

Your nerves and veins share real estate in the crook of your elbow, and once every 21,000 blood draws, that roommate situation turns ugly. Maybe you woke up the morning after a routine blood test feeling like your fingers were wrapped in static. Maybe a sharp zap ran down your arm during the draw itself. Maybe your hand just feels weirdly weak today, and you can’t explain why. Take a breath. You’re in the right place, and this guide will walk you through exactly what’s happening and what to do next.
Table of Contents
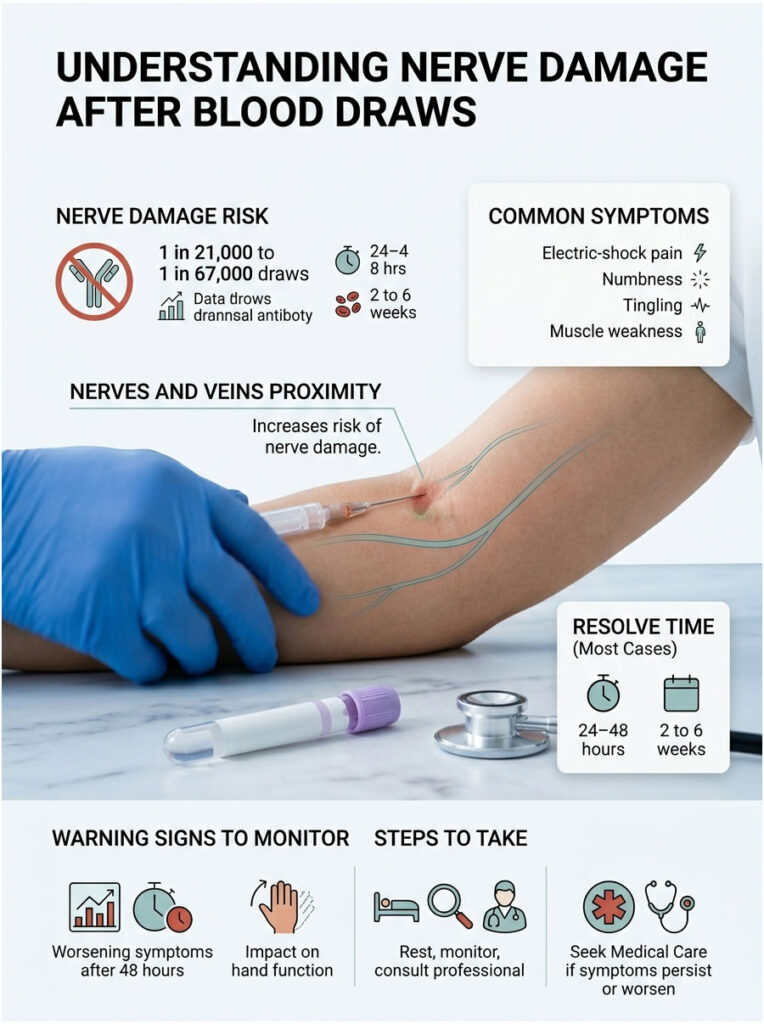
Quick Answer: Nerve damage after a blood draw happens in roughly 1 in 21,000 to 1 in 67,000 procedures, making it rare but real. Most cases involve mild nerve irritation that resolves within 2 to 6 weeks. Warning signs include electric-shock pain during the draw, persistent numbness, tingling that spreads to the fingers, and muscle weakness. Seek medical care if symptoms worsen after 48 hours or affect hand function.
At a Glance:
- Incidence ranges from 1 in 21,000 to 1 in 67,000 blood draws
- 70% of cases resolve within 1 month, 96% within 6 months
- Top 3 red flags: electric-shock pain, persistent numbness past 48 hours, hand weakness
- Most at-risk site: the inner (medial) aspect of the elbow crease
- Diabetes, thin arms, and multiple attempts raise risk
- Cold compress for first 24 hours, then switch to heat
- Go to urgent care if fingers turn cold, pale, or blue
- Full recovery is the rule, not the exception
What Nerve Damage After a Blood Draw Actually Feels Like
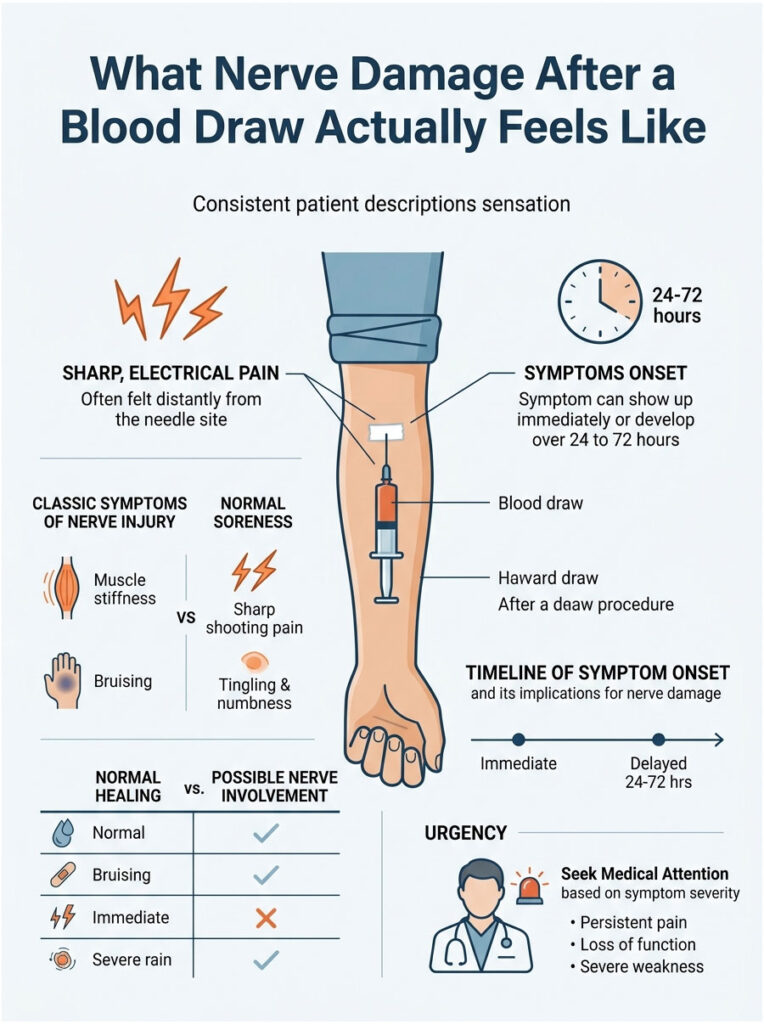
Patients describe it in pretty consistent ways once you know what to listen for. It’s not the dull ache of a flu shot or the tender spot of a small bruise. It’s sharper, electrical, and often far from where the needle went in. That disconnect, pain in your thumb when the needle went into your elbow, is the clearest tell.
One patient I worked with described the moment like “someone flipped a light switch inside my arm.” She felt the zap at the needle, ignored it, walked out, and an hour later her ring and pinky fingers were numb. That delayed spread is more common than most people realize, and recognizing it early saves weeks of recovery.
The 5 Classic Symptoms
- Electric-shock pain: Sharp, zapping pain that shoots down the arm during or right after needle insertion. Usually the first and loudest signal.
- Persistent tingling: A pins-and-needles sensation that lasts hours or days, often traveling to the hand or fingers rather than staying at the draw site.
- Numbness: A loss of sensation in a specific patch of skin, usually the forearm, thumb, or first two fingers depending on which nerve was affected.
- Burning or stabbing pain: A hot, radiating discomfort that feels nothing like normal soreness and doesn’t ease with movement.
- Muscle weakness: Difficulty gripping a cup, dropping small objects, or a “heavy” feeling in the affected hand.
Symptoms can show up immediately, or build slowly over 24 to 72 hours. Both patterns are real. Delayed onset often points to a hematoma (deep bruise) pressing on a nerve rather than direct needle contact.
Normal Soreness vs. Nerve Injury
Most post-draw discomfort is not nerve damage. It’s bruising, mild muscle soreness, or skin tenderness, and it fades within 48 hours. The table below makes the difference obvious.
| Symptom | Normal Healing | Possible Nerve Involvement | When to Act |
| Bruising | Small, yellow-purple, fades in 5-7 days | Large, spreading, feels firm | Call provider if it grows after day 2 |
| Tenderness | Localized at needle site, fades with rest | Radiates up or down the arm | Monitor for 48 hours |
| Tingling | Brief, during the draw only | Persistent, travels to fingers | Contact doctor at 48 hours |
| Electric pain | Not normal at any stage | Present during or after draw | Same-day medical attention |
| Numbness | None expected | Loss of feeling in arm or hand | Urgent care within 24 hours |
| Weakness | None expected | Can’t grip, fingers feel heavy | ER or urgent care immediately |
Symptom Timeline, What Shows Up When
The way symptoms arrive tells you a lot about what happened. Immediate pain during insertion almost always means direct nerve contact. Pain that builds over 12 to 48 hours usually means a hematoma is compressing a nerve. Symptoms appearing a week later are rare but can signal Complex Regional Pain Syndrome (CRPS), which needs prompt attention.
Why Blood Draws Hit Nerves, The Anatomy Explained
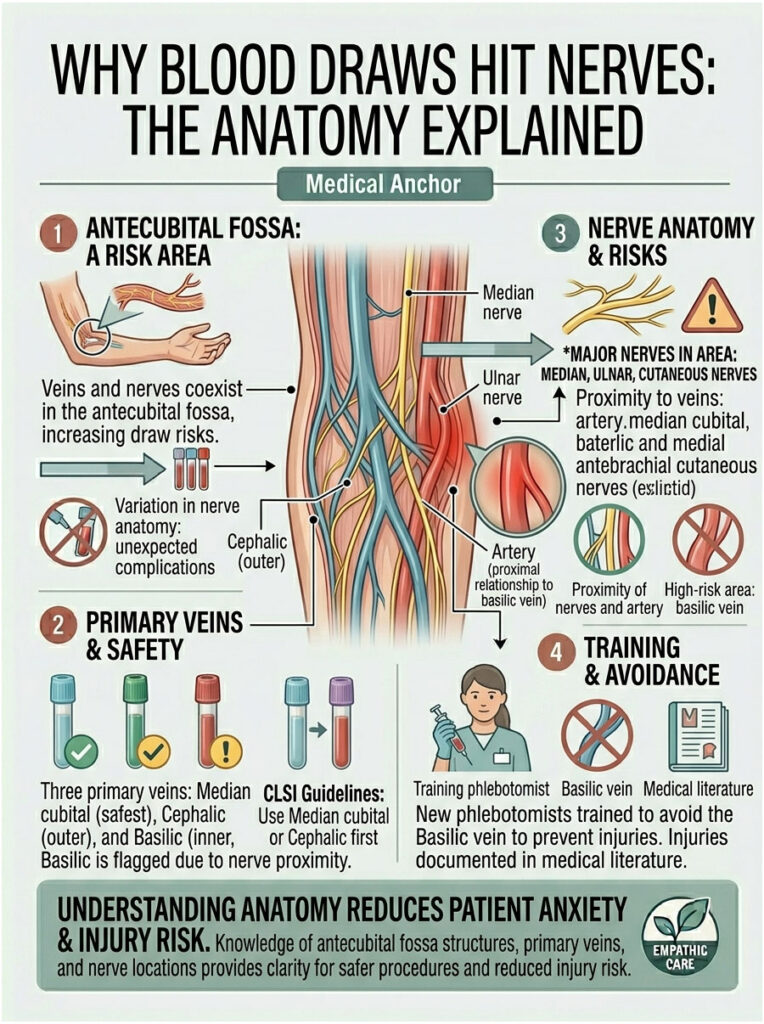
Here’s the uncomfortable truth. Your veins and nerves are roommates. In the bend of your elbow, known medically as the antecubital fossa, major sensory nerves run right alongside the veins phlebotomists target. Even a textbook-perfect draw carries a small risk, because human anatomy varies more than people expect.
Cadaveric studies published in peer-reviewed journals show dramatic variation in how nerves route through this area. One patient’s median nerve may sit safely deep under muscle; another’s may run within millimeters of the vein. You can’t see this from the outside, which is why experienced phlebotomists follow site-selection rules religiously.
The Antecubital Fossa, A Crowded Neighborhood
Three veins serve as standard blood draw targets: the median cubital vein (safest, center of the elbow crease), the cephalic vein (outer side), and the basilic vein (inner side). The nerves in the neighborhood include the median nerve, ulnar nerve, and branches of the lateral and medial antebrachial cutaneous nerves. The closer a vein sits to any of these nerves, the higher the injury risk.
The Danger Zone, Why the Basilic Vein Is Risky
The Clinical and Laboratory Standards Institute (CLSI) GP41 standard, which is the rulebook US phlebotomists follow, flags the medial (inner) aspect of the antecubital fossa as the highest-risk draw area. The basilic vein lives there, and so does the brachial artery and the median nerve. CLSI guidance is clear: phlebotomists should survey both arms for a safer median cubital or cephalic vein first, and only use the basilic vein when nothing else is accessible.
In my experience training new phlebotomists, this is the single hardest habit to build. The basilic vein often looks the most prominent, which makes it tempting, and that’s exactly why patients get hurt when technicians rush.
Which Nerves Are Most Commonly Injured
Per published case reports and the Journal of Hand Microsurgery, the injury ranking goes:
- Lateral antebrachial cutaneous nerve: Most commonly injured. Causes numbness or burning along the thumb-side forearm.
- Medial antebrachial cutaneous nerve: Second most common. Creates tingling and sensory loss on the pinky-side forearm.
- Median nerve: Less common but more serious. Can affect thumb, index, and middle finger sensation and movement.
- Ulnar nerve: Uncommon. Causes pinky and ring finger symptoms.
- Radial nerve: Rare, reported in only a handful of published cases. Affects wrist extension.
How Long Does Nerve Damage from a Blood Draw Last
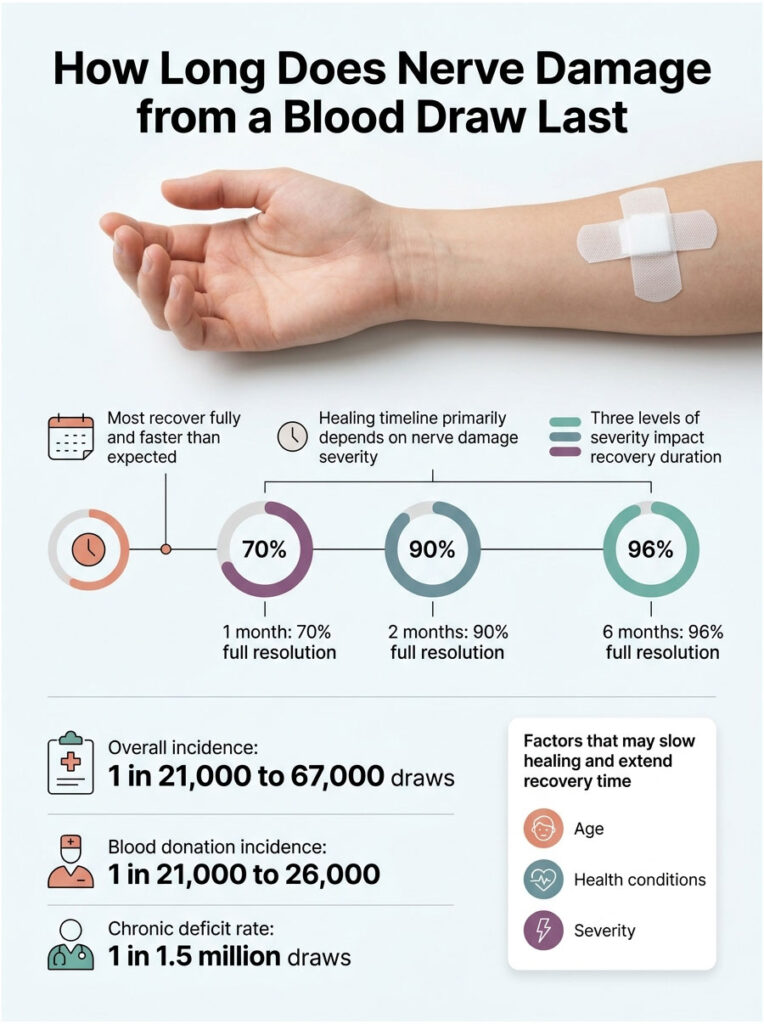
Most people recover fully, and faster than they fear. The healing timeline depends on one factor more than any other: how badly the nerve was affected.
The Three Severity Levels
- Neuropraxia (mildest): The nerve was irritated or bruised but not structurally damaged. This accounts for the majority of cases and resolves in days to a few weeks.
- Axonotmesis (moderate): The nerve fibers were damaged, but the protective outer sheath stayed intact. Recovery runs weeks to 6 months as the nerve regrows (roughly 1 mm per day).
- Neurotmesis (severe, rare): The nerve is partially or fully severed. This is very uncommon from a blood draw and may require surgical repair.
The 1-2-6 Recovery Timeline
The research here is remarkably consistent. The numbers below come from peer-reviewed studies and give you a realistic expectation of how recovery unfolds.
| Time Since Injury | Percentage Recovered | Source |
| 1 month | 70% full resolution | Newman & Waxman, Transfusion (1996) |
| 2 months | 90% full resolution | Newman & Waxman, Transfusion (1996) |
| 6 months | 96% full resolution | Newman & Waxman, Transfusion (1996) |
| Chronic deficit rate | 1 in 1.5 million draws | Horowitz, Transfusion (2000) |
| Overall incidence | 1 in 21,000 to 67,000 | PMC Case Report (2021) |
| Blood donation incidence | 1 in 21,000 to 26,000 | American Red Cross data |
When Healing Takes Longer Than Expected
Some factors slow the healing clock. If you fall into one of these categories, your timeline may stretch, and that’s worth knowing so you don’t panic when recovery feels slower than the averages above.
- Pre-existing diabetes or peripheral neuropathy
- Age over 65
- Hematoma compressing the nerve rather than direct injury alone
- Delayed diagnosis (more than 72 hours before medical evaluation)
- Chronic conditions affecting circulation
What to Do in the First 48 Hours
The first two days after a suspected nerve injury shape your recovery and your options. Good decisions now, simple ones, meaningfully improve outcomes. The single most important thing to do right away is document what happened, in writing, with timestamps.
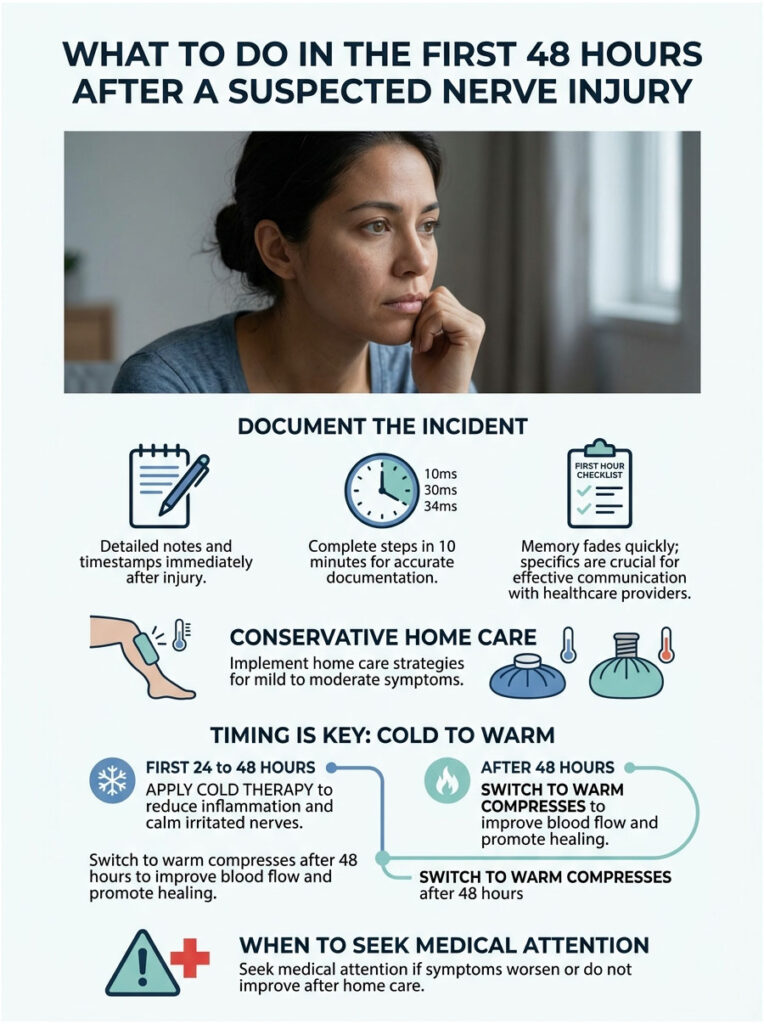
The First Hour Checklist
Work through these steps in order. It takes 10 minutes and creates a record that helps both your doctor and, if needed, any future complaint or claim.
- Rest the affected arm. Don’t carry groceries, lift bags, or do repetitive motions.
- Apply a cold compress for 15 to 20 minutes. Wrap ice in a thin towel, never directly on skin.
- Photograph the draw site from two angles, even if nothing looks wrong.
- Write down the exact timeline: time of draw, time symptoms started, which arm, which vein location (inner, outer, or center of the elbow crease).
- Note the facility and phlebotomist name. Check your appointment confirmation or receipt.
- Rate your pain on a 0 to 10 scale and log it every 4 hours for the first day.
In practice, patients who document within the first hour have much clearer conversations with their primary care doctor the next morning. Memory fades fast under stress, and specifics matter.
Days 1 to 2, Home Care That Actually Helps
For mild to moderate symptoms, conservative home care handles the job. Here’s what the evidence supports:
- Cold compress protocol: 20 minutes on, 20 minutes off, throughout the first 24 hours to reduce inflammation
- OTC pain relief: Acetaminophen or ibuprofen per FDA OTC dosing guidance, confirming any existing medication interactions with your pharmacist
- Gentle movement: Slow range-of-motion exercises for fingers, wrist, and elbow. Avoid locking the arm in one position, which can worsen stiffness
- Elevate the arm when resting, especially if swelling appears
- What NOT to do: Skip heavy lifting, avoid repetitive motions (typing for hours, lifting weights, carrying a baby on that side), and don’t sleep on the affected arm
When to Switch from Cold to Heat
Here’s a simple rule that trips up a lot of people. Cold for the first 24 to 48 hours because it reduces inflammation and calms irritated nerves. Warm compresses after that window because they improve blood flow to the healing tissue. Switching too early keeps swelling active; switching too late slows recovery.
When to See a Doctor, A Clear Decision Framework
Not every tingle warrants an ER visit. Not every symptom is safe to ignore. The table below maps the scenarios I see most often in consultations to the action that actually fits them.

| Symptom Scenario | Recommended Action | Timeframe |
| Mild tingling, no spread | Home care, monitor symptoms | Reassess at 48 hours |
| Persistent numbness past 48 hours | Call primary care doctor | Within 24 hours |
| Electric-shock pain continues hours after draw | Urgent care visit | Same day |
| Progressive weakness in hand or grip | ER or urgent care | Immediately |
| Color change, cold or blue fingers | ER, possible CRPS | Immediately |
| Fever, red streaking, or warmth at site | ER, possible infection | Immediately |
| Complete inability to move fingers | ER | Immediately |
Red Flags That Warrant Same-Day Care
CRPS is rare, but early recognition changes outcomes dramatically. These are the warning signs I train staff to spot and act on without hesitation:
- Swelling that doesn’t fit the small size of the bruise
- Skin color changes, especially pale, blue, or mottled patches
- Temperature differences between your two arms
- Extreme sensitivity to light touch (a shirt sleeve hurts)
- Progressive weakness over hours or days
- Shiny or stretched-looking skin near the draw site
What to Tell Your Doctor
Bring a clear script with you. The more specific you are, the faster your provider can rule in or rule out a serious injury. Share:
- Exact date and time of the draw
- Which arm, and where on the arm (inner vs. outer elbow crease)
- First symptom and when it started
- Current symptoms and pain scale rating
- Any photos you took
- Name of the facility and phlebotomist, if available
Treatment Options, From Home Care to Specialist Care
The vast majority of blood draw nerve injuries resolve on their own with basic care. Knowing the escalation path, though, means you won’t be caught off guard if symptoms linger or worsen.

Conservative Treatment (First Line)
For mild neuropraxia, which covers most cases, conservative care is the gold standard:
- OTC pain relievers: Acetaminophen for general pain, ibuprofen if swelling is present
- Cold-then-heat therapy: First 48 hours cold, after that warm compresses
- Activity modification: Stop doing the motions that aggravate symptoms, usually for 7 to 14 days
- Gentle stretching: Finger and wrist range-of-motion exercises, 2 to 3 times daily
- Monitor and wait: Expect improvement within 2 to 4 weeks
Most patients never need anything beyond this list. I’ve watched full recovery happen in under 3 weeks for the majority of cases my team has tracked.
Medical Interventions When Symptoms Persist
If symptoms don’t improve or worsen by the 2-week mark, your doctor may escalate to diagnostic testing. The gold standard tools include:
- Nerve conduction studies (NCS) and electromyography (EMG): These measure electrical nerve function and pinpoint the damage location.
- Ultrasound imaging: Increasingly used to visualize the affected nerve and surrounding tissue.
From there, treatment options depend on what the tests reveal. Your doctor may recommend:
- Nerve blocks: Targeted anesthetic injections to reduce pain and, in some cases, promote healing.
- Neuropathic pain medications: Gabapentin or pregabalin for burning, electric-type pain.
- Physical therapy: Targeted exercises and desensitization protocols for longer recovery cases.
- TENS (Transcutaneous Electrical Nerve Stimulation): Used for chronic pain modulation in persistent cases.
Surgical Options (Rare Cases)
Less than 1% of blood draw nerve injury cases need surgery. When they do, options include nerve decompression (freeing the nerve from scar tissue or hematoma compression) or nerve repair (reconnecting a severed nerve). Surgeons typically wait 3 to 6 months before considering these interventions, giving the nerve a chance to regenerate on its own.
How to Prevent Nerve Damage on Your Next Blood Draw
Prevention splits neatly into two halves. What you can control as the patient, and what your phlebotomist controls as the professional. Both halves matter.
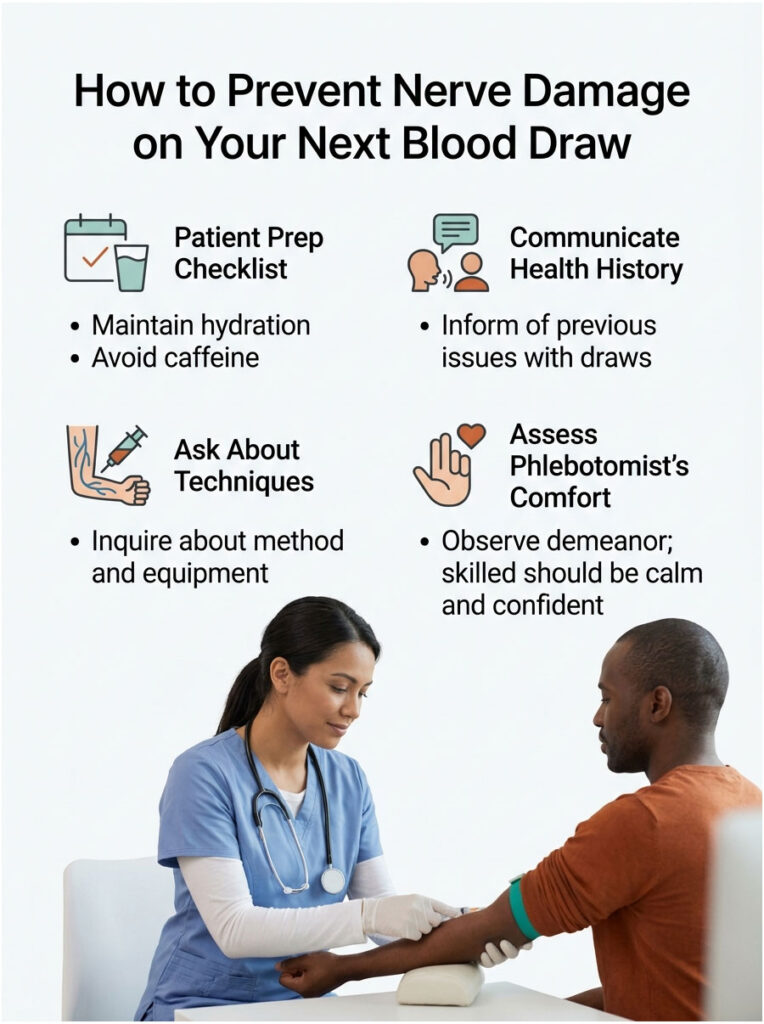
Patient Prep Checklist, What You Control
Simple habits before the appointment reduce your risk more than most people realize:
- Hydrate 24 hours ahead. Well-hydrated veins are easier to find and stay stable during the draw.
- Eat a light meal beforehand, unless you’re fasting for a specific test.
- Warm the arm with a warm cloth 5 to 10 minutes before the draw to bring veins to the surface.
- Wear short sleeves or easy-roll sleeves. Tight cuffs create pressure problems.
- Flag any past blood draw issues at check-in, out loud.
- Stay relaxed during the draw. Clenching tightens everything and raises pressure on nearby nerves.
- Speak up instantly if you feel any electric or shooting pain.
What to Ask Your Phlebotomist
A good phlebotomist welcomes these questions. A defensive one is a warning sign. You have every right to ask:
- Which vein are you planning to use?
- Can we try the median cubital vein first (the safest site)?
- Can we use the other arm if this one’s tricky?
- How many attempts will you make before we stop and try another day?
Choosing a Skilled Phlebotomist
You can spot competence in the first 60 seconds of a draw. Skilled phlebotomists:
- Survey both arms before selecting a site
- Feel the vein, not just look at it
- Use a 15-degree insertion angle (not steeper)
- Stop immediately if you report shooting pain
- Follow the CLSI two-attempt rule, no endless probing
- Document any complication in your chart
Special Populations, Who Faces Higher Risk
Some groups need extra care. If you’re in one of these categories, raise it with the phlebotomist before the needle comes out.
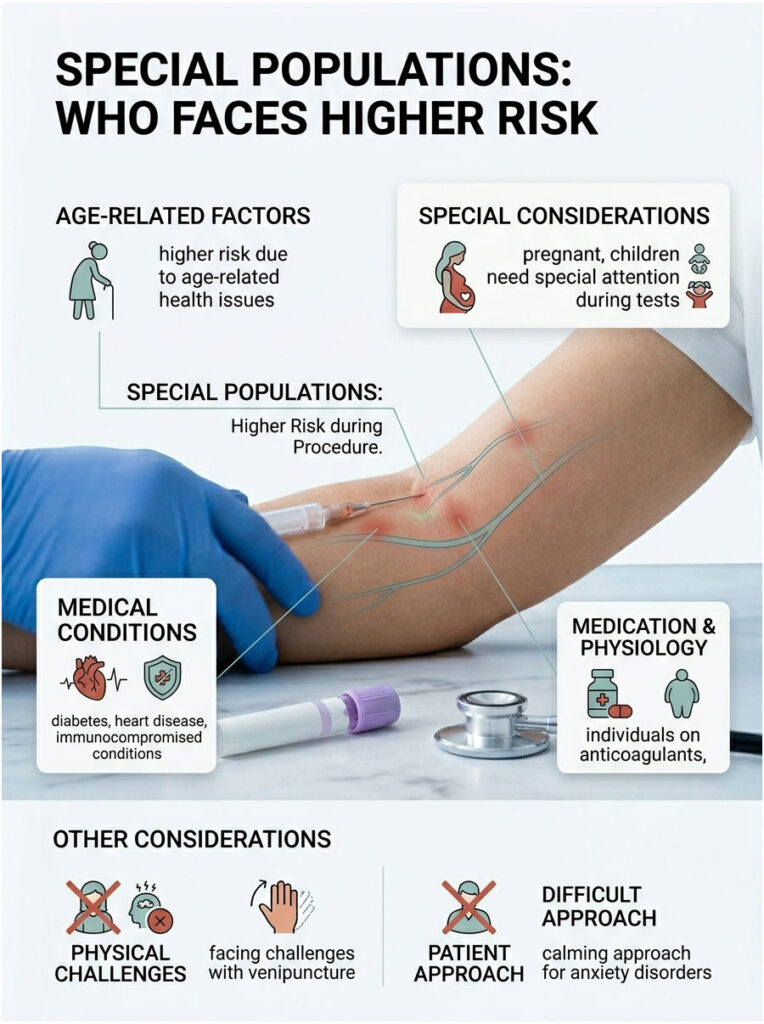
- Diabetics with neuropathy: Already-sensitive nerves mean smaller provocations produce bigger symptoms
- Chemotherapy patients: Chemo-induced neuropathy makes nerves more fragile
- Older adults (65+): Thinner skin, smaller veins, and slower healing
- Thin-armed individuals: Less tissue padding between skin and nerves
- Patients on blood thinners: Higher risk of hematoma, which can compress nerves
- People with a prior nerve injury history: Ask specifically for an experienced phlebotomist
- Mastectomy patients: Never draw from the surgical-side arm
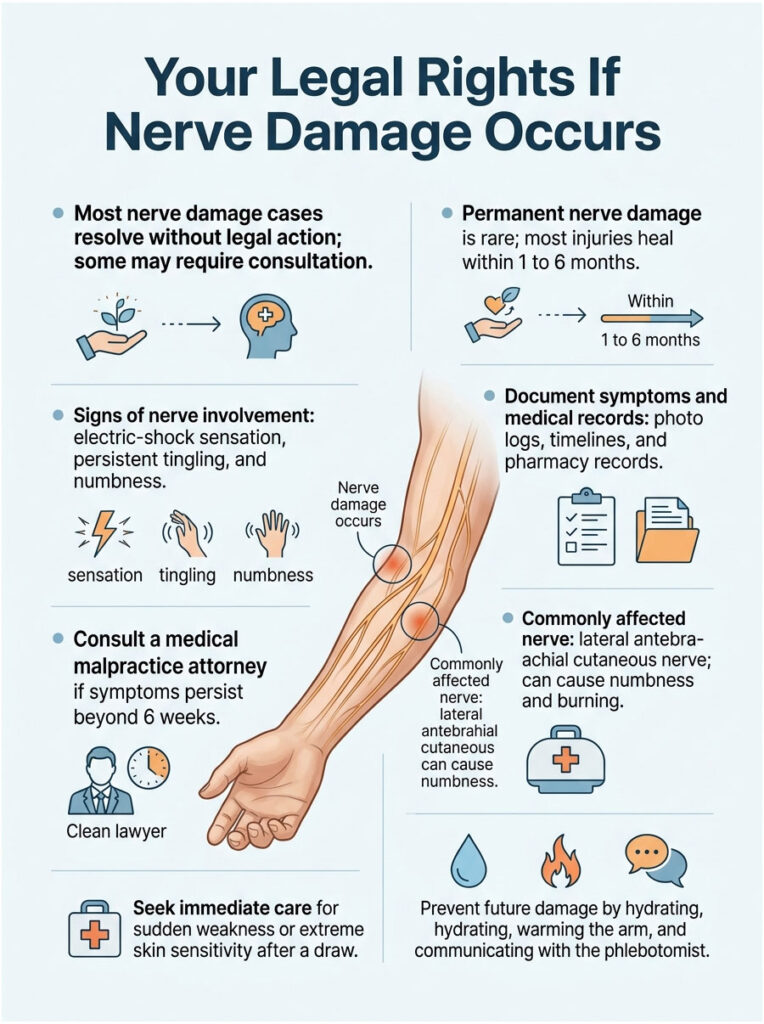
Your Legal Rights If Nerve Damage Occurs
Most cases resolve without lawyers. Some don’t. If you believe the draw went outside the standard of care, you have options.
A claim may hold weight if any of the following happened:
- The phlebotomist continued the draw after you reported shooting or electric pain
- More than 2 needle attempts were made in the same area against CLSI guidance
- The draw was taken from a wrist vein (never acceptable under standard protocols)
- Lateral needle probing occurred in the medial aspect of the elbow
- Documentation of the incident was refused
Documentation strengthens any future claim: your photo log, written timeline, pharmacy records of pain meds, medical evaluation records, and follow-up visit notes. If symptoms persist beyond 6 weeks or interfere with work, a consultation with a medical malpractice attorney is reasonable. Most offer free initial reviews.
Frequently Asked Questions
How do I know if a nerve was hit during my blood draw?
The clearest sign is an electric-shock sensation during needle insertion, often shooting toward the wrist, thumb, or fingers. Normal draws cause only a brief pinch. Persistent tingling, numbness, or sharp radiating pain after the needle is removed also signals possible nerve involvement and warrants a call to your doctor.
Can a blood draw cause permanent nerve damage?
Permanent nerve damage from a blood draw is extremely rare, occurring in roughly 1 in 1.5 million procedures per peer-reviewed data. Most injuries resolve fully within 1 to 6 months. When symptoms last beyond 6 months without improvement, it may signal more serious damage that benefits from specialist evaluation and nerve conduction studies.
How long should arm pain last after a blood draw?
Normal soreness fades within 24 to 48 hours. Mild bruising may linger 5 to 7 days. Pain lasting more than 3 days, especially if sharp, radiating, or accompanied by tingling or numbness, points to possible nerve irritation. Persistent pain beyond a week should prompt a visit to your primary care provider.
What does nerve damage from a blood draw feel like?
Patients most often describe electric-shock pain during the draw, followed by tingling, numbness, or burning that travels from the elbow to the fingers. The pain tends to feel sharper than normal soreness and may worsen with certain movements. Muscle weakness or a heavy-feeling hand can also appear within hours to days.
Can I sue for nerve damage from a blood draw?
You may have a valid claim if the phlebotomist ignored clear warning signs like shooting pain, attempted more than twice in the same spot, or drew from an unsafe site like the wrist. Medical malpractice requires proving a breach of standard of care. Consult a medical malpractice attorney for a free case evaluation if symptoms persist significantly.
Is tingling in fingers after a blood draw normal?
Brief tingling during a draw is common and usually harmless. Tingling that lasts more than an hour, travels down the arm, or comes with numbness or weakness is not normal. It suggests the needle was close to a sensory nerve. Call your provider if symptoms persist beyond 48 hours.
Should I go to the ER for nerve pain after a blood draw?
Go to the ER if you experience sudden weakness, inability to move fingers, cold or color-changed fingers, spreading numbness, or extreme skin sensitivity. These can indicate serious nerve compression or CRPS. For milder symptoms like mild tingling or light soreness, home care and a call to your primary care provider within 24 hours is usually sufficient.
What nerve is most commonly damaged during a blood draw?
The lateral antebrachial cutaneous nerve is most frequently affected, per published case reports. It runs close to the cephalic vein on the thumb-side of the forearm. Injuries to this nerve cause numbness and burning along the outer forearm. The median nerve and medial antebrachial cutaneous nerve are also at risk, particularly when basilic vein draws go wrong.
Can a bad blood draw cause complex regional pain syndrome (CRPS)?
Yes, though rarely. CRPS can develop when a nerve is injured or a hematoma compresses a nerve for an extended period. Warning signs include swelling out of proportion to the injury, skin color or temperature changes, extreme sensitivity to light touch, and worsening pain over days. Early treatment within weeks of onset improves outcomes significantly.
Why does my arm feel weak days after a blood draw?
Delayed weakness usually points to a hematoma pressing on a motor nerve, rather than direct needle injury. Blood that pooled after the draw can compress nearby structures as it grows. Progressive weakness over 24 to 72 hours is a red flag that needs same-day medical evaluation to rule out significant nerve compression.
Is it safe to get another blood draw after nerve damage?
Yes, but take precautions. Wait until symptoms fully resolve, use the opposite arm when possible, and request an experienced phlebotomist. Tell every new phlebotomist about your history and specifically ask them to avoid the inner elbow area. Many labs can accommodate hand-vein draws or use smaller butterfly needles to reduce risk.
How can I prevent nerve damage in future blood draws?
Hydrate well 24 hours ahead, warm the arm beforehand, and stay relaxed during the draw. Ask the phlebotomist to use the median cubital vein in the center of the elbow. Speak up immediately if you feel electric pain or intense tingling. Request the two-attempt limit and consider hand-vein draws if you’ve had prior issues.
Medical Disclaimer
This article provides general educational information about blood draw nerve damage and should not replace personalized medical advice. If you’re experiencing symptoms after a blood draw, contact a licensed healthcare provider for diagnosis and treatment. In emergencies, call 911 or visit your nearest emergency room.
References
- Diagnosis and Treatment of Nerve Injury Following Venipuncture, PMC (NIH)
- Radial Nerve Injury After Venipuncture, PMC (NIH)
- CDC Best Practices for Safe Venipuncture
- Clinical and Laboratory Standards Institute, GP41 Standard
- Newman & Waxman, Blood Donation-Related Neurologic Needle Injury, Transfusion (1996)
- Horowitz, Venipuncture-Induced Causalgia, Transfusion (2000)
- Mayo Clinic, Peripheral Nerve Injuries
- FDA, OTC Pain Reliever Safety
- American Society for Clinical Pathology
- U.S. Bureau of Labor Statistics, Phlebotomists Occupational Outlook





