

Two hormones, names almost identical, separated by a single syllable. Yet one is built by your own ovaries, and the other is built in a factory.
Table of Contents
That small difference in spelling hides a big difference in behavior. Inside the uterus, progesterone and progestin do nearly the same job. Almost everywhere else in the body, they can part ways.
If you’ve ever taken birth control, weighed hormone therapy for menopause, or tried to make sense of a lab result, the distinction matters. Here’s how each one actually works, in plain English.
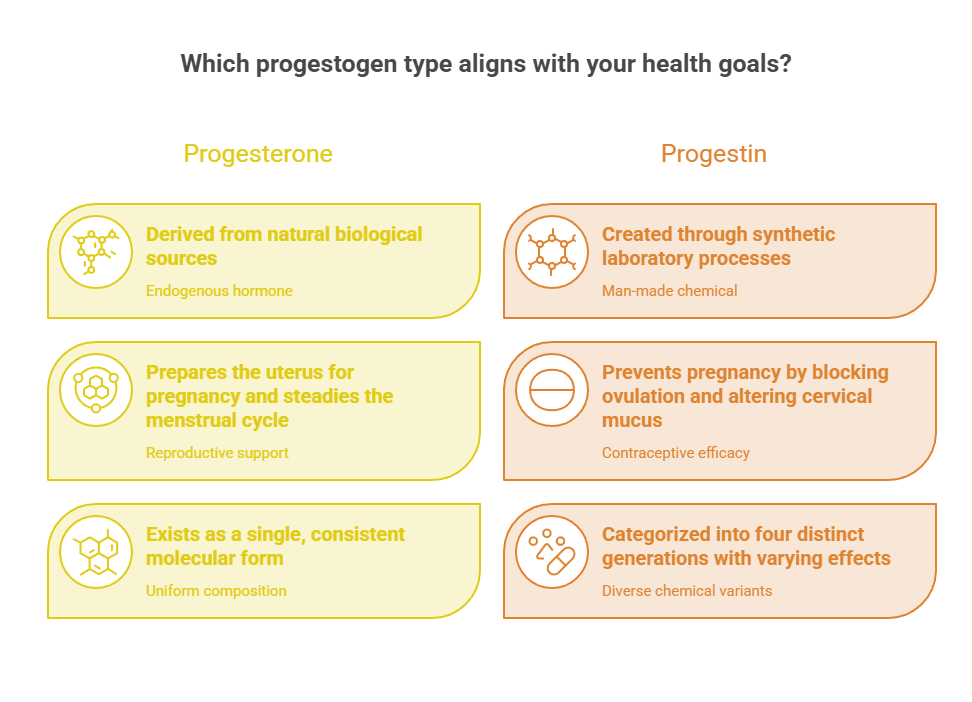
Quick Answer: Progesterone is a natural steroid hormone your body makes, mainly in the ovary after ovulation. Progestin is a synthetic, lab-made version designed to mimic it. Both belong to a family called progestogens, and both work by binding progesterone receptors inside your cells, which switch certain genes on or off. Because their chemical structures differ slightly, progestins can produce effects natural progesterone doesn’t, especially outside the uterus.
At a Glance
- Progesterone is natural; progestin is synthetic. Together they’re called progestogens.
- Both act on the same progesterone receptors to change how cells behave.
- Progesterone prepares the uterus for pregnancy and steadies the menstrual cycle.
- Progestins prevent pregnancy three ways: blocking ovulation, thickening cervical mucus, and thinning the uterine lining.
- There are four generations of progestins, each with slightly different effects.
- About 65% of US women aged 15 to 49 use contraception, and the pill is the second most common method.
What Are Progesterone and Progestin?
The confusion is understandable. The words rhyme, they’re often used loosely, and even some clinicians use them interchangeably in casual conversation.
They are not the same thing, though. Getting the definitions straight is the foundation for everything that follows, including which option might suit you.
Progesterone: The Natural Hormone
Progesterone is a steroid hormone your body produces on its own. The main source is the corpus luteum, the structure left behind on the ovary after an egg is released at ovulation.
Your adrenal glands make small amounts too, and during pregnancy the placenta becomes a major producer. While it’s known as a female reproductive hormone, male, female, and intersex bodies all make some progesterone.
Across patients we serve, this is the point that surprises people most. Progesterone isn’t a drug first; it’s a hormone your own biology runs on every single month. When you do not ovulate, you make very little of it, which is a clue we’ll return to later.
Progestin: The Lab-Made Version
Progestin is a synthetic chemical designed to mimic progesterone’s effects. Scientists initially produced progestins when they noticed the human body wasn’t absorbing oral progesterone well enough.
The chemical structures are close but not identical. That structure affects which hormone receptors progestins bind to and how they work, so each family causes slightly different side effects and treats different conditions.
Progestins come in many forms: pills, injections, gels, creams, patches, suppositories, IUDs, and implants. The type and dose depend entirely on why a person is taking it, which is why two prescriptions for a progestin can look nothing alike.
Progestogens: The Family Name
Here’s the word that ties it all together. Progesterone and progestins both belong to a class called progestogens (sometimes written progestagens).
Think of progestogen as the family surname. Both bioidentical (micronized) progesterone and synthetic progestins are progestogens; they act on the same progesterone receptors, but their chemical structures differ slightly, which means they can produce effects natural progesterone doesn’t.
Our medical reviewers note that this single framing clears up most of the confusion. Same family, different members, overlapping but not identical jobs.
How Progesterone Works in Your Body
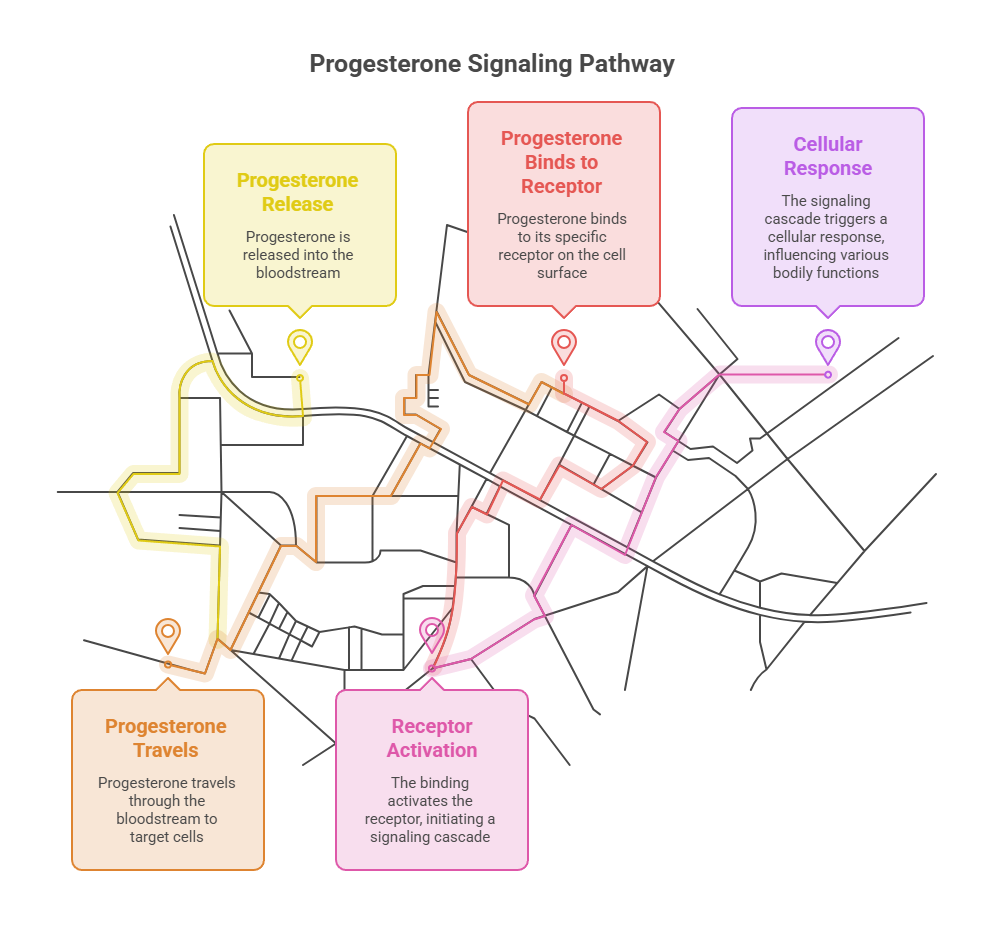
To answer the real question in the title, you have to zoom in to the level of the cell. Hormones are messengers, and progesterone delivers its message through a specific receptor.
Once you see that mechanism, the menstrual cycle, pregnancy, and even sleep effects all start to make sense as variations on one theme.
It Starts at the Progesterone Receptor
Progesterone works by binding to progesterone receptors inside your cells. These receptors are part of the nuclear receptor family and include progesterone receptor-A (PR-A) and progesterone receptor-B (PR-B), which come from the same gene but differ by their start sites.
These aren’t receptors sitting on the cell surface like a doorbell. They live inside the cell, waiting for the hormone to arrive and slip in. The PR-A and PR-B split matters because the two forms can pull a cell in slightly different directions, which is how one hormone produces different effects in different tissues.
Turning Genes On and Off
This is where the actual work happens. When progesterone binds, the receptors change shape, allowing the hormone-receptor complex to enter the cell nucleus, where it binds specific DNA sequences called progesterone response elements (PREs).
That binding acts like a dimmer switch on your genes. It modulates the transcription of target genes, turning them up or down, affecting processes like cell growth, differentiation, and programmed cell death.
In short, progesterone tells cells which instructions to read. Both receptor types function mainly as ligand-activated transcription factors, and the balance between PR-A and PR-B shapes the response in each tissue.
Its Job Across the Menstrual Cycle
The cycle is progesterone’s clearest stage. For the first half, estrogen builds up the uterine lining. After ovulation, progesterone takes over.
Once progesterone levels rise, they stimulate the endometrium to become more glandular and vascular, creating a welcoming environment for a possible embryo. This shift is called the secretory phase.
If fertilization doesn’t happen, progesterone levels drop, and the lining sheds as your period. Progesterone peaks in the mid-luteal phase and falls in the late luteal phase, when the corpus luteum breaks down roughly 9 to 11 days after ovulation.
Estrogen and progesterone also keep each other in check. Earlier in the cycle, estrogen increases the number of progesterone receptors, priming the lining to respond. Progesterone then tends to dial down estrogen’s activity in the uterus, a built-in balance that helps the cycle reset cleanly.
Its Role in Pregnancy
If a pregnancy begins, progesterone shifts from preparation to protection. Its job becomes keeping the uterus stable and quiet.
It’s primarily known as the pregnancy hormone, and most of its function relates to maintaining pregnancy by preparing the endometrium, decreasing uterine muscle contractions for implantation, supporting gestation, and holding off lactation until after birth.
During pregnancy, progesterone promotes relaxation of the uterine muscle and keeps the cervix closed; withdrawal of that signaling helps trigger labor. Patients booking tests through HealthCareOnTime often ask why progesterone is checked in early pregnancy, and this stabilizing role is exactly why.
Effects Beyond Reproduction
Progesterone doesn’t stop at the uterus. It also acts on the brain as a neurosteroid, which explains some of its mood and sleep effects.
It can modulate neurotransmitter systems including gamma-aminobutyric acid (GABA), which has calming effects on the brain. This GABA activity is part of why some people feel more relaxed or sleep better when progesterone is higher.
It plays a role in bone and other tissues too. Reviews of progesterone physiology describe its actions on the endometrium, uterus, mammary gland, and cardiovascular system. Worth knowing: progesterone is the first sex hormone to decline in perimenopause, often starting in a person’s mid-to-late 30s, which is why sleep and mood can shift years before periods stop.
How Progestin Works (and Why It’s Different)
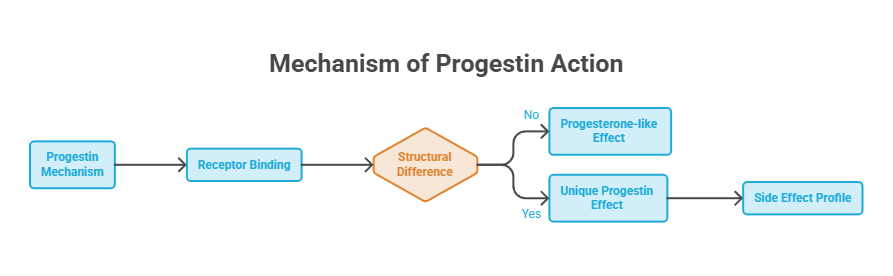
Progestins borrow progesterone’s mechanism, then add their own twists. They reach the same receptor, but the slightly different shape changes the outcome in places progesterone wouldn’t touch.
This is the part most articles skip, and it’s where the practical differences in side effects come from.
Same Receptor, Slightly Different Key
Picture progesterone as a key cut to fit your receptors perfectly. A progestin is a copied key: it opens the same lock, but the slightly different shape can rattle other locks too.
Most progestins are derived from other hormones, namely progesterone or testosterone, so they share a similar structure and can sometimes have unintended effects on those systems. A progestin built from a testosterone-like backbone, for example, can act a little androgenic.
That’s the heart of the difference. The uterine effect stays similar, while the off-target effects vary by molecule. It also explains a striking observation clinicians make: progestins and progesterone can have the same thinning effect on the uterine lining yet act quite differently in the breasts and brain.
Three Ways Progestins Prevent Pregnancy
When progestins are used for birth control, they block conception through several overlapping actions. They don’t rely on just one, which is part of why they’re so effective.
First, they suppress ovulation, so no egg is released. Second, they thicken cervical mucus, which makes it harder for sperm to get through. Levonorgestrel, a common progestin, works primarily by preventing ovulation and closing off the cervix to the passage of sperm.
Third, they thin and alter the uterine lining, making implantation less likely. Norethindrone, another widely used progestin, thickens cervical mucus, suppresses ovulation, lowers the mid-cycle hormone peaks, and changes endometrial thickness.
Why Some Progestins Act Differently
Not all progestins behave alike, and the differences are practical. Each progestin has slight variations in its estrogenic, androgenic, or progestational activity.
Levonorgestrel and norgestrel carry high androgenic activity and are more prone to cause acne, unwanted hair growth, weight gain, and fatigue than progestins with less androgenic activity. Drospirenone sits at the other end. It’s structurally similar to spironolactone and has a mild potassium-sparing, water-releasing effect, so it may suit people who notice fluid retention.
In cases reviewed by our medical team, this variation is why two people can have completely different experiences on what looks like the same kind of pill.
| Feature | Progesterone (natural) | Progestin (synthetic) | Why It Matters |
| Source | Made by your body (ovary, adrenals, placenta) | Made in a lab | One is a hormone, the other a medication |
| Chemical structure | The body’s own molecule | Close mimic, slightly different | Drives the off-target effects |
| Receptor | Binds progesterone receptors | Binds the same receptors | Explains the shared uterine effect |
| Effect on uterine lining | Thins and matures it | Thins and alters it | Both protect or reset the lining |
| Effects elsewhere | Generally calming, neutral | Can be androgenic or anti-fluid | Side effects vary by molecule |
| Common forms | Micronized capsules, gel, cream | Pills, IUDs, implants, shots, patches | Wider delivery options for progestins |
The Many Types of Progestins
Progestin isn’t one drug. It’s a category holding dozens of molecules, usually grouped into generations based on when they were developed and how they behave.
Knowing the generation gives you a quick read on likely effects, which is handy when comparing birth control options with a provider.
Progestin Generations Explained
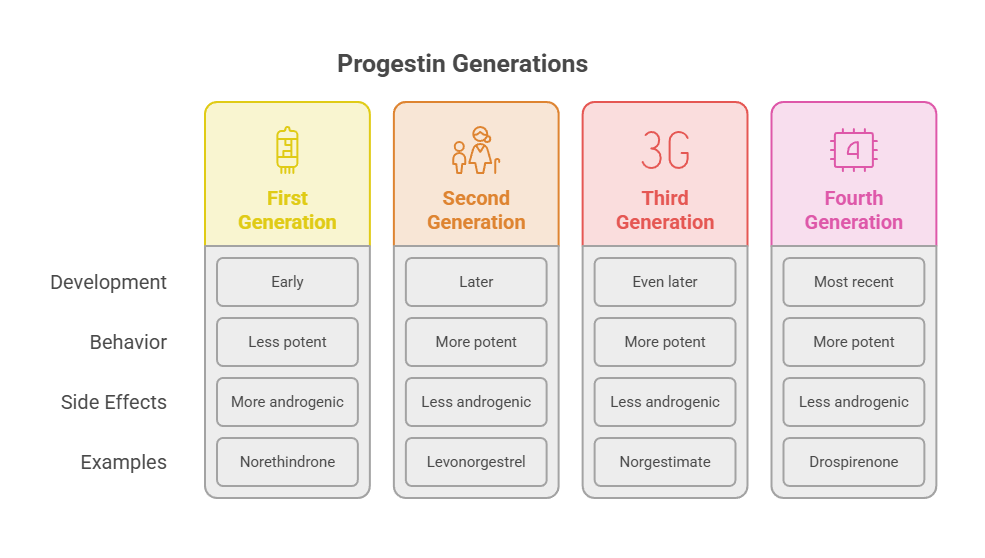
Researchers typically sort progestins into four generations. Each newer wave aimed to keep the contraceptive benefit while trimming certain side effects.
The grouping isn’t a ranking of best to worst. It’s more a family tree, and the right choice depends on the individual, not the generation number. A second-generation progestin can be the perfect fit for one person and a poor one for another.
The story stretches back decades. Levonorgestrel, still one of the most-used progestins, was patented in 1960 and brought into medical use in 1970. Each later generation reflected an effort to fine-tune how the molecule behaves once it reaches the receptor.
First and Second Generation
The earliest progestins are still in heavy use. First-generation progestins (the estrane family) include norethindrone, norethynodrel, norethindrone acetate, and ethynodiol diacetate.
Second-generation progestins (gonanes) include levonorgestrel and norgestrel. These tend to be more androgenic, which is why they’re linked more often to acne and similar effects, but they’re well-studied and reliable. Levonorgestrel and norgestrel are the ones most prone to acne, hair growth, and weight gain among the group.
Third and Fourth Generation
Newer progestins were engineered to soften androgenic effects. Third-generation progestins include desogestrel, gestodene, and norgestimate, while fourth-generation options include dienogest, drospirenone, and nomegestrol acetate.
Drospirenone is the unusual one. It isn’t derived from progesterone or testosterone like most others, which gives it a different side-effect profile. That heritage is why it behaves more like a water pill than its cousins.
| Generation | Example Progestins | Known For | Found In |
| First | Norethindrone, ethynodiol diacetate | Long track record, mild | Many combined and mini-pills |
| Second | Levonorgestrel, norgestrel | More androgenic, well-studied | Mirena IUD, many pills, Opill |
| Third | Desogestrel, norgestimate, gestodene | Less androgenic | Various combination pills |
| Fourth | Drospirenone, dienogest | Anti-fluid or anti-acne traits | Yaz, Yasmin, others |
Where You’ll Find Them: Common Uses
Progestogens show up across a person’s life, from the teenage years to well past menopause. The same receptor mechanism gets aimed at very different goals.
Understanding the use helps explain why a doctor might pick progesterone in one situation and a specific progestin in another.
Birth Control
This is the most familiar use. Three types of oral contraceptive pills are broadly prescribed: combined estrogen-progesterone, progestin-only, and continuous or extended-use pills.
Progestins also power long-acting methods. Levonorgestrel is the active ingredient in IUDs like Mirena and Skyla, and in birth control implants. Other progestin-only options include the etonogestrel implant and the depot medroxyprogesterone acetate (DMPA) injection, given as 150 mg into muscle or 104 mg under the skin.
The mini-pill is progestin-only. Three progestin-only pill formulations are currently available in the United States: norethindrone, norgestrel, and drospirenone. These rely more heavily on progestin’s direct effects on mucus and lining than on shutting down ovulation every cycle.
Emergency Contraception
Levonorgestrel also appears in the morning-after pill, a higher single dose used after unprotected sex. It works mainly by delaying or preventing ovulation, not by ending an established pregnancy. Available over the counter in the US, it’s most effective the sooner it’s taken.
Menopause and Hormone Therapy
During menopause hormone therapy, a progestogen rarely works alone. It’s usually paired with estrogen for a specific safety reason.
Menopause hormone therapy often combines estrogen with a progestogen to protect the uterine lining, since estrogen alone can overstimulate it. Without that protection, the lining can build up dangerously.
For this reason, progestogens are included in menopausal hormone therapy for people with a uterus, to guard against the cancerous overgrowth that unopposed estrogen can cause. Many providers favor micronized (bioidentical) progesterone here, which tends to be well tolerated. People who’ve had a hysterectomy often skip the progestogen, since the lining it protects is no longer there.
Periods, PCOS, and Other Conditions
Beyond contraception and menopause, progestins treat a range of gynecologic issues. They’re a common tool when cycles go off track.
Common uses include treating irregular menstrual periods, including absent periods (amenorrhea) and abnormal bleeding. They also feature in the management of endometriosis and other conditions driven by the uterine lining. Patients commonly ask us whether a hormone prescribed for heavy periods is the same as the one in their friend’s birth control, and often it is the same progestin at a different dose.
For endometriosis specifically, both the levonorgestrel IUD and the medroxyprogesterone injection have been studied as longer-term options to calm the lining and ease pain. The same progestin that prevents pregnancy can do double duty managing a chronic condition.
| Statistic | Figure | Source |
| US women aged 15-49 using contraception | About 65% | CDC / NCHS |
| Women using the pill as their method | 12.6% (2nd most common) | CDC |
| Pregnancies per 100 progestin-only pill users (typical use) | About 7 | CDC |
| Women who use contraception at some point in life | About 99% | CDC |
| Levonorgestrel released by Mirena IUD daily | 20 mcg | US Pharmacist |
| First OTC daily birth control pill (Opill, norgestrel) | FDA-approved July 2023 | FDA |
The numbers show how widespread these molecules are. In 2015 to 2017, about 65% of the 72.2 million US women aged 15 to 49 were currently using contraception, with the pill among the most common methods. In July 2023, the FDA approved the first nonprescription daily oral contraceptive, Opill (norgestrel), which reached stores in early 2024.
Natural Progesterone or Synthetic Progestin: How to Think About It
People often want to know which is better. The honest answer is that it depends on the goal, your health history, and how your body responds.
This is a conversation for you and your provider, not a one-size verdict. Still, a few patterns help frame it.
When Bioidentical Progesterone Fits
Natural, body-identical progesterone has a specific appeal. Micronized progesterone is made so it has a molecular structure identical to the progesterone your body produces.
In menopause hormone therapy, micronized progesterone is generally well tolerated. Products such as Prometrium and Crinone are FDA-approved forms. People sensitive to the side effects of synthetic progestins sometimes do better here, and the calming, sleep-friendly profile can be a bonus at night.
When a Progestin Is the Better Choice
Progestins earn their place through versatility and strength. For preventing pregnancy, they’re highly effective and come in convenient long-acting forms a daily capsule of progesterone can’t match.
They also let a provider target a specific trait, such as choosing an anti-androgenic option for someone with acne. Some people tolerate progesterone better, while others do better on a progestin; it’s very individualized, and decisions should be made with a women’s health provider.
| If You… | Option to Discuss | Why |
| Want reliable, low-effort birth control | A progestin IUD, implant, or pill | Highly effective, long-acting forms |
| Are in menopause and have a uterus | Estrogen plus a progestogen | Protects the uterine lining |
| React badly to synthetic progestins | Micronized (bioidentical) progesterone | Body-identical, often better tolerated |
| Struggle with acne or oily skin | A less androgenic or anti-androgenic progestin | Gentler on skin and hair |
| Notice cyclical fluid retention | A drospirenone-based option | Mild anti-fluid effect |
| Are breastfeeding | A progestin-only (mini) pill | Estrogen-free option |
Side Effects, Risks, and What to Watch
No hormone medication is free of trade-offs. The good news is that side effects are well documented, and many fade as the body adjusts.
Knowing what’s typical, and what isn’t, helps you have a productive talk with your provider rather than a worried one.
Common Side Effects
Both natural progesterone and progestins can cause side effects, and the likelihood varies by person and product. Mood changes, bloating, breast tenderness, and spotting are among the more common reports.
Reactions to natural progesterone differ widely. Some people feel calmer on progesterone, while others get PMS-like symptoms such as bloating or feeling down. The androgenic progestins, as noted, lean more toward acne and similar effects.
Irregular bleeding or spotting is one of the most common early complaints, especially with progestin-only methods, and it often settles within the first few months. Tracking the pattern helps your provider tell a normal adjustment from something worth a closer look.
When to Talk to a Doctor
Most side effects are manageable, but some signs deserve prompt attention. Severe leg pain, chest pain, trouble breathing, sudden severe headaches, or vision changes are reasons to seek care quickly, since hormone therapy can affect clotting risk in some people.
Our medical reviewers note that your full history matters here. It’s important to discuss your complete health history, including allergies and current medications, because certain drugs can interact with progestins. One small but real example: Prometrium is made in a peanut oil base, which means people with peanut allergies can’t take it.
How to Check Your Progesterone Levels
If you’re tracking fertility, investigating irregular cycles, or simply curious about your hormone balance, a progesterone test is straightforward. Here’s how to approach it.
- Talk with your provider about why you want the test, since timing and interpretation depend on your goal.
- For cycle-related testing, schedule the blood draw for the mid-luteal phase, often around 7 days after suspected ovulation, when progesterone peaks.
- Note your cycle day, current medications, and any hormone products you use, so results can be read in context.
- Get the simple blood test done; progesterone is measured from a standard blood sample.
- Review the results with your provider rather than self-interpreting, since normal varies by cycle phase, pregnancy status, and age.
What the number means depends on context. A low mid-luteal progesterone reading may suggest ovulation didn’t occur that cycle, while levels are expected to run high in pregnancy. That’s why the same result can be reassuring in one situation and worth following up in another.
In cases seen across our diagnostic network, a single progesterone reading is most useful when paired with the right timing and a few related hormones. A number on its own rarely tells the whole story, which is why context and a professional read matter so much.
Frequently Asked Questions
Is progestin the same as progesterone?
No. Progesterone is a natural hormone your body makes, while progestin is a synthetic version made in a lab to mimic it. Both belong to the progestogen family and act on the same receptors, but their slightly different structures mean progestins can cause effects natural progesterone doesn’t.
How does progesterone work in the body?
Progesterone binds receptors inside your cells (PR-A and PR-B), then enters the nucleus and attaches to specific DNA sites. This switches certain genes up or down, which changes how cells behave. That single mechanism drives its effects on the uterus, pregnancy, and even brain chemistry.
How do progestins prevent pregnancy?
Progestins work three ways at once. They suppress ovulation so no egg is released, thicken cervical mucus to block sperm, and thin or alter the uterine lining to discourage implantation. Different progestins lean on these actions to different degrees, but the combined effect is highly reliable contraception.
Is natural progesterone safer than progestin?
Not automatically. Micronized progesterone is body-identical and often well tolerated, especially in menopause therapy. But progestins are highly effective and come in convenient forms. Safety depends on your health history, the specific product, and how your body responds, so the right choice is individual and provider-guided.
What are the generations of progestins?
Progestins are sorted into four generations. First includes norethindrone, second includes levonorgestrel and norgestrel, third includes desogestrel and norgestimate, and fourth includes drospirenone and dienogest. Newer generations were designed to reduce androgenic side effects like acne, though the best fit varies by person.
Why do I need progesterone with estrogen in HRT?
If you have a uterus, taking estrogen alone can overstimulate the uterine lining and raise the risk of overgrowth and cancer. Adding a progestogen protects that lining. People without a uterus often take estrogen alone, since this protective role is no longer needed.
Does progesterone help you sleep?
It can for some people. Progesterone acts on the brain as a neurosteroid and boosts GABA activity, which has a calming effect. This is part of why some feel more relaxed or sleep better when progesterone is higher, such as in the second half of the menstrual cycle.
What is micronized or bioidentical progesterone?
Micronized progesterone is processed into tiny particles so the body absorbs it better, and it has a molecular structure identical to your own progesterone. FDA-approved forms include Prometrium and Crinone. It’s commonly used in menopause hormone therapy and is often described as bioidentical or body-identical.
Can progestins cause weight gain?
Some can, particularly more androgenic ones like levonorgestrel, which are linked to weight gain and fluid changes in certain people. Others, like drospirenone, have a mild anti-fluid effect. Responses vary widely, so weight changes on one progestin don’t predict your response to another.
What’s the difference between the mini-pill and the combined pill?
The combined pill contains both estrogen and a progestin. The mini-pill is progestin-only, with no estrogen, which makes it a common choice during breastfeeding or for people who should avoid estrogen. Both prevent pregnancy, but the mini-pill relies more heavily on progestin’s direct actions.
When does progesterone rise in the menstrual cycle?
Progesterone rises after ovulation, during the luteal phase, when the corpus luteum forms. It peaks in the mid-luteal phase, roughly a week after ovulation. If pregnancy doesn’t occur, levels fall in the late luteal phase, which triggers your period to begin.
Is Opill a progestin?
Yes. Opill contains norgestrel, a progestin, and no estrogen, making it a progestin-only pill. The FDA approved it in July 2023 as the first nonprescription daily oral contraceptive in the United States, and it became available over the counter in early 2024.
Medical Disclaimer: This article is for general informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Hormone decisions, including birth control and menopause therapy, should be made with a qualified healthcare provider who knows your full history. Never start, stop, or change a medication based on this article alone.





