Patients walk up to my pharmacy counter every day with new prescriptions for serious inflammation. They’re hoping for fast relief from joint pain, asthma flare-ups, or autoimmune attacks. And during those first consultations, one question comes up again and again: do steroids cause diarrhea?
The short answer is yes, they certainly can.
Table of Contents
Most patients walk in worried about weight gain or sleepless nights. But digestive trouble is far more common than people realize. As a clinical pharmacist with over 15 years behind the counter, I spend a lot of my day helping patients manage these uncomfortable side effects.
Your digestive tract is incredibly sensitive to hormonal and chemical shifts. When you introduce synthetic hormones into your system, the body reacts in ways most people don’t expect. The body redirects its energy and resources, leaving the gut exposed and vulnerable.
Quick Answer
Yes, both oral and injected corticosteroids can cause diarrhea. These medications block protective chemicals in the stomach lining, alter the natural gut microbiome, and speed up bowel motility. Taking your dose with a substantial meal and following a proper tapering schedule can significantly cut down these uncomfortable digestive side effects.
Key Statistics on Steroids and Digestive Health
- Up to 20% of patients on high-dose oral corticosteroids report significant gastrointestinal distress in clinical trials.
- The risk of severe gastric bleeding goes up 4 times when steroids are combined with NSAIDs like Ibuprofen.
- Changes in gut microbiota can show up within 48 to 72 hours of starting a high-dose oral steroid regimen.
- Over 60% of anabolic steroid users report altered bowel habits during active cycles.
- Proper tapering reduces the risk of withdrawal-induced rapid gut motility by nearly 80%.
- Patients taking proton pump inhibitors alongside their steroid see a 50% drop in upper GI complications.
Understanding Corticosteroids and Gut Sensitivity
To understand why these drugs upset your stomach, we need to define what they actually do inside the body. Synthetic corticosteroids are designed to mimic cortisol, a hormone naturally produced by your adrenal glands.
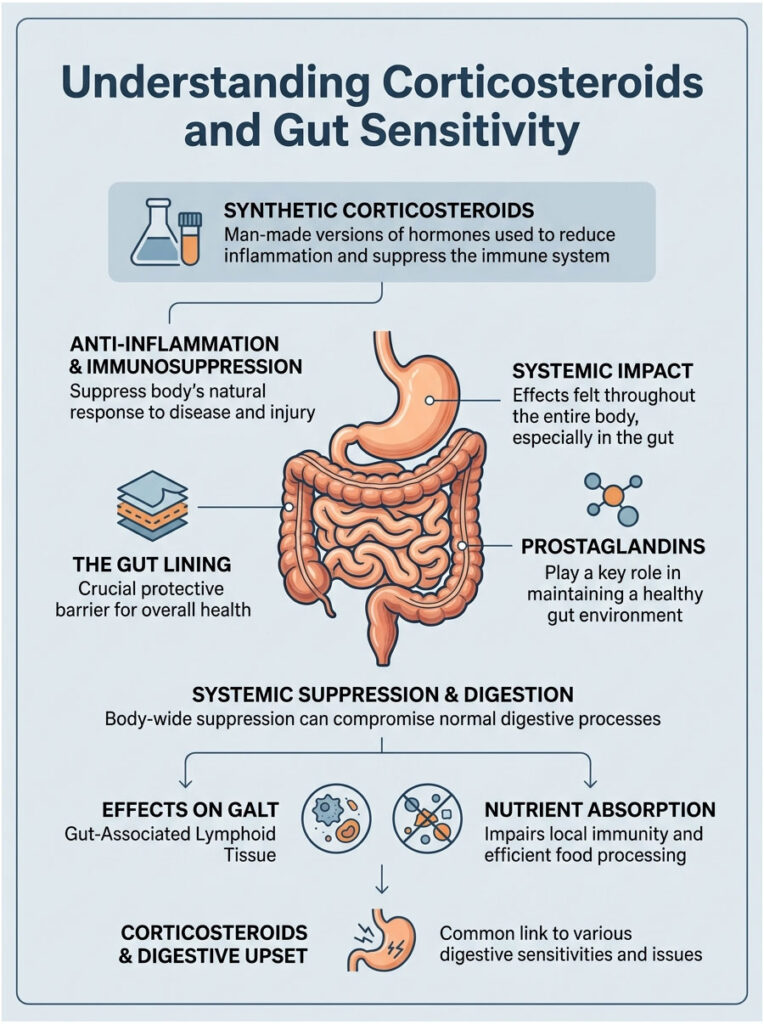
Doctors prescribe them for their powerful anti-inflammatory and immunosuppressive effects. They’re literal lifesavers for conditions ranging from rheumatoid arthritis to severe allergic reactions. But this systemic suppression doesn’t just target your inflamed knee or swollen airways. It affects your entire body, head to toe.
Your stomach and intestines are lined with a specialized protective barrier that defends delicate tissues from harsh digestive juices. When we alter the chemicals that maintain this barrier, the downstream effects are immediate and severe.
What Corticosteroids Actually Are
Corticosteroids aren’t the same as the muscle-building drugs you hear about in sports. Medical steroids like prednisone and dexamethasone are classed as glucocorticoids. They bind to receptors inside your cells and switch off the genes that drive inflammation.
While shutting down inflammation sounds great, your body actually uses mild inflammatory signals for routine maintenance and repair. When you turn off these pathways completely, you interrupt normal cellular healing. This is where the connection between these drugs and digestive upset begins.
The medication essentially tricks your body into a state of constant stress management. During this time, secondary functions like optimal digestion take a back seat.
Here’s the thing: your gut needs steady blood flow to function well. When synthetic hormones tell your body it’s in emergency mode, blood flow to the gut gets restricted. That restriction slows healing of the intestinal lining.
How the Gut Lining Stays Protected
Your digestive tract is a hostile environment by design. Stomach acid is strong enough to dissolve some metals. To stop your body from digesting itself, the GI mucosa secretes a thick layer of protective mucus and bicarbonate.
This barrier depends heavily on chemical messengers called prostaglandins. Prostaglandins are the unsung heroes of your stomach. They keep blood flowing to the stomach lining and stimulate constant production of protective mucus.
Without them, the stomach lining thins out fast. The irritation doesn’t stay in the stomach either. It travels down into the intestines, causing inflammation throughout the digestive network.
Expert Insight: Think of prostaglandins as the maintenance crew for your stomach lining. Corticosteroids basically send this crew on vacation. Without routine upkeep, the protective barrier degrades, which is why stomach upset is such a common reality for patients.
How Systemic Suppression Alters Digestion
When you swallow a pill, it dissolves and enters your bloodstream through the liver. From there, the active ingredients circulate everywhere. The digestive tract is one of the first systems to feel the impact.
A huge portion of your immune system actually lives in your gut. We call it gut-associated lymphoid tissue, or GALT. When you suppress the GALT, the gut handles food and bacteria differently. The intestines become less efficient at absorbing nutrients and water, which is a major reason for loose, unformed stools.
Why Steroids Trigger Diarrhea: The Real Mechanisms
Going from swallowing a pill to suddenly running for the bathroom involves several biological pathways. It isn’t just a pill irritating your stomach lining directly. Systemic changes alter how your entire digestive system works.
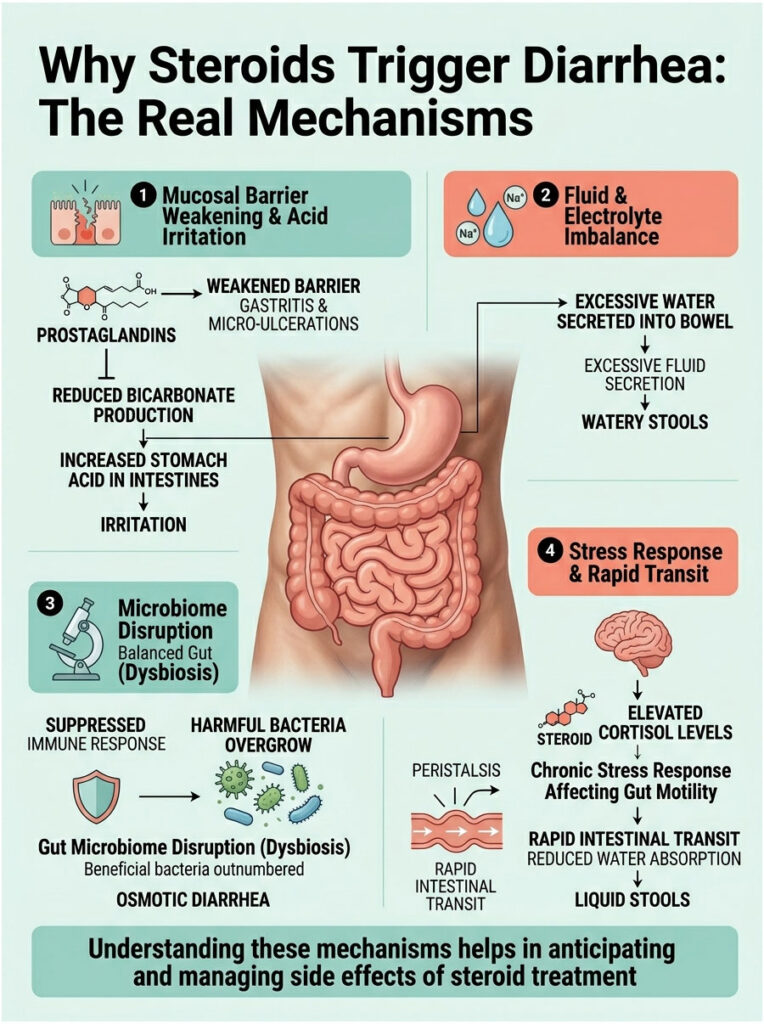
We can break this down into three categories: chemical inhibition of protective barriers, bacterial imbalance in the intestines, and the neurological signals controlling bowel movements. Together, these three pillars explain why loose stools are so common in the first few days of starting treatment.
Prostaglandin Inhibition and a Weakened Mucosal Barrier
The main pharmacological action of corticosteroids is blocking the cyclooxygenase pathway, often called the COX pathway. By blocking COX, the body stops making prostaglandins.
As we already discussed, low prostaglandins weaken the mucosal barrier. This leads to medication-induced gastritis and tiny micro-ulcerations along the intestinal wall. The body senses this damage and tries to flush out the irritant by secreting excess water into the bowel. That extra water mixes with digesting food, causing watery stools.
But there’s more. Blocking prostaglandins also reduces bicarbonate production. Bicarbonate is your body’s natural antacid. Without it, harsh stomach acid spills into the small intestine, causing chemical burns and further irritation.
Gut Microbiome Disruption (Dysbiosis)
Your intestines are home to trillions of beneficial bacteria. This ecosystem, the gut microbiome, helps digest complex carbs and regulates stool consistency. Medication-induced dysbiosis happens when drugs throw this delicate bacterial balance out of whack.
Synthetic hormones suppress your immune system, which lets opportunistic, harmful bacteria overgrow in the small and large intestines. The beneficial strains that normally firm up your stool get outnumbered fast.
Recent clinical data shows that hormonal shifts directly impact these bacterial colonies. The imbalance leads to a specific pattern called osmotic diarrhea, where altered bacteria produce excess gas and pull water into the colon.
Hypercortisolism and Speed of Digestion
Hypercortisolism just means having too much cortisol in your bloodstream. When you take prescription steroids, you artificially trigger this state. Elevated cortisol kicks off a chronic stress response.
Your enteric nervous system, which runs your gut, is highly sensitive to stress hormones. Cortisol-induced motility happens when these hormones tell your intestines to empty quickly. The body thinks it’s in danger and prepares to flee.
Because of this rapid motility, food moves through your digestive tract too fast. The large intestine doesn’t have time to absorb water from the waste, so the stool stays liquid by the time it exits.
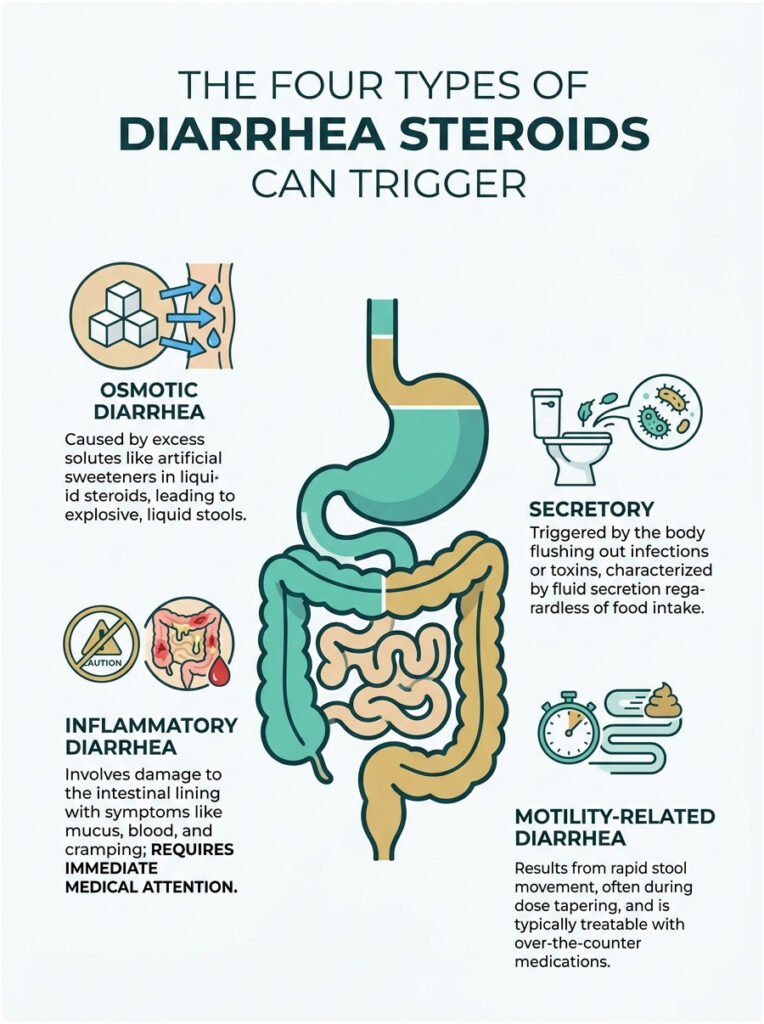
The Four Types of Diarrhea Steroids Can Trigger
Not all diarrhea is the same. In medicine, we categorize loose stools by the specific mechanism causing the problem. Steroids are unique because they can trigger multiple types at once.
Knowing which type you have helps your doctor tailor treatment. You can’t just pop an anti-diarrheal and call it done. You have to address the root cause.
1. Osmotic Diarrhea
Osmotic diarrhea happens when too many solutes stay in your intestine. Water flows into the bowel to balance them out. Some liquid steroid formulations contain artificial sweeteners like sorbitol that act as osmotic laxatives.
These sweeteners pull water from surrounding tissues into the colon. The result is sudden, explosive, mostly liquid bowel movements. This is incredibly common in pediatric patients on liquid prescriptions, and the inactive flavoring ingredients are often the real culprit, not the active drug.
2. Secretory Diarrhea
Secretory diarrhea happens when the body actively pumps electrolytes and water into the bowel. It’s usually a defense against an infection or toxin. Because steroids suppress the immune system, patients are more vulnerable to hidden gut infections.
If you develop a bacterial infection while on steroids, your gut secretes fluid to flush the bacteria out. This type of diarrhea happens whether you’ve eaten or not. It will wake you up at night.
Think of it this way: your gut is turning on the fire hose to clean house. The medication lowered your defenses, and now the body is trying to wash out the invader.
3. Inflammatory Diarrhea
Also called exudative diarrhea, this type involves direct damage to the intestinal lining. As the mucosal barrier breaks down from prostaglandin inhibition, the intestinal walls become raw and inflamed. They start leaking blood, pus, and serum into the stool.
Patients with inflammatory diarrhea often see mucus or dark spots in the toilet, along with severe cramping and a low-grade fever. This is a major red flag. If the medication has caused enough damage to trigger inflammatory diarrhea, you need immediate medical evaluation. It points to severe ulceration or medication-induced colitis.
4. Motility-Related Diarrhea
We touched on this earlier when talking about the gut-brain axis. Motility-related diarrhea is driven entirely by speed. Stool moves so fast that the colon can’t reabsorb water properly.
This is the most common type during a dose taper. As hormone levels swing, the enteric nervous system spasms and pushes waste through too quickly.
The good news is this type is the easiest to treat. Over-the-counter medications that slow gut contractions work very well, and the issue usually resolves once hormone levels stabilize.
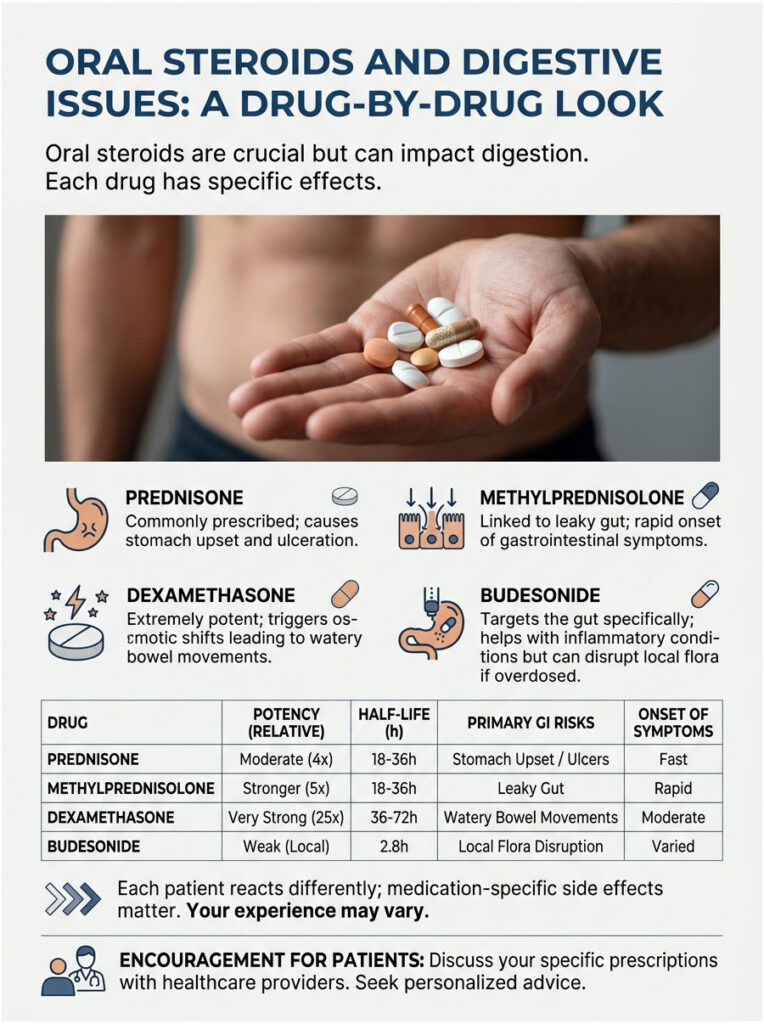
Oral Steroids and Digestive Issues: A Drug-by-Drug Look
Not all oral steroids are created equal. The specific drug your doctor picks heavily influences your digestive experience. Some are mild and short-acting. Others are extremely potent and stick around for days.
In my pharmacy practice, I see distinct patterns of side effects depending on the prescription. Whether you’re on a short course for poison ivy or a long-term regimen for an autoimmune disease, knowing your specific medication matters.
Prednisone and Its Reputation for Stomach Trouble
Prednisone is the most commonly prescribed oral steroid in the United States. It’s incredibly effective but notoriously rough on the stomach. Because it processes systemically through the liver, it affects the entire digestive tract.
Prednisone digestive issues are so common that I routinely warn patients before they leave the counter. The prostaglandin inhibition is profound with this drug. Take it on an empty stomach and severe upset is almost guaranteed within 48 hours. Its chemical structure makes it particularly aggressive on the gastric lining.
Methylprednisolone and Intestinal Permeability
Methylprednisolone is often dispensed as a pre-packaged dose pack starting with a heavy loading dose on day one. Patients frequently ask if loose stools are a side effect of these packs.
The heavy loading phase is strongly linked to increased intestinal permeability, often called leaky gut. The sudden influx of hormones weakens the tight junctions between intestinal cells. During the first 48 to 72 hours, this lets undigested food particles irritate the gut lining. Rapid onset of symptoms is the hallmark of this drug.
Dexamethasone and Osmotic Imbalance
Dexamethasone is a heavy hitter, with potency 25 to 30 times stronger than natural hydrocortisone. Doctors reserve it for severe inflammation, oncology support, or serious respiratory distress.
Because of its extreme potency, dexamethasone causes intense metabolic effects. It can trigger rapid osmotic shifts in the colon, pulling large amounts of water from surrounding tissues. The result is explosive, watery bowel movements. It’s a highly disruptive medication for the digestive tract.
Budesonide: The Gut-Targeted Exception
Budesonide deserves a special mention because it works differently. It’s specifically designed to target the gut and is often prescribed for Crohn’s disease and Ulcerative Colitis.
Unlike prednisone, budesonide has a high first-pass metabolism. It works locally in the intestines and is mostly destroyed by the liver before reaching the rest of the body. Because it acts locally, it actually helps stop inflammatory diarrhea. That said, if the dose is too high it can still cause localized dysbiosis.
Clinical Comparison of Common Oral Corticosteroids
| Medication | Relative Potency | Half-Life | Primary GI Risk | Onset of GI Symptoms |
|---|---|---|---|---|
| Hydrocortisone | Low (1x) | Short (8 to 12 hrs) | Mild mucosal irritation | 3 to 5 days |
| Prednisone | Medium (4x) | Intermediate (18 to 36 hrs) | Prostaglandin inhibition, ulceration | 2 to 4 days |
| Methylprednisolone | Medium (5x) | Intermediate (18 to 36 hrs) | Intestinal permeability, dysbiosis | 48 to 72 hrs |
| Dexamethasone | High (25x to 30x) | Long (36 to 54 hrs) | Severe osmotic imbalance | 24 to 48 hrs |
| Budesonide | High (Local) | Short (Systemic) | Localized flora disruption | Variable |
This table makes it clear why side effects vary so wildly from person to person. A patient on hydrocortisone has a vastly different experience from someone on high-dose dexamethasone.
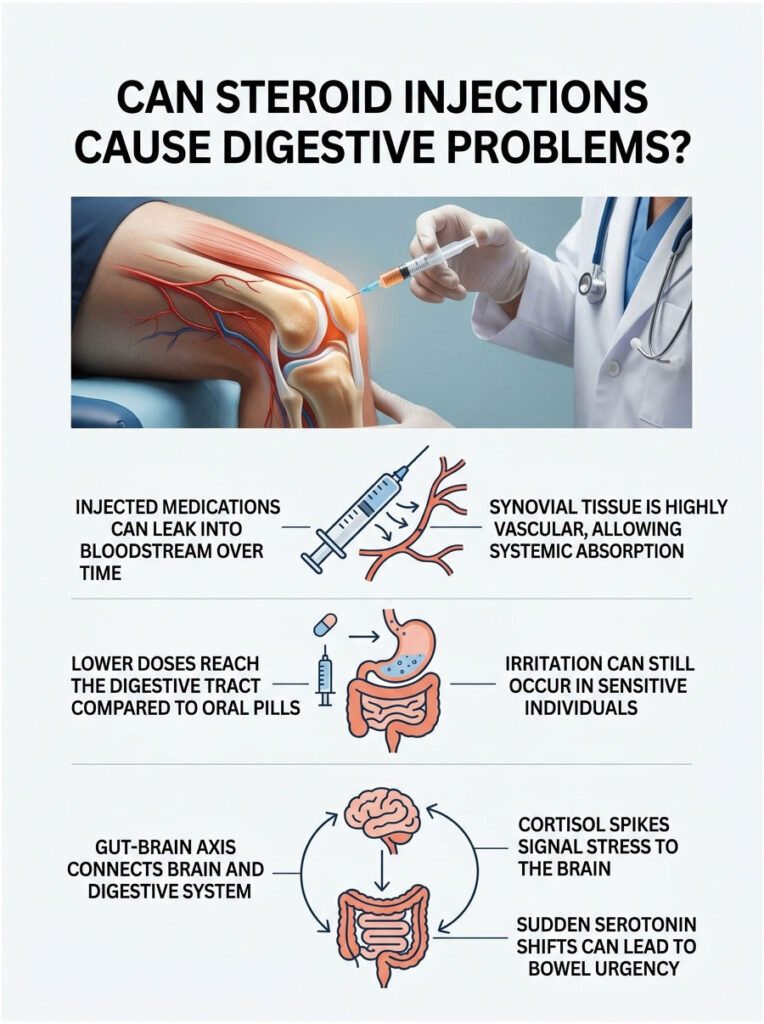
Can Steroid Injections Cause Digestive Problems?
A common patient assumption is that injections bypass the digestive system completely. People think that since they’re not swallowing a pill, their stomach is safe. In reality, that’s not entirely true.
Whether you get an intra-articular shot for a bad knee or an epidural for back pain, the medication doesn’t stay localized forever. The body is an interconnected network of blood vessels and nerves.
Systemic Absorption from Localized Shots
When a doctor injects medication into a joint space, the goal is targeted relief. But the synovial tissue around your joints is highly vascular, packed with tiny blood vessels.
Over the days after the injection, some of that medication slowly leaks into your systemic bloodstream. Once in the blood, it travels throughout the body and reaches the digestive tract. This triggers the same prostaglandin inhibition we see with oral pills. The total dose reaching the stomach is lower than with a pill, but it can still cause irritation in sensitive people.
The Gut-Brain Axis at Work
There’s another fascinating pathway here. Your brain and your enteric nervous system constantly communicate through the vagus nerve, a connection known as the gut-brain axis.
Sudden cortisol spikes from an injection send immediate alarm signals to the brain. The brain reads the spike as acute stress and tells the gut to speed up. This neurological signaling can cause temporary, stress-induced diarrhea without the medication ever physically touching your stomach lining.
The vagus nerve is a superhighway for neurotransmitters. When the injection hits your system, it alters serotonin production. Over 90% of your body’s serotonin is made in the gut, and sudden serotonin shifts directly cause bowel urgency.
Anabolic Steroids and Bowel Movements: The Fitness Risk
So far, we’ve focused on medical glucocorticoids. Now we need to shift to Anabolic-Androgenic Steroids, the synthetic testosterone derivatives used in bodybuilding and fitness communities.
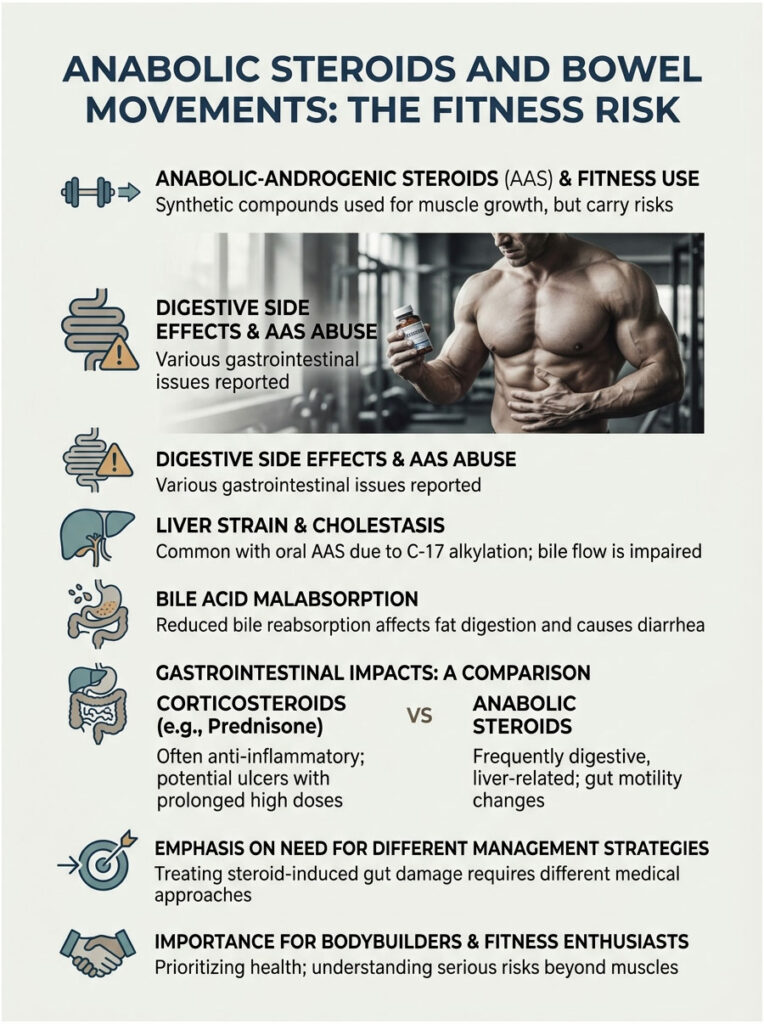
The digestive side effects of anabolic abuse are severe but rarely talked about openly. The mechanisms here are completely different from medical anti-inflammatories. Anabolic drugs put a massive burden on the body’s filtration systems.
Liver Strain and Cholestasis
Oral anabolic steroids are chemically modified to survive the first pass through the liver. That modification makes them highly toxic to liver cells. They place massive strain on liver enzymes and structures.
This strain can cause cholestasis, where the flow of bile from the liver to the digestive tract is reduced or blocked. Bile is essential for breaking down dietary fats. When bile flow is interrupted, undigested fats pass straight into the large intestine, triggering severe, foul-smelling diarrhea.
Bile Acid Malabsorption
Bile acids work as natural laxatives in your digestive system. Normally they help digest fat and then get reabsorbed at the end of the small intestine. Anabolic misuse completely disrupts this delicate flow.
The result is bile acid malabsorption. Excess unabsorbed bile acids spill into the colon, where they stimulate severe water secretion and rapid contractions. This causes chronic, watery diarrhea that is incredibly hard to manage. For many bodybuilders, it shows up as severe IBS-like symptoms.
Post-Cycle Therapy (PCT) and Gut Rebound
The problems don’t stop when the cycle ends. Bodybuilders use Post-Cycle Therapy drugs like Clomid or Nolvadex to restart natural testosterone production. These come with their own digestive side effects.
During PCT, the body experiences massive hormonal swings. Estrogen may spike or crash while testosterone slowly rebuilds. These wild swings wreak havoc on the enteric nervous system. Many users report their worst diarrhea actually happens during PCT, not during the active cycle.
Corticosteroids vs. Anabolic Steroids: GI Impact
| Feature | Medical Corticosteroids | Anabolic-Androgenic Steroids |
|---|---|---|
| Primary Use | Anti-inflammatory, immunosuppression | Muscle growth, hormone replacement |
| Main GI Mechanism | Prostaglandin inhibition, mucosal thinning | Hepatotoxicity, altered bile acids |
| Diarrhea Type | Osmotic or inflammatory | Secretory or malabsorptive |
| GI Risks | Peptic ulcers, GI bleeding, dysbiosis | Cholestasis, severe IBS flares |
| Management | Take with food, probiotics, tapering | Stop anabolics, liver support |
You can’t treat anabolic-related gut damage the same way you treat prednisone-related issues. The root causes need completely different interventions.
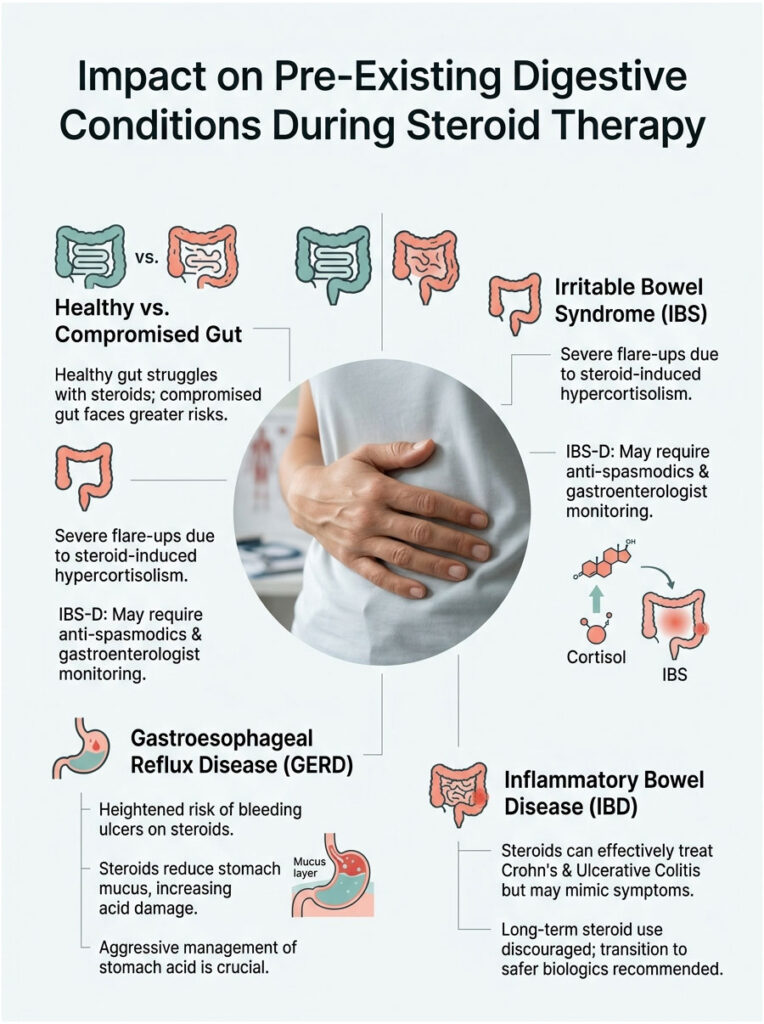
Impact on Pre-Existing Digestive Conditions
A healthy gut will struggle with these medications. A gut that’s already compromised faces an uphill battle. Patients with existing digestive conditions need to be especially careful when starting steroid therapy.
As a pharmacist, I always review medical history before dispensing these drugs. If I see certain chronic illnesses, I flag the prescription for a consultation right away.
IBS Flare-Ups
IBS is a functional disorder marked by a hypersensitive enteric nervous system. Patients with IBS already deal with erratic motility. Adding a synthetic stress hormone is like throwing gasoline on a fire.
The hypercortisolism induced by steroids triggers severe IBS flares. Patients with IBS-D (diarrhea-predominant) see a major spike in bathroom urgency. Standard dietary buffering often isn’t enough. They may need anti-spasmodics to keep the colon calm during therapy, with close monitoring by a gastroenterologist.
GERD and Stomach Acid Damage
GERD involves stomach acid flowing backward into the esophagus. Because steroids reduce protective stomach mucus, that acid becomes much more destructive, damaging the stomach lining and esophageal sphincter.
GERD patients on oral steroids face a high risk of bleeding ulcers. Acid erosion happens much faster when the mucosal barrier is compromised, and that upper GI damage often leads to inflammatory diarrhea further down the tract.
What does this mean for you? If you have GERD, you must aggressively manage stomach acid while on steroids. Doctors will almost always prescribe a proton pump inhibitor alongside to prevent serious internal damage.
The IBD Paradox
Here’s the ultimate paradox. Steroids are frequently used to treat Crohn’s disease and Ulcerative Colitis. They’re highly effective at stopping the autoimmune attack on the intestines.
But once the initial inflammation is suppressed, the drug’s side effects can mimic the disease itself. Patients get confused, wondering if their disease is flaring or if the medication is causing the diarrhea.
This is why long-term use in IBD patients is discouraged. They’re meant as a bridge therapy to calm acute flares, after which patients transition to safer biologics that don’t destroy the mucosal barrier.
How Different Patients Experience Side Effects
Age and metabolism play a massive role in how your body handles these drugs. A growing child processes them very differently than a senior. Side effects show up uniquely across different demographics.
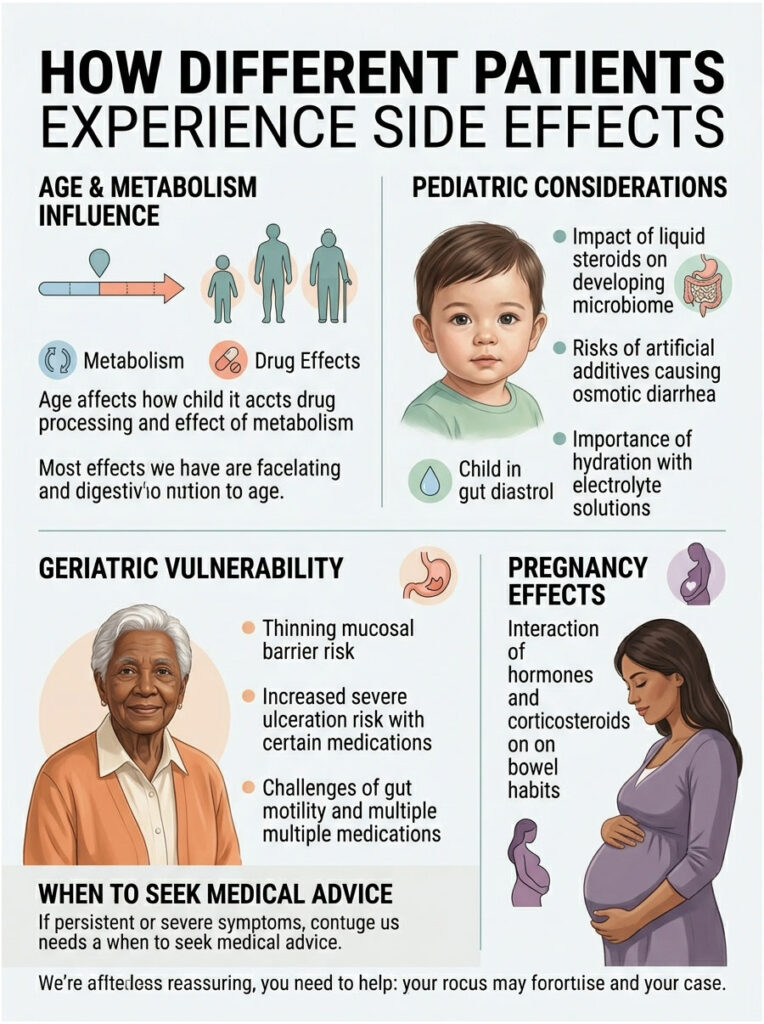
Pediatric Considerations
Children are often prescribed liquid steroids for severe asthma or croup. The pediatric gut is still developing its microbiome. Exposing this fragile ecosystem to powerful immunosuppressants causes immediate dysbiosis.
Liquid formulations are also packed with artificial sweeteners and dyes to mask the bitter taste. These additives are notorious for causing osmotic diarrhea in young kids. Parents must keep their child well-hydrated, since a child can become dangerously dehydrated within hours. I always recommend pediatric electrolyte solutions alongside the prescription.
Geriatric Vulnerability
As we age, our bodies naturally produce less protective stomach mucus. The mucosal barrier in a 70-year-old is much thinner than in a 30-year-old. Adding a prostaglandin inhibitor sharply raises the risk of severe ulceration.
Elderly patients also have slower gut motility at baseline, so when the medication speeds things up, it’s a real shock. They’re prone to severe cramping and loss of bowel control. Elderly patients also tend to take multiple medications, raising the risk of dangerous interactions, particularly with daily aspirin or arthritis NSAIDs.
Pregnancy and the Digestive Tract
Sometimes pregnant women need steroid therapy for severe asthma or autoimmune conditions. Pregnancy already puts pressure on the digestive tract, and pregnancy hormones naturally slow digestion, often causing constipation.
Add synthetic corticosteroids and you create a chaotic battle. The pregnancy hormones are slowing things down while the synthetic cortisol speeds them up. The result is erratic, unpredictable bowel habits. Pregnant women should only use these medications under strict OB supervision, since dehydration from severe diarrhea threatens fetal health and amniotic fluid levels.
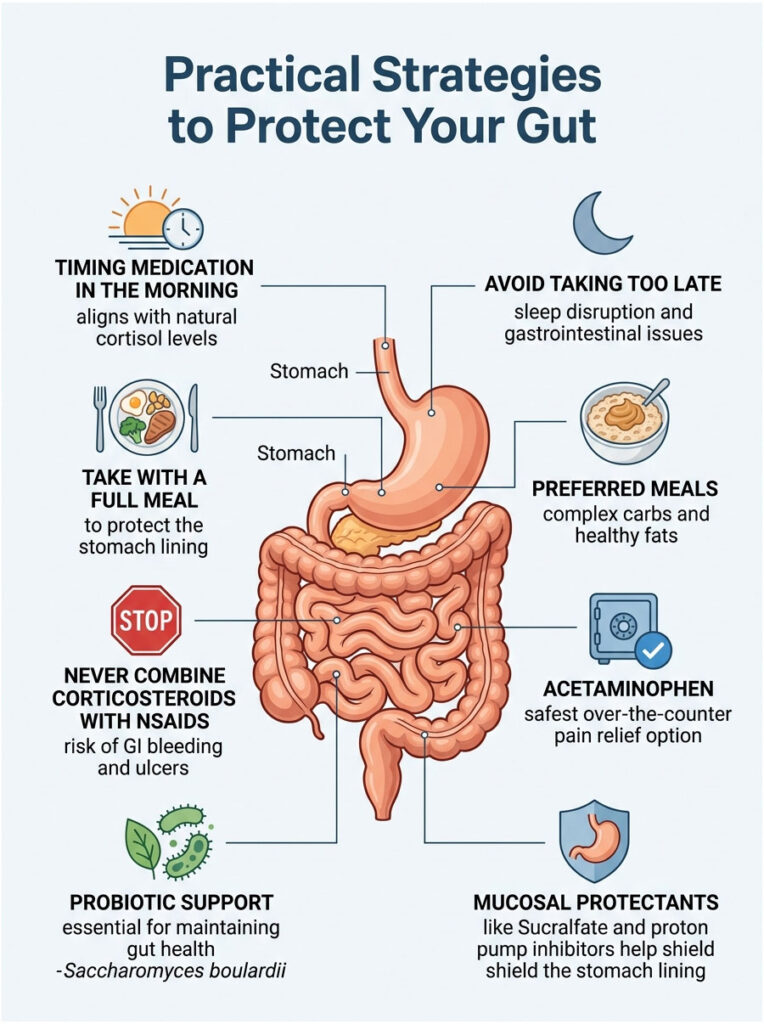
Practical Strategies to Protect Your Gut
Knowing these medications upset your stomach is only half the battle. My main goal as a pharmacist is helping patients prevent the side effects before they start. You don’t have to suffer in silence.
There are highly effective strategies you can use at home. By changing how and when you take your medication, you can create a buffer for your stomach lining.
The Golden Rule: Take It With Food
The golden rule of oral corticosteroids is simple. Never take them on an empty stomach. Taking your pills with a full, dense meal is non-negotiable for protecting your gut.
Food acts as a literal barrier between the drug and the gastric lining. A piece of dry toast isn’t enough. You need a meal with complex carbs and healthy fats to slow the drug’s absorption.
I recommend oatmeal with peanut butter or eggs with whole-wheat toast. The fat and fiber coat the stomach lining and slow the release of the medication into the bloodstream.
Expert Insight: I always tell patients to take their prednisone halfway through breakfast. Eat half your food, take the pill, then finish the meal. This sandwiches the medication inside the food, drastically reducing direct contact with the stomach wall.
Timing and Your Circadian Rhythm
Timing matters more than people realize. Your body naturally produces its highest cortisol levels first thing in the morning. Taking your daily dose in the morning aligns with this natural rhythm.
This alignment cuts down on nighttime stomach upset and helps maintain a more natural digestive rhythm. If you take it too late in the afternoon, it can disrupt sleep and cause nocturnal diarrhea. If your doctor prescribes a split dose, try to take the second one no later than 2:00 PM.
Avoiding Dangerous Drug Interactions
One of the most important warnings I give patients involves over-the-counter pain relievers. You must avoid combining corticosteroids with NSAIDs like Ibuprofen, Naproxen, or Aspirin.
Both drug classes inhibit prostaglandins. Used together, they cause synergistic destruction of the mucosal lining. The combination dramatically raises the risk of GI bleeding, ulcers, and severe diarrhea.
If you need pain relief while on a steroid, acetaminophen is the only safe over-the-counter option. Avoiding NSAIDs is one of your best defenses against serious GI problems.
Probiotics and Mucosal Protectors
To counter dysbiosis, proactive probiotic support is highly recommended. You need strains that can survive a harsh gastric environment.
Saccharomyces boulardii is a beneficial yeast that works exceptionally well. It isn’t destroyed by standard antibiotics and survives the altered gut environment. It helps maintain stool consistency and prevents harmful bacteria from taking over.
For high-risk patients, doctors may prescribe mucosal protectants like Sucralfate or proton pump inhibitors like Omeprazole. These reduce stomach acid and shield the lining.
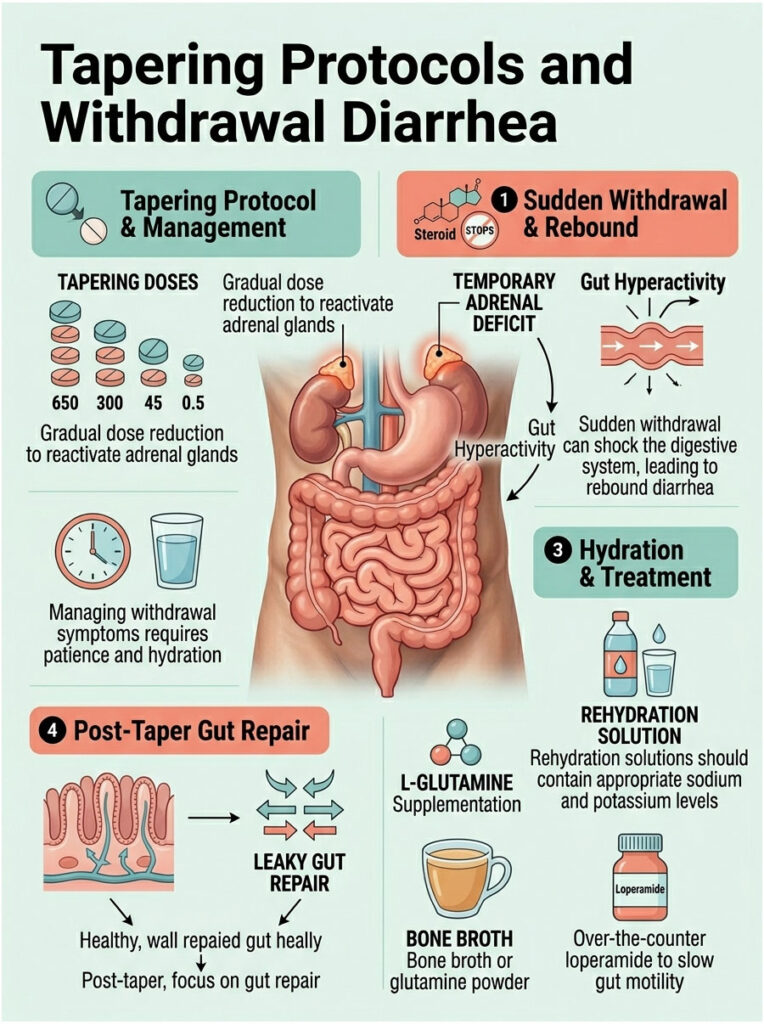
Tapering Protocols and Withdrawal Diarrhea
Getting off these medications is just as complex as starting them. You can’t stop a corticosteroid cold turkey. Your body needs a slow, calculated dose reduction so your natural adrenal glands can wake back up.
During tapering, the digestive system goes through another major transition. The sudden drop in artificial hormones can shock the gut, causing a new wave of bathroom trips.
The Rebound Effect
A taper is a biological necessity. When you take exogenous hormones, your adrenal glands go dormant. As you lower the dose, your body temporarily enters an adrenal deficit, with not enough natural cortisol to go around.
This sudden withdrawal leaves the body scrambling for equilibrium. The GI system reacts with a massive rebound effect. The enteric nervous system becomes hyperactive, causing the intestines to spasm and contract rapidly. The body is essentially throwing a physiological tantrum as it adjusts.
Managing Symptoms After Stopping
Managing diarrhea that hits after stopping the medication takes patience and aggressive hydration. The rebound effect is temporary, usually lasting a few days as natural adrenal function returns to baseline.
Hydration is critical here. You need to replace water and electrolytes lost through rapid bowel movements. Oral rehydration solutions with proper sodium and potassium ratios work best.
Over-the-counter loperamide is generally acceptable during withdrawal. It slows gut motility, directly counteracting the rapid transit time of the taper.
L-Glutamine for Gut Repair
Once you’ve tapered off completely, the focus shifts to repairing the damaged mucosal lining. L-Glutamine is an amino acid that fuels intestinal cells.
Supplementing with L-Glutamine after therapy can dramatically speed up healing. It helps rebuild the tight junctions between cells, reversing medication-induced leaky gut. I often suggest patients add bone broth or a quality glutamine powder to their diet for two weeks after stopping.
When to Seek Emergency Medical Care
Mild to moderate loose stools are a known side effect, but there’s a clear line between a nuisance and a medical emergency. Steroids mask inflammation, which means they can hide early warning signs of serious internal damage.

You need to know which symptoms mean a trip to the ER instead of a phone call to the pharmacy. Ignoring red flags can lead to life-threatening complications.
Signs of Severe GI Bleeding
The most dangerous complication of oral steroid use is severe gastrointestinal bleeding. Because the medication thins the stomach lining, deep ulcers can form and bleed quickly. Watch your stool carefully for color changes.
Critical red flags include black or tarry stools, which indicate digested blood from the upper GI tract. Vomit that looks like dark coffee grounds is another absolute emergency. Severe, unrelenting abdominal pain combined with dizziness or lightheadedness may mean a perforated ulcer. Get to the ER immediately.
Screening for C. diff
Because these drugs suppress your immune system, you’re vulnerable to severe intestinal infections. The most notorious is Clostridioides difficile, or C. diff.
Steroids can mask early inflammatory symptoms of C. diff, making it dangerous. The infection causes severe, foul-smelling, watery diarrhea and devastating colitis. If your symptoms come with high fever, severe cramping, or blood in the stool, you must be screened for C. diff right away. The immunosuppression makes fighting it without targeted antibiotics very difficult.
Recognizing Severe Dehydration
Chronic diarrhea quickly depletes fluids and electrolytes. Dehydration can sneak up on you, especially since the medication may mask normal fatigue signals.
Signs of severe dehydration include extreme dizziness when standing, dark amber urine, inability to produce tears, severely dry mouth, and sudden confusion. If you can’t keep fluids down and watery stools continue, you need IV fluids. Don’t try to tough it out at home. Severe electrolyte imbalances can cause dangerous cardiac arrhythmias.
Key Takeaways
We’ve covered a lot of clinical ground in this guide. The human body is intricate, and adding synthetic hormones disrupts that delicate balance in profound ways.
So, do steroids cause diarrhea? Yes, they absolutely do. It happens through a combination of mucosal irritation, bacterial dysbiosis, and rapid gut motility driven by the enteric nervous system.
The key to surviving your prescription is proactive, intelligent management. Take your medication with dense food to buffer the stomach lining. Absolutely avoid NSAIDs like Ibuprofen to prevent ulcers. Follow your doctor’s tapering schedule carefully to prevent severe rebound symptoms. Add specific probiotic strains and stay focused on hydration to protect your gut microbiome.
If you’re struggling with severe symptoms, don’t suffer in silence. Talk openly with your prescribing physician or clinical pharmacist about any digestive side effects. Adjusting your dose, adding a mucosal protectant, or changing the timing can make a world of difference in your recovery.
Frequently Asked Questions
Does taking prednisone lead to diarrhea or stomach upset?
Yes, prednisone is a potent glucocorticoid that inhibits the production of prostaglandins. Prostaglandins are essential for maintaining the integrity of the gastrointestinal mucosa. When these are suppressed, the stomach and intestinal lining thin out, leading to medication-induced gastritis and loose, unformed stools.
How do corticosteroids affect the gut microbiome?
Synthetic steroids can cause medication-induced dysbiosis by suppressing the gut-associated lymphoid tissue (GALT). This systemic suppression alters the bacterial balance in your intestines within 48 to 72 hours, often allowing opportunistic, pathogenic bacteria to overgrow, which results in osmotic diarrhea.
Can a localized steroid injection, like a joint shot, cause digestive issues?
Even though an injection is localized, systemic absorption occurs as the medication enters the bloodstream through vascular synovial tissues. This spike in circulating cortisol can trigger the gut-brain axis via the vagus nerve, signaling the enteric nervous system to accelerate motility and cause sudden bathroom urgency.
What is the best way to prevent stomach irritation when taking oral steroids?
The golden rule is dietary buffering. You should never take oral steroids on an empty stomach. Taking your dose halfway through a dense meal containing complex carbohydrates and healthy fats—such as oatmeal with peanut butter—creates a physical barrier that protects the gastric lining and slows the drug’s absorption rate.
Is it safe to take Ibuprofen for pain while on a steroid prescription?
As a pharmacist, I strongly advise against this. Both corticosteroids and NSAIDs like Ibuprofen or Naproxen inhibit the COX pathway and prostaglandin synthesis. Combining them creates a synergistic destructive effect on the mucosal barrier, increasing the risk of severe gastrointestinal bleeding and peptic ulcers by four times.
Why do I experience diarrhea while tapering off my steroid dose?
This is known as withdrawal-induced rapid gut motility. As you reduce the dosage, your body enters a temporary state of adrenal deficit. The enteric nervous system often reacts with a rebound effect, causing the intestines to spasm and contract rapidly as they struggle to find equilibrium without the synthetic hormone.
Do anabolic steroids used for bodybuilding cause different digestive problems than medical ones?
Yes, anabolic-androgenic steroids are often hepatotoxic and can induce cholestasis, which impairs bile flow. When bile acid production is disrupted, it leads to bile acid malabsorption. This causes excess bile to spill into the colon, triggering chronic, foul-smelling secretory diarrhea that is distinct from the irritation caused by medical glucocorticoids.
Which probiotics help manage steroid-induced diarrhea?
I frequently recommend Saccharomyces boulardii, a beneficial yeast that is particularly resilient against the chemical shifts caused by immunosuppressant drugs. It helps maintain stool consistency and prevents opportunistic bacteria from taking over the gut during your treatment cycle.
Can steroids make Irritable Bowel Syndrome (IBS) worse?
Yes, the hypercortisolism induced by these medications triggers a chronic stress response in the body. This overstimulates the gut-brain axis, which can lead to severe flare-ups in patients with diarrhea-predominant IBS (IBS-D) due to increased intestinal permeability and accelerated transit times.
When should I be concerned about diarrhea while taking steroids?
You must seek immediate medical intervention if you notice ‘red flag’ symptoms such as black or tarry stools (melena), vomit that resembles coffee grounds, or severe, stabbing abdominal pain. These are indicators of a perforated ulcer or significant gastrointestinal bleeding masked by the drug’s anti-inflammatory properties.
Is Dexamethasone harsher on the stomach than Prednisone?
Dexamethasone is significantly more potent, with a relative potency roughly 25 to 30 times higher than natural hydrocortisone. Because of its long biological half-life and extreme potency, it is more likely to cause severe osmotic imbalances and rapid transit-related diarrhea compared to intermediate-acting steroids like prednisone.
Can taking steroids increase the risk of a C. diff infection?
Yes, because these drugs are immunosuppressive, they can mask the early inflammatory symptoms of a Clostridioides difficile infection. If you experience relentless, watery diarrhea accompanied by a high fever and severe cramping, you should be screened for C. diff immediately as your body’s natural defenses are lowered.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. The information provided by a clinical pharmacist is intended to supplement, not replace, the relationship between a patient and their physician. Always consult a qualified healthcare professional before starting, stopping, or changing a medication regimen, especially regarding corticosteroids and gastrointestinal symptoms.
References
- Mayo Clinic – https://www.mayoclinic.org/drugs-supplements/corticosteroid-oral-route-parenteral-route/side-effects/drg-20070491 – Comprehensive list of oral corticosteroid adverse reactions and GI complications.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – https://www.niddk.nih.gov/health-information/digestive-diseases/drug-induced-liver-injury – Data on how synthetic hormones and drugs impact liver and digestive health.
- Journal of Clinical Medicine – “Gastrointestinal Complications of Glucocorticoid Therapy” – A peer-reviewed study detailing the inhibition of prostaglandins and mucosal damage.
- Cleveland Clinic – https://my.clevelandclinic.org/health/drugs/4812-corticosteroids – Expert insight into the systemic effects of glucocorticoids on the human body.
- American Gastroenterological Association (AGA) – https://gastro.org/practice-guidance/gi-patient-center/ – Guidelines on managing medication-induced dysbiosis and osmotic diarrhea.
- FDA Medication Guides – https://www.accessdata.fda.gov/ – Official prescribing information for Prednisone and Dexamethasone regarding gastrointestinal warnings.