

Most women have never been told what a normal period actually looks like in numbers. So when your flow soaks through a pad in an hour, or your cycle drags past a week, you assume it’s just how your body works. For millions of American women, that quiet assumption hides a treatable condition.
Table of Contents
Heavy menstrual bleeding isn’t something you have to live around. Once you know the real thresholds, the causes, and the options, you can stop guessing and start fixing it.
Quick answer: Heavy menstrual bleeding (menorrhagia) means losing more than 80 mL of blood per cycle, or bleeding in ways that disrupt your life: periods lasting more than 7 days, soaking through a pad or tampon every hour for several hours, passing clots larger than a quarter, or needing to double up on protection. It often causes iron-deficiency anemia. Effective treatments exist, from a hormonal IUD to non-hormonal pills to minor surgery.
At a glance:
- You likely have heavy bleeding if you soak a pad or tampon hourly, bleed past 7 days, or pass large clots.
- It affects about 1 in 5 American women, more than 10 million each year.
- Iron-deficiency anemia is the most common complication, causing fatigue and weakness.
- Causes range from fibroids and hormonal imbalance to bleeding disorders, mapped by the PALM-COEIN system.
- The levonorgestrel IUD is the most effective medical treatment, cutting blood loss by up to 95%.
- Bleeding after menopause, or flooding with dizziness, needs prompt medical care.
What Counts as Heavy Menstrual Bleeding?
The hardest part of this condition is recognizing it. Period flow varies so much between women that “heavy” feels subjective, but there are real, measurable lines you can use.
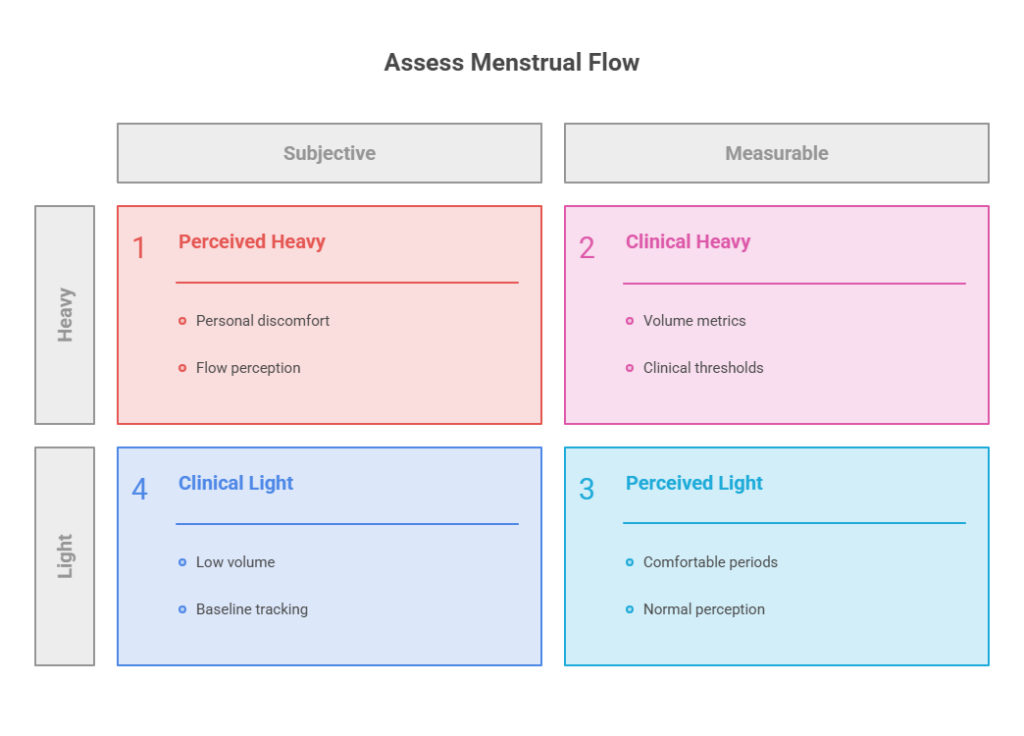
The Clinical Definition
Doctors define heavy menstrual bleeding as losing more than 80 mL (about 5 to 6 tablespoons) of blood in a single cycle, or bleeding that lasts longer than 7 days. For comparison, a typical period sheds only around 30 to 40 mL total.
In practice, almost no one measures milliliters. So the CDC and gynecologists rely on practical signs instead, which matter far more for everyday decisions.
The Real-World Signs You Can Measure
You may have heavy menstrual bleeding if you need to change a pad or tampon after less than 2 hours, or if your flow soaks through one or more every hour for several hours straight.
Other clear signals include doubling up on pads to control the flow, waking at night to change protection, and passing blood clots the size of a quarter or larger. Many women also find they plan their whole day around bathroom access during their heaviest days.
Our medical reviewers note that one signal stands out above the rest. If your period regularly interferes with work, sleep, or your social life, that alone meets the practical definition, no matter what the milliliter count would say.
Heavy menstrual bleeding is far more common than most people realize. According to the CDC, it affects more than 10 million American women each year, which works out to about 1 in every 5 women.
Why Heavy Periods Are Worth Taking Seriously
Heavy bleeding often gets brushed off as a nuisance, something to endure with extra tampons and a heating pad. The real concern is what steady blood loss does to the rest of your body over time.
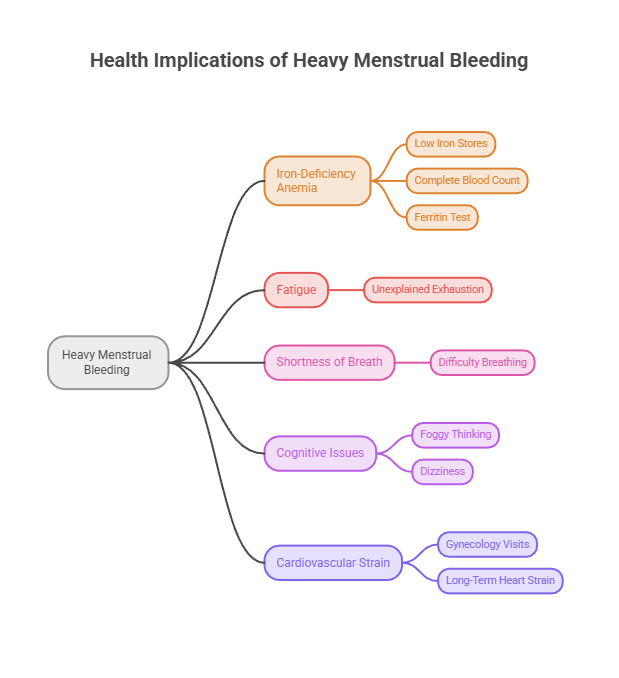
The main complication is iron-deficiency anemia. When you lose more blood than your body can rebuild, iron stores fall, and you’re left tired, weak, short of breath, and sometimes foggy or dizzy.
Patients booking blood work through HealthCareOnTime often discover their unexplained exhaustion traces straight back to heavy periods they had stopped noticing. A simple complete blood count paired with a ferritin test usually tells the story.
The ripple effects reach past fatigue. Heavy menstrual bleeding drives roughly one-third of all gynecology visits in the United States, and research has connected the resulting iron-deficiency anemia to added strain on the heart over the long run.
The Hidden Toll on Daily Life
Beyond the physical risks, heavy periods quietly shrink how women live. Many skip workouts, miss work or school, cancel plans, and avoid light-colored clothes or long trips during their heaviest days.
That monthly disruption adds up. Research measuring quality of life finds that heavy menstrual bleeding drags down work productivity, sleep, and emotional wellbeing in ways that rarely show up in a single doctor’s visit.
Yet many women wait years before raising it, partly because they assume nothing can be done and partly because periods still carry a stigma that keeps the conversation quiet. Naming the problem is the first step toward fixing it.
Heavy Menstrual Bleeding by the Numbers in America
| Statistic | Figure | Source |
| US women affected each year | More than 10 million | CDC |
| Share of US women with the condition | About 1 in 5 | CDC |
| Share of US gynecology visits | About one-third | NIH-indexed review |
| Clinical threshold for heavy loss | Over 80 mL per cycle | ACOG standard |
| Bleeding disorder among those evaluated | About 20% | Clinical reviews |
| Adolescent prevalence | About 37% | Systematic review |
Across the patients our network serves, the pattern holds. The women who feel worst are rarely the ones with a single dramatic episode; they’re the ones who have quietly bled heavily, month after month, for years without a benchmark to tell them it wasn’t normal.
What Causes Heavy Menstrual Bleeding?
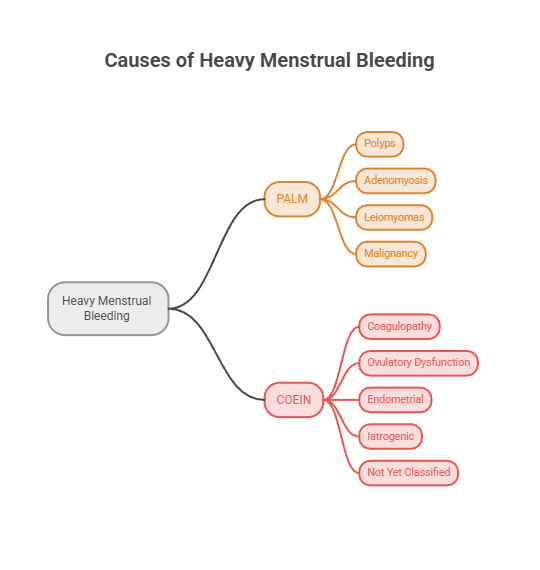
Before the list of causes feels overwhelming, here’s a simple way to think about it. Gynecologists use a framework called PALM-COEIN, created by the International Federation of Gynecology and Obstetrics, that sorts every cause into two buckets: structural problems you can often see on a scan (PALM), and non-structural ones you can’t (COEIN).
You don’t need to memorize it. The point is that your doctor is working through an organized checklist, not guessing.
Structural Causes (PALM)
These are physical changes in or on the uterus.
Polyps and Fibroids
Polyps are small, usually benign growths on the uterine lining. Fibroids (leiomyomas) are noncancerous muscular tumors in the uterine wall, and they rank among the most common causes of heavy bleeding, especially as women reach their 30s and 40s.
Fibroids enlarge the surface area of the uterine cavity and interfere with how the uterus squeezes down, and those two effects together push the flow higher.
Adenomyosis
In adenomyosis, tissue that normally lines the uterus grows into the muscular wall itself. The result is a tender, enlarged uterus, heavier periods, and often noticeably worse cramping.
It tends to be underdiagnosed, partly because its symptoms overlap with fibroids and it usually takes imaging to confirm. If your heavy periods come with deep, worsening pain, it’s worth raising.
Malignancy and Hyperplasia
This is the category nobody likes to talk about, but it’s important to name. Endometrial hyperplasia, an overgrowth of the uterine lining, can be precancerous.
According to ACOG, heavy menstrual bleeding can be an early sign of endometrial cancer. Most cases are found in women in their mid-60s who are past menopause, and the good news is that it’s often caught early, when treatment is most effective. That’s exactly why new or post-menopausal bleeding always deserves a look.
Non-Structural Causes (COEIN)
Here the uterus may look completely normal, yet something disrupts how it bleeds.
Coagulopathy
Bleeding disorders keep blood from clotting the way it should. Von Willebrand disease is the most common one. Although such disorders affect only 1 to 2% of the general population, they show up in roughly 20% of women evaluated specifically for heavy menstrual bleeding.
Our medical team has reviewed many cases where lifelong “heavy periods” turned out to be the first and only clue to an undiagnosed clotting disorder. A coagulation panel belongs in any thorough workup, particularly if you’ve bled heavily since your very first periods.
Ovulatory Dysfunction
When you don’t ovulate regularly, the balance between estrogen and progesterone tips, the uterine lining overgrows, and it eventually sheds heavily. This is common during puberty and perimenopause, when cycles are naturally erratic.
It also appears with polycystic ovary syndrome (PCOS) and thyroid problems, especially an underactive thyroid. That connection is why a thyroid (TSH) blood test often earns a spot in the evaluation.
Endometrial, Iatrogenic, and Unexplained
Some women have a problem with how the uterine lining itself manages bleeding. Others bleed more because of a medication or device, which doctors call iatrogenic causes: blood thinners, aspirin, the breast-cancer drug tamoxifen, or a copper IUD, particularly during its first year of use.
In a real share of cases, no specific cause turns up at all. Doctors label this idiopathic, and the reassuring part is that it can still be treated effectively, even without a named culprit.
Heavy Bleeding at Different Life Stages
Heavy menstrual bleeding can show up at any age, but the most likely causes shift across a woman’s life. Knowing the common pattern for your stage helps frame the conversation with your doctor and sets realistic expectations.
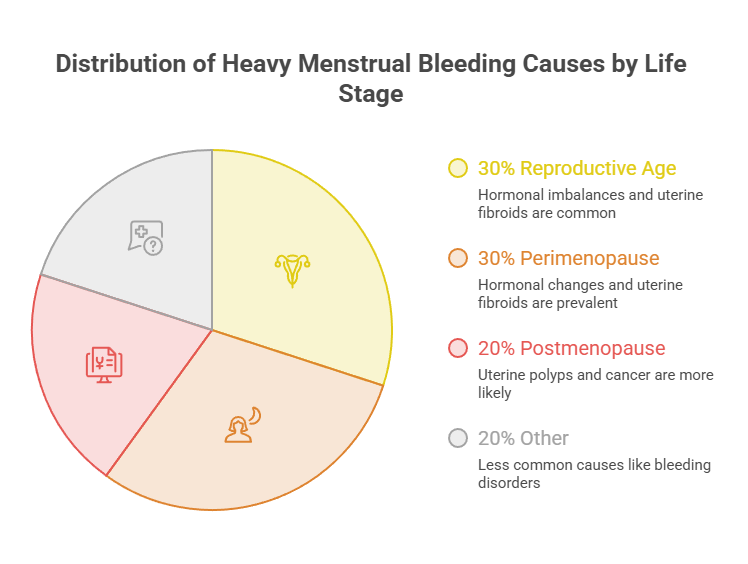
Teens and Early Periods
In the first few years after a girl’s first period, cycles are often irregular because ovulation hasn’t settled into a steady rhythm. That hormonal immaturity is the most common reason for heavy teen bleeding.
Even so, bleeding disorders like Von Willebrand disease appear more often in this group than many parents expect. Heavy periods that have been there from the very start, especially with easy bruising or frequent nosebleeds, deserve a proper evaluation rather than a wait-and-see approach.
The Reproductive Years
Through the 20s, 30s, and 40s, structural causes become more likely. Fibroids, polyps, and adenomyosis often emerge in this window, and pregnancy-related causes enter the picture too.
This is also the stage where treatment choices hinge most on future fertility plans, since some options preserve the ability to conceive while others do not. It’s worth being upfront with your doctor about whether children are part of your plans.
Perimenopause and Beyond
As menopause approaches, hormone levels swing and cycles can turn heavy and unpredictable again. Most of this is hormonal, but the risk of endometrial hyperplasia and cancer rises with age.
That’s why doctors are quicker to recommend an endometrial biopsy for heavy or irregular bleeding in this stage. It’s also why any bleeding after menopause is never treated as normal and always gets checked.
Symptoms and Warning Signs
Recognizing the symptoms helps you tell the difference between one heavy month and a pattern that needs attention.
Everyday Symptoms
The core symptom is the bleeding itself: soaking through protection quickly, passing clots, and lasting more than a week. Cramping often tags along, because the uterus has to work harder to push out clots and tissue.
Past the bleeding, watch for the quieter signs of low iron: ongoing tiredness, weakness, pale skin, frequent headaches, and feeling winded by ordinary activity. As Yale Medicine points out, anemia symptoms like fatigue and shortness of breath are part of the classic picture, and they’re easy to blame on a busy life instead.
Red-Flag Symptoms That Need Prompt Care
A handful of symptoms shouldn’t wait for a routine appointment. Sudden flooding that soaks through your clothes, bleeding with lightheadedness, a pounding heart, or fainting can all signal dangerous blood loss.
Any vaginal bleeding after menopause needs prompt evaluation to rule out serious causes. So does heavy bleeding during a known or possible pregnancy, which can point to a miscarriage or an ectopic pregnancy.
How Doctors Diagnose the Cause
A solid workup is methodical, and you can speed it along by showing up prepared.
It usually opens with your history. Your provider will ask about cycle length, how often you change protection, the size of any clots, your family’s bleeding history, and how the bleeding affects daily life. Tracking two or three cycles on a calendar or app beforehand makes this far more useful.
Next comes a pelvic exam and bloodwork. As Cleveland Clinic explains, blood tests typically screen for anemia, thyroid function, and clotting problems.
Patients commonly ask us which tests to expect. The usual panel includes a complete blood count, a ferritin level to gauge iron stores, a thyroid (TSH) test, and clotting studies when a bleeding disorder is on the table.
Imaging completes the structural picture. A pelvic ultrasound checks for fibroids, polyps, and adenomyosis. When the lining needs a closer look, your doctor may add a saline sonohysterogram, a hysteroscopy, or an endometrial biopsy to examine the tissue directly, especially for women over 45 or those with risk factors for cancer.
What to Bring to Your Appointment
A little preparation makes your visit far more productive. Bring a record of your last two or three cycles, including start and end dates, how often you changed protection, and the size of any clots.
Note any symptoms of anemia, such as fatigue or breathlessness, and write down your family history of heavy bleeding or clotting problems. List every medication and supplement you take, since blood thinners, aspirin, and some hormones can all affect bleeding. Clear, specific details help your provider reach the right diagnosis faster.
Treatment Options for Heavy Menstrual Bleeding
Here’s the encouraging part: heavy menstrual bleeding responds well to treatment. The right choice depends on the cause, your symptoms, your age, and whether you hope to get pregnant later. Care usually starts with the least invasive option that fits your situation.
Medical (Non-Surgical) Treatments
Most women begin here, and many never need anything more.
Hormonal Options
The levonorgestrel-releasing IUD (sold as Mirena and Liletta) is the most effective medical treatment available. It releases a small, steady dose of progestin right into the uterus, thinning the lining so it sheds much less.
Studies show it cuts menstrual blood loss by 71 to 95%, with treatment success around 85%. It also preserves fertility and is fully reversible, which is why clinical guidelines often list it first.
Combined hormonal contraceptives (the pill, patch, or ring) regulate the cycle and usually reduce blood loss by roughly 40 to 60%, while doubling as birth control. Cyclic or long-course oral progestins are another route, effective at lowering flow though they sometimes cause irregular spotting.
Non-Hormonal Options
Tranexamic acid (sold as Lysteda) is a non-hormonal pill you take only on your heaviest days. It helps blood clot normally and reduces menstrual blood loss by roughly 26 to 60%, often about half.
Our lab partners report that it’s a favorite for women who can’t or would rather not use hormones, including those actively trying to conceive. It isn’t appropriate if you have a history of blood clots.
NSAIDs like ibuprofen and naproxen, taken during your period, trim flow by about 20 to 40% and ease cramps at the same time. They’re inexpensive and sold over the counter. Iron supplements won’t slow the bleeding, but they treat or prevent the anemia that so often comes with it.
Treatment Options Compared by Effectiveness
| Treatment | Type | Blood-Loss Reduction | Best For / Key Notes |
| Levonorgestrel IUD (Mirena) | Hormonal device | 71 to 95% | Most effective medical option; preserves fertility, reversible |
| Tranexamic acid (Lysteda) | Non-hormonal pill | About 50% | Taken only on bleeding days; avoid with clot history |
| NSAIDs (ibuprofen, naproxen) | Non-hormonal, OTC | 20 to 40% | Also eases cramps; cheap; taken during the period |
| Combined pill, patch, or ring | Hormonal | 40 to 60% | Regulates cycle; also provides contraception |
| Endometrial ablation | Minor surgery | Up to ~90%, often stops periods | Only if childbearing is complete; not for future pregnancy |
| Hysterectomy | Definitive surgery | 100%, periods end | Permanent cure; ends fertility; reserved as a last resort |
Surgical Treatments
When medication isn’t enough, or a structural cause like large fibroids is driving the bleeding, several procedures can help.
Endometrial ablation destroys the uterine lining in a short outpatient procedure and frequently stops or sharply reduces bleeding, but it isn’t an option if you want a future pregnancy. Myomectomy removes fibroids while keeping the uterus intact, which can preserve fertility.
Uterine artery embolization shrinks fibroids by cutting off their blood supply. Hysterectomy, removal of the uterus, is the only guaranteed cure, but it permanently ends both fertility and periods, so it’s generally a last resort after other options have been weighed.
Choosing With Your Doctor
The best treatment isn’t the strongest one; it’s the one that fits your life. A woman hoping to have children soon will weigh the choices very differently from one approaching menopause.
In cases reviewed by our medical team, the plans that succeed start with honest conversations about fertility goals, how much the bleeding bothers you, and the underlying cause. Good counseling about what to expect, especially the first few months of spotting with an IUD, makes a real difference in whether women stick with a treatment long enough to see it work.
When to See a Doctor
Use this guide to match a symptom to the right next step. When you’re unsure, a quick call to your provider is always a reasonable move.
If You Have This Symptom, Do This
| Your Symptom | What It Might Mean | What to Do |
| Soaking a pad or tampon every hour for several hours | Excessive blood loss | Call your provider promptly; track the pattern |
| Periods lasting more than 7 days | Possible menorrhagia | Book a gynecology visit; ask about a blood count |
| Passing clots larger than a quarter | Heavy flow worth evaluating | Note the frequency; mention it at your appointment |
| Constant fatigue, pale skin, or shortness of breath | Possible iron-deficiency anemia | Ask for a CBC and ferritin test |
| Any bleeding after menopause | Needs cancer ruled out | See a doctor without delay |
| Sudden flooding with dizziness or fainting | Acute, dangerous blood loss | Seek urgent care; call 911 if severe |
Living With Heavy Periods: Practical Tips
While you sort out the cause and treatment, a few habits make heavy cycles more manageable day to day.
Track every cycle in an app, noting flow, clot size, and how often you change protection. That record speeds up diagnosis and shows clearly whether a treatment is working.
Stock up on higher-capacity products like overnight pads, menstrual cups, or period underwear for your heaviest days, and keep a spare kit at work or in your bag. Work iron-rich foods such as lean red meat, beans, lentils, and leafy greens into your meals, and pair them with vitamin C to help your body absorb the iron.
If heavy days affect your job, know that you’re not alone, and small adjustments help: a discreet supply kit in your bag, easy bathroom access, and dark clothing on your heaviest days. Some women find it worth a quiet word with a trusted manager so they can step away when needed.
Above all, don’t normalize it. Bleeding that controls your calendar is a medical issue with real solutions, not a personal weakness to push through in silence.
Frequently Asked Questions
What is considered heavy menstrual bleeding?
Heavy menstrual bleeding means losing more than 80 mL per cycle or bleeding that disrupts your life. Practical signs include periods lasting over 7 days, soaking a pad or tampon every hour for several hours, passing large clots, or doubling up on protection to manage the flow.
How many pads or tampons a day is too many?
There’s no single magic number, but soaking through one pad or tampon every hour for several hours in a row signals heavy bleeding. Needing to change protection every 2 hours or less all day, or doubling up to stay dry, also points to a flow worth discussing with your doctor.
Is it normal to pass large blood clots?
Small clots are common and usually normal. Passing clots larger than a quarter, especially regularly, suggests heavy menstrual bleeding. Clots form when blood pools faster than your body’s anticlotting factors can break it down, so frequent large clots are worth mentioning to your provider.
Can heavy periods cause anemia?
Yes. Iron-deficiency anemia is the most common complication of heavy menstrual bleeding. Losing more blood than your body replaces depletes iron stores, leaving you tired, weak, pale, and short of breath. A complete blood count and ferritin test confirm it, and treatment restores both your iron and your energy.
What is the most effective treatment for heavy periods?
The levonorgestrel IUD (Mirena) is the most effective medical treatment, reducing menstrual blood loss by 71 to 95%. It works locally in the uterus, preserves fertility, and is reversible. The best option for you depends on the cause, your symptoms, and your pregnancy plans, so decide together with your doctor.
Does the Mirena IUD stop heavy bleeding?
Often, yes. The Mirena IUD thins the uterine lining and can reduce bleeding by up to 95%, with many users having very light periods or none after several months. Expect some irregular spotting in the first 3 to 6 months, which usually settles as the treatment fully takes hold.
Does tranexamic acid stop period bleeding?
Tranexamic acid (Lysteda) reduces menstrual blood loss by roughly 26 to 60%, often around half. It’s a non-hormonal pill taken only on your heaviest days that helps your blood clot normally. It’s a strong choice if you prefer to avoid hormones, but not if you have a history of clotting.
When should I see a doctor about heavy bleeding?
See a doctor if you soak protection hourly, bleed longer than 7 days, pass large clots, or feel constantly tired and short of breath. Seek prompt care for any bleeding after menopause, and urgent care for sudden flooding paired with dizziness or fainting.
Can heavy menstrual bleeding be a sign of cancer?
It can be, though most cases have benign causes. Heavy or abnormal bleeding can be an early sign of endometrial cancer, usually in women past menopause. Because it’s often caught early when treatment works well, any new, unusual, or post-menopausal bleeding should be evaluated by a doctor.
What blood tests check for heavy menstrual bleeding causes?
A typical workup includes a complete blood count to check for anemia, a ferritin test to measure iron stores, a thyroid (TSH) test, and clotting studies when a bleeding disorder is suspected. These tests, paired with a pelvic ultrasound, help pinpoint both the cause and the impact on your body.
Do heavy periods always mean fibroids?
No. Fibroids are a common cause but far from the only one. Heavy bleeding can stem from polyps, adenomyosis, hormonal imbalances, thyroid problems, bleeding disorders, certain medications, or no identifiable cause at all. Imaging and bloodwork help your doctor find which factor actually applies to you.
Can heavy menstrual bleeding go away on its own?
Sometimes. Heavy bleeding tied to puberty, a short-term hormonal shift, or perimenopause may settle without treatment. But persistent heavy periods usually have an ongoing cause that won’t resolve alone. Since untreated bleeding can lead to anemia, it’s safer to get evaluated than to simply wait it out.
Disclaimer: This article is for general education and isn’t medical advice. It doesn’t replace diagnosis or treatment from a licensed clinician. If your bleeding is persistent, worsening, or affecting your health, talk to your doctor. For sudden, severe blood loss with dizziness, fainting, or a racing heart, seek emergency care or call 911.
References
- Centers for Disease Control and Prevention (CDC), About Heavy Menstrual Bleeding
- American College of Obstetricians and Gynecologists (ACOG), Heavy Menstrual Bleeding
- Cleveland Clinic, Menorrhagia (Heavy Menstrual Bleeding)
- Yale Medicine, Heavy Menstrual Bleeding (Menorrhagia)
- Mayo Clinic, Menorrhagia (Heavy Menstrual Bleeding)
- Medical Management of Heavy Menstrual Bleeding, NIH/PMC





