

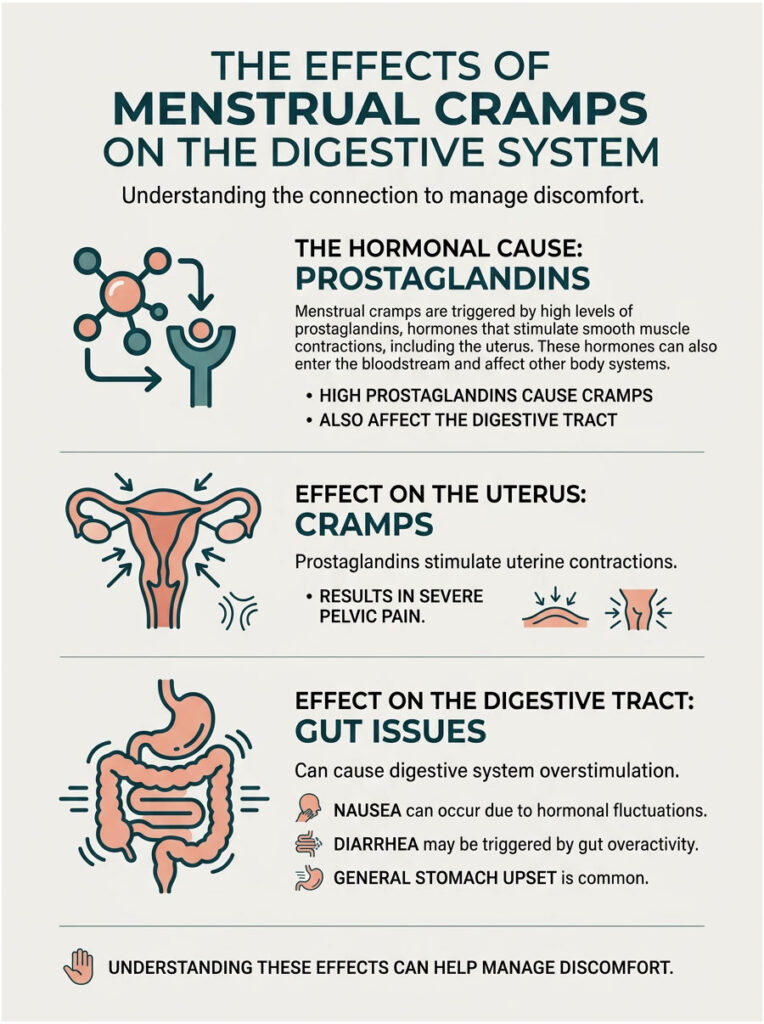
Yes, menstrual cramps can absolutely cause nausea and diarrhea. Your body produces high levels of hormone-like chemicals called prostaglandins right before and during your period. These chemicals force the uterus to contract, but they also spill into the bloodstream and overstimulate your digestive tract. The result is a miserable mix of severe pelvic pain, loose stools, waves of nausea, and general stomach upset.
Table of Contents
Key Statistics on Menstrual Digestive Symptoms
- 73% of menstruating individuals report at least one gastrointestinal symptom before or during their period (BMC Women’s Health, 2014).
- Prostaglandin levels peak roughly 24 to 48 hours before bleeding starts.
- 28% of women say period diarrhea and nausea seriously interfere with work or school.
- About 1 in 10 women have endometriosis, a condition frequently misdiagnosed as irritable bowel syndrome because of overlapping gut symptoms.
- Pre-emptive NSAID therapy reduces primary dysmenorrhea and related bowel problems in up to 80% of cases.
- 15% of women experience significant vomiting during their period due to vagus nerve stimulation.
The Biological Link Between Menstrual Cramps, Nausea, and Diarrhea
Every week, patients walk into my exam room exhausted and frustrated, asking the same question: “Am I actually sick, or is this just my period?” As a Board-Certified OB-GYN with over 15 years of clinical experience, I hear this concern more than almost any other.
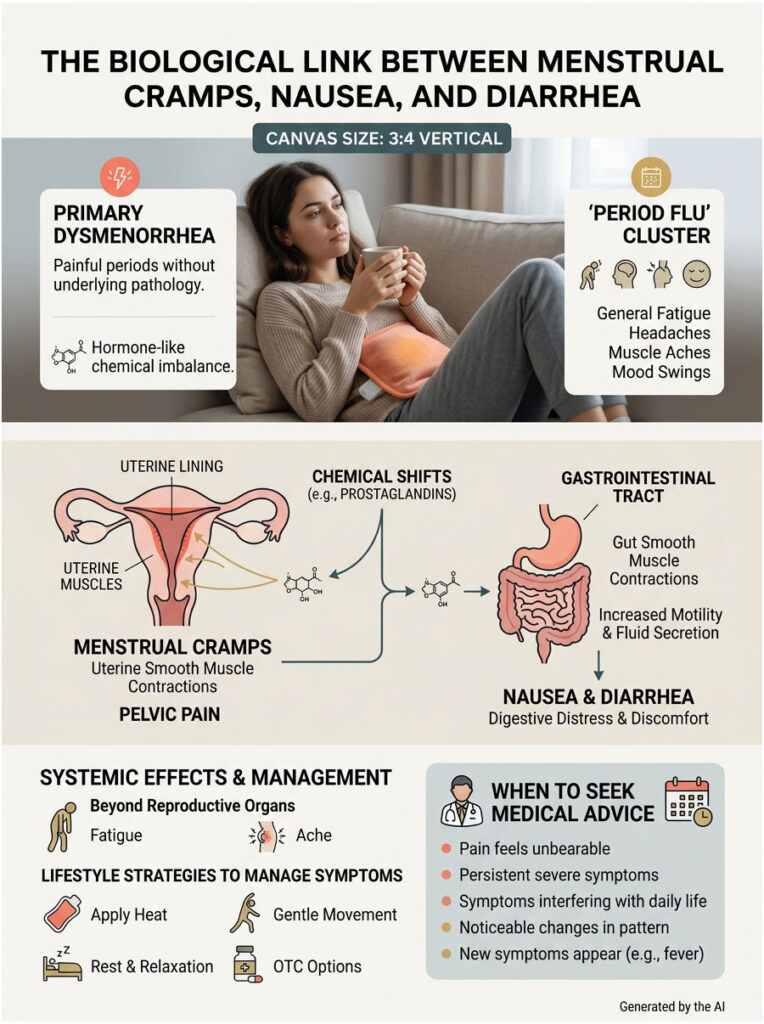
You are not imagining things. The medical community sometimes calls this cluster of symptoms the “period flu,” and it is a real, biologically driven event that hits millions of women each month.
When you have primary dysmenorrhea, which simply means painful periods without an underlying disease, your body goes through intense chemical shifts. That severe pelvic pain is almost always paired with digestive chaos. This is not a coincidence.
Here is what is really going on: cellular compounds escape from the uterus and directly irritate the gut. According to the American College of Obstetricians and Gynecologists (ACOG), the systemic effects of menstruation reach well beyond the pelvis. These powerful chemicals do not stay in one place.
In this guide, we will break down exactly why your digestive system goes haywire during your cycle, look at the hard science behind period diarrhea and nausea, and share evidence-based strategies that can help you take back your month.
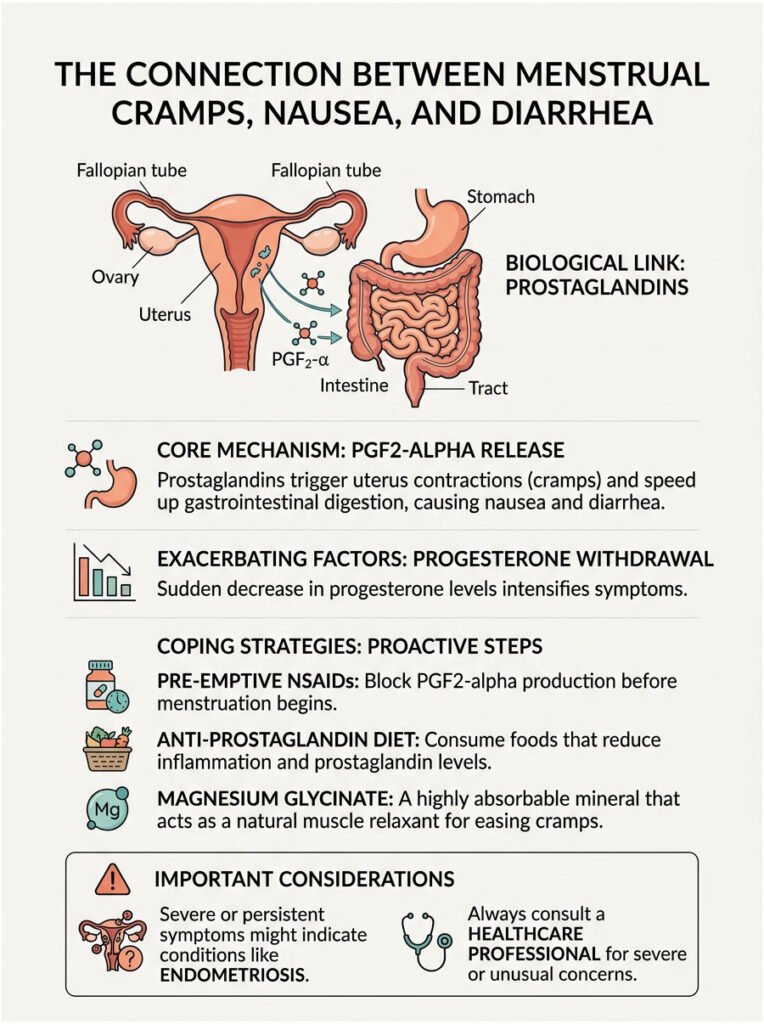
What Are Prostaglandins and PGF2-alpha?
To understand why your stomach hurts as much as your pelvis, you need to look at the cellular level. The reproductive system and the gastrointestinal tract sit very close together inside the abdomen. But their strongest connection is chemical, not just physical.
Every month, the endometrium (the inner lining of the uterus) prepares for a possible pregnancy. When pregnancy does not happen, the body needs to shed this lining efficiently. To get the job done, endometrial cells produce specialized lipid compounds called prostaglandins.
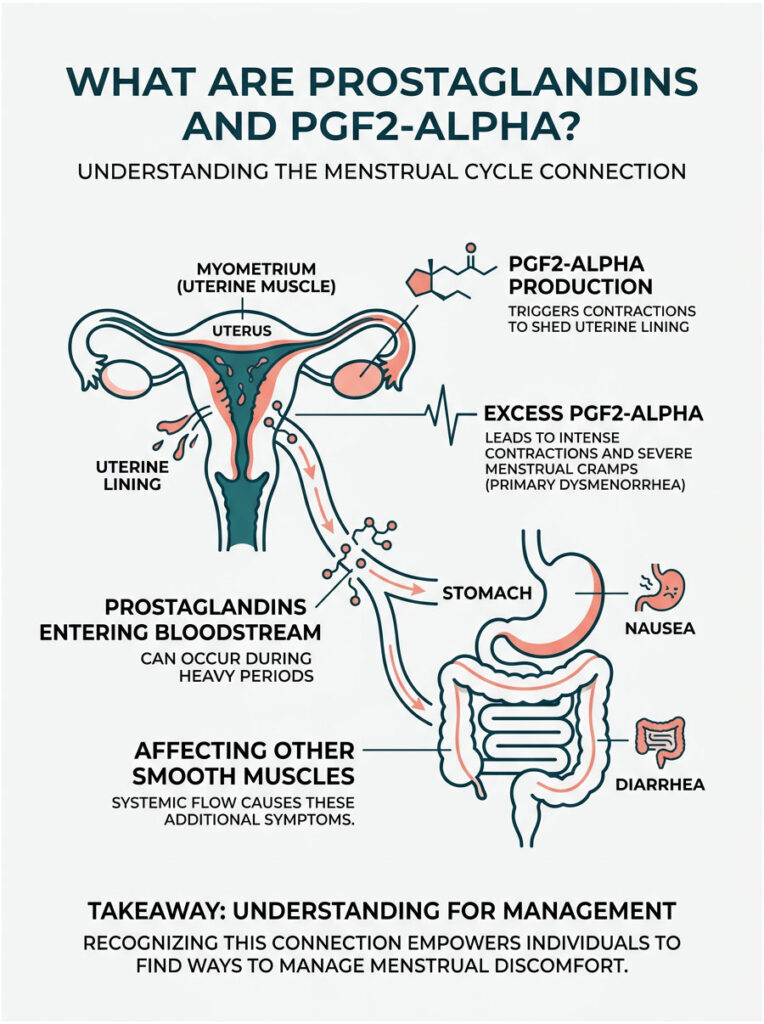
There are many types of prostaglandins in the body, but one dominates the menstrual cycle: Prostaglandin F2-alpha (PGF2-alpha). It is an extremely powerful inflammatory mediator. Its main job is to make the myometrium, the thick muscular wall of the uterus, contract and squeeze. These contractions compress blood vessels in the uterus and temporarily cut off the oxygen supply to the tissue.
That oxygen loss lets the uterine lining detach and shed normally. This is the root biological cause of primary dysmenorrhea. When your body produces unusually high levels of PGF2-alpha, your cramps become severe and debilitating.
How Prostaglandins Escape the Uterus
The contractions get so intense that they cause significant, stabbing pain in the lower pelvis. But the story does not end there. These chemicals do not just stay inside the uterus where they belong.
During a heavy or especially painful period, the endometrium produces an overwhelming amount of PGF2-alpha. The uterus simply cannot contain all of it. The excess spills into the systemic bloodstream.
Once in the blood, PGF2-alpha travels throughout the entire body. It specifically targets smooth muscle tissue wherever it can find it. Your uterus is made of smooth muscle, but so are your intestines, your colon, and your stomach lining.
Patients are often stunned when I explain this in clinic. The exact same chemical that is causing uterine cramps is literally squeezing the intestines at the same time. That is why primary dysmenorrhea rarely happens in isolation.
The systemic circulation of PGF2-alpha makes sure your whole lower abdomen feels the effects. This chemical escape is the core reason why period diarrhea and nausea happen together so often. Your gut is simply reacting to the inflammatory signals it is receiving from the bloodstream.
Why Menstrual Cramps Cause Diarrhea: The Lower Gut Reaction
Now that the chemical triggers are clear, let us look at exactly what happens in the lower digestive tract. Many patients feel embarrassed to bring up their bowel habits. But as a doctor, I want you to know this is entirely normal and very treatable.
For most patients, the lower GI issues are their biggest complaint. The sudden, unpredictable shift in bowel habits can derail daily life and work routines completely.
The “Period Poops” Phenomenon
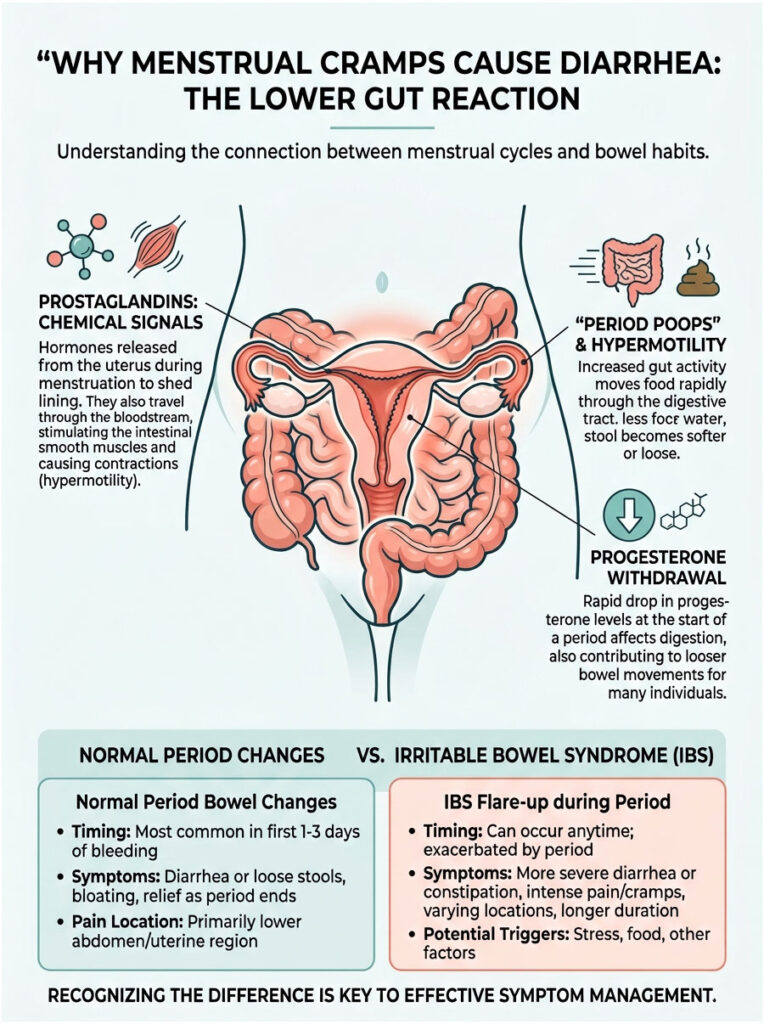
The internet calls this “period poops,” but the medical reality is genuinely interesting. Prostaglandins cause a condition called hypermotility, meaning the digestive tract moves much faster than its normal pace.
When PGF2-alpha binds to smooth muscle receptors in the gastrointestinal tract, it forces the intestines to contract rapidly. Under normal conditions, the colon absorbs water from waste as it moves slowly through the system. That slow process creates solid, well-formed stools.
But with prostaglandins flooding the system, waste moves far too quickly. The colon does not have time to absorb the necessary water. The result? Loose, watery, and urgent stools.
This rapid transit time is a hallmark of primary dysmenorrhea. The more PGF2-alpha your body produces, the worse your period diarrhea will be. It is a direct dose-response relationship.
Progesterone Withdrawal Diarrhea
Prostaglandins are not the only culprit. Shifting hormone levels, especially progesterone, also play a major role. Progesterone withdrawal diarrhea is common, yet rarely discussed.
In the two weeks before your period, progesterone levels run high. Progesterone is a relaxing hormone that slows smooth muscle contractions, which often leads to that frustrating premenstrual constipation many women recognize.
Right before your period, progesterone drops sharply. That sudden fall removes the “brakes” from your digestive system all at once. This rebound effect is what doctors call progesterone withdrawal diarrhea.
When you combine progesterone withdrawal with active PGF2-alpha stimulation, you get a perfect storm. Your gut is being told to speed up while simultaneously losing its ability to slow down. That dual action is exactly why period diarrhea hits so hard.
Normal Period Bowel Changes vs. Irritable Bowel Syndrome
It can be tough to tell if your symptoms are just a rough period or something more chronic. Many women spend years assuming they have a bowel disorder when it is actually their cycle. Here is a comparison to help clarify the differences.
| Feature | Normal Hormonal Diarrhea | IBS Flare-up |
| Timing | Starts 24-48 hours before bleeding, lasts up to day 3. | Can happen anytime, but often worsens during menstruation. |
| Main Trigger | PGF2-alpha excess and progesterone withdrawal. | Food triggers, stress, and cross-organ sensitization. |
| Pain Location | Lower central pelvis, radiating to lower back and rectum. | Generalized abdominal cramping, often relieved by defecation. |
| Stool Changes | Loose, frequent, watery stools tied to heaviest bleeding days. | Alternating between constipation and explosive diarrhea. |
| Duration | Resolves naturally by day 4 as prostaglandins drop. | Chronic, lifelong condition needing ongoing management. |
If your symptoms match the middle column closely, standard hormonal fluctuations are likely to blame. But if symptoms persist well after your period ends, it is time to look deeper. Many patients actually deal with both conditions at once, since menstrual inflammation can trigger a dormant IBS flare-up.
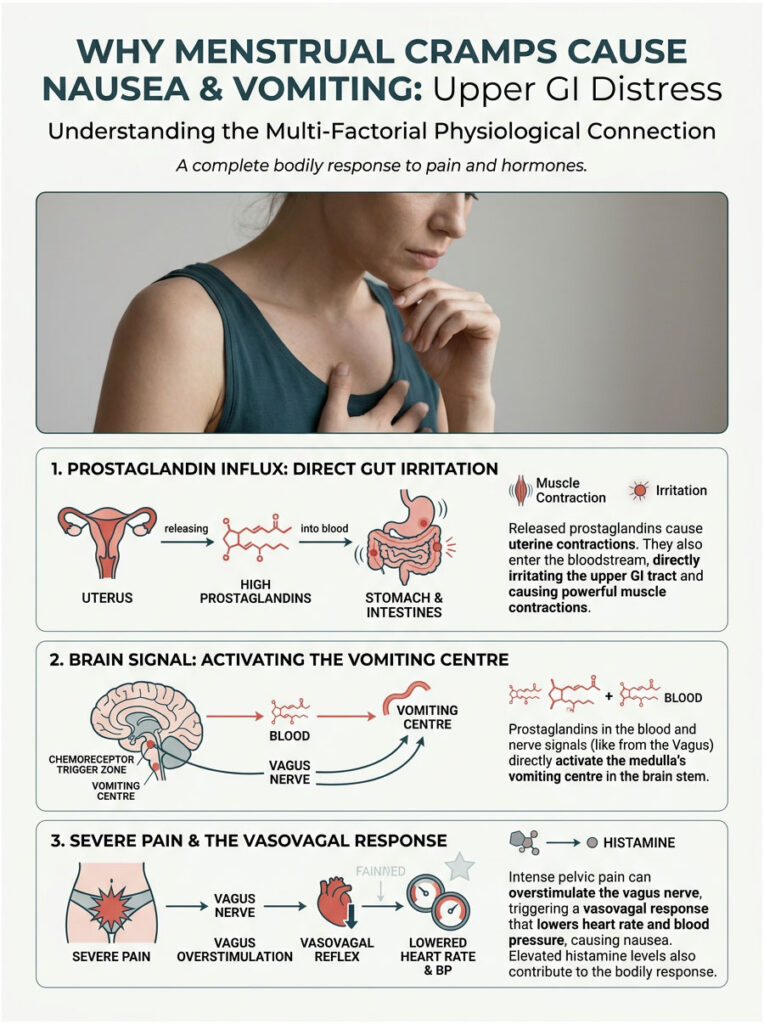
Why Menstrual Cramps Cause Nausea and Vomiting: Upper GI Distress
We have covered the lower digestive tract, but what about the upper half? Many patients feel a deep, paralyzing wave of sickness in the stomach during their cycle. For a lot of women, the nausea is actually the most debilitating part.
Period diarrhea and nausea tend to show up at the same time because they share the same root triggers. You are not catching a bug every month; your body is reacting to an internal chemical flood.
How Prostaglandins Affect the Stomach
Just as PGF2-alpha travels to the intestines, it also reaches the stomach. The stomach lining is highly sensitive to inflammatory chemicals in the blood. When PGF2-alpha hits the stomach lining, it causes immediate, localized irritation.
On top of that, this chemical can directly stimulate the brain’s chemoreceptor trigger zone, which is essentially the body’s master vomiting center. When it detects high levels of inflammatory chemicals in the blood, the brain assumes you have ingested something dangerous.
The brain responds defensively by triggering nausea to stop you from eating anything else. In severe cases, it triggers vomiting to expel the “toxin.” That is why primary dysmenorrhea so often comes with a complete loss of appetite.
The Vasovagal Response to Severe Pain
There is another, more neurological reason for upper stomach upset: the vasovagal response. This reaction proves that period pain is a whole-body event, not just a pelvic issue.
The vagus nerve is a large, complex cranial nerve that runs from the brain, through the chest, and down into the abdomen. It controls resting heart rate, blood pressure, and involuntary digestion. When you experience severe, stabbing pelvic pain, the sheer intensity can overstimulate this nerve.
That overstimulation causes a sudden drop in heart rate and blood pressure. You might experience cold sweats, dizziness, ringing in the ears, and overwhelming nausea. In my practice, I regularly see patients who actually faint from this response.
This nervous system reaction is exactly why period diarrhea and nausea are so tightly connected. Your brain, nerves, and gut are all caught in the crossfire of uterine cramps.
Histamine and Menstrual Nausea
Histamine also plays a role. During menstruation, the body releases higher levels of histamine alongside prostaglandins. Elevated histamine can cause systemic inflammation, headaches, fatigue, and deep nausea.
The stomach lining has specific histamine receptors that, when activated, increase stomach acid production. That excess acid can make you incredibly nauseous, particularly on an empty stomach.
When you combine excess stomach acid, vagus nerve stimulation, and prostaglandin-triggered brain signals, the nausea becomes severe. This triad of upper GI distress explains why even sipping water can make you feel like throwing up. It is a complex biochemical cascade that often needs targeted intervention to resolve.
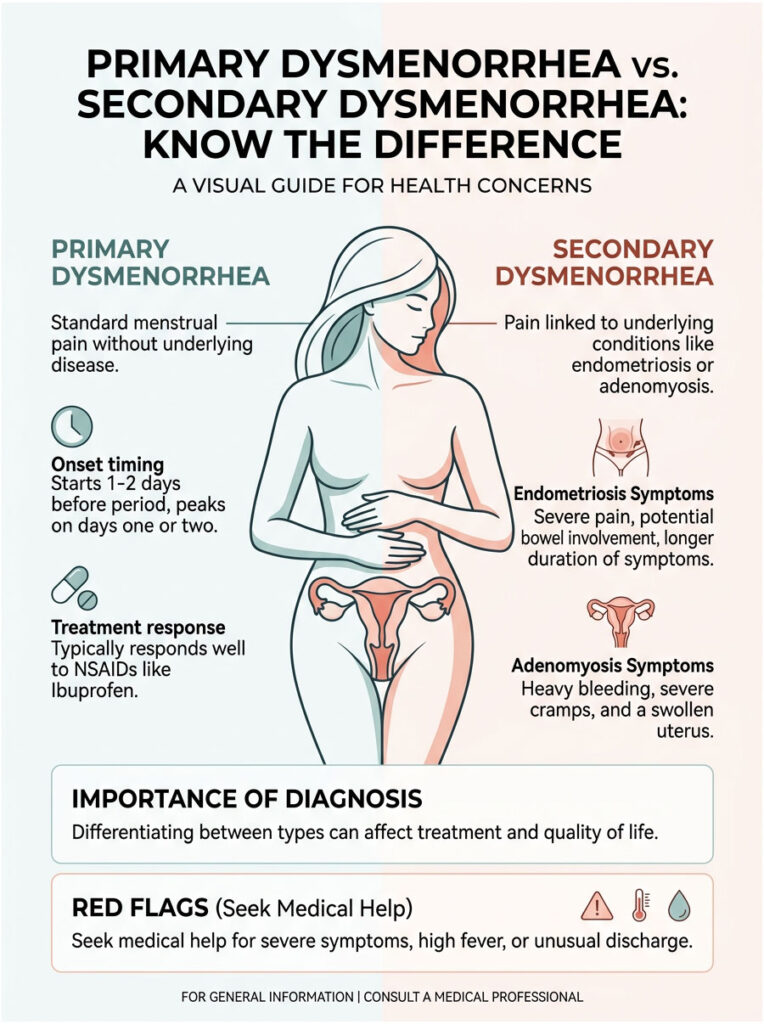
Primary Dysmenorrhea vs. Secondary Dysmenorrhea: Know the Difference
While these symptoms are common, there is a line where they cross into dangerous territory. Understanding the difference between normal chemical reactions and underlying pelvic pathology is vital. Ignoring red flags can mean years of unnecessary suffering.
What Is Primary Dysmenorrhea?
Primary dysmenorrhea is standard menstrual pain that occurs without any underlying pelvic disease. It is simply the result of your body producing too much PGF2-alpha. There is no structural damage or disease process going on.
With primary dysmenorrhea, pain usually starts a day or two before your period, peaks on day one or two, and then gradually fades. Period diarrhea and nausea follow the same predictable timeline each month. This condition usually responds very well to basic medical treatments.
When Could It Be Endometriosis?
Endometriosis is a chronic condition where tissue similar to the uterine lining grows outside the uterus. It affects roughly 1 in 10 women, yet takes an average of seven years to be properly diagnosed.
The key differences lie in the location, duration, and severity of pain. Rogue endometrial tissue can grow on the ovaries, fallopian tubes, pelvic floor, and even the bowels. During your period, this misplaced tissue also produces PGF2-alpha and tries to bleed.
Because there is no natural exit for this blood, it creates severe internal inflammation. If you have bowel endometriosis, the prostaglandin effects on your bowels are magnified dramatically. You might experience excruciatingly painful bowel movements, visible rectal bleeding, or chronic pelvic pain that lingers long after your period ends.
Endometriosis requires specialized care, often including excision surgery. Primary dysmenorrhea, on the other hand, is usually managed with medication and lifestyle adjustments.
The Threat of Adenomyosis
Another frequently overlooked condition is adenomyosis. While endometriosis involves tissue growing outside the uterus, adenomyosis involves tissue growing deep into the uterine muscle wall. This creates a bulky, enlarged, and highly inflamed uterus.
Women with adenomyosis often experience incredibly heavy, prolonged bleeding alongside severe cramps. The uterine muscle is essentially infiltrated by bleeding tissue, so contractions are extremely strong, flooding the bloodstream with prostaglandins.
The resulting period diarrhea and nausea can be incapacitating. Patients often describe it as a “heavy, dragging” sensation radiating down their thighs. If your uterus feels chronically tender and swollen, adenomyosis should be investigated with ultrasound or MRI.
Cross-Organ Sensitization and Pelvic Inflammatory Disease
Because the pelvic organs and the gut share the same nerve pathways, chronic inflammation in one organ can make the adjacent organ hypersensitive. They essentially share the same neurological switchboard.
For example, chronic pelvic pain can leave your gut nerves permanently sensitized. Even normal digestion can feel painful during your period. It becomes a vicious feedback loop of pain and inflammation.
We must also rule out Pelvic Inflammatory Disease (PID) when symptoms are severe. PID is a serious bacterial infection of the reproductive organs requiring immediate antibiotics. If your period diarrhea and nausea come with a high fever, unusual vaginal discharge, or pain during urination, seek emergency medical attention right away.
Primary vs. Secondary Dysmenorrhea: Symptom Comparison
| Factor | Primary Dysmenorrhea | Secondary Dysmenorrhea |
| Onset | Starts 1-2 days before or at the beginning of bleeding. | Pain may start weeks before and linger after bleeding stops. |
| NSAID Response | Usually responds well to Ibuprofen or Naproxen. | Often resistant to standard over-the-counter pain relief. |
| GI Severity | Mild to moderate nausea, a few days of loose stools. | Extremely painful bowel movements, rectal bleeding, or severe vomiting. |
| Daily Impact | Manageable with heat, rest, and basic medication. | Frequently causes missed work, school, or requires bed rest. |
| Root Cause | Excess PGF2-alpha during normal lining shedding. | Structural issues like fibroids, adenomyosis, or endometrial lesions. |
Bring this information to your next gynecologist appointment. Pointing out exactly where your symptoms fall can help your doctor understand the real severity. Do not let anyone dismiss secondary symptoms as “just bad cramps.”
The Psychological Toll of Severe Menstrual Symptoms
We have covered the physical biology in depth, but the mental toll deserves attention too. Dealing with severe period diarrhea and nausea every single month is psychologically exhausting. The anticipation alone can create real anxiety.
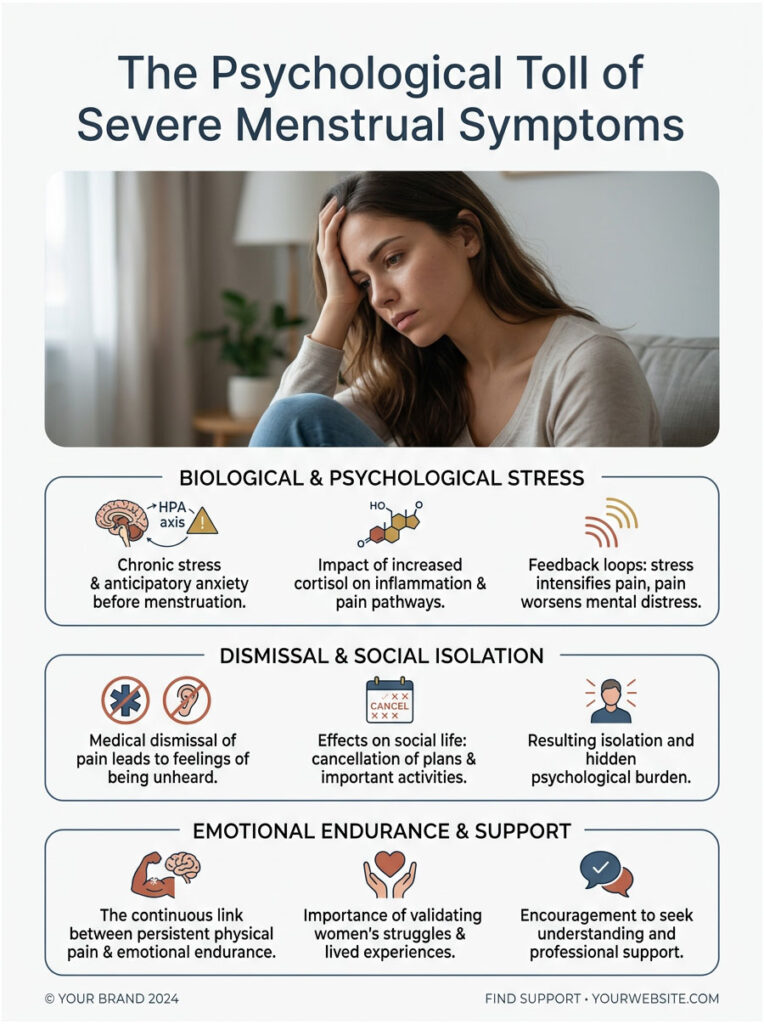
Many women develop what is called anticipatory anxiety in the week before their period. They know the chemical storm is coming and feel powerless. That chronic stress raises cortisol levels, which can paradoxically worsen inflammation and pain.
On top of that, the medical dismissal of women’s pain is a well-documented problem. For decades, women have been told that severe menstrual pain is normal, or that it is “all in their heads.” Being repeatedly brushed off by doctors leads to isolation and depression.
When you are constantly worried about needing sudden bathroom access, your social life takes a hit. You might cancel plans, skip the gym, or call in sick out of sheer embarrassment. The disruption to your professional and personal life is real and deeply unfair.
Acknowledging this psychological burden matters. You are not weak for struggling with these symptoms. Validating the physical pain also validates the emotional endurance it takes to live with it month after month.
Clinical Case Studies: How These Symptoms Play Out in Real Life
To see how these biological mechanisms look in practice, here are three blinded clinical examples from my practice. These case studies show how we systematically approach severe menstrual GI symptoms.
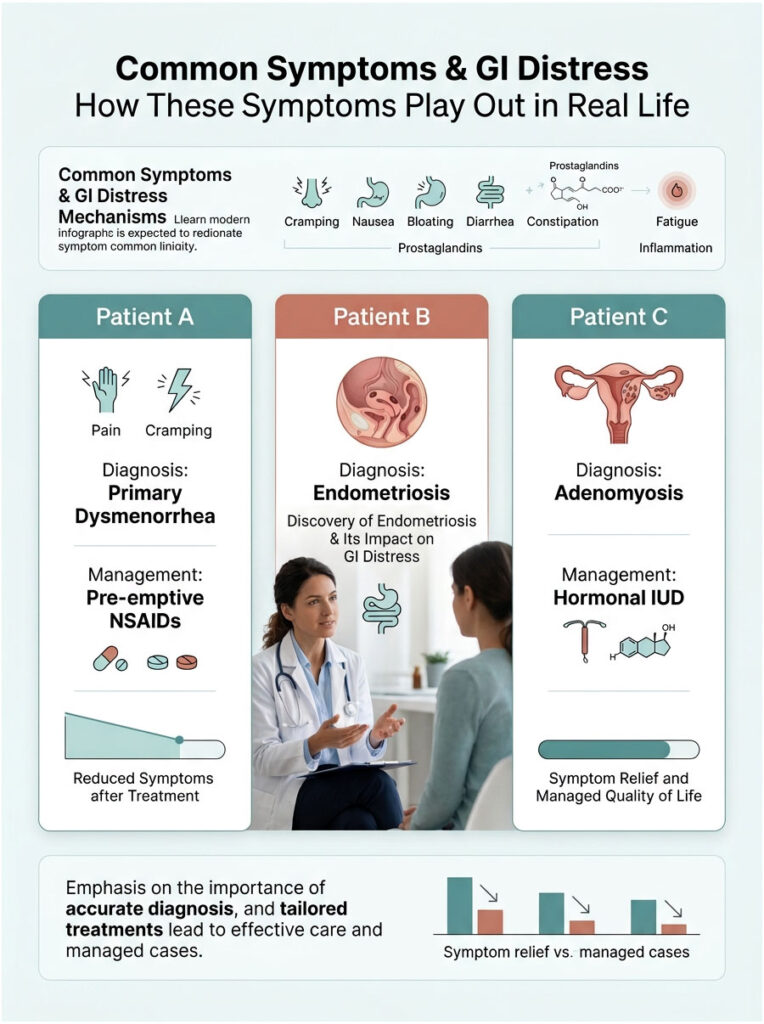
Case 1: Severe GI Distress Managed with Pre-emptive NSAIDs
Patient A, a 24-year-old teacher, came to my clinic nearly in tears. She missed at least one day of work every month because of explosive diarrhea and nausea during her period. She genuinely believed she just had a weak stomach.
Her evaluation revealed classic, textbook primary dysmenorrhea. Pain started exactly on day one, accompanied by dizziness from a vasovagal response. Her progesterone withdrawal diarrhea was severe, lasting precisely 48 hours before clearing up.
I explained the role of PGF2-alpha and started her on a strict 48-hour pre-emptive NSAID protocol with Ibuprofen 600mg. Instead of waiting for the pain to hit, she began the medication two full days before her expected period.
The results were life-changing. By blocking PGF2-alpha production before it could peak, we eliminated the prostaglandin effects on her bowels entirely. She reported a 90% reduction in diarrhea and nausea within the very first cycle.
Case 2: Uncovering Hidden Endometriosis
Patient B, a 31-year-old accountant, had a very different story. Her timeline raised immediate red flags for secondary dysmenorrhea. She felt like she had severe food poisoning for a full week before her period even started.
Her deep pelvic pain did not respond to high-dose NSAIDs. She experienced sharp pain during intercourse, and bowel movements were excruciatingly painful, not just loose. I suspected cross-organ sensitization was hiding a deeper structural issue and referred her for specialized laparoscopic evaluation.
The surgeon found deep infiltrating endometriosis growing on her rectum and pelvic floor. Her symptoms were the direct result of endometrial tissue bleeding onto her bowels. After surgical excision, her severe GI distress resolved completely. This case is a clear example of why proper diagnosis matters.
Case 3: Adenomyosis Treated with a Hormonal IUD
Patient C, a 40-year-old mother of two, had heavy, dragging pelvic pain alongside relentless nausea. Her bleeding was so heavy she was becoming clinically anemic. Ultrasound showed a bulky, enlarged uterus consistent with adenomyosis.
Her uterine muscle was thick and inflamed, pumping out massive amounts of prostaglandins. Oral medications could not penetrate the tissue effectively. We placed a Levonorgestrel-releasing intrauterine device (IUD).
The hormonal IUD delivered progesterone directly to the uterine lining, thinning it out drastically over three months. With less tissue to shed, prostaglandin production plummeted. Her heavy bleeding stopped, and her monthly nausea and diarrhea disappeared.
Evidence-Based Strategies for Relief: Taking Back Your Month
Now for the part that matters most: what you can actually do about it. You do not have to suffer through period diarrhea and nausea in silence every month. Here are expert-approved strategies based on real clinical guidelines.

My approach with patients always starts with building a customized, multi-modal treatment plan. We want to target PGF2-alpha from multiple angles at once.
The Pre-emptive NSAID Protocol
The most effective first-line treatment for primary dysmenorrhea is proper use of NSAIDs like Ibuprofen, Naproxen, or Celecoxib. But the vast majority of people take them incorrectly.
NSAIDs are not just pain maskers. They are active prostaglandin inhibitors. They work by blocking the enzyme cyclooxygenase (COX), which your body uses to manufacture PGF2-alpha.
Expert Tip: Do not wait for the pain to start. Begin taking NSAIDs 24 to 48 hours before your expected period. By the time cramps begin, your body has already flooded your system with PGF2-alpha. Pre-emptive dosing stops production before it peaks, drastically reducing the prostaglandin effects on your bowels.
If you wait until you are already experiencing period diarrhea and nausea, the NSAIDs take much longer to work. The inflammatory chemicals are already circulating. You need to stay ahead of the chemical curve.
Hormonal Interventions and Birth Control
If NSAIDs are not enough, hormonal birth control is often the next step. Oral contraceptive pills, hormonal IUDs, patches, and vaginal rings are highly effective at managing primary dysmenorrhea because they alter the fundamental biology of your cycle.
These methods work by preventing ovulation and thinning the endometrium. A thinner uterine lining means significantly less tissue available to produce PGF2-alpha. It is a straightforward issue of volume reduction.
Continuous birth control methods can also stabilize hormone levels completely, preventing the sudden progesterone drop that triggers withdrawal diarrhea in the first place.
Dietary Adjustments: The Anti-Prostaglandin Diet
What you eat directly affects how much inflammation your body produces. I recommend patients adopt an anti-prostaglandin diet in the week leading up to their period.
This means reducing foods that promote inflammation: refined sugars, red meat, heavily processed foods, and saturated fats. Instead, load up on Omega-3 fatty acids found in wild-caught salmon, walnuts, and chia seeds. Omega-3s naturally inhibit inflammatory prostaglandin production by competing with Omega-6 fatty acids, essentially acting as a natural COX inhibitor.
You should also adjust fiber intake strategically. To combat progesterone withdrawal diarrhea, increase soluble fiber from sources like oats, applesauce, and bananas. Soluble fiber absorbs excess water in the gut and helps firm up loose stools.
Magnesium Supplementation for Period Cramps
Using magnesium for period cramps is one of the most effective evidence-based natural interventions. Magnesium works as a natural smooth muscle relaxant and mild antispasmodic.
By relaxing the myometrium, magnesium reduces the severity of uterine contractions. It also helps calm the nervous system, which can directly counter the vasovagal response causing dizziness and nausea.
Be careful about the type you choose. Magnesium citrate pulls water into the bowels and can make period diarrhea worse. I recommend Magnesium Glycinate instead. It provides the muscle relaxation benefits with optimal absorption and zero laxative effect. Taking 300mg to 400mg daily in the week before your period can make a significant difference.
Heat Therapy and TENS Machines
Do not underestimate external physical therapies. Applying continuous heat to the lower abdomen increases pelvic blood flow, which helps flush accumulated prostaglandins from uterine tissue faster.
Transcutaneous Electrical Nerve Stimulation (TENS) machines are also excellent tools. These small devices send mild electrical pulses through the skin that block pain signals from reaching the brain, providing immediate, drug-free relief.
Combining a TENS machine with a heating pad and pre-emptive NSAIDs creates a powerful triad of relief. It tackles pain neurologically, physically, and chemically all at once. This multi-modal approach is the gold standard for period pain management.
Long-Term Management and When to Consider Surgery
For some women, lifestyle changes and basic medications are simply not enough. If you have tried the pre-emptive NSAID protocol, dietary changes, and hormonal management without meaningful improvement, it is time to escalate your care. Chronic, debilitating pain is never something you should just accept.
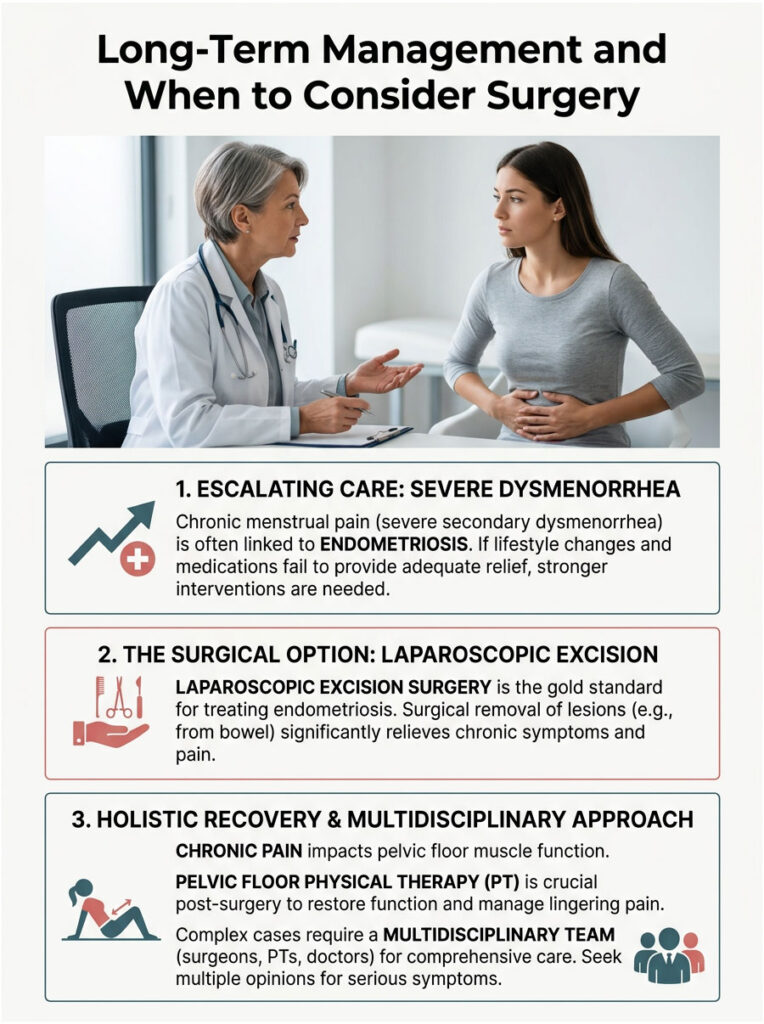
If severe secondary dysmenorrhea is suspected, particularly endometriosis, surgery may be appropriate. Laparoscopic excision surgery is currently the gold standard for diagnosing and treating endometriosis. A skilled specialist can physically remove the inflammatory lesions from the pelvis and bowels.
For patients with bowel endometriosis, this surgery can completely resolve chronic period diarrhea and nausea. It is a major procedure, but the quality of life improvement is often remarkable.
Post-surgery, or as an alternative, pelvic floor physical therapy is extremely beneficial. Years of chronic pelvic pain cause the pelvic floor muscles to tighten and spasm. A specialized therapist can release these trigger points, dramatically improving painful bowel movements and general comfort.
Complex cases require a multidisciplinary team. You may need to work with an OB-GYN, a gastroenterologist, and a pelvic pain specialist simultaneously. Do not hesitate to seek a second or third opinion if your current doctor is not taking your GI symptoms seriously.
Summary and Key Takeaways
We started with a simple but important question: can menstrual cramps cause nausea and diarrhea?
Yes, they absolutely can. This is a well-documented, biologically driven process that affects millions of women. You are not imagining things, and your symptoms are completely valid.
The core issue is the systemic release of PGF2-alpha. This inflammatory chemical escapes the uterus and wreaks havoc on the gastrointestinal tract, speeding up digestion, triggering the vomiting center in the brain, and overstimulating the vagus nerve. Combine that with sudden progesterone withdrawal, and it is no wonder so many women feel like they have the stomach flu every month.
The bottom line: You do not have to accept this as your normal. Start with the pre-emptive NSAID strategy to block PGF2-alpha before it peaks. Adopt an anti-prostaglandin diet and try Magnesium Glycinate to relax smooth muscle naturally.
If your symptoms stubbornly persist, or if your pain profile looks more like secondary dysmenorrhea, seek a professional medical evaluation. Understanding the difference between normal cramps and conditions like endometriosis is essential for protecting your long-term health.
Now you know the answer to “can menstrual cramps cause nausea and diarrhea,” and you know exactly what steps to take.
Frequently Asked Questions
Why do I get diarrhea every time I start my period?
This phenomenon, often called ‘period poops,’ is caused by high levels of Prostaglandin F2α (PGF2α). While these chemicals are meant to contract your uterus, they often escape into the bloodstream and target the smooth muscles of your intestines. This leads to hypermotility, where your colon moves waste too quickly to absorb water, resulting in loose, urgent stools.
Can menstrual cramps actually cause severe nausea and vomiting?
Yes. Systemic prostaglandins can irritate the stomach lining and stimulate the brain’s chemoreceptor trigger zone, which is the body’s master vomiting center. Additionally, the intense pelvic pain of primary dysmenorrhea can trigger a vasovagal response, overstimulating the vagus nerve and causing sudden nausea, dizziness, and cold sweats.
What exactly is the ‘period flu’?
The ‘period flu’ is an informal term used by medical professionals to describe a cluster of systemic symptoms including nausea, diarrhea, fatigue, and muscle aches that occur just before or during menstruation. It is not a viral infection but rather a biological reaction to the inflammatory chemical flood of prostaglandins and sudden hormone shifts.
How does the pre-emptive NSAID protocol help with period-related GI issues?
NSAIDs like Ibuprofen and Naproxen are COX inhibitors that block the production of prostaglandins. By starting these medications 24 to 48 hours before your period begins, you prevent the ‘chemical storm’ from peaking. This significantly reduces the amount of PGF2α available to stimulate both uterine contractions and intestinal hypermotility.
Why does progesterone withdrawal cause bowel changes?
Progesterone is a muscle relaxant that slows down the digestive tract, often causing premenstrual constipation. When levels drop sharply right before your period, the ‘brakes’ are removed from your gut. This sudden withdrawal, combined with the rise of prostaglandins, creates a perfect storm for diarrhea and gastrointestinal distress.
Is it normal to feel dizzy or faint during bad menstrual cramps?
While common, it is a sign of a vasovagal response. The severe, stabbing pain of cramps can overstimulate the vagus nerve, leading to a sudden drop in heart rate and blood pressure. This can cause you to feel nauseous, experience ringing in the ears, or even lose consciousness (fainting).
How can I tell the difference between normal period diarrhea and IBS?
The primary indicator is timing. Hormonal diarrhea typically begins 24-48 hours before bleeding and resolves by day four of your cycle. Irritable Bowel Syndrome (IBS) is a chronic condition with symptoms that occur randomly throughout the month, though many patients find their IBS symptoms flare significantly during their period due to cross-organ sensitization.
Which type of magnesium is best for reducing period cramps and nausea?
I recommend Magnesium Glycinate. It acts as a natural smooth muscle relaxant to calm uterine contractions and the nervous system without the laxative effect found in other forms. You should avoid Magnesium Citrate during your period, as it pulls water into the bowels and can worsen period-induced diarrhea.
Could my severe period nausea and diarrhea be a sign of endometriosis?
It is possible. If your gastrointestinal symptoms are debilitating, involve excruciatingly painful bowel movements, or are resistant to standard NSAIDs, it may indicate bowel endometriosis. This is where endometrial-like tissue grows on the intestines, causing localized inflammation that is much more severe than standard primary dysmenorrhea.
What is ‘cross-organ sensitization’ in the context of period pain?
Because the pelvic organs and the gut share the same neurological ‘switchboard’ or nerve pathways, chronic inflammation in the uterus can make the adjacent intestines hypersensitive. This means that during your period, normal digestive processes can feel painful or cause exaggerated reactions like nausea and cramping.
How does an anti-prostaglandin diet reduce menstrual symptoms?
An anti-prostaglandin diet focuses on Omega-3 fatty acids (found in salmon and walnuts), which naturally inhibit the production of inflammatory chemicals. By avoiding pro-inflammatory triggers like refined sugars and red meat in the week leading up to your period, you can chemically lower the severity of your systemic symptoms.
When should I see a specialist for my menstrual GI symptoms?
You should seek a professional evaluation if your symptoms cause you to miss work or school, if you experience rectal bleeding during your period, or if your pain lasts longer than the first few days of bleeding. These are red flags for secondary dysmenorrhea, such as endometriosis or adenomyosis, which require specialized medical or surgical intervention.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. The biological links between menstruation and gastrointestinal distress discussed are based on clinical experience and research, but individual symptoms vary. Always consult a qualified healthcare professional or OB-GYN before starting new medications, such as pre-emptive NSAID protocols, or if you experience severe, debilitating pelvic pain.
References
- BMC Women’s Health – https://bmcwomenshealth.biomedcentral.com – 2014 study detailing that 73% of individuals experience GI symptoms during menstruation.
- American College of Obstetricians and Gynecologists (ACOG) – https://www.acog.org – Clinical guidelines on the systemic effects of prostaglandins and primary dysmenorrhea management.
- Journal of Clinical Medicine – Publication on the efficacy of NSAIDs as cyclooxygenase (COX) inhibitors for menstrual pain relief.
- Endometriosis Foundation of America – https://www.endofound.org – Statistics and diagnostic criteria for distinguishing secondary dysmenorrhea from normal cramps.
- National Institutes of Health (NIH) – https://www.nih.gov – Research on the role of Magnesium Glycinate as a smooth muscle relaxant in reproductive health.
- International Journal of Molecular Sciences – Study on Prostaglandin F2α (PGF2α) and its direct impact on gastrointestinal hypermotility.





