

For years, biologics were the treatment doctors saved for last. You tried the older drugs, you waited, and only after they failed did a biologic enter the conversation. That script has flipped. Many specialists now reach for biologics early, because the timing of treatment may matter almost as much as the drug itself.
Table of Contents
If you have Crohn’s disease, the real question is rarely whether biologics work. It is when they apply to you. This guide walks through who qualifies, the main drug classes, what the evidence shows, the risks and screening involved, the cost reality, and what starting one actually looks like.
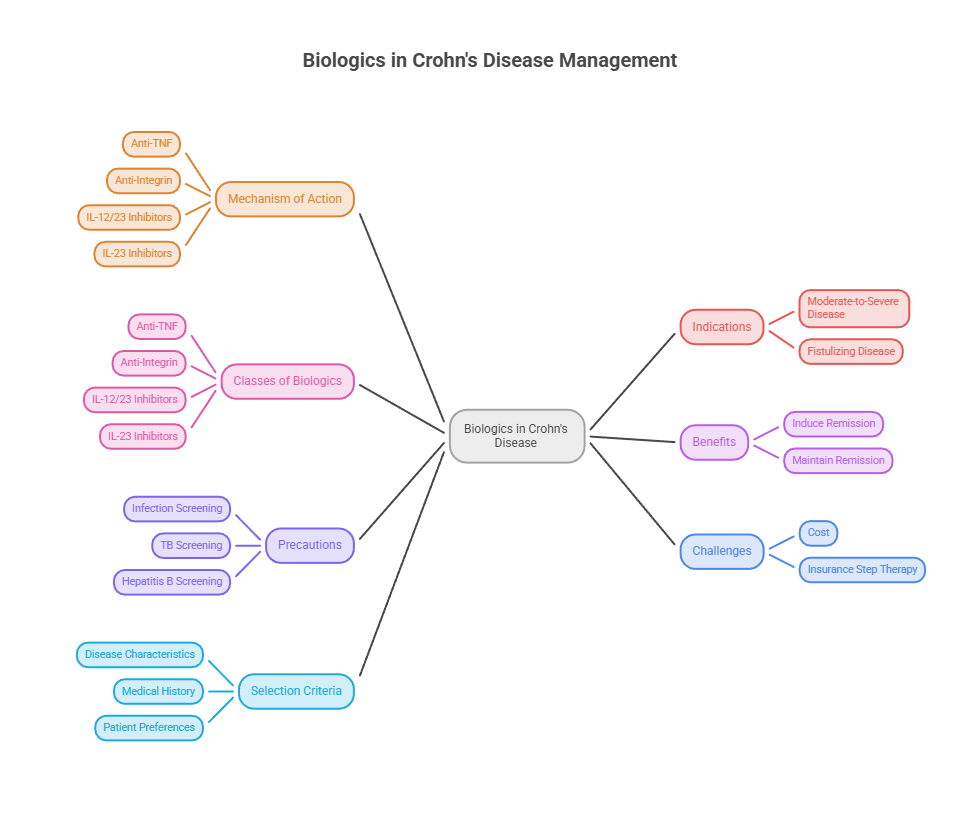
Quick Answer: Biologics are usually an option once Crohn’s disease is moderate to severe, is causing fistulas, or is not controlled by aminosalicylates, steroids, or immunomodulators. Major US guidelines now favor using them early rather than as a last resort. The main classes are anti-TNF, anti-integrin, and interleukin (IL-12/23 and IL-23) inhibitors. They are prescription drugs, and the choice belongs to you and your gastroenterologist.
At a Glance
- Biologics target specific proteins that drive Crohn’s inflammation.
- They are favored early in moderate-to-severe or fistulizing disease.
- Main classes are anti-TNF, anti-integrin, and IL-12/23 or IL-23 inhibitors.
- They can induce and maintain remission, not just ease symptoms.
- Infection screening (TB, hepatitis B) is required before starting.
- Cost and insurance step therapy are common real-world hurdles.
- The best choice depends on your disease, history, and preferences.
What Biologics Are (and How They Work)
Biologics are prescription drugs made from living cells rather than synthesized from simple chemicals. Instead of broadly dampening the whole immune system, they target the specific proteins that fuel inflammation in Crohn’s disease.
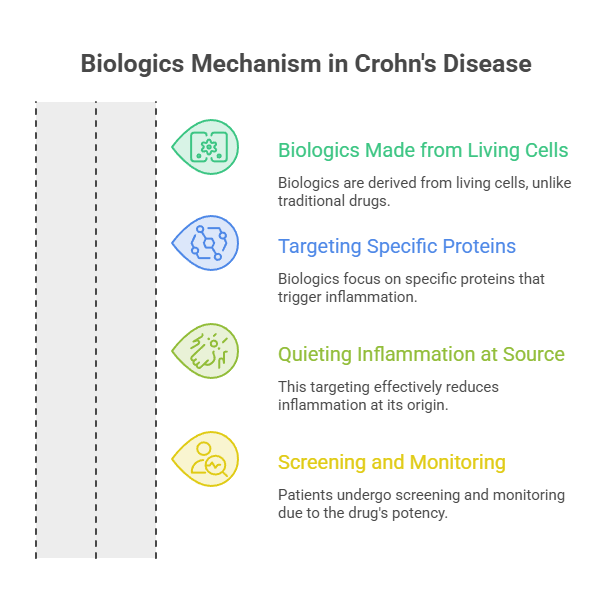
That precision is the point. These drugs work on your immune system by targeting specific proteins involved in the inflammation process, which can quiet the disease at its source rather than masking it.
This targeting explains both the strengths and the cautions. A drug precise enough to switch off part of your immune defense is powerful, which is exactly why screening and monitoring matter.
Biologics vs. Conventional Crohn’s Drugs
It helps to see where biologics sit in the wider toolkit. The older tiers include aminosalicylates (like mesalamine), corticosteroids (like prednisone) for short-term flares, and immunomodulators (like azathioprine or methotrexate).
These conventional drugs still have a role, especially for milder disease or as bridges during a flare. Steroids in particular are meant for short stretches, since long-term use carries real harms.
Biologics differ by acting on defined inflammatory pathways and by their goal: durable remission and healing of the bowel lining, not just symptom relief. Patients we serve often ask why a stronger drug comes earlier now, and the short answer is that controlling inflammation early helps prevent the damage that leads to surgery.
How Biologics Target Inflammation
Each class blocks a different signal. Anti-TNF drugs act on a protein called TNF-alpha that is part of the inflammation process. Natalizumab and vedolizumab stop immune-system molecules called integrins from attaching to the lining of your intestines. Ustekinumab blocks the proteins interleukin 12 and 23, while risankizumab blocks IL-23.
In plain terms, some biologics intercept an inflammatory alarm signal, while others block immune cells from reaching the gut wall in the first place. Different targets suit different patients.
This variety is good news. When one pathway does not respond, another class often can, which gives you and your gastroenterologist more than one path to remission.
When Are Biologics an Option for Crohn’s?
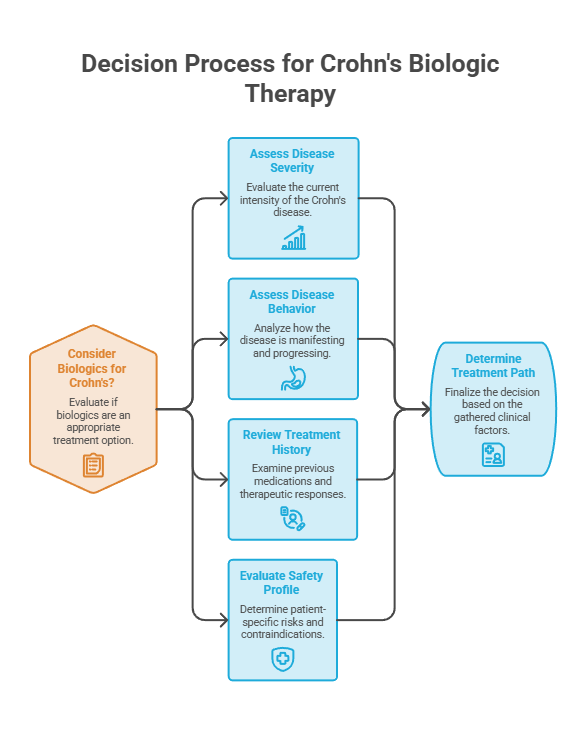
This is the heart of the matter. Biologics are not for every case of Crohn’s, and they are not only for the most extreme. The decision turns on disease severity, behavior, your treatment history, and your safety profile.
Moderate-to-Severe and Fistulizing Disease
The clearest signal is disease that is more than mild. In the trials that define this space, moderate to severe maps to a measurable disease-activity range. The landmark SONIC trial enrolled patients with moderately to severely active Crohn’s, defined by a baseline Crohn’s Disease Activity Index of 220 to 450.
Fistulizing disease, where inflammation tunnels abnormal connections between the bowel and other tissues, is another strong indication. Anti-TNF agents in particular have a track record here.
Severity is not only about how you feel on a given day. It also reflects inflammation seen on labs, imaging, and colonoscopy, which is why objective testing guides the call.
Early “Top-Down” Use vs. the Old “Step-Up” Approach
The biggest change is timing. The old model, called step-up, started with the mildest drugs and added stronger ones only as each failed. The newer model, top-down, brings effective therapy in early.
US guidance now leans top-down for the right patients. The American Gastroenterological Association recommends introducing biologics early for patients with luminal and fistulizing Crohn’s, rather than waiting until other treatments fail.
The reasoning is preventive. The AGA bases this on studies showing that people who started biologics early had lower rates of relapse, fewer disease-related complications, and were more likely to reach remission than those who began them later.
That marks a real shift in practice. Historically, doctors reserved biologics for people who had not responded to several other medications, and less than 1% of people with Crohn’s began a biologic as their first medication. The expectation now is that earlier use becomes more common.
When Other Drugs Fail or Complications Escalate
Even outside the early-use model, biologics become an option when conventional therapy is not holding. Repeated flares, steroid dependence, or worsening symptoms all push the conversation forward.
Warning signs of escalating disease matter too. Persistent abdominal pain, ongoing diarrhea, weight loss, fistulas, or hospitalizations signal that current treatment is not enough.
Across the IBD cases our diagnostic partners support, the pattern is consistent: the longer active inflammation runs unchecked, the higher the risk of strictures, fistulas, and surgery. That is the case for acting rather than waiting.
Who May Need to Wait or Avoid Them
Biologics are not automatically right for everyone at every moment. An active, untreated infection usually has to be handled first, and certain conditions call for extra caution.
Screening is mandatory before starting. People taking a biologic should be evaluated for underlying infections that could become active during treatment, including tuberculosis and hepatitis B, and should be up to date on vaccinations such as influenza, pneumococcal, and COVID-19.
The table below maps common situations to what they typically suggest and a sensible next step. It is a starting point for a conversation with your specialist, not a substitute for one.
| Your situation | What it suggests | Typical next step |
| Mild Crohn’s, well controlled on mesalamine | Biologic may not be needed yet | Stay on current plan, monitor |
| Moderate-to-severe disease at diagnosis | Early biologic is often favored | Discuss top-down therapy with GI |
| Steroid-dependent or frequent flares | Conventional therapy is failing | Evaluate for a biologic |
| Fistulizing (especially perianal) disease | Strong indication for anti-TNF | Specialist referral, imaging |
| Failed or lost response to anti-TNF | Switch class, do not give up | Consider ustekinumab or vedolizumab |
| Active untreated infection (TB, hepatitis B) | Biologic must wait | Screen and treat infection first |
About one million Americans live with this disease, so this is far from a niche decision. A 2023 study in Gastroenterology estimated that 2.39 million Americans have IBD, including 1.01 million with Crohn’s disease. Many of them will face the biologic question at some point.
Special Situations to Discuss With Your Doctor
Some life stages change the calculation, though they rarely rule biologics out. Pregnancy is the clearest example, where the goal is controlling disease while weighing each drug’s profile, and decisions are made jointly with a gastroenterologist and obstetrician.
Older adults are another group that warrants a closer look. Because infection risk rises with age and other conditions, the choice of agent and the monitoring plan are tailored accordingly.
Biologics are also used in children with Crohn’s, and several anti-TNF agents have an established pediatric track record. Whatever the age, our medical reviewers stress that these are individualized calls, not one-size decisions.
The Types of Biologics for Crohn’s Disease
Once a biologic is on the table, the next question is which one. The FDA has approved several classes, and the menu has grown quickly. Patients booking tests with HealthCareOnTime often ask how these differ, so here is the practical breakdown.
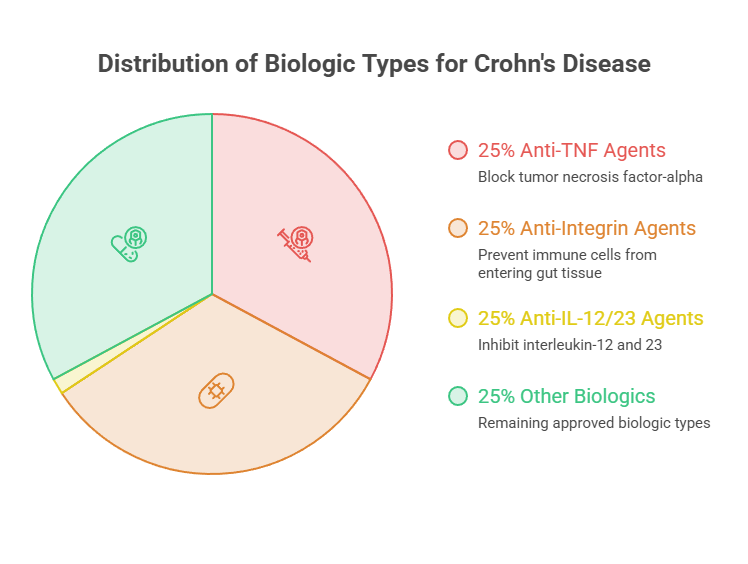
Anti-TNF Agents
Anti-TNF drugs were the first biologics for Crohn’s and remain widely used. This group includes infliximab (Remicade), adalimumab (Humira), and certolizumab pegol (Cimzia).
They block TNF-alpha, a central driver of inflammation, and they have decades of data behind them. They also carry the most established evidence for fistulizing disease.
A practical advantage is access and price. Adalimumab and infliximab now have biosimilars, lower-cost versions that work the same way, which has widened options for many patients.
Anti-Integrin Agents
The second class blocks immune cells from migrating into the gut. Integrin receptor antagonists include natalizumab (Tysabri) and vedolizumab (Entyvio); they stop proteins on cell surfaces that let immune cells attach and move into inflamed areas.
Vedolizumab is notable for acting mostly in the gut, which appeals to patients and doctors who want a more targeted safety profile. The AGA suggests vedolizumab as a first-line option.
This gut-selective action often comes up when infection risk is a particular concern, though every choice has trade-offs worth reviewing with your team.
IL-12/23 and IL-23 Inhibitors
The newest and fastest-growing group targets interleukins. Ustekinumab (Stelara) blocks IL-12 and IL-23, while a wave of newer drugs block IL-23 alone.
The 2025 expansions reshaped this class. Mirikizumab (Omvoh) was approved for moderate-to-severe Crohn’s in January 2025, and guselkumab (Tremfya) in March 2025; both are IL-23 inhibitors, joining risankizumab (Skyrizi).
This class is increasingly used first. In North America, IL-23 therapy has begun displacing anti-TNF as the first-line standard for Crohn’s, after trials showed that targeting IL-23 alone delivered stronger endoscopic outcomes than blocking IL-12 and IL-23 together.
Where JAK Inhibitors and Biosimilars Fit
Two other categories belong in the picture, even though one is not technically a biologic. JAK inhibitors are small-molecule pills, not biologics, but they treat the same disease. Upadacitinib (Rinvoq) is FDA approved for Crohn’s and is taken orally as a tablet.
Biosimilars are the cost story. The arrival of biosimilar ustekinumab created a new price floor, with seven FDA-approved biosimilars entering the US market in 2025.
The table below compares the main classes by what they target, how they are given, and where they tend to fit. Brand names are examples, not endorsements.
| Class | Examples (brand) | Target | How it’s given | Best-fit use |
| Anti-TNF | infliximab (Remicade), adalimumab (Humira), certolizumab (Cimzia) | TNF-alpha | IV infusion or injection | Broad use, strong for fistulizing disease |
| Anti-integrin | vedolizumab (Entyvio), natalizumab (Tysabri) | Gut integrins | IV infusion | Gut-selective, infection-risk concerns |
| IL-12/23 inhibitor | ustekinumab (Stelara) | IL-12 and IL-23 | IV then injection | Durable option, biosimilars available |
| IL-23 inhibitor | risankizumab (Skyrizi), mirikizumab (Omvoh), guselkumab (Tremfya) | IL-23 (p19) | IV then injection | Rising first-line choice |
| JAK inhibitor (not a biologic) | upadacitinib (Rinvoq) | JAK enzymes | Oral pill | Fast-acting, often after other therapy |
| Biosimilars | adalimumab, infliximab, ustekinumab versions | Same as reference drug | IV or injection | Lower-cost equivalents |
Do Biologics Actually Work? What the Evidence Shows
Effectiveness is the reason biologics moved up the treatment ladder. The data, drawn from large US and international trials, show meaningful rates of remission and bowel healing.
Remission and Healing Rates
Start with the anti-TNF benchmark. In the SONIC trial of 508 patients with moderate-to-severe Crohn’s who were naive to immunomodulators and biologics, nearly 57% who received combination therapy with infliximab and azathioprine achieved steroid-free remission at 26 weeks.
The newer IL-23 data are also strong. In the phase 3 VIVID-1 trial, 53% of patients treated with mirikizumab achieved clinical remission at one year compared with 36% on placebo, and 46% showed an endoscopic response versus 23% on placebo.
Durability looks promising too. An open-label extension study indicated that nearly 90% of patients who achieved both clinical remission and endoscopic response at one year maintained those outcomes. Endoscopic healing, not just symptom relief, is the modern goal because it tracks with fewer surgeries.
What “Remission” Really Means
Remission is not a single finish line, which surprises many patients. Doctors separate clinical remission, meaning symptoms have settled, from endoscopic remission, meaning the bowel lining actually looks healed on a scope.
Deep remission combines both, and it is increasingly the target because healed tissue predicts fewer flares and fewer surgeries down the line. That is why your gastroenterologist may order a colonoscopy even during a stretch when you feel completely fine.
Across patients we serve, the lesson is that feeling better is the start, not proof the job is done. Objective testing confirms whether a biologic is truly controlling the disease beneath the surface.
Which Biologic Is Best for Your Situation
There is no single best biologic, but evidence does point in useful directions, and your prior treatment matters. The split is usually between people who have never tried an anti-TNF and those who have.
For people new to these drugs, anti-TNF therapy ranks highly. In a network meta-analysis, anti-TNF combination therapy was the most efficacious option in biologic-naive patients, while upadacitinib ranked highest in biologic-exposed patients.
For those who have already failed an anti-TNF, the guidance shifts. In patients who have not responded to anti-TNF agents, the AGA recommends ustekinumab or vedolizumab. Our medical team adds that safety, dosing convenience, and insurance coverage all factor into the final pick.
How Long They Take to Work
Biologics are not instant. Many use an induction phase of more frequent dosing to bring inflammation down, followed by maintenance dosing to keep it there.
Response often shows over weeks, not days. Some patients feel better within the first month or two, while bowel healing can take longer and is confirmed by follow-up testing.
Patience and follow-through matter. Stopping early or skipping doses can let inflammation rebound, which is why staying on schedule and keeping monitoring appointments is part of the plan.
The figures below put the numbers and the scale of the disease side by side, with sources noted inside the table.
| Metric | Figure | Source |
| Americans with Crohn’s disease | About 1.01 million | Gastroenterology (2023) |
| Infliximab + azathioprine remission (26 wks) | About 57% steroid-free | NEJM / SONIC |
| Mirikizumab clinical remission (1 yr) | 53% vs 36% placebo | VIVID-1 trial |
| Mirikizumab endoscopic response (1 yr) | 46% vs 23% placebo | VIVID-1 trial |
| Patients first prescribed a biologic (historically) | Less than 1% | Medical News Today / AGA |
| IBD patients who take biologics | Less than 20% | GoodRx analysis |
Risks, Side Effects, and Required Screening
No effective Crohn’s drug is risk-free, and honesty about trade-offs is part of good care. Because biologics quiet part of the immune system, infection is the central concern.
Infection Risk and the Pre-Treatment Workup
Screening comes first for a reason. Before and during treatment, patients should be evaluated for infections such as tuberculosis and hepatitis B that could become active, and should be current on recommended vaccines.
Staying alert during treatment matters as well. Any symptoms of infection, such as fever, cough, or chills, should be discussed with a healthcare professional quickly to help avoid serious illness.
Patients we serve sometimes worry this makes biologics dangerous. It is better framed the other way: screening and monitoring are what make these drugs safe to use, much like a pre-flight checklist.
Other Risks and How Doctors Monitor Them
Beyond infection, the warning labels list less common risks that vary by drug. Ustekinumab, for example, may raise the odds of serious infection or sepsis, and labels note possible allergic reactions, lung inflammation, and rare concerns about certain cancers or nervous system disorders.
Some drugs require lab checks. With certain agents, your doctor monitors liver function before, during, and after treatment, and may pause therapy if there are signs of liver trouble.
The JAK pill class carries its own profile. Compared with selective IL-23 inhibitors, JAK inhibitors appear to carry a higher infection risk, and clinicians check for underlying cardiac disease or a clotting disorder before starting one, though overall risk remains low.
Cost, Insurance, and Getting Approved
For many patients, the hardest part of biologics is not the medicine but the paperwork and the price. These are specialty drugs, and the sticker numbers are large.
What Biologics Cost and How Biosimilars Help
The annual figures are steep. A 2017 study found infliximab infusion therapy cost $38,782 in year one and $49,897 in year two, with vedolizumab in a similar range.
Other agents vary. Some biologics, such as Stelara, can run up to almost $40,000 per fill, while the JAK pill upadacitinib costs roughly $6,781 to $12,650 per fill.
Biosimilars are bending the curve. Three drug classes now have biosimilars in the $10,000 range rather than the $100,000 range, which expands access and makes combination strategies more feasible. What you actually pay depends heavily on insurance and copay assistance.
Step Therapy, Prior Authorization, and Patient Assistance
This is where guidelines and insurance often collide. One study found that 98% of insurance policies are inconsistent with AGA treatment guidelines, requiring step-wise drug failure before approving a biologic.
The delays are real. Prior authorizations are the most common barrier, affecting 51% of biologic prescriptions, and step therapy mandates affect 11%, with median delays of 29 days for a first appeal and 73 days for an external review.
Help exists, and using it pays off. The Crohn’s & Colitis Foundation maintains a directory of patient financial assistance programs and recommends appealing denials with a letter of medical necessity, supporting records, and peer-reviewed evidence. Our medical reviewers urge patients never to stop a biologic for cost reasons without first asking the prescriber’s office about assistance.
What to Expect When You Start a Biologic
Starting a biologic is a process, not a single appointment. Knowing the shape of it ahead of time makes the experience far less daunting.
Induction and Maintenance
Most biologics begin with loading doses to bring inflammation under control, then settle into a steady maintenance rhythm. A common pattern is an initial IV dose, then ongoing doses every several weeks, with some agents shifting to a shot every 8 weeks.
Delivery varies by drug. Some are intravenous infusions given in a clinic, while others are subcutaneous injections you can learn to give yourself at home.
That home option matters for daily life. Subcutaneous administration done at home is possible for several biologics, which reduces clinic visits and gives many patients more autonomy.
Combination Therapy and Monitoring Response
Sometimes a biologic is paired with an immunomodulator, especially with anti-TNF drugs, to improve response and reduce the chance the body forms antibodies against the drug.
Monitoring tells you whether it is working. Your gastroenterologist tracks symptoms, blood markers such as CRP, stool tests like fecal calprotectin, and periodic endoscopy to confirm healing.
If a drug stops working, that is not the end of the road. Switching to another class is common, and response is highly individual, so a second or third option may succeed where the first did not.
Do Biologics Replace Surgery for Crohn’s?
A common hope is that the right biologic makes surgery a thing of the past. The honest answer is that biologics reduce the need for surgery for many people, but they do not erase it entirely.
Some complications still call for an operation. Strictures that block the bowel, abscesses, and fistulas that do not respond to medication may need surgical repair, sometimes alongside ongoing drug therapy.
Even so, controlling inflammation early changes the odds. By calming the disease before it scars the bowel, biologics can delay or prevent some procedures, which is a central reason guidelines now favor starting them sooner rather than later.
Frequently Asked Questions
When are biologics recommended for Crohn’s disease?
Biologics are generally recommended for moderate-to-severe or fistulizing Crohn’s, or when conventional drugs fail. US guidelines now favor early use rather than waiting through multiple failures, because starting sooner is linked to lower relapse rates and fewer complications. Your gastroenterologist decides based on disease severity, testing, and your history.
What is the first-line biologic for Crohn’s?
There is no single answer, and practice is shifting. The AGA lists anti-TNF agents or ustekinumab as first-line, with vedolizumab suggested. More recently, IL-23 inhibitors like risankizumab and guselkumab have moved toward first-line use in North America based on strong endoscopic results. The right pick depends on your case.
How long do biologics take to work for Crohn’s?
Biologics are not instant. Many patients notice symptom improvement within the first few weeks to a couple of months during the induction phase. Bowel healing can take longer and is confirmed by follow-up labs or endoscopy. Staying on schedule is important, since missed doses can let inflammation return.
Do I have to fail other drugs before starting a biologic?
Clinically, not necessarily, since guidelines support early use in moderate-to-severe disease. In practice, many insurers require step therapy, meaning you try and fail cheaper drugs first. If that conflicts with your doctor’s recommendation, an appeal with a letter of medical necessity and supporting records can sometimes secure approval.
Are biologics for Crohn’s safe long term?
Biologics have a long safety record, especially anti-TNF agents used for decades. The main risk is infection, since they suppress part of the immune response. Screening for tuberculosis and hepatitis B, staying current on vaccines, and ongoing monitoring keep that risk low. Talk with your doctor about your individual profile.
What is the difference between a biologic and a biosimilar?
A biosimilar is a lower-cost version of an existing biologic, similar to how a generic relates to a brand drug. It works the same way, treats the same conditions, and has comparable safety and effectiveness. Biosimilars for adalimumab, infliximab, and ustekinumab have meaningfully reduced costs for Crohn’s patients.
How are biologics for Crohn’s given, IV or injection?
Both, depending on the drug. Some biologics are intravenous infusions given at a clinic or infusion center, often during induction. Others are subcutaneous injections that you can learn to give yourself at home every few weeks. Several drugs start with an IV dose, then switch to home injections for maintenance.
How much do Crohn’s biologics cost?
List prices are high. Infliximab infusion therapy can run roughly $38,000 to $50,000 per year, and some agents cost up to about $40,000 per fill. Biosimilars and copay assistance often reduce out-of-pocket costs dramatically for insured patients. Always ask your prescriber’s office and the Crohn’s & Colitis Foundation about assistance programs.
Can biologics put Crohn’s into remission?
Yes, that is the goal. In trials, a meaningful share of patients reach clinical remission and bowel healing. Combination infliximab and azathioprine achieved about 57% steroid-free remission at 26 weeks in one major study, and newer IL-23 drugs show strong one-year remission rates. Individual results vary.
What are JAK inhibitors, and how do they compare to biologics?
JAK inhibitors are pills, not biologics, that also target inflammation in Crohn’s. Upadacitinib is FDA approved and acts fast. Compared with selective IL-23 inhibitors, JAK drugs may carry a somewhat higher infection risk, and doctors screen for heart and clotting issues first. They are often used when other therapy is inadequate.
What tests are needed before starting a biologic?
Before starting, doctors screen for infections that could flare during treatment, including tuberculosis and hepatitis B, and check that your vaccinations are current. Baseline bloodwork is common, and some biologics require liver function monitoring. This workup protects you, since the drug quiets part of your immune defense.
What happens if a biologic stops working?
Losing response is common over time and is not a dead end. Doctors may adjust the dose, check drug levels, or switch to a different class entirely. For patients who previously failed an anti-TNF, options like ustekinumab, vedolizumab, or a JAK inhibitor are frequently effective. The plan is tailored to you.
Disclaimer: This article is for general education and is not a substitute for professional medical advice, diagnosis, or treatment. Crohn’s disease and biologic therapy decisions are highly individual. Our medical reviewers urge you to discuss your symptoms, treatment history, and options with a qualified gastroenterologist before starting, stopping, or changing any medication.
References
- AGA recommends early use of biologics in moderate-to-severe Crohn’s disease, American Gastroenterological Association https://gastro.org/press-releases/aga-recommends-early-use-of-biologics-in-patients-with-moderate-to-severe-crohns-disease/
- Biologic drugs for Crohn’s disease, Medical News Today https://www.medicalnewstoday.com/articles/biologics-treatment-crohns-disease
- Biologics for Crohn’s Disease Treatment: Purpose, Risks, Benefits, WebMD https://www.webmd.com/ibd-crohns-disease/crohns-disease/crohns-biologics
- FDA approves Lilly’s Omvoh (mirikizumab) for Crohn’s disease, Eli Lilly https://investor.lilly.com/news-releases/news-release-details/fda-approves-lillys-omvohr-mirikizumab-mrkz-crohns-disease
- FDA’s 2025 GI Approvals Bolster IBD Care, MedCentral https://www.medcentral.com/gastroenterology/ibd/fdas-2025-gi-approvals-bolster-ibd-care
- SONIC: 2-Drug Combo Twice as Effective for Crohn’s Remission, Gastroenterology https://www.gastrojournal.org/article/S0016-5085(10)00740-7/fulltext
- Comparative Efficacy of Therapies for Moderate to Severe Crohn’s Disease, Network Meta-Analysis (NIH) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12546778/
- How Much Does Crohn’s Medication Cost?, HealthCentral https://www.healthcentral.com/condition/crohns-disease/cost-of-crohns-disease-medication
- The True Cost of Crohn’s Disease, GoodRx https://www.goodrx.com/conditions/crohns-disease/true-cost-of-crohns-disease
- Paying for IBD Treatment: Costs, Insurance, and Assistance, Aidy https://aidyhq.com/learn/paying-for-uc-treatment-costs-insurance-patient-assistance-programs





