

A Cardiologist Explains the Surprising Link Between Fluid Loss and Hypertension
In 15 years of clinical cardiology, one question has come up more often than you might expect. Patients sit across from me, stare at their elevated readings, and ask: can dehydration actually cause high blood pressure? The short answer is yes, absolutely.
Table of Contents
Most people assume that when you lose fluid, your blood volume drops and your pressure should naturally fall. On the surface, that logic sounds perfectly reasonable. But your cardiovascular system is not a simple set of static pipes. It is a highly dynamic biological environment driven by aggressive survival mechanisms.
When your body senses a drop in fluid levels, it does not passively accept the loss. It panics. It launches a cascade of chemical and hormonal reactions designed to keep blood flowing to your brain and heart at all costs. These survival mechanisms squeeze your arteries, trap sodium, and force your pressure upward, sometimes dramatically.
In this guide, we will explore exactly how fluid deficits trigger systemic vasoconstriction. We will look at serum osmolality, endothelial dysfunction, and baroreceptor sensitivity. By the end, you will understand why proper hydration is a non-negotiable pillar of cardiovascular health.
Quick Answer: Can Dehydration Cause High Blood Pressure?
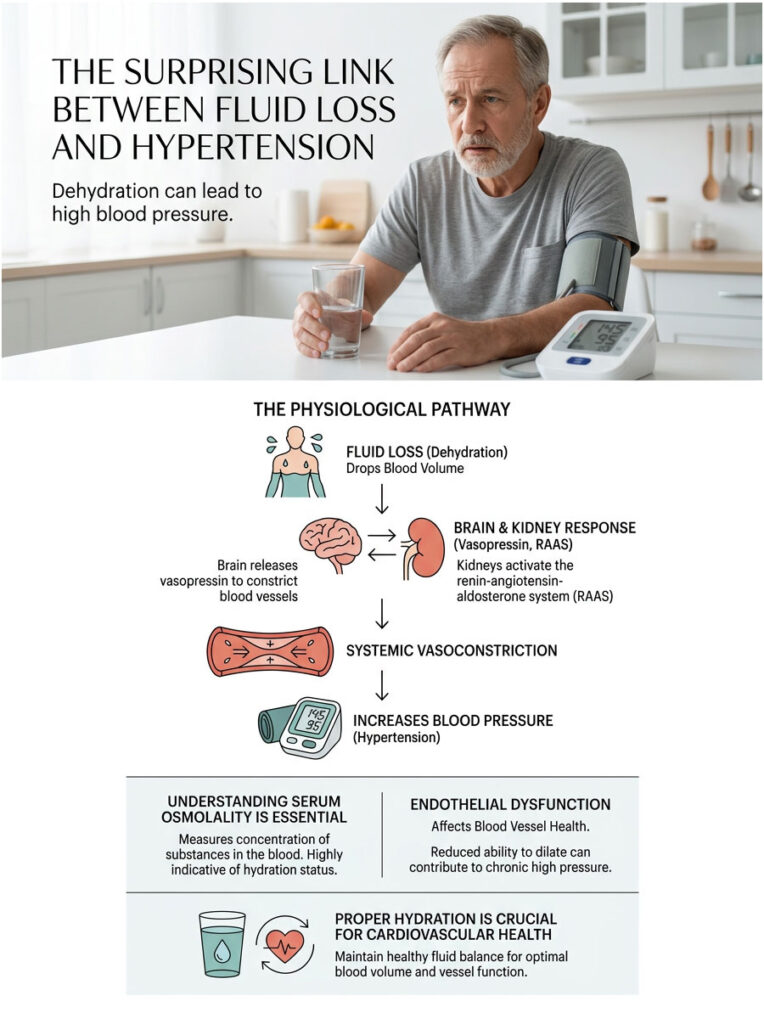
Yes. When the body loses fluid, blood volume drops. To protect vital organs, the brain releases vasopressin, a hormone that constricts blood vessels. At the same time, the kidneys activate the renin-angiotensin-aldosterone system (RAAS), which further narrows arteries and retains sodium. This systemic vasoconstriction causes blood pressure to rise significantly, even though total fluid volume is low.
Key Statistics: Dehydration and Cardiovascular Health
- Up to 75% of American adults function in a state of chronic mild dehydration.
- A fluid loss of just 2% of body weight can trigger a 15 mmHg increase in systolic blood pressure.
- The National Academies of Sciences, Engineering, and Medicine recommends 3.7 liters of daily fluid for men and 2.7 liters for women.
- Chronic suboptimal hydration is linked to a 20% higher risk of developing essential hypertension over a 10-year period.
- ER visits for dehydration-related high blood pressure spike by 30% during summer heatwaves.
- Roughly 45% of elderly patients admitted for hypertensive crises show clinical markers of severe fluid deficits.
- Proper daily hydration can improve arterial compliance by as much as 12% in middle-aged adults.
The Physiology Behind Dehydration and High Blood Pressure
To understand the connection between dehydration and hypertension, you have to look under the hood of human physiology. Your body operates on a strict set of priorities, and survival always comes first.
When you don’t drink enough water, your blood volume begins to drop. Your brain and kidneys detect this immediately through specialized cellular sensors. They don’t care about maintaining a textbook-perfect 120/80 reading. Their only concern is keeping enough pressure in the system to push oxygenated blood to your brain, heart, and lungs. To make that happen, they trigger several powerful biological alarms.
Vasopressin: The Dual-Action Survival Hormone
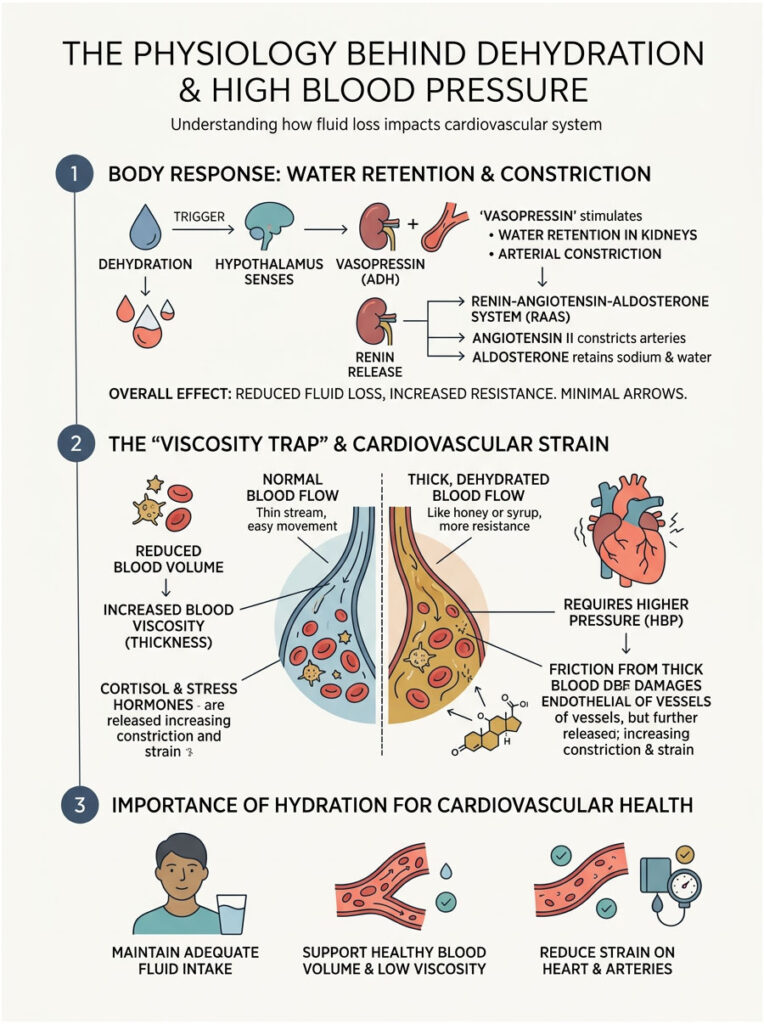
Vasopressin, also known as anti-diuretic hormone (ADH), is one of the most powerful chemicals your body produces. It plays a dual role: managing water retention and controlling arterial constriction.
When you are dehydrated, your blood becomes thicker. Sodium and other solutes concentrate rapidly, a state known clinically as high serum osmolality. The hypothalamus detects this change instantly and signals the pituitary gland to release a surge of vasopressin.
Vasopressin travels to your kidneys and tells them to stop producing urine, forcing your body to hold onto every drop of water it can. But that is only half the story. Vasopressin also binds to V1 receptors on the smooth muscle lining your arterial walls, causing your blood vessels to clamp down and tighten.
This systemic squeezing drastically increases peripheral vascular resistance. Think of it like pressing your thumb over the end of a running garden hose. The volume of water decreases, but the pressure shooting out of the nozzle jumps dramatically. This is the first major reason fluid loss pushes your blood pressure up.
The Renin-Angiotensin-Aldosterone System (RAAS) Cascade
The second major survival mechanism fires inside your kidneys. Your kidneys act as highly sensitive pressure sensors, filtering your blood around the clock. When blood volume drops, blood flow reaching the kidneys slows down. They interpret this as a life-threatening emergency.
In response, specialized juxtaglomerular cells release an enzyme called renin into the blood. This triggers a chain reaction known as the renin-angiotensin-aldosterone system. Renin converts a liver-produced protein into Angiotensin I, which then gets converted in the lungs into Angiotensin II.
Angiotensin II is one of the most aggressive vasoconstricting chemicals your body can produce. It forces your arteries to narrow dramatically from head to toe. On top of that, it triggers the release of aldosterone from your adrenal glands. Aldosterone forces your kidneys to reabsorb sodium, and where sodium goes, water follows.
This combination of severe vasoconstriction and heavy sodium retention creates a perfect storm for elevated readings. RAAS activation is the primary driver of dehydration-induced hypertension.
Blood Viscosity and Endothelial Damage
Beyond hormonal cascades, there is a purely physical problem. When you lack water, your blood literally changes texture. It becomes thicker, stickier, and much harder to pump.
High plasma osmolality means your blood is densely concentrated with excess solutes like sodium and glucose. Pumping this thick fluid requires a massive amount of mechanical effort. Your heart has to beat with greater force just to move it through the system, which directly elevates systolic pressure.
But there is a more insidious issue happening inside your arteries. The inner lining of your blood vessels, called the endothelium, is a delicate single-cell layer responsible for producing nitric oxide. Nitric oxide is the molecule that keeps your blood vessels relaxed, flexible, and wide open.
When thick, viscous blood scrapes against the endothelium, it causes microscopic friction and damage. This leads to endothelial dysfunction. The damaged lining stops producing enough nitric oxide, and your blood vessels lose the ability to relax. They lock into a stiff, constricted state, further driving up your numbers.
Cortisol and Stress Hormones: The Hidden Amplifier
Your body treats dehydration as a severe physiological stressor. It does not distinguish between the stress of running from a predator and the stress of ignoring your thirst. Both scenarios activate your sympathetic nervous system.
When you stay dry too long, your adrenal glands release cortisol and adrenaline, the classic “fight or flight” hormones. These increase your heart rate and cause immediate vascular constriction. Cortisol makes your blood vessels extra sensitive to adrenaline’s squeezing effect and promotes sodium retention, compounding the damage from aldosterone.
Chronically elevated cortisol from poor hydration keeps your nervous system locked in overdrive. You might feel anxious, jittery, or unable to concentrate. Meanwhile, your blood pressure stays artificially elevated due to constant chemical stress.
The Viscosity Trap: Imagine trying to suck water through a thin straw. It is easy and takes almost no effort. Now imagine trying to suck a thick milkshake through that same straw. You have to pull with immense force. That “force” is your blood pressure, and the milkshake is your blood when you ignore your daily water needs.
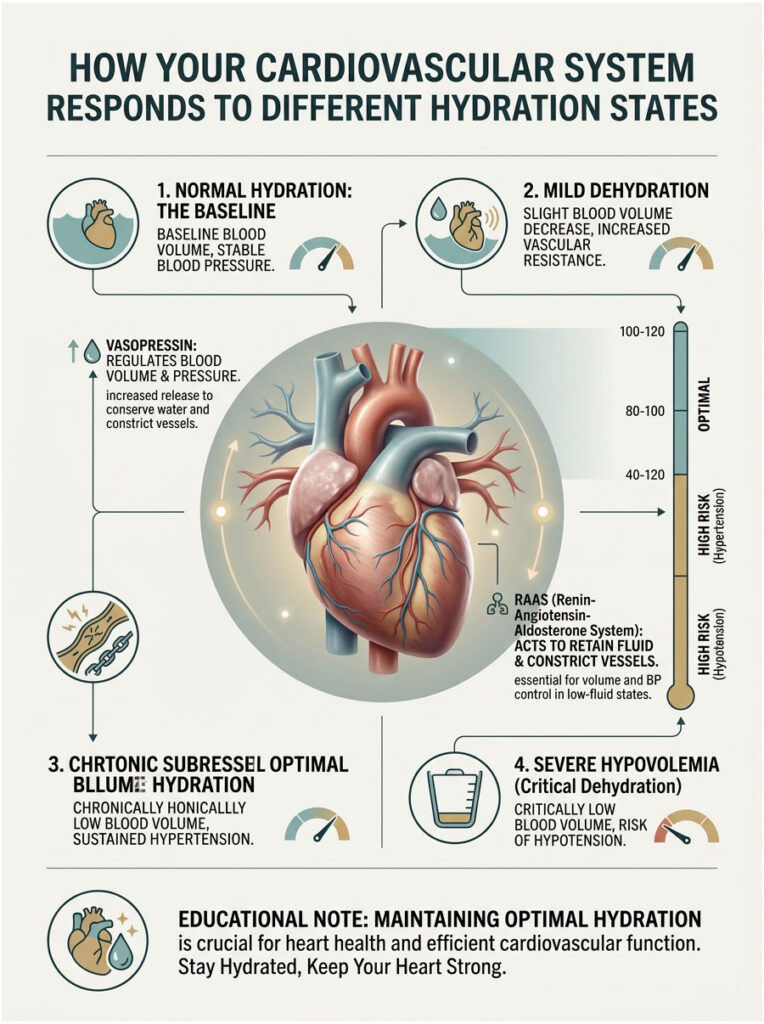
How Your Cardiovascular System Responds to Different Hydration States
| Hydration State | Blood Volume | Vasopressin | RAAS Activity | Vascular Resistance | BP Impact |
| Optimal | Normal | Baseline | Suppressed | Normal / Relaxed | Stable |
| Mild Dehydration | Slightly Low | Elevated | Mildly Active | Increased | Systolic Spike Likely |
| Chronic Suboptimal | Chronically Low | Chronically High | Highly Active | Stiffened / High | Sustained Hypertension |
| Severe Hypovolemia | Critically Low | Maximized | Maximized | Failing | Hypotension (Crash) |
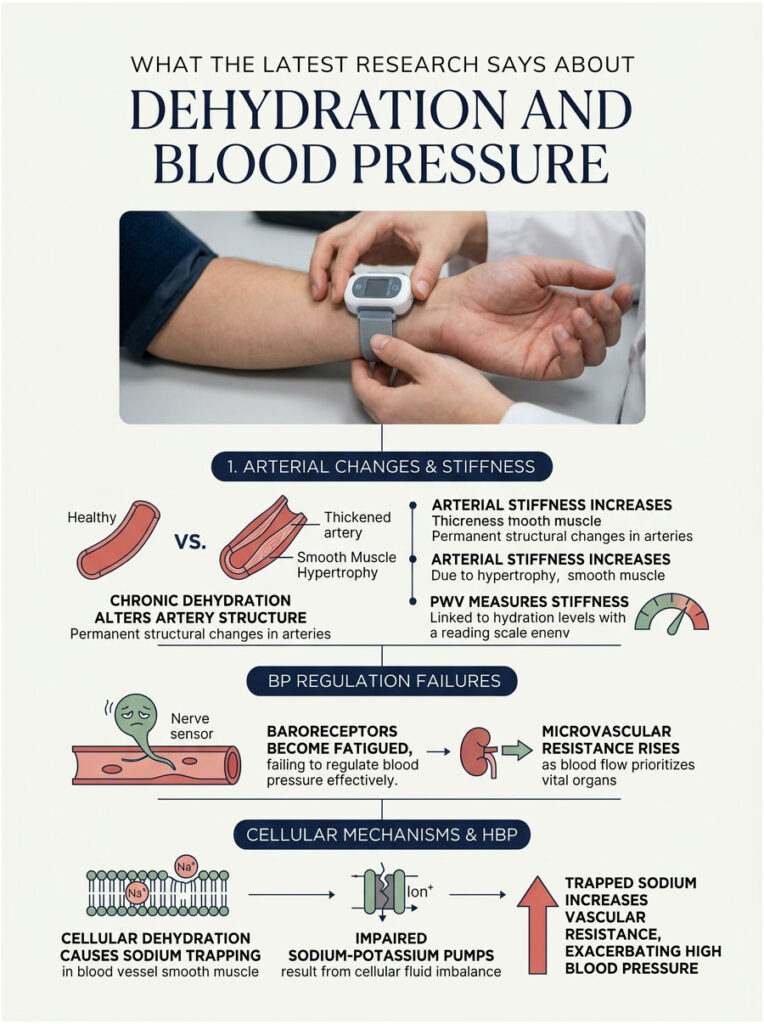
What the Latest Research Says About Dehydration and Blood Pressure
The relationship between blood pressure and water intake has been studied extensively in recent years, and the data paints a clear picture. Poor hydration habits don’t just cause a temporary blip on your blood pressure cuff. Over time, they cause permanent structural changes to your cardiovascular system.
Arterial Stiffness and Chronic Dehydration
Your arteries are designed to be highly flexible, expanding and contracting smoothly with every heartbeat. This elasticity keeps your blood pressure within a healthy range. However, chronic dehydration fundamentally alters this elasticity at a cellular level.
When you are consistently low on fluids, your body resets its natural pressure set-point. Because the RAAS cascade stays constantly activated, your arteries never fully relax. Over time, the smooth muscles in the arterial walls physically thicken, a process called hypertrophy. This thickening leads to permanent loss of flexibility.
Researchers measure this using a metric called Pulse Wave Velocity (PWV). Studies consistently show that individuals with low daily water intake have significantly higher markers of arterial stiffness. When your arteries lose compliance, every heartbeat generates a higher pressure wave, locking in a dangerous state of chronic hypertension.
Microvascular Resistance and Baroreceptor Failure
We also need to discuss your smallest blood vessels. Your microscopic capillaries feed oxygen directly to organs and tissues. When you are dehydrated, your body aggressively prioritizes blood flow to the brain and heart by clamping down on capillaries in your skin, muscles, and extremities.
This clamping creates intense microvascular resistance. Your heart has to pump much harder to push blood through these narrowed capillary beds, which drives systolic readings higher. At the same time, something dangerous happens in your nervous system.
Baroreceptors are tiny pressure sensors in your carotid arteries and aortic arch. Their job is to monitor blood pressure and tell your brain to make adjustments. But when these sensors are constantly bombarded by viscous blood and hormonal alarms, they become dull and fatigued. They literally stop telling the brain to lower the pressure. Your body accepts the new, dangerously high baseline as normal, and this blunted baroreceptor sensitivity makes it incredibly hard to bring your numbers back down.
Cellular Dehydration and Sodium Trapping
There is more to the story than just the blood in your veins. Your body contains trillions of cells, and they all need water to function. When you don’t drink enough, your body steals water from the interstitial fluid (the fluid surrounding your cells) to keep blood volume up.
Once that runs low, your body starts pulling water directly from inside the cells themselves. This impairs the sodium-potassium pumps on cell membranes. These pumps need a perfect fluid balance to push sodium out and pull potassium in. When cells shrink from dehydration, the pumps fail.
Sodium gets trapped inside the smooth muscle cells of your blood vessels, which causes calcium to flood in and trigger intense, unrelenting contractions. This cellular mechanism is a primary reason why dehydration drives up vascular resistance so aggressively.
Acute Spikes vs. Chronic Hypertension: Understanding the Difference
How dehydration affects your heart depends entirely on how fast you lose fluid and how long you stay dry. Many patients confuse a sudden pressure spike with chronic essential hypertension. While both are dangerous, they require completely different approaches.
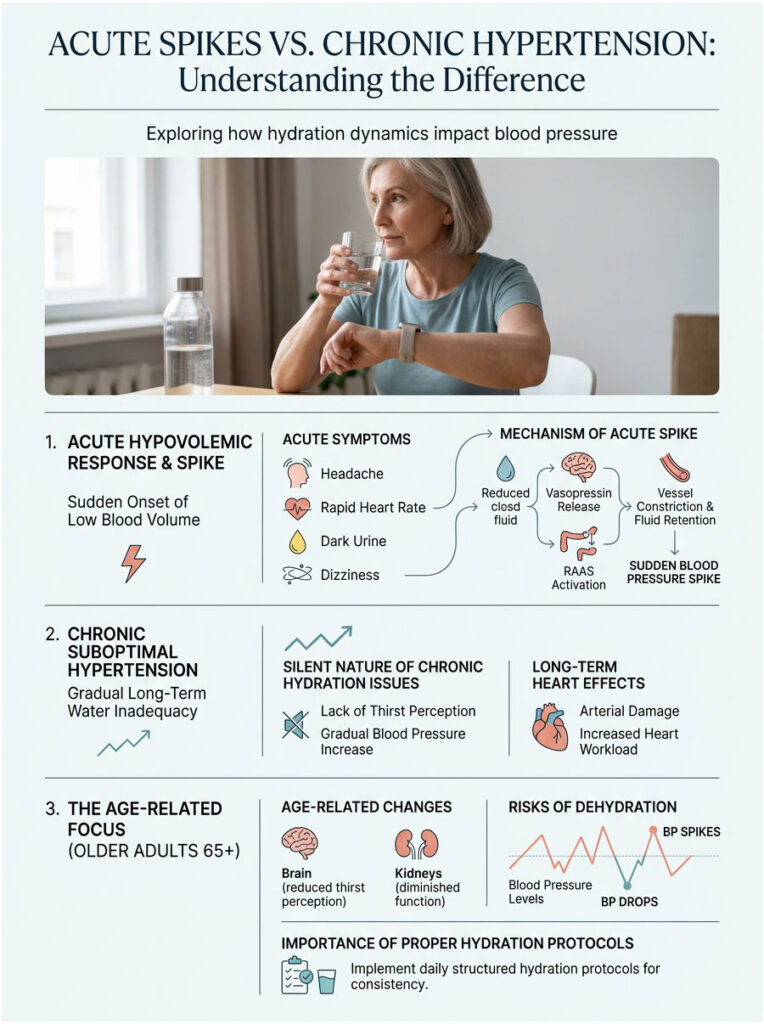
The Acute Hypovolemic Response
An acute response happens suddenly and aggressively. Picture doing intense yard work on a hot July afternoon without a water bottle, or recovering from a severe stomach illness with rapid fluid loss.
In these scenarios, blood volume drops fast over just a few hours. Your body floods the system with vasopressin, RAAS kicks into overdrive, and you experience classic symptoms: pounding headache, rapid heart rate, dark urine, and dizziness when standing (orthostatic hypotension).
If you check your pressure during this acute phase, you will likely see a frightening systolic spike. This is your body desperately trying to keep you conscious. Once you absorb enough fluids and electrolytes, the hormonal alarms shut off and pressure usually normalizes within hours.
The Silent Danger of Chronic Suboptimal Hydration
Chronic suboptimal hydration is a completely different problem, and far more insidious. This is the silent pattern that damages your heart over decades. It happens when you consistently fail to meet your daily fluid needs for months or years.
You might drink a few cups of coffee, maybe a small glass of water with dinner, and assume you are fine. Patients in this category rarely feel “thirsty” anymore. Their thirst mechanism has adapted to a constant, low-level drought.
But functionally, their bodies are struggling. They live in a permanent state of elevated plasma osmolality. Because the fluid deficit is mild but constant, the body maintains a low-grade RAAS activation. This steady drip of Angiotensin II slowly stiffens the arteries year after year, with no sudden spikes to sound the alarm. Baseline pressure just creeps up, point by point, over time.
Age-Related Changes in Thirst and Vascular Compliance
As we age, our bodies undergo significant changes in how they handle water. The aging brain naturally blunts thirst perception. Older adults often don’t feel thirsty even when they are clinically dehydrated. At the same time, aging kidneys lose the ability to concentrate urine effectively, meaning elderly individuals lose more water throughout the day.
Combine this with naturally stiffening arteries, and you have a recipe for erratic blood pressure. Mild dehydration in older patients can cause dangerous drops when standing, followed by severe spikes when lying down. Proper hydration protocols are absolutely critical for anyone over 65.
Acute vs. Chronic Dehydration: A Clinical Comparison
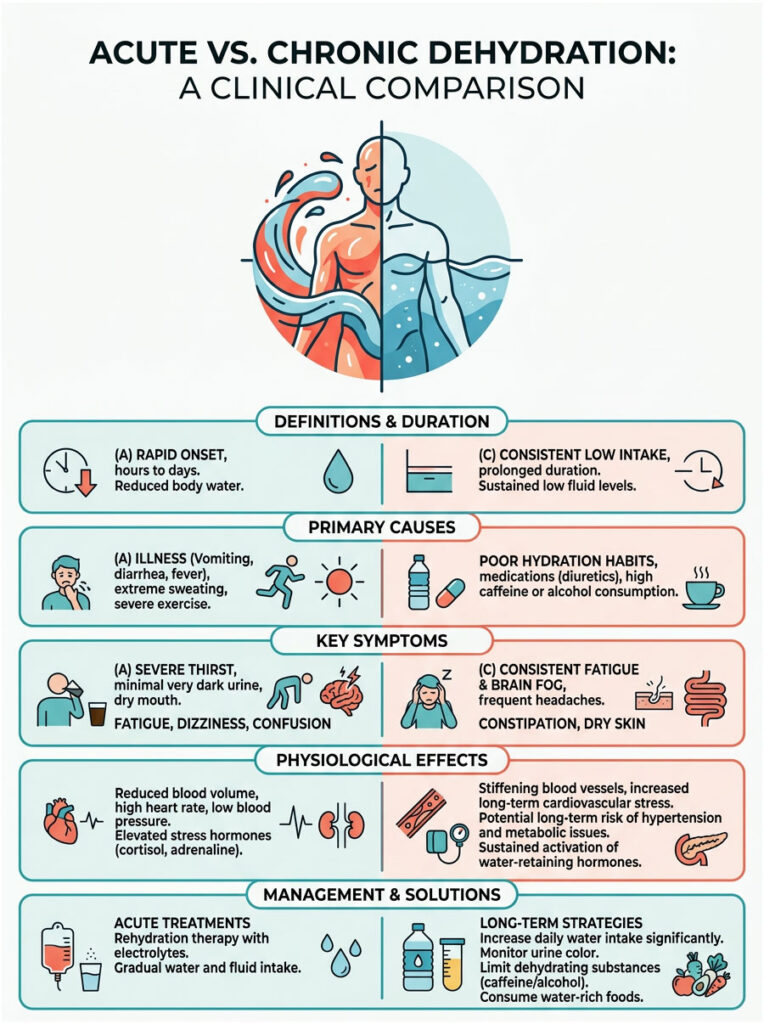
| Clinical Feature | Acute Dehydration | Chronic Suboptimal Hydration |
| Primary Cause | Heavy sweating, illness, heat exposure | Consistently failing to meet daily fluid needs |
| Symptoms | Rapid heart rate, dizziness, dark urine, headache | Brain fog, chronic fatigue, slow BP creep |
| CV Effect | Sudden, sharp systolic spike | Gradual increase in arterial stiffness |
| Hormonal Driver | Massive vasopressin release | Sustained low-grade RAAS activation |
| Treatment | Immediate fluid and electrolyte rescue | Long-term lifestyle and habit changes |
Evidence-Based Hydration Strategies for Blood Pressure Control
Knowing the science is only the first step. The real value is in knowing how to fix the problem. Managing blood pressure through hydration requires a strategic, calculated approach. You cannot simply chug a gallon of water at the end of the day and expect your arteries to heal.
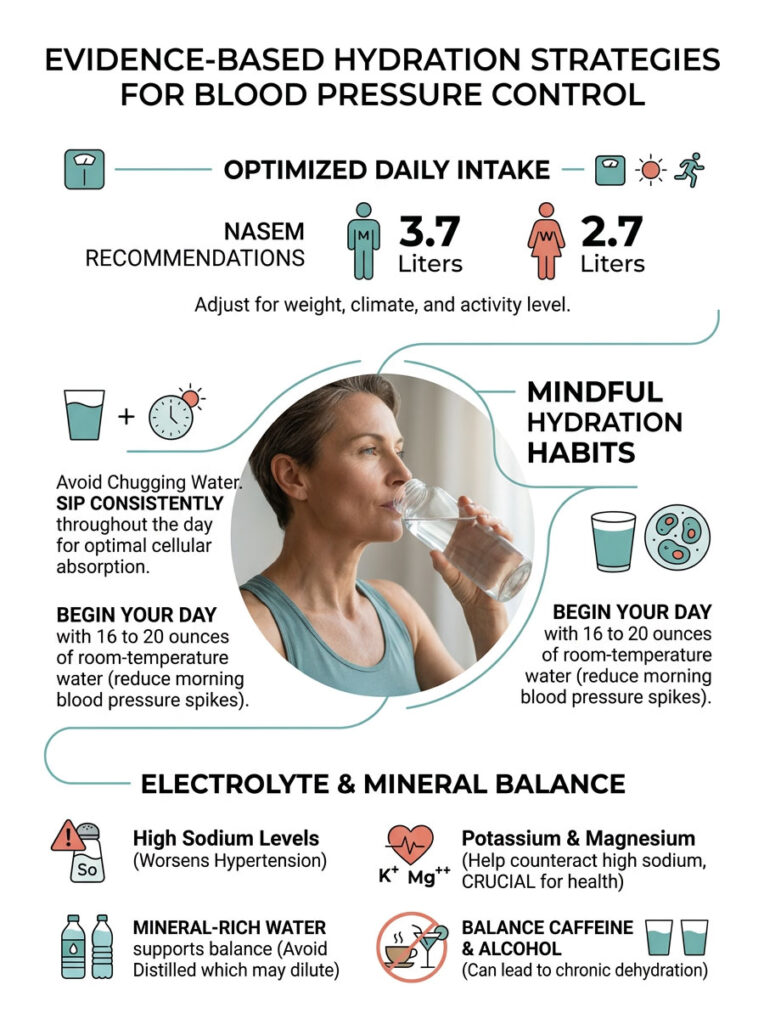
Meeting the NASEM Guidelines
The old “eight glasses a day” rule is not sufficient for cardiovascular management. The National Academies of Sciences, Engineering, and Medicine (NASEM) recommends approximately 3.7 liters (125 ounces) of total daily fluid for men and 2.7 liters (91 ounces) for women. This includes water, healthy beverages, and water-rich foods like fruits and vegetables.
However, this is a baseline for the average sedentary adult. You need to adjust upward based on your weight, climate, and activity level. If you live in a hot, humid environment, invisible sweat loss alone demands significantly more intake. Effective hydration requires daily mindfulness, not guesswork.
Why Electrolytes Matter as Much as Water
Water alone is not enough. Your cardiovascular system runs on electricity, and electrolytes are the conductive minerals that make it work. The link between dehydration and hypertension is heavily influenced by your sodium, potassium, and magnesium levels.
When you are dehydrated, serum sodium concentrates rapidly (hypernatremia). High sodium worsens the hypertensive effect by pulling water out of cells and forcing it into the bloodstream, increasing arterial wall pressure and amplifying Angiotensin II vasoconstriction.
To counteract this, you need adequate potassium and magnesium. These minerals act as natural vasodilators. Potassium helps your kidneys excrete excess sodium. Magnesium relaxes arterial smooth muscle, fighting off endothelial dysfunction. Clinical guidelines for hypertensive patients typically recommend 3,500 to 4,700 milligrams of potassium daily, ideally from dietary sources like spinach, avocados, and bananas.
The Problem with Coffee, Alcohol, and Diuretic Habits
Many of my patients drink coffee all day to fight fatigue. While a cup or two is generally fine, relying on caffeinated beverages as your primary fluid source is a guaranteed path to chronic suboptimal hydration. Caffeine has a well-documented diuretic effect.
Alcohol is even worse. It temporarily suppresses vasopressin release, causing frequent urination. But the next morning, your body rebounds aggressively, triggering a massive vasopressin surge to reclaim lost fluid. This severe rebound leads to morning blood pressure spikes that are strongly correlated with morning strokes and heart attacks. If you drink alcohol, match every serving with a full glass of water.
Mineral Water and Optimal Cellular Absorption
Not all water is created equal for cardiovascular health. Drinking pure distilled water stripped of all minerals can actually dilute your blood’s electrolyte pool, leading to hyponatremia. I recommend mineral-rich water or adding a high-quality, sugar-free electrolyte powder to your daily routine.
Equally important: sip water slowly throughout the day rather than chugging large amounts at once. When you drink 30 ounces in one sitting, your kidneys perceive a sudden fluid overload and flush most of it before it can properly hydrate your tissues. Sipping 4 to 6 ounces every 30 minutes ensures steady cellular absorption and keeps your RAAS cascade suppressed all day.
The Morning Hydration Window: You lose nearly a pound of water overnight through breathing and sweating. You wake up mildly dehydrated every single morning. Before reaching for coffee, drink 16 to 20 ounces of room-temperature water. This immediately suppresses morning vasopressin levels and blunts the natural early-morning rise in blood pressure.
How Dehydration Interacts with Blood Pressure Medications
If you are already taking prescription medication for hypertension, dehydration becomes an even bigger concern. Blood pressure drugs alter your body’s natural fluid and hormonal balance. Mix them with poor hydration, and you can create dangerous physiological conflicts.
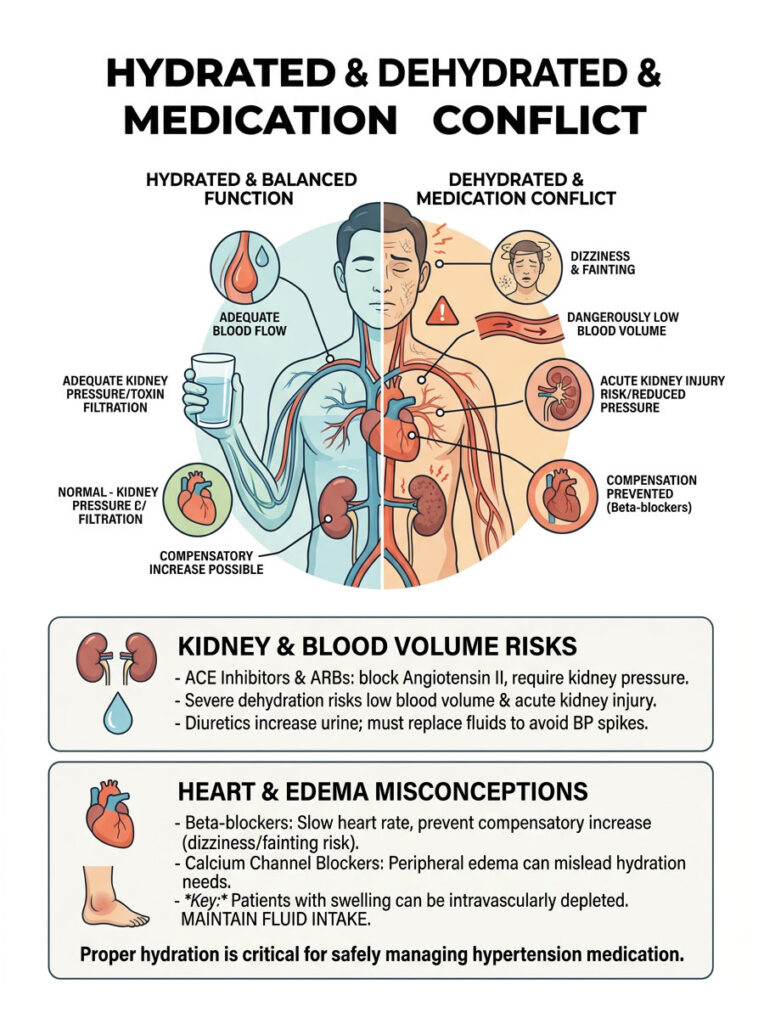
ACE Inhibitors and ARBs
ACE inhibitors (like Lisinopril) and ARBs (like Losartan) lower blood pressure by blocking the RAAS cascade. They prevent Angiotensin II from squeezing your blood vessels. The catch: your kidneys rely on a certain amount of pressure to filter toxins.
If you become severely dehydrated while on these drugs, blood volume drops dangerously low. Because the medication prevents your vessels from constricting to compensate, kidney pressure plummets. This can lead directly to acute kidney injury. Patients on ACE inhibitors or ARBs must be exceptionally careful about maintaining daily water intake.
Beta-Blockers and Heart Rate Compensation
Beta-blockers (like Metoprolol or Atenolol) block adrenaline’s effects on your heart, forcing it to beat slower and with less force. Under normal circumstances, this is great for blood pressure. But during dehydration, your heart naturally tries to beat faster to maintain blood flow to the brain. Beta-blockers prevent this compensatory response.
If a patient on beta-blockers becomes dehydrated in summer heat, their heart literally cannot speed up to compensate. Blood pressure crashes, leading to severe dizziness, fainting, and potential falls. Proper hydration is essential when your heart rate is artificially capped.
Calcium Channel Blockers and Diuretics
Calcium channel blockers (like Amlodipine) relax blood vessels by preventing calcium from entering muscle cells. A common side effect is peripheral edema, or swelling in the ankles and feet. Many patients mistakenly assume they have “too much water” and stop drinking. This is a serious clinical error.
The fluid in swollen ankles is trapped in interstitial tissue, not in the bloodstream. These patients are actually intravascularly depleted, meaning their blood volume is dangerously low despite the visible swelling.
Prescription diuretics (“water pills” like Hydrochlorothiazide) force the kidneys to excrete sodium and water. If a patient on diuretics doesn’t replace the fluid loss, they trigger massive dehydration-induced pressure spikes. The kidneys sense the extreme drop and fight back, rendering the medication useless.
Real-World Cases: Dehydration and Blood Pressure in Practice
Science is fascinating, but clinical application is what saves lives. Here are three scenarios from my own practice that illustrate how dehydration impacts blood pressure in very different ways.
Case 1: The Summer Exercise Spike
John, a 55-year-old with borderline blood pressure, spent a Saturday afternoon landscaping in 92-degree heat for five hours. He drank only two small bottles of water. By 4 PM, he had a pounding headache, racing heart, and dizziness. His wife checked his pressure at home: 175/105.
The physiology was straightforward. Massive fluid loss caused blood volume to plummet. Vasopressin surged. RAAS kicked in with intense vasoconstriction. His heart was hammering at 110 bpm just to push thickened blood through constricted arteries.
We gave him two liters of IV normal saline. No blood pressure medication at all. Within 90 minutes, his heart rate dropped to 72 bpm and his pressure settled back to his normal 128/82. The hormonal alarms shut off the moment fluid volume was restored.
Case 2: The Chronic Coffee Drinker
Sarah, a 45-year-old executive, came in with resistant hypertension. Despite taking a low-dose ACE inhibitor, her readings hovered around 145/90 for over a year. She wanted a stronger prescription.
During our consultation, I asked about her fluid intake. She drank three large coffees each morning, a diet soda at lunch, and maybe one small glass of water at dinner. She rarely felt thirsty. Her BUN-to-creatinine ratio was highly elevated, a classic marker of chronic dehydration.
Instead of increasing medication, I prescribed a strict hydration protocol: 90 ounces of mineral water daily, a sugar-free electrolyte supplement with potassium and magnesium, and cutting coffee to just one cup. Four weeks later, her average readings had dropped to 122/78. We removed the biological stressor driving her hypertension without adding a single pill.
Case 3: The Elderly Patient with Erratic Readings
Robert, a 72-year-old retiree, had wildly unpredictable blood pressure. Mornings: 160/90. Afternoons after standing: 90/60 with severe dizzy spells. His doctor kept adjusting medications with no success.
The problem was simple. Robert’s aging brain had lost its thirst perception. He was drinking less than 30 ounces daily. His stiff arteries could not compensate for the low blood volume. Standing pulled blood into his legs (causing the crashes), and his body would flood the system with adrenaline and vasopressin afterward (causing the spikes).
We put Robert on a “hydration by the clock” schedule: 6 ounces of water every hour, regardless of thirst, plus a slight increase in dietary sodium to help retain fluid. Within two weeks, the erratic swings stabilized completely. Morning spikes and afternoon crashes both disappeared.
Summary and Key Takeaways
Your cardiovascular system is remarkably complex, but it depends on basic fundamentals to stay healthy. The triad of dehydration-induced hypertension involves massive vasopressin release, unrelenting RAAS activation, and dangerous increases in blood viscosity. When you fail to drink enough water, your body will sacrifice long-term arterial health to maintain immediate blood flow to your brain.

- Survival Trumps Health: Your body will always constrict blood vessels and raise pressure to keep you alive during a fluid deficit.
- Hormonal Cascades: Vasopressin and Angiotensin II are powerful vasoconstrictors released when fluid intake falls short.
- Viscosity Matters: Thick, dehydrated blood damages your endothelium, blocks nitric oxide production, and forces your heart to work harder.
- Electrolytes Are Essential: Water needs potassium and magnesium to properly enter your cells and relax arterial walls.
- Medication Risks: Dehydration can cause dangerous interactions with ACE inhibitors, beta-blockers, and diuretics.
Proper hydration is not just about quenching thirst. It is a fundamental, non-pharmacological pillar of cardiovascular disease management. By meeting daily fluid guidelines and maintaining proper electrolyte balance, you protect your endothelium and keep your arteries flexible.
If you are struggling with your numbers, start by paying close attention to your daily water intake. The connection between dehydration and high blood pressure is real, well-documented, and entirely within your power to control. Drink your water, balance your minerals, and protect your heart.
Medical Disclaimer
The information in this article is for educational and informational purposes only and does not constitute medical advice. Always consult with a board-certified cardiologist or your primary care physician before making changes to your hydration routine or medication, especially if you have a history of cardiovascular disease or kidney problems.
Frequently Asked Questions
Can dehydration cause high blood pressure?
Yes, dehydration can lead to high blood pressure through several physiological mechanisms. When the body lacks sufficient fluid, the brain releases vasopressin (anti-diuretic hormone), which causes systemic vasoconstriction. Simultaneously, the kidneys activate the renin-angiotensin-aldosterone system (RAAS), which forces the arteries to narrow and the body to retain sodium, both of which significantly elevate blood pressure readings.
How does blood viscosity affect cardiovascular workload during dehydration?
As fluid levels drop, the concentration of solutes in the blood increases, a state known as high serum osmolality. This makes the blood thicker and more viscous. To move this ‘thick’ blood through the circulatory system, the heart must beat with significantly more contractile force, which directly increases systolic blood pressure and places additional mechanical stress on the arterial walls.
What are the common symptoms of high blood pressure caused by dehydration?
Clinical markers often include a pounding headache, a rapid heart rate (tachycardia), and dark-colored urine. Patients may also experience dizziness or lightheadedness when standing up, known as orthostatic hypotension, as the body struggles to maintain adequate blood flow to the brain despite the systemic vasoconstriction.
Can a small amount of fluid loss impact my blood pressure readings?
Clinical data suggests that a fluid loss of just 2% of total body weight can trigger a significant physiological response, potentially leading to a 15 mmHg increase in systolic blood pressure as the body initiates survival-based vasoconstriction to protect vital organ perfusion.
How does chronic dehydration lead to permanent arterial stiffness?
When the body is in a state of chronic suboptimal hydration, the renin-angiotensin-aldosterone system (RAAS) remains constantly active. This persistent hormonal signaling causes the smooth muscles in the arterial walls to hypertrophy or thicken over time. This leads to a loss of arterial compliance and a permanent increase in Pulse Wave Velocity (PWV), which are hallmarks of chronic hypertension.
Why is potassium essential for managing dehydration-induced hypertension?
Potassium acts as a natural vasodilator and is critical for the function of cellular sodium-potassium pumps. In a dehydrated state, sodium often becomes trapped inside vascular cells, causing them to contract. Adequate potassium intake helps the kidneys excrete excess sodium and allows the blood vessels to relax, counteracting the hypertensive effects of fluid deficits.
Is it dangerous to be dehydrated while taking ACE inhibitors or ARBs?
Yes, it can be clinically dangerous. ACE inhibitors and ARBs block the body’s natural ability to constrict blood vessels to maintain pressure. If you become severely dehydrated while on these medications, your blood volume may drop so low that your kidneys cannot maintain enough filtration pressure, potentially leading to acute kidney injury (AKI).
How do beta-blockers interact with dehydration and heat?
Beta-blockers prevent the heart rate from increasing to compensate for low blood volume. If a patient on beta-blockers becomes dehydrated, their heart cannot speed up to maintain circulation. This often results in a sudden crash in blood pressure, leading to severe dizziness, fainting, or syncopal episodes.
What is the relationship between alcohol consumption and morning blood pressure spikes?
Alcohol is a potent diuretic that suppresses vasopressin, causing rapid fluid loss. However, once the alcohol wears off, the body often experiences a ‘rebound’ effect where it releases massive amounts of vasopressin to conserve water. This hormonal surge leads to significant blood pressure spikes the following morning, increasing the risk of cardiovascular events.
Why do elderly patients experience more erratic blood pressure swings due to dehydration?
Aging often blunts the brain’s thirst perception and reduces the kidneys’ ability to concentrate urine. Furthermore, older adults often have reduced baroreceptor sensitivity. When dehydration occurs, these sensors fail to properly regulate pressure, leading to dangerous fluctuations between high readings and sudden drops when standing.
How much water should I drink daily to support healthy blood pressure?
According to NASEM guidelines, men should aim for approximately 3.7 liters (125 ounces) and women should aim for 2.7 liters (91 ounces) of total daily fluid. This baseline should be adjusted upward based on body weight, activity level, and environmental heat to prevent the activation of hypertensive hormonal cascades.
Does drinking water immediately lower high blood pressure?
In cases of acute dehydration-induced hypertension, rehydrating with water and electrolytes can lower blood pressure relatively quickly by suppressing the release of vasopressin and deactivating the RAAS cascade. However, for chronic hypertension driven by arterial stiffness, long-term consistent hydration is required to improve vascular compliance.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. The relationship between hydration and hypertension is complex and varies by individual. Always consult a qualified healthcare professional or cardiologist before making changes to your blood pressure management plan, fluid intake, or medication schedule.
References
- National Academies of Sciences, Engineering, and Medicine (NASEM) – Dietary Reference Intakes for Water and Electrolytes – Provides the official daily fluid intake standards for men and women.
- American Heart Association (AHA) – Hypertension Journal – Research regarding the role of the Renin-Angiotensin-Aldosterone System in vascular resistance.
- The Lancet – Medical Journal – Clinical studies on vasopressin levels and their direct impact on peripheral vascular resistance during hypovolemia.
- Journal of Hypertension – Clinical Research – Data correlating chronic suboptimal hydration with increased Pulse Wave Velocity and arterial stiffness.
- World Health Organization (WHO) – Cardiovascular Disease Fact Sheets – Statistical data regarding global hypertension risks and lifestyle intervention efficacy.
- National Institutes of Health (NIH) – PubMed Central – Peer-reviewed studies on blood viscosity and its relationship to endothelial dysfunction.





