Your blood is doing something remarkable right now: staying liquid while it flows, yet ready to clot the instant you get a cut. Warfarin steps into that balance and tips it, on purpose, so clots form less easily. For millions of Americans with an irregular heartbeat or a history of blood clots, that shift can prevent a stroke.
Table of Contents
But warfarin is a medication that demands respect. Take too much and you risk dangerous bleeding; take too little and a clot slips through. This guide covers how warfarin works, what it protects against, how doctors set the dose, and why the INR blood test sits at the center of using it safely.
| Quick Answer: Warfarin (Coumadin, Jantoven) is a blood thinner that blocks vitamin K, which your liver uses to make clotting factors. This makes blood clot more slowly, which helps prevent strokes and dangerous clots. Because too much causes bleeding and too little lets clots form, you need regular INR blood tests to stay in a safe range, usually 2.0 to 3.0, plus a steady vitamin K diet. |
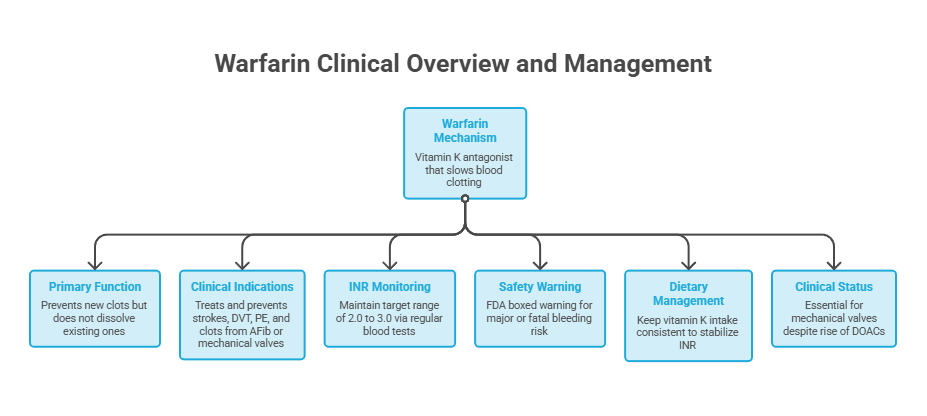
| At a Glance Warfarin is a vitamin K antagonist that makes blood take longer to clot; it prevents new clots but does not dissolve existing ones.It treats and prevents strokes, deep vein thrombosis, pulmonary embolism, and clots linked to atrial fibrillation or mechanical heart valves.The standard INR target is 2.0 to 3.0, checked with regular blood tests to keep you in range.Bleeding is the main risk; warfarin carries an FDA boxed warning for major or fatal bleeding.Keep vitamin K intake consistent rather than cutting it out; big diet swings throw off your INR.Newer blood thinners (DOACs) have largely replaced warfarin, but it stays essential for mechanical valves and a few other conditions. |
What Is Warfarin, and Why Doctors Still Prescribe It
Warfarin is an oral anticoagulant, the medical term for a blood thinner. Sold under the brand names Coumadin and Jantoven, it has been a mainstay of clot prevention in the United States since the 1950s. It belongs to a drug class called vitamin K antagonists.
The name “blood thinner” is a little misleading. Warfarin does not actually thin your blood or make it more watery. Instead, it slows down your blood’s ability to form clots, which is what Cleveland Clinic explains keeps unwanted clots from forming inside your blood vessels or heart.
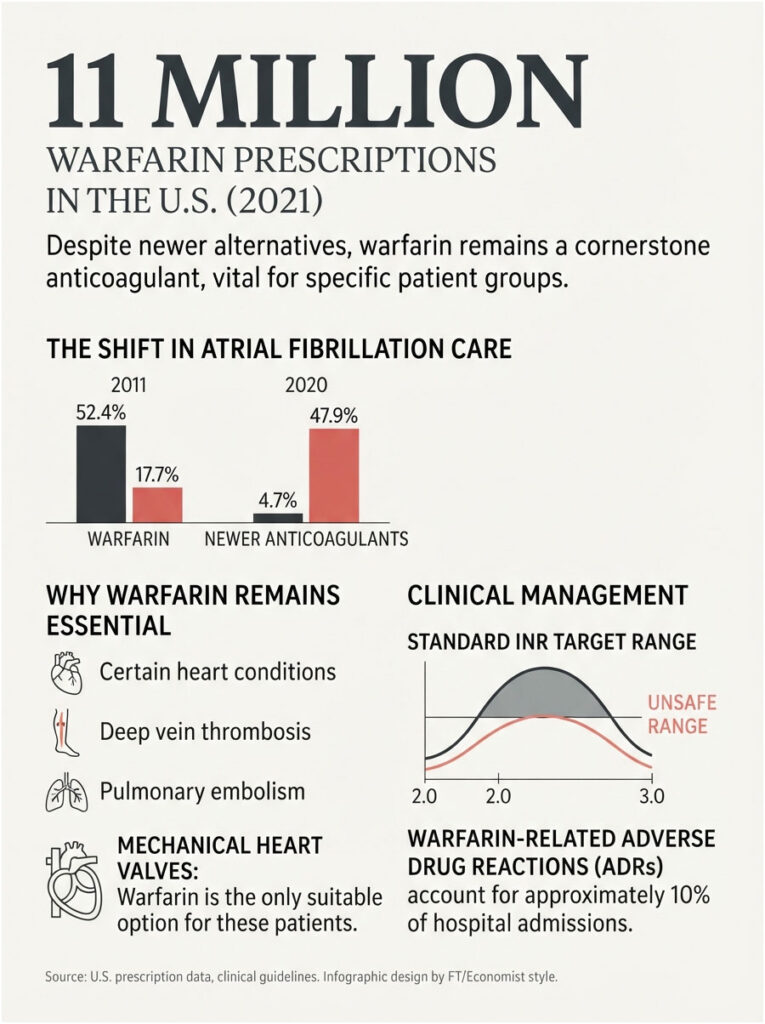
Its role has changed a lot over the past 15 years. Newer drugs have taken over much of the market, and the numbers show it clearly. Among patients with atrial fibrillation, warfarin use fell from 52.4% in 2011 to 17.7% in 2020, while newer blood thinners climbed from under 5% to nearly half.
Even so, warfarin is far from obsolete. It was still prescribed an estimated 11 million times in the United States in 2021, and for certain patients it remains the only appropriate choice. HealthCareOnTime’s editorial approach follows current cardiology guidelines here: newer is not automatically better for everyone.
| Warfarin in the US | Figure | Source |
| Estimated US prescriptions (2021) | ~11 million | Published usage analysis |
| Share of AF patients on warfarin (2011 to 2020) | Fell from 52.4% to 17.7% | AHA Journal |
| Share of AF patients on newer blood thinners (2011 to 2020) | Rose from 4.7% to 47.9% | AHA Journal |
| Standard INR target, most conditions | 2.0 to 3.0 | StatPearls / AHA-ACC |
| Hospital admissions for drug reactions linked to warfarin | ~10% | Pirmohamed study |
| First year a newer blood thinner was FDA approved | 2010 | FDA |
The Conditions Warfarin Treats
Doctors prescribe warfarin to prevent and treat clots in several situations. The most common is atrial fibrillation, an irregular heartbeat that lets blood pool and clot in the heart, then travel to the brain as a stroke.
It also treats deep vein thrombosis (a clot in a deep vein, usually the leg) and pulmonary embolism (a clot that reaches the lungs). Beyond that, Mayo Clinic notes it is used for clots tied to certain heart conditions, open-heart surgery, or a recent heart attack.
One group depends on it especially: people with a mechanical heart valve. Newer blood thinners are not safe for these patients, so warfarin remains the standard. The same holds for moderate-to-severe mitral valve narrowing.
How Warfarin Works in Your Body
Here is the mechanism in plain terms. Your liver uses vitamin K to build several of the proteins that make blood clot, known as clotting factors. Warfarin blocks the enzyme that recycles vitamin K, so your liver makes fewer working copies of those factors.
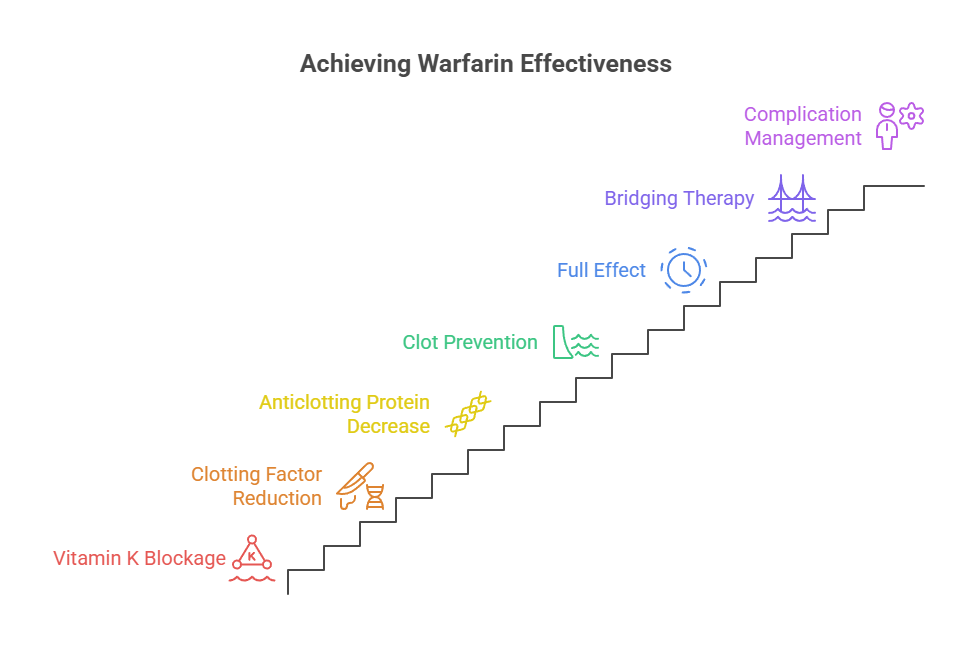
More specifically, warfarin reduces the active form of clotting factors II, VII, IX, and X. With fewer of these in circulation, the clotting process runs slower, and it takes longer for a clot to form. That is the entire point of the drug.
Warfarin also lowers two natural anticlotting proteins, protein C and protein S, which matters mainly in the first days of treatment and shapes how doctors start the drug. It is a balancing act built into the medication.
One detail matters more than most people realize. Warfarin prevents new clots from forming and stops existing clots from growing, but it does not dissolve a clot that is already there. Your body breaks down old clots on its own; warfarin just keeps new trouble from piling on.
Why Warfarin Takes Days to Work
Swallowing a warfarin tablet does not thin your blood by that evening. The clotting factors already circulating in your bloodstream have to wear off first, and some of them last for a couple of days. Full effect usually takes about five to seven days.
That delay creates a practical problem when someone has a clot that needs treating right now. In those cases, doctors often start a fast-acting injectable blood thinner like heparin at the same time, a step called bridging, until warfarin catches up.
The slow onset also explains a rare early complication. Because protein C falls quickly at the start, a temporary imbalance can, in rare cases, cause a serious skin reaction called warfarin skin necrosis. It is uncommon, but it is why starting doses are handled carefully.
The Benefits: What Warfarin Protects Against
The central benefit is stroke prevention, and the effect is large. In people with atrial fibrillation, warfarin reduces the risk of stroke by about two-thirds compared with taking nothing, a benefit confirmed across decades of clinical trials.
Beyond that, warfarin treats and prevents deep vein thrombosis and pulmonary embolism, two conditions that can turn deadly fast. For patients with a mechanical heart valve, it prevents clots from forming on the valve, which is life-saving protection that newer drugs cannot safely provide.
Warfarin carries two more advantages worth knowing. It is inexpensive as a generic, which matters for anyone paying out of pocket. And its effect can be reversed with vitamin K when bleeding or surgery makes that necessary, giving doctors a clear “off switch” that newer drugs do not all share.
Warfarin Dosage: How It’s Determined and Adjusted
There is no single correct warfarin dose. The right amount is deeply personal, shaped by your age, weight, genetics, diet, other medications, and how your liver processes the drug. Two people the same size can need very different doses.
Warfarin comes as color-coded tablets in strengths of 1, 2, 2.5, 3, 4, 5, 6, 7.5, and 10 mg, each scored so it can be split if your provider adjusts the dose. The usual maintenance dose lands somewhere between 2 and 10 mg a day, though some people need as little as 1 mg and others as much as 20 mg.
Here is the part that trips people up. Your dose is not fixed at the start and left alone. It is set and re-set based on your INR blood test results, sometimes several times before the right level is found. That back-and-forth early on is normal and expected, not a sign that something is wrong.
Take warfarin at the same time each day, most often in the evening, to keep levels steady. Consistency in timing is as much a part of safe dosing as the milligrams themselves.
Starting Warfarin and Missed Doses
When you first start, expect frequent blood tests and dose tweaks until your INR settles into range. This stretch takes patience, and it is not a red flag.
If you miss a dose, take it as soon as you remember on the same day. If you do not remember until the next day, skip the missed dose and take your normal amount, and never double up to catch up. Doubling raises your bleeding risk.
One rule stands above the rest: do not stop warfarin on your own. Suddenly quitting can let a dangerous clot form. Any change should go through your care team, in line with Mayo Clinic’s guidance to never stop or change warfarin without talking to your provider.
INR Blood Test Monitoring: The Key to Safe Warfarin Use
If you remember one thing about warfarin, make it this: the drug only works safely with regular blood testing. The test is called the prothrombin time, reported as the INR, or international normalized ratio, which measures how long your blood takes to clot.
Monitoring exists because warfarin has what pharmacists call a narrow therapeutic range. The gap between too little (clot risk) and too much (bleeding risk) is small, so your INR has to be checked and kept inside a target window. This is the safeguard that makes long-term use possible.
You can get the test at a lab, a dedicated anticoagulation clinic, or, once you are stable, with a home meter. According to StatPearls, testing is done frequently at first, then spaced out once you hold steady, often to every one to four weeks.
The INR target itself depends on why you are taking warfarin. Most conditions aim for 2.0 to 3.0, but mechanical valves in certain positions call for a higher range.
| Condition | Target INR | Typical Range |
| Atrial fibrillation | 2.5 | 2.0 to 3.0 |
| DVT or pulmonary embolism | 2.5 | 2.0 to 3.0 |
| Mechanical aortic valve (bileaflet) | 2.5 | 2.0 to 3.0 |
| Mechanical mitral valve | 3.0 | 2.5 to 3.5 |
| Tissue (bioprosthetic) valve, first 3 months | 2.5 | 2.0 to 3.0 |
| To reduce recurrent heart attack | 3.0 | 2.5 to 3.5 |
Reading Your INR: What the Numbers Mean
An INR result is not just a number to file away; it tells you and your provider what to do next. The table below is a general guide, not a substitute for your own care team’s instructions, since your target and plan are set for your specific situation.
| INR Range | What It Means | What to Do |
| Below 2.0 | Blood clotting too readily; clot risk | Provider may raise your dose; keep testing |
| 2.0 to 3.0 | In range for most conditions | Continue current dose as directed |
| 3.1 to 4.0 | Slightly high; bleeding risk rising | Provider may lower dose; watch for bleeding |
| 4.1 to 5.0 | Too high | Often hold a dose; call your clinic |
| Above 5.0 (no bleeding) | High bleeding risk | Contact your clinic now; vitamin K may be given |
| Any major bleeding | Emergency | Go to the ER immediately |
Home INR Testing and Time in Range
Once your dose is stable, you may qualify to test at home with a small meter that reads a fingerstick drop of blood, similar to a glucose monitor. Mayo Clinic offers a home monitoring program after a patient has been stable for at least three months. Fewer lab trips often means better day-to-day control.
Providers also track a measure called time in therapeutic range, or TTR, the share of time your INR stays inside your target window. A higher TTR means safer, more effective treatment. If your INR bounces around often, your care team will hunt for the cause rather than just chasing each result.
What Makes Your INR Swing
Even on a steady dose, your INR can drift. Knowing the common triggers helps you catch problems early, and it explains why your provider asks about your week at every visit.
Illness is a big one. Fever, vomiting, or diarrhea can shift your INR, and being sick often changes what you eat. Call your clinic if you are unwell for more than a day or two.
New medications matter just as much. Starting or stopping almost any drug, especially antibiotics, can push your INR up or down. Always mention that you take warfarin whenever you are prescribed something new.
Diet changes move the needle too. A sudden jump or drop in vitamin K foods shifts your INR, as does crash dieting or losing your appetite. Alcohol adds another variable, since heavy or binge drinking can raise both your INR and your bleeding risk.
Missed or extra doses and travel round out the list. Skipping or doubling changes your level, so a pill organizer helps, and time zones plus restaurant food can nudge your INR on a long trip. When any of these change, your provider may test more often until things settle.
The Risks and Side Effects You Should Know
Every benefit of warfarin comes from the same action that creates its main danger. Because the drug slows clotting, it can cause bleeding, and that risk is serious enough that warfarin carries an FDA boxed warning for the risk of major or fatal bleeding.
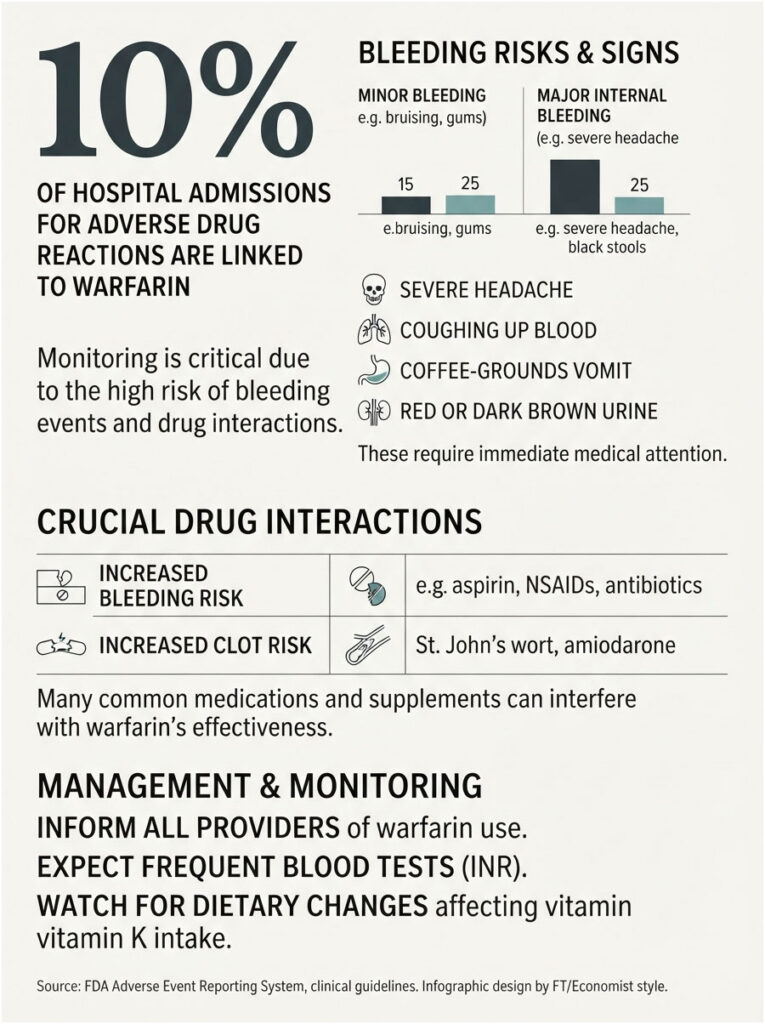
Most bleeding is minor, like easy bruising, bleeding gums, or nosebleeds. But warfarin can also cause internal bleeding that is not obvious, which is why knowing the warning signs matters. This is not meant to frighten you off a helpful drug, only to keep you alert.
Two rarer side effects deserve a mention. Warfarin skin necrosis, noted earlier, can appear in the first days of treatment. And warfarin is unsafe in pregnancy, because it can harm a developing baby, so it is generally avoided by anyone who is pregnant or may become pregnant.
Warfarin Bleeding Red Flags
Some signs mean you should get medical help without waiting. Call your provider or seek emergency care for a severe headache, coughing up blood, vomit that looks like coffee grounds, or red or dark brown urine.
Also watch for black or tarry stools, bleeding that will not stop, unusual or large bruises appearing on their own, or feeling weak, faint, or dizzy. These can signal bleeding you cannot see.
The scale of this risk is real. One landmark study found warfarin was responsible for roughly 10% of all hospital admissions for adverse drug reactions, a reminder of why monitoring and awareness are not optional.
Drug and Supplement Interactions
Warfarin interacts with a long list of medications, and many common ones either boost its effect (raising bleeding risk) or blunt it (raising clot risk). Antibiotics, antifungals, the heart drug amiodarone, and pain relievers like aspirin and NSAIDs are frequent culprits.
Supplements count too. Garlic, ginkgo biloba, green tea, and St. John’s wort can all interfere with warfarin. The safest habit is simple: tell every provider, dentist, and pharmacist that you take warfarin, and check before starting anything new, even something sold as natural.
Warfarin and Your Diet: The Vitamin K Balance
This is where warfarin earns its reputation for being high-maintenance, and where the most confusion lives. Since warfarin works by blocking vitamin K, the vitamin K in your food directly affects how well the drug works.
The goal is not to avoid vitamin K. That advice is outdated and cuts out healthy foods. The real rule is consistency. If you eat about the same amount of vitamin K from day to day, your provider can match your warfarin dose to it and keep your INR steady.
Here is the mechanism in practice. Eat a lot more vitamin K than usual and your INR drops, raising clot risk. Eat a lot less and your INR climbs, raising bleeding risk. A systematic review found a measurable effect on clotting mainly at higher intakes, above roughly 150 micrograms a day, which is around 30 grams of cooked spinach. So a normal serving of salad is not off-limits, as long as your intake stays steady.
| High Vitamin K (keep steady) | Moderate Vitamin K | Low Vitamin K |
| Kale, cooked | Brussels sprouts | Corn |
| Spinach, cooked or raw | Cabbage | Mushrooms |
| Collard and turnip greens | Asparagus | Onion |
| Broccoli | Green peas | Potato |
| Swiss chard | Green beans | Summer squash |
| Parsley | Lettuce, small amounts | Most fruits (berries, apples) |
Food and drink beyond leafy greens can matter too. Vitamin K is found in canola, soybean, and olive oils, so salad dressings and mayonnaise carry it as well. Green tea, cranberry juice, grapefruit juice, alcohol, and large amounts of mango can also affect warfarin, so keep those consistent and flag any big changes to your provider.
Warfarin vs Newer Blood Thinners (DOACs)
You have probably heard of newer blood thinners like apixaban (Eliquis), rivaroxaban (Xarelto), dabigatran (Pradaxa), and edoxaban (Savaysa). Known as DOACs, they are the reason warfarin’s use has dropped so sharply.
Their appeal is convenience. They come in fixed doses, do not require routine INR blood tests, and have far fewer food interactions. For many people with atrial fibrillation or a leg or lung clot, that is a meaningful quality-of-life difference.
Warfarin still wins in specific cases, though. Newer drugs are not safe for people with a mechanical heart valve or moderate-to-severe mitral stenosis, where warfarin remains the standard. Warfarin is also cheaper, and its reversibility can be an advantage. The table below lays out the trade-offs.
| Feature | Warfarin | Newer Blood Thinners (DOACs) | Why It Matters |
| Routine blood tests | Yes, regular INR | No routine testing | Convenience and clinic visits |
| Diet restrictions | Consistent vitamin K needed | Few or none | Daily flexibility |
| Dosing | Individualized, adjusted often | Fixed dose | Simplicity |
| Onset | Several days | Within hours | Speed of protection |
| Reversal agent | Vitamin K, widely available | Specific agents, not everywhere | Emergency bleeding care |
| Mechanical heart valve | Safe and standard | Not safe | Valve patients rely on warfarin |
| Cost | Low (generic) | Higher | Out-of-pocket affordability |
Living Safely on Warfarin: Practical Tips
Warfarin fits into daily life well once you build a few habits around it. Small precautions lower your bleeding risk without turning your life upside down.
Wear a medical ID bracelet so emergency responders know you take a blood thinner. Switch to a soft-bristle toothbrush and an electric razor to cut down on bleeding from small nicks, and take sensible steps to prevent falls, since a fall on warfarin carries extra risk.
Keep the routine tight. Take your dose at the same time daily, eat a steady amount of vitamin K, and never skip your INR appointments. Tell every dentist and provider you see, and if you are traveling, plan ahead for where you will get tested. Following the AHRQ’s blood thinner safety guidance on these basics goes a long way toward avoiding problems.
Warfarin, Surgery, and Dental Procedures
Any planned procedure, from a colonoscopy to a tooth extraction, needs advance planning when you take warfarin. Because the drug slows clotting, surgeons and dentists need to know well before the appointment, not on the day of it.
For many minor procedures, including routine dental cleanings and simple fillings, you can usually stay on warfarin at your normal dose. Your dentist may just take extra local steps to control any bleeding.
Bigger operations are different. Your care team may have you pause warfarin a few days beforehand so your INR drops to a safer level, then restart it afterward. If your clot risk is high, they may bridge with a short-acting injectable blood thinner during the gap.
The key rule still holds: never stop warfarin on your own to prepare for a procedure. Let the doctor managing your warfarin and the one performing the procedure coordinate the plan together.
Frequently Asked Questions
How does warfarin thin the blood?
Warfarin does not literally thin blood. It blocks vitamin K, which your liver needs to make several clotting factors. With fewer active clotting factors, your blood takes longer to clot, so new clots form less easily and existing clots are less likely to grow.
What is a normal INR level while taking warfarin?
For most conditions, the target INR is 2.0 to 3.0. Some situations, like certain mechanical heart valves, call for a higher range of 2.5 to 3.5. Your provider sets your specific target based on why you take warfarin, so follow their number, not a general one.
How often will I need blood tests on warfarin?
At first, expect frequent tests, sometimes every few days, until your INR settles into range. Once you are stable, testing usually spaces out to every one to four weeks. Starting a new medication, getting sick, or changing your diet may mean more frequent checks for a while.
How long does warfarin take to start working?
Warfarin does not work right away. It takes about five to seven days to reach full effect, because the clotting factors already in your blood have to wear off first. If you need immediate protection, your doctor may start a fast-acting injectable blood thinner alongside it.
What foods should I avoid while taking warfarin?
There is no strict “avoid” list. The key is keeping vitamin K intake consistent, not eliminating it. Leafy greens like kale and spinach are highest in vitamin K. You can still eat them; just keep the amount steady from day to day, and tell your provider about big diet changes.
What are the signs that my warfarin dose is too high?
Warning signs include unusual or heavy bruising, bleeding gums, frequent nosebleeds, red or dark urine, black or tarry stools, or coughing up blood. A severe headache or feeling faint can signal internal bleeding. Contact your care team promptly, and seek emergency care for heavy or uncontrolled bleeding.
Can I drink alcohol while taking warfarin?
Occasional light drinking may be acceptable, but alcohol affects warfarin and your INR, and binge drinking is risky. Heavy or variable drinking can raise bleeding risk. Ask your provider what is safe for you, and keep your intake consistent rather than swinging from none to a lot.
Is warfarin safe during pregnancy?
Generally, no. Warfarin can cross the placenta and harm a developing baby, so it is usually avoided during pregnancy, especially early on. Anyone who is pregnant, planning pregnancy, or could become pregnant should discuss safer anticoagulant options with their doctor before starting or continuing warfarin.
What happens if I miss a dose of warfarin?
Take it as soon as you remember on the same day. If you do not remember until the next day, skip the missed dose and take your regular amount. Never double up to make up for a missed dose, since that raises your bleeding risk. Tell your provider if you miss doses often.
How is a high INR or warfarin bleeding reversed?
Vitamin K reverses warfarin’s effect and can be given by mouth or IV depending on severity. For serious bleeding, hospitals may also use clotting factor concentrates or plasma to restore clotting quickly. This is one reason warfarin is still valued: its effect can be undone when needed.
Is warfarin being replaced by newer blood thinners?
Largely, yes. Newer blood thinners have overtaken warfarin for conditions like atrial fibrillation because they need no routine INR testing and have fewer food interactions. But warfarin remains essential for mechanical heart valves and some other conditions where newer drugs are not safe.
Can I stop taking warfarin once my clot is gone?
Only if your provider says so. For a one-time clot, warfarin may be prescribed for a set number of months. For ongoing conditions like atrial fibrillation or a mechanical valve, it is often lifelong. Stopping on your own can let a dangerous clot form, so never quit without medical guidance.
| Disclaimer: This article is for general informational purposes and is not a substitute for professional medical advice, diagnosis, or treatment. Warfarin dosing is highly individual and must be managed by a qualified healthcare provider. Always follow your care team’s instructions, keep your INR appointments, and seek emergency care for signs of serious bleeding. |
References
- Warfarin, StatPearls, National Center for Biotechnology Information
- Warfarin (oral route), Mayo Clinic
- Warfarin side effects: Watch for interactions, Mayo Clinic
- Warfarin: A Blood-Thinning Drug, Cleveland Clinic
- Warfarin oral tablet, Healthline
- Vitamin K, NIH Office of Dietary Supplements
- Trends in Oral Anticoagulant Use, Journal of the American Heart Association
- Dietary Vitamin K and Vitamin K Antagonists, Systematic Review, NCBI
- Blood Thinner Pills: Your Guide to Using Them Safely, Agency for Healthcare Research and Quality