
Here is a number BlueChew will never print on its homepage. PDE5 inhibitors are effective in only about 60% to 70% of patients, and up to 40% of men do not get a satisfactory response from them. If your chew did nothing on Saturday night, you are not broken and you are not unusual. You are standing in a very crowded room.
Table of Contents
Quick Answer: BlueChew may not work because of eight fixable problems: a dose below the standard starting strength, wrong timing, a high-fat meal or heavy alcohol, missing sexual arousal, too few attempts to judge it fairly, an untreated condition like diabetes or low testosterone, an interfering medication, or lifestyle factors. Most non-responders become responders once the dose is titrated and the real cause is tested for.
At a Glance
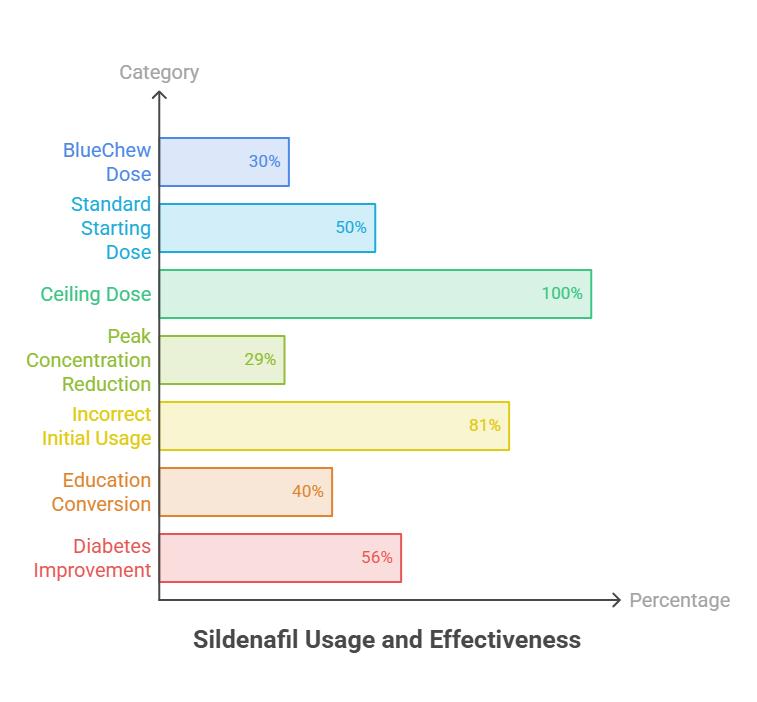
- BlueChew’s entry sildenafil chew is 30 mg. The standard starting dose of prescription sildenafil is 50 mg, and the ceiling is 100 mg.
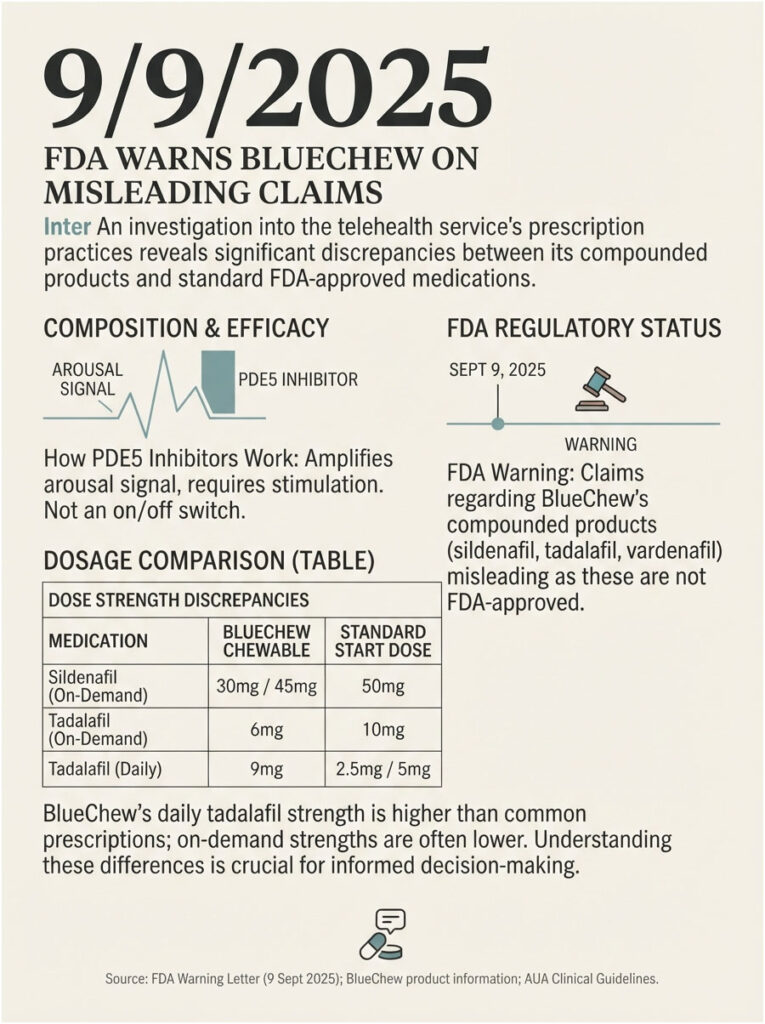
- In September 2025, the FDA warned BlueChew’s parent company that claims implying its compounded products are the same as FDA-approved drugs are false or misleading.
- A high-fat meal cuts peak sildenafil concentration by 29% and delays it by a full hour.
- One study found 81% of men took sildenafil incorrectly at first, and education alone converted 40% of previous non-responders into responders.
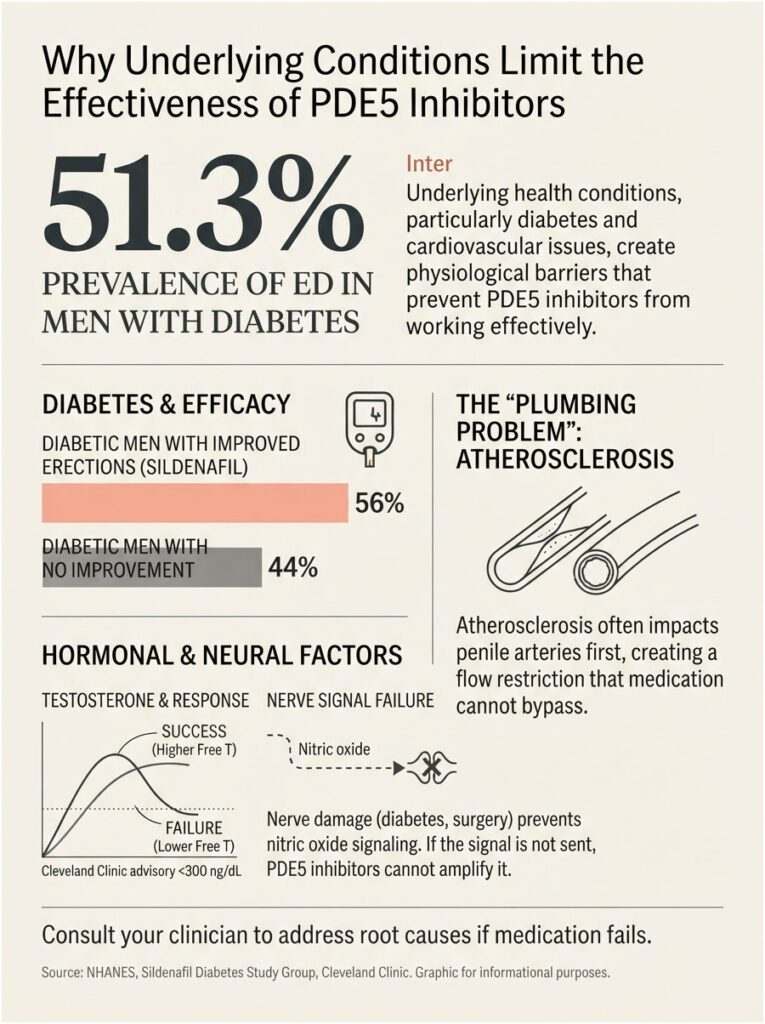
- In men with diabetes, sildenafil improved erections in 56% of patients versus 10% on placebo.
- ED can be an early warning that a heart attack or stroke may follow within 3 to 5 years.
- A pill that fails is a reason to run blood work, not a reason to double the dose.
The 8 Reasons BlueChew May Not Be Working
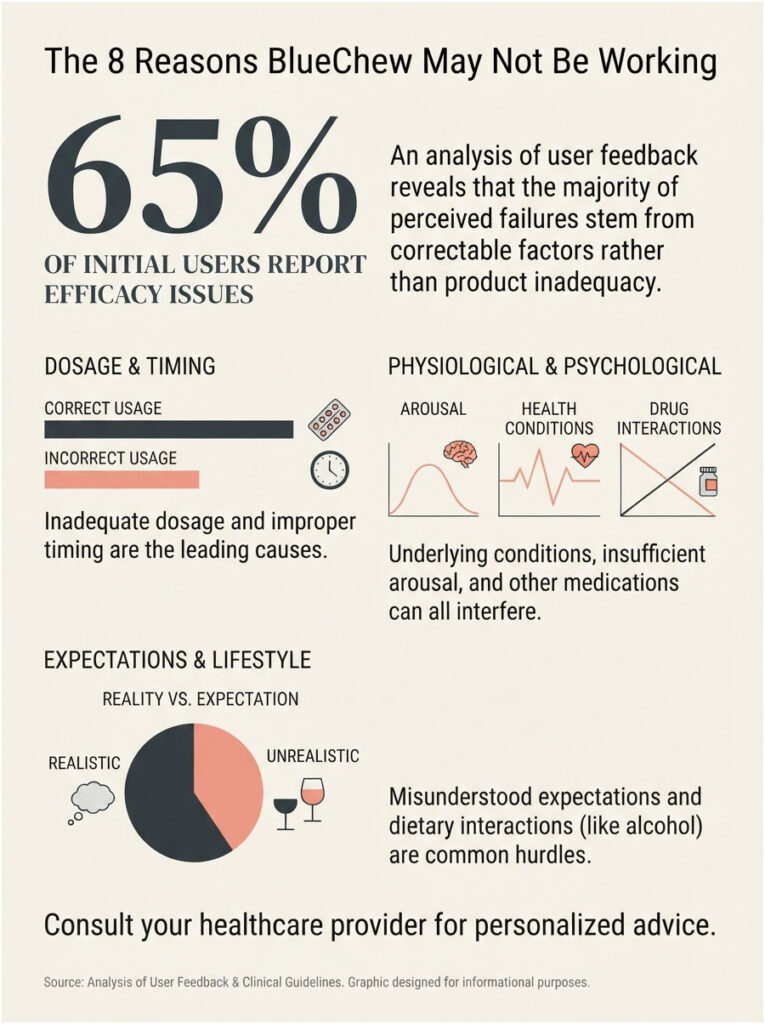
- Your dose sits below the standard starting strength for that molecule.
- You took it too close to sex, or after a heavy meal.
- Arousal was missing, and the pill had nothing to amplify.
- You have not attempted enough times to judge it fairly.
- An untreated condition (diabetes, heart disease, low testosterone) is outrunning the drug.
- Another prescription in your cabinet is canceling it out.
- Smoking, weight, sleep apnea, or alcohol are blunting the vascular response.
- It worked before and stopped, which usually means something else changed.
Work down that list in order. Roughly half of men who believe the medication failed them have simply not reached the bottom of it.
What BlueChew Actually Is (and What It Cannot Do)
BlueChew is a US telehealth subscription that mails chewable tablets after an online consultation. The chews contain sildenafil, tadalafil, or vardenafil, the same active drugs found in Viagra, Cialis, and Levitra.
They arrive compounded into chewable form at strengths that differ from standard pharmacy tablets. That last detail turns out to matter enormously, and we will come back to it.
How a PDE5 inhibitor actually works
Sexual arousal signals nerve endings in penile tissue to release nitric oxide. Nitric oxide triggers cyclic GMP, which relaxes smooth muscle and lets blood flow in. An enzyme called PDE5 then breaks that cyclic GMP back down.
All three BlueChew drugs block PDE5. They protect a signal your body already sent, which is why they only work when sexual stimulation is present.
Read that sequence twice, because it quietly explains half the failures in this article. The pill is an amplifier. It is not a switch.
Compounded, not FDA-approved, and why the phrase matters
On September 9, 2025, the FDA’s Center for Drug Evaluation and Research issued a warning letter to Dermacare LLC dba BlueChew. The agency stated that claims about the company’s compounded sildenafil and tadalafil products were false or misleading, because compounded drug products are not FDA-approved and the claims implied equivalence to approved products.
That is a regulatory finding about labeling, not a safety verdict on the molecules. Sildenafil, tadalafil, and vardenafil carry decades of clinical data behind them.
What it does mean is that the specific chewable tablet in your pocket has not been reviewed by FDA for potency, purity, and batch consistency the way an approved tablet has. Our medical reviewers note that “same active ingredient” does a great deal of quiet work in ED marketing. Same molecule is not the same as same dose, same delivery, or same tested performance.
| Medication | BlueChew Chewable Strength | Standard Starting Dose (Approved Tablet) | Standard Maximum Dose | Approval Status of the Chewable |
| Sildenafil (Viagra) | 30 mg or 45 mg | 50 mg | 100 mg | Compounded, not FDA-approved |
| Tadalafil, on demand (Cialis) | 6 mg or 9 mg | 10 mg | 20 mg | Compounded, not FDA-approved |
| Tadalafil, daily (Cialis Daily) | 9 mg | 2.5 mg | 5 mg | Compounded, not FDA-approved |
| Vardenafil (Levitra) | 8 mg | 10 mg | 20 mg | Compounded, not FDA-approved |
| Vardenafil ODT (Staxyn) | Not offered | 10 mg (single strength) | 10 mg | FDA-approved; explicitly not interchangeable with Levitra |
Look closely and you will see the mismatch runs both directions. BlueChew’s daily tadalafil at 9 mg is actually stronger than the 2.5 mg and 5 mg strengths most commonly prescribed for daily use, while every on-demand strength sits below the usual starting dose.
Neither direction is automatically wrong. Both are worth knowing before you decide a drug failed you.
How Often ED Pills Actually Fail (The Numbers Nobody Quotes You)
Failure is common. It is also, in most cases, reversible.
Across large multicenter trials, 30% to 35% of patients fail to respond to PDE5 inhibitors. The listed causes run from severe underlying disease to unrecognized low testosterone to something as ordinary as taking the drug wrong.
| Population or Scenario | Response or Failure Rate | Source | Publication |
| General ED population on PDE5 inhibitors | 60% to 70% respond; up to 40% unsatisfied | Cleveland Clinic | Cleveland Clinic Journal of Medicine |
| Broad review of PDE5 non-response | 30% to 35% fail to respond | NIH / PMC review | Postgraduate Medical Journal |
| Men who dosed sildenafil incorrectly at first | 81% dosed it wrong; education rescued 40% of prior non-responders | NIH / PMC review | Postgraduate Medical Journal |
| Men with diabetes on sildenafil (50 to 100 mg) | 56% improved vs 10% placebo at 12 weeks | Sildenafil Diabetes Study Group | JAMA |
| US men with diabetes who have ED | 51.3% | NHANES analysis | American Journal of Medicine |
| US men with cardiovascular disease who have ED | 50.0% | NHANES analysis | American Journal of Medicine |
| US men living with ED overall | 30 million to 50 million | NIDDK | National Institutes of Health |
Patients booking blood tests through HealthCareOnTime often ask whether a failed ED pill means something is permanently damaged. The data points the other way for most men.
The pill usually did not fail. The conditions around it did.
Reason 1: Your Dose May Sit Below the Standard Starting Dose
This is the reason almost nobody in the search results will state plainly, and it belongs at the top of your list.
The 30 mg question
BlueChew’s sildenafil comes in 30 mg and 45 mg. Standard sildenafil tablets come in 25 mg, 50 mg, and 100 mg, and the usual first prescription is 50 mg.
That makes the entry chew roughly 40% weaker than a typical starting tablet and 70% weaker than the ceiling dose. Tadalafil follows the same pattern, at 6 mg against a 10 mg standard start.
If you tried 30 mg twice and quit, you did not test sildenafil. You tested a fraction of it.
Why “chewables absorb better” is not the same as “equivalent”
The counterargument deserves a fair hearing. A chewable or sublingual route can improve absorption, so in principle less drug might be needed.
FDA agrees that route changes exposure. Its own approved orally disintegrating vardenafil, Staxyn, is explicitly not interchangeable with Levitra 10 mg film-coated tablets, because the disintegrating version delivers higher systemic exposure.
Here is the part that decides the argument. Staxyn can make that claim because a manufacturer ran the pharmacokinetic studies and FDA reviewed them. A compounded chewable has no comparable public dataset. “Absorbs better” is a marketing assertion, not a number you can dose against.
What proper titration looks like
The American Urological Association’s ED guideline is unambiguous. For men prescribed an oral PDE5 inhibitor, the dose should be titrated to provide optimal efficacy. That is a Strong Recommendation at Evidence Level B, and it sits alongside a second Strong Recommendation that patients be given instructions to maximize efficacy.
Titration is the standard of care. It is not an upsell, and you are entitled to it.
The one thing you must never do
Do not escalate on your own. Do not take two chews. Do not stack a chew on a leftover tablet from a friend.
Message the prescriber, describe exactly what happened, name the food and the timing, and ask for a documented dose review. In cases reviewed by our medical team, the single most common reversible reason an ED drug “fails” is that nobody ever moved the dose off the lowest rung.
Reason 2: Timing and Food Are Quietly Working Against You
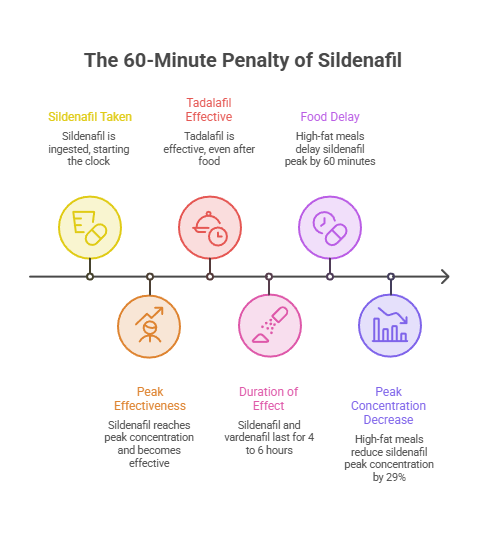
The 60-minute penalty
The FDA label for Viagra is blunt. When sildenafil is taken with a high-fat meal, absorption slows, peak concentration arrives a mean of 60 minutes later, and peak concentration drops by a mean of 29%.
Now stack that on a dose that already starts below the standard. A 30 mg chew swallowed after a burger and fries can deliver a reduced peak of an already-reduced dose, arriving an hour after you planned.
The math is not on your side, and the drug takes the blame for arithmetic.
Three drugs, three different clocks
Sildenafil and vardenafil are as-needed drugs. They take 30 to 60 minutes to work and stay active for roughly 4 to 6 hours.
Tadalafil behaves completely differently, and that difference is useful. Cleveland Clinic guidance is that sildenafil should be taken 30 to 60 minutes before intercourse on an empty stomach, while on-demand tadalafil is not affected by food and works best when taken 60 to 120 minutes ahead.
If dinner is part of the evening, tadalafil is the smarter molecule for you. That is a prescriber conversation, not a self-experiment.
Where alcohol actually crosses the line
A drink or two is generally fine. The problem is volume, not the existence of alcohol.
Heavy drinking is a central nervous system depressant. It suppresses the arousal signal itself, and no PDE5 inhibitor can amplify a signal your brain never sent.
A timing protocol worth screenshotting
- Sildenafil chew: take 60 minutes ahead, on a light or empty stomach
- Vardenafil chew: take 60 minutes ahead, skip the high-fat meal
- Tadalafil chew, on demand: take 60 to 120 minutes ahead, food does not matter
- Cap alcohol at one or two standard drinks
- Never take a second dose within 24 hours
Reason 3: Arousal Is Missing (The Pill Amplifies, It Does Not Start)
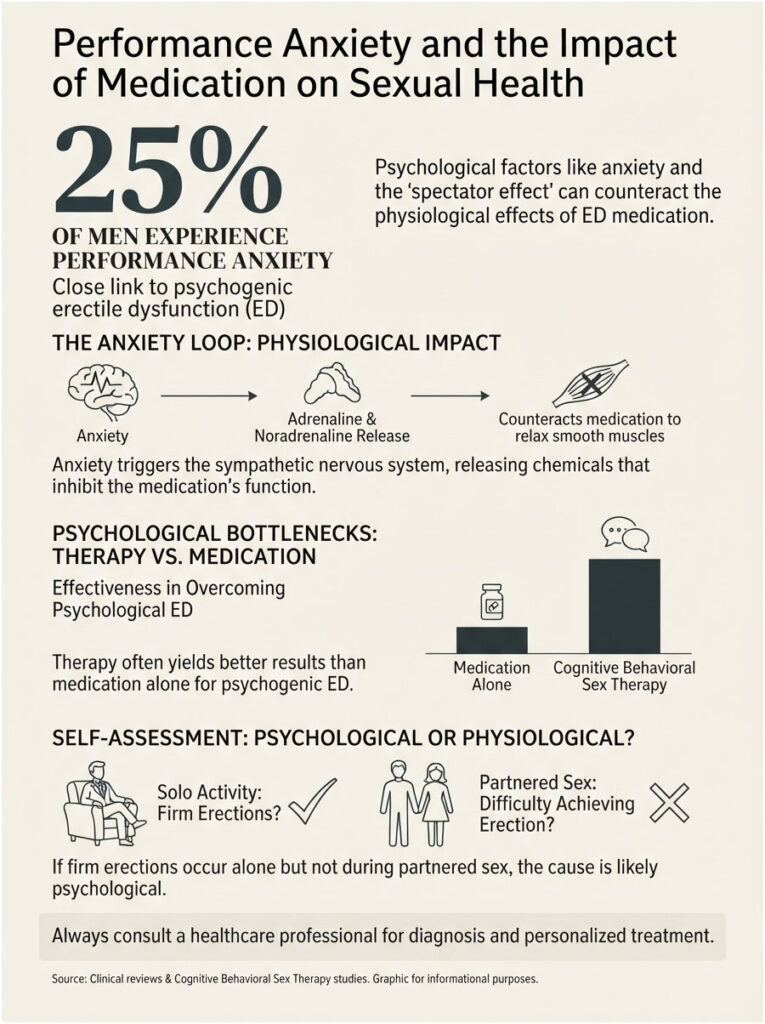
Performance anxiety and the adrenaline problem
Anxiety activates your sympathetic nervous system. Adrenaline and noradrenaline constrict the exact smooth muscle the medication is working to relax.
You end up with a tablet pushing one way and your nervous system shoving harder the other way. In plenty of men, the nervous system wins outright, and the chew gets blamed for a fight it was never equipped to win.
Roughly one in four men experience performance anxiety at some point, and it is strongly tied to psychogenic ED.
The spectator effect
There is a specific trap worth naming. Once you have had one disappointing night, part of your attention detaches from the encounter and starts monitoring your own erection like a nervous referee.
Sex researchers call this spectatoring. The monitoring itself generates the anxiety, the anxiety releases adrenaline, and the adrenaline produces exactly the outcome you were watching for.
The loop is self-sealing, and no dose increase reaches inside it. Cognitive behavioral sex therapy is the tool that does.
The partner and expectation variable
Clinical reviews of PDE5 failure list unrealistic expectations, difficult relationship dynamics, and severe performance anxiety among the leading reasons treatment appears to fail.
None of those show up on a lab report. None of them respond to a stronger tablet. Combining therapy with medication frequently outperforms medication alone for men in this group.
A simple self-test
If you get firm morning erections, or firm erections during solo arousal, but nothing during partnered sex, the bottleneck is very likely psychological.
Raising the dose is the wrong lever. It adds side effects without adding function.
Reason 4: You Have Not Given It a Fair Trial Yet
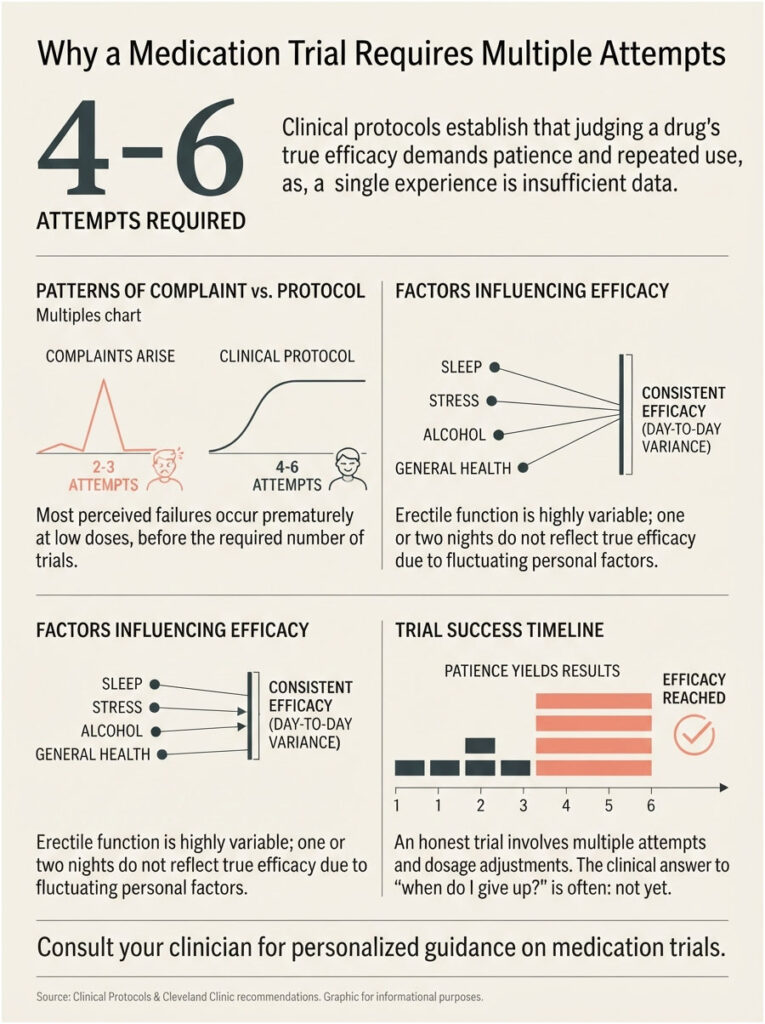
The four-to-eight attempt standard
Clinical protocols do not let a drug off the hook after one disappointing night. Research protocols titrate patients to an optimal effective dose, then require a minimum of four to six attempts at that stabilized dose, over several weeks, before efficacy is judged at all.
Cleveland Clinic’s stated position is that before deciding a medication has failed, several trials with at least 24 hours between doses should be attempted.
Why two bad nights prove nothing
Most complaints arrive after two or three attempts. Almost always at the lowest dose. Usually after dinner and drinks. Nearly always on a high-pressure night.
That is not a drug trial. That is a coin flip with a spectator.
Erectile function fluctuates with sleep, stress, that day’s blood pressure, alcohol, and how the encounter itself unfolds. A single failure tells you almost nothing.
How to run an honest trial
- Fix the dose with your prescriber and keep it constant
- Attempt at least six times, spaced at least 24 hours apart
- Follow the timing and food rules every single time
- Keep a two-line log: what you ate, what you drank, how long before, what happened
- Judge the drug only after the sixth attempt, log in hand
The question our readers send us most often is some version of “how long before I give up?” The clinical answer is almost always: not yet.
Reason 5: An Underlying Condition Is Outrunning the Drug
PDE5 inhibitors improve a vascular response. They do not rebuild a damaged vascular system. When the underlying hardware is failing, a software patch stops helping.
Diabetes and blood sugar control
NHANES data puts ED prevalence at about 51.3% among US men with diabetes and 50.0% among men with a cardiovascular disease history.
The landmark JAMA trial from the Sildenafil Diabetes Study Group remains the reference point. At 12 weeks, 56% of diabetic men taking sildenafil reported improved erections, against 10% on placebo.
That is a real treatment effect with a visibly lower ceiling. Note also that it was achieved with doses starting at 50 mg and adjustable to 100 mg, well above BlueChew’s entry strength.
A 2023 analysis compared 288 PDE5 inhibitor failures against 225 responders. Higher HbA1c, lower free testosterone, and higher sex hormone-binding globulin were the factors that separated the two groups.
Cardiovascular disease and endothelial damage
Atherosclerosis narrows penile arteries before it narrows coronary arteries, for the simple reason that penile arteries are smaller.
If plaque and endothelial dysfunction have already reduced inflow, a drug that relaxes vessels can only work with the pipe it is handed. That is a plumbing problem, not a pharmacy problem.
Low testosterone, and the honest state of the evidence
Testosterone regulates PDE5 expression in penile tissue. Low testosterone can mean fewer targets for the drug to act on.
Cleveland Clinic guidance calls for an early morning testosterone draw before 11:00 am, and notes that levels below 300 ng/dL alongside symptoms such as low libido, fatigue, and loss of body hair may warrant replacement therapy.
Now the honest part, because the evidence here genuinely splits. A 2004 trial in the Journal of Urology found testosterone gel added to sildenafil improved erectile function scores by 4.4 points versus 2.1 for sildenafil alone at four weeks in hypogonadal non-responders. A larger 2012 randomized trial of 140 men, whose sildenafil dose had already been optimized, found the added benefit was about 1 point and not statistically significant.
Testing testosterone is worthwhile. Assuming testosterone will rescue the pill is not. Across the men who book testosterone and HbA1c panels with us, that distinction saves a lot of wasted months.
Nerve damage
After radical prostatectomy, pelvic radiation, spinal cord injury, or advanced diabetic neuropathy, the nitric oxide signal may never arrive.
No PDE5 inhibitor can amplify a signal that was never sent. Men in this group typically need injections, devices, or an implant, not a stronger chew.
Reason 6: Another Medication Is Canceling It Out
The FAERS top offenders
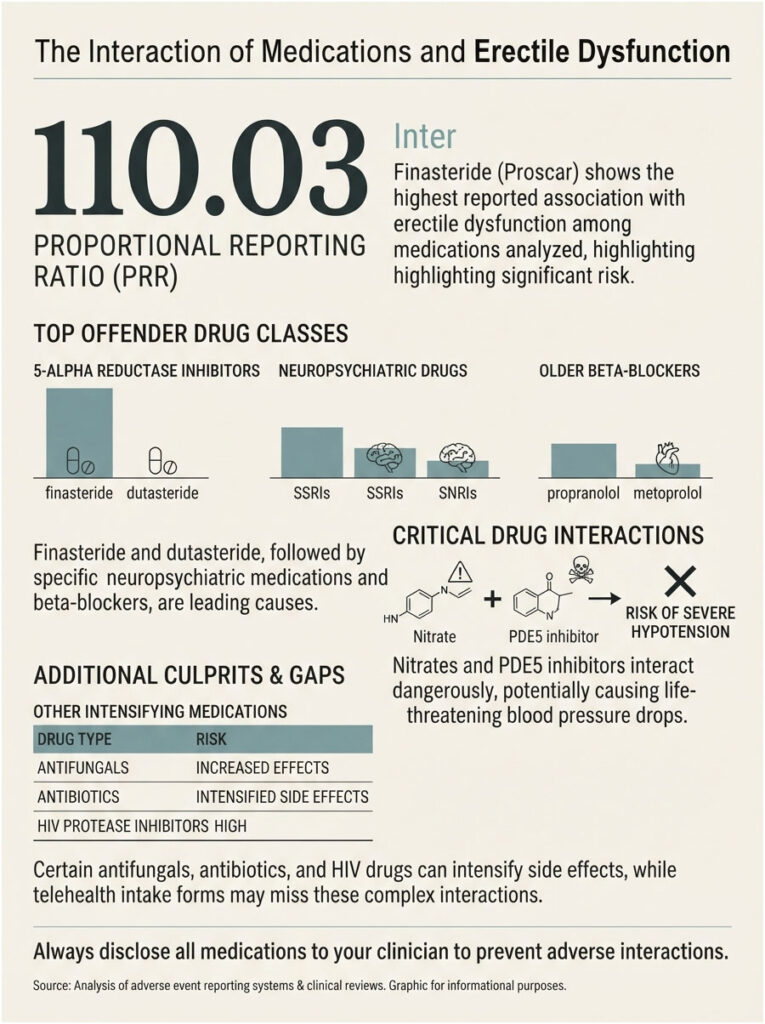
Researchers queried FDA’s Adverse Event Reporting System for erectile dysfunction reports filed between 2010 and 2020. Finasteride and dutasteride produced by far the highest proportional reporting ratios of any medications analyzed, at 110.03 and 9.40 respectively, with 5-alpha reductase inhibitors and neuropsychiatric drugs topping the list overall.
If you take finasteride for hair loss or an enlarged prostate, you have a live suspect sitting in your medicine cabinet right now.
Antidepressants, beta-blockers, and diuretics
SSRIs and SNRIs commonly reduce arousal and delay orgasm. Older beta-blockers including propranolol, metoprolol, and atenolol are associated with ED, while nebivolol appears gentler on erectile function.
High-dose thiazide diuretics have been linked to worse erectile function than other blood pressure drugs.
Never stop a blood pressure or psychiatric medication on your own. Bring the full list to your prescriber and ask whether a swap is reasonable. Treating hypertension stays the priority, and changing those drugs is not always clinically appropriate.
The combinations that are dangerous, not merely useless
Nitrates, including nitroglycerin, isosorbide mononitrate, and recreational “poppers,” can cause a severe and potentially life-threatening drop in blood pressure when combined with any PDE5 inhibitor. Alpha-blockers prescribed for prostate enlargement or blood pressure carry a related risk.
Certain antifungals, some antibiotics, and HIV protease inhibitors raise drug levels in the blood, intensifying both effects and side effects.
If the telehealth intake form did not ask about every one of these, that is a screening gap, not a pharmacology mystery.
Reason 7: Lifestyle Is Blunting the Response
Smoking and vascular damage
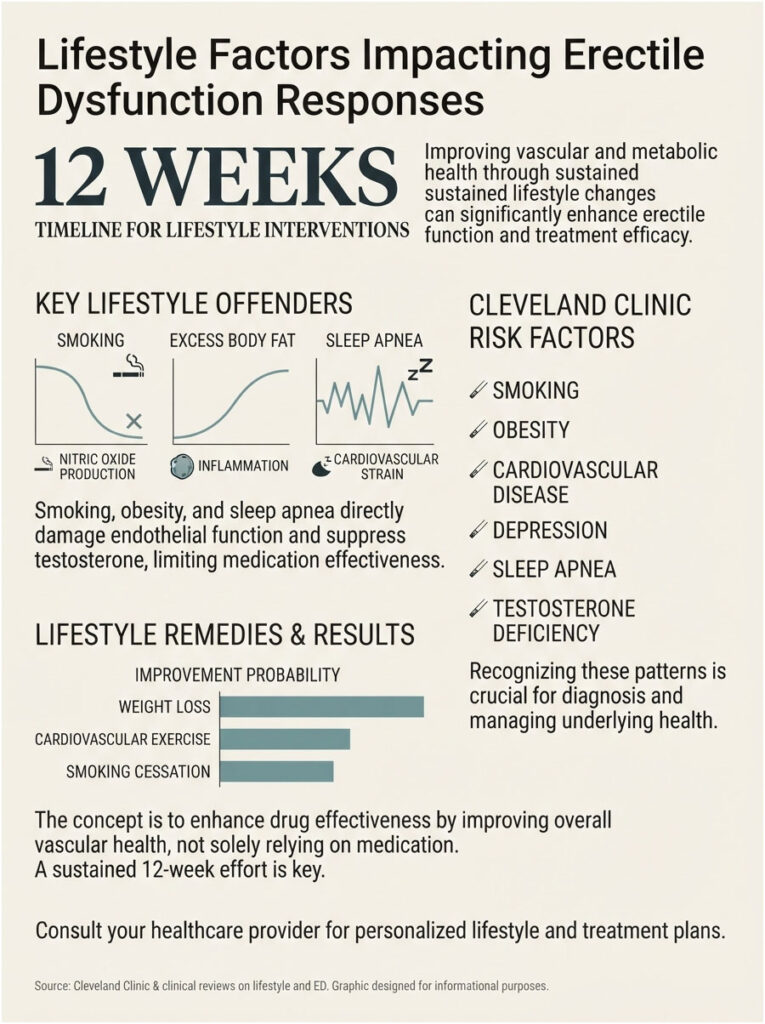
Smoking damages the endothelium, the vessel lining that produces nitric oxide in the first place. Damage the factory and the pill has less product to protect.
Weight and testosterone
Excess body fat converts testosterone to estradiol and drives inflammation that worsens endothelial function. Obesity is an independent ED risk factor in NHANES data.
Sleep apnea, the one nobody checks
Untreated obstructive sleep apnea deserves its own paragraph. It fragments sleep, suppresses overnight testosterone production, and strains the cardiovascular system at the same time.
Snoring, morning headaches, and daytime exhaustion in a man whose ED pill stopped working is a pattern worth investigating.
What actually moves the needle in 12 weeks
Cleveland Clinic lists smoking, obesity, cardiovascular disease, depression, prostate surgery, penile trauma, obstructive sleep apnea, and testosterone deficiency among the leading ED risk factors. It also notes that weight loss, more cardiovascular exercise, reduced alcohol, and quitting smoking can partially relieve symptoms.
None of this produces a result by Friday. Over 12 weeks, though, these changes alter the vascular substrate the pill is working on.
That is the difference between a drug with something to amplify and a drug shouting into an empty room.
Reason 8: It Worked Before, and Then It Stopped
Is tolerance real?
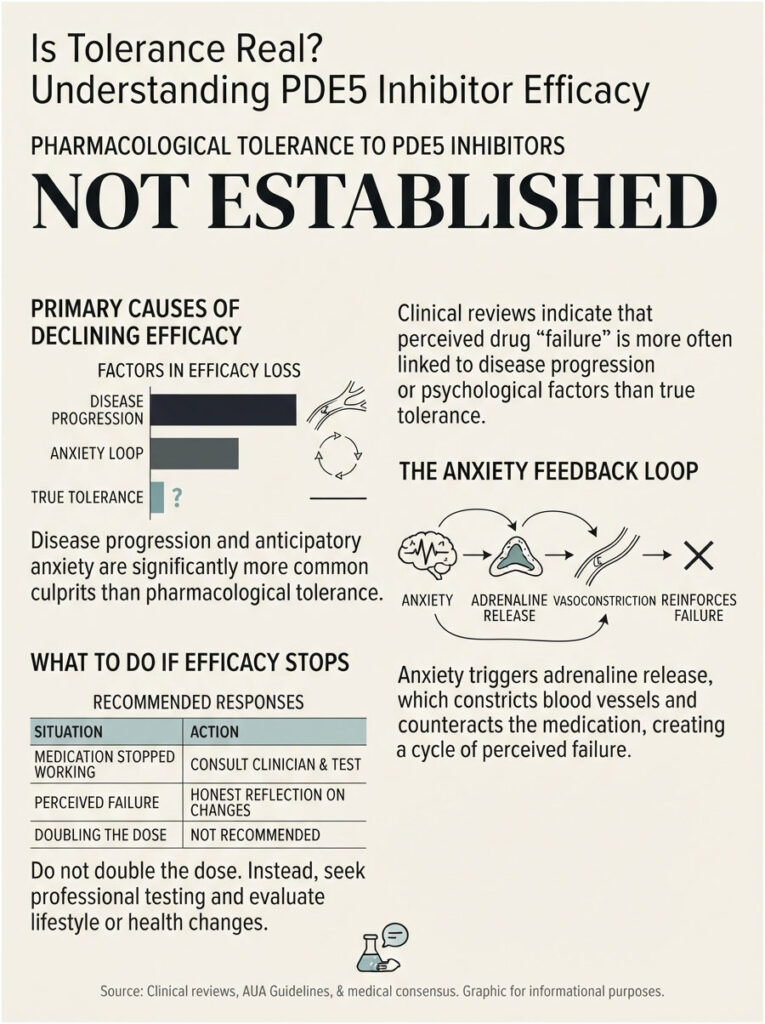
True pharmacological tolerance to PDE5 inhibitors is not well established. Clinical reviews do list tachyphylaxis, or drug tolerance, among possible causes of delayed failure, alongside worsening endothelial dysfunction and progression of penile atherosclerosis.
Tolerance sits low on that list. Disease progression sits high on it.
What “it stopped working” usually means
Something else changed. The usual suspects:
- ED progressed because a vascular or metabolic condition progressed
- A new prescription entered the picture
- Weight, blood pressure, or blood sugar drifted the wrong way
- Sleep debt, work stress, or relationship strain increased
- One bad night created anticipatory anxiety that now runs the show
The anticipatory anxiety loop
That last one is underrated. A drug that worked for eight months can appear to stop working purely because a single failure installed a fear of failure.
The fear releases adrenaline. The adrenaline constricts vessels. The constriction produces another failure, which reinforces the fear.
Our lab partners report that men in this loop very often have entirely normal blood work. The chemistry is fine. The feedback loop is not.
A pill that worked and then stopped is a signal to get tested and to be honest about what changed. It is not a signal to double the dose.
The Blood Tests Worth Running Before You Give Up
The core panel
- HbA1c and fasting glucose
- Early morning total testosterone, drawn before 11:00 am, repeated if low
- Free testosterone and SHBG
- Lipid profile
- TSH
- Prolactin, if libido or testosterone is low
- Complete blood count and kidney function
How to read what comes back
Total testosterone under 300 ng/dL alongside low libido, fatigue, and loss of body hair points toward hypogonadism worth treating.
HbA1c at or above 6.5% points to diabetes. Above 7% in someone already diagnosed suggests glycemic control that is actively undermining vascular health.
A poor lipid profile paired with ED is a cardiovascular conversation, not merely a sexual one. Patients booking tests with us often want a single clean answer. What this panel actually produces is a shortlist: what is treatable, what is progressing, and what needs a specialist.
| If This Sounds Like You | Most Likely Reason | What To Do Next | Test or Action to Request |
| Took it after a steak dinner and three beers | Absorption blunted, arousal suppressed | Retry on a light stomach, 60 minutes ahead, one drink max | No test needed yet; fix the protocol first |
| Tried it twice, nothing happened | Inadequate trial | Complete six attempts at a set dose, 24 hours apart | Keep a log of timing, food, alcohol, arousal |
| Works occasionally at 30 mg, never reliably | Dose below standard starting strength | Ask the prescriber for a documented dose review | Request titration to 45 mg or a standard 50 mg tablet |
| Firm morning erections, nothing with a partner | Psychogenic ED, performance anxiety | Address the anxiety, not the dose | Ask about sex therapy or CBT referral |
| No morning erections at all | Vascular or hormonal cause | Get tested before escalating any medication | Morning total and free testosterone, lipid profile |
| Low libido, fatigue, low mood alongside ED | Possible low testosterone | Confirm with a repeat morning draw | Total testosterone, free testosterone, SHBG, prolactin |
| Diabetic with HbA1c above 7% | Glycemic damage outrunning the drug | Tighten glycemic control alongside ED treatment | HbA1c, fasting glucose, kidney function |
| Snoring, morning headaches, daytime exhaustion | Untreated obstructive sleep apnea | Request a sleep study before changing ED meds | Sleep apnea screening, morning testosterone |
| Take finasteride, an SSRI, or a beta-blocker | Drug-induced ED | Review the full medication list with the prescriber | Ask about alternative agents; never stop on your own |
What BlueChew Costs You Versus the Alternatives
The subscription math
BlueChew plans start around $25 per month and climb toward $130, with per-chew pricing that starts near $2.95 for sildenafil, $3.58 for tadalafil, and $4.34 for vardenafil. Health insurance does not cover it.
The company also does not issue refunds on prescription medication, and it does not ship to North Dakota. Veterans and first responders are offered a lifetime discount.
Generic sildenafil at a US pharmacy
Sildenafil, tadalafil, and vardenafil all lost patent protection years ago. Generic versions are now widely available in the US and dramatically cheaper than they were a decade ago.
They also come in FDA-approved strengths, which means the 50 mg and 100 mg rungs are available to you when 30 mg does nothing. That is not a small advantage when your entire problem is an underdose.
How BlueChew compares to Hims and Ro
Competitor chewables are not identical. Hims offers as-needed tadalafil chews at 11.2 mg, stronger than BlueChew’s 9 mg, and its daily tadalafil chewable runs 8.5 mg against Roman’s 7 mg.
Switching brands is not a strategy on its own. Switching to a properly titrated, FDA-approved dose is.
What Comes After BlueChew (The Escalation Ladder)
Step 1: Fix the fixable variables
Timing, food, alcohol, arousal, adequate trial. This step alone rescues a large share of so-called non-responders.
One study found 81% of patients initially took sildenafil incorrectly, and education alone resolved the problem in 40% of men who had previously failed. Another reported a 55% response rate after education.
Step 2: Ask about dose titration
If 30 mg does nothing after a fair trial, 45 mg is the next rung. Standard-strength tablets from a regular pharmacy are the rung after that.
Step 3: Switch the molecule or go daily
Sildenafil and tadalafil feel different in real life. Low-dose daily tadalafil keeps drug in your system continuously and removes timing pressure entirely, which helps men whose main obstacle is anticipatory anxiety.
Step 4: Combination therapy, supervised only
Daily tadalafil plus on-demand higher-dose tadalafil or sildenafil may be considered by a clinician. Never assemble that combination yourself.
Step 5: Injections, vacuum devices, and implants
Intracavernosal injection therapy produces erections adequate for intercourse in 53.7% to 100% of patients. Vacuum erection devices work mechanically and can be combined with oral drugs.
More than 90% of men who received an inflatable penile prosthesis were able to engage in normal sexual activity, and the procedure carries the highest satisfaction rate of any ED treatment.
What not to spend money on
A randomized controlled trial found no difference between radial wave therapy and sham therapy for treating ED. The Sexual Medicine Society of North America’s position is that stem cell and platelet-rich plasma therapies should not be used in clinical practice.
Men’s clinics market all three aggressively, often blurring radial wave therapy with low-intensity extracorporeal shockwave therapy, which is a separate and more promising technology that the Society still classifies as investigational.
When cancelling is the right call
Cancel when you have run a fair trial at a titrated dose, ruled out interfering medications, tested for the common metabolic and hormonal causes, and still see no useful response.
At that point the subscription is not the answer, and a urologist is.
Red Flags: When ED Is Not a Bedroom Problem
The 3-to-5 year warning window
The American Heart Association’s journal Circulation states it plainly. Because endothelial dysfunction, the first stage of atherosclerosis, usually affects the penis first, ED can be a warning sign that a heart attack or stroke may follow, often within the next 3 to 5 years.
Mayo Clinic notes that Princeton IV consensus recommendations urge clinicians to treat ED as a warning sign for cardiovascular disease, particularly in younger men.
An ED pill that stops working is not a customer service issue. It can be an early cardiovascular finding wearing a deeply inconvenient disguise.
Get care today, not next month
- Chest pain, pressure, or severe dizziness during sex
- An erection lasting longer than 4 hours, which is a medical emergency
- Sudden vision loss, or sudden hearing loss or ringing in one or both ears
- ED that appeared abruptly in your 30s or 40s alongside fatigue or breathlessness
Frequently Asked Questions
Why is BlueChew not working?
Usually one of eight things: a dose below the standard starting strength, poor timing, a high-fat meal or heavy alcohol, missing arousal, too few attempts, an untreated condition such as diabetes or low testosterone, an interfering medication, or lifestyle factors. Most are correctable without abandoning the medication entirely.
Is 30 mg of BlueChew sildenafil the same as 50 mg of Viagra?
No published bioequivalence study confirms that. BlueChew argues chewable absorption is more efficient, which is plausible, but compounded products are not FDA-reviewed for potency or consistency. Treat 30 mg as a starting dose to titrate upward from, not as a proven equivalent to a 50 mg tablet.
How many times should you try BlueChew before deciding it does not work?
Clinical protocols require at least four to six attempts at a properly set dose, spaced 24 hours apart, over several weeks. Two or three tries at the lowest strength, after dinner and drinks, is not a fair trial by any medical standard anywhere.
Is BlueChew FDA approved?
The active ingredients are FDA-approved. The chewable tablets are not. They are compounded products, and in September 2025 the FDA warned BlueChew’s parent company that implying otherwise was false or misleading. That is a regulatory distinction about the tablet, not a safety verdict on the molecule.
Can you take two BlueChew tablets at once?
Do not. Doubling any PDE5 inhibitor without supervision raises the risk of dangerous blood pressure drops, headaches, vision changes, and priapism. If the dose feels too low, message your prescriber and request a documented dose review instead of improvising.
Does food really stop BlueChew from working?
A high-fat meal delays peak sildenafil concentration by about an hour and reduces it by roughly 29%, per the FDA label. It rarely blocks the drug outright, but it can make an already-low dose land too weakly and too late. Tadalafil is unaffected by food.
Why does BlueChew work some nights and not others?
Erectile function varies daily with sleep, stress, alcohol, blood pressure, and arousal. A dose sitting right at your response threshold will succeed when conditions are favorable and fail when they are not. Inconsistency usually signals a dose too low, not an unreliable drug.
Can low testosterone stop BlueChew from working?
It can contribute. Testosterone regulates PDE5 expression in penile tissue, so low levels may mean fewer drug targets. Get an early morning total testosterone drawn before 11:00 am. Evidence on whether replacement rescues a failing PDE5 inhibitor is genuinely mixed, so test before assuming.
Does BlueChew work if you have diabetes?
Often, but with a lower success rate. In the landmark JAMA trial, 56% of diabetic men on sildenafil reported improved erections versus 10% on placebo, using doses of 50 mg to 100 mg. Poor glycemic control and longer diabetes duration both reduce the response.
Can you build a tolerance to BlueChew?
True tolerance is not well established. When a PDE5 inhibitor stops working after months of success, more likely explanations are progressing vascular or metabolic disease, a new medication, weight or blood pressure changes, or anticipatory anxiety. That pattern calls for testing, not a bigger dose.
What blood tests help when ED pills are not working?
An HbA1c, an early morning total and free testosterone with SHBG, a lipid profile, TSH, prolactin, and basic kidney function. A 2023 study found high HbA1c, low free testosterone, and high SHBG were the factors distinguishing PDE5 inhibitor failures from responders.
Should you cancel BlueChew if it is not working?
Not yet. First fix the timing, food, and alcohol variables, complete a fair six-attempt trial, request a dose review, and run the blood work. If a properly titrated dose still does nothing after all of that, cancel and book a urology consult instead.
Medical Disclaimer: This article is for general education and is not medical advice, diagnosis, or treatment. HealthCareOnTime does not prescribe medication. Never start, stop, combine, or change the dose of any prescription drug without speaking to a licensed clinician. If you take nitrates or guanylate cyclase stimulators, PDE5 inhibitors can be life-threatening. Seek emergency care for chest pain, sudden vision or hearing loss, or an erection lasting longer than 4 hours.
References
- FDA Warning Letter, Dermacare LLC dba BlueChew, September 9, 2025
- NIDDK (NIH), Definition and Facts for Erectile Dysfunction
- Cleveland Clinic Journal of Medicine, Erectile Dysfunction: What Are the Options When PDE5 Inhibitors Fail?
- American Urological Association, Erectile Dysfunction Guideline
- FDA Prescribing Information, VIAGRA (sildenafil citrate)
- FDA Prescribing Information, STAXYN (vardenafil orally disintegrating tablets)
- JAMA, Sildenafil for Erectile Dysfunction in Men With Diabetes (Sildenafil Diabetes Study Group)
- NIH, Treating Erectile Dysfunction When PDE5 Inhibitors Fail
- Cureus, Predictors of PDE5 Inhibitor Treatment Failure in Patients Diagnosed With Erectile Dysfunction
- Sexual Medicine, Medications Most Commonly Associated With Erectile Dysfunction (FDA FAERS Analysis)
- American Heart Association, Circulation: Cardiovascular Implications of Erectile Dysfunction
- Mayo Clinic, Erectile Dysfunction: A Vital Sign for Cardiovascular Health
- American Journal of Medicine, Prevalence and Risk Factors for Erectile Dysfunction in the US (NHANES)
- Journal of Urology, Randomized Study of Testosterone Gel as Adjunctive Therapy to Sildenafil in Hypogonadal Men Who Do Not Respond to Sildenafil Alone
- Annals of Internal Medicine, Effect of Testosterone Replacement on Response to Sildenafil Citrate





