

As a board-certified gastroenterologist and hepatologist with over 15 years of clinical experience, I see patients every week who come in terrified by sudden stomach swelling. The question they always ask is the same: what causes fluid in the abdomen, and how do I make it stop?
Table of Contents
It is a valid concern. Unexplained abdominal swelling is not something to brush off. It could signal a serious underlying problem that needs attention right away.
In this article, I will walk you through the medical reasons behind this condition, the warning signs you should never ignore, the diagnostic tests we use, and the treatments available today. Whether you are a patient, a caregiver, or just someone trying to understand what is happening inside your body, this guide will give you the clarity you need.
Quick Answer: What Is Ascites?
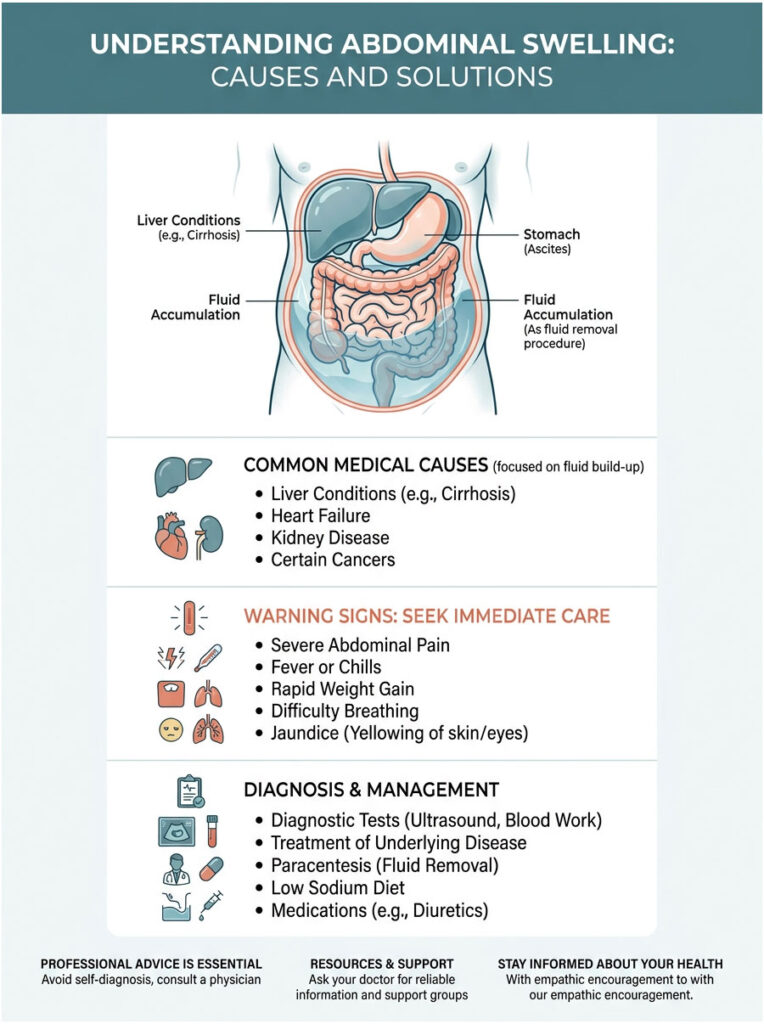
Ascites is the medical term for an abnormal buildup of fluid inside the peritoneal cavity, the space between the lining of your abdomen and your internal organs. In most cases, it is driven by portal hypertension and advanced liver cirrhosis. It always requires prompt medical evaluation to identify the root cause and prevent dangerous complications like infection or kidney failure.
Key Statistics on Abdominal Fluid Buildup
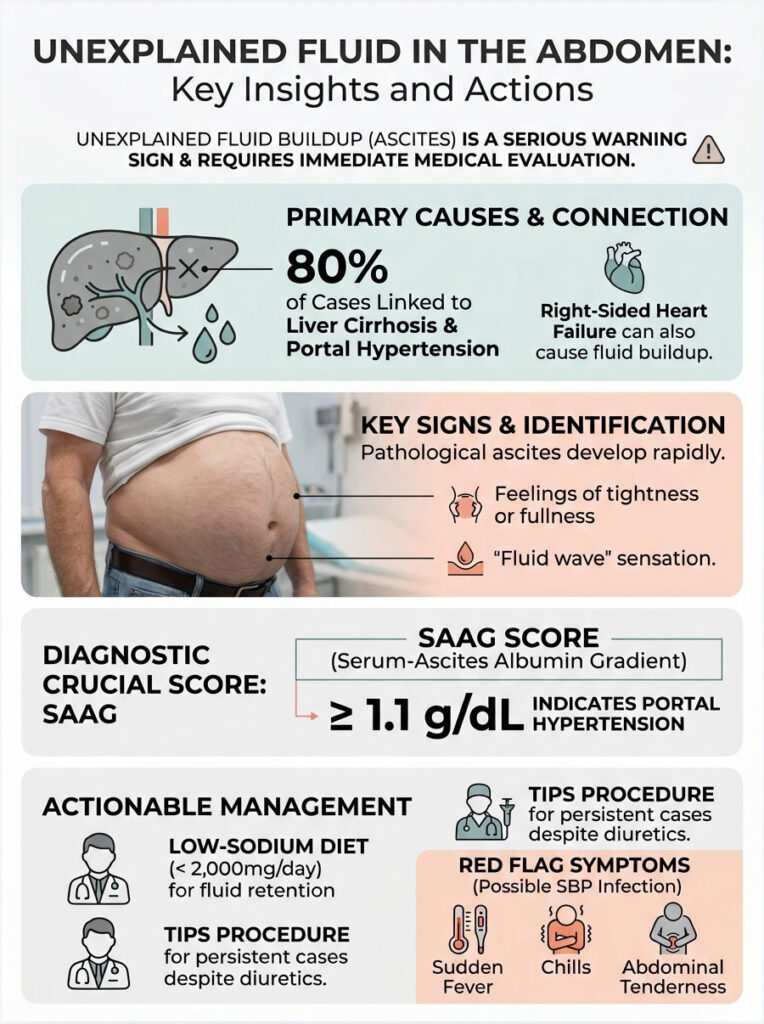
- About 80% of all cases are caused by advanced liver cirrhosis (American Association for the Study of Liver Diseases).
- Roughly 10% of cases are linked to malignant tumors or metastatic cancers.
- Around 3% of cases stem from severe right-sided congestive heart failure.
- Patients with cirrhosis who develop ascites face a 50% mortality rate within two years without a transplant.
- A daily sodium intake below 2,000 mg is required as a baseline management strategy.
- Diagnostic paracentesis carries a complication rate under 1%, making it both safe and reliable.
What Causes Fluid in the Abdomen: The Core Pathophysiology
To understand what causes fluid in the abdomen, you first need a basic picture of what is happening inside your body. The peritoneal cavity is a hollow space between the tissue layers that line your belly and wrap around your internal organs.
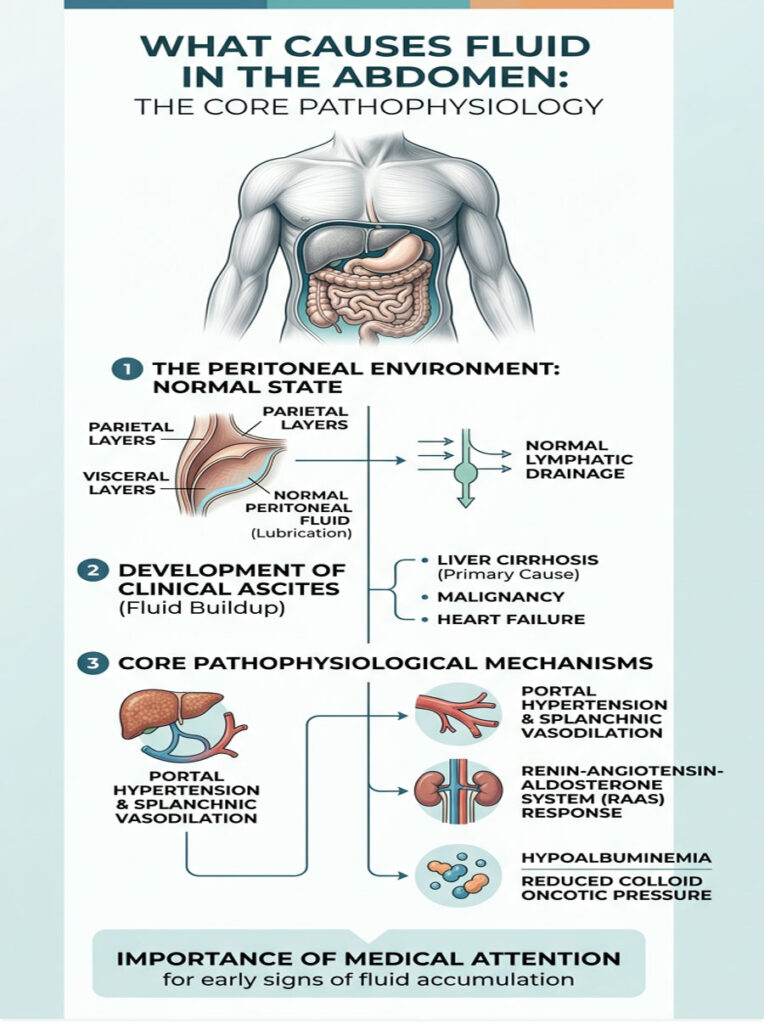
In a healthy person, this space holds only a few tablespoons of clear liquid. That small amount works as a lubricant, helping your intestines glide smoothly during digestion. But when something goes wrong with a major organ system, fluid production spirals out of control. In severe cases, dozens of liters can accumulate.
The Anatomy of the Peritoneal Cavity
The peritoneum is a two-layered membrane. The outer layer lines the abdominal wall, while the inner layer wraps around the stomach and intestines. Between these layers sits a potential space where fluid can collect.
Normally, your lymphatic system works like a sump pump, steadily draining away any excess moisture. But when that drainage system gets overwhelmed, or when pressure inside the blood vessels forces fluid out faster than it can be removed, the cavity floods. That flooding is what we call clinical ascites.
Splanchnic Vasodilation and the RAAS System
The process usually starts with abnormal changes in blood flow. In patients with severe liver disease, the blood vessels in the digestive tract widen far more than they should. This causes systemic blood pressure to drop, and the body misreads the drop as severe dehydration.
In response, the kidneys activate the Renin-Angiotensin-Aldosterone System (RAAS). They release hormones that force the body to hold onto large amounts of sodium. Because the liver is heavily scarred, the extra retained water cannot flow through normally. Instead, it seeps directly into the belly.
Hypoalbuminemia and the Loss of Oncotic Pressure
A second major mechanism involves a protein called albumin. A healthy liver constantly produces albumin, which circulates in your bloodstream and acts like a molecular sponge, keeping water locked inside your blood vessels.
When the liver fails, albumin production drops sharply. This creates a condition called hypoalbuminemia. Without enough albumin, blood loses its ability to hold water. The fluid leaks through vessel walls and pools in the lowest point of gravity, typically the belly.
Expert Insight
In my clinic, patients often mistake early fluid accumulation for stubborn belly fat. If your stomach feels tight like a drum and your belly button starts pushing outward, get a medical ultrasound right away. Do not wait for it to resolve on its own.
Primary Hepatic Drivers: Liver Disease and Portal Hypertension
Abdominal swelling is never a standalone disease. It is always a symptom of something larger going wrong inside the body. Hepatic causes, meaning those related to the liver, account for the vast majority of cases.
Cirrhosis and Scar Tissue Formation
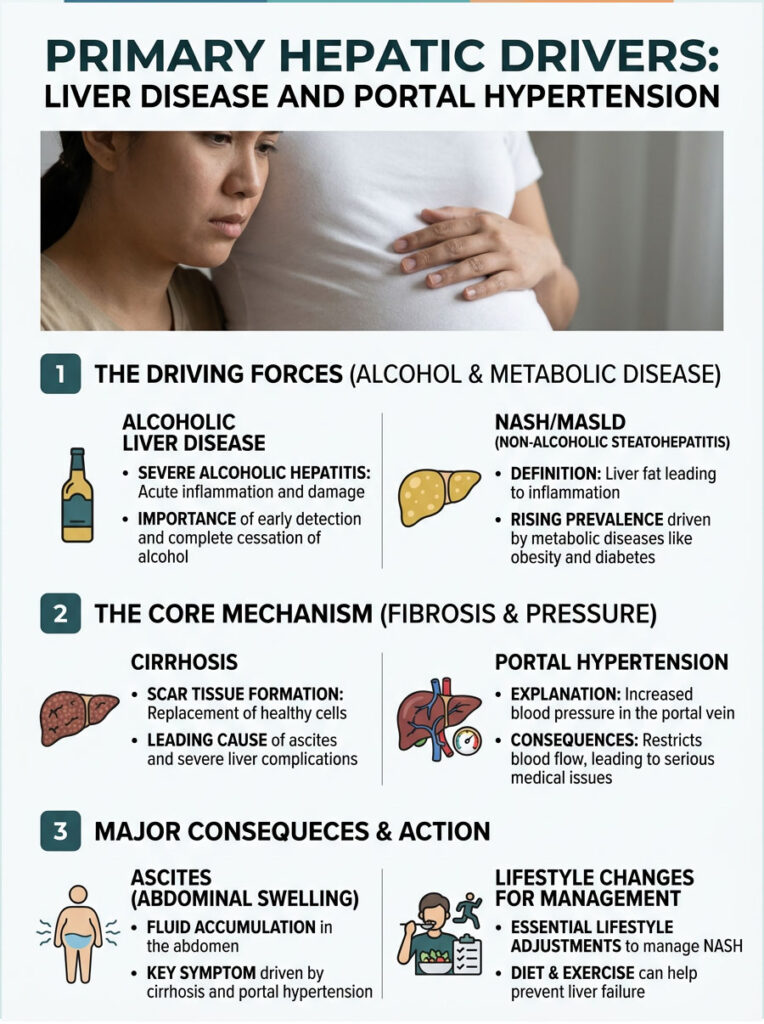
Liver cirrhosis is the most common cause of ascites worldwide. When the liver sustains repeated damage from alcohol, viruses, or fatty deposits, it tries to heal itself. That healing process produces dense, inflexible scar tissue.
This scarring leads to portal hypertension. The portal vein, which carries nutrient-rich blood from your digestive organs to the liver, becomes blocked by scar tissue. Blood cannot flow through easily, so pressure inside the vein spikes. That high pressure forces clear plasma to seep out of the liver’s surface and into the surrounding cavity.
Severe Alcoholic Hepatitis
Severe alcoholic hepatitis is an acute, life-threatening condition caused by heavy, prolonged drinking. It triggers massive inflammation inside the liver, leading to rapid fluid accumulation, sometimes liters within days.
Unlike chronic cirrhosis, alcoholic hepatitis can sometimes be partially reversed if caught early. But the patient must stop drinking entirely. Even a single drink can trigger a fatal chain of organ failure.
Non-Alcoholic Steatohepatitis (NASH/MASLD)
We are seeing a sharp rise in cases driven by metabolic disease. Non-Alcoholic Steatohepatitis, recently renamed MASLD, is quickly becoming a leading cause of liver failure. It is driven by obesity, diabetes, and poor diet.
Excess fat infiltrates the liver cells and causes chronic, silent inflammation. Over decades, it produces the same scarring as heavy alcohol use. Many patients are genuinely shocked to learn they have end-stage liver disease without ever having been heavy drinkers.
Managing NASH requires aggressive lifestyle changes: weight loss, blood sugar control, and cholesterol management. Without intervention, it inevitably leads to portal hypertension and severe swelling.
Cardiac and Malignant Triggers: When the Liver Is Not to Blame
Not every case of abdominal fluid points to the liver. Your internal organs are connected through a complex vascular system. When the heart fails, the liver suffers the consequences almost immediately. And aggressive cancers can trigger massive internal swelling on their own.
Right-Sided Congestive Heart Failure
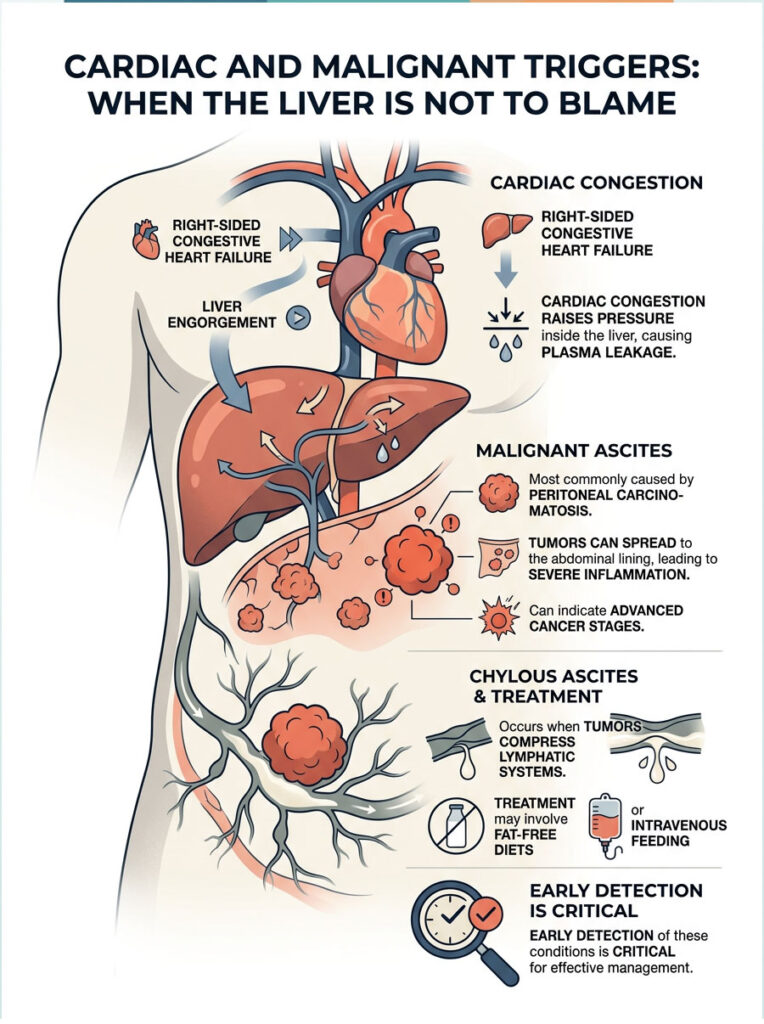
The right side of your heart pumps returning venous blood into the lungs. If that muscle weakens, it can no longer pump efficiently, and blood begins to back up through the venous system. That backup travels down the inferior vena cava and into the hepatic veins, engorging the liver with trapped blood.
This cardiac congestion raises pressure inside the liver, mimicking portal hypertension. The result is the same: plasma leaks from the engorged liver and fills the surrounding space.
Peritoneal Carcinomatosis and Cancer Seeding
When tumors cause this type of fluid buildup, we call it malignant ascites. The most common cause is peritoneal carcinomatosis, which happens when cancers of the ovary, pancreas, or colon spread to the abdominal lining.
Microscopic tumor cells seed themselves along the delicate peritoneal membrane, causing severe inflammation. The body responds by producing large amounts of inflammatory fluid. Tragically, malignant ascites is often the very first sign that leads to a stage-four cancer diagnosis.
Lymphatic Obstruction and Chylous Ascites
Growing tumors can also physically crush the lymphatic system. If a large tumor compresses a major lymphatic trunk, fluid has nowhere to drain. This can lead to a rare condition called chylous ascites, where the fluid appears milky white because it is packed with undigested fats.
Treatment involves placing patients on strict fat-free diets or intravenous feeding while oncologists target the obstructing tumor.
Renal Failure and Rare Systemic Infections
The kidneys are the ultimate regulators of your body’s water and electrolyte balance. When they sustain severe damage, systemic swelling follows quickly. Infections, while rare in developed countries, can also mimic organ failure.
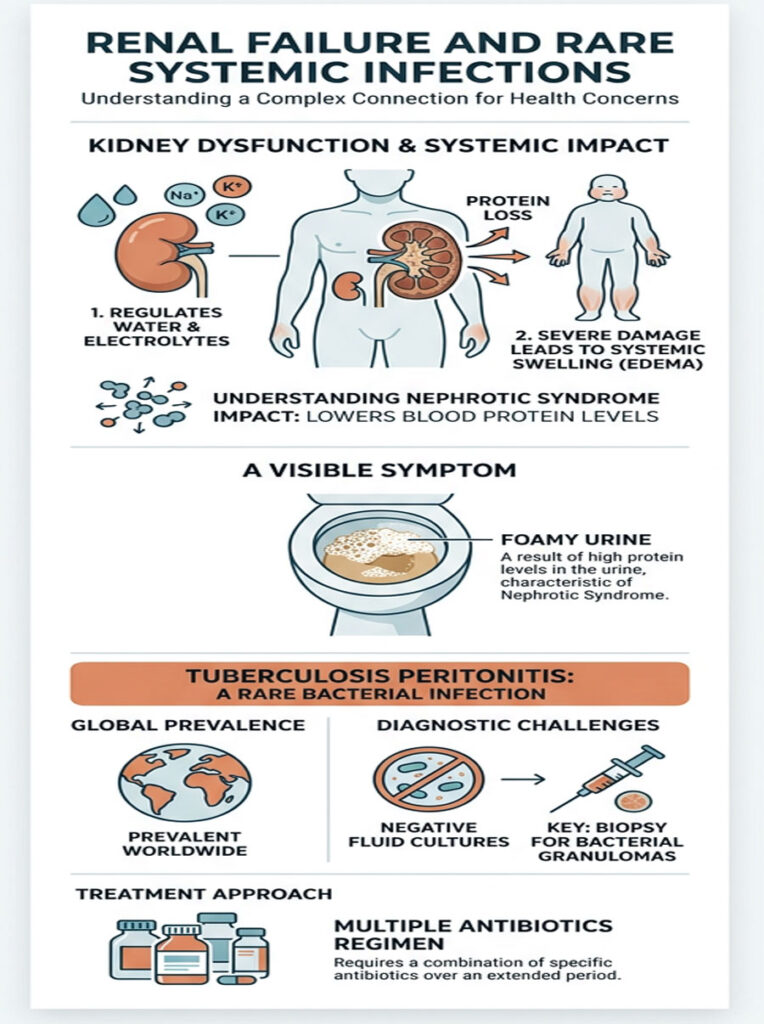
Nephrotic Syndrome and Protein Loss
Nephrotic syndrome damages the kidney’s filtering units, causing them to spill large amounts of protein into the urine. This rapidly depletes blood protein levels. Just like in advanced liver failure, the loss of protein destroys your oncotic pressure, and fluid leaks into soft tissues and the belly.
Patients with this condition often notice their urine looks foamy. Catching it early can save the kidneys from permanent, irreversible damage.
Tuberculosis Peritonitis
While rare in the United States, tuberculosis peritonitis still occurs frequently worldwide. TB can infect the peritoneal lining, causing a chronic inflammatory effusion that is notoriously hard to diagnose.
Standard fluid cultures often come back negative. Surgeons typically need to biopsy the lining to find hidden bacterial granulomas. Once diagnosed, treatment involves four antibiotics taken daily for up to nine months.
Recognizing the Symptoms: How to Tell Bloating From Dangerous Fluid
One of the most common questions I hear is: how do I know if this is just bloating or something serious? The clinical presentation of ascites is actually quite distinct.
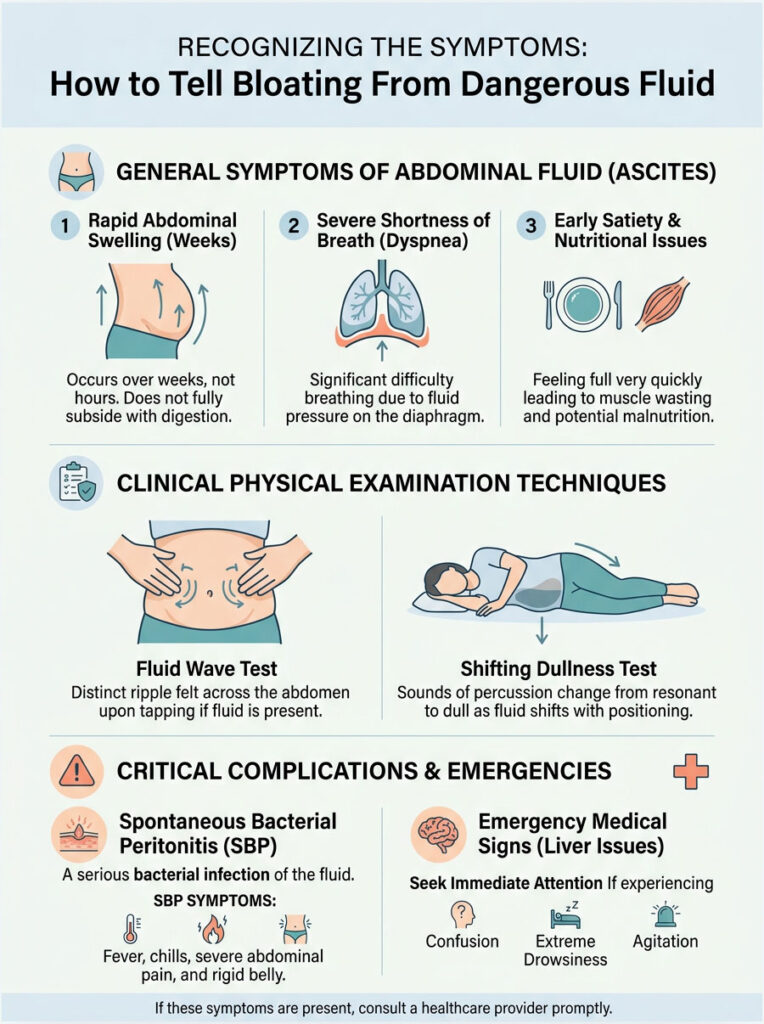
What You Might Notice at Home
The most obvious sign is a rapid, unexplainable increase in abdominal size. Your pants suddenly stop fitting over a period of weeks, not months. This is much faster than typical weight gain.
You may also notice severe shortness of breath. Trapped fluid pushes upward against the diaphragm, preventing the lungs from fully expanding, especially when lying flat at night.
Early satiety is another common complaint. Because the stomach is physically compressed by surrounding pressure, you feel full after just a few bites of food. This often leads to muscle wasting and malnutrition.
Physical Examination Signs
Hepatologists perform specific bedside tests to confirm the presence of free-flowing fluid.
The fluid wave test involves pressing a hand along the midline of the bare stomach, then tapping sharply on one side. If fluid is present, a distinct ripple is felt on the opposite side. Fat tissue does not transmit a wave like this.
The shifting dullness test involves tapping across the abdomen while the patient lies flat, then asking them to roll onto their side. If the dull sounds shift with gravity, it confirms free-flowing, uncontained fluid.
Spontaneous Bacterial Peritonitis: A Life-Threatening Red Flag
One complication every liver specialist watches for is spontaneous bacterial peritonitis (SBP), a sudden infection of the trapped fluid. Symptoms include a spiking fever with chills, severe abdominal pain that does not ease, and a belly that becomes rigid and tender to the lightest touch.
If a patient with a swollen abdomen suddenly becomes confused, extremely drowsy, or unusually agitated, they need emergency care immediately. This can indicate ammonia toxins are bypassing the liver and affecting the brain.
Ascites vs. Bloating: A Clinical Comparison
Understanding the difference between pathological fluid and everyday bloating is critical. Here is a side-by-side comparison:
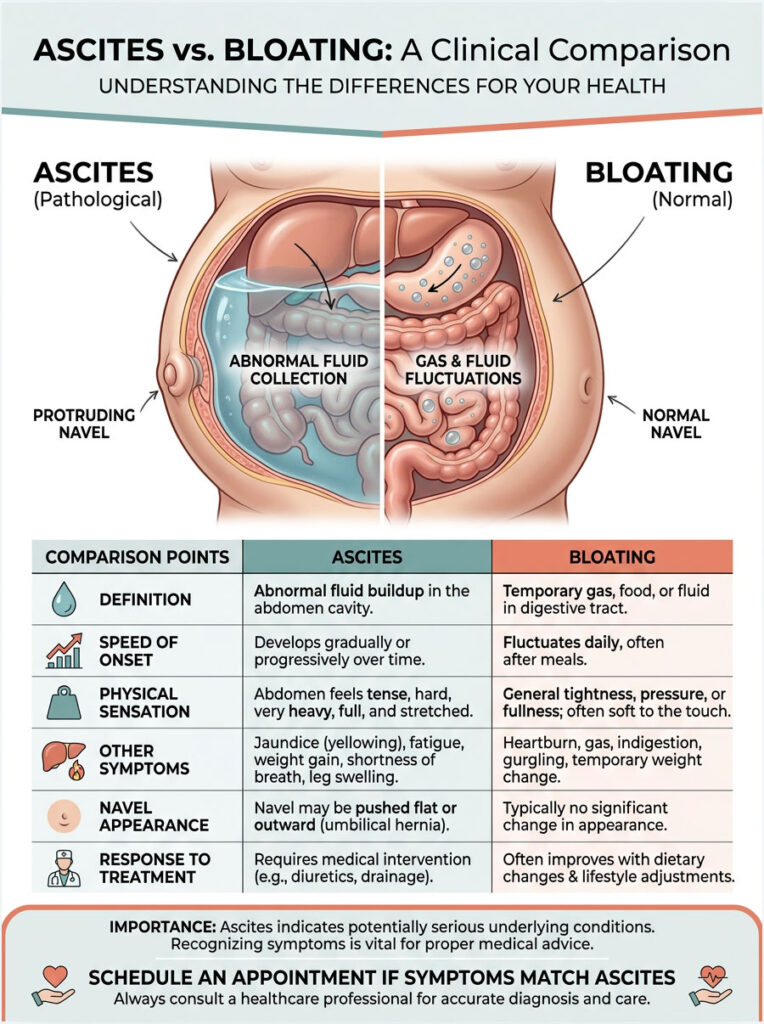
| Feature | Pathological Ascites | Normal Bloating |
| Speed of Onset | Develops over days to weeks; progressive. | Fluctuates daily; often worse in the evening. |
| Physical Sensation | Heavy, tight, shifting with gravity. | General tightness; often relieved by passing gas. |
| Other Symptoms | Jaundice, swollen ankles, extreme fatigue. | Mild heartburn, indigestion, dietary triggers. |
| Navel Appearance | Often pushed outward (everted). | Stays normal or deepens slightly. |
| Response to Treatment | Requires diuretics and sodium restriction. | Improves with diet changes, fiber, or antacids. |
If your symptoms match the ascites column, do not wait. Schedule an appointment with a gastroenterologist for proper imaging.
Diagnostic Pathways: How Doctors Confirm What Causes Fluid in the Abdomen
When a patient arrives at the emergency room with these symptoms, we follow strict, standardized diagnostic protocols. We combine needle extractions, lab work, and advanced imaging to identify the exact cause.
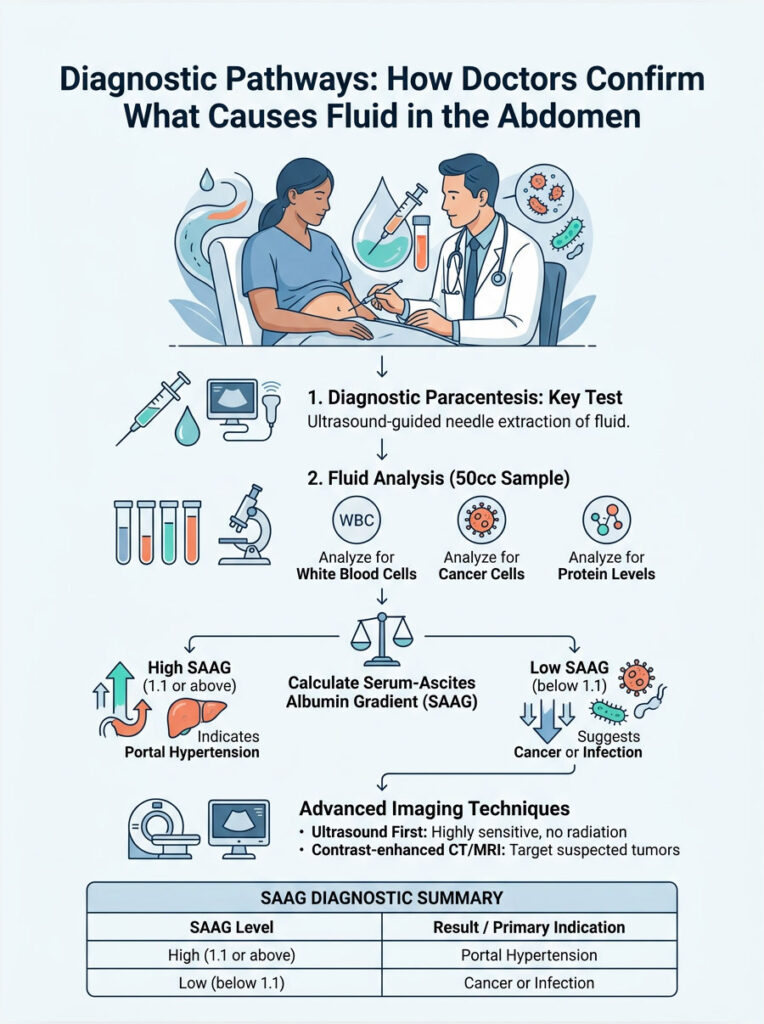
Diagnostic Paracentesis
The single most important test is a diagnostic paracentesis. Using a high-frequency ultrasound, I map out a safe pocket of fluid, avoiding the arteries and bowel. After numbing the skin with lidocaine, I insert a thin, specialized needle through the abdominal wall.
A small 50cc sample is extracted and sent to the lab on ice. Pathologists check it for white blood cells, cancer cells, and specific protein levels.
The Serum-Ascites Albumin Gradient (SAAG)
The most critical calculation we make from that fluid sample is the SAAG, which stands for the Serum-Ascites Albumin Gradient. We subtract the albumin level found in the belly fluid from the albumin level in your blood.
For example, if your blood albumin is 3.2 and your fluid albumin is 1.0, your SAAG is 2.2. A high SAAG (1.1 or greater) confirms portal hypertension as the driving force. A low SAAG (below 1.1) points toward cancer or infection. This single calculation shapes your entire treatment plan.
Advanced Imaging
Alongside the paracentesis, we rely on advanced imaging. An abdominal ultrasound with Doppler is typically the first step. It is sensitive, radiation-free, and can detect even small amounts of hidden fluid. It also lets us examine the liver’s texture and check the portal vein for blood clots.
If we suspect a malignant cause based on a low SAAG score, we order a contrast-enhanced CT scan or MRI. These detailed scans help locate primary tumors in the ovaries, pancreas, or stomach lining.
SAAG Diagnostic Summary
| Marker | High SAAG (1.1 or above) | Low SAAG (below 1.1) |
| Primary Mechanism | Portal Hypertension (high pressure). | Inflammatory or malignant mechanisms. |
| Common Causes | Cirrhosis, right heart failure, alcoholic hepatitis. | Ovarian cancer, tuberculosis, severe pancreatitis. |
| Fluid Appearance | Usually clear, pale yellow (transudate). | Often cloudy, bloody, or milky white (exudate). |
| Total Protein | Typically low (below 2.5 g/dL). | Typically high (above 2.5 g/dL). |
Modern Medical Treatments and Interventions
The field of hepatology is advancing rapidly. We have moved well beyond basic water pills. Modern medicine now offers a range of life-saving techniques for managing severe abdominal fluid.
Diuretic Medication Protocols
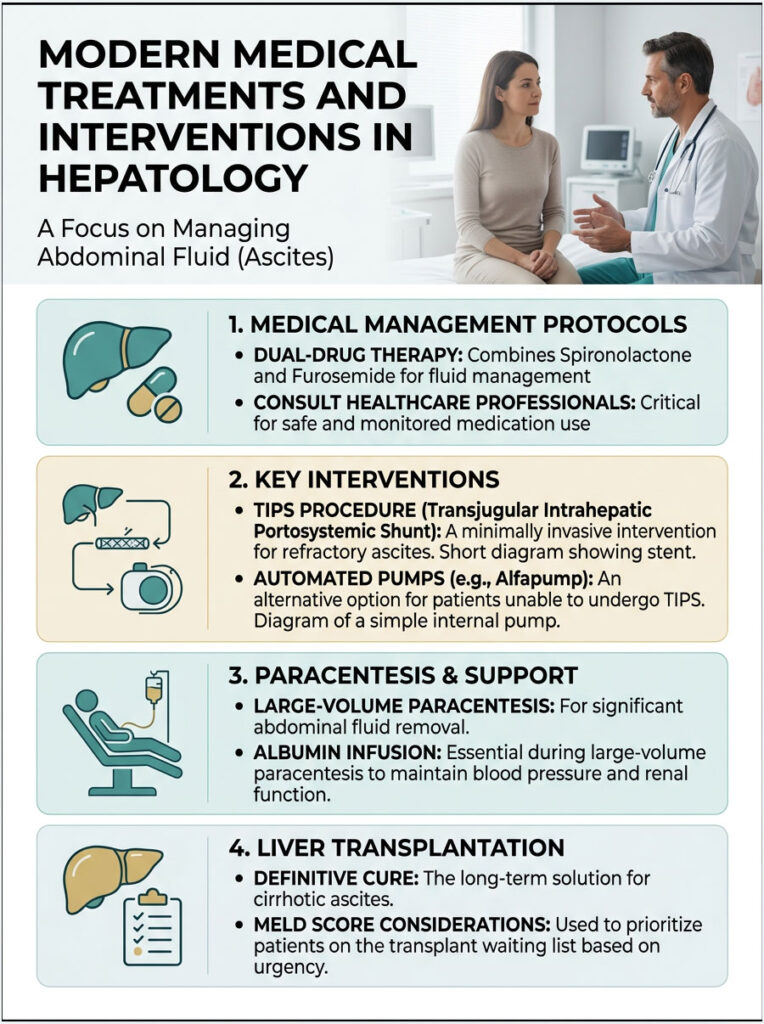
The gold standard treatment is a dual-drug therapy combining Spironolactone and Furosemide. Spironolactone works as an aldosterone antagonist in the kidney, helping you lose water while retaining potassium. Furosemide, a loop diuretic, accelerates water loss but depletes potassium.
Taken together in a 100mg-to-40mg ratio, these drugs keep your electrolytes balanced. Never skip a dose or take extra without consulting your physician. Improper use can cause dangerous heart arrhythmias from sudden potassium shifts.
The TIPS Procedure for Refractory Cases
When maximum doses of diuretics fail to control the swelling, we call it refractory ascites. One of the best tools for this situation is the TIPS procedure, which stands for Transjugular Intrahepatic Portosystemic Shunt.
During this minimally invasive surgery, an interventional radiologist navigates a wire through the neck vein and places a metal stent directly through the scarred liver. This creates a new, low-resistance tunnel for blood flow, instantly reducing portal pressure and stopping the fluid leak at its source.
Albumin Infusion During Large-Volume Paracentesis
When patients need large volumes drained to breathe comfortably (often 8 to 10 liters), blood pressure can drop dangerously. To prevent this, we administer an intravenous albumin infusion during the procedure.
If we remove more than five liters, the albumin replaces the lost oncotic pressure and protects the kidneys from sudden failure.
Automated Pumps and Liver Transplantation
For patients too ill for a TIPS procedure, newer technologies offer real hope. Surgically implanted pump systems (like the Alfapump) continuously move trapped fluid from the belly to the urinary bladder, allowing the patient to simply urinate it away.
Ultimately, the only true cure for cirrhotic ascites is a liver transplant. Developing ascites automatically raises a patient’s MELD score, moving them higher on the transplant waiting list. All other therapies are bridges to keep the patient alive until a donor organ becomes available.
Managing Your Condition at Home: Practical Strategies
Even the best hospital treatments have limits. Your daily habits play a huge role in long-term outcomes. Managing this condition at home requires real discipline.

Strict Dietary Sodium Restriction
The cornerstone of managing ascites is a strict low-sodium diet. Sodium acts like a magnet for water in your tissues. If you eat too much salt, your body traps water, and your medications become far less effective.
You need to limit total sodium to under 2,000 milligrams per day. This is harder than most people realize. Processed foods, canned soups, frozen dinners, and restaurant meals are loaded with hidden salt.
Learn to read nutrition labels carefully. Stop using the salt shaker entirely. Flavor your food with fresh lemon, garlic, herbs, and salt-free spice blends instead.
Daily Weight Monitoring
Buy a reliable digital scale and weigh yourself every morning, right after using the restroom and before eating or drinking anything. Keep a written log of your daily weights.
A sudden gain of more than two pounds in a single day is a major red flag. It means your kidneys are struggling to excrete sodium and you are retaining fluid. If you see a rapid upward trend over three days, call your hepatology clinic right away. We can often adjust your medications over the phone.
Fluid Restriction: Clearing Up a Common Myth
Many patients mistakenly believe they need to stop drinking water to reduce swelling. Let me be clear: fluid restriction is usually not necessary for most liver patients.
Your body is holding onto sodium, not just water. Cutting your water intake will only make you feel dizzy and dehydrated. You only need to restrict fluids if your blood sodium drops dangerously low, a condition called hyponatremia. Drink enough water to satisfy your thirst. Focus your energy on cutting salt instead.
Clinical Case Studies: Lessons From the Hospital
Medical theory can be hard to grasp on its own. Real-world examples help bring the science to life. Here are two anonymized cases from my clinical practice.
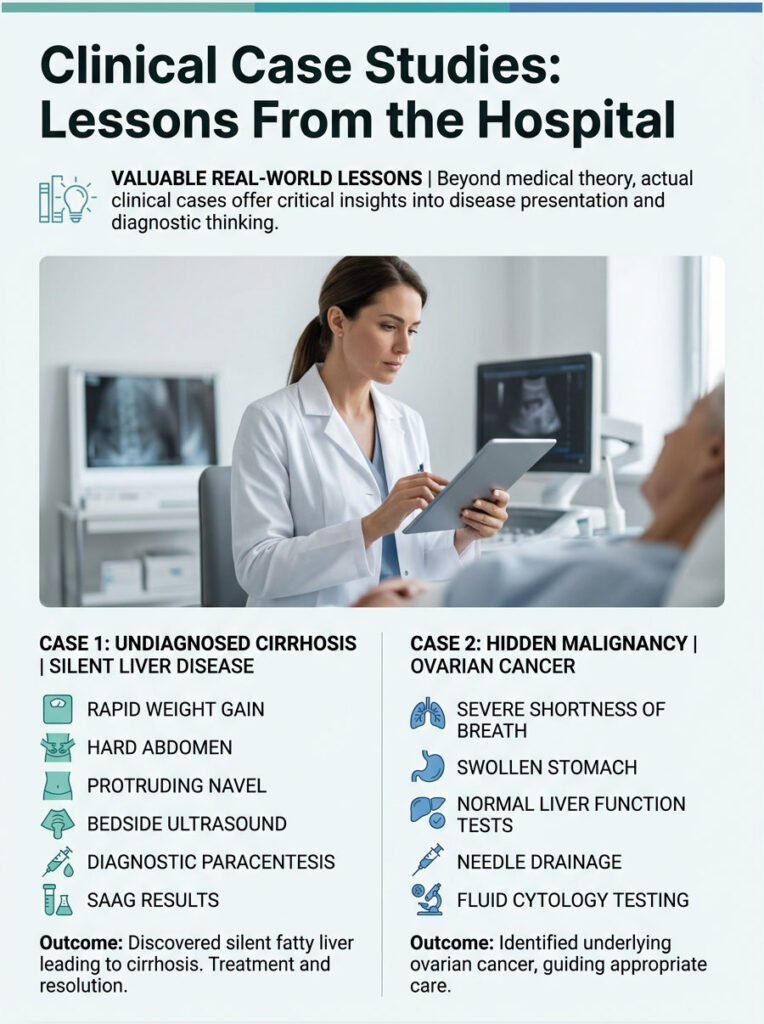
Case 1: The Undiagnosed Cirrhotic Patient
A 55-year-old man came to my clinic complaining of rapid weight gain. His primary care doctor had dismissed it as typical middle-aged weight gain and suggested a diet plan. But his belly was rock-hard, and his navel was protruding outward.
I performed a bedside ultrasound and found a large amount of free-floating fluid. We did a diagnostic paracentesis that same afternoon. The SAAG came back at 1.4 g/dL, confirming portal hypertension.
Further testing revealed silent fatty liver disease that had quietly progressed to end-stage cirrhosis. He had never been a heavy drinker, which had initially confused his doctor. Within three weeks on a strict sodium restriction and dual diuretic therapy, his swelling resolved completely. He lost 25 pounds of pure water weight and is now on the liver transplant waiting list.
Case 2: Identifying Hidden Malignancy
A 62-year-old woman arrived at the emergency room with severe shortness of breath and a massively swollen stomach. She had no history of alcohol use, diabetes, or liver disease. Her liver blood tests were perfectly normal.
We performed an urgent needle drain. The fluid was cloudy and distinctly bloody. Her SAAG was just 0.8 g/dL, immediately ruling out liver involvement.
Cytology testing revealed aggressive ovarian cancer cells floating in the sample, a textbook presentation of malignant ascites driven by peritoneal carcinomatosis. Her abdominal swelling was the very first symptom of a hidden stage-four cancer. She was immediately transferred to a gynecological oncologist for surgery and chemotherapy.
This case is exactly why we test the fluid every single time.
The Psychological Impact of Chronic Abdominal Swelling
Doctors often focus on the physical mechanics of disease and forget about the person living through it. The psychological toll of chronic abdominal swelling can be devastating.
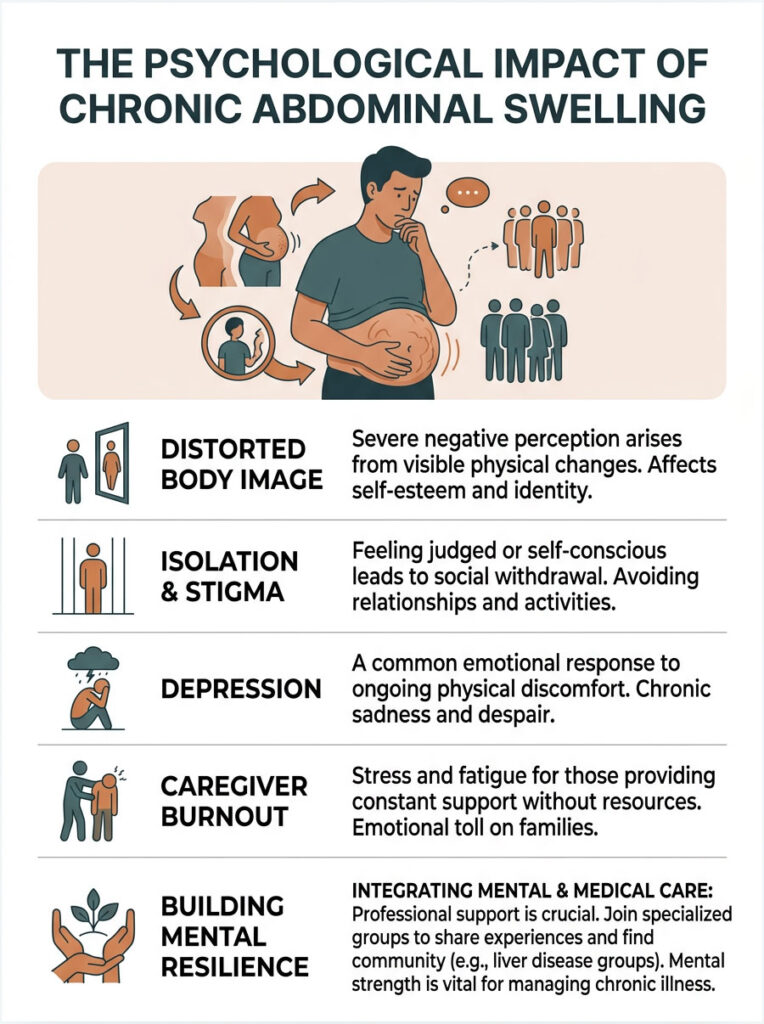
Patients often deal with profound body image issues as their stomachs swell to the size of a full-term pregnancy while their arms and legs waste away. Social isolation, depression, and caregiver burnout are all common.
I strongly encourage patients to seek professional mental health support and join specialized liver disease support groups. Connecting with others who understand the daily challenges of diuretic management and dietary restriction can be incredibly healing. Mental resilience matters just as much as medication when you are fighting a chronic illness.
Summary and Key Takeaways
Unexplained fluid in the abdomen is a major systemic warning sign. It is never just bloating or simple weight gain. It signals that a vital organ system, whether the liver, heart, kidneys, or something else entirely, needs immediate expert evaluation.
We have covered the full spectrum of causes, from cirrhosis and portal hypertension to hidden cancers and rare infections. You now understand the mechanical forces at play, the role of sodium, and the critical importance of oncotic protein balance.
Remember: early detection saves lives. If your stomach swells rapidly and feels tight, demand a diagnostic ultrasound and a SAAG calculation. Follow your low-sodium diet, take your medications as prescribed, and work closely with a specialist to manage what causes fluid in the abdomen. Your health depends on it.
Frequently Asked Questions
What is the primary medical cause for sudden fluid accumulation in the abdomen?
As a board-certified hepatologist, I find that approximately 80% of all cases are driven by advanced liver cirrhosis. This condition leads to portal hypertension, where dense scar tissue creates a structural blockage in the liver, forcing clear plasma to leak out of the portal vein and into the peritoneal cavity.
How can I distinguish between normal weight gain and pathological ascites?
Unlike gradual adipose tissue accumulation, pathological fluid develops rapidly over days or weeks. Key clinical indicators include a belly that feels tight like a drum, a navel that begins to push outward (everted umbilical hernia), and a ‘fluid wave’ sensation where a physical ripple can be felt across the abdomen when tapped.
What is a SAAG score, and why is it necessary for an accurate diagnosis?
The Serum-Ascites Albumin Gradient (SAAG) is the ultimate diagnostic compass. By subtracting the albumin level in the abdominal fluid from the albumin level in the blood, we can determine the cause. A score of 1.1 g/dL or higher confirms portal hypertension, while a lower score points toward malignancy, infection, or pancreatitis.
Can heart problems lead to fluid buildup in the stomach area?
Yes, specifically right-sided congestive heart failure. When the right side of the heart weakens, blood backs up into the venous system and the hepatic veins. This increased pressure causes the liver to become engorged, mimicking portal hypertension and causing fluid to seep into the abdominal space.
What are the ‘red flag’ symptoms that indicate a life-threatening complication?
You must seek emergency care if you experience a sudden fever, chills, or intense abdominal tenderness. These are hallmark signs of Spontaneous Bacterial Peritonitis (SBP), a dangerous infection of the trapped fluid. Additionally, rapid mental confusion or extreme sleepiness suggests that toxins are bypassing the liver and affecting the brain.
Why do specialists perform a diagnostic paracentesis for abdominal swelling?
Paracentesis is the gold standard procedure for evaluating this condition. By using a thin, ultrasound-guided needle to extract a sample of the liquid, we can analyze it for white blood cells to check for infection, protein levels to calculate the SAAG, and cytology to rule out malignant cancer cells.
How does a low-sodium diet help manage abdominal fluid retention?
Sodium acts like a microscopic magnet for water. In patients with liver disease, the kidneys activate the RAAS system, which aggressively retains salt. Limiting intake to less than 2,000mg per day is the cornerstone of treatment, as it prevents the body from trapping the extra water that fuels the swelling.
What is the TIPS procedure, and when is it recommended?
The Transjugular Intrahepatic Portosystemic Shunt (TIPS) is a minimally invasive surgery where an interventional radiologist places a stent to create a bypass through the scarred liver. This is typically reserved for ‘refractory’ cases where the fluid returns relentlessly despite maximum doses of diuretic medications.
Why does liver failure cause fluid to leak out of the blood vessels?
A failing liver stops producing albumin, a vital protein that maintains oncotic pressure. Without enough albumin to hold water inside the vessels (hypoalbuminemia), the blood loses its holding power, allowing liquid to leak through porous vessel walls and pool in the abdominal cavity due to gravity.
Can cancer be the cause of fluid in the abdomen if my liver tests are normal?
Absolutely. This is known as malignant ascites. Cancers of the ovaries, pancreas, or colon can spread to the abdominal lining (peritoneal carcinomatosis). These tumor cells irritate the lining, causing localized inflammation and the production of an inflammatory exudate that fills the cavity regardless of liver health.
Is it necessary to restrict my water intake to cure the swelling?
This is a common misconception. Most patients do not need to restrict pure water; the primary focus must be on dietary sodium restriction. You only need to limit oral fluids if your blood tests show dangerously low sodium levels, a specific condition known as hyponatremia.
Why do I feel full after only a few bites of food when my belly is distended?
This is called ‘early satiety.’ The massive volume of fluid in your peritoneal cavity physically compresses the stomach and other digestive organs. This intense pressure prevents the stomach from expanding normally during meals, which often leads to unintended weight loss and muscle wasting despite the swelling.
Disclaimer
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. The content is written by a medical professional but is intended to provide general education. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
References
- American Association for the Study of Liver Diseases (AASLD) – https://www.aasld.org – Provided clinical practice guidelines for the management of adult patients with ascites due to cirrhosis.
- Mayo Clinic – https://www.mayoclinic.org – Source for the pathophysiology of hypoalbuminemia and oncotic pressure loss in renal and hepatic failure.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – https://www.niddk.nih.gov – Provided statistical data regarding the prevalence of NASH (MASLD) and its progression to cirrhosis.
- Journal of Hepatology – European Association for the Study of the Liver (EASL) – Detailed the mechanisms of splanchnic vasodilation and the RAAS system activation.
- Cleveland Clinic – https://my.clevelandclinic.org – Provided diagnostic criteria for the Serum-Ascites Albumin Gradient (SAAG) and its clinical applications.
- American Heart Association (AHA) – https://www.heart.org – Referenced for the connection between right-sided congestive heart failure and hepatic congestion.
- The Lancet Gastroenterology & Hepatology – Provided research on the safety and efficacy of diagnostic paracentesis and the TIPS procedure.





