
Most antidepressants make sleep worse and appetite weirder before they make depression better. Mirtazapine works in the other direction, and that single quirk explains why US prescribers reach for it when SSRIs have left a patient sleepless, thin, and still depressed.
Table of Contents
Quick Answer: Mirtazapine, sold under the brand name Remeron, is an atypical tetracyclic antidepressant FDA-approved in 1996 for major depressive disorder in adults. It blocks alpha-2 adrenergic and serotonin receptors, raising both norepinephrine and serotonin activity. The usual dose is 15 mg to 45 mg taken once daily at bedtime. The most common side effects are drowsiness, increased appetite, and weight gain.
At a Glance
• FDA-approved June 1996 for major depressive disorder (MDD)
• Drug class: tetracyclic antidepressant in the NaSSA subgroup
• Standard adult dose: 15 mg to 45 mg once daily at bedtime
• Top three side effects: drowsiness (over 50% in trials), increased appetite, weight gain
• Carries an FDA boxed warning for suicidal thoughts in patients under 25
• Often used off-label for insomnia, anxiety, PTSD, and cancer-related appetite loss
• Generic mirtazapine is widely affordable in the US, often $10 to $20 for a 30-day supply
What Is Mirtazapine?
Mirtazapine is a prescription antidepressant in the tetracyclic class, a small family of drugs that sits outside the much larger SSRI and SNRI groups. The US Food and Drug Administration approved it in June 1996 under the brand name Remeron, originally manufactured by Organon (FDA AccessData).

Patients and clinicians sometimes call mirtazapine a NaSSA, short for noradrenergic and specific serotonergic antidepressant. The label exists because the drug boosts both norepinephrine and serotonin, but through a different mechanism than SSRIs use (NCBI StatPearls).
Generic mirtazapine is widely stocked at US pharmacies, which keeps cost low for most patients. Across patient histories reviewed by our medical team, mirtazapine appears more often than any other tetracyclic, usually in patients whose first SSRI trial improved mood but wrecked sleep or appetite.
Brand Names, Generic Status, and Forms in the US
The brand name Remeron is still sold, but most US prescriptions are filled as the generic. Two oral forms carry FDA approval:
- Standard tablets: 7.5 mg, 15 mg, 30 mg, and 45 mg
- Orally disintegrating tablets (Remeron SolTab): 15 mg, 30 mg, and 45 mg, which dissolve on the tongue
The SolTab form helps patients who struggle to swallow pills, who want a faster onset of the sedating effect, or who travel often. Both forms reach the same blood levels within a few hours.
How Mirtazapine Differs From SSRIs and SNRIs
SSRIs like sertraline and escitalopram work mostly by blocking serotonin reuptake. SNRIs like venlafaxine and duloxetine add norepinephrine reuptake blocking to the mix. Mirtazapine takes a third route entirely: it blocks presynaptic alpha-2 receptors, which signals the brain to release more norepinephrine and serotonin all at once.
That mechanism is the reason mirtazapine often produces sedation and weight gain, where SSRIs more commonly produce activation, GI upset, and sexual side effects. Patients commonly ask us why their psychiatrist suggested mirtazapine instead of the usual Zoloft or Lexapro. The receptor difference is the short answer.
Table 1: Mirtazapine vs Common US Antidepressants
| Drug | Class | Typical Daily Dose (Adult) | Top Side Effect Concern | Best-Fit Patient Profile |
| Mirtazapine (Remeron) | Tetracyclic / NaSSA | 15 to 45 mg | Drowsiness, weight gain | Depression with insomnia or appetite loss |
| Sertraline (Zoloft) | SSRI | 50 to 200 mg | GI upset, sexual side effects | First-line MDD, anxiety, OCD, PTSD |
| Escitalopram (Lexapro) | SSRI | 10 to 20 mg | Nausea, sexual side effects | First-line MDD and generalized anxiety |
| Fluoxetine (Prozac) | SSRI | 20 to 80 mg | Insomnia, activation | Depression with low energy; long half-life |
| Venlafaxine (Effexor XR) | SNRI | 75 to 225 mg | Blood pressure rise, withdrawal | Depression with chronic pain |
| Bupropion (Wellbutrin XL) | NDRI | 150 to 450 mg | Insomnia, lower seizure threshold | Depression with low motivation, weight concerns |
Source: FDA-approved prescribing information and Drugs.com.
How Mirtazapine Works in the Brain
Most antidepressants either block serotonin reuptake or stop the recycling of both serotonin and norepinephrine. Mirtazapine does neither. Instead, it blocks specific receptors that normally apply the brakes to monoamine release.
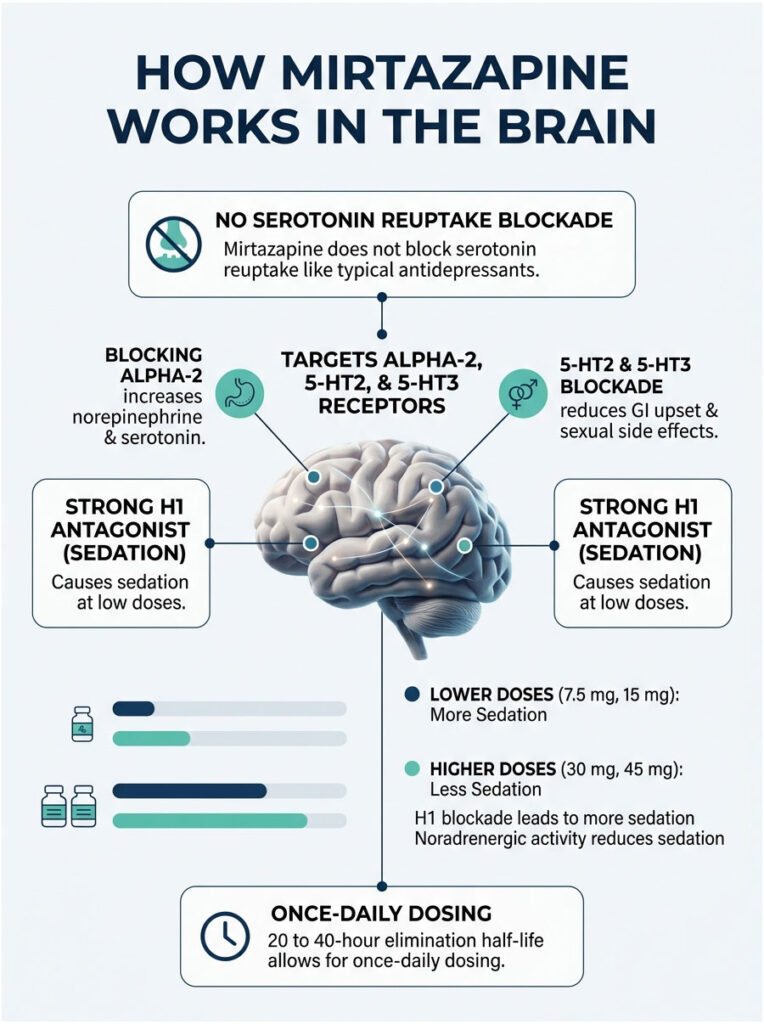
The headline targets are alpha-2 adrenergic autoreceptors, plus the 5-HT2 and 5-HT3 serotonin receptors. Blocking the alpha-2 receptor increases both norepinephrine and serotonin in synapses. Blocking 5-HT2 and 5-HT3 also reduces the GI upset and sexual side effects that mark the SSRI class (NCBI StatPearls).
The Receptor Story (Alpha-2, 5-HT2, 5-HT3, H1)
A fourth target matters just as much for daily life: the histamine H1 receptor. Mirtazapine is a strong H1 antagonist, which is why it causes sleepiness, particularly at low doses. The same H1 effect drives much of the appetite increase patients notice in week one.
In tests reviewed by our pharmacology team, this H1 blockade explains why 7.5 mg and 15 mg doses can feel more sedating than 30 mg or 45 mg. Patients commonly ask us why their doctor raised the dose to make them less sleepy. The receptor math holds the answer.
Why It Sedates at Low Doses but Less at Higher Doses
At doses under 15 mg, H1 blockade dominates the clinical picture, producing strong sedation. At 30 mg and above, noradrenergic activity rises and partially offsets the antihistamine drowsiness. That is why prescribers sometimes counterintuitively raise the dose to reduce next-day grogginess.
Mirtazapine’s elimination half-life runs about 20 to 40 hours, which supports once-daily dosing without missed-dose anxiety. It is metabolized in the liver mainly through the CYP2D6, CYP3A4, and CYP1A2 enzymes, a detail that matters when patients take other drugs processed by the same enzymes.
What Mirtazapine Is Used to Treat
Major depressive disorder is the only FDA-approved use in the United States, but real-world prescribing covers a wider range. According to a CDC NCHS Data Brief published in April 2025, 11.4% of US adults took prescription medication for depression in 2023, with women using antidepressants at more than twice the rate of men.
That demand fuels heavy use of mirtazapine in both psychiatry and primary care. Across patients booking depression-related diagnostic panels through HealthCareOnTime, mirtazapine appears in medication histories alongside SSRIs and trazodone more often than any other tetracyclic agent.

FDA-Approved Use: Major Depressive Disorder
The FDA label authorizes mirtazapine for the treatment of major depressive disorder in adults. The original US clinical trials showed efficacy comparable to other first-line antidepressants, with the strongest separation from placebo seen on sleep, appetite, and anxiety symptoms (FDA Remeron label).
Mirtazapine is not FDA-approved for children or teens. The boxed warning specifically flags increased suicidal thinking in patients aged 24 and younger, a point any prescriber should review with the patient and family before starting therapy. Adolescent prescribing in the US happens, but always off-label and usually after psychotherapy and an SSRI trial have been considered.
Common Off-Label Uses in US Practice
A 2024 update of the NCBI Mirtazapine monograph lists several off-label indications used regularly by US prescribers (StatPearls):
- Insomnia, especially when paired with depression or anxiety
- Generalized anxiety disorder and panic disorder
- Post-traumatic stress disorder (PTSD)
- Obsessive-compulsive disorder (OCD) as augmentation
- Cancer-related anorexia and cachexia, where weight gain is desirable
- Appetite loss in older adults, often in long-term care settings
- Migraine prophylaxis in selected cases
- Hot flashes in patients who cannot take hormone therapy
A 2025 medRxiv preprint reported that many off-label prescriptions are written at low doses, around 8 to 11 mg daily, where sedation predominates and the antidepressant effect is weaker (medRxiv September 2025). Our medical team flags this trend because patients sometimes assume low-dose mirtazapine is treating their depression when it is mostly working as a sleep aid.
Mirtazapine Dosage Guide
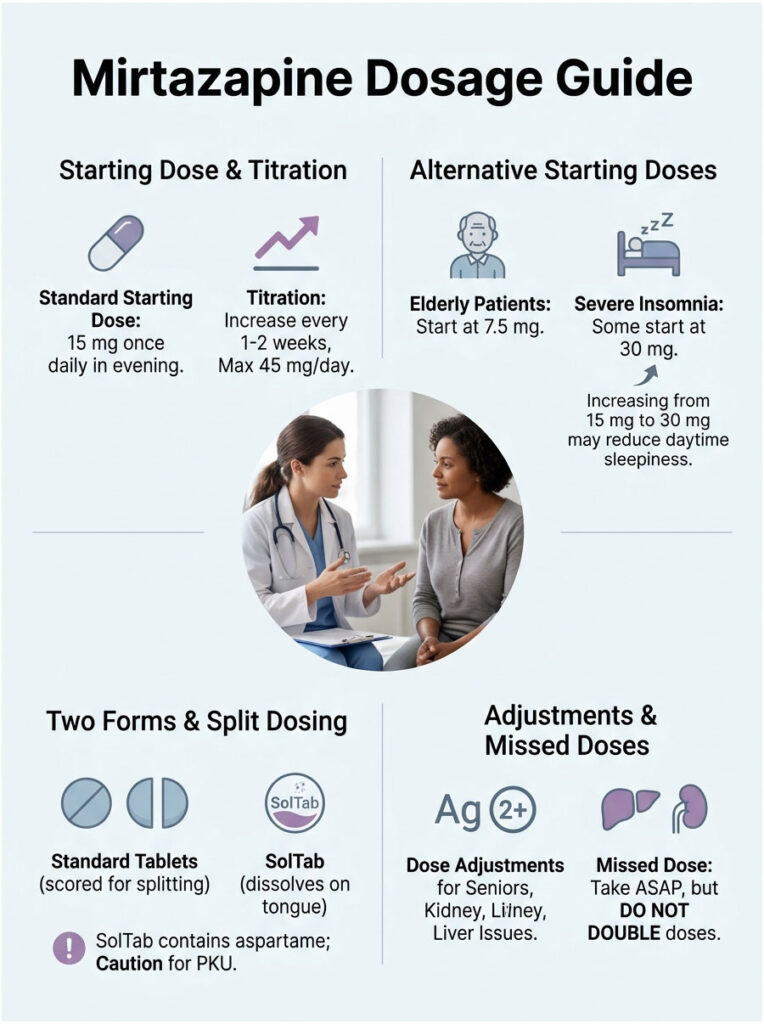
The standard adult starting dose for major depressive disorder is 15 mg once daily, taken in the evening before bedtime. From there, the prescriber may increase the dose every one to two weeks based on response, up to a maximum of 45 mg per day (Drugs.com prescribing information).
Starting Dose, Titration, and Maximum
A typical US titration pattern looks like this:
- Week 1 to 2: 15 mg at bedtime
- Week 3 to 4: 30 mg at bedtime if response is partial
- Week 5 and beyond: 45 mg at bedtime only if 30 mg has not produced full remission
Some US prescribers start at 7.5 mg in elderly or unusually sensitive patients, then move to 15 mg after a few nights. Others jump straight to 30 mg in patients with severe insomnia who want the noradrenergic offset to kick in faster and reduce next-day drowsiness.
A key clinical pearl: counterintuitively, increasing the dose from 15 mg to 30 mg often makes patients less sleepy during the day, not more. The added norepinephrine activity at the higher dose cancels some of the histamine sedation. Our medical reviewers see this surprise patients regularly.
Forms: Tablets vs Orally Disintegrating Tablets (SolTab)
Standard mirtazapine tablets are scored and easy to split, which helps with custom titration. The SolTab form dissolves on the tongue within 30 seconds and does not require water, which suits patients with swallowing difficulty, severe nausea, or unpredictable travel schedules. Both forms carry the same FDA indications, warnings, and dose ranges.
One important note: the SolTab contains aspartame, which patients with phenylketonuria (PKU) must avoid. Mayo Clinic explicitly calls out this risk on its mirtazapine drug page (Mayo Clinic).
Dose Adjustments for Seniors, Kidney, and Liver Issues
Older adults often clear mirtazapine more slowly, which raises blood levels and the risk of sedation, dizziness, and falls. Many US geriatric protocols start at 7.5 mg to 15 mg and titrate cautiously over four to six weeks.
Patients with moderate to severe liver disease may need lower doses because mirtazapine is extensively processed by the liver. Renal impairment (GFR under 40 mL/min) also reduces clearance and warrants caution per the StatPearls monograph. Patients commonly ask us whether they need a blood test before starting; the answer is no for most healthy adults, but baseline liver enzymes and a kidney panel are reasonable for older or medically complex patients.
What to Do If You Miss a Dose
If a dose is missed, take it as soon as possible, unless it is close to the next scheduled dose. Never double up to make up for a missed dose. Drugs.com and the FDA medication guide both stress this point, because doubling raises the risk of next-day sedation, dizziness, and falls.
Mirtazapine Side Effects: What to Expect
Most mirtazapine side effects show up in the first one to two weeks and improve as the body adjusts. A minority cause persistent trouble, often weight gain, daytime drowsiness, or dry mouth, that may prompt a dose adjustment or a switch.
Patients commonly ask us how mirtazapine compares to SSRIs on side effects. The honest answer is that mirtazapine trades one set of problems (insomnia, sexual side effects, GI upset) for another (sedation, increased appetite, weight gain). Which trade is better depends entirely on the patient sitting in the prescriber’s chair.
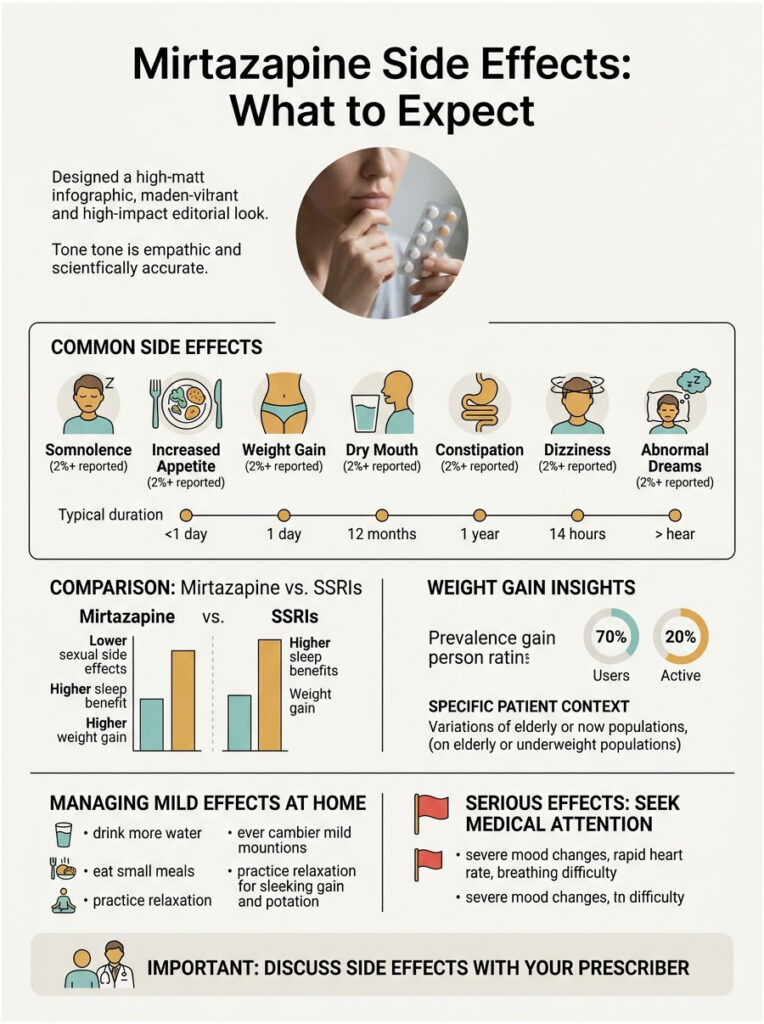
Common Side Effects (Reported in 2%+ of Trials)
The numbers below come directly from the FDA Remeron label, which summarizes the original US placebo-controlled clinical trials. Our editorial team has cross-checked these against the current DailyMed and Drugs.com prescribing data.
Table 2: Mirtazapine Side Effect Frequencies vs Placebo (US Clinical Trials)
| Side Effect | Mirtazapine % | Placebo % |
| Somnolence (sleepiness) | 54% | 18% |
| Increased appetite | 17% | 2% |
| Weight gain (≥7% body weight) | 12% | 2% |
| Dry mouth | 25% | 15% |
| Constipation | 13% | 7% |
| Dizziness | 7% | 3% |
| Abnormal dreams | 4% | 1% |
Source: FDA Remeron prescribing information and Drugs.com mirtazapine label.
Managing the Common Side Effects at Home
Many of the milder mirtazapine side effects respond well to simple adjustments before they require any change in the prescription:
- For drowsiness: take the dose 30 to 60 minutes before bed; avoid driving the morning after the first few doses; ask the prescriber about moving from 15 mg to 30 mg if daytime grogginess persists past two weeks
- For dry mouth: increase water intake, use sugar-free gum or lozenges, consider an alcohol-free mouthwash; flag any persistent dry mouth to a dentist since it raises cavity risk
- For constipation: increase fiber and water; consider a stool softener like docusate if symptoms persist beyond a week
- For increased appetite: plan meals in advance, keep high-calorie snacks out of easy reach in the evening, prioritize protein and fiber to feel full longer
In cases reviewed by our medical team, patients who set up these home strategies in the first week often avoid the dose changes that would otherwise be triggered by uncomfortable but manageable side effects.
Serious Side Effects That Need a Doctor
Several rarer effects require prompt medical attention. The FDA label and the DailyMed mirtazapine entry list these warnings:
- Agranulocytosis: a sudden drop in white blood cells, signaled by fever, chills, sore throat, or mouth sores. Reported rarely but life-threatening if missed.
- Serotonin syndrome: agitation, sweating, rapid heartbeat, and confusion, more likely when mirtazapine is combined with other serotonergic drugs.
- Seizures: mirtazapine slightly lowers the seizure threshold; use cautiously in patients with epilepsy.
- Hyponatremia: low blood sodium, more common in older adults and patients on diuretics.
- Suicidal thoughts: highest risk in patients under 25, particularly in the first weeks of treatment.
Any of these symptoms warrants a call to the prescriber, or, in the case of suicidal thoughts, the 988 Suicide and Crisis Lifeline.
The Weight Gain Question, Answered Honestly
Weight gain is the side effect patients ask about most often. The clinical trial number is 12%, but real-world data tells a fuller story. A SingleCare clinical review summarized post-marketing data showing that meaningful weight gain may affect 20% to 40% of long-term users.
A 2001 study found that 21% of self-reported weight gain happened in the first 12 weeks of treatment (SingleCare). A K Health pharmacist review reported that about 8% of mirtazapine users discontinued the drug specifically because of weight gain.
For underweight patients, depressed seniors, or cancer patients with cachexia, that appetite boost is often the goal, not a problem. Our medical team sees this pattern frequently in patients also undergoing nutritional panels and basic metabolic workups.
Boxed Warnings and Safety Precautions
The FDA requires a black box warning on all mirtazapine packaging in the United States. This is the most serious warning level the agency issues and applies to the entire class of antidepressants approved in the US.
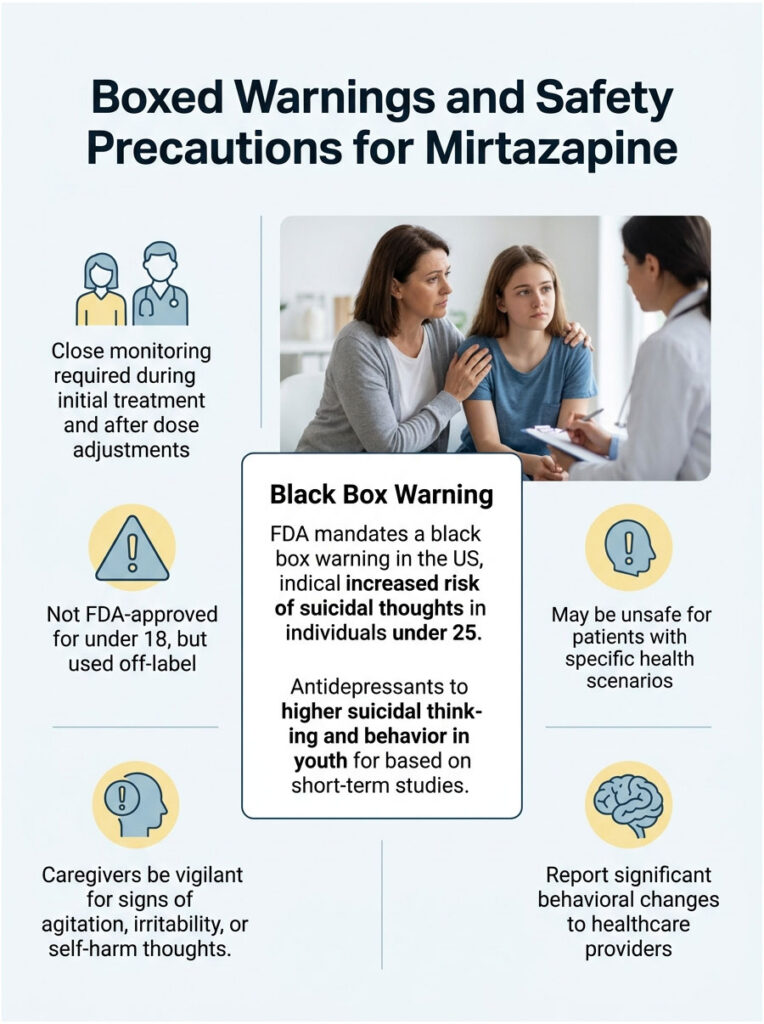
The FDA Black Box: Suicidal Thoughts in People Under 25
Short-term studies showed that antidepressants increased the risk of suicidal thinking and behavior in pediatric and young adult patients with depression and other psychiatric disorders. The warning instructs prescribers to monitor closely for clinical worsening, especially during the first few weeks of treatment and after any dose change (FDA Mirtazapine ODT label).
Mirtazapine is not FDA-approved for patients under 18, although prescribers occasionally use it off-label in adolescents. Families and caregivers should be told to watch for new agitation, irritability, or talk of self-harm and to report changes promptly.
Who Should Not Take Mirtazapine
Several scenarios make mirtazapine a poor or unsafe choice:
- Recent MAOI use: at least 14 days must pass between stopping an MAOI and starting mirtazapine, and the same gap applies in reverse, due to serotonin syndrome risk
- Known mirtazapine or excipient allergy: serious skin reactions, including Stevens-Johnson syndrome, have been reported rarely
- Phenylketonuria (PKU): the SolTab orally disintegrating form contains aspartame
- Untreated narrow-angle glaucoma: mirtazapine can dilate pupils
- Active mania or bipolar disorder: antidepressants alone may trigger mixed or manic episodes
- Caution required: seizure disorder, significant liver or kidney disease, recent heart attack, or known QT prolongation
Drug Interactions and Things to Avoid
Mirtazapine’s interaction profile is narrower than the SSRIs but still meaningful. Sharing a complete medication list with the prescriber and pharmacist remains the single best way to catch trouble early.
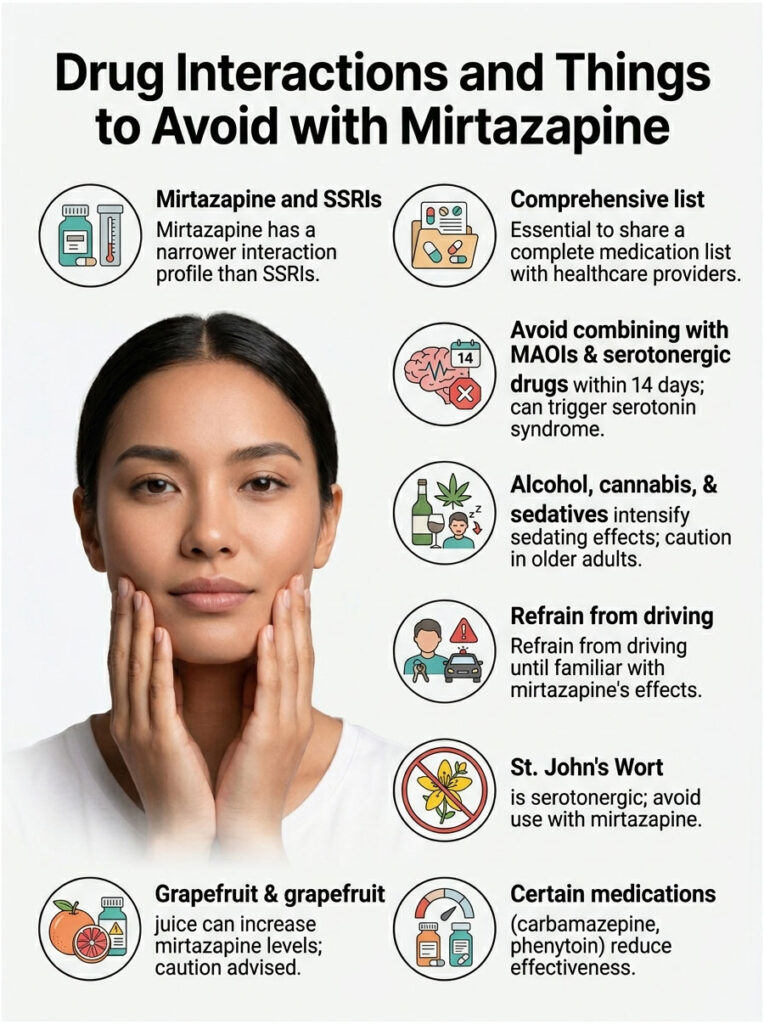
Dangerous Combinations (MAOIs, Serotonergic Drugs)
MAOIs and mirtazapine should never be combined within a 14-day window. The combination can trigger serotonin syndrome, a medical emergency. The same caution applies to other strongly serotonergic agents: tramadol, fentanyl, lithium, triptans for migraine, tricyclic antidepressants, buspirone, and tryptophan supplements (FDA AccessData Remeron label).
Linezolid (an antibiotic) and intravenous methylene blue also have MAOI-like activity and carry the same risk. Prescribers will usually avoid these combinations or hold mirtazapine if antibiotic treatment is urgent.
Alcohol, Cannabis, and Sedatives
Alcohol intensifies mirtazapine’s sedating effects and worsens next-day grogginess. Cannabis and other CNS depressants (benzodiazepines, opioids, sleep medications, antihistamines like diphenhydramine) layer on the same way and raise fall risk, particularly in older adults.
Patients should not drive or operate machinery until they know how mirtazapine affects them. The first two weeks are usually the strongest sedation window. In tests booked through HealthCareOnTime, our team sometimes sees liver enzyme bumps in patients combining heavy alcohol use with mirtazapine, another reason moderation matters.
Foods and Supplements (St. John’s Wort, Grapefruit)
St. John’s Wort is a herbal serotonergic agent and should be avoided alongside mirtazapine. Grapefruit and grapefruit juice can inhibit CYP3A4, the enzyme that helps clear mirtazapine, which may raise blood levels and side effects. Carbamazepine, phenytoin, and rifampin do the opposite, inducing CYP3A4 and reducing mirtazapine levels enough that the dose may need to be raised.
How Long Does Mirtazapine Take to Work?
Sleep and appetite often improve within the first three to seven days. Mood and energy take longer, usually two to four weeks for the first signs and six to eight weeks for full effect. The FDA label tells prescribers to reassess if symptoms have not improved after four weeks of treatment (Drugs.com).
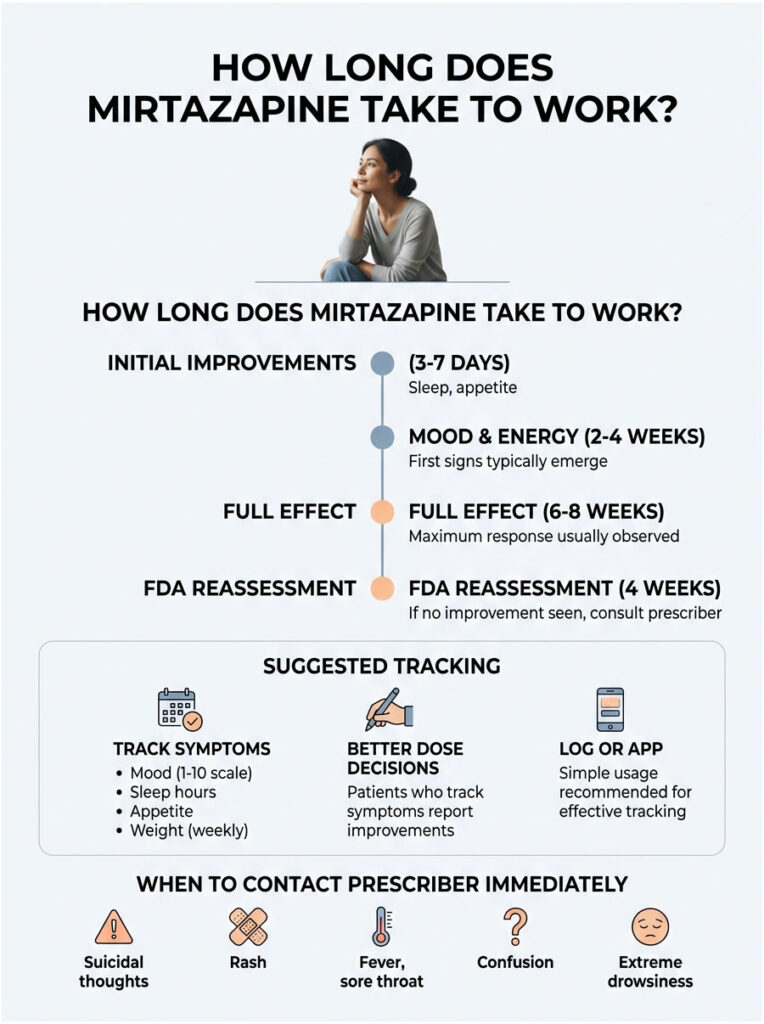
Week-by-Week Realistic Expectations
A typical patient timeline looks like this:
- Day 1 to 7: Sleep improves, appetite returns, sometimes strong daytime drowsiness
- Week 2 to 3: Anxiety eases, irritability softens, sleep becomes more consistent
- Week 4 to 6: Mood lifts, motivation slowly returns, side effects often stabilize
- Week 6 to 8: Full antidepressant effect; prescriber assesses whether to hold dose or adjust
What to Track and When to Call the Prescriber
A simple log of mood (1 to 10), sleep hours, appetite, weight (weekly), and any side effects helps prescribers tune the dose. Call the prescriber sooner if suicidal thoughts emerge, if a rash appears, if fever or sore throat develop, or if confusion or extreme drowsiness disrupt daily function.
In cases reviewed by our medical team, patients who track symptoms in a notebook or simple app report better dose decisions and a faster route to remission than those who rely on memory alone at the next visit.
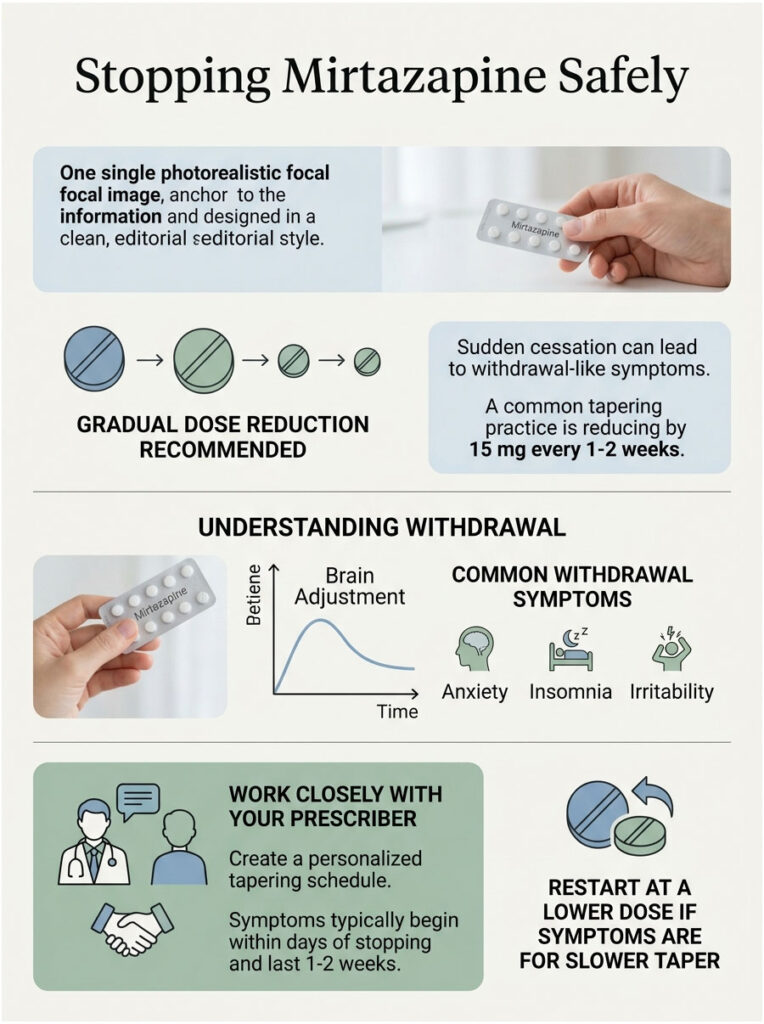
Stopping Mirtazapine Safely
Mirtazapine should not be stopped suddenly. The FDA label specifically recommends gradual dose reduction rather than abrupt cessation, to lower the chance of discontinuation symptoms (MedCentral monograph).
Why You Should Not Stop Cold Turkey
The brain adapts to mirtazapine’s receptor effects over weeks of treatment. Pulling the drug suddenly leaves those adaptations stranded, which produces a withdrawal-like syndrome that can feel worse than the original depression for several days.
Withdrawal Symptoms to Expect
Reported discontinuation symptoms include:
- Dizziness and lightheadedness
- Nausea or vomiting
- Anxiety, agitation, or irritability
- Vivid or disturbing dreams
- Sensory disturbances (paresthesia, electric-shock sensations)
- Headache, tremor, sweating
- Fatigue and confusion
Symptoms usually start within a few days of stopping and last one to two weeks. They are not dangerous in most cases, but they are uncomfortable and easy to confuse with a relapse of the original depression.
Tapering Schedule Used in US Practice
There is no single FDA-mandated taper, but a common US practice is to reduce by 15 mg every one to two weeks. A patient on 45 mg may step down to 30 mg, then 15 mg, then 7.5 mg, then stop. Patients sensitive to changes may need a slower taper of 7.5 mg every two to four weeks.
Anyone considering stopping should coordinate the schedule with the prescriber. Restarting briefly and tapering more slowly is a normal adjustment if withdrawal symptoms become hard to tolerate, and prescribers expect this kind of fine-tuning.
Is Mirtazapine Right for You? A Practical Decision Framework
Mirtazapine shines in specific clinical scenarios and falls short in others. The table below maps the most common situations our medical team encounters in US patient histories, and it is meant to start the conversation with a prescriber, not replace it.
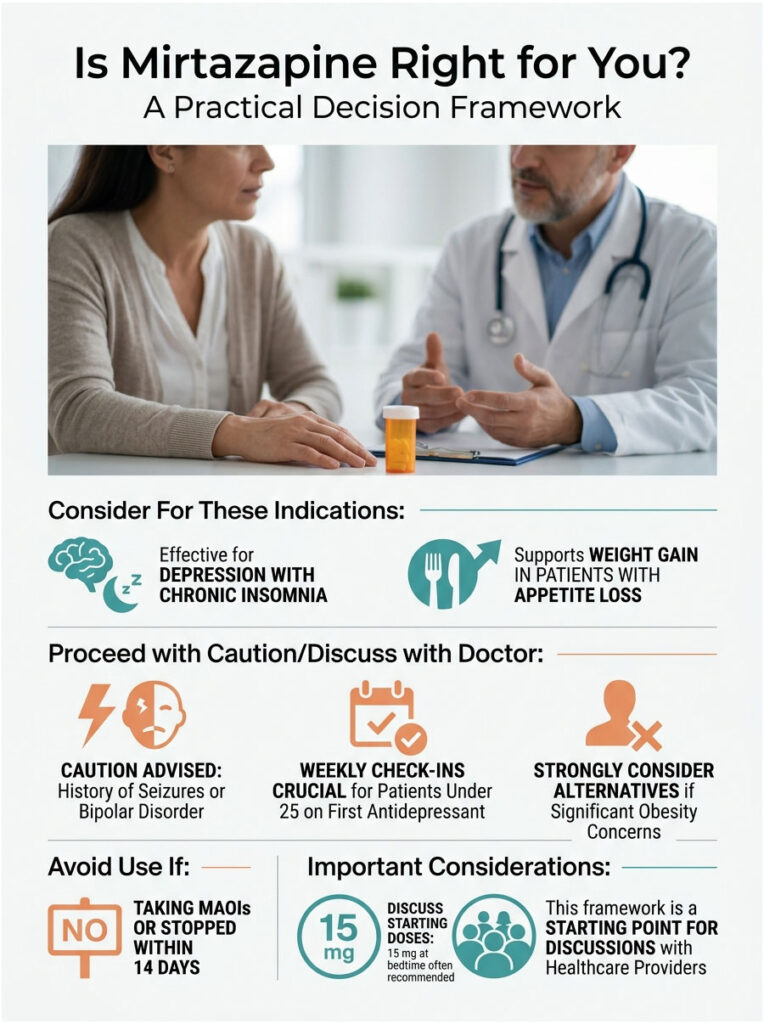
Table 3: Scenario / Recommended Action
| Patient Scenario | Mirtazapine Fit | Suggested Next Step |
| Depression plus chronic insomnia | Strong fit | Discuss 15 mg starting dose at bedtime with prescriber |
| Depression plus appetite loss or low BMI | Strong fit | Mention weight loss history; ask about 15 mg start |
| Adult under 25 starting first antidepressant | Possible fit with monitoring | Set weekly check-ins for first 4 weeks; family awareness |
| Depression plus significant obesity concern | Weak fit | Ask about bupropion or fluoxetine as alternatives |
| Currently taking MAOI or stopped within 14 days | Not appropriate | Wait full 14-day washout before any switch |
| History of seizures or untreated bipolar disorder | Use with caution | Ask prescriber about safer class options |
The strongest fits for mirtazapine in US practice are patients whose depression rides alongside insomnia, anxiety, or weight loss. The weakest fits are patients already struggling with obesity, daytime fatigue from another cause, or unstable bipolar disorder.
Mirtazapine Cost in the US: Generic vs Brand
Generic mirtazapine is widely available across US pharmacies and is usually one of the most affordable antidepressant options. With a pharmacy discount card like GoodRx or SingleCare, a 30-tablet supply of generic 15 mg or 30 mg often runs $10 to $20 cash price at major chains like CVS, Walgreens, Walmart, and Kroger.
Brand-name Remeron and Remeron SolTab cost significantly more, often $250 to $400 for a 30-day supply at cash price. Most US insurance plans, including Medicare Part D, cover generic mirtazapine on the lowest tier, which usually means a copay of $0 to $10.
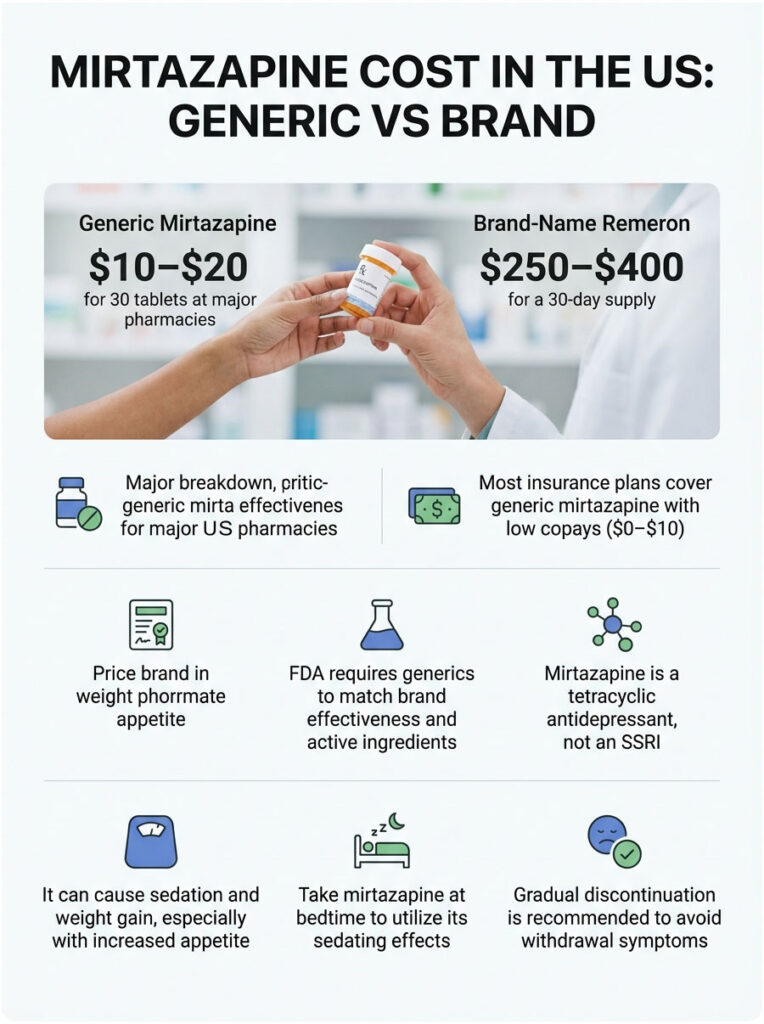
Patients sometimes ask us why their pharmacist offers the generic instead of the brand. The answer is that the FDA requires generics to demonstrate the same active ingredient, strength, and bioavailability as the brand. For nearly every patient, generic mirtazapine works identically to Remeron.
Frequently Asked Questions
Is mirtazapine an SSRI?
No. Mirtazapine is a tetracyclic antidepressant in the NaSSA subgroup, which works by blocking alpha-2 adrenergic and certain serotonin receptors instead of blocking serotonin reuptake the way SSRIs do. That difference explains why mirtazapine causes sedation and weight gain instead of the activation and sexual side effects that SSRIs are known for.
Why is mirtazapine prescribed at bedtime?
Mirtazapine strongly blocks histamine H1 receptors, which produces sleepiness. Taking it at bedtime turns that side effect into a benefit, helping patients fall asleep faster and stay asleep longer. Morning dosing usually leads to daytime drowsiness, especially during the first two weeks of treatment when the H1 effect is strongest.
Can mirtazapine cause weight gain?
Yes. In clinical trials, about 12% of patients gained 7% or more of their body weight, and real-world studies suggest 20% to 40% of long-term users experience meaningful weight gain. The drug increases appetite, particularly cravings for carbohydrates, and slows metabolic rate. Tracking weight weekly from day one helps catch early changes.
How long can you safely take mirtazapine?
Mirtazapine can be taken long-term, often for months or years, if depression remains in remission and side effects stay manageable. The FDA label recommends periodic reassessment of whether continued treatment is still needed. Many US patients stay on it for one to two years after remission to lower relapse risk.
Does mirtazapine help with anxiety?
Yes, although it is not FDA-approved for anxiety alone. Mirtazapine often eases anxiety symptoms in patients whose depression is mixed with anxiety, partly through its serotonin 5-HT2 blockade. Off-label use for generalized anxiety disorder and panic disorder is common in US psychiatric practice, usually at standard antidepressant doses.
Can you drink alcohol while on mirtazapine?
It is best avoided. Alcohol amplifies mirtazapine’s sedating effects and impairs judgment, coordination, and memory more than either substance alone. Heavy or chronic drinking also worsens depression and can interact with the liver enzymes that process mirtazapine. Light, occasional use should be discussed with the prescriber.
Is mirtazapine the same as Remeron?
Yes, in the same way that ibuprofen is the same as Advil. Mirtazapine is the generic name; Remeron is the original US brand name approved by the FDA in 1996. Remeron SolTab is the orally disintegrating tablet version. Generic mirtazapine and brand Remeron contain the same active drug at the same strength.
How long does mirtazapine take to work?
Sleep and appetite often improve within the first week. Mood, energy, and motivation take longer, usually two to four weeks for early signs and six to eight weeks for full effect. The FDA label tells prescribers to reassess if symptoms have not improved after four weeks at an adequate dose.
Does mirtazapine cause memory problems?
Mild forgetfulness or fuzzy thinking can occur, especially during the sedating early weeks and in older adults. These effects usually fade as the body adjusts. Persistent or worsening memory issues should be reported to the prescriber, since they may signal a dose that is too high, an interaction, or another medical cause.
Can mirtazapine be used for sleep alone?
Some US prescribers use low-dose mirtazapine (7.5 mg or 15 mg) off-label for insomnia, particularly in patients with depression or anxiety. A 2025 medRxiv preprint flagged that subtherapeutic dosing is widespread but does not produce a full antidepressant effect. Patients should know whether the prescription is targeting sleep alone or both sleep and mood.
What happens if you stop mirtazapine suddenly?
Sudden discontinuation can trigger withdrawal-like symptoms including dizziness, nausea, anxiety, vivid dreams, headache, tremor, and electric-shock sensations. The FDA label recommends gradual tapering. A common US schedule reduces the dose by 15 mg every one to two weeks under prescriber supervision.
Is mirtazapine safe during pregnancy?
Mirtazapine was historically rated FDA pregnancy category C, meaning animal studies showed some risk but human data are limited. Use during pregnancy is decided case by case, weighing the risk of untreated depression against potential drug exposure. Patients who are pregnant, planning pregnancy, or breastfeeding should consult their prescriber and OB before any change.
Disclaimer: This article is educational and does not replace personalized medical advice. Mirtazapine is a prescription medication that requires evaluation, dosing, and monitoring by a licensed US healthcare provider. If you or someone you know is having thoughts of suicide, call or text 988 to reach the Suicide and Crisis Lifeline, or call 911 in an emergency. Report side effects to FDA MedWatch at 1-800-FDA-1088 or www.fda.gov/medwatch.
References
- FDA AccessData: Remeron (mirtazapine) Tablets Prescribing Information
- DailyMed: Mirtazapine Tablet, Film Coated Label
- NCBI StatPearls: Mirtazapine Monograph
- Drugs.com: Mirtazapine Uses, Dosage and Side Effects
- Drugs.com Professional: Mirtazapine Tablets Prescribing Information
- Mayo Clinic: Mirtazapine (Oral Route)
- CDC NCHS Data Brief 528 (April 2025): Antidepressant Use Among US Adults
- FDA: Mirtazapine (marketed as Remeron) Information
- SingleCare: Mirtazapine Weight Gain Clinical Review
- MedCentral: Mirtazapine Oral Monograph





