Here’s something that catches a lot of people off guard: you can have a flagged MCHC on your lab report and feel completely fine. That little “L” or “H” beside the number sends plenty of Americans straight to a search bar, worried they’ve missed something serious. Most of the time, the real story is calmer than it looks.
Table of Contents
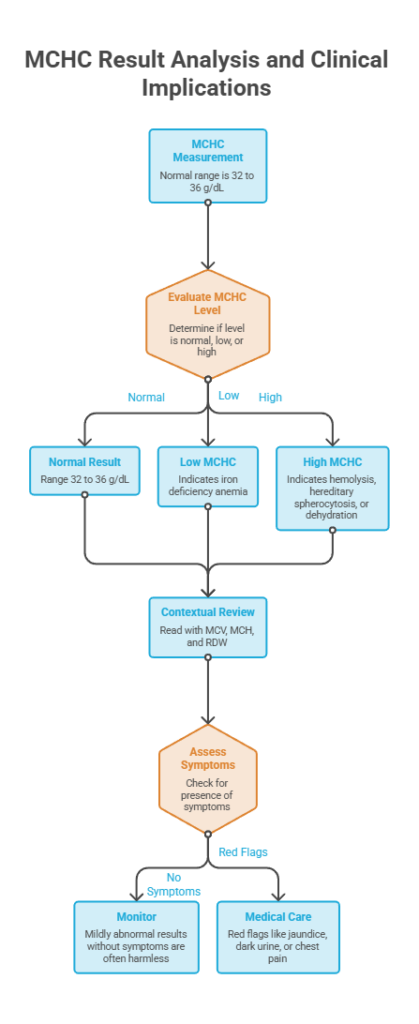
Quick Answer: MCHC (mean corpuscular hemoglobin concentration) measures the average concentration of hemoglobin packed inside your red blood cells. The normal range is about 32 to 36 g/dL. A low MCHC usually points to iron deficiency anemia, while a high MCHC is less common and can signal hereditary spherocytosis, hemolysis, dehydration, or a lab artifact. On its own, MCHC never makes a diagnosis. Doctors read it alongside the rest of your CBC.
At a Glance
- Normal MCHC runs about 32 to 36 g/dL, though labs vary slightly.
- Low MCHC most often means iron deficiency anemia.
- High MCHC is rarer and can point to hemolysis, hereditary spherocytosis, or dehydration.
- MCHC is one of several red blood cell indices, read together with MCV, MCH, and RDW.
- A mildly abnormal result with no symptoms is often harmless.
- Red flags like jaundice, dark urine, or chest pain need prompt medical care.
- Most causes of an abnormal MCHC are treatable once the reason is found.
What Is MCHC on a Blood Test?
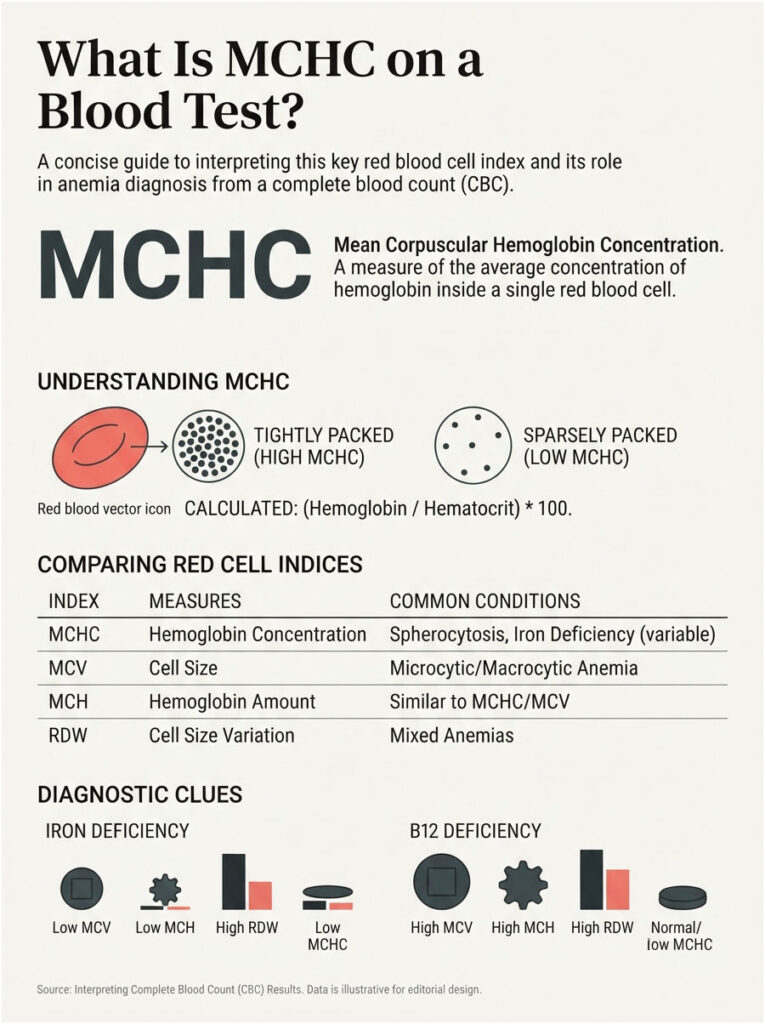
MCHC stands for mean corpuscular hemoglobin concentration. It tells you how tightly hemoglobin, the iron-rich protein that carries oxygen, is packed inside an average red blood cell.
Picture each red blood cell as a small delivery truck. MCHC doesn’t count the trucks or measure their size. It measures how full each truck is with cargo, relative to how much room it has.
This value appears automatically on a complete blood count (CBC), one of the most frequently ordered lab tests in the United States. You don’t request MCHC on its own; it arrives bundled with your CBC.
Among the routine blood panels booked through HealthCareOnTime, MCHC is one of the values patients most often ask about, precisely because it sounds technical and shows up flagged without explanation. The short version: it helps your doctor sort out what kind of anemia might be present, which points toward the right fix.
How MCHC Is Calculated
In most labs, MCHC isn’t measured directly. It’s derived from two other CBC values through a simple relationship.
The formula divides your hemoglobin by your hematocrit, then multiplies by 100. Hematocrit is the share of your blood volume made up of red cells, so MCHC reflects hemoglobin content per unit of packed red cells.
Because it’s a calculated ratio, an odd MCHC can sometimes trace back to a measurement quirk rather than a genuine blood problem. That distinction is a big part of why doctors often repeat an unusual result before acting on it.
MCHC vs MCH vs MCV: Clearing Up the Confusion
These three abbreviations look nearly identical, and mixing them up is easy. Each one describes a different feature of your red blood cells.
MCV (mean corpuscular volume) measures the average size of a red cell. MCH (mean corpuscular hemoglobin) measures the average amount of hemoglobin per cell. MCHC measures the concentration, meaning hemoglobin amount relative to cell size.
A coffee analogy makes it stick. MCV is the size of the cup. MCH is how much coffee is inside. MCHC is how strong that coffee tastes. Two cups can hold the same amount of coffee yet taste completely different in strength.
Where MCHC Sits in Your CBC
Your CBC reports red cell count, hemoglobin, hematocrit, and a cluster of indices including MCV, MCH, MCHC, and RDW (red cell distribution width). Read together, these numbers tell a fuller story than any single figure.
MCHC rarely stands out as the headline result. The hematologists who guide our lab reporting treat it as a supporting clue that sharpens the diagnosis once hemoglobin or MCV is already flagged.
The table below shows how the indices combine to suggest a likely cause. This pattern-reading is the part most quick articles skip, and it’s exactly where the real diagnostic value lives.
| MCV (Size) | MCH (Amount) | MCHC (Conc.) | RDW (Variation) | Likely Pattern |
| Low | Low | Low | High | Iron deficiency anemia |
| Low | Low | Low or normal | Normal | Thalassemia trait |
| Normal | Normal | Normal | Normal | No anemia or early chronic disease |
| High | High | Normal | High | B12 or folate deficiency (macrocytic) |
| Low | Low | High | Normal/high | Hereditary spherocytosis |
| Normal/high | Normal | High | High | Autoimmune hemolytic anemia |
MCHC Normal Range: What Counts as Low or High
For most adults, a normal MCHC falls between 32 and 36 g/dL. Some labs use a slightly tighter window, and the American Board of Internal Medicine lists 33 to 36 g/dL as its reference.
Below roughly 32 g/dL is generally considered low, a state called hypochromia. Above about 36 g/dL is considered high, and it turns up far less often in everyday practice.
Always read your result against the reference range printed on your report. Different labs calibrate their equipment differently, so a value flagged at one facility might sit comfortably inside the range at another.
Does MCHC Differ by Age or Sex?
Unlike hemoglobin, which has clearly different cutoffs for men, women, and children, MCHC ranges stay fairly steady across adults. The 32 to 36 g/dL window applies broadly regardless of sex.
Newborns and infants can run a touch higher, and certain inherited conditions shift the number from birth. For the typical adult reading a routine panel, the standard range is what counts.
A common question we field is whether the normal MCHC for a woman differs from the male range. In practice, it barely moves. What differs between the sexes is how often low values appear, driven largely by menstrual blood loss.
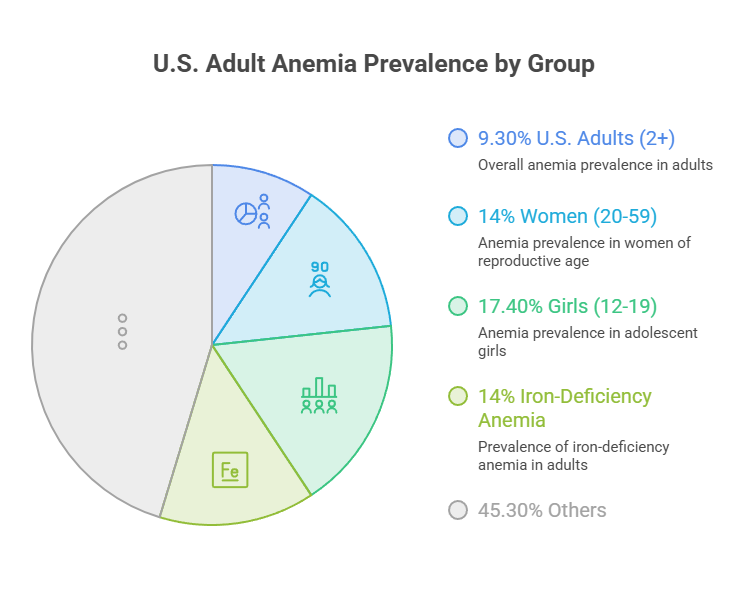
The numbers below put American anemia and iron patterns in context. These figures come straight from federal health surveys and national nutrition data.
| Statistic | Figure | Source |
| US anemia prevalence (age 2+) | 9.3% | CDC / NHANES 2021–2023 |
| Anemia in women ages 20 to 59 | 14.0% | CDC / NHANES 2021–2023 |
| Anemia in girls ages 12 to 19 | 17.4% | CDC / NHANES 2021–2023 |
| US adults with iron-deficiency anemia | About 14% | NHANES / StatPearls |
| Americans with iron-deficiency anemia yearly | 4 to 5 million | Harvard Nutrition Source |
| Iron RDA, women ages 19 to 50 | 18 mg/day | NIH, Dietary Iron |
Why Is Your MCHC Low? Causes & Symptoms
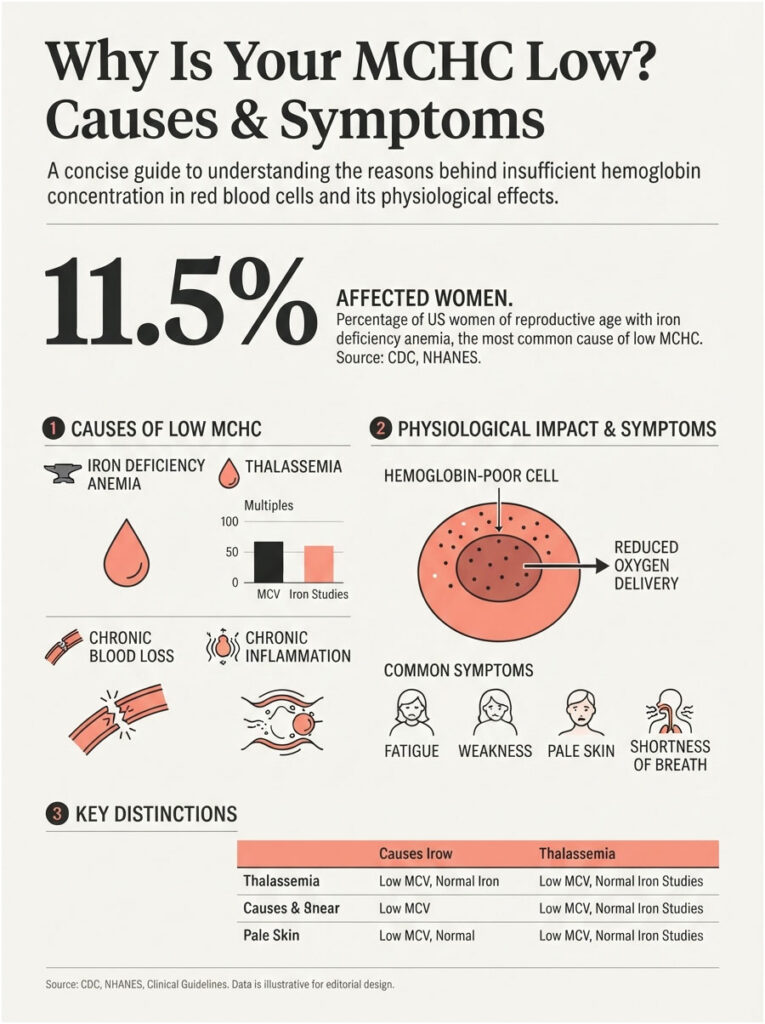
A low MCHC means your red blood cells carry less hemoglobin than they should for their size. When cells look pale and under-filled under a microscope, hematologists call them hypochromic.
Most of the time, one culprit sits at the top of the list. Getting to that cause quickly is what turns a scary lab flag into a manageable fix.
Iron Deficiency Anemia
Iron deficiency is far and away the most common reason for a low MCHC. Without enough iron, your body can’t build hemoglobin properly, so each red cell ends up short on cargo.
This is a large problem in the US. CDC and NHANES data show anemia rising among women of reproductive age, climbing from 7.8% in 2000 to 11.5% in 2018, with adolescent girls and women in their childbearing years carrying the heaviest load.
The classic laboratory picture is low MCHC paired with low MCV and low MCH, the microcytic hypochromic pattern. Of all the low-MCHC reports processed across our diagnostic network, this trio is the single most frequent reason the value gets flagged.
Thalassemia and Genetic Causes
Thalassemia is an inherited condition that affects how the body makes hemoglobin. It can produce small, pale red cells that mimic iron deficiency on a CBC, sometimes with a low or low-normal MCHC.
The tell-tale difference: in thalassemia trait, MCV often runs quite low while the red cell count stays relatively high, and iron studies come back normal. That combination is a clue your doctor watches for.
This matters because treating thalassemia with iron supplements won’t help and can cause harm through iron overload. It’s a prime example of why the cause behind a low MCHC needs to be pinned down, not assumed.
Chronic Blood Loss and Inflammation
Slow, steady blood loss drains iron over time. Heavy menstrual periods, bleeding ulcers, and other digestive sources can quietly deplete your stores long before you notice symptoms, UPMC clinicians point out.
Chronic inflammation adds a second twist. Long-term infections, autoimmune disease, and inflammatory disorders can interfere with how your body uses iron, sometimes lowering MCHC even when iron levels look adequate on paper.
Because these mechanisms differ, the fix differs too. Replacing iron helps blood-loss anemia, but inflammation-driven anemia usually needs the underlying condition addressed first.
Less Common Causes
A handful of other issues can lower MCHC. Vitamin B6 plays a role in hemoglobin synthesis, and a shortage can leave cells under-filled.
Lead exposure is another. Lead interferes with the machinery that builds hemoglobin, and in both children and adults it can present as a hypochromic picture on the CBC.
These are less frequent, but they’re worth knowing about when the usual iron workup comes back clean and the low MCHC persists.
Symptoms of Low MCHC
Low MCHC itself often causes no symptoms, especially early on. When symptoms do appear, they reflect the anemia behind the number rather than the number itself.
The most common complaints are fatigue, weakness, and a general run-down feeling. Pale skin, shortness of breath during activity, dizziness, and cold hands or feet round out the list.
A question that comes up again and again from readers is why they feel wiped out despite eating well. Reduced oxygen delivery is the usual answer, since hemoglobin-poor cells simply can’t move oxygen as efficiently.
Why Is Your MCHC High? Causes & Symptoms
A high MCHC means red cells hold an unusually dense concentration of hemoglobin. Because there’s a physical ceiling on how much hemoglobin a cell can pack, truly elevated values are uncommon and always deserve a second look.
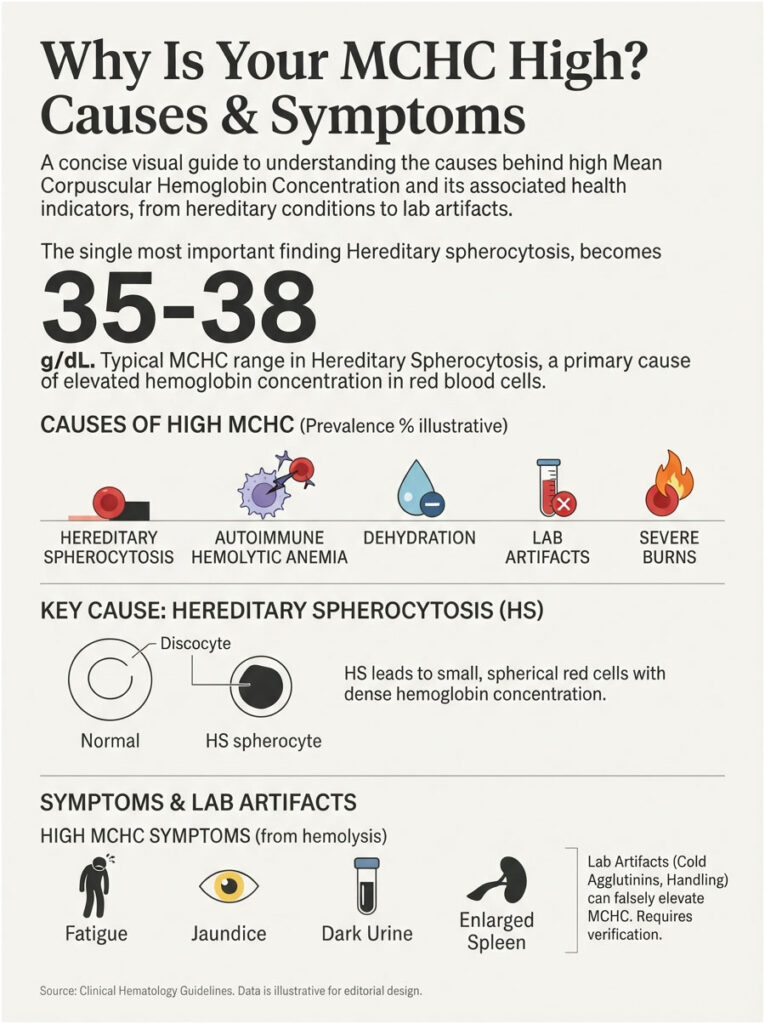
When MCHC climbs above the reference range, the cause tends to fall into one of a few buckets: a red cell membrane problem, active destruction of red cells, dehydration, or a measurement error.
Hereditary Spherocytosis
Hereditary spherocytosis (HS) is an inherited disorder of the red cell membrane. The cells lose surface area and become small spheres instead of flexible discs, which concentrates the hemoglobin inside them.
According to Medscape’s workup guidance, an MCHC above the upper limit of normal is a characteristic feature of HS, driven by mild cellular dehydration, while MCV often runs low. Values in the 35 to 38 g/dL range are common in affected patients.
HS is one of the more frequent causes of inherited hemolytic anemia. Severity varies widely, and some people carry it for years with only mild signs like occasional jaundice or gallstones.
Autoimmune Hemolytic Anemia
In autoimmune hemolytic anemia (AIHA), the immune system mistakenly attacks the body’s own red blood cells. As cells are destroyed, the surviving population can show a raised MCHC.
Medical News Today notes that AIHA sometimes develops on its own and sometimes alongside conditions like lupus or lymphoma, or as a reaction to certain medications. Symptoms can include fatigue, jaundice, and dark urine.
AIHA is a situation where speed matters. Rapid red cell destruction can drop hemoglobin quickly, so the safe move is prompt evaluation whenever it’s suspected rather than a wait-and-see approach.
Severe Burns and Hemoglobin Variants
Severe burns can damage red blood cells directly, leading to hemolysis and, in some cases, a temporarily elevated MCHC. These patients are managed in a hospital setting where blood counts are watched closely.
Certain hemoglobin variants also nudge the number up. Sickle cell disease and hemoglobin C disease alter the shape or chemistry of red cells in ways that can raise MCHC on the CBC.
These causes are far less common than iron deficiency on the low side, which is part of why a genuinely high MCHC prompts a more focused investigation.
Dehydration and Lab Artifacts
Not every high MCHC signals disease. Dehydration concentrates the blood and can temporarily push the number upward, which usually corrects once fluids are replaced.
Lab artifacts are the sneaky one. Cold agglutinins (antibodies that clump red cells at low temperatures), very high blood fats (lipemia), and certain sample-handling issues can all falsely elevate MCHC. In these cases, a repeat test under proper conditions often reads normal.
This is exactly why doctors so often recheck a high MCHC before launching a full workup. A number that looks alarming on Monday can quietly resolve on the repeat draw.
Symptoms of High MCHC
When a high MCHC comes from active hemolysis, the symptoms reflect red cell breakdown. Fatigue and pale skin overlap with low-MCHC anemia, which makes the number itself, not the symptoms, the differentiator.
More specific signs of hemolysis include yellowing of the skin or eyes (jaundice), dark or tea-colored urine, and an enlarged spleen. A rapid heartbeat can accompany a fast drop in red cells.
If the high reading traces back to dehydration or a lab artifact, there may be no meaningful symptoms at all, another reminder that context shapes what the number means.
Low vs High MCHC at a Glance
Seeing both sides together makes the differences click. The table below distills the causes, patterns, and next steps for each direction.
| Aspect | Low MCHC | High MCHC | Recommended Next Step |
| What it means | Cells hold too little hemoglobin (hypochromia) | Cells hold an unusually high hemoglobin concentration | Confirm with a repeat CBC |
| Most common cause | Iron deficiency anemia | Hereditary spherocytosis or hemolysis | Iron studies vs a hemolysis workup |
| Usual MCV pattern | Low (microcytic) | Low to normal, cells often dense | Read MCV alongside MCHC |
| Hallmark symptom | Fatigue, pale skin | Jaundice, dark urine (if hemolysis) | Track red-flag symptoms |
| Confirming test | Ferritin and iron panel | Coombs test, blood smear, osmotic fragility | Ask your doctor which applies |
| First-line treatment | Iron replacement, treat blood loss | Treat the cause; folate, sometimes steroids | Individualized by diagnosis |
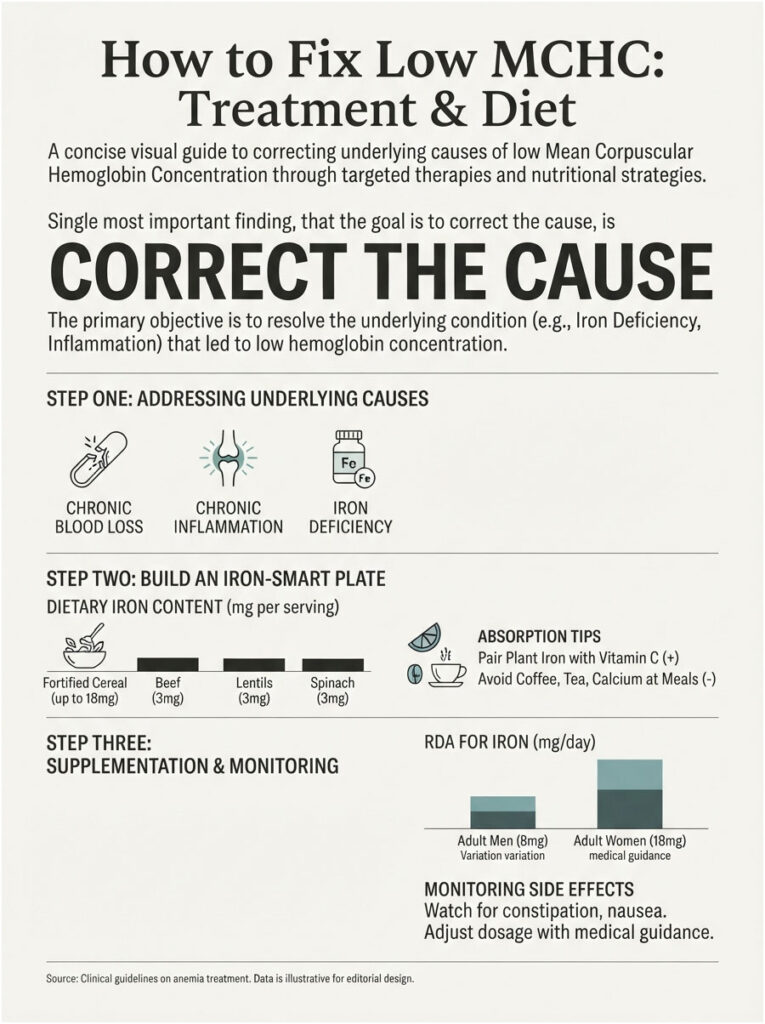
How to Fix Low MCHC: Treatment & Diet
The goal isn’t to chase the MCHC number for its own sake. It’s to correct whatever is keeping hemoglobin low, and the number follows once that’s handled.
Treatment for a low MCHC almost always starts with confirming iron status, then matching the fix to the finding. Here’s the practical sequence most people follow.
Step One: Treat the Underlying Cause
If iron deficiency is the driver, the plan centers on restoring iron and stopping ongoing losses. When heavy periods or a digestive bleed is behind the deficiency, addressing that source is every bit as important as the iron itself.
For inflammation-related anemia, the underlying condition takes priority. Loading up on iron won’t move the needle much if the real issue is a chronic inflammatory process quietly locking iron away.
Step Two: Build an Iron-Smart Plate
Diet is the first line for mild iron deficiency. Two types of iron exist: heme iron from animal foods, which absorbs efficiently, and non-heme iron from plants, which absorbs less readily.
The table below shows the iron content of common US foods, using values from the NIH Office of Dietary Supplements. Notice how a single serving of fortified cereal can rival a full day’s requirement.
| Food | Serving | Iron (mg) | Type |
| Fortified breakfast cereal | 1 serving | Up to 18 | Non-heme |
| Cooked oysters | 3 oz | 8 | Heme |
| Canned white beans | 1 cup | 8 | Non-heme |
| Dark chocolate (45–69% cacao) | 3 oz | 7 | Non-heme |
| Boiled lentils | 1/2 cup | 3 | Non-heme |
| Cooked spinach | 1/2 cup | 3 | Non-heme |
| Braised beef | 3 oz | 2 | Heme |
Absorption is half the battle. Pair plant iron with a vitamin C source such as citrus, bell peppers, or tomatoes to boost uptake, and keep coffee, tea, and calcium supplements away from your iron-heavy meals, since they can blunt absorption when taken together.
Step Three: Add Supplements If Needed
When diet alone isn’t enough, doctors often recommend an oral iron supplement. The NIH sets the iron RDA at 18 mg/day for women ages 19 to 50, 8 mg/day for men and postmenopausal women, and 27 mg/day during pregnancy.
The tolerable upper limit for adults is 45 mg/day, above which stomach upset becomes common. That’s one reason self-dosing high amounts without guidance isn’t a good idea.
Iron supplements can cause constipation and nausea in some people. Taking them with a little vitamin C and, if needed, adjusting the dose or timing usually helps. Rechecking labs after a few weeks confirms the treatment is working, since food and pill changes take time to show up in your blood.
When B12 or Folate Is the Real Problem
Not every anemia is about iron. If MCV runs high instead of low, vitamin B12 or folate deficiency is more likely, and that calls for a different fix.
Restoring B12 (through diet, oral supplements, or injections depending on the cause) and folate corrects that type of anemia. The clinicians who oversee our reporting stress matching treatment to the actual deficiency rather than defaulting to iron for every low blood count.
How to Fix High MCHC: Treatment Options
Because a high MCHC has fewer common causes, treatment hinges entirely on which one is at play. The first step is often confirming the result is even real.
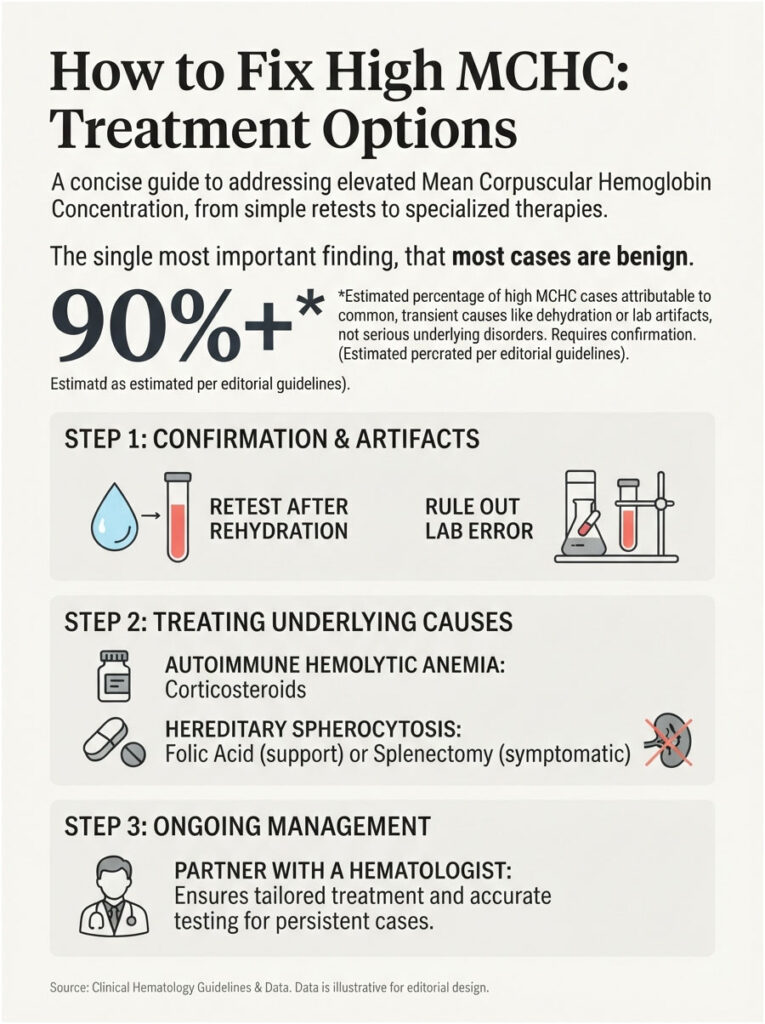
Once the cause is clear, the path forward becomes far more straightforward.
Correcting Dehydration or a Lab Error
When dehydration is suspected, rehydrating and repeating the test frequently resolves the elevation. A high reading tied to fluid status usually isn’t a lasting concern.
If a lab artifact is the likely explanation, the lab may re-run the sample under warmed conditions or with adjusted handling to rule out cold agglutinins or lipemia. A normal repeat often closes the case with no further action needed.
Managing Hemolytic Anemia
For autoimmune hemolytic anemia, treatment often involves corticosteroids to calm the immune attack, with other immune-modifying medications reserved for tougher cases. Care is guided by a hematologist who monitors the response over time.
For hereditary spherocytosis, the Merck Manual notes that folic acid supports red cell production, and that splenectomy (spleen removal, after appropriate vaccination) is reserved for patients with symptomatic hemolysis or complications like gallstones. Mild cases may need no specific treatment at all.
Partnering With Your Doctor
High MCHC is one of those results where a specialist’s read adds real value. A hematologist can order the right confirmatory tests and tailor a plan to your specific situation.
The reassuring part: many people with a mildly high MCHC turn out to have dehydration or an artifact, not a serious blood disorder. The workup exists to separate the two safely, not to alarm you.
How Doctors Diagnose the Cause
MCHC is a starting clue, not a final answer. The value of the number lies in where it points your doctor next.
A logical sequence of follow-up tests usually turns an abnormal MCHC into a clear diagnosis within a visit or two.
Tests That Come Next
For a low MCHC, iron studies lead the way. Ferritin, serum iron, total iron-binding capacity, and transferrin saturation together reveal whether iron deficiency is truly present, and ferritin in particular reflects your iron stores. A reticulocyte count shows how actively your marrow is making new cells.
For a high MCHC or suspected hemolysis, the workup shifts toward a peripheral blood smear, a Coombs test (direct antiglobulin test) to check for immune-driven destruction, and osmotic fragility or specialized membrane testing when hereditary spherocytosis is on the table.
Vitamin B12 and folate levels come into play when the cells are large rather than small. Each test narrows the field until the cause is clear, which is why the follow-up panel is often more revealing than the original CBC.
Why MCHC Is Never Read Alone
A single index in isolation can mislead. MCHC gains its meaning from the company it keeps, chiefly MCV, MCH, RDW, and the actual hemoglobin level.
This is the core lesson worth carrying away. The pattern across the whole panel, not any one flagged value, is what identifies the type of anemia and the right response.
When to Worry About an Abnormal MCHC
Most mildly abnormal MCHC results are not emergencies. Knowing which situations call for prompt attention keeps your concern proportionate to the actual risk.
Use the guide below to match your result to a sensible next move.
| Your Situation | What It Might Mean | Recommended Action |
| MCHC slightly below 32, no symptoms | Often mild or lab variation | Recheck in a few weeks; mention at your next visit |
| Low MCHC + low MCV + fatigue | Likely iron deficiency anemia | Get ferritin and iron studies; discuss iron therapy |
| High MCHC + jaundice or dark urine | Possible hemolysis | Seek prompt medical evaluation |
| High MCHC but you were dehydrated | Possibly temporary or an artifact | Rehydrate and retest |
| Any abnormal MCHC during pregnancy | Needs closer monitoring | Contact your OB provider |
| MCHC normal but you feel exhausted | Cause may lie elsewhere | Ask about a full anemia and thyroid workup |
Red-Flag Symptoms
Some symptoms warrant same-day medical care regardless of the exact number. Chest pain, severe shortness of breath, fainting, and a racing heartbeat all signal that oxygen delivery may be compromised.
Signs of active red cell destruction deserve prompt attention too: yellowing skin or eyes, dark urine, and sudden worsening fatigue. Clinical guidance lists these as reasons to seek urgent care rather than wait it out.
When a Mildly Off Number Is Harmless
If your MCHC sits just outside the range and you feel well, it’s frequently nothing to lose sleep over. Small deviations can reflect normal lab variation or a passing state like mild dehydration.
The sensible approach is a recheck and a conversation with your provider, not panic. Among the borderline results readers bring to us, the calm, confirm-then-investigate path is almost always the right one.
Frequently Asked Questions
What is a normal MCHC level?
For most adults, a normal MCHC is roughly 32 to 36 g/dL, and some labs use 33 to 36 g/dL. Always compare your result to the reference range printed on your own report, since equipment and calibration differ slightly from one lab to another.
Is low MCHC serious?
Usually not on its own, and it’s often treatable. A low MCHC most commonly reflects iron deficiency anemia, which responds well to diet and iron replacement. It becomes more pressing when it comes with significant symptoms or an underlying condition, so follow-up testing matters.
What is the most common cause of low MCHC?
Iron deficiency is the leading cause by a wide margin. Without enough iron, your body can’t fill red cells with hemoglobin, producing pale, under-loaded cells. The classic lab pattern is low MCHC alongside low MCV and low MCH, confirmed with ferritin and iron studies.
Does high MCHC mean I have anemia?
Not necessarily. A high MCHC can point to hemolysis or hereditary spherocytosis, but it can also stem from dehydration or a lab artifact, with no true blood disorder. Because falsely high readings are common, doctors often repeat the test before pursuing a full workup.
How can I raise my MCHC naturally?
If iron deficiency is the cause, focus on iron-rich foods like lean meat, beans, lentils, and fortified cereals, and pair plant iron with vitamin C to boost absorption. Limit coffee and tea around iron-heavy meals. Confirm the cause first, since not every low count needs iron.
Can dehydration cause high MCHC?
Yes. Dehydration concentrates the blood and can temporarily push MCHC above the normal range. This kind of elevation typically corrects once you rehydrate. That’s one reason a high MCHC is often rechecked, so a passing state isn’t mistaken for a lasting blood condition.
What is the difference between MCHC and MCH?
MCH measures the average amount of hemoglobin in a red cell, while MCHC measures its concentration, meaning amount relative to cell size. Using a coffee analogy, MCH is how much coffee is in the cup and MCHC is how strong that coffee tastes.
What does low MCHC with normal iron mean?
When iron studies come back normal but MCHC stays low, thalassemia trait is a common explanation, especially if MCV is quite low and the red cell count is relatively high. Chronic inflammation can also lower MCHC despite adequate iron. Your doctor may order further testing.
Is an MCHC of 30 or 31 too low?
Both sit just below the typical 32 g/dL threshold, so they’d usually be flagged as mildly low. Whether that matters depends on your symptoms and the rest of your CBC. A slightly low value with no symptoms often warrants a simple recheck rather than immediate concern.
Can high MCHC be a lab error?
Absolutely. Cold agglutinins, very high blood fats (lipemia), and sample-handling issues can all falsely raise MCHC. In these situations, repeating the test under proper conditions usually returns a normal result. Falsely high readings are one of the most frequent reasons for an unexpected elevation.
What foods increase MCHC the fastest?
For iron-related low MCHC, heme iron from red meat, poultry, and fish absorbs most efficiently, while beans, lentils, spinach, and fortified cereals supply non-heme iron. Adding vitamin C sources speeds absorption. Food changes take weeks to reflect in labs, so patience and a follow-up test help.
Should I see a doctor for an abnormal MCHC?
Yes, at least to discuss it. A mildly abnormal result with no symptoms may only need a recheck, but any significant abnormality, red-flag symptom, or abnormal MCHC during pregnancy deserves professional evaluation. Your doctor can order the right follow-up tests and interpret the full panel together.
Medical Disclaimer: This article is for general educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. MCHC results should always be interpreted by a qualified healthcare provider in the context of your full blood count and personal health history. Never start, stop, or change any supplement or treatment based on a lab value alone. If you have concerning symptoms, contact a licensed clinician promptly.
References
- Cleveland Clinic, MCH Blood Test
- CDC / NHANES, Anemia Prevalence: United States, August 2021–August 2023
- NCBI / StatPearls, Iron-Deficiency Anemia
- NCBI / StatPearls, Dietary Iron
- Harvard T.H. Chan School of Public Health, The Nutrition Source: Iron
- Merck Manual, Hereditary Spherocytosis and Hereditary Elliptocytosis
- Medscape, Hereditary Spherocytosis Workup
- Medical News Today, High MCHC: Causes, Treatment, and Symptoms
- UPMC HealthBeat, What Does Low MCHC Mean?