One in every 37 babies born in the United States now arrives with the help of assisted reproductive technology, according to CDC data compiled by USAFacts. That number has more than doubled in a decade.
Table of Contents
Yet the moment everything hinges on is quiet and quick. After weeks of injections, monitoring, and lab work, the embryo transfer itself takes about five minutes and needs no anesthesia.
Understanding what happens, which type fits your situation, and what the two-week wait really feels like can turn a nerve-wracking step into a clear one. Here’s the full picture.
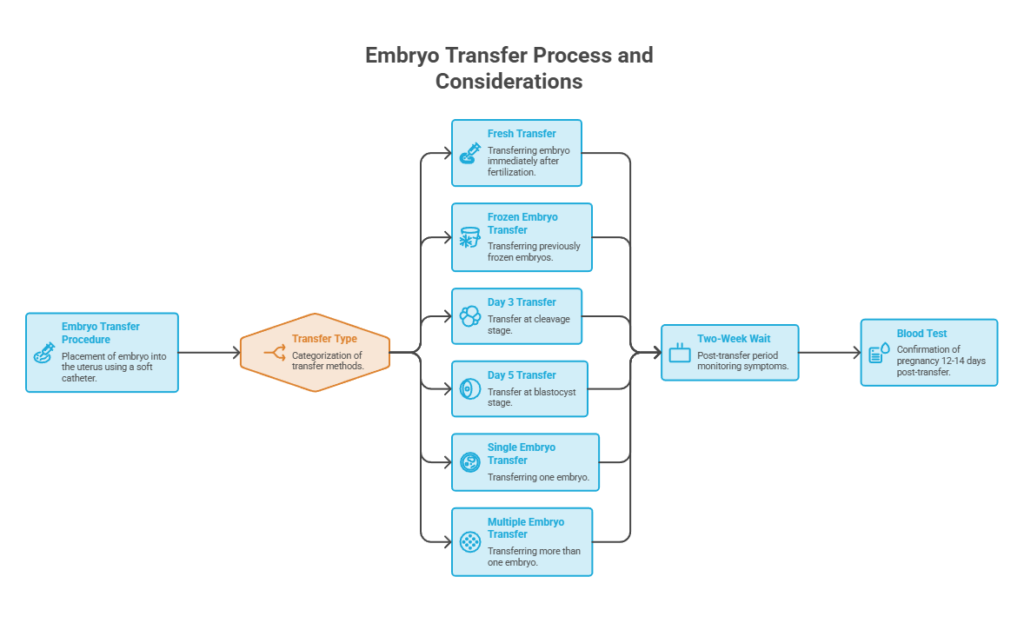
Quick answer: Embryo transfer is the final step of in vitro fertilization (IVF), where a fertilized embryo is placed into the uterus through a thin catheter guided by ultrasound. The procedure takes about five minutes, usually needs no anesthesia, and requires no recovery time. Transfers can be fresh or frozen, done at day 3 (cleavage) or day 5 (blastocyst), and can involve a single embryo or, less often, more than one.
At a Glance
- Embryo transfer is the last stage of IVF; the embryo is placed into the uterus with a soft catheter, not surgically implanted.
- The main types are fresh vs frozen (FET), day 3 vs day 5, and single vs multiple embryo transfer.
- The procedure itself takes roughly five minutes, with no anesthesia and no bed rest afterward.
- Success depends heavily on age: US live birth rates run near 50% under age 35 and fall sharply after 40.
- Frozen transfers are now the most common type and allow time for genetic testing.
- During the two-week wait, symptoms are unreliable; progesterone can mimic early pregnancy, and 10-15% of people feel nothing yet still conceive.
- A blood test around 12 to 14 days after transfer is the only reliable confirmation.
What Is Embryo Transfer?
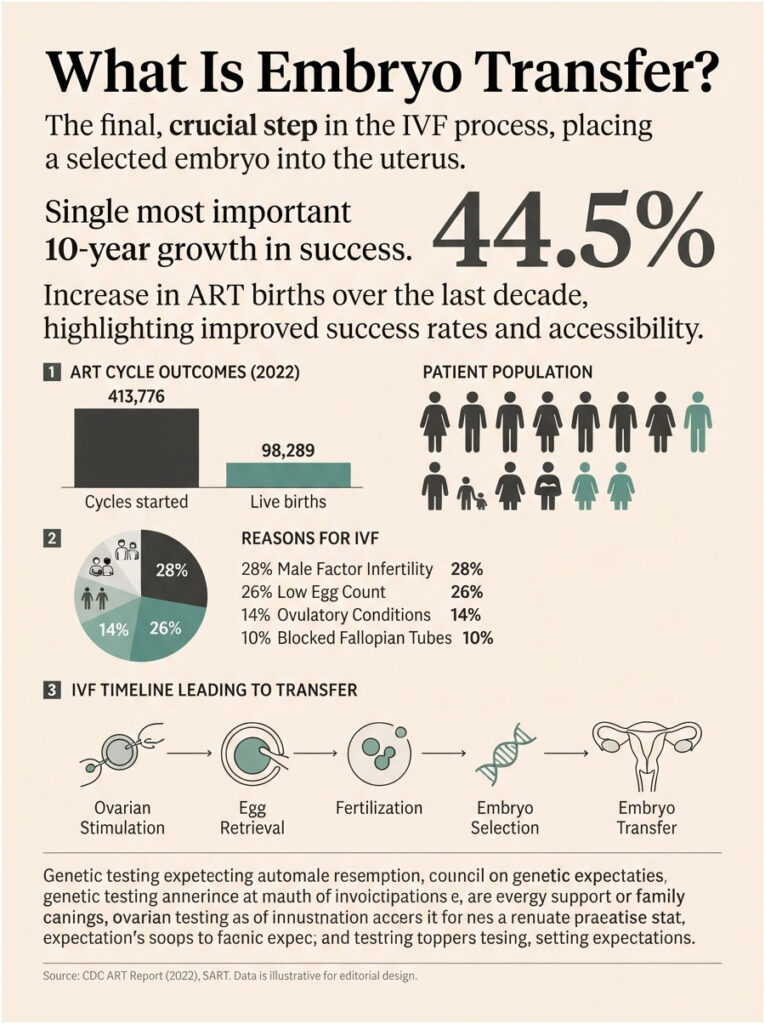
Embryo transfer is the procedure that places a fertilized, developing embryo into a woman’s uterus, where the goal is implantation and pregnancy. It is the concluding step of an IVF cycle.
The name can be slightly misleading. The embryo is not surgically implanted or attached by the doctor. It is gently released near the middle of the uterine cavity, and implantation happens on its own over the following days.
Our medical reviewers note that this is one of the most searched fertility topics precisely because it sounds more dramatic than it is. For most people, the transfer feels similar to a Pap smear.
The scale of IVF in America is large and growing. In 2022, 251,542 patients started 413,776 ART cycles, producing 98,289 babies, a 44.5% rise in ART births over the prior decade.
How It Fits Into the IVF Timeline
Embryo transfer only makes sense in context, so here’s the sequence that leads up to it. IVF begins with ovarian stimulation, using injectable medications to grow multiple eggs at once.
Once the follicles mature, the eggs are collected during egg retrieval, a short procedure done under sedation. In the lab, those eggs are combined with sperm, either through standard insemination or ICSI, where a single sperm is injected into each egg.
The fertilized eggs then grow in culture for several days while embryologists watch their development. The strongest embryos are selected, and one is transferred to the uterus. Any extra good-quality embryos can be frozen for a later cycle.
That final placement is the transfer. Everything before it exists to produce a healthy embryo, and everything after it depends on implantation.
Who Needs Embryo Transfer
Embryo transfer is part of IVF, so anyone using IVF to build a family goes through it. The reasons people reach IVF vary widely, and understanding yours helps set expectations.
According to CDC figures, common drivers include male factor infertility (around 28% of patients), low egg counts or diminished ovarian reserve (about 26%), ovulatory conditions like PCOS (roughly 14%), and blocked or damaged fallopian tubes (about 10%).
Others use IVF specifically to allow genetic testing of embryos before transfer, which can matter for those with inherited conditions. In cases reviewed by our medical team, unexplained infertility and recurrent pregnancy loss are also frequent paths to treatment.
Same-sex couples and single parents using donor eggs, donor sperm, or a gestational carrier also rely on embryo transfer. The procedure is the same regardless of how the embryo was created.
Types of Embryo Transfer
Not all transfers are the same. The type depends on whether the embryo is fresh or thawed, how many days it grew in the lab, and how many embryos go in. The table below lays them out side by side.
| Type | What It Is | Timing | Best Suited For | Key Consideration |
| Fresh transfer | Embryo transferred in the same cycle as egg retrieval | Day 3 or day 5 after retrieval | Those with a receptive lining and no OHSS risk | No freeze-thaw step; less time for hormone recovery |
| Frozen (FET) | Previously frozen embryo thawed and transferred later | Any cycle after freezing | Most patients today; those doing genetic testing | Allows lining prep and PGT; now the most common type |
| Day 3 (cleavage) | Embryo transferred at 6 to 8 cells | 3 days after fertilization | Cases with few embryos to culture longer | Less selection information than blastocyst |
| Day 5 (blastocyst) | Embryo transferred at the blastocyst stage | 5 days after fertilization | Those with several strong embryos | Better selection; slightly higher success per transfer |
| Single (eSET) | One embryo transferred | Fresh or frozen | Most patients, to avoid multiples | Lower twin risk; now the standard of care |
| Multiple | More than one embryo transferred | Fresh or frozen | Select older patients, guided by clinic policy | Raises multiple-birth and preterm risk |
Fresh vs Frozen Embryo Transfer (FET)
A fresh transfer uses an embryo from the current cycle, placed a few days after egg retrieval. A frozen embryo transfer, or FET, thaws an embryo saved from an earlier cycle and transfers it later.
Frozen transfers have become the most common approach in the United States. They let the uterine lining recover from stimulation hormones, allow time for genetic testing, and reduce the risk of ovarian hyperstimulation syndrome (OHSS).
Patients researching fertility care often ask us whether frozen embryos are somehow weaker. Modern vitrification (fast freezing) has made frozen and fresh transfers broadly comparable in success for blastocysts.
Which one fits you comes down to specifics. If you’re at risk of OHSS, want genetic testing, or your lining wasn’t ideal during stimulation, a frozen cycle often makes sense. If your lining is receptive and there’s no reason to wait, a fresh transfer avoids the freeze-thaw step.
Day 3 (Cleavage) vs Day 5 (Blastocyst)
The other major choice is how long the embryo grows before transfer. A day 3 embryo, called a cleavage-stage embryo, has roughly 6 to 8 cells. A day 5 embryo has reached the blastocyst stage, a more developed structure with distinct cell types.
Growing embryos to day 5 gives the lab more information about which are strongest, since weaker embryos often stall before then. A Cochrane review found blastocyst transfer raised pregnancy rates by about 3 to 10% and live birth rates by 3 to 13% compared with cleavage-stage transfer.
There’s a tradeoff. Some embryos that might have survived in the uterus do not make it to day 5 in the lab, so patients with only a few embryos may transfer at day 3. Our medical reviewers note that the right day depends on how many quality embryos you have.
Day 5 has become the default at many clinics because it supports single embryo transfer and genetic testing. Day 3 remains a sound choice when extending culture would risk losing a scarce embryo.
Single vs Multiple Embryo Transfer (eSET)
For years, clinics transferred several embryos to boost the odds. That practice has largely ended in favor of elective single embryo transfer (eSET), which moves one embryo at a time.
The reason is safety. Twins and higher-order multiples carry real risks, including preterm birth, low birth weight, and complications for the mother. Babies conceived through IVF are multiples 12.5% of the time versus 3.2% overall, and clinics work hard to lower that number.
The strategy is working. In 2023, singleton births made up 96.74% of IVF deliveries. Transferring more than one embryo is now reserved for specific situations, often older patients or those with repeated failed cycles, and is governed by professional guidelines from groups like ASRM.
Patients researching fertility care sometimes assume two embryos double their chances. With a strong single blastocyst, the added pregnancy benefit is often small while the multiples risk climbs sharply, which is why clinics counsel carefully.
PGT-Tested Transfers and Embryo Grading
Many transfers today use embryos screened with preimplantation genetic testing (PGT-A), which checks for the correct number of chromosomes. This is one reason frozen transfers have grown so popular, since testing requires time to complete.
Screening aims to select a chromosomally normal embryo, which can improve implantation and lower miscarriage risk. Across the patients we educate, PGT is common for those over 35 or with prior losses, though it is not required for everyone.
Even without genetic testing, embryologists grade embryos on appearance. Blastocyst grading looks at how expanded the embryo is and the quality of the two cell groups that become the baby and the placenta.
Grading guides which embryo to transfer first, but it isn’t a guarantee. A top-graded embryo has better odds, yet lower-graded embryos still lead to healthy pregnancies, which is why your team weighs grading alongside your history.
The Embryo Transfer Procedure, Step by Step
The transfer is one of the simplest procedures in the entire IVF journey. Knowing the sequence removes most of the anxiety around it.
Before the Transfer
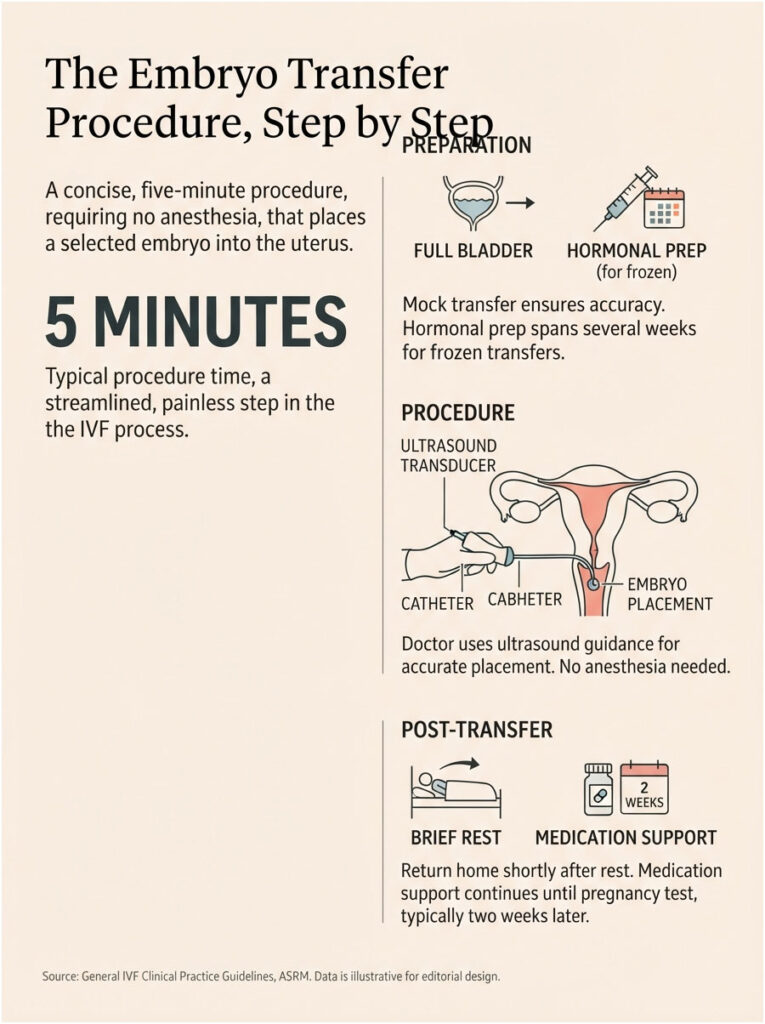
Preparation starts before transfer day. Many clinics perform a mock transfer earlier in the process, a practice run that maps the path through the cervix so the real transfer goes smoothly.
On the day itself, you’ll usually be asked to arrive with a full bladder. A full bladder gently straightens the angle between the cervix and uterus and gives a clearer ultrasound image, which helps the doctor place the embryo accurately.
The embryologist makes a final assessment of your embryos that morning and recommends how many to transfer. Our medical reviewers note that this decision reflects embryo quality, embryo age, and your history with previous cycles.
For a frozen transfer, your body is prepared over the preceding weeks with estrogen and progesterone to build a receptive lining, timed so the lining and embryo are in sync.
During the Transfer
The transfer itself is quick and needs no anesthesia. Shady Grove Fertility describes it as about a five-minute procedure with no recovery time afterward.
You lie back as you would for a Pap smear. The doctor inserts a speculum, then guides a thin, soft catheter loaded with the embryo through the cervix and into the uterus, watching the whole time on an ultrasound monitor.
The embryo is released with a small amount of fluid near the middle of the uterine cavity. The doctor then slowly withdraws the catheter to limit any uterine contractions.
As a final check, the embryologist examines the empty catheter under a microscope to confirm the embryo was delivered and didn’t stick to the tubing. Many clinics also verify your identity and embryo details on a monitor before the transfer.
Right After the Transfer
There’s no surgical recovery to worry about. Once the catheter is removed, you can empty your bladder, and most clinics let you go home shortly after a brief rest.
You return to normal activity the same day. Patients researching fertility care often ask us if they need to lie flat for hours afterward, and current guidance says no.
You’ll continue progesterone and any other prescribed medications to support the lining. The next milestone is the pregnancy test, typically about two weeks later, and everything between the transfer and that test is the two-week wait.
Embryo Transfer Success Rates
Success rates are the number people most want and the number competitors report least clearly. The most reliable US figures come from the CDC’s national ART data, which every fertility clinic is legally required to report under the Fertility Clinic Success Rate and Certification Act.
| Metric | Figure | Source |
| Live birth per cycle, under age 35 (own eggs) | 49.7% | CDC / USAFacts, 2022 |
| Live birth per cycle, ages 35-37 | 36.3% | CDC / USAFacts, 2022 |
| Live birth per cycle, ages 38-40 | 23.1% | CDC / USAFacts, 2022 |
| Live birth per cycle, over age 40 | 7.7% | CDC / USAFacts, 2022 |
| Live birth per transfer, donor eggs/embryos | 42.2% to 52.0% | CDC / USAFacts, 2022 |
| Singleton share of IVF births (2023) | 96.74% | CDC, 2023 |
Across all ages, about 37.5% of ART cycles resulted in live births, and nearly 40% of embryo transfers led to a live birth. These are national averages, and your own odds can differ from them.
Success by Age
Age is the single strongest predictor of success, because egg quality and quantity decline over time. The CDC data shows the gradient clearly, from roughly half of cycles under 35 to under 10% past 40 using your own eggs.
This is why donor-egg transfers, which use younger eggs, hold steadier success across recipient ages. Our medical reviewers note that the age that matters is egg age, which is why donor cycles behave differently from age-matched own-egg cycles.
One more nuance helps here. A single cycle’s rate can look daunting, but many patients undergo more than one cycle, and cumulative odds over several attempts are higher than any single number suggests.
Fresh vs Frozen Success
For blastocysts, fresh and frozen transfers now produce broadly similar live birth rates. Frozen transfers carry the added advantages of hormone recovery time and the option to test embryos before transfer.
Individual results still depend on embryo quality and the lining. In cases reviewed by our medical team, freezing also protects patients at risk of OHSS, who often do better waiting for a planned frozen cycle.
What Affects Your Odds
Beyond age, several factors move the needle. Embryo quality and grading, the thickness and receptivity of the uterine lining, the underlying cause of infertility, and the quality of the embryology lab all play a part.
The CDC also offers a free IVF Success Estimator that factors in your characteristics for a personalized estimate. Our medical reviewers note that these are population-based estimates, useful for planning but not a personal guarantee.
Lifestyle factors like smoking and weight can also influence outcomes, which is why clinics often address them before a cycle. Small, controllable steps won’t override age, but they can help you start from a stronger position.
What to Expect After Embryo Transfer
The two-week wait is often the hardest part emotionally. Understanding what’s actually happening inside your body helps you read the signs without overreading them.
Day by Day: The Implantation Timeline
The embryo does not attach immediately. For the first day or two, a blastocyst hatches from its outer shell and begins settling toward the uterine lining.
Implantation typically begins around days 3 to 6 after transfer, as the embryo burrows into the lining. If it succeeds, the body starts producing hCG, the pregnancy hormone, roughly a week after transfer.
From about day 9 onward, hCG rises enough to eventually register on a test. This timeline is exactly why testing too early gives unreliable results, since the hormone simply isn’t high enough yet.
Common Symptoms and Why Progesterone Fools You
After transfer, many people notice mild cramping, light spotting, bloating, breast tenderness, or fatigue. The catch is that these are also side effects of the progesterone and estrogen used to support the cycle.
That overlap makes symptoms a poor predictor. As several fertility centers stress, the same signs appear in cycles that do and do not result in pregnancy, so reading into them rarely helps.
Just as telling, about 10 to 15% of patients feel no symptoms at all and still have a successful transfer. Patients researching fertility care often ask us whether no symptoms is a bad sign, and it is not.
Light spotting around five to seven days after transfer can reflect implantation, but it can also be a medication effect or a false alarm. The honest takeaway is that only a test settles the question.
The Bed Rest Myth
One of the most persistent myths is that you must stay on strict bed rest to protect the embryo. Current evidence does not support this, and most clinics no longer recommend it.
The embryo will not fall out if you stand, walk, or go about your day. In fact, prolonged bed rest can increase stress and anxiety without improving outcomes.
Light movement like walking is fine and may even help blood flow to the uterus. Our medical reviewers note that most specialists now advise a normal, comfortable routine rather than lying flat for days.
Dos and Don’ts During the Two-Week Wait
A few sensible habits help. Take your prescribed progesterone exactly as directed, stay hydrated, sleep well, and keep activity gentle by avoiding heavy lifting and high-intensity workouts.
On the avoid list, most clinics suggest skipping alcohol, tobacco, hot tubs, saunas, and hot baths, since raising core body temperature is not ideal during this window. Many also recommend pelvic rest until the pregnancy test.
Treat your body as though you might already be pregnant, including following any dietary guidance your clinic gives. Across the patients we educate, that framing tends to reduce second-guessing during a stressful stretch.
It also helps to protect your headspace. Staying off symptom-checker forums, leaning on your support people, and keeping your normal routine can make the wait more bearable.
When to Take a Pregnancy Test (Beta hCG)
The urge to test early is strong, but timing matters more than most people expect. Most clinics schedule a blood test, called a beta hCG, about 12 to 14 days after transfer.
The blood test measures hCG precisely and is far more reliable than a home urine test. Testing too soon risks a false negative, because hCG may not be high enough yet, or a false positive if a trigger shot is still clearing your system.
If the result is positive, the fertility clinic usually monitors you with repeat blood work and early ultrasounds until about 8 to 10 weeks, then transfers your care to an OB-GYN. If it’s negative, your team can review what happened and discuss next steps and support.
Home tests taken during the wait are a common source of distress. Because their timing and sensitivity vary, an early result, positive or negative, can mislead, which is why clinics point to the scheduled blood test as the real answer.
Risks and Signs to Watch For
The transfer itself is very low risk. Most of what you’ll feel afterward is normal, but a few signs warrant a call. Use the table below to sort them.
| Symptom / Scenario | Urgency | Recommended action |
| Mild cramping, light spotting, bloating | Normal | No action needed; expected after transfer |
| No symptoms at all | Normal | Reassuring; wait for your scheduled test |
| Heavy bleeding like a full period | Urgent | Contact your clinic promptly for guidance |
| Severe abdominal pain or cramping | Urgent | Contact your clinic; do not wait it out |
| Fever, or signs of infection | Urgent | Call your clinic right away |
| Rapid bloating, weight gain, shortness of breath (possible OHSS) | Urgent | Call your clinic immediately |
The main procedural risks are minor, such as brief cramping or light spotting from the catheter. The larger risks in IVF relate to multiple pregnancy, which is why single embryo transfer has become the standard of care.
OHSS is a separate concern tied to ovarian stimulation, not the transfer itself, and freezing embryos for a later cycle is one way clinics reduce it. Our medical reviewers note that any severe or sudden symptom deserves a call rather than a wait.
It’s also worth remembering that a failed transfer, while painful, is common and not a sign you did something wrong. Many people conceive on a later attempt, and your clinic can adjust the plan based on what the first cycle showed.
Frequently Asked Questions
What is embryo transfer in simple terms?
Embryo transfer is the final step of IVF, where a fertilized embryo is placed into the uterus using a thin catheter. The embryo is not surgically attached; it’s gently released and implants on its own over the following days. The procedure takes about five minutes and needs no anesthesia.
How long does an embryo transfer take?
The transfer itself takes roughly five minutes, though you’ll spend longer at the clinic for preparation and verification. There’s no anesthesia and no recovery time, so most people go home shortly after and return to normal activity the same day. It’s often compared to a Pap smear.
Is embryo transfer painful?
Most people find embryo transfer painless or only mildly uncomfortable, similar to a Pap smear. The main discomfort usually comes from the full bladder needed for ultrasound guidance, which you can empty right after. Anesthesia is not typically required, though clinics can offer a mild sedative if you’re anxious.
Fresh vs frozen embryo transfer: which is better?
Neither is universally better. Frozen transfers (FET) are now the most common because they allow hormone recovery, genetic testing, and lower OHSS risk. For blastocysts, fresh and frozen produce broadly similar live birth rates. Your reproductive endocrinologist recommends one based on your lining, embryo testing, and OHSS risk.
Day 3 vs day 5 embryo transfer: what’s the difference?
A day 3 embryo has about 6 to 8 cells (cleavage stage), while a day 5 embryo has reached the more developed blastocyst stage. Growing to day 5 gives better selection and slightly higher success per transfer. Patients with fewer embryos may transfer at day 3 to avoid losing them in extended culture.
How many embryos should be transferred?
Most patients now have a single embryo transferred (eSET) to avoid the risks of twins and higher-order multiples. Transferring more than one is reserved for specific cases, often older patients, and follows professional guidelines. Your embryologist and doctor decide based on embryo quality, your age, and your history.
How many days after transfer does implantation happen?
Implantation typically begins around 3 to 6 days after a blastocyst transfer, as the embryo burrows into the uterine lining. The embryo does not attach immediately; it spends the first day or two settling in. hCG, the pregnancy hormone, usually starts rising about a week after transfer.
Do you need bed rest after embryo transfer?
No. Strict bed rest is a myth and is no longer recommended by most clinics, since it doesn’t improve success and can increase stress. The embryo will not fall out when you walk or stand. Light activity is fine and may help blood flow; just avoid heavy lifting and intense exercise.
What are the common symptoms after embryo transfer?
Common sensations include mild cramping, light spotting, bloating, breast tenderness, and fatigue. Importantly, these can also be side effects of progesterone medication, so they don’t reliably predict pregnancy. About 10 to 15% of people feel nothing at all and still conceive, so symptoms alone can’t confirm success.
When can I take a pregnancy test after embryo transfer?
Most clinics schedule a blood test (beta hCG) about 12 to 14 days after transfer, which is the most reliable confirmation. Testing earlier with a home kit risks a false negative if hCG is still low, or a false positive if a trigger shot hasn’t cleared. Waiting for the clinic test gives the clearest answer.
What are the do’s and don’ts after embryo transfer?
Do take your progesterone as prescribed, stay hydrated, sleep well, and keep activity gentle. Don’t do heavy lifting, high-intensity workouts, hot tubs, saunas, alcohol, or tobacco, and follow your clinic’s guidance on pelvic rest. Treating your body as if you might be pregnant is a sensible general approach during the wait.
What is the success rate of embryo transfer?
Success depends heavily on age. Using CDC 2022 data, live birth rates per cycle run near 49.7% under age 35, 36.3% at 35-37, 23.1% at 38-40, and 7.7% over 40 with your own eggs. Donor-egg transfers range from about 42% to 52%. Nearly 40% of transfers overall led to a live birth.
Disclaimer: This article is for general education and is not a substitute for professional medical advice. Fertility outcomes vary widely by individual, and only a licensed reproductive endocrinologist can assess your situation and recommend a treatment plan. Statistics reflect national averages and do not predict any individual result. Always follow the specific guidance of your fertility clinic.