

The word is right there. You can picture the object, you know exactly what you mean, and yet the sound won’t come. For millions of stroke survivors, that gap between a clear mind and a stuck voice is the hardest part of recovery, and the most misunderstood.
Table of Contents
Here’s the truth that matters most: trouble speaking is not the same as trouble thinking. Communication is a skill, and like other skills lost to a stroke, much of it can be rebuilt with the right help and steady effort.
Quick Answer: A stroke can disrupt communication through aphasia (language), dysarthria (muscle control), or apraxia of speech (coordination). About 1 in 3 stroke survivors are affected. Most improvement comes in the first months, but recovery can continue for years with speech-language therapy, daily practice, communication tools, and steady family support. Aphasia does not lower intelligence, and meaningful progress is possible at almost any stage.
At a Glance
- Three different conditions can affect communication after a stroke, and each is treated differently.
- Aphasia changes language, not intelligence; the person is still fully themselves.
- The fastest gains come early, but the brain keeps rewiring for years.
- Speech-language therapy plus daily practice is the single most effective combination.
- Families shape recovery as much as therapists do.
- Starting early and getting enough therapy matters more than any single technique.
How a Stroke Changes Communication
A stroke happens when blood flow to part of the brain is blocked or a vessel bursts, starving brain cells of oxygen. When that damage lands in the brain’s language zones, communication takes the hit.
The effect can feel sudden and disorienting. One day speech is automatic, the next it stalls, and the survivor often understands far more than they can express.
For many survivors, that first realization is the scariest moment of the whole stroke. The body may regain its strength while words lag behind, which is why communication recovery deserves the same attention and effort as learning to walk again.
Which Part of the Brain Controls Language
For most people, language lives mainly in the left hemisphere. Two regions matter most: Broca’s area, which helps produce speech, and Wernicke’s area, which helps understand it.
A stroke on the left side is the usual culprit behind communication loss. Where the damage sits, and how much, shapes whether someone struggles to speak, to understand, or both. Our medical reviewers note that two survivors with the same diagnosis can present very differently depending on the exact area affected.
The right hemisphere matters too. Damage there can flatten the melody and rhythm of speech or blunt the social side of communication, like reading tone or facial expressions, even when the words themselves stay intact.
Why It’s a Skill You Can Rebuild
The brain is not fixed. Through neuroplasticity, healthy regions can take over functions and rebuild the pathways that connect words to meaning. That’s the biology that makes recovery possible.
This matters because communication loss is common, and treatable. According to the National Institute on Deafness and Other Communication Disorders, about one third of stroke survivors have aphasia, and roughly 2 million people in the United States are living with it. Across stroke survivors we work with, the ones who treat speech like daily rehab, not a waiting game, tend to make the steadiest gains.
The Three Communication Conditions After Stroke
People often lump every speech problem under one label, but a stroke can cause three distinct conditions, sometimes more than one at once. Knowing which one you’re dealing with points you toward the right help.
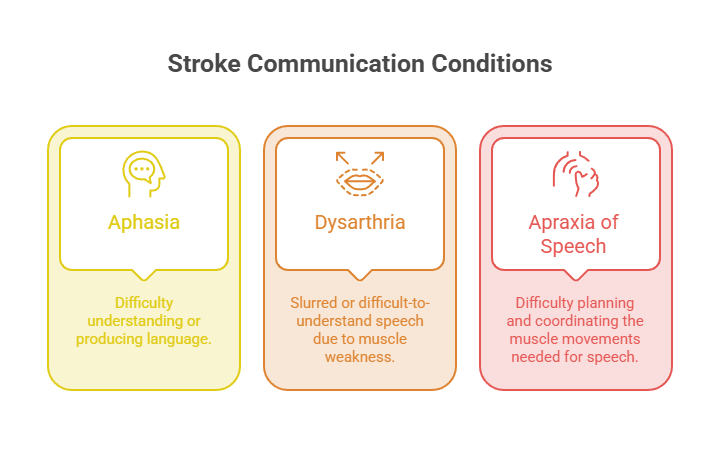
Aphasia (Language)
Aphasia is a language disorder. It can affect speaking, understanding, reading, and writing, in any combination, because the brain’s language processing itself is disrupted.
There are several patterns. Expressive aphasia (often called Broca’s) means the person knows what they want to say but struggles to get words out. Receptive aphasia (Wernicke’s) means speech may flow but make little sense, and understanding others is hard.
Anomic aphasia shows up mainly as word-finding trouble, that maddening tip-of-the-tongue feeling. When damage is widespread, global aphasia can affect every channel at once.
Picture a retired teacher who still solves the crossword in her head but says “the thing for writing” instead of “pen.” Her mind is intact; the label just won’t load. That’s the heart of aphasia, and it explains the one rule that matters most.
The single most important thing to understand is this: aphasia does not affect intelligence. The person is as sharp and aware as ever; the language tool is just jammed.
Diagnosis usually comes from a speech-language pathologist, who tests speaking, listening, reading, and writing to map the specific pattern. That map matters, because therapy for expressive aphasia looks quite different from therapy aimed at receptive aphasia.
Aphasia is also more common than most people realize. The American Speech-Language-Hearing Association reports that roughly 25% to 50% of all strokes result in aphasia, and that risk climbs with age. About 15% of people under 65 experience aphasia after a first ischemic stroke, rising to 43% for those 85 and older.
Dysarthria (Muscle Control)
Dysarthria is a physical problem, not a language one. A stroke can weaken or partly paralyze the muscles of the face, tongue, throat, or breathing, so speech comes out slurred, slow, quiet, or strained.
The person knows the words and can think them clearly. The machinery that turns those words into clear sound is what’s struggling.
Patients commonly ask us why their speech sounds “drunk” when their mind feels sharp. That mismatch is the signature of dysarthria, and targeted muscle and breathing work often helps over time.
Practical strategies help in the meantime. Slowing down, over-articulating each word, facing the listener, and pausing to breathe between phrases can make speech far clearer while the muscles regain strength.
Apraxia of Speech (Coordination)
Apraxia of speech sits between the two. The muscles are strong enough and the language is intact, but the brain can’t reliably sequence the movements needed to form sounds.
The result is groping for sounds and inconsistent errors. A word might come out perfectly one moment and scramble the next. As Franciscan Health’s clinicians describe it, the brain knows the word but doesn’t deliver it correctly to the muscles that control speech.
Therapy leans heavily on repetition and rhythm. Practicing target words slowly, watching the therapist’s mouth, and tapping out syllables all help the brain relearn the sequence, and progress often surprises families who feared the worst.
Cognitive-Communication and Swallowing Overlap
Communication leans on thinking skills too. A stroke can affect attention, memory, and organization, making it hard to follow a conversation, stay on topic, or process quickly. That’s called cognitive-communication difficulty.
Swallowing often gets tangled in here as well. The same muscles and nerves matter, and a speech-language pathologist typically screens for swallowing problems (dysphagia) as part of the picture. In cases reviewed across our diagnostic network, untreated swallowing issues frequently slow speech progress.
For families, this overlap explains a lot. A loved one who seems distracted or forgetful in conversation may be wrestling with attention or processing speed, not disinterest, and naming that difference eases frustration on both sides.
| Condition | What’s Affected | What It Sounds or Feels Like | Common Signs | Main Therapy Focus |
| Aphasia | Language: speaking, understanding, reading, writing | Knowing the thought but losing the word | Word-finding gaps, wrong words, trouble understanding | Relearning language, functional communication |
| Dysarthria | Muscle strength and control for speech | Slurred, slow, quiet, or strained speech | Mumbled words, weak or hoarse voice | Strengthening, breath and articulation drills |
| Apraxia of speech | Coordination and sequencing of speech movements | The mouth won’t make the planned sounds | Groping for sounds, inconsistent errors | Motor-planning practice, structured repetition |
| Cognitive-communication difficulty | Attention, memory, organization | Losing the thread or processing slowly | Off-topic replies, disorganized or delayed speech | Cognitive strategies, structured practice |
What Recovery Really Looks Like
Survivors and families almost always ask the same question first: how long will this take? The honest answer is that timelines vary widely, but the pattern of recovery is fairly predictable.
The First Weeks (Spontaneous Recovery)
The early period after a stroke is when the brain is most adaptable. As swelling settles and healing begins, many people see rapid, sometimes dramatic gains. Clinicians call this the spontaneous recovery phase.
This is also when starting therapy pays off most. Our care team frequently sees that survivors who begin speech work without delay build momentum faster than those who wait.
Months 1 to 6
This stretch is the intensive therapy window, where consistent speech-language sessions and daily home practice do the heavy lifting. Progress can come in bursts, with quiet plateaus in between.
It rarely moves in a straight line. A frustrating week can be followed by a sudden leap, which is why steady effort beats chasing quick results. Tracking small wins, a new word, a clearer sentence, keeps motivation alive through the flat stretches.
Some clinics offer intensive comprehensive aphasia programs that pack many therapy hours into a few short weeks. They aren’t right for everyone, but for motivated survivors they can jump-start gains that ordinary weekly sessions then build on.
Six Months and Beyond
A common myth is that recovery stops at six months or a year. It doesn’t. Neuroplasticity continues well past those marks, and people improve years after a stroke.
The research backs this up. A landmark trial published in The Lancet found that intensive language therapy produced significant improvements in patients with chronic aphasia, six months or more after their stroke. A Cochrane review reached a related conclusion, reporting that functional communication was significantly better in people who received therapy at higher intensity, higher dose, or over a longer duration.
| Measure | US Figure | Source |
| New or recurrent strokes per year | About 795,000 | CDC |
| Americans living with aphasia | About 2 million | NIDCD / NIH |
| New aphasia cases per year | Nearly 180,000 | National Aphasia Association |
| Stroke survivors who develop aphasia | About 1 in 3 (25 to 50% of strokes) | ASHA |
| Americans who have heard of aphasia | About 40% | American Stroke Association |
| Depression rate with post-stroke aphasia | Up to about 70% | Stroke research (Qin et al.) |
The takeaway is hopeful. Recovery is rarely fast or complete, but it is real, and the window stays open far longer than most people assume.
Therapies That Help You Recover
There’s no single cure for aphasia or its cousins, but there are proven ways to rebuild communication. The foundation is professional therapy, layered with daily practice and the right tools.
Speech-Language Therapy (the Foundation)
A speech-language pathologist (SLP) is the specialist who assesses, diagnoses, and treats communication problems at every stage. They map out what’s affected and build a plan around functional, everyday communication.
Good therapy targets real life, not just drills. The goal is helping you order coffee, talk with grandkids, and handle a phone call, not just pass an exercise. Families booking assessments through HealthCareOnTime often ask what to expect, and the honest answer is structured practice plus homework between sessions.
A typical plan starts with a thorough evaluation of speaking, understanding, reading, writing, and swallowing. From there, the SLP sets specific goals, then adjusts as progress comes, so the work always stays a step ahead of current ability.
Sessions may be one-on-one, in a small group, or a mix of both. The right format depends on the person’s goals, stamina, and stage of recovery, and it often shifts as they improve.
Proven Techniques
SLPs draw from several evidence-based methods. Melodic intonation therapy uses melody and rhythm to access language, since singing can be easier than speaking for some people with aphasia.
Constraint-induced language therapy pushes verbal communication while limiting workarounds, to strengthen speech directly. Script training rehearses common conversations, like ordering at a restaurant, so they feel automatic when they count.
Group therapy adds something drills can’t: real interaction with others who understand. It rebuilds confidence, reduces isolation, and turns practice into something closer to ordinary life.
Researchers are also studying brain-stimulation add-ons, such as transcranial magnetic or direct-current stimulation, paired with speech therapy. These remain investigational, so treat them as possible future tools rather than standard care, and lean on your SLP’s guidance about what’s appropriate.
AAC and Communication Apps
Augmentative and alternative communication (AAC) tools bridge the gap while speech recovers, and can speed recovery itself. These range from simple picture boards to speech-generating devices that turn taps or typing into spoken words.
Apps have made daily practice far more accessible. Tools like Constant Therapy, Lingraphica, and Tactus Therapy offer guided exercises with progress tracking, often adjusting difficulty as skills improve. Research suggests AAC use can even improve spoken language over time, not just replace it.
Low-tech options matter just as much. A laminated card with common needs, a notebook for writing or drawing, and a phone’s notes app can all carry a conversation when words fail, and they cost almost nothing to set up.
Treating Swallowing Too
Because speech and swallowing share muscles and nerves, an SLP often addresses both. Strengthening and coordinating those muscles supports clearer speech and safer eating.
Our lab partners report that survivors progress more smoothly when swallowing problems are caught and treated early rather than left to linger. It’s one reason a full SLP evaluation looks beyond speech alone.
Daily Strategies and At-Home Exercises
Therapy sessions are only part of the work. What happens at home, every day, often determines how far recovery goes.
Strategies for the Survivor
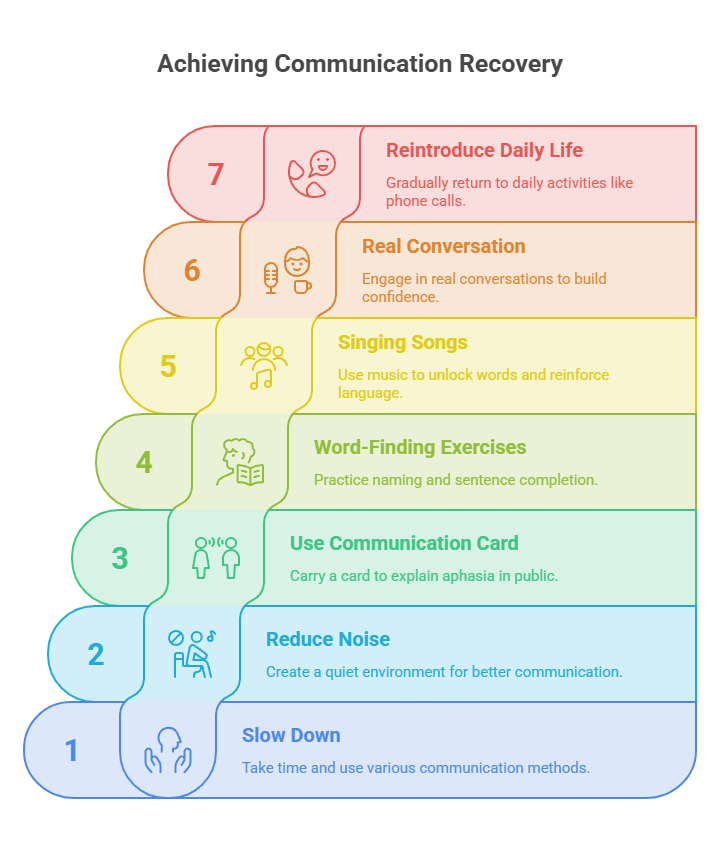
Slowing down is the first move. Take your time, and use whatever channels help: gestures, drawing, pointing, writing a key word, or a picture book.
Set yourself up for success. Cut background noise, talk in quieter spaces, and start conversations one-on-one with someone you trust before tackling groups.
It also helps to carry a small card explaining your aphasia, plus contact information, in case communication breaks down in public. A quick written note can turn a frustrating moment with a stranger into a manageable one.
Word-Finding and Speech Exercises
Simple, repeatable drills build the “word-finding muscles.” Naming exercises work well: list every fruit, city, or animal you can think of in a minute.
Sentence completion (“A picture is worth a thousand ___”) and reading aloud both reinforce language. Singing familiar songs taps a different brain route and can unlock words that won’t come in plain speech.
Keep sessions short and frequent rather than long and rare. Ten focused minutes several times a day usually beats one exhausting hour, and the consistency is what rewires the brain.
A simple weekly rhythm helps: pick two or three target activities, repeat them daily, and add a harder version once they feel easy. Writing the plan on a fridge calendar turns good intentions into a habit the whole household can support.
Building Confidence Through Real Conversation
Practice has to leave the worksheet. Real conversation, even short and imperfect, is one of the strongest forms of therapy.
The American Stroke Association puts it plainly: socializing is one of the best ways to maximize recovery. Start small, celebrate effort over perfection, and widen your circle as confidence grows.
Easing Back Into Daily Life
Communication touches everything: phone calls, appointments, driving directions, work. Reintroduce these gradually, starting with low-pressure versions, like calling a familiar friend before tackling a customer-service line.
Some survivors return to work or driving with accommodations; others adjust their roles for a while. An SLP and the wider care team can advise on timing, since pushing too fast can frustrate while waiting too long can deepen isolation.
| What You Notice | What It May Mean | What to Try |
| Knows the idea but can’t find the word | Anomic or expressive aphasia | Offer choices, allow gestures or writing, give extra time |
| Slurred speech but accurate words | Dysarthria | Slow the pace, face the person, reduce background noise |
| Groping, inconsistent sound errors | Apraxia of speech | Repetition practice and slow modeling with an SLP |
| Understands little of what’s said | Receptive aphasia | Short sentences, yes/no questions, visual cues |
| Frustration, withdrawal, low mood | Post-stroke depression risk | Support groups, a mental-health referral, keep socializing |
| Little change after weeks of home practice | Under-dosed therapy | Ask about more intensive sessions or teletherapy |
How Families and Caregivers Can Help
Communication takes two people, so families are not bystanders in recovery. The way loved ones talk, and listen, can speed progress or quietly stall it.
Communication Do’s
Face the person, make eye contact, and use normal adult language. Keep sentences to single thoughts, ask questions that can be answered yes or no, and offer a few clear choices when things get complex.
Give time, far more than feels natural. MedlinePlus advises that you keep distractions and noise down and make eye contact when talking, then confirm what was understood before moving on.
A simple example: instead of “What do you want for lunch?”, try “Soup or sandwich?” while showing both. Narrowing the choices takes pressure off word-finding and keeps the person in control of the answer.
Speech-language pathologists can teach families directly through communication-partner training. Learning a few proven techniques, supported conversation, gentle cueing, and patience, often improves everyday exchanges as much as the survivor’s own practice does.
Communication Don’ts
Don’t shout; unless there’s also a hearing problem, volume won’t help and can feel demeaning. Don’t finish their sentences or rush them, even with good intentions.
And don’t pretend to understand when you don’t. Patients we serve consistently say that being quietly “managed” is more isolating than an honest “let’s try that again.”
Protecting Mental Health
The emotional toll is real and often hidden. Depression is far more common among survivors with aphasia, with post-stroke aphasia patients showing roughly a 70% depression rate, partly because communicating that distress is itself so hard.
Watch for withdrawal, and keep the person connected. Support groups, where survivors and families swap strategies, can lift both mood and motivation. The link between staying social and recovering well runs in both directions.
When and Where to Get Help
The earlier communication therapy starts, the better, and the more consistently it continues, the more it tends to pay off. Two practical things make the biggest difference: starting promptly and getting enough of it.
Start Early, Keep Going
Ask for a speech-language evaluation as soon as the medical team allows, often during the hospital stay or right after. Then push for an adequate dose, since the evidence favors intensity and duration.
If progress stalls at home, that’s a signal to ask about more frequent sessions, not to give up. Our care team frequently sees plateaus break once therapy intensity increases.
It also helps to keep a running list of questions for the care team, from therapy frequency to home-program ideas. Survivors and families who advocate clearly tend to get more tailored, more useful care.
Coverage and Access
Speech-language therapy after a stroke is often covered by Medicare and many insurance plans, though specifics depend on your plan, diagnosis, and setting. Care may happen in outpatient clinics, at home through home-health services, or remotely by teletherapy.
Teletherapy in particular has widened access for people who can’t easily travel, letting survivors practice with a licensed SLP from home. Coverage rules change and vary by individual, so confirm details with your provider and insurer. HealthCareOnTime is not a substitute for that personalized guidance, but knowing the options helps you ask the right questions.
Build a Support Network
Recovery is easier with company. National organizations like the National Aphasia Association and the American Stroke Association list support groups, aphasia-friendly programs, and family resources across the country.
Connecting with other survivors normalizes the ups and downs and surfaces practical tips a clinic visit can miss. June, National Aphasia Awareness Month, is a good time to find local events, though support exists year-round.
Frequently Asked Questions
How long does it take to recover communication skills after a stroke?
Recovery varies widely. The fastest gains usually come in the first weeks to six months, but improvement can continue for years with ongoing therapy and practice. Timelines depend on stroke size, location, severity, age, and how early and intensively therapy begins.
Can you fully recover from aphasia?
Some people, especially with mild aphasia, recover fully, sometimes spontaneously in the early days. Many others regain significant communication without reaching their exact pre-stroke level. Any degree of recovery improves quality of life, and progress remains possible long after the stroke.
Does aphasia mean a loss of intelligence?
No. Aphasia affects language, not intelligence. The person thinks, reasons, and feels exactly as before; they simply have trouble expressing or understanding words. Treating someone with aphasia as less capable is both inaccurate and discouraging, so use normal adult language and give them time.
What’s the difference between aphasia, dysarthria, and apraxia of speech?
Aphasia is a language problem affecting words and meaning. Dysarthria is muscle weakness that slurs speech. Apraxia of speech is a coordination problem where the brain can’t sequence speech movements. A stroke can cause one or several at once, and each calls for different therapy.
How can I help a loved one with aphasia communicate?
Face them, use short sentences and yes/no questions, cut background noise, and give plenty of time. Offer pictures, writing, or gestures as backups. Don’t shout, finish their sentences, or pretend to understand. Confirm what they mean, and keep them socially engaged rather than isolated.
Can speech come back years after a stroke?
Yes. Neuroplasticity continues well beyond the first year, and studies show people with chronic aphasia improve with intensive therapy six months or more after a stroke. Consistent practice and continued speech-language therapy can produce meaningful gains years later.
What speech exercises can be done at home?
Try naming drills (list items in a category), sentence completion, reading aloud, and describing photos. Singing familiar songs can help when speech stalls. Communication apps offer guided practice with progress tracking. Daily, consistent repetition matters more than long, occasional sessions.
Are communication apps and AAC devices effective?
Yes. Augmentative and alternative communication tools, from picture boards to speech-generating apps, help people communicate now and can improve spoken language over time. Apps like Constant Therapy and Lingraphica provide structured practice. An SLP can recommend the right tool for the person’s needs.
Why does my family member say the wrong word?
This is a classic aphasia symptom. The brain’s link between meaning and words is disrupted, so a person may say “cat” while meaning “dog,” or “yes” while meaning “no.” They know what they intend; the wrong word slips out. Gentle clarification and patience help.
Does Medicare or insurance cover speech therapy after a stroke?
Often, yes. Medicare and many private plans cover medically necessary speech-language therapy after a stroke, though coverage limits, settings, and copays vary by plan and diagnosis. Confirm specifics with your insurer and provider, and ask about outpatient, home-health, and teletherapy options.
Is more frequent therapy better?
Generally, evidence favors higher intensity, higher dose, or longer duration of speech-language therapy for better functional communication. That said, very intensive schedules don’t suit everyone. The right plan balances what the research supports with what the survivor can realistically sustain.
What should I avoid saying to someone with aphasia?
Avoid shouting, talking down to them, or using childish language. Don’t rush them or finish their sentences, and never pretend to understand when you don’t. Skip “just relax” type pressure. Instead, slow down, offer choices, and treat them as the capable adult they still are.
Disclaimer: This article is for general information and education only. It isn’t a substitute for professional medical advice, diagnosis, or treatment. Always consult a physician or a licensed speech-language pathologist about communication problems after a stroke, and call 911 immediately if you notice new stroke signs such as face drooping, arm weakness, or slurred speech.
References
- Aphasia, National Institute on Deafness and Other Communication Disorders (NIH)
- Aphasia Practice Portal, American Speech-Language-Hearing Association (ASHA)
- Aphasia: Be in the Know, American Stroke Association
- The Incidence of Aphasia, National Aphasia Association
- Speech and language therapy for aphasia following stroke, Cochrane Review
- Communicating with someone with aphasia, MedlinePlus (NIH)
- Prevalence and Impact of Aphasia among Patients with Acute Ischemic Stroke





