

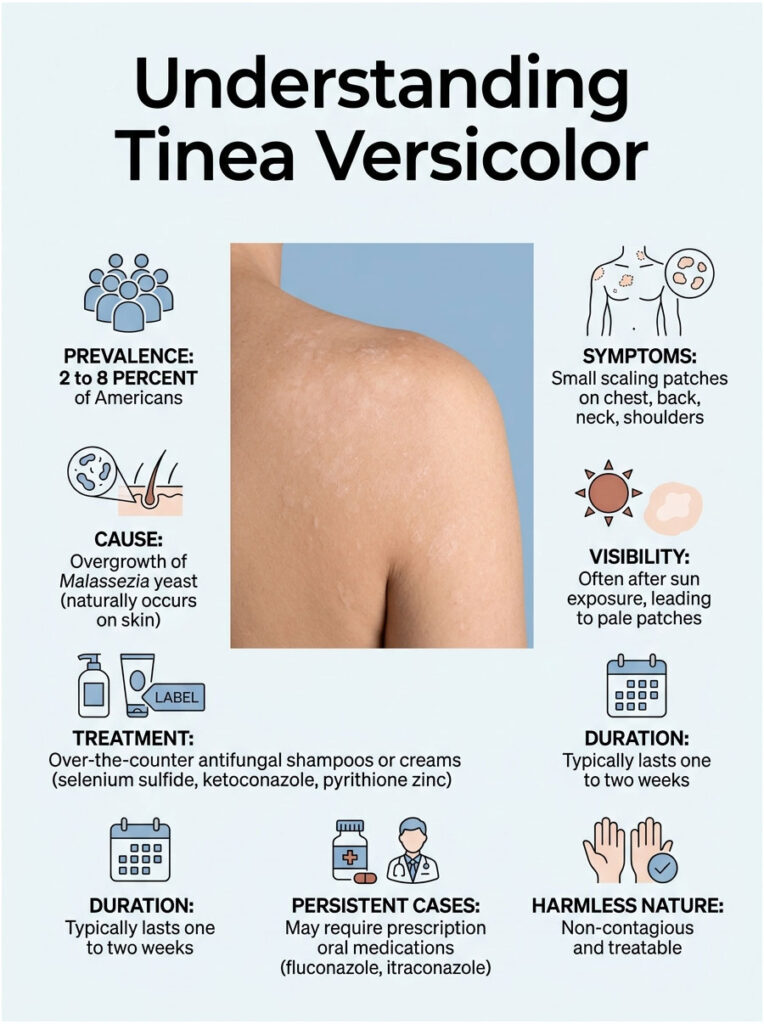
Roughly 2 to 8 percent of Americans will deal with tinea versicolor at some point, and most of them won’t notice it until a beach vacation. The tan comes in, the patches stay pale, and suddenly your back looks like a connect-the-dots puzzle. It is harmless, treatable, and confusing in equal measure. The good news: a five-dollar bottle from any US drugstore clears most cases.
Table of Contents
Quick Answer: Tinea versicolor is a common, non-contagious fungal skin infection caused by an overgrowth of Malassezia yeast that already lives on your skin. It shows up as small, lightly scaling patches that are paler, pinker, or darker than the surrounding skin, usually on the chest, back, neck, and shoulders. Treatment is straightforward: antifungal shampoos or creams containing selenium sulfide, ketoconazole, or pyrithione zinc, applied daily for one to two weeks. Stubborn or widespread cases respond to prescription oral fluconazole or itraconazole.
At a Glance
- Tinea versicolor (also called pityriasis versicolor) is a yeast overgrowth, not a contagious ringworm-style infection
- It is most common in teens and adults aged 15 to 24, when oil glands are most active
- Patches can be lighter, darker, pink, or tan depending on your natural skin tone
- OTC selenium sulfide or ketoconazole shampoo clears about 80 percent of cases
- Skin color usually evens out within a few weeks to several months after the yeast is gone
- Recurrence is the norm, not the exception, in warm and humid US climates
- See a dermatologist if it spreads, recurs frequently, or you cannot tell it apart from vitiligo
What Tinea Versicolor Actually Is
Tinea versicolor is a superficial fungal skin infection caused by a yeast called Malassezia. That yeast already lives on almost every adult’s skin without causing any trouble. When conditions tip in its favor (heat, sweat, oil, hormonal changes), the yeast switches into an overgrowth form and produces compounds that mess with your skin’s pigment.
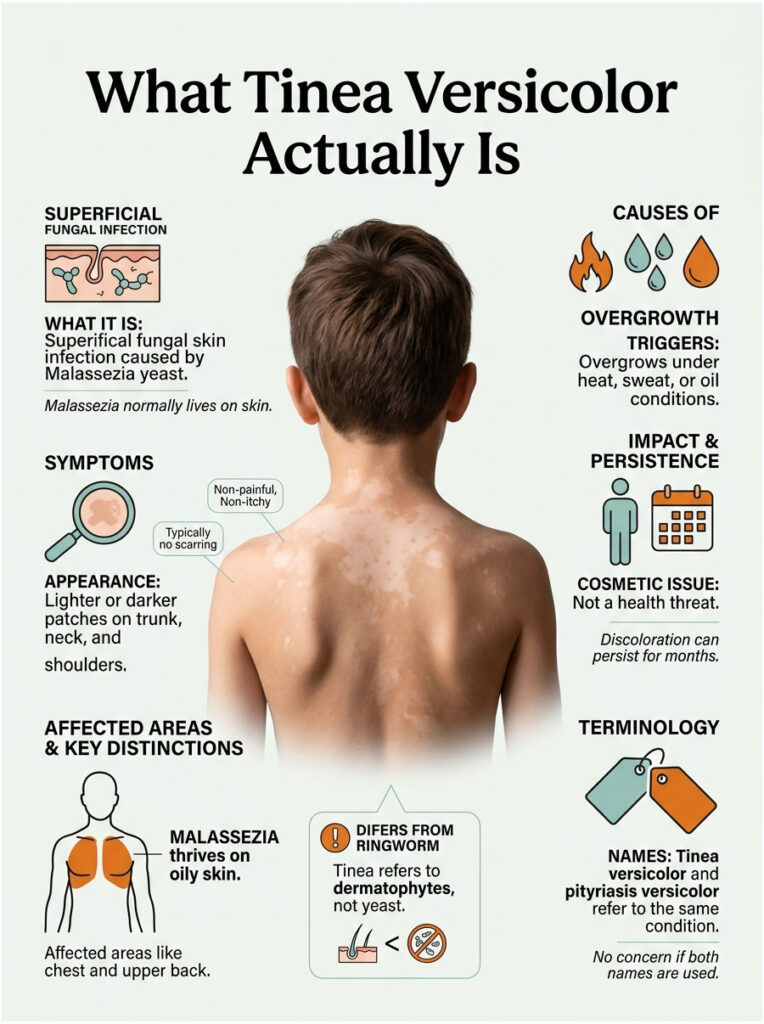
The result is a patchwork of lighter or darker spots, usually on the trunk, neck, shoulders, and upper arms. The patches do not hurt, rarely itch, and never scar. They just look strange.
Patients commonly ask our dermatology reviewers whether tinea versicolor is dangerous. The honest answer is no. It is a cosmetic nuisance, not a health threat, but the visible pigment changes can stick around for months after the yeast itself is dead.
The Yeast Behind It
Malassezia is a genus of lipid-loving yeasts. They feed on the oils your sebaceous glands produce, which is why tinea versicolor concentrates on oily skin zones (chest, upper back, shoulders) and rarely shows up on dry areas like your shins or forearms.
Two species do most of the work in US cases: Malassezia furfur and Malassezia globosa. The yeast itself is normal. The mycelial (filament-producing) form it switches into during a flare is what causes the visible rash.
Why It Is Not “Ringworm” Despite the “Tinea” Name
The word “tinea” is a clinical hangover from when dermatologists thought all scaly fungal infections were related. Real tinea infections (tinea corporis, tinea pedis, tinea cruris) come from dermatophytes, a totally different fungal family that does cause contagious ringworm.
Tinea versicolor is caused by a yeast, not a dermatophyte. That single difference explains why it does not spread between people, does not respond to ringworm-only antifungals, and behaves nothing like athlete’s foot.
Tinea Versicolor vs Pityriasis Versicolor
These are two names for the same condition. Most dermatology textbooks prefer pityriasis versicolor because it is technically more accurate. Patient-facing sites and search results still favor tinea versicolor.
If your dermatologist writes “pityriasis versicolor” on your visit summary, do not panic. You have not been re-diagnosed with anything new.
How Tinea Versicolor Looks on Different Skin Tones
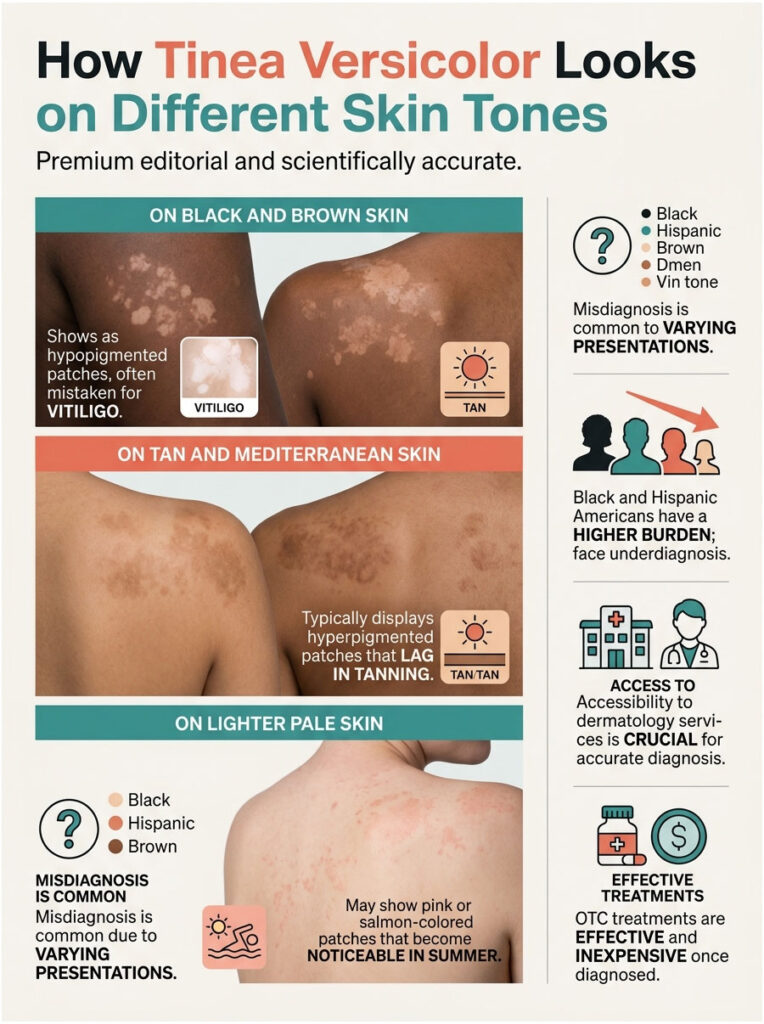
The “versicolor” in the name means “many colors,” and that is not marketing. The patches can look pale, pink, tan, or brown depending on whether the affected skin is interacting with sun exposure and your baseline pigment. This is the single biggest source of misdiagnosis, especially across the wide range of US skin tones.
On Black and Brown Skin
Tinea versicolor most often shows up as hypopigmented (lighter than baseline) patches on Black and Brown skin. The contrast can be dramatic and often prompts worry about vitiligo or post-inflammatory hypopigmentation.
In cases reviewed across our diagnostic network, the visible color drop on darker skin is one of the most common reasons patients first book a dermatology visit. Wood’s lamp examination and a quick KOH scraping settle the question fast.
On Tan and Mediterranean Skin
Patches more often look subtly darker (hyperpigmented) than baseline, with a brown or tan-brown tint. They become obvious in summer when the surrounding skin tans further and the affected zones lag behind.
On Lighter Pale Skin
The patches often look pink, salmon, or a slightly warmer tan than the rest of your trunk. People with naturally pale skin who avoid sun exposure may not notice the infection at all until the patches start to flake during a hot summer.
Skin-of-Color Burden in the US
Recent data from the NIH All of Us Research Program show that Black and Hispanic Americans carry a higher overall burden of pityriasis versicolor. Uninsured patients, lower-income households, and people with limited access to dermatology face higher rates of underdiagnosis. Our dermatology reviewers consistently flag this as a fixable gap, since OTC treatments are inexpensive once the diagnosis is made.
What Tinea Versicolor Looks and Feels Like
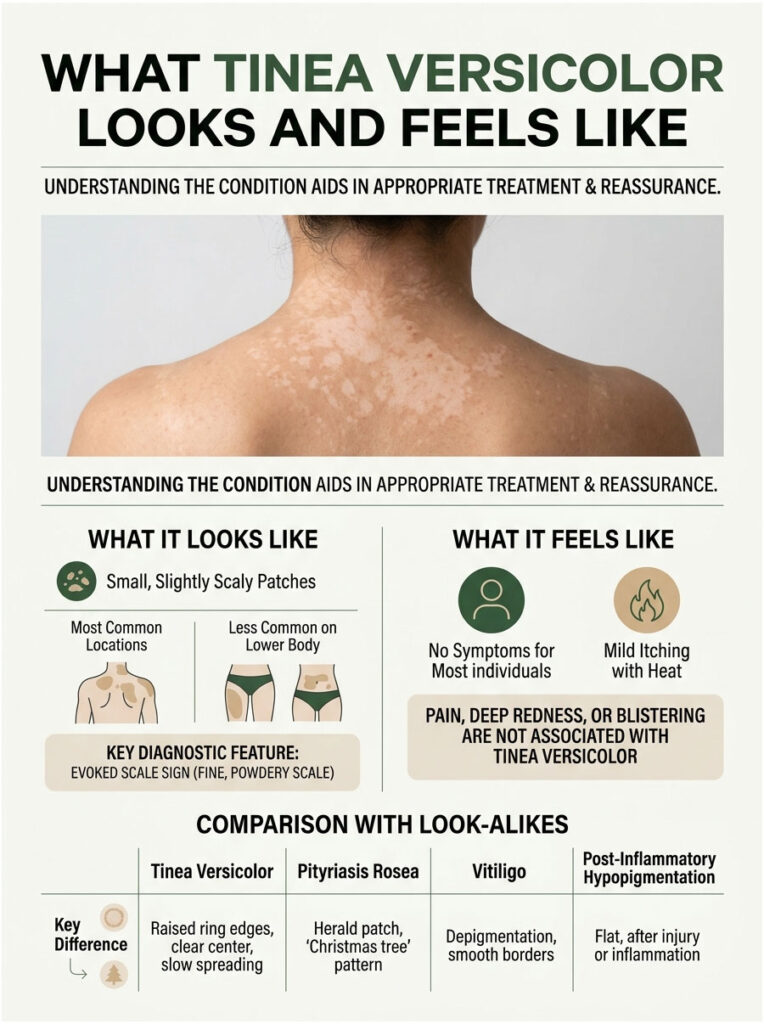
Tinea versicolor has a signature look once you have seen it. The patches are usually small (less than half an inch across at first), oval or round, slightly scaly when scratched gently with a fingernail, and clustered rather than isolated.
Classic Patches: Where They Show Up
The infection prefers areas with the highest concentration of oil glands. In US adults that translates to the upper back, chest, sides of the neck, shoulders, and upper arms. In teens, it can extend onto the face, particularly the temples and hairline.
Lower-body involvement (thighs, abdomen below the navel) is uncommon in adults. When tinea versicolor does spread that far, dermatologists often suspect an immune system issue or a long-untreated recurrent case.
Itch, Scale, and Other Sensations
Most people feel nothing. Some report mild itching, especially when sweating or after a hot shower. A gentle fingernail scrape across a patch usually reveals fine, powdery scale (clinicians call this the “evoked scale sign”), which is one of the diagnostic giveaways.
Pain, deep redness, blistering, or rapid spreading are not features of tinea versicolor. If you see those, you are dealing with something else.
Table 1: Tinea Versicolor vs Common Look-Alikes
| Condition | Cause | Typical Color | Itch | Scale | Distribution |
| Tinea versicolor | Malassezia yeast overgrowth | Pale, pink, tan, or brown patches | Mild or none | Fine, powdery, scratch-revealed | Chest, back, neck, shoulders |
| Vitiligo | Autoimmune pigment loss | Sharply demarcated milky white | None | No scale | Hands, face, body folds, symmetrical |
| Pityriasis alba | Mild eczema variant | Faint pale patches | Mild | Fine, dry | Face, upper arms (mostly kids) |
| Post-inflammatory hypopigmentation | After eczema, burn, or trauma | Light spots tracking prior injury | Variable | None | Wherever the injury occurred |
| Seborrheic dermatitis | Malassezia + inflammation | Pink with greasy yellow scale | Often itchy | Greasy, yellow | Scalp, eyebrows, nose folds, chest |
| Ringworm (tinea corporis) | Dermatophyte fungus | Red ring with clearer center | Often itchy | Ring-edge scale | Any body area; contagious |
| Eczema (atopic dermatitis) | Skin barrier dysfunction | Red, sometimes weepy | Intensely itchy | Dry or cracked | Elbows, knees, hands, neck folds |
What Causes It and Who Gets It
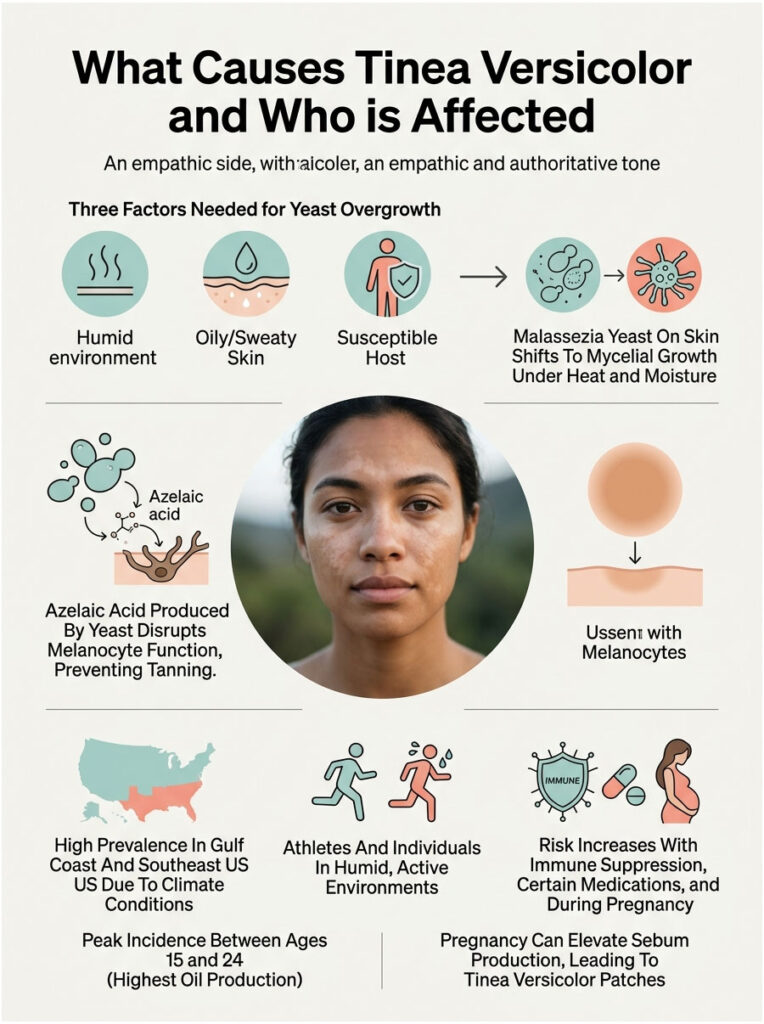
Three factors have to line up for the resident yeast to flip into overgrowth mode: a humid environment, oily or sweaty skin, and a susceptible host. Take away any one of them and the yeast stays quiet.
The Fungal Overgrowth Trigger
Your skin always carries Malassezia in its yeast form. When sebum (skin oil), sweat, and warmth cluster together, the yeast shifts into mycelial (thread-like) growth and produces azelaic acid, which interferes with melanocytes (the cells that make pigment).
That is why the patches don’t tan. The pigment-producing cells are temporarily disabled wherever the active yeast colonizes.
Heat, Humidity, and Sweat (US Geography Matters)
If you live anywhere from the Gulf Coast through the Southeast (Florida, Louisiana, Texas, Georgia, the Carolinas, Mississippi, Alabama), you have built-in conditions for tinea versicolor. Per Medscape data, US prevalence climbs in regions with sustained high temperature and humidity.
Athletes, military personnel stationed in tropical climates, hot-yoga regulars, and anyone whose workout clothes stay damp for hours show up more often in dermatology clinics with active cases.
Hormones, Oily Skin, and Adolescence
The peak incidence in the US falls between ages 15 and 24, the same window when sebaceous gland activity is at its lifetime high. That is not a coincidence. More sebum means more food for the yeast.
This is also why tinea versicolor is rare in young children (before puberty) and uncommon in adults over 65, when oil production tapers.
Immune System, Medications, and Pregnancy
Anything that suppresses your immune system or alters skin oil production raises risk. The main triggers our medical reviewers see flagged in patient histories include systemic corticosteroids, chemotherapy, organ transplant medications, uncontrolled diabetes, HIV, and pregnancy.
Pregnancy increases progesterone levels, which can boost sebum production and humidity at the skin surface. That combination explains why some women see their first tinea versicolor patches during the second or third trimester.
How Doctors Diagnose Tinea Versicolor
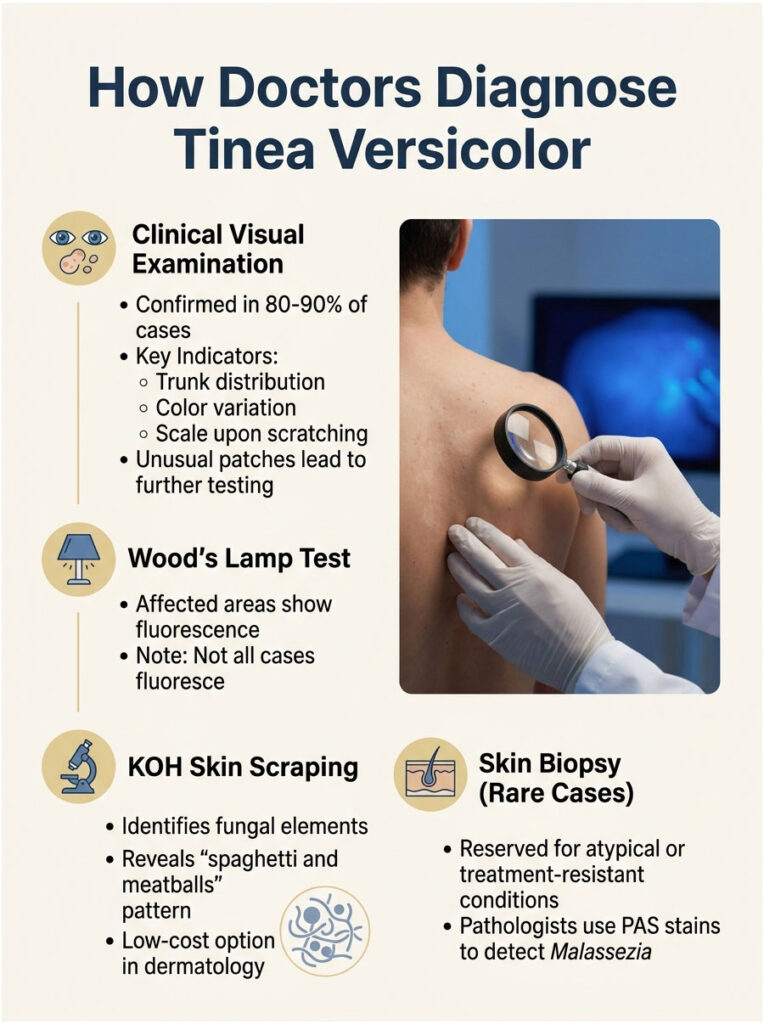
Most dermatologists diagnose tinea versicolor in under a minute. The visual pattern is distinctive enough that the diagnosis is usually clinical, with confirmation tests reserved for atypical cases.
The Visual Exam
A dermatologist looks at the distribution (trunk-dominant), the color variation, and the scratch-revealed scale. That alone confirms the diagnosis in roughly 80 to 90 percent of cases seen in US dermatology clinics.
If the patches are in unusual places (face only, palms, soles) or you have systemic symptoms, the workup gets more thorough.
Wood’s Lamp (UV Light) Test
A Wood’s lamp is a handheld ultraviolet light. When shined on tinea versicolor patches in a darkened room, the affected areas often fluoresce a pale yellow or coppery orange. The test is fast, painless, and free in most clinic visits.
Not every case fluoresces (estimates suggest only about a third do), so a negative Wood’s lamp result does not rule out tinea versicolor.
KOH Skin Scraping and Microscopy
When the visual diagnosis is uncertain, dermatologists scrape a tiny amount of surface scale onto a glass slide, add potassium hydroxide solution, and view it under a microscope. The classic finding is the “spaghetti and meatballs” pattern: short fungal filaments mixed with round yeast cells.
In tests booked through HealthCareOnTime’s lab partners, the KOH scraping is one of the lowest-cost diagnostic confirmations available in dermatology, typically running well under standard dermatology copays in US insurance plans.
When a Biopsy Is Needed
Skin biopsies are rare for tinea versicolor and are reserved for cases that mimic other conditions or refuse to respond to standard treatment. A pathologist using a periodic acid-Schiff (PAS) stain can spot Malassezia in tissue sections clearly.
How to Treat Tinea Versicolor
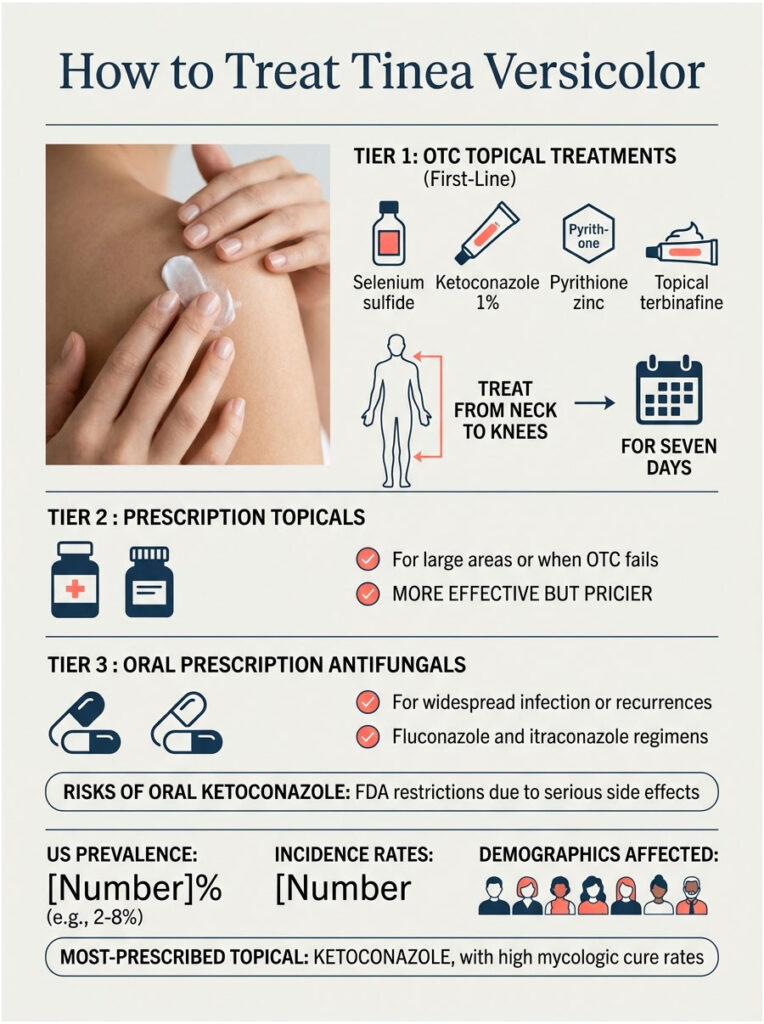
Treatment falls into three tiers: OTC topical, prescription topical, and oral prescription. Most US adults can clear their infection without ever seeing a dermatologist, but knowing when to escalate saves time and money.
First-Line OTC Treatments
The four ingredients with the strongest US dermatology backing for self-treatment are selenium sulfide (Selsun Blue, Head & Shoulders Clinical Strength), ketoconazole 1 percent (Nizoral A-D shampoo), pyrithione zinc (most dandruff shampoos), and topical terbinafine (Lamisil AT cream or spray).
All four are sold at every CVS, Walgreens, Walmart, and Target in the US for less than 20 dollars. Selenium sulfide 1 percent (the OTC strength) and pyrithione zinc shampoos typically run 5 to 10 dollars per bottle.
Step-by-Step OTC Application Protocol
The trick that most people miss is that these products only work if they sit on the skin long enough. Lathering and rinsing immediately does nothing.
A proven seven-day protocol our reviewers recommend looks like this:
- Shower as usual and pat skin damp
- Apply selenium sulfide or ketoconazole shampoo to all affected areas plus a generous margin
- Lather lightly and leave on for 10 minutes (set a timer; do not skip this step)
- Rinse thoroughly
- Repeat once daily for 7 to 14 consecutive days
- After clearance, drop to once weekly for one month
- Then shift to once monthly maintenance through the warm season
Treating from the neck down to the knees (even on apparently clear skin) catches subclinical colonies that would otherwise restart the infection within weeks.
Prescription Topicals
When OTC fails or the infection covers large areas, dermatologists move up to prescription-strength options:
- Ketoconazole 2 percent cream or shampoo
- Ciclopirox 0.77 percent cream, gel, or shampoo (brand names Loprox, Penlac)
- Econazole 1 percent cream
- Sertaconazole 2 percent cream
- Terbinafine 1 percent solution (twice daily)
These are more expensive (often 30 to 80 dollars without insurance), but they cut treatment time significantly and improve clearance rates in stubborn cases.
Oral Antifungals and When They Are Used
Oral medications are reserved for widespread infection, frequent recurrences, or cases that fail topical therapy. The two workhorses are fluconazole (Diflucan) and itraconazole (Sporanox, Onmel).
Typical regimens look like fluconazole 300 mg once weekly for two to four weeks, or itraconazole 200 mg daily for five to seven days. Both require liver-function monitoring in some patients and have drug-interaction profiles your doctor will check against your full medication list.
Why Oral Ketoconazole Is No Longer Prescribed
This one is worth knowing. The FDA placed serious restrictions on oral ketoconazole in 2013 because of fatal liver injuries, adrenal gland problems, and dangerous drug interactions. Oral ketoconazole is now contraindicated for tinea versicolor and most other skin fungal infections.
Topical ketoconazole (cream, shampoo, foam) remains safe, effective, and widely used. The restriction applies only to the oral form.
Table 2: US Tinea Versicolor Statistics and Treatment Data
| Metric | US Data | Source |
| US prevalence | 2 to 8 percent of the population | Medscape Tinea Versicolor Overview |
| US incidence (insurance database) | 2.8 per 1,000 person-years | JAAD / 32,679 case analysis |
| Peak age range | 15 to 24 years | Medscape epidemiology |
| Patients prescribed antifungal | 67.7 percent | JAAD US insurance database |
| Most-prescribed topical | Ketoconazole (47.9 percent of topicals) | JAAD US insurance database |
| Mycologic cure with ketoconazole 2% shampoo | About 80 percent | StatPearls / AAP review |
| Higher PV burden in US | Black and Hispanic patients | NIH All of Us Research Program |
| Hot-humid US states with elevated rates | Florida, Texas, Louisiana, Gulf Coast | Medscape epidemiology |
How Long It Takes, What to Expect, and Why Skin Color Lingers
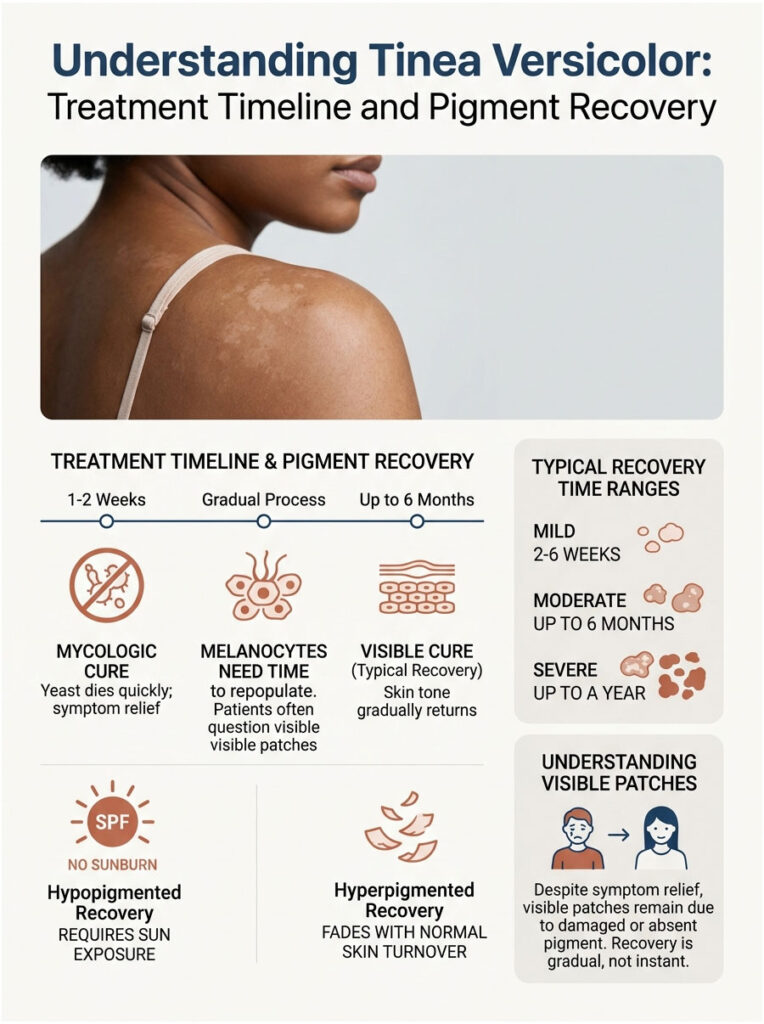
This is the single most misunderstood part of tinea versicolor recovery. The yeast dies within days to a couple weeks. The pigment changes can take months.
Treatment Timeline (Mycologic Cure vs Visible Cure)
Mycologic cure (the yeast is dead) usually happens within 1 to 2 weeks of consistent topical treatment. You can confirm this with a KOH scrape, though most people skip the recheck.
Visible cure (your skin color looks even again) takes much longer. Patients booking follow-up consults with HealthCareOnTime’s partner dermatologists routinely ask why their patches are still visible weeks after the itching is gone, and the answer is almost always: the yeast is dead, the pigment is still recovering.
Why the Patches Stay Pale (or Dark) for Months After
The melanocytes that the yeast disabled need time to repopulate the affected area and start producing pigment again. For hypopigmented patches, that means weeks of careful sun exposure for the lighter spots to catch up. For hyperpigmented patches, it means waiting for the excess pigment to fade through normal skin turnover.
Typical pigment recovery in US adults: 2 to 6 weeks for mild cases, 3 to 6 months for moderate cases, occasionally up to a year for severe widespread cases on darker skin tones.
Sun Exposure and Pigment Recovery
Modest sun exposure helps the hypopigmented patches catch up faster, but with two caveats: use SPF 30+ daily everywhere (so the surrounding skin does not darken further) and avoid sunburns, which trigger inflammation that delays recovery.
Recurrence and Prevention
If you live somewhere humid in the US, expect recurrence. Roughly 60 to 80 percent of patients have at least one relapse within two years if no maintenance routine is in place.
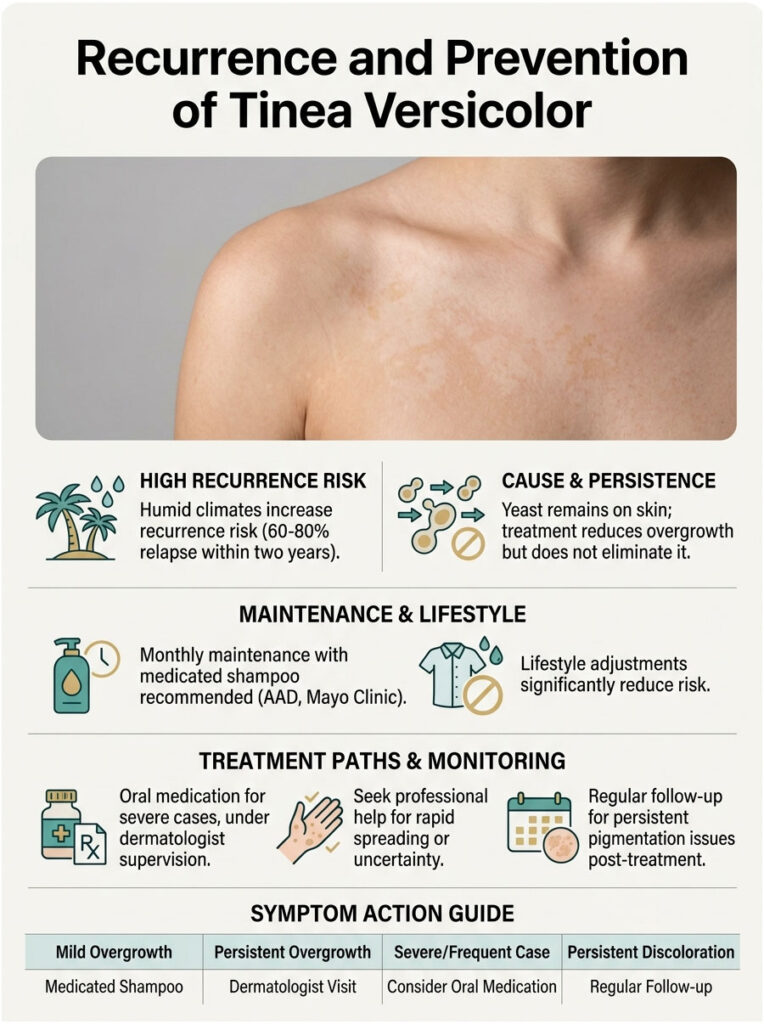
Why It Keeps Coming Back
The yeast that causes tinea versicolor never actually leaves your skin. Treatment knocks down the overgrowth, but the resident population is still there. Once the warm season returns or your sweat and sebum tick back up, the yeast can flare again.
A Practical Monthly Maintenance Schedule
The simplest prevention plan, backed by both the AAD and Mayo Clinic, is to use a medicated shampoo (selenium sulfide, ketoconazole, or pyrithione zinc) as a body wash once a month. A workable schedule for US humid climates:
- May, June, July, August, September: once weekly application, neck-to-knees, 5-10 minute contact, then rinse
- October through April: once monthly application using the same routine
- Set the same calendar reminder each month so you do not forget
This works as well as any oral preventive plan for most patients, costs almost nothing, and avoids the liver-function monitoring that oral antifungal prophylaxis requires.
Lifestyle Adjustments
A few small shifts cut recurrence risk meaningfully:
- Shower and change out of damp workout clothes promptly after exercise
- Choose moisture-wicking or loose cotton clothing in warm weather
- Skip heavy oil-based body lotions on the chest and back if you flare often
- Use a fragrance-free body wash daily during humid months
When Prophylactic Oral Medication Makes Sense
For patients with severe, widespread, or frequently recurring infection (typically more than three flares per year), dermatologists sometimes prescribe oral fluconazole or itraconazole as monthly prophylaxis. This is a specialist call, not a self-treatment decision.
Table 3: Decision and Action Reference
| Your Scenario | Recommended Action | Timeframe |
| A few small patches, first time noticing | OTC selenium sulfide or ketoconazole shampoo, 10-min daily contact | 7 to 14 days |
| Patches covering most of your back or chest | OTC topical + see dermatologist if no clearance in 2 weeks | 2 to 4 weeks |
| Cleared once but recurring every summer | Weekly maintenance shampoo May to September, neck-to-knees | Ongoing each year |
| Recurring more than 3 times in 12 months | Dermatologist visit; possible oral antifungal prophylaxis | Same month |
| Patches on the face or spreading rapidly | Dermatologist visit; rule out look-alikes | Within 1 to 2 weeks |
| Unsure if it is tinea versicolor or vitiligo | Wood’s lamp and KOH scrape with a dermatologist | Within 2 weeks |
| Pregnant, immunocompromised, or on steroids | Dermatologist visit before self-treating | Within 1 to 2 weeks |
| Pigment still uneven 6 months after treatment | Re-confirm cure with KOH; discuss pigment options | Same month |
When to See a Dermatologist
Self-treatment works for most US adults with tinea versicolor, but knowing when to escalate prevents weeks of frustration and unnecessary product spending.

Self-Treat Green-Light Scenarios
Try OTC for two weeks first if you have small to moderate patches on the trunk, neck, or shoulders, no fever or systemic symptoms, no facial involvement, and you are otherwise healthy.
If the patches lighten and stop spreading within two weeks, you are on the right track. Pigment will continue evening out over the following weeks.
Yellow-Flag Signs That Say “Book a Visit”
Schedule a dermatology appointment within one to two weeks if:
- OTC treatment shows no improvement after 14 days
- The patches keep returning every few months
- You cannot tell whether it is tinea versicolor or vitiligo
- You are pregnant, immunocompromised, or on corticosteroids
- The patches cover large body areas or have moved onto your face
Red-Flag Signs That Need Same-Week Dermatology
Make a same-week appointment (or teledermatology visit) if patches are painful, deeply red, blistering, oozing, or rapidly spreading. Those features point away from tinea versicolor toward bacterial infection, eczema flare, or another condition entirely.
Frequently Asked Questions
Is tinea versicolor contagious?
No. Every adult already has Malassezia yeast on their skin. Tinea versicolor is an overgrowth of yeast you already carry, not an infection passed from another person. You cannot catch it from a partner, family member, locker room, or shared towel. Tanning beds, pools, and gyms do not transmit it either.
Can tinea versicolor go away on its own?
Sometimes the visible patches fade in cooler, drier weather, but the yeast overgrowth typically does not resolve without treatment. Most cases either persist or recur until you use an antifungal topical. Waiting it out usually means a longer course of pigment changes and a higher chance the patches spread before you finally treat them.
What is the fastest way to get rid of tinea versicolor?
The fastest evidence-backed approach is ketoconazole 2 percent shampoo (prescription) applied to affected areas, lathered, and left on for 5 minutes daily for 1 to 3 days. A single treatment can reach roughly 80 percent mycologic cure. OTC ketoconazole 1 percent and selenium sulfide work nearly as well over a 7-day course.
Why does my tinea versicolor keep coming back?
The causative yeast is part of your normal skin flora and never leaves. Heat, humidity, sweat, and oily skin reawaken the overgrowth. Most US adults in humid climates have at least one recurrence within two years of their first episode. A monthly maintenance shampoo (selenium sulfide or ketoconazole) cuts that risk substantially.
What does tinea versicolor look like on dark skin?
On Black and Brown skin, tinea versicolor most often appears as lighter (hypopigmented) patches that are easy to mistake for vitiligo or post-inflammatory hypopigmentation. The patches usually have fine, dry scale when scratched. A Wood’s lamp exam or KOH scraping by a dermatologist quickly tells them apart.
Can I use Selsun Blue dandruff shampoo for tinea versicolor?
Yes. Selsun Blue (selenium sulfide 1 percent OTC) is one of the most common DIY treatments. Apply to affected skin, leave on for 10 minutes, rinse. Repeat daily for 7 to 14 days. Selenium sulfide 2.5 percent (prescription) works faster, but the OTC version clears most mild to moderate cases just fine.
Is tinea versicolor the same as ringworm?
No. Despite the shared “tinea” name, ringworm is a contagious infection caused by dermatophyte fungi and looks like ring-shaped red lesions with clearing centers. Tinea versicolor is a non-contagious yeast overgrowth caused by Malassezia and presents as flat discolored patches. Treatments overlap but are not identical.
How long does it take for skin color to return to normal?
After the yeast is killed, expect 2 to 6 weeks for mild cases, 3 to 6 months for moderate cases, and up to a year for severe widespread cases on darker skin. Sun exposure (with sunscreen on surrounding skin) can speed evening of hypopigmented patches. Pigment recovery is not a sign treatment failed.
Can stress cause tinea versicolor?
Stress does not directly cause tinea versicolor, but it can contribute to flares indirectly. Stress affects sleep, immune function, and skin oil production, which together can tip the balance toward yeast overgrowth. Managing stress alone will not clear an active case; you still need antifungal treatment plus lifestyle adjustments.
Does tinea versicolor mean I have a weak immune system?
Not usually. Most cases in healthy adults happen because of heat, humidity, and oil-producing skin. Recurrent or unusually widespread tinea versicolor can sometimes signal an immune concern (diabetes, HIV, steroid use, organ transplant medications). If you have repeat infections without an obvious environmental trigger, mention it to your doctor.
Can tinea versicolor spread to my face?
Facial involvement is less common in adults but does happen in teens, athletes, and people who use oily facial products. The temples, hairline, and beard area can develop patches. Treatment is the same, though dermatologists usually recommend gentler formulations on the face and shorter contact times to avoid irritation.
Is tinea versicolor more common in summer?
Yes, dramatically. Heat, humidity, and sweat fuel the yeast overgrowth, and increased sun exposure makes existing patches visually obvious because they refuse to tan. US dermatology clinics see the highest tinea versicolor volume from May through September, especially across the Southeast and Gulf states.
Disclaimer: This article is for general health education only and is not a substitute for personalized medical evaluation by a licensed US dermatologist or healthcare provider. If your skin patches do not respond to OTC treatment within two weeks, are spreading, are accompanied by pain or other symptoms, or you are uncertain about the diagnosis, please consult a board-certified dermatologist. HealthCareOnTime does not provide direct medical care for US patients and recommends seeing a local physician for in-person evaluation.
References
- Mayo Clinic. Tinea versicolor: Symptoms and causes — https://www.mayoclinic.org/diseases-conditions/tinea-versicolor/symptoms-causes/syc-20378385
- Mayo Clinic. Tinea versicolor: Diagnosis and treatment — https://www.mayoclinic.org/diseases-conditions/tinea-versicolor/diagnosis-treatment/drc-20378390
- Cleveland Clinic. Tinea Versicolor: Symptoms, Causes & Treatments — https://my.clevelandclinic.org/health/diseases/17719-tinea-versicolor
- American Academy of Dermatology. Tinea versicolor: Diagnosis and treatment — https://www.aad.org/public/diseases/a-z/tinea-versicolor-treatment
- StatPearls / NCBI Bookshelf. Tinea Versicolor — https://www.ncbi.nlm.nih.gov/books/NBK482500/
- Medscape. Tinea Versicolor: Background, Pathophysiology, Etiology — https://emedicine.medscape.com/article/1091575-overview
- JAAD / PMC. Pityriasis versicolor epidemiology in a US commercial insurance database — https://pmc.ncbi.nlm.nih.gov/articles/PMC11745915/
- NIH All of Us Research Program / Skin Health and Disease. Tinea versicolor in underrepresented groups — https://pmc.ncbi.nlm.nih.gov/articles/PMC9892469/
- MedlinePlus. Tinea versicolor encyclopedia entry — https://medlineplus.gov/ency/article/001465.htm
- Johns Hopkins Medicine. Tinea Versicolor overview — https://www.hopkinsmedicine.org/health/conditions-and-diseases/tinea-versicolor
- Harvard Health. Tinea Versicolor A to Z — https://www.health.harvard.edu/diseases-and-conditions/tinea-versicolor-a-to-z
- Cedars-Sinai. Tinea Versicolor (Pityriasis Versicolor) — https://www.cedars-sinai.org/health-library/diseases-and-conditions/t/tinea-versicolor-pityriasis-versicolor.html





