Opening the blocked artery, taking prescribed medications, and improving risk factors can restore function and sharply lower the chance of another event. Cardiac rehab supports long-term recovery.
How serious is acute coronary syndrome?
Very serious. ACS is a medical emergency that can damage the heart or be fatal without fast treatment. Outcomes are far better when blood flow is restored quickly, which is why calling 911 at the first sign matters so much. Delays cause preventable harm.
What causes acute coronary syndrome?
Most ACS starts with plaque buildup in a coronary artery. When a plaque ruptures, a blood clot forms and suddenly blocks blood flow to the heart. Less often, a coronary artery spasm is the trigger. Risk factors like high blood pressure, high cholesterol, smoking, and diabetes raise the odds.
How is ACS different from stable angina?
Stable angina is predictable chest pain that appears with exertion and eases with rest, reflecting a fixed narrowing. ACS is sudden and dangerous, often striking at rest, and signals a new or worsening blockage. Unstable angina, which is part of ACS, is a key warning that needs urgent evaluation.
Do women have different ACS symptoms?
Often, yes. Women are more likely to have atypical symptoms like unusual fatigue, shortness of breath, nausea, or pain in the jaw, neck, or back, sometimes without prominent chest pain. These signs are easy to dismiss but just as serious, and they warrant an immediate 911 call.
How is acute coronary syndrome diagnosed?
Doctors use an EKG to check the heart’s electrical activity, blood tests for troponin to detect muscle damage, and a physical exam and history. Imaging like an echocardiogram or a coronary angiogram can confirm and locate blockages. Diagnosis happens fast so treatment can start right away.
Can you have ACS with normal troponin?
Yes. Unstable angina is ACS with normal troponin, because blood flow is reduced but the heart muscle hasn’t been damaged yet. It’s still an emergency, since unstable angina can progress to a heart attack quickly. Doctors often repeat troponin over hours to confirm the trend is truly normal.
What should you do if you think you’re having ACS?
Call 911 immediately. Don’t drive yourself or wait to see if symptoms pass. If a dispatcher advises it and aspirin is safe for you, chew one. Then rest and wait for paramedics, who can begin treatment on the way. Acting in the first minutes saves heart muscle.
Disclaimer: This article is for general education and isn’t a substitute for professional medical care. Acute coronary syndrome is a medical emergency. If you think you or someone else may be having ACS or a heart attack, call 911 immediately. Always follow the guidance of qualified healthcare providers for diagnosis and treatment.
References
- Acute Coronary Syndrome, American Heart Association
- Heart Disease Facts, Centers for Disease Control and Prevention (CDC)
- Heart Disease Remains Leading Cause of Death (2025 Heart Disease and Stroke Statistics), American Heart Association
- Acute Coronary Syndrome (ACS): Symptoms & Treatment, Cleveland Clinic
- Acute Coronary Syndrome, MedlinePlus (NIH)
- Overview of Acute Coronary Syndromes (ACS), Merck Manual





