Patients walk into my urology clinic clutching their lower backs in pure agony. They’re sweating, restless, and completely thrown off by what’s happening to their body. Along with the back pain, their stomach is in revolt. And almost every single one of them looks at me with the same desperate question: can kidney stones cause diarrhea?
The short answer is yes, they absolutely can.
Table of Contents
As a board-certified urologist with over 15 years of clinical experience, I see this confusing combination of symptoms nearly every week. Most people connect kidney stones with sharp back pain or blood in the urine. They never expect their digestive system to completely fall apart during a urological emergency.
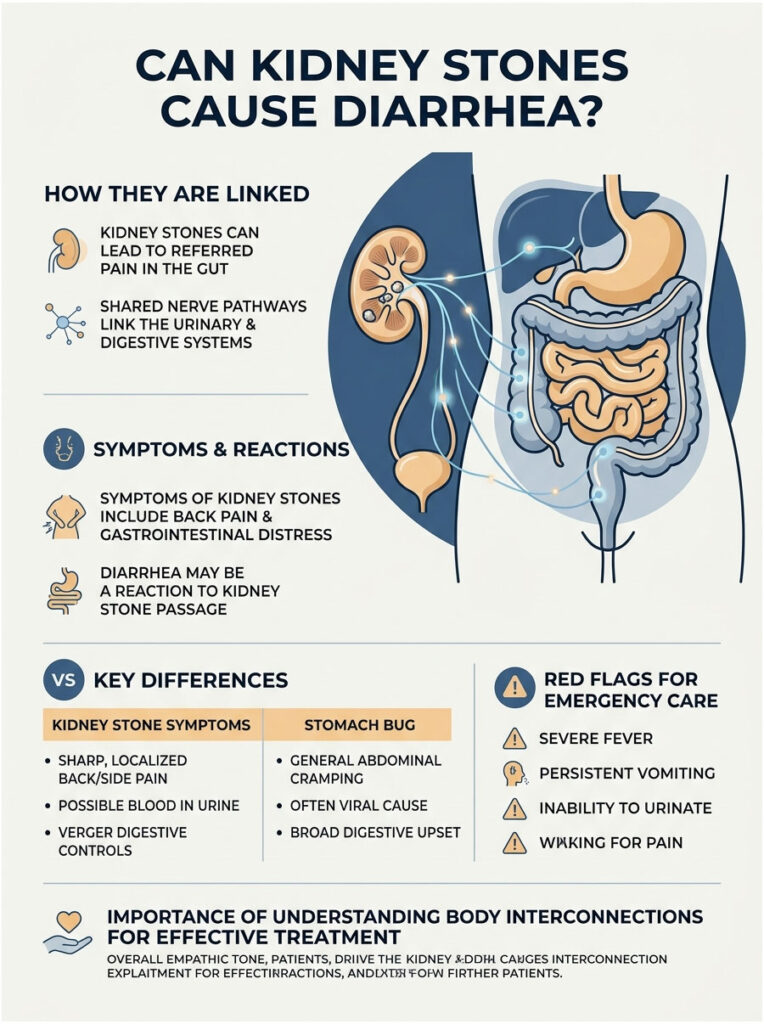
But the human body is deeply interconnected. Your urinary tract and your gut share nerve pathways and chemical signals, which means a problem in your kidneys can quickly spill over into your intestines. Your bowels can react violently to something happening entirely inside your kidney.
In this guide, I’ll walk you through the exact biology behind this referred pain. We’ll cover how to tell the difference between a passing stone and a stomach bug, look at how chronic diarrhea can actually cause kidney stones, and finish with the red flags that mean you need emergency care right now.
Quick Answer
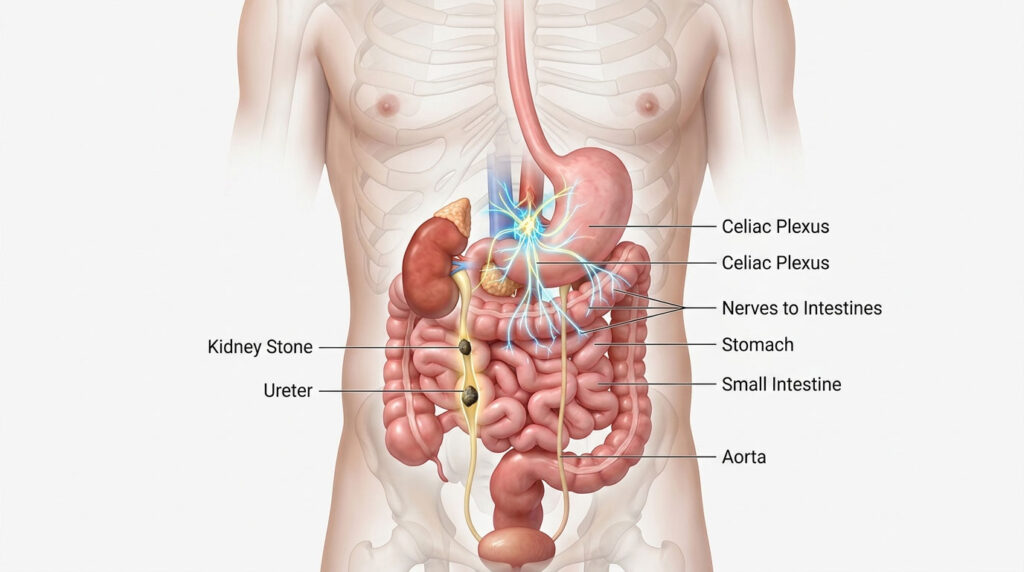
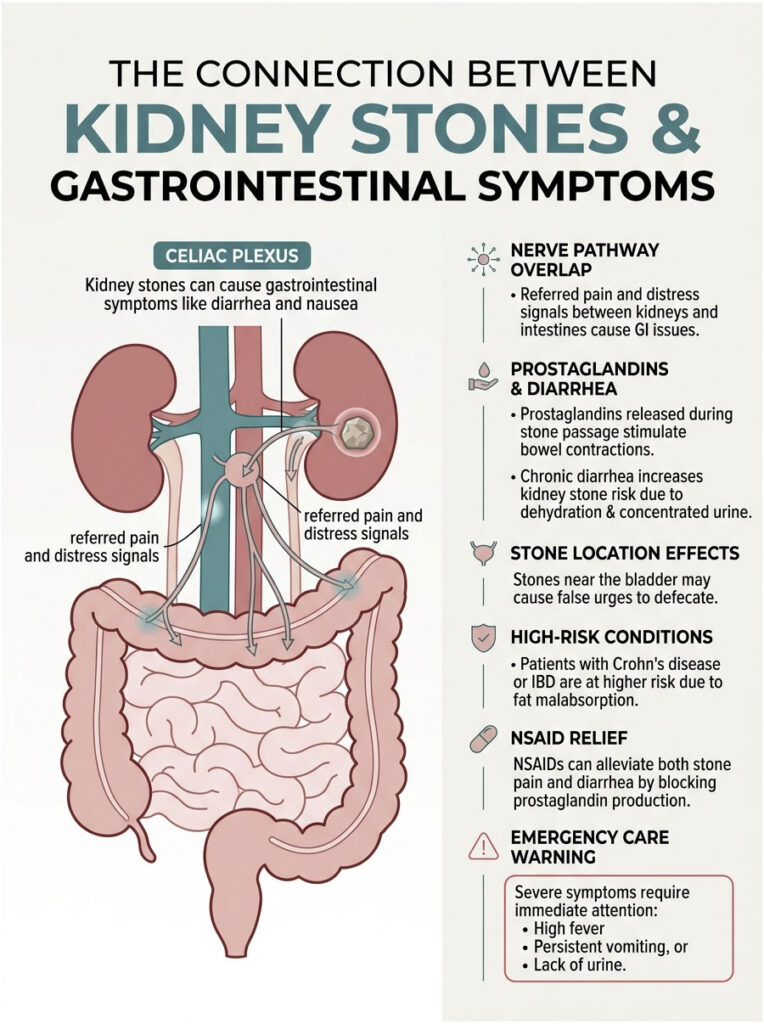
Yes, kidney stones can cause diarrhea, severe nausea, and unpredictable digestive upset. The kidneys and your gastrointestinal tract share the same nerve pathways, especially the vagus nerve and the celiac plexus. When a stone triggers intense pain, those shared nerves flood your body with distress signals that disrupt normal digestion. On top of that, your body releases inflammatory chemicals called prostaglandins to help push the stone out, and those same chemicals stimulate the smooth muscles in your bowels, causing cramping and loose stools.
Key Statistics on Kidney Stones and GI Symptoms
- About 11% of men and 9% of women in the United States will develop a kidney stone in their lifetime.
- Up to 74% of patients having an acute stone attack report some kind of gastrointestinal distress when they reach the emergency room.
- Nausea and vomiting are the most common GI complaints, affecting roughly 60% of acute renal colic patients.
- Around 18% of patients experience active diarrhea, especially when the stone reaches the lower pelvic region near the bladder.
- Chronic dehydration from ongoing diarrhea raises the risk of new stone formation by 32%.
- Patients with Inflammatory Bowel Disease (IBD) are up to 100 times more likely to develop calcium oxalate stones than the general population.
The Biology: How Renal Colic Triggers Gut Distress
To understand why your stomach goes haywire during a stone attack, you need to look closely at your anatomy. The pain itself is intense, but the body’s full response is even more complex. Let me walk you through what’s actually happening inside.
What Is Nephrolithiasis?
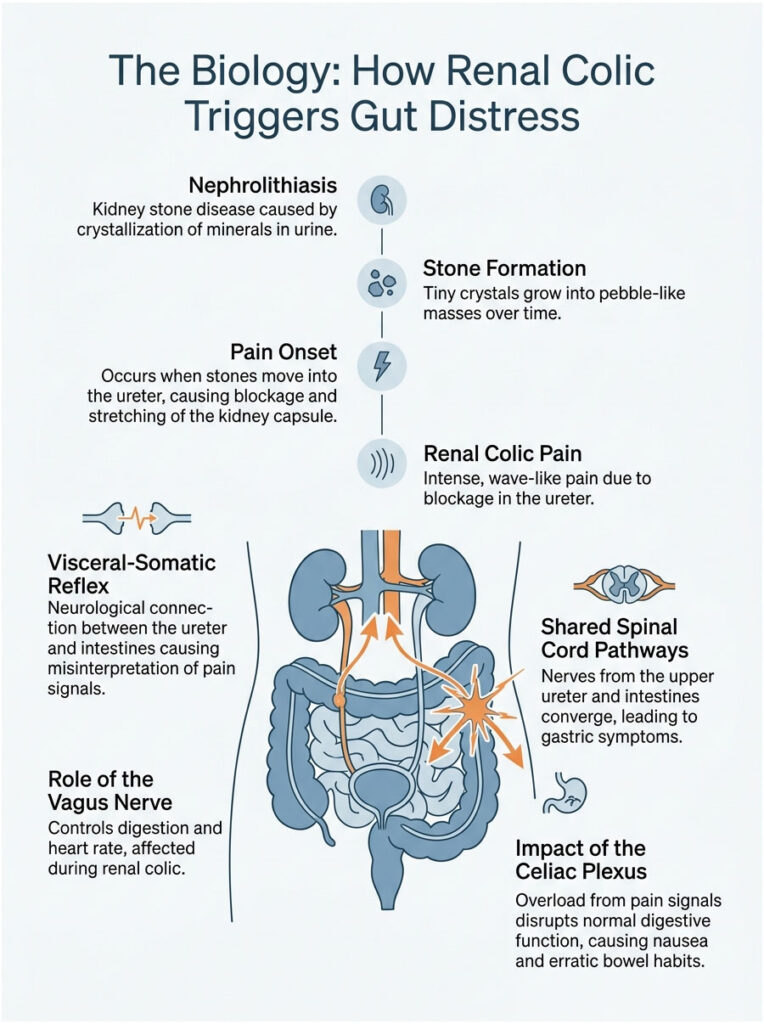
The medical term for kidney stone disease is nephrolithiasis. It happens when minerals in your urine concentrate, crystallize, and bind together. Over months or years, those tiny crystals form hard, pebble-like masses inside your kidney.
As long as a stone sits quietly inside the spacious kidney chambers, it usually causes no pain at all. Trouble begins when the stone drops into the ureter, the narrow muscular tube that carries urine from your kidney to your bladder.
When a jagged stone gets stuck in this tight tube, urine can no longer flow downward. The blockage causes urine to back up, stretching the sensitive kidney capsule. That sudden stretching produces the wave-like, excruciating pain we call renal colic.
The Visceral-Somatic Reflex
So how does a blocked ureter mess with your bathroom habits? It comes down to something called the visceral-somatic reflex. Think of it as a hidden neurological bridge between completely different organs.
When your ureter stretches and spasms around a stuck stone, it fires massive pain signals straight into your spinal cord. The nerves coming from the upper ureter enter the spinal cord at the same level (T10 to L1) as the nerves from your intestines.
Because all these signals arrive at the same junction, your brain gets confused. It misreads where the pain is actually coming from and broadcasts general distress signals to your nearby intestines, as if they were under attack too.
This is the main neurological reason patients suddenly develop kidney stone GI symptoms. Your gut isn’t infected or damaged. It’s just responding to a false alarm caused by crossed wires in the spinal cord.
The Vagus Nerve and Celiac Plexus
The connection runs even deeper than the spinal cord. Your kidneys and upper digestive tract share a huge autonomic nerve supply, and this shared wiring is key to understanding your symptoms.
The vagus nerve is a major cranial nerve that controls things like resting digestion and heart rate. Right alongside it sits the celiac plexus, a nerve hub that acts as a central relay for both the kidneys and the upper digestive system.
During severe renal colic, pain signals overload the celiac plexus. That overload disrupts your normal digestive rhythm almost instantly. According to anatomical guidelines from the American Urological Association, this shared autonomic pathway is exactly why intense flank pain triggers nausea, vomiting, and erratic bowel habits.
Expert Insight: When I treat anxious patients in the ER, I always tell them their gut isn’t actually sick. Their intestines are reacting in sympathy to the pain signals racing through the celiac plexus. Once we treat the stone and relieve the blockage, the digestive symptoms vanish.
The Chemical Side: Prostaglandins and Bowel Spasms
Nerves only tell half the story. The link between kidney stones and bowel movements is also driven by powerful chemicals flooding your bloodstream. Let’s look at the microscopic battle happening inside your blocked ureter.
Inflammation in the Ureter
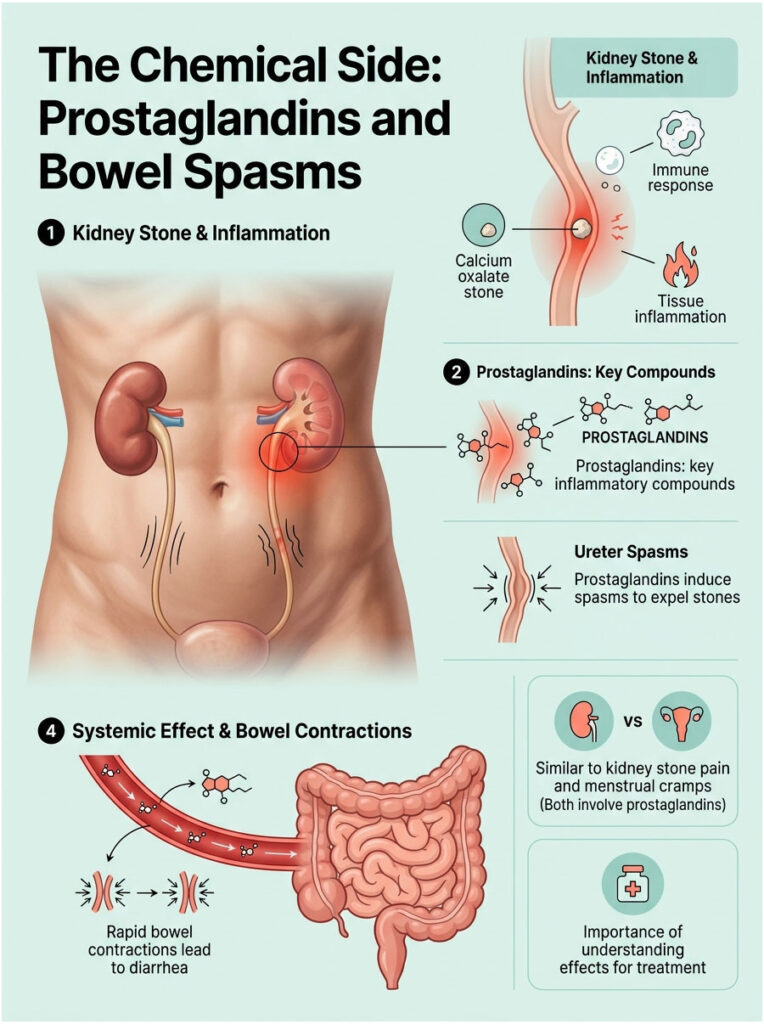
Imagine dragging a sharp piece of glass across the inside of your cheek. That’s basically what a calcium oxalate stone does to the delicate lining of your ureter. The scraping causes immediate trauma, swelling, and inflammation.
Your immune system treats the stuck stone as a foreign invader. White blood cells rush in, the local tissues swell, and unfortunately that swelling makes the narrow tube even tighter around the trapped stone.
This trauma sets off a chemical alarm system throughout the body. To force the stone out, the surrounding tissues start producing powerful inflammatory compounds.
How Prostaglandins Stimulate the Bowel
The most important of these chemicals are prostaglandins, hormone-like compounds that control inflammation, blood flow, and muscle contractions. During a kidney stone attack, prostaglandins force the ureter to spasm violently and push the stone toward the bladder.
Here’s the catch: these chemicals don’t stay inside the urinary tract. They leak into the bloodstream and travel straight to your digestive system.
Prostaglandins are well known for stimulating smooth muscle contractions in the bowels. They make your intestines squeeze rapidly and forcefully, which leads to sudden cramping and watery stools.
The Systemic Effect
This systemic prostaglandin response is well documented. Peer-reviewed pharmacology research confirms that high prostaglandin levels during renal colic speed up the entire digestive process. Food moves through your system too quickly to absorb water properly, which causes diarrhea.
Interestingly, this is the same chemistry that causes severe diarrhea during menstrual cramps. The uterus releases prostaglandins to shed its lining, and those chemicals leak over to stimulate the bowels.
Understanding this chemical cascade matters because it explains why some medications work wonders while others do almost nothing. We’ll talk about how to block these chemicals later in the management section.
Does Stone Location Matter? Tracking the Stone’s Journey
Not all urinary stones cause the same symptoms. The pain and digestive upset you feel depend heavily on where the stone is currently stuck. Experienced urologists can often guess a stone’s location from your symptoms alone, before we even run a CT scan.
The Ureteropelvic Junction (UPJ)
When a stone first leaves the kidney, it hits its first major bottleneck: the ureteropelvic junction, or UPJ. This sits high in your back, just under the lower ribs.
A blockage here causes textbook renal colic. Patients usually feel sharp, stabbing pain in the flank that radiates around to the upper abdomen. Because of the high location, the shared nerves mainly trigger the upper stomach, so UPJ stones cause intense nausea, dry heaving, and vomiting. Diarrhea is actually rare at this stage.
The Mid-Ureter
If the stone makes it past the UPJ, it slowly travels down the tube. As it reaches the mid-ureter, the pain pattern shifts lower. It moves down the side of the abdomen toward the belly button.
Patients often describe this as feeling like a bad stomach ache or food poisoning. The pain waves space out a bit but stay intense when they hit. The intestines become highly irritable, and prostaglandin-driven contractions start affecting the middle sections of the bowel. You might notice bloating, trapped gas, and the first signs of loose stools.
The Ureterovesical Junction (UVJ)
Symptoms change dramatically when the stone reaches the bottom of the urinary tract. The narrowest spot in the entire system is where the ureter joins the bladder, called the ureterovesical junction, or UVJ.
A stone lodged at the UVJ causes very specific and distressing symptoms. This area sits deep in the bony pelvis, right next to the rectum and lower colon. Because of how close everything is, inflammation here directly irritates the lower bowels.
When a stone gets stuck at the UVJ, patients almost always develop something called rectal tenesmus. This is a constant, maddening false sensation that you urgently need to have a bowel movement. Inflamed nerves trick your brain into thinking your rectum is full.
This is exactly why patients say they’re “pooping more” with a kidney stone. Pressure and swelling at the UVJ create referred pain that makes you run to the bathroom over and over. It’s the clearest example of how kidney stones and bowel movements are linked.
Kidney Stone or Stomach Bug? How to Tell the Difference
Because the symptoms overlap, figuring out the cause at home is tricky. Many patients assume they ate something bad or caught a stomach bug from their kids. Helping you tell the difference between a true urological emergency and a regular GI issue is a big part of my job.
Ruling Out Appendicitis and Diverticulitis
Right-sided abdominal pain with nausea and vomiting is concerning for any doctor. A stone in the right ureter can perfectly mimic acute appendicitis. Both make you want to double over.
A left-sided stone often mimics diverticulitis, an infection of small pouches in the lower colon. Both cause left lower quadrant pain and loose stools, so the picture looks almost identical.
ER doctors have to act fast here. A ruptured appendix or perforated colon are surgical emergencies. A passing kidney stone, while brutally painful, rarely needs immediate surgery.
Identifying Gallbladder Attacks
Gallbladder issues also enter the picture with upper abdominal pain. A right-sided stone high near the ribs can mimic a gallbladder attack (cholecystitis), since both cause back pain and severe nausea.
The difference is that gallbladder pain usually flares up after a heavy, greasy meal. Renal colic strikes randomly. A kidney stone doesn’t care if you just ate a cheeseburger or fasted all day.
Gallbladder pain also tends to radiate to the right shoulder blade. Kidney stone pain moves downward, from the flank into the groin. Tracking the direction of the pain is a major diagnostic clue.
The “Stone Dance” Test
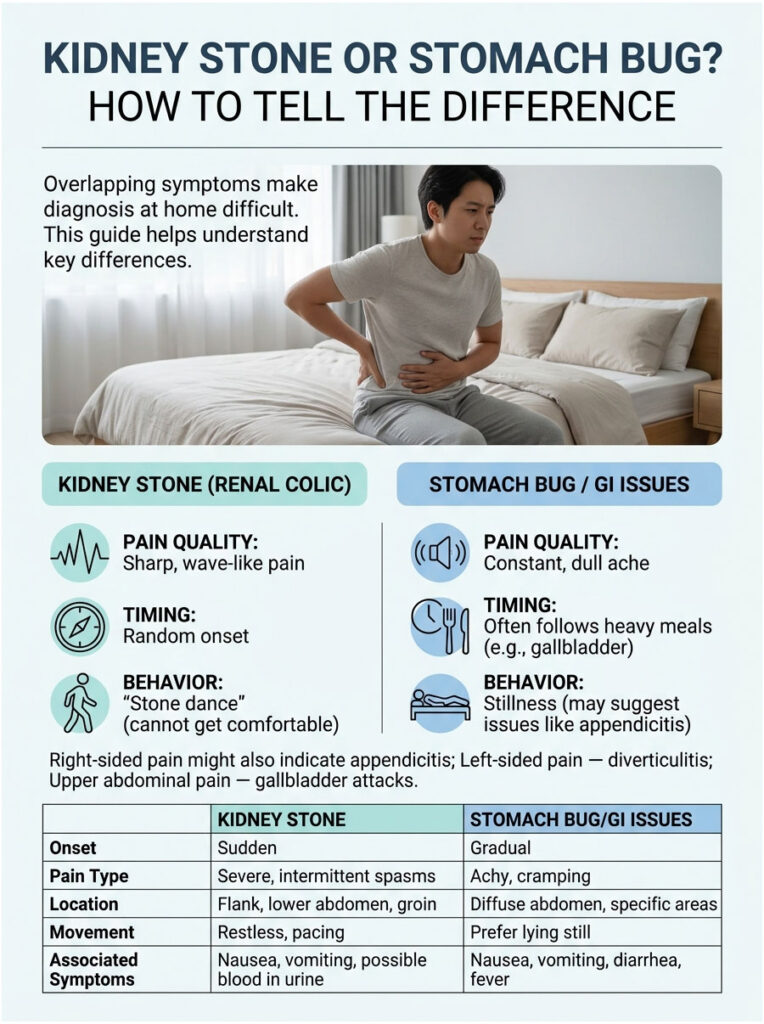
The most reliable way to tell the difference without a scan is to watch how the patient behaves. In urology, we call it the “stone dance.” A patient with renal colic is restless, pacing, writhing, and unable to find a comfortable position.
A patient with peritonitis or a ruptured appendix does the opposite. They lie completely still, often curled into a fetal position. Any movement, even a deep breath, makes their pain worse.
Another clue is the quality of the pain. Referred pain from a stone comes in intense waves, spiking to a 10, easing for twenty minutes, then returning hard. Most GI illnesses give you a constant, dull, unrelenting ache.
Table 1: Kidney Stone (Renal Colic) vs. GI Illness
| Clinical Feature | Kidney Stone (Renal Colic) | GI Illness (Virus or Infection) |
|---|---|---|
| Primary Pain Location | One-sided flank or lower back, radiating toward the groin | Generalized cramping or pain in specific gut quadrants |
| Quality of Pain | Sharp, stabbing, comes in severe waves | Constant dull ache or cramps before bowel movements |
| Visible Blood in Urine | Common (urine looks pink, red, or cola-colored) | Rare, unless severe dysentery is present |
| Patient Movement | Restless, pacing, can’t sit still | Lethargic, prefers fetal position |
| Fever | Only if a urinary infection develops | Common early sign of viral or bacterial infection |
The Reverse Link: How Chronic Diarrhea Causes Kidney Stones
So far we’ve talked about how a moving stone triggers loose stools. But in my clinic, I often see the opposite scenario. Chronic, unmanaged digestive issues are a major risk factor for developing kidney stones in the first place.
This cyclical relationship between gut and kidneys needs careful management. Fix the gut, and you often fix the kidneys. Here’s how a sick stomach creates hard stones.
Fluid Loss and Concentrated Urine
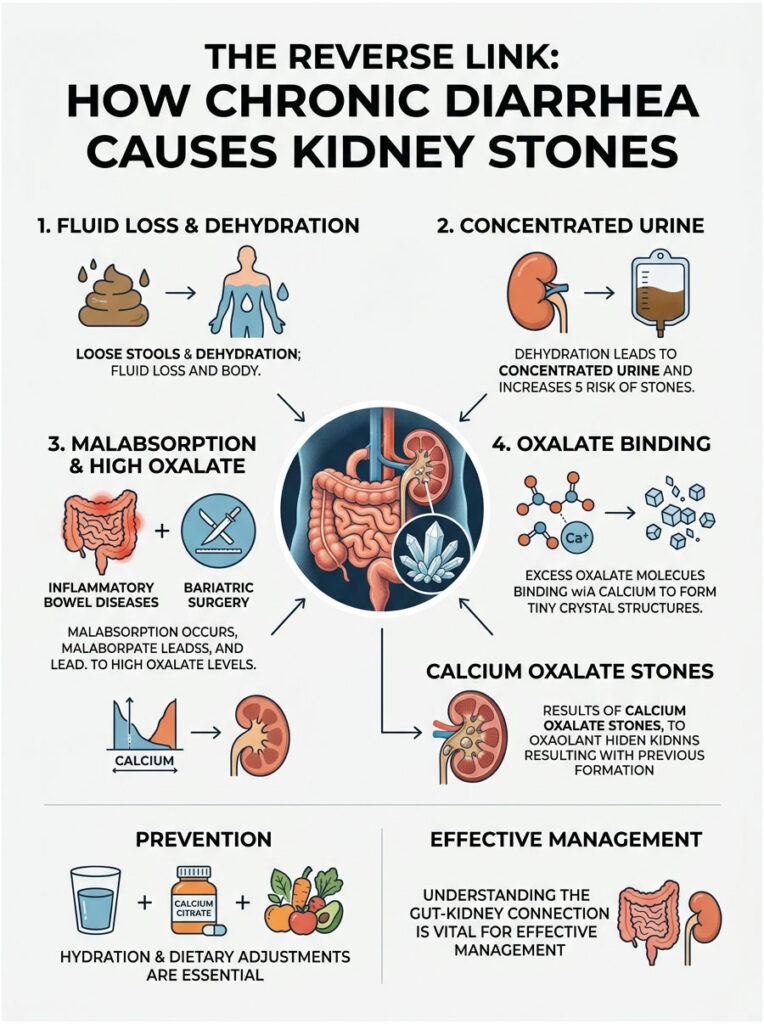
Your kidneys are master filters, and they need a lot of water to flush out daily waste. Chronic loose stools cause rapid fluid loss through the bowels, leading to ongoing dehydration.
When you’re dehydrated, blood volume drops. Your kidneys hold onto as much water as possible, so urine output falls and what comes out is dark and concentrated.
Concentrated urine is the perfect breeding ground for new stones. Without enough water to dilute waste, minerals like calcium, oxalate, and uric acid bump into each other and bind together, forming the crystals that eventually grow into stones.
Malabsorption and Enteric Hyperoxaluria
Patients with Inflammatory Bowel Diseases like Crohn’s or Ulcerative Colitis face a unique urological risk. These conditions damage the lining of the small intestine, preventing proper absorption of dietary fats.
When unabsorbed fat sits in the intestines, it binds to dietary calcium. Normally, calcium binds to a plant compound called oxalate in your stomach, allowing oxalate to pass harmlessly out of your body in stool.
When fat hijacks the calcium, oxalate is left floating free in the gut. Damaged intestines absorb this free oxalate into the bloodstream, and the kidneys have to filter out the excess.
This condition is called enteric hyperoxaluria. The high oxalate levels in urine quickly bind with whatever calcium is available, forming rapidly growing calcium oxalate stones. It’s another example of how deeply kidney stones and bowel movements are connected.
Bariatric Surgery and Stone Risk
We’re also seeing a sharp rise in stone formation among weight loss surgery patients. Procedures like Roux-en-Y gastric bypass change the digestive anatomy and intentionally cause malabsorption to help patients lose weight.
Unfortunately, that intentional malabsorption creates the same enteric hyperoxaluria seen in Crohn’s disease. Bariatric patients also tend to have chronic loose stools, which compounds the dehydration risk.
Urologists now work closely with bariatric surgeons to monitor these patients. We often prescribe calcium citrate supplements to be taken with meals, ensuring there’s enough calcium in the gut to bind oxalate before it reaches the kidneys.
Table 2: Stone Types Linked to Gut Disorders
| Stone Type | Link to Gut Health | Prevention |
|---|---|---|
| Uric Acid Stones | Chronic diarrhea causes loss of bicarbonate, leading to acidic urine | Hydration, alkalizing agents like potassium citrate, less purine-rich meat |
| Calcium Oxalate Stones | Fat malabsorption leaves free oxalate for kidneys to filter | Take calcium with meals to bind oxalate in the stomach |
What Recent Research and Case Studies Tell Us
Medical understanding of kidney stone GI symptoms has come a long way over the past decade. Urologists no longer view the urinary system in isolation from the rest of the body. We rely on extensive clinical data and real-world cases to guide modern treatment.
Data on Atypical Presentations
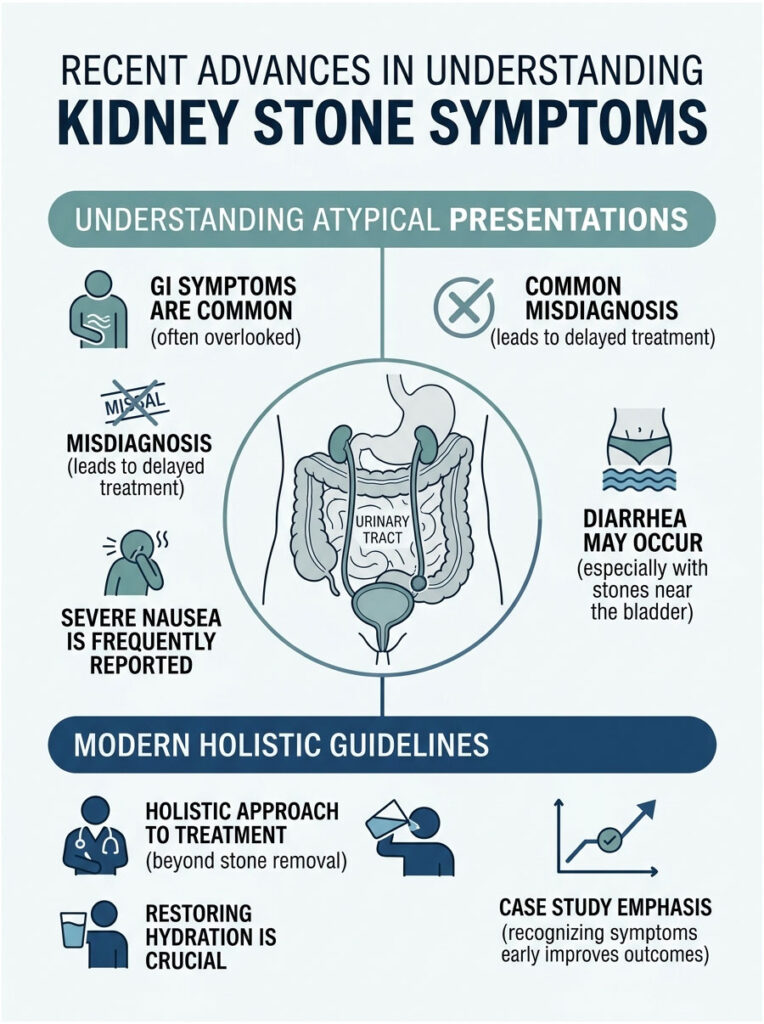
Classic flank pain and bloody urine are easy to spot. Atypical presentations need a sharper clinical eye. Recent studies show just how common confusing, overlapping symptoms really are.
Data from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) shows that most stone patients experience severe nausea. A specific subset present with diarrhea as their main complaint, almost always when the stone is trapped deep in the pelvis near the bladder.
Researchers note that these atypical cases often get misdiagnosed in urgent care. Patients are sent home with a label of gastroenteritis, told to drink ginger ale and rest. They only return days later when the renal colic becomes unbearable and the flank pain finally appears.
A Real ER Case
Let me share a case I see often. Last month I consulted on a 45-year-old man with severe lower abdominal cramping and frequent watery diarrhea. He had no fever but felt a constant urge to use the bathroom.
The ER physician initially suspected food poisoning or an IBS flare. He was given IV fluids and anti-nausea meds. But he stayed restless, constantly shifting in bed.
I ordered a non-contrast CT KUB scan to rule out a stone. The scan showed a 5-millimeter calcium oxalate stone wedged at the left ureterovesical junction. His diarrhea was entirely a referred symptom caused by inflammation pressing against his lower colon.
Insights from Current Guidelines
Modern urological guidelines push for a holistic approach. When a patient presents with overlapping GI and urological symptoms, we look at the entire clinical picture, not just the localized pain.
In my own practice, I follow strict protocols for these confusing cases. When a patient asks if kidney stones can cause diarrhea, the first thing I check is hydration status. The combination of vomiting, loose stools, and reduced fluid intake creates a dangerous cycle of dehydration fast.
Guidelines say restoring fluid balance is just as important as removing the stone. IV fluids are often the first treatment in the ER. This protects kidney function while calming the irritated digestive tract.
Managing Pain and Bowel Symptoms at Home
If you’re at home passing a stone right now, you need practical advice. Managing the pain and the unpredictable bowel symptoms takes a careful approach. Here’s what I tell my own patients to help them get through the worst of it.
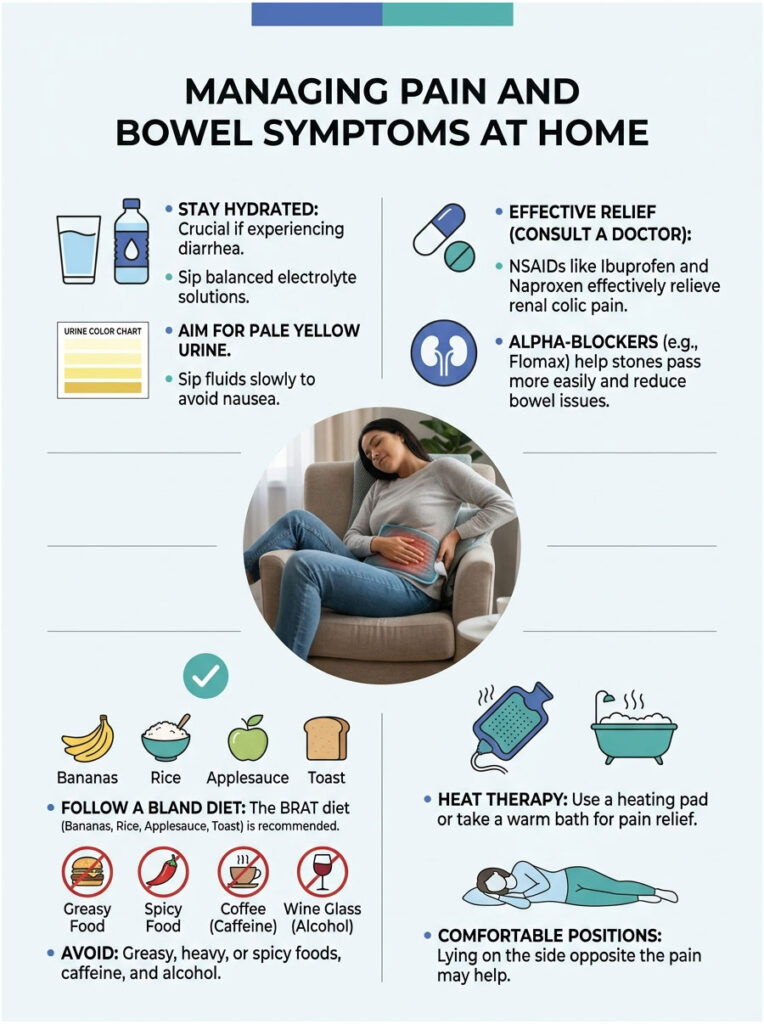
Hydration Done Right
Hydration is your best weapon against a passing stone. But there’s a real difference between chugging water and hydrating effectively. If you’re having loose stools, plain water might not be enough.
Diarrhea strips your body of essential electrolytes like sodium, potassium, and magnesium. I recommend balanced electrolyte solutions or oral rehydration salts. Sip them slowly throughout the day.
Gulping large amounts of water at once is a bad idea. It triggers stretch receptors in your stomach, worsens nausea, and you’ll likely vomit it back up. Your goal is pale yellow urine, which means you’re properly hydrated.
Medications That Actually Work
Over-the-counter medications play a huge role in home management. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) like Ibuprofen or Naproxen are very effective for renal colic. They work much better than acetaminophen (Tylenol).
NSAIDs work because they block the body’s production of prostaglandins. By stopping prostaglandin release, you reduce ureteral spasms. More importantly, blocking these chemicals also stops the smooth muscle contractions in your bowels, which directly treats the diarrhea.
Doctors also frequently prescribe alpha-blockers like Flomax (Tamsulosin). These relax the smooth muscles at the bottom of the ureter, helping the stone drop into the bladder with less resistance and quickly resolving the bowel-related issues.
Eat Bland, Eat Simple
While you’re passing a stone, your digestive tract is sensitive and easily irritated. Skip heavy, greasy, or spicy foods, which only make things worse.
Switch to a bland, easy-to-digest diet until the stone passes. The classic BRAT diet works well: Bananas, Rice, Applesauce, and Toast. These foods are gentle and contain soluble fiber that helps firm up loose stools.
Avoid caffeine and alcohol completely during an attack. Both act as diuretics, pulling water from your body and worsening dehydration.
Heat Therapy and Comfort Positions
Don’t underestimate simple physical comfort. Heat therapy is incredibly effective for the referred pain of renal colic. A heating pad on your flank or lower abdomen brings real relief.
Heat increases local blood flow and relaxes cramping muscles in both your back and gut. A warm bath or hot shower can also calm your nervous system. Many patients say the hot water distracts them from the pain.
Finding a comfortable position is hard during a stone attack. Some patients get temporary relief lying on the side opposite the pain, with a pillow between their knees. Experiment, but don’t be surprised if the stone dance keeps you moving.
Recovery: Restoring Your Gut and Kidney Health
Passing the stone is a huge relief, but the journey isn’t quite over. The physical stress, medications, and dehydration take a toll. You need a plan to restore both your gut and your kidneys.
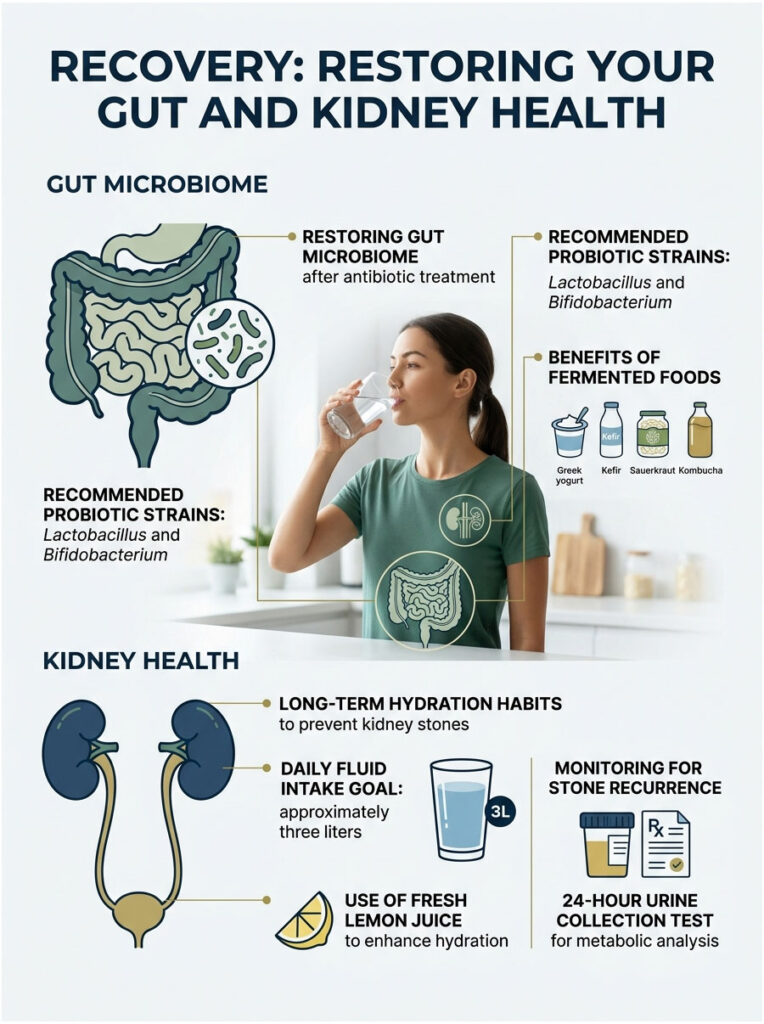
Rebuild Your Gut Microbiome
If you were treated in the ER, you probably received IV antibiotics to prevent infection. Lifesaving as they are, antibiotics wipe out the good bacteria in your gut, which can leave you with lingering diarrhea for weeks.
Start a high-quality probiotic right after finishing any prescribed antibiotics. Look for strains like Lactobacillus and Bifidobacterium, which are proven to restore intestinal balance.
Add fermented foods to your daily meals too. Greek yogurt, kefir, sauerkraut, and kombucha are great natural sources of beneficial bacteria. Restoring this balance clears up any lingering GI symptoms.
Build Long-Term Hydration Habits
Once you’ve formed one stone, your risk of forming another within five years is roughly 50%. The best way to prevent recurrence is to permanently change your hydration habits. You can’t go back to drinking only soda and coffee.
Aim for around three liters of fluid daily. I recommend adding fresh lemon juice to your water. Lemons are packed with citrate, which prevents calcium and oxalate from binding in your urine.
Carry a water bottle everywhere. If you work in heat or exercise heavily, drink even more to make up for sweat loss. Your urine should stay pale yellow throughout the day.
Monitor for Recurrence
If you catch a stone in a strainer, bring it to your urologist. We’ll send it to a lab for chemical analysis. Knowing exactly what your stone is made of (calcium oxalate, uric acid, struvite) lets us build a specific prevention plan.
For patients with recurrent stones or chronic gut issues like Crohn’s, we order a 24-hour urine collection test. It measures your daily output of calcium, oxalate, citrate, and total volume, giving us a metabolic snapshot of your kidney function.
Based on the results, we may prescribe potassium citrate or thiazide diuretics, and refer you to a renal dietitian who can help you balance the dietary needs of both your gut and kidneys.
Red Flags: When to Get Emergency Care
Most small stones (under 5 millimeters) pass safely at home with time and hydration. But certain symptoms mean a life-threatening complication is developing. You need to know when home care is no longer safe.
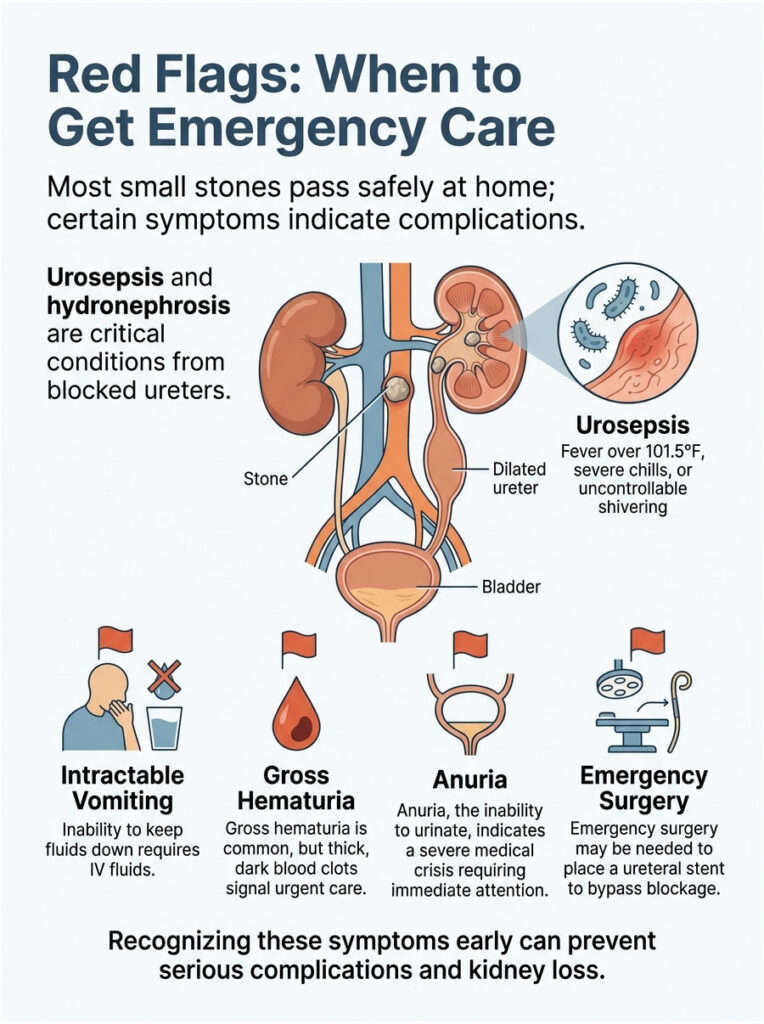
Signs of Urosepsis and Hydronephrosis
The most dangerous complication of nephrolithiasis is an infected blockage. When a stone fully blocks the ureter, urine pools inside the kidney chamber. Bacteria multiply quickly in that warm, stagnant pool, creating a serious infection.
The backup of urine causes the kidney to swell like a water balloon, a condition called hydronephrosis. If left untreated, hydronephrosis can permanently damage the kidney’s filtering tissues within days. You don’t want to lose a kidney over a small stone.
If infected urine spills back into your bloodstream, you develop urosepsis, a deadly blood infection that crashes your blood pressure. If you have a fever over 101.5°F, severe chills, or uncontrollable shivering with your renal colic, go to the emergency room immediately.
Intractable Vomiting and Heavy Bleeding
Mild nausea is normal. Intractable vomiting is a major red flag. If you can’t keep fluids down for more than a few hours, you’ll become dangerously dehydrated and need IV fluids in the hospital.
Visible blood in the urine, called gross hematuria, is common as the stone scrapes the ureter. Urine may look pink, bright red, or cola-colored. But pay attention to the texture.
If you’re passing thick, dark blood clots that look like jelly, get medical help immediately. Large clots can cause secondary blockages in the bladder, leading to a painful condition called urinary retention.
The Danger of Anuria
The most critical red flag is anuria, the complete inability to urinate. If you feel a strong urge but nothing comes out, you’re facing a severe medical crisis.
Anuria suggests one of two terrifying scenarios: stones blocking both ureters at once, or a blocked solitary kidney. Either way, your body has lost the ability to filter toxins from your blood.
This requires emergency surgery within hours. Urologists perform a cystoscopy to place a plastic ureteral stent past the stone. The stent bypasses the blockage, drains the kidney, and prevents permanent failure.
What to Expect at the Urology Clinic
Walking into a busy ER or urology clinic in severe pain is frightening. Knowing what tests we’ll run can ease some of that anxiety. We use specific tools to confirm a stone and rule out other dangerous abdominal emergencies.
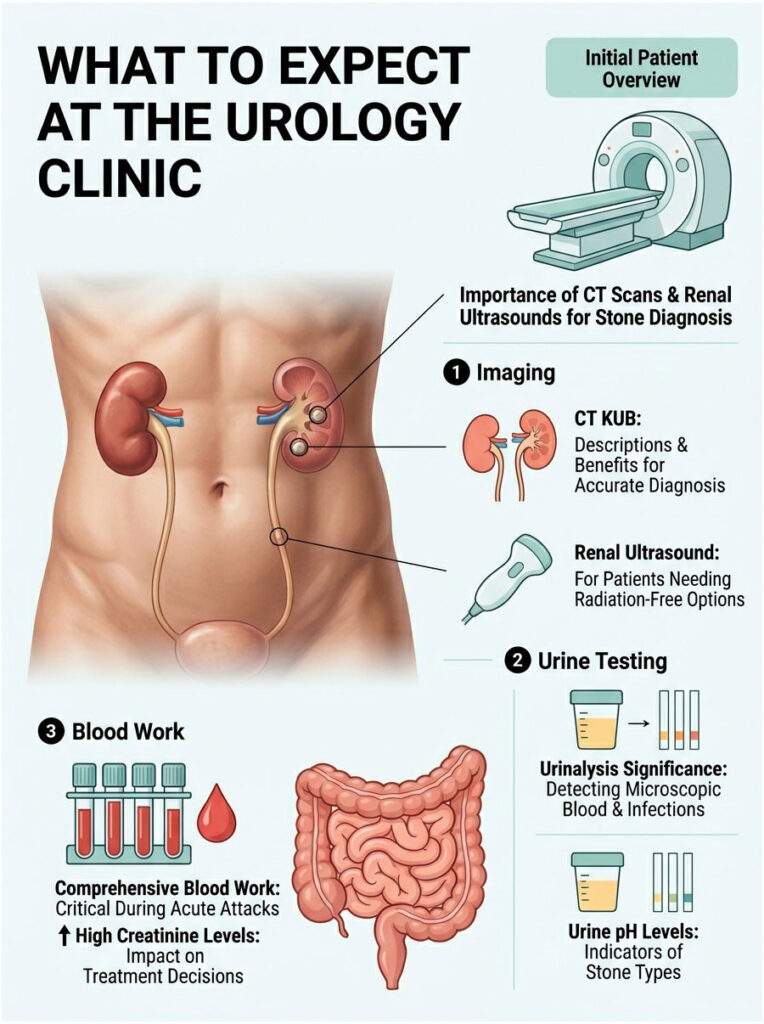
CT Scans and Renal Ultrasounds
The gold standard for diagnosing a urinary stone is a non-contrast CT scan. We order a CT KUB, which looks specifically at the Kidneys, Ureters, and Bladder. It’s fast, painless, and gives us a 3D map of your urinary tract.
A CT KUB tells us the exact size of the stone in millimeters and its density in Hounsfield units, which helps us guess if it’s hard calcium or softer uric acid. It also rules out life-threatening conditions like appendicitis or a ruptured aortic aneurysm.
For pregnant patients or kids needing multiple follow-ups, we avoid radiation entirely and use renal ultrasound instead. Ultrasound can’t always catch tiny stones in the middle ureter, but it’s excellent at spotting kidney swelling.
Urinalysis and Infection Checks
We always ask for a fresh urine sample on arrival. Urinalysis checks for microscopic red blood cells, which confirms the ureter is being scraped. Finding this microscopic blood is a strong clue that a stone is present.
We also look for white blood cells and nitrites, which indicate a hidden bacterial infection brewing behind the stone. If we see signs of infection, we send the urine for culture to identify the exact bacteria.
Urine pH is another diagnostic clue. Highly acidic urine (under 5.5) suggests uric acid stones. Highly alkaline urine (over 7.2) suggests struvite stones, which are infection stones.
Comprehensive Blood Work
Blood tests are equally important during an acute attack. We check your Complete Blood Count (CBC) for elevated white blood cells, a clear sign of infection or potential urosepsis.
We also run a Comprehensive Metabolic Panel (CMP) to check organ function, including Creatinine and Blood Urea Nitrogen (BUN). Creatinine is a muscle waste product that healthy kidneys easily filter out.
If your Creatinine is abnormally high, the blockage is impairing kidney function. This result determines whether we send you home with pain pills or admit you for emergency surgery.
Key Takeaways
The human body is deeply interconnected. When patients ask me whether kidney stones can cause diarrhea, I tell them their overlapping symptoms make perfect biological sense. The intense pain of a passing stone doesn’t stay neatly isolated in your back.
Because the kidneys and intestines share the celiac plexus nerve connection, severe pain easily triggers the visceral-somatic reflex. This neurological confusion causes nausea, vomiting, and unpredictable bowel changes. On top of that, the prostaglandins released to push the stone out also stimulate your bowels to contract.
Remember that the stone’s location dictates your symptoms. A stone at the ureterovesical junction causes intense pelvic pressure and a maddening, false urge to defecate. Understanding this link between kidney stones and bowel movements can really cut down the anxiety during a painful episode.
While GI symptoms during a stone attack are normal, stay alert. Watch your temperature. If you develop a fever, can’t stop vomiting, or stop producing urine, get emergency care immediately. Proper hydration, smart pain management, and quick medical care are your best tools for safely getting through a stone attack.
Frequently Asked Questions
Can kidney stones actually cause diarrhea and stomach upset?
Yes, kidney stones can absolutely cause diarrhea, nausea, and severe stomach upset. As a urologist, I frequently see patients where gastrointestinal distress is a primary symptom. This occurs because the kidneys and the digestive tract share the same nerve pathways, specifically the celiac plexus and the vagus nerve. When a stone causes intense pain (renal colic), these shared nerves send distress signals that disrupt normal bowel function, leading to loose stools and cramping.
What is the biological reason for diarrhea during a kidney stone attack?
The primary biological trigger is the release of inflammatory chemicals called prostaglandins. When a stone scrapes the lining of the ureter, your body releases prostaglandins to help the ureter contract and push the stone out. However, these chemicals leak into the bloodstream and stimulate the smooth muscles of your intestines, causing them to contract rapidly. This increased motility results in sudden, watery diarrhea.
Does the location of the kidney stone change the type of digestive symptoms I feel?
Absolutely. If a stone is high up at the ureteropelvic junction (UPJ), you are more likely to experience intense nausea and vomiting. However, when the stone reaches the ureterovesical junction (UVJ)—the narrowest point near the bladder—it sits very close to the rectum. This proximity often causes ‘rectal tenesmus,’ a false sensation of needing to have a bowel movement, which frequently presents as diarrhea.
How can I tell if my pain is a kidney stone or a stomach bug like gastroenteritis?
One of the most reliable indicators is the ‘stone dance.’ Patients with kidney stones are typically extremely restless, pacing or writhing to find a comfortable position. In contrast, those with a stomach virus or appendicitis usually prefer to lie perfectly still. Additionally, kidney stone pain is paroxysmal (coming in waves) and is often accompanied by hematuria (blood in the urine), which is rare in standard GI illnesses.
Can chronic diarrhea lead to the formation of new kidney stones?
Yes, there is a strong reverse relationship. Chronic diarrhea causes rapid fluid loss, leading to systemic dehydration. When you are dehydrated, your urine becomes highly concentrated (supersaturated) with minerals like calcium and oxalate. This concentration makes it significantly easier for crystals to bind together and form stones. In fact, chronic dehydration increases your stone risk by approximately 32%.
Why do people with Crohn’s disease or IBD get kidney stones more often?
Patients with Inflammatory Bowel Disease (IBD) often suffer from fat malabsorption. Normally, dietary calcium binds to oxalate in the gut to be excreted. When excess fat is present, it ‘steals’ the calcium, leaving the oxalate free to be absorbed into the bloodstream and filtered by the kidneys. This process, known as enteric hyperoxaluria, leads to the rapid formation of calcium oxalate stones.
What is the ‘visceral-somatic reflex’ in relation to kidney stones?
The visceral-somatic reflex is a neurological phenomenon where the brain misinterprets pain signals. Because the nerves from the ureters and the intestines enter the spinal cord at the same levels (T10 to L1), the brain can become ‘confused’ by the massive influx of pain data from a stone. It then broadcasts distress signals to the nearby intestines, causing them to react as if they are also under attack, resulting in referred GI symptoms.
Can weight loss surgery increase my risk of developing stones and diarrhea?
Yes, bariatric procedures like the Roux-en-Y gastric bypass alter the anatomy of the digestive tract, which can lead to malabsorption and chronic loose stools. This anatomical change often results in enteric hyperoxaluria, where the kidneys are forced to filter excessive amounts of oxalate, significantly increasing the risk of stone recurrence. We closely monitor these patients and often recommend calcium citrate supplements to bind oxalate in the gut.
What medications help stop both the stone pain and the diarrhea?
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), such as Ibuprofen or Naproxen, are the gold standard. Unlike standard pain relievers, NSAIDs specifically inhibit the production of prostaglandins. By blocking these chemicals, you reduce the painful spasms in the ureter and simultaneously calm the chemically-induced contractions in your bowels, effectively treating both the renal colic and the diarrhea.
When should I seek emergency care for kidney stone-related diarrhea?
You must seek immediate emergency care if your diarrhea and pain are accompanied by a high fever (over 101.5°F), chills, or uncontrollable shivering. These are red flags for urosepsis, a life-threatening blood infection caused by an infected blockage. Other emergency signs include intractable vomiting (inability to keep fluids down) and anuria, which is the complete inability to pass urine.
What is the best way to stay hydrated if I have both a stone and loose stools?
If you are losing fluids through both vomiting and diarrhea, plain water may not be enough. You need medical-grade oral rehydration salts or balanced electrolyte solutions to replace sodium and potassium. I advise my patients to sip these fluids slowly and steadily; chugging large amounts of water can trigger the stomach’s stretch receptors and worsen nausea, leading to further fluid loss.
How do urologists diagnose a stone when the symptoms look like a GI issue?
The gold standard diagnostic tool is a non-contrast CT KUB (Kidneys, Ureters, and Bladder). This scan allows us to see the stone’s exact size and location while ruling out GI emergencies like appendicitis or diverticulitis. We also perform a urinalysis to look for microscopic blood and infection markers (nitrites/leukocytes) and check blood creatinine levels to ensure the stone isn’t causing acute kidney injury.
Disclaimer
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The relationship between urological and gastrointestinal symptoms can be complex and may indicate serious underlying conditions. Always consult a qualified healthcare professional or urologist before making health decisions or if you are experiencing severe pain. If you have a high fever or cannot urinate, seek emergency medical attention immediately.
References
- American Urological Association (AUA) – https://www.auanet.org/ – Provided clinical guidelines on the management of acute renal colic and autonomic nerve pathways.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – https://www.niddk.nih.gov/ – Source for statistics on kidney stone prevalence and gastrointestinal symptom frequency.
- Urology Care Foundation – https://www.urologyhealth.org/ – Expert insights into the symptoms of stones at the ureterovesical junction (UVJ).
- Journal of Endourology – Peer-reviewed data regarding the systemic effects of prostaglandins on smooth muscle contractions in the bowel.
- Crohn’s & Colitis Foundation – https://www.crohnscolitisfoundation.org/ – Authoritative information on the link between IBD, malabsorption, and calcium oxalate stones.
- Mayo Clinic – https://www.mayoclinic.org/ – Clinical descriptions of nephrolithiasis and the differential diagnosis of abdominal pain.