Two people walk into a USA primary-care clinic on the same morning. Both cough every day. Both wheeze climbing stairs. Both feel a tight band squeeze across the chest at night. One walks out with an asthma inhaler. The other walks out with a COPD treatment plan. Same symptoms, very different diseases, and getting that fork in the road right changes everything that follows.
Table of Contents
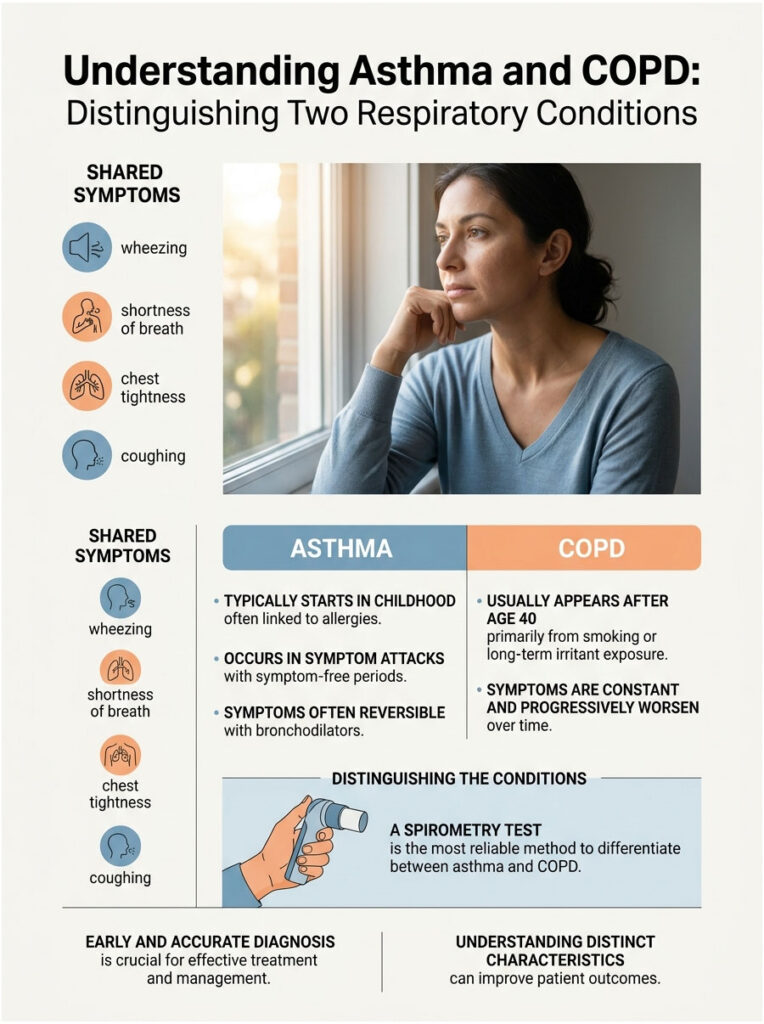
Quick Answer: Asthma and COPD both cause wheezing, shortness of breath, chest tightness, and coughing, which is why they get confused. Asthma typically starts in childhood, comes in attacks, links to allergies, and is mostly reversible with a bronchodilator. COPD usually appears after age 40, is driven mainly by smoking or long-term irritant exposure, produces constant symptoms, and progressively worsens. A spirometry test is the most reliable way to tell them apart.
At a Glance
- About 25 million Americans live with asthma; roughly 16 million US adults are diagnosed with COPD, with millions more undiagnosed.
- COPD was the 5th leading cause of death in the US in 2023, with 141,733 deaths (CDC).
- Asthma is largely reversible; COPD damage to the alveoli is not.
- Up to one in three asthma or COPD diagnoses are wrong when spirometry isn’t used.
- Asthma-COPD overlap (ACO) affects 15-20% of adults with either condition, often after age 40.
- Inhalers, steroids, and pulmonary rehab look similar across the two, but the dosing logic is very different.
- Well-controlled asthma allows a normal lifespan; COPD outcomes track closely with GOLD stage and smoking status.
What Asthma and COPD Actually Are, in Plain English
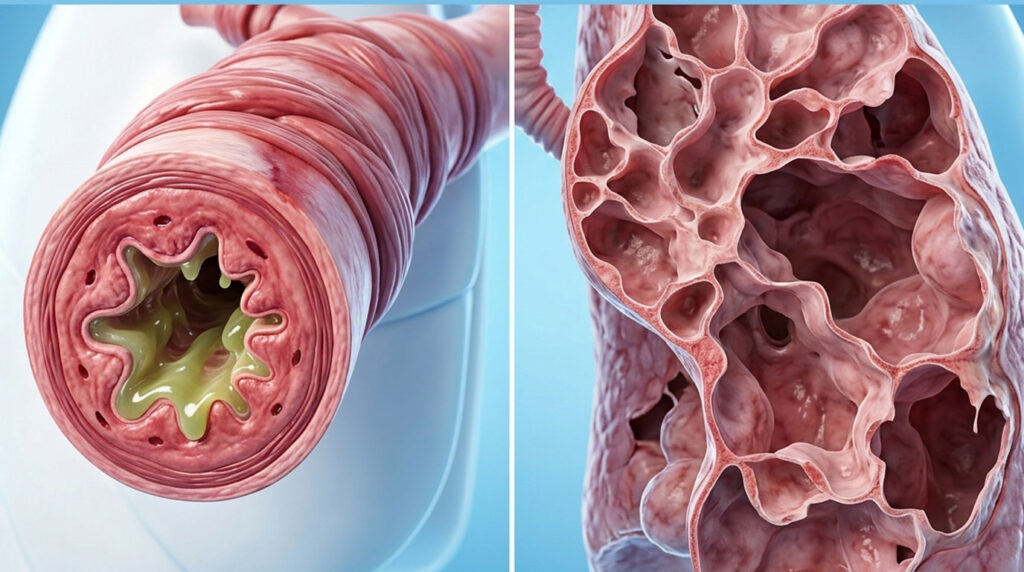
Asthma is a chronic inflammatory disease of the airways. The tubes that carry air to your lungs get swollen, the muscles around them clamp down, and the airway lining churns out sticky mucus. The result feels like breathing through a coffee stirrer for a few minutes, a few hours, or a few days, and then things calm down again.
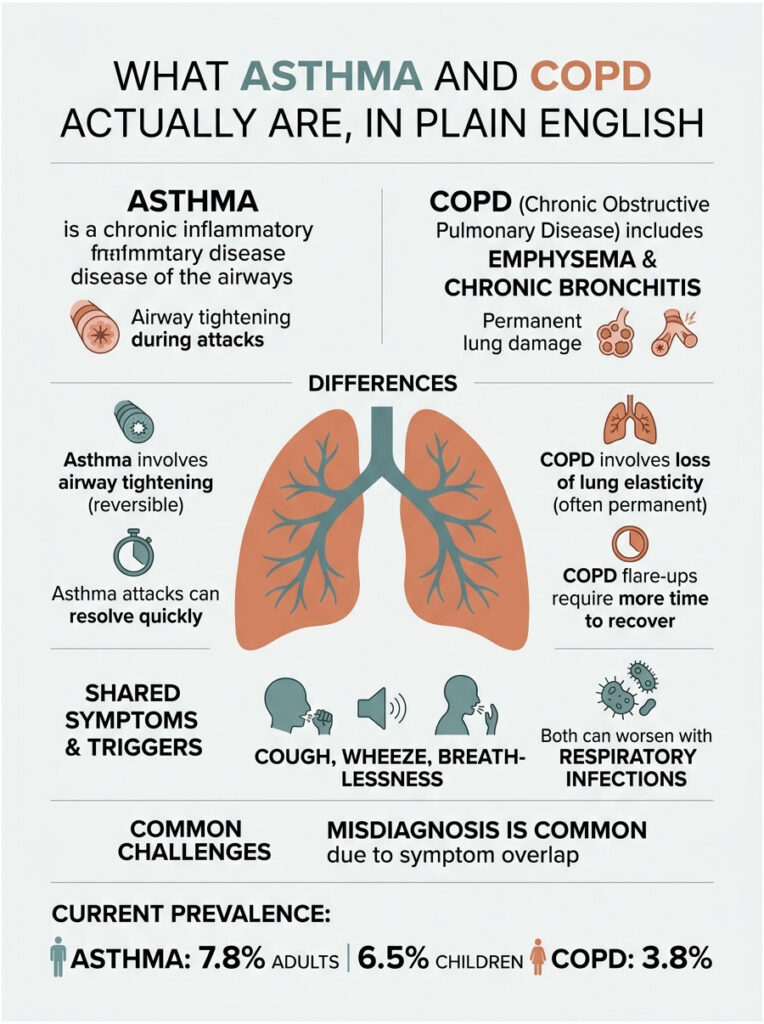
COPD (chronic obstructive pulmonary disease) is an umbrella term covering two overlapping problems: emphysema (damage to the tiny air sacs called alveoli) and chronic bronchitis (long-term inflammation of the bronchial tubes with daily mucus production). Both pieces reduce the lung’s ability to move air in and out, and the damage is permanent.
Keep this mental shortcut handy: asthma is mostly about the airways tightening, while COPD is mostly about the lung tissue itself losing elasticity and being destroyed. That structural difference explains why an asthma attack can resolve in minutes with an inhaler, while a COPD flare-up takes days to recover from even with steroids and antibiotics.
Why USA Primary-Care Doctors Mix Them Up
The symptom overlap is real. Both cause cough, wheeze, and breathlessness. Both flare with respiratory infections. Both improve at least a little with a bronchodilator puff. And both show up in middle-aged adults with smoking histories who also had a childhood touch of asthma. Patients booking pulmonary function panels through HealthCareOnTime often arrive carrying one diagnosis and leave with the other, because the symptom interview alone misses about a third of cases.
The CDC National Health Interview Survey puts current adult asthma at around 7.8% and current pediatric asthma at 6.5% in 2024, while the CDC NCHS Data Brief 529 (May 2025) puts age-adjusted COPD prevalence at 3.8% in 2023. The two conditions overlap in roughly 15% of patients with either diagnosis, which is why the testing pathway matters more than the patient history.
Asthma vs COPD: The Side-by-Side Comparison That Settles It
If you only read one section of this article, read this one. Our medical reviewers built the table below using the 2024-2025 USA clinical guidance from the American Lung Association and the GOLD 2025 Report.
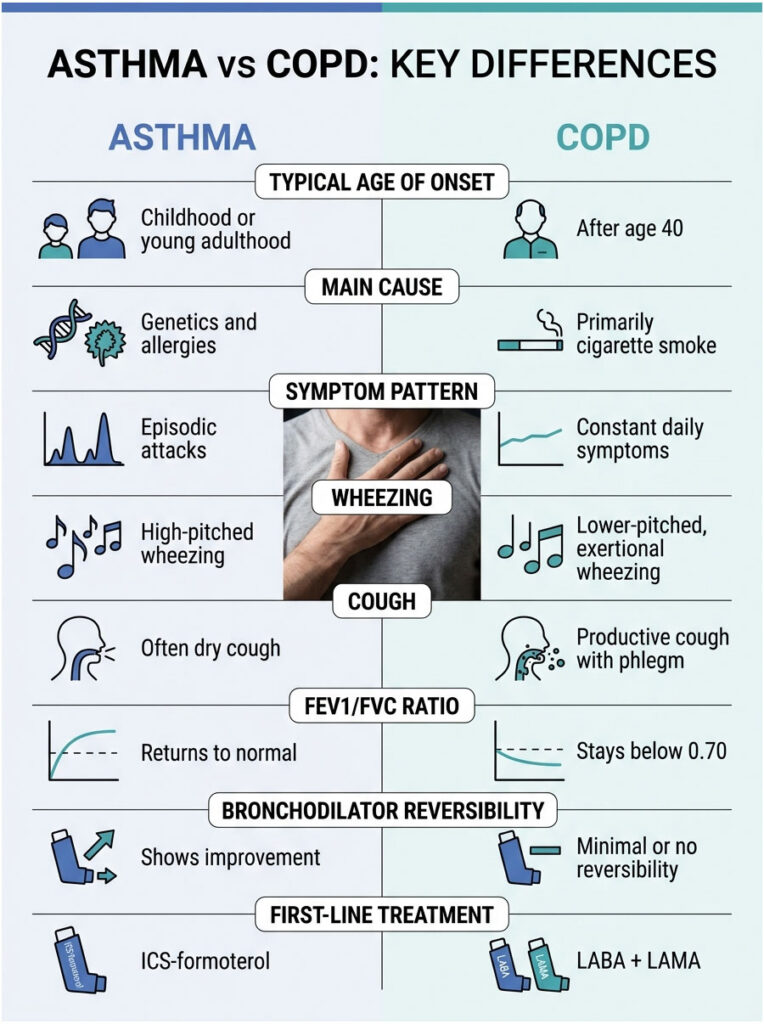
Table 1: Asthma vs COPD on Every Dimension That Matters
| Dimension | Asthma | COPD | Why This Matters |
| Typical age of onset | Childhood or young adulthood (under 20) | After age 40, often 50-65 | Sets the first clinical hypothesis |
| Main cause | Genetics + allergies + viral triggers | Cigarette smoke (85-90% of US cases), occupational dust, biomass smoke | Drives risk counseling |
| Symptom pattern | Episodic attacks with normal breathing between | Constant daily symptoms that progressively worsen | Changes treatment urgency |
| Wheezing | High-pitched, episodic, often at night | Lower-pitched, more chronic, on exertion | Stethoscope clue |
| Cough | Often dry; productive only during attacks | Productive most mornings, lots of phlegm | “Smoker’s cough” pattern |
| FEV1/FVC ratio (post-bronchodilator) | Returns to normal (>=0.75) | Stays below 0.70 | Diagnostic gold standard |
| Bronchodilator reversibility | >=12% and >=200 mL improvement in FEV1 | Minimal or no reversibility | Single test that splits them |
| Inflammatory cell type | Eosinophils, IgE-driven | Neutrophils, macrophages | Predicts steroid response |
| Disease trajectory | Stable to improving with treatment | Progressive decline (GOLD 1 -> GOLD 4) | Shapes long-term outlook |
| First-line USA treatment (2024-2025) | ICS-formoterol (SMART therapy) | LABA + LAMA combination inhaler | Different drug classes |
That last row alone is the reason getting the diagnosis right matters. Treat COPD with only an asthma rescue inhaler and the patient stays under-treated while lung decline speeds up. Treat asthma with only a long-acting muscarinic antagonist and the inflammatory driver gets ignored entirely.
Shared Symptoms (Where the Confusion Lives)
The four classic symptoms below sit at the center of both conditions. The trick isn’t which symptoms you have, it’s how they behave.
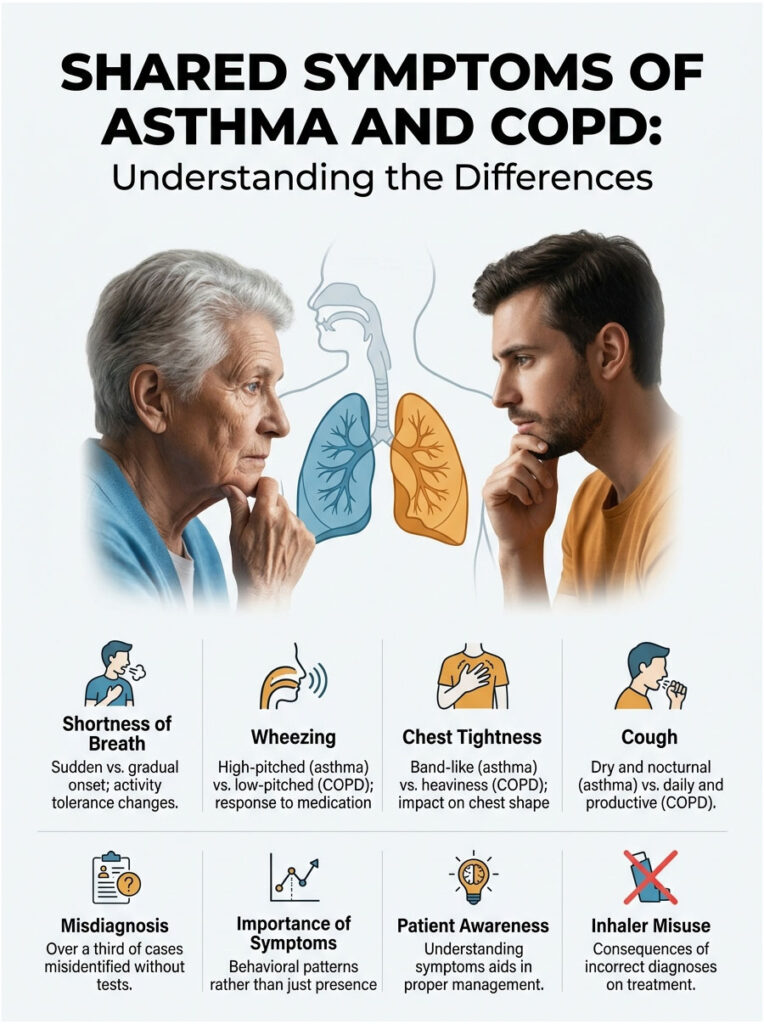
Shortness of Breath
In asthma, breathlessness shows up suddenly, often triggered by allergens, cold air, exercise, or a viral cold. Between flares, lung function returns to near-normal, and you can usually run for a bus without thinking about it. In COPD, breathlessness creeps in over years: first on stairs, then on flat ground, then while talking, then while resting in advanced disease. The COPD Foundation calls this the “shrinking life space” pattern, where activity tolerance drops by inches each year.
Wheezing
Both conditions whistle on exhale. Asthma wheezing is typically high-pitched, polyphonic, and reverses within minutes of an albuterol puff. COPD wheezing runs lower-pitched, monophonic, and only partially clears with the same medication. Listening with a stethoscope alone isn’t enough, but it’s a strong first clue our medical team uses on intake.
Chest Tightness
Asthma chest tightness feels like a band; COPD chest tightness feels more like heaviness or fullness from trapped air (hyperinflation). When emphysema flattens the diaphragm, the chest cavity sits in a permanently expanded position, which is why classic COPD patients develop the “barrel chest” appearance over time.
Cough
This one is the cleanest differentiator. Asthma cough is usually dry, worse at night, and tied to attacks. COPD cough is daily, productive (clear, white, yellow, or green mucus), worse in the morning, and present for at least three months a year over two consecutive years to meet the chronic bronchitis definition.
One peer-reviewed study referenced by Cleveland Clinic found that without pulmonary function testing, more than a third of asthma and COPD diagnoses were incorrect based on symptoms alone. That number alone explains why so many USA patients carry the wrong inhaler for years.
The Real Differences USA Doctors Look For
A 15-minute consult relies on five concrete signals more than any textbook description. Here’s what an experienced US pulmonologist actually weighs in real time.
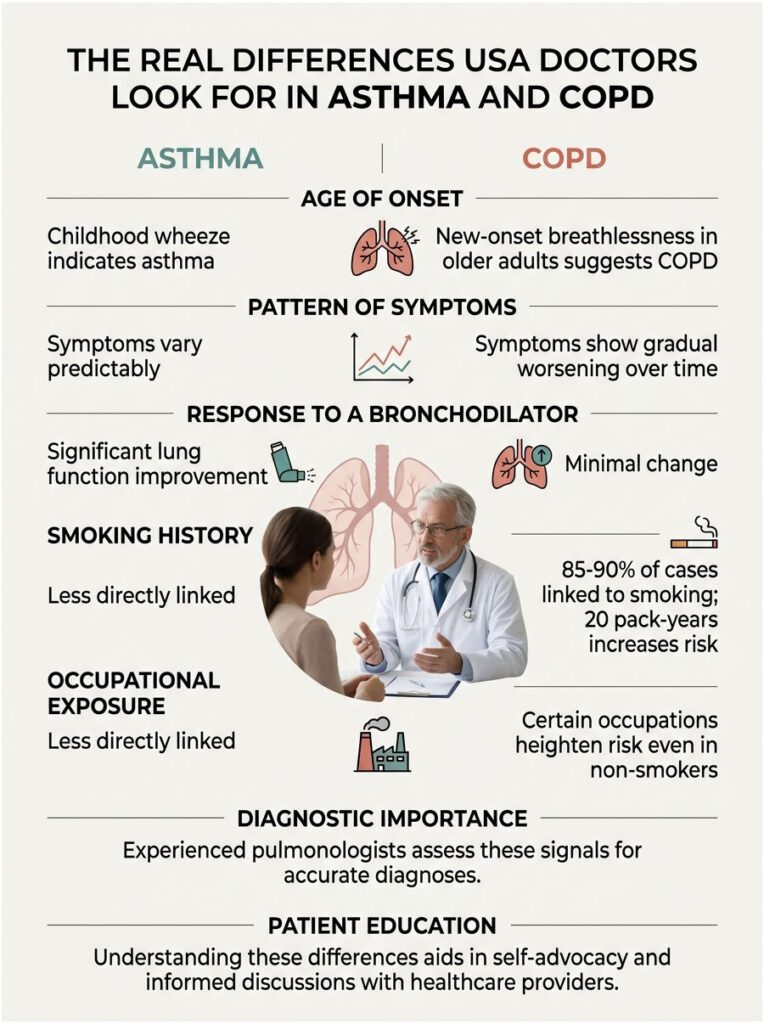
Age of Onset
Childhood-onset wheeze with eczema, hay fever, or a parent who had asthma points almost unambiguously to asthma. New-onset breathlessness in a 55-year-old former smoker with no allergy history points almost unambiguously to COPD. The middle group, adults aged 30-50 with mixed histories, is where ACO lives.
Pattern of Symptoms
Asthma symptoms wax and wane on a clock you can almost predict (worse at night, worse during allergy seasons, worse after cold exposure). COPD symptoms have a baseline that creeps up year over year, with episodic exacerbations triggered mostly by respiratory infections.
Response to a Bronchodilator
This is the single most useful in-office test. After two puffs of albuterol, a person with asthma usually shows a meaningful jump in lung function (>=12% and >=200 mL improvement in FEV1). A person with COPD shows little to no change. In cases reviewed across our diagnostic network, this reversibility test resolves about 70% of ambiguous presentations on its own.
Smoking History and Occupational Exposure
The American Lung Association reports that smoking causes 85-90% of US COPD cases. Twenty pack-years (one pack a day for 20 years, or two packs a day for 10 years) is the threshold where COPD risk climbs sharply. Patients with chemical, dust, or biomass smoke exposure (construction, agriculture, mining, restaurant kitchens, firefighting) carry similar elevated risk, even as non-smokers.
Allergy and Family History
Roughly 80% of asthma patients carry at least one allergic comorbidity (allergic rhinitis, eczema, food allergy, or nasal polyps). COPD shows no such allergic clustering, though a family history of alpha-1 antitrypsin deficiency (an inherited cause of early-onset emphysema, often before age 45) should always be screened in COPD diagnosed under age 50.
Causes and the USA Risk Profile
Asthma and COPD share some triggers (tobacco smoke, air pollution, respiratory viruses), but the underlying causes diverge sharply.
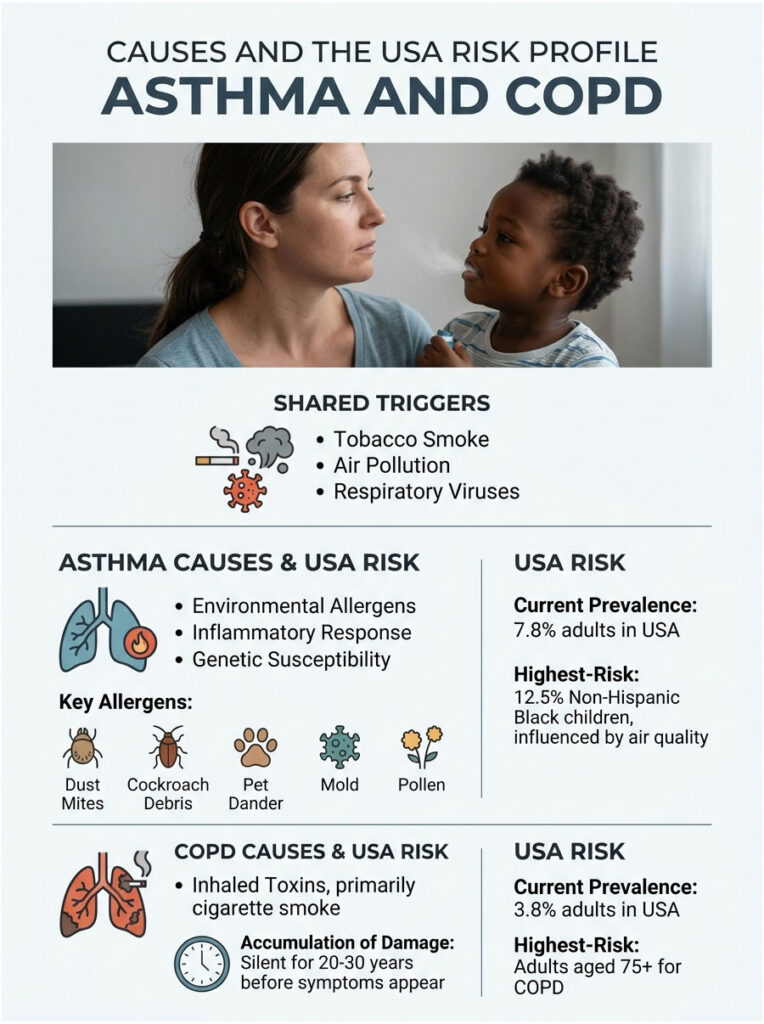
Asthma is driven by an inflammatory cascade in genetically susceptible people, set off by environmental allergens like dust mites, cockroach debris, pet dander, mold, pollen, viral upper-respiratory infections, exercise in cold dry air, NSAIDs (in aspirin-sensitive subtypes), and sulfites in food and wine. The AAFA April 2025 update lists non-Hispanic Black children at 12.5% asthma prevalence in the US, the highest of any racial group, with ZIP-code-level air quality explaining a significant share of that disparity.
COPD is driven primarily by inhaled toxins. Cigarette smoke remains the single biggest cause in the United States, but secondhand smoke, wood-burning stove smoke, industrial dust (silica, coal, cotton, grain), diesel exhaust, and outdoor PM2.5 pollution all push risk higher. The damage accumulates silently for 20-30 years before symptoms appear.
Table 2: Asthma and COPD by the USA Numbers
| Metric | Asthma (USA) | COPD (USA) | Source |
| Current prevalence (adults, 2023-2024) | 7.8% (~21 million adults) | 3.8% (~9.4 million diagnosed adults) | CDC NHIS 2024; CDC Data Brief 529, May 2025 |
| Current prevalence (children, 2024) | 6.5% (~4.7 million children) | Rare under 40 | CDC FastStats 2024 |
| Annual ER visits (primary diagnosis) | ~1.4 million | ~1.5 million | CDC NEDS; AHRQ HCUP |
| Annual US deaths (most recent) | ~3,500 (2021) | 141,733 (2023, 5th leading cause) | CDC NVSS; CDC Data Brief 529 |
| Annual US medical cost | $50+ billion (asthma, 2013-2018 base) | $24 billion (adults 45+) | AAFA; CDC Data Brief 529, May 2025 |
| Highest-risk demographic | Non-Hispanic Black children (12.5%) | Adults age 75+ (10.5%) | AAFA 2025; CDC Data Brief 529 |
The cost figures alone shape why USA insurers push hard for accurate diagnosis. A patient mislabeled with asthma when they actually have COPD costs the system significantly more over a decade through preventable hospitalizations.
How Doctors Tell Them Apart: The Tests That Matter
A clinical interview gets you 60% of the way there. The remaining 40% requires objective lung function testing. Patients commonly ask us which tests are worth paying for if budget is tight, and the answer is almost always: start with spirometry.
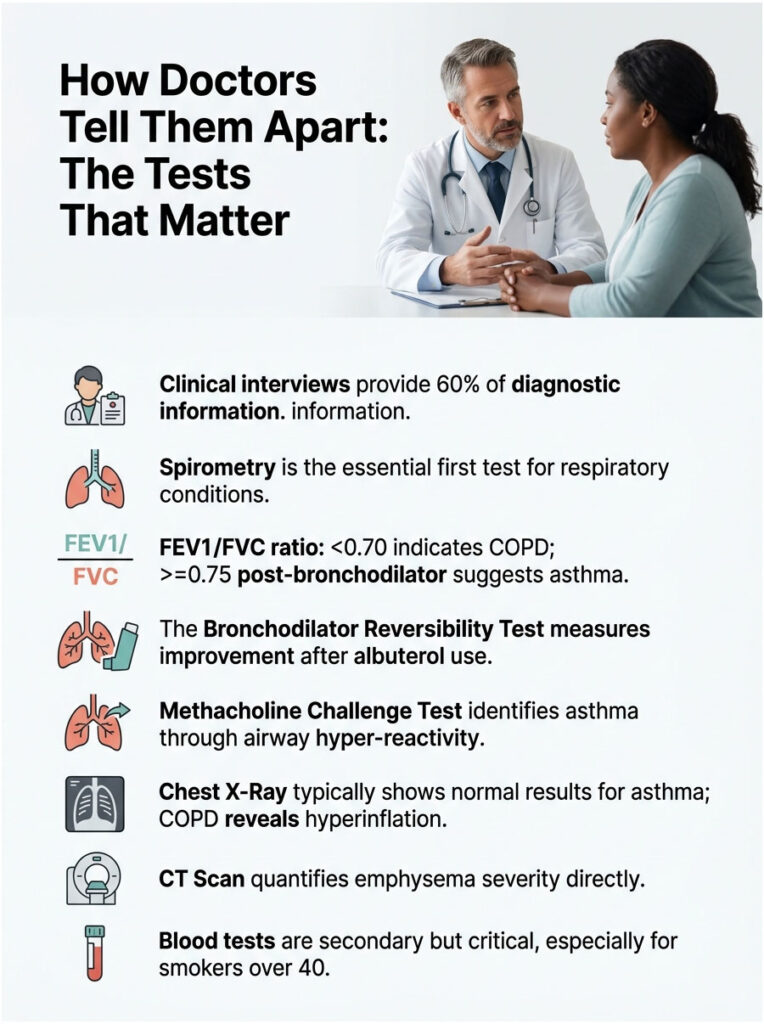
Spirometry (The Single Most Important Test)
You blow as hard and as long as you can into a tube. The machine reports three numbers:
- FVC (Forced Vital Capacity): total volume of air you can exhale in one breath
- FEV1 (Forced Expiratory Volume in 1 second): how much of that volume comes out in the first second
- FEV1/FVC ratio: the percentage of total lung volume you can blow out in one second
A post-bronchodilator FEV1/FVC ratio below 0.70 confirms COPD. A ratio that returns to >=0.75 after a bronchodilator points to asthma. A 2022 peer-reviewed Dutch primary-care study found that adding spirometry to history alone boosted diagnostic accuracy (AUC) from 0.84 to 0.89, a meaningful clinical jump.
Bronchodilator Reversibility Test
You do baseline spirometry, take two puffs of albuterol, wait 15 minutes, and repeat the spirometry. An improvement of >=12% and >=200 mL in FEV1 strongly suggests asthma. Less change suggests COPD or mixed disease.
Methacholine Challenge Test
You inhale increasing doses of methacholine (a chemical that narrows airways). People with asthma respond at very low doses because the airways are hyper-reactive. People without asthma don’t react until much higher doses. This test is mostly used when symptoms suggest asthma but spirometry is normal.
Chest X-Ray and CT Scan
Asthma usually leaves chest imaging looking normal. COPD shows hyperinflation, flattened diaphragms, and (in emphysema) visible bullae or low-attenuation areas on CT. A CT scan is the only way to quantify emphysema severity directly.
Blood Tests
- Eosinophil count: elevated in eosinophilic asthma; can also be elevated in some COPD phenotypes
- Total IgE and allergen-specific IgE: elevated in allergic asthma
- Alpha-1 antitrypsin level: mandatory screening for any COPD patient under 50 or non-smoker with COPD
- Arterial blood gas: measures oxygen and CO2 levels, used in advanced COPD
Our medical reviewers consistently recommend spirometry over symptom checklists alone, particularly for adults over 40 with a smoking history. Skipping the test almost guarantees a one-in-three diagnostic error rate.
Asthma-COPD Overlap (ACO): When You Have Both
About 15-20% of US adults with either asthma or COPD actually carry features of both. The condition has gone by several names (ACOS, ACO, mixed obstructive airway disease), but the clinical reality is the same: persistent airflow obstruction (COPD-like) combined with significant bronchodilator reversibility or eosinophilic inflammation (asthma-like).
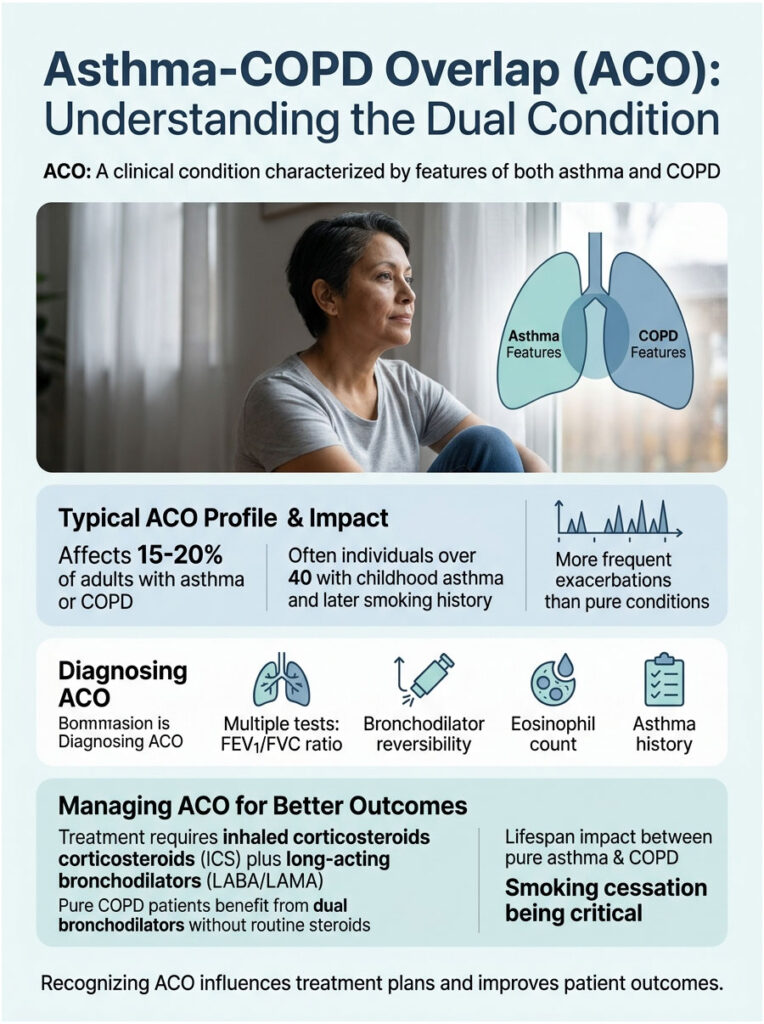
Who Typically Develops ACO
The classic ACO profile is a person over 40, often with a childhood asthma history, who later smoked or worked in irritant-heavy environments (construction, manufacturing, agriculture, firefighting). Adult-onset asthma in an ever-smoker also falls into this group. ACO patients tend to experience more frequent exacerbations than either pure condition and use more healthcare resources year over year.
How ACO Gets Diagnosed
There is no single ACO test. Pulmonologists use a combination of post-bronchodilator FEV1/FVC below 0.70 (COPD criterion), meaningful bronchodilator reversibility (>=12% and >=200 mL improvement, asthma criterion), elevated blood eosinophil count (often >=300 cells/microL), and a documented history of asthma before age 40 or strong allergic comorbidity. Patients booking lung function panels with us routinely get all four pieces in a single visit, which speeds up the ACO call.
Why the Label Matters for Treatment
The 2025 GOLD Report notes that ACO patients should be treated with an inhaled corticosteroid plus a long-acting bronchodilator combination, never with bronchodilators alone, because the underlying eosinophilic inflammation needs steroid suppression. Pure COPD patients without eosinophilia, by contrast, do better on dual bronchodilators (LABA + LAMA) without routine steroids. Getting ACO recognized therefore changes the prescription, not just the chart label.
Patients commonly ask us whether ACO shortens lifespan. Current research suggests outcomes sit between pure asthma (better) and pure COPD (worse), with smoking cessation being the single biggest modifiable factor.
Treatment Differences (Inhalers, Steroids, Rehab)
The treatment maps look similar from a distance and very different up close.
Asthma First-Line Treatment
The 2024 GINA (Global Initiative for Asthma) report recommends ICS-formoterol (inhaled corticosteroid plus formoterol) as both maintenance and rescue therapy for most adults and adolescents. This is called SMART therapy (Single Maintenance and Reliever Therapy). The shift away from albuterol-only rescue has been the biggest USA asthma treatment change of the past five years.
Add-on options include leukotriene receptor antagonists (montelukast), long-acting muscarinic antagonists (tiotropium), and biologics for severe eosinophilic or allergic asthma (omalizumab, mepolizumab, dupilumab, benralizumab, tezepelumab).
COPD First-Line Treatment
The 2025 GOLD Report recommends starting most symptomatic COPD patients on a LABA + LAMA combination inhaler (long-acting beta-agonist plus long-acting muscarinic antagonist). Inhaled corticosteroids are added only for patients with frequent exacerbations or eosinophilic phenotype. Rescue short-acting bronchodilators (albuterol, ipratropium) handle breakthrough symptoms.
Beyond inhalers, COPD care includes pulmonary rehabilitation (a structured exercise and education program), oxygen therapy for advanced cases, smoking cessation support, and annual influenza, COVID-19, RSV, and pneumococcal vaccinations. Severe emphysema may eventually require lung volume reduction surgery or lung transplant.
Where the Two Overlap
Both diseases use inhaled corticosteroids (sometimes), both use bronchodilators (always), and both benefit from vaccines, weight management, and avoiding tobacco smoke. The big rule: never give a COPD patient inhaled corticosteroids without a long-acting bronchodilator, and never give an asthma patient a long-acting beta-agonist without inhaled corticosteroids. Getting either wrong has caused FDA black-box warnings in the past.
Outlook, Prognosis, and Life Expectancy
Asthma, when controlled well, typically does not shorten lifespan. Most US adults with well-managed asthma live a normal lifespan with normal activity levels. Severe, poorly controlled asthma carries higher mortality, especially in the absence of inhaled corticosteroid use.
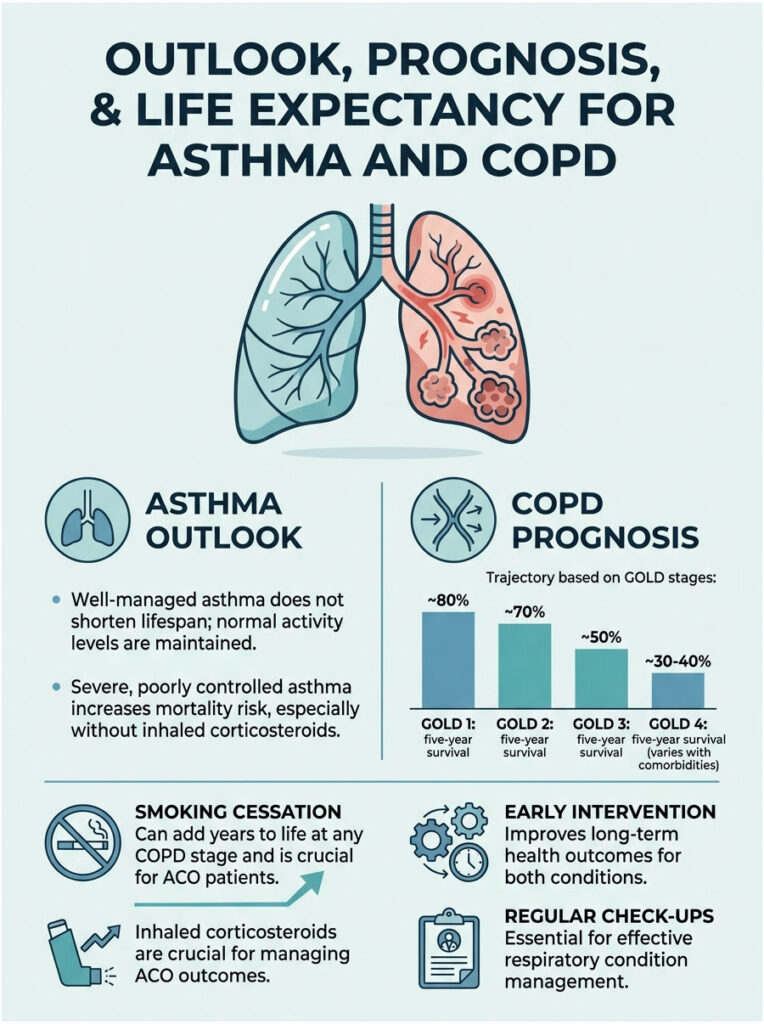
COPD has a more sobering trajectory. The GOLD staging system (1 mild through 4 very severe) predicts five-year survival roughly as follows: GOLD 1 around 80%, GOLD 2 around 70%, GOLD 3 around 50%, and GOLD 4 around 30-40% depending on comorbidities. Smoking cessation at any stage adds years of life and slows decline more than any medication can.
ACO outcomes sit in between, with the biggest modifiable factor being whether the person stops smoking and receives appropriate inhaled corticosteroid therapy.
When to See a Doctor: A Decision Matrix
Use the table below as a quick triage tool. Patients booking diagnostic appointments through HealthCareOnTime often use a version of this matrix to decide whether to wait, see a primary-care doctor, see a pulmonologist, or head straight to the ER.
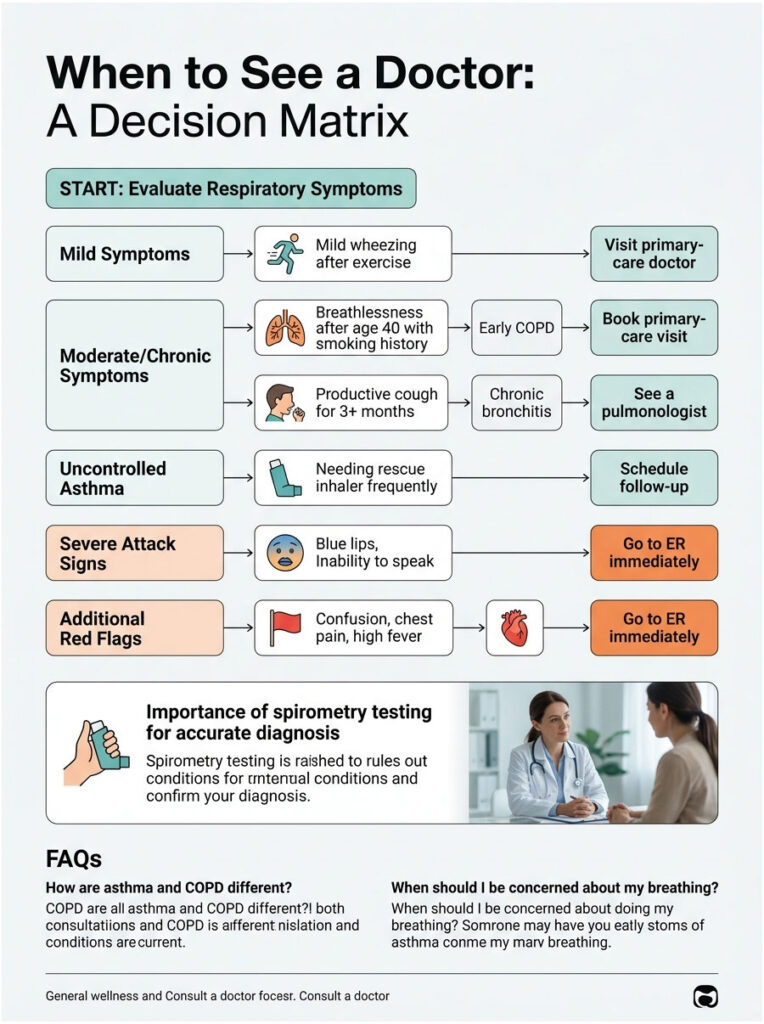
Table 3: Symptom Scenario to Recommended Action
| Scenario | What It Likely Suggests | Recommended Action |
| You wheeze occasionally after exercise or pollen exposure, with normal breathing in between | Possible mild asthma | Book a primary-care visit; ask for spirometry within 2-4 weeks |
| You’re over 40, smoked for 15+ years, and notice creeping breathlessness on stairs | Possible early COPD | Book a primary-care visit; request spirometry plus chest X-ray |
| You cough productive mucus most mornings for 3+ months, no infection | Chronic bronchitis (COPD subtype) | See a pulmonologist; full pulmonary function test recommended |
| You have known asthma and now need your rescue inhaler more than twice a week | Uncontrolled asthma | Book a follow-up within 7 days; ICS-formoterol upgrade likely |
| You have lips or fingernails turning blue, can’t finish a sentence, or rescue inhaler isn’t working | Severe attack or COPD exacerbation | Call 911 or go to the nearest ER immediately |
Red-flag ER signs apply to both conditions: blue or gray lips, confusion or drowsiness, inability to speak in full sentences, peak flow under 50% of personal best, chest pain, or fever above 102 degrees Fahrenheit with breathing difficulty.
Frequently Asked Questions
Can asthma turn into COPD over time?
Not directly, no. Asthma doesn’t transform into COPD on its own. However, decades of poorly controlled asthma, especially combined with smoking or heavy occupational exposure, can cause permanent airway remodeling that resembles COPD on spirometry. People in this group are usually diagnosed with ACO rather than either pure disease.
Can a non-smoker get COPD?
Yes. Roughly 10-15% of US COPD cases occur in lifetime non-smokers. Causes include long-term secondhand smoke exposure, indoor biomass smoke, occupational dust and chemical exposure, severe childhood respiratory infections, untreated asthma, and the inherited alpha-1 antitrypsin deficiency. Anyone diagnosed with COPD under age 50, or with no smoking history, should be tested for alpha-1.
Which is more dangerous, asthma or COPD?
COPD carries higher mortality on average because the lung damage is permanent and progressive. COPD was the 5th leading cause of death in the US in 2023 with 141,733 deaths. Asthma deaths were about 3,500 in 2021. That said, a severe asthma attack can kill within hours if untreated, so neither condition is harmless.
Can you have both asthma and COPD at the same time?
Yes. This is called asthma-COPD overlap (ACO) and affects roughly 15-20% of adults with either diagnosis. ACO often shows up after age 40 in people who had childhood asthma and later smoked or worked in irritant-heavy environments. Treatment usually requires inhaled corticosteroids plus a long-acting bronchodilator combination.
How accurate is a spirometry test for telling them apart?
Spirometry plus bronchodilator reversibility testing is the diagnostic gold standard. A 2022 peer-reviewed study showed that adding spirometry to clinical history increased diagnostic accuracy (AUC) from 0.84 to 0.89, with sensitivity and specificity above 90% in some validated diagnostic algorithms. Symptom history alone misses about a third of cases.
Does an asthma inhaler work for COPD?
A short-acting albuterol inhaler provides quick relief for both conditions, but it doesn’t treat the underlying disease in either. Long-term asthma control requires inhaled corticosteroids; long-term COPD control requires long-acting bronchodilators with or without steroids. Using only a rescue inhaler for COPD leaves the patient under-treated and speeds up lung decline.
What is the life expectancy with COPD in the US?
It depends on the GOLD stage at diagnosis, smoking status, and comorbidities. Five-year survival ranges from roughly 80% in mild (GOLD 1) disease to 30-40% in very severe (GOLD 4) disease. Quitting smoking at any stage adds years, and modern combination inhalers plus pulmonary rehab significantly improve quality-of-life metrics.
Are asthma and COPD genetic?
Asthma has a strong genetic component; having one parent with asthma roughly doubles a child’s risk, and having both parents with asthma raises it further. COPD genetics are more limited, with alpha-1 antitrypsin deficiency being the single clearly inherited cause. Most COPD risk in the US still traces back to tobacco and occupational exposure, not genes.
Can air pollution cause both asthma and COPD?
Air pollution worsens both conditions and contributes to causing both. Long-term exposure to PM2.5, ozone, nitrogen dioxide, and traffic-related pollutants raises COPD incidence in adults and triggers asthma development in genetically susceptible children. EPA air-quality data tracks these exposures by US county, and high-risk ZIP codes show measurably higher prevalence rates.
Is COPD curable in 2026?
No. Current 2025-2026 medical science can slow COPD progression, manage symptoms, and improve quality of life, but it cannot reverse damage to the alveoli or rebuild lost lung tissue. Lung transplant is the only “reset,” and it carries its own significant risks. Asthma, by contrast, is highly controllable and often near-symptom-free with good treatment.
What is the best test for diagnosing COPD vs asthma?
Post-bronchodilator spirometry is the single best test. A reduced FEV1/FVC ratio that remains below 0.70 after bronchodilator confirms COPD. A ratio that normalizes (and a >=12%, >=200 mL improvement in FEV1) confirms asthma. Chest imaging, blood eosinophil counts, and alpha-1 antitrypsin testing fill in the rest. Symptom interviews alone are not enough.
Does HealthCareOnTime offer pulmonary function testing?
Yes. Our diagnostic network supports spirometry, pulmonary function panels, allergy IgE panels, and alpha-1 antitrypsin screening across major US cities, with home-collection options for selected blood tests. Patients booking tests with us often pair a baseline spirometry with an allergy panel to clarify whether their wheezing has an allergic, fixed-obstruction, or mixed driver.
Medical Disclaimer: This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Symptoms that resemble asthma or COPD can also be caused by other serious conditions, including heart failure, pulmonary embolism, vocal cord dysfunction, and lung cancer. Always consult a licensed US healthcare provider before starting, stopping, or changing any treatment. If you experience severe breathing difficulty, blue lips, chest pain, or confusion, call 911 immediately.
References
- Centers for Disease Control and Prevention: COPD Data Brief 529 (May 2025)
- CDC FastStats: Asthma (2024)
- CDC: Most Recent National Asthma Data
- AAFA: Asthma Facts and Figures (April 2025)
- American Lung Association: COPD
- Cleveland Clinic: Asthma vs. COPD
- AAAAI: Asthma and COPD Differences and Similarities
- Global Initiative for Asthma (GINA) Reports
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) Reports
- MedlinePlus: Alpha-1 Antitrypsin Deficiency
- NCBI PMC: Diagnostic differentiation between asthma and COPD using lung function testing