
A single word on your blood report, something like “poikilocytosis” or “anisopoikilocytosis,” can carry more diagnostic weight than all the numbers stacked above it. The shape of a red blood cell is a fingerprint, and a trained eye reads it like one.
Table of Contents
Most people glance past the smear comment entirely. Yet that one line often tells your provider exactly where to look next, sometimes before any single value on the count looks clearly off.
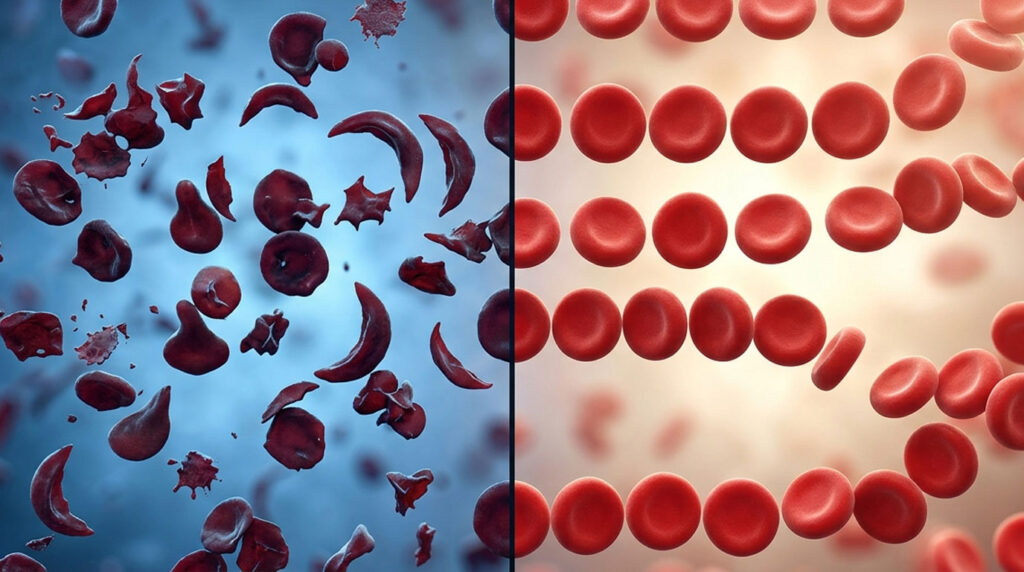
Quick Answer: RBC morphology is the study of the shape, size, color, and internal features of your red blood cells under a microscope. Normal red blood cells are biconcave discs with a pale center. When more than 10% take on abnormal shapes, it’s called poikilocytosis. Abnormal morphology is a clue to an underlying condition such as anemia, a hemoglobin disorder, or liver disease, not a diagnosis on its own.
At a Glance
- Normal red blood cells are uniform biconcave discs about 6 to 8 micrometers wide, with central pallor covering roughly a third of the cell.
- Poikilocytosis means abnormal shapes; anisocytosis means abnormal size variation; the two often appear together.
- Each abnormal shape points toward specific conditions, which is why pathologists call the smear a hematologic fingerprint.
- Schistocytes (cell fragments) can signal a medical emergency and warrant fast evaluation.
- Morphology is read on a peripheral blood smear, where a human reviewer catches what the automated analyzer flags.
- Many abnormal shapes reverse once the underlying cause, like iron deficiency, is treated.
What Is RBC Morphology?
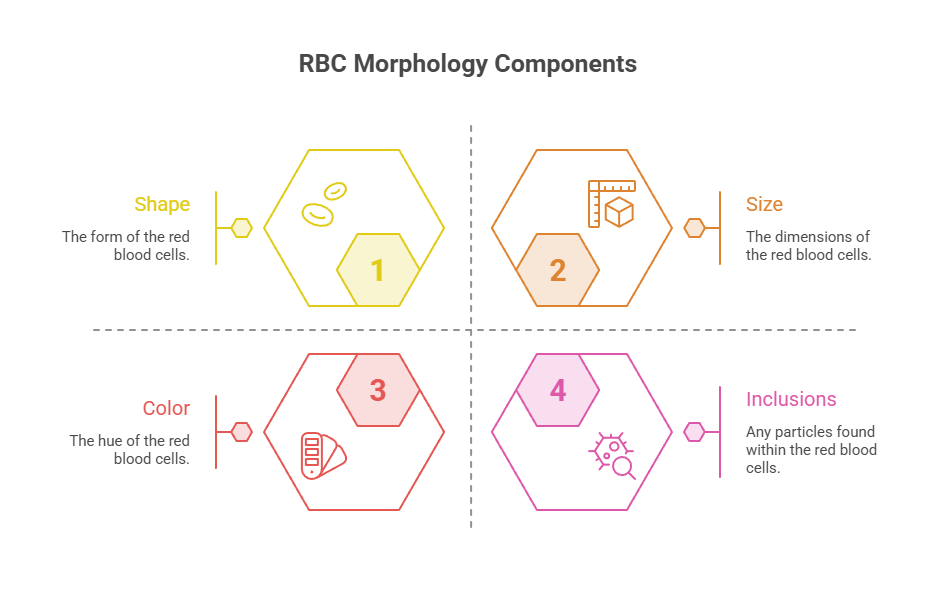
RBC morphology is simply how your red blood cells look under magnification. A lab reviews four things: shape, size, color, and any inclusions sitting inside the cells.
These features matter because a red blood cell’s job depends on its form. The right shape lets it bend through the narrowest capillaries and carry oxygen efficiently from your lungs to your tissues.
Shape, Size, Color, and Inclusions
Shape tells whether cells are round discs or something irregular. Size flags whether they’re too small, too large, or uneven. Color reflects hemoglobin content, and inclusions are tiny structures that shouldn’t normally be there.
Patients reviewing a CBC with us often ask what the smear comment means when their actual cell count looks normal. The answer is that morphology can reveal a problem the raw numbers haven’t fully captured yet.
What a Normal Red Blood Cell Looks Like
Under the microscope, a healthy red blood cell is a round, biconcave disc. According to Cleveland Clinic, normal cells are disk-shaped with a flattened center on both sides.
The pale middle, called central pallor, normally takes up about one-third of the cell’s diameter. A typical red blood cell measures roughly 6 to 8 micrometers across, slightly smaller than a small lymphocyte used for size comparison on the slide.
Why Shape Equals Function
That biconcave shape isn’t an accident. It maximizes surface area for oxygen exchange and gives the cell the flexibility to squeeze through vessels narrower than the cell itself.
When shape changes, function usually suffers. Rigid or fragile cells get trapped and destroyed faster, which is how many abnormal-shape conditions lead to anemia, fatigue, and shortness of breath.
How RBC Morphology Is Assessed
Morphology is read from a peripheral blood smear, a thin film of blood spread on a glass slide and stained so the cells stand out. It remains the foundation of hematology diagnosis.
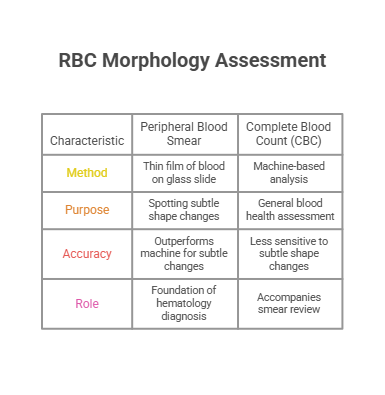
The smear usually accompanies a complete blood count. Patients booking a CBC through HealthCareOnTime are sometimes surprised that a slide reviewed by eye still outperforms the machine for spotting subtle shape changes.
The Peripheral Blood Smear
A drop of blood is spread across a slide and treated with a Wright or Leishman stain, which colors the cells so a reviewer can judge shape, size, and color. The whole preparation takes only minutes.
A pathologist or trained technologist then examines the film under magnification. Per PubMed, the smear lets a reviewer interpret diagnostically meaningful findings in red cell shape, size, color, inclusions, and arrangement.
Analyzer Flags vs Trained Human Review
Modern hematology analyzers count and size cells quickly, and they flag possible abnormalities. They do not reliably name a teardrop cell or distinguish a schistocyte from a bite cell.
That gap is why a flagged sample triggers manual review. Our lab partners report that the analyzer works like a smoke detector, while the human reviewer is the one who walks in and identifies the actual fire.
How Morphology Fits the Full CBC
Morphology is most useful read alongside the numbers. The mean corpuscular volume (MCV) confirms average cell size, and the red cell distribution width (RDW) quantifies how much the sizes vary.
A high RDW lines up with anisocytosis on the smear, while MCV sorts anemia into small-cell, normal-cell, and large-cell types. The shape comments then narrow the cause further. A reticulocyte count adds whether the marrow is responding.
Why Your Doctor Checks RBC Morphology
A smear and morphology review isn’t ordered at random. It’s usually triggered by a clue in your symptoms or an unexpected pattern in your complete blood count that needs a closer look.
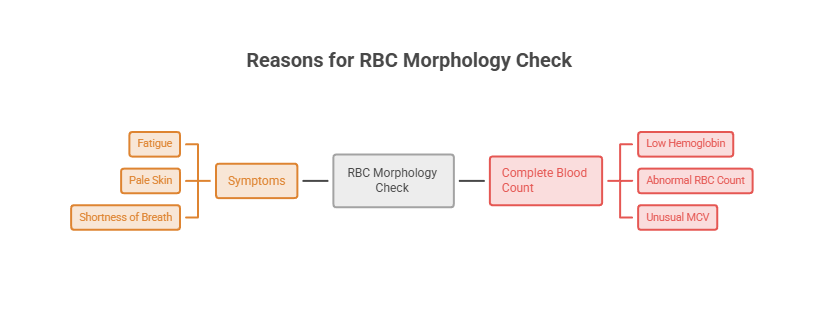
Symptoms That Prompt a Smear
Persistent fatigue, weakness, pale skin, or shortness of breath can point to anemia, and a smear helps explain why. Jaundice or unusually dark urine may suggest red cells are breaking down too fast.
Patients we serve are often referred for a smear after a routine CBC flags an abnormal MCV or RDW. Unexplained bruising, recurrent infections, or a known family history of a blood disorder can prompt one too.
Conditions It Helps Diagnose
Morphology helps sort out the cause of anemia, separating iron deficiency from B12 deficiency, thalassemia, or hemolysis. It can also flag inherited conditions like sickle cell disease and hereditary spherocytosis.
The smear supports diagnosing bone marrow disorders, certain infections, and microangiopathic emergencies. In each case, the shapes guide which confirmatory test comes next, which saves both time and guesswork.
Normal vs Abnormal: The Key Terms
Two terms appear constantly on smear reports, and patients mix them up all the time. Knowing the difference makes a confusing report far less intimidating.
Poikilocytosis describes abnormal shapes. Anisocytosis describes abnormal size. They frequently show up together, in which case the report may read “anisopoikilocytosis.”
Poikilocytosis (Shape Variation)
Poikilocytosis is the umbrella term for red blood cells of abnormal shape, which are called poikilocytes. Cleveland Clinic notes the label applies when more than 10% of red blood cells are abnormally shaped.
The framing matters here. StatPearls stresses that poikilocytosis is a morphologic finding, not a diagnosis, and serves as a fingerprint pointing toward an underlying disease.
Anisocytosis (Size Variation)
Anisocytosis means the red blood cells vary noticeably in size, with some too small and others too large. It often reflects a developing or mixed anemia.
When both size and shape are off, the smear is described as anisopoikilocytosis. This combination tends to appear in more advanced anemia and usually drives the RDW markedly higher than normal.
Color: Normochromic, Hypochromic, Polychromasia
Color reflects how much hemoglobin a cell carries. Normochromic cells have normal color and central pallor, while hypochromic cells look pale with an enlarged pale center.
Polychromasia describes a bluish tint in some cells, a sign of young red blood cells (reticulocytes) released early from the marrow. Our medical reviewers note that polychromasia often means the marrow is working hard to replace lost cells.
Abnormal Red Blood Cell Shapes Explained
What each abnormal shape looks like, and what it tends to mean, is the heart of any morphology report. The table below works as a quick lookup, followed by detail on the shapes you’re most likely to see.
| Cell Type | Appearance | Commonly Associated Conditions | What It Signals |
| Sickle cells (drepanocytes) | Crescent or “C” shaped, rigid | Sickle cell disease | Abnormal hemoglobin (HbS) polymerizing |
| Target cells (codocytes) | Bullseye, central spot ringed by pallor | Thalassemia, liver disease, HbC, after spleen removal | Excess membrane relative to hemoglobin |
| Spherocytes | Round, no central pallor | Hereditary spherocytosis, autoimmune hemolytic anemia | Membrane loss, fragile cells |
| Elliptocytes (ovalocytes) | Oval to cigar-shaped | Hereditary elliptocytosis, iron deficiency | Membrane skeleton defect |
| Schistocytes | Jagged fragments, helmet shapes | TTP, HUS, DIC, mechanical heart valves | Physical shearing of cells (often urgent) |
| Echinocytes (burr cells) | Evenly spaced short spicules | Uremia, pyruvate kinase deficiency, artifact | Membrane or metabolic change |
| Acanthocytes (spur cells) | Irregular, uneven spicules | Severe liver disease, abetalipoproteinemia | Lipid imbalance in the membrane |
| Teardrop cells (dacrocytes) | Single pointed end, teardrop | Myelofibrosis, thalassemia | Marrow stress or fibrosis |
| Stomatocytes | Slit-like central pallor | Liver disease, alcohol use, hereditary stomatocytosis | Membrane water imbalance |
| Bite cells (degmacytes) | Look like a bite was taken out | G6PD deficiency, oxidative damage | Spleen removing damaged hemoglobin |
Sickle Cells (Drepanocytes)
Sickle cells are rigid, crescent-shaped red blood cells. They form when abnormal hemoglobin (HbS) polymerizes under low-oxygen conditions, stiffening the cell into its signature curve.
These cells get stuck in small vessels, causing pain and organ damage over time. Their presence on a smear points strongly toward sickle cell disease, an inherited condition confirmed with hemoglobin testing.
Target Cells (Codocytes)
Target cells look like a bullseye, with a dark center surrounded by a pale ring and an outer rim of hemoglobin. They form when a cell carries too much membrane for its hemoglobin content.
In smears reviewed across our diagnostic network, target cells most often trace to thalassemia trait, liver disease, or a hemoglobin variant like HbC. They can also appear after the spleen is removed.
Spherocytes
Spherocytes are small, round cells that have lost their central pallor. The loss of membrane makes them rigid and fragile, so the spleen destroys them earlier than normal.
They classically appear in hereditary spherocytosis, a genetic membrane disorder, and in autoimmune hemolytic anemia, where the immune system attacks red blood cells. Both can cause ongoing hemolysis and anemia.
Schistocytes (the Urgent One)
Schistocytes are fragments of red blood cells, often jagged or helmet-shaped. They form when cells are physically sheared apart as they pass through damaged or obstructed vessels.
This is the shape that can’t wait. Schistocytes raise concern for microangiopathic processes like TTP, HUS, or DIC, conditions that may need rapid treatment, so a smear showing them usually triggers urgent evaluation.
Other Shapes in Brief
Several more shapes round out the catalog. Elliptocytes are oval or cigar-shaped and appear in hereditary elliptocytosis and iron deficiency, while teardrop cells suggest marrow stress or myelofibrosis.
Acanthocytes carry irregular spurs and point toward severe liver disease, whereas echinocytes have even spicules linked to uremia. Bite cells, with a scalloped edge, are a hallmark of G6PD deficiency after oxidative stress.
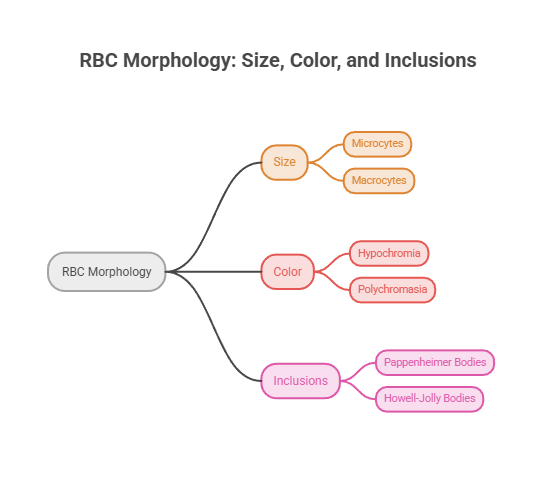
Size, Color, and Inclusions
Morphology is more than shape. Size and color round out the red cell picture, and tiny inclusions inside the cells add another layer of clues.
These features often appear together with shape changes. Reading them as a group is what turns a smear into a useful diagnostic map rather than a single data point.
Microcytes and Macrocytes (Size)
Microcytes are abnormally small red blood cells, usually under about 7 micrometers. They show up in conditions that impair hemoglobin production, especially iron deficiency anemia and the thalassemias.
Macrocytes are abnormally large cells. They commonly reflect vitamin B12 or folate deficiency (megaloblastic anemia), and they can also appear with liver disease and heavy alcohol use. The MCV usually confirms what the smear suggests.
Hypochromia and Polychromasia (Color)
Hypochromic cells look pale because they carry less hemoglobin, with the central pallor expanding as hemoglobin drops. This pale appearance is a classic sign of iron deficiency.
Polychromasia describes immature, bluish-tinged red cells released early from the marrow. Patients we serve with active blood loss or recovering anemia often show polychromasia as the marrow ramps up production to compensate.
Inclusions
Inclusions are structures inside red blood cells that shouldn’t be there in healthy adults, and each type carries its own meaning. They’re easy to miss without a careful manual review.
Howell-Jolly bodies are leftover DNA fragments seen after spleen removal or poor spleen function. Basophilic stippling can indicate lead poisoning or thalassemia, while Heinz bodies point to oxidative damage as in G6PD deficiency. Pappenheimer bodies contain iron and appear in certain anemias.
Cell Arrangement: Rouleaux and Agglutination
Beyond individual cells, how red blood cells arrange themselves on the slide adds another clue. Two arrangement patterns stand out to a reviewer.
Rouleaux describes red cells stacked like a roll of coins, often linked to high protein levels from inflammation or conditions such as multiple myeloma. Agglutination is irregular clumping, which can point to cold agglutinin disease, where antibodies make red cells stick together.
What Abnormal Morphology Reveals (Conditions Behind the Shapes)
Abnormal shapes aren’t the problem themselves; they’re the visible sign of something upstream. Causes fall into two broad groups: inherited and acquired.
The conditions below are among the most common drivers of abnormal morphology in the United States, with real figures attached so you can see the scale.
| Condition | US Statistic | Source |
| Sickle cell disease | Affects more than 100,000 Americans | NHLBI |
| Sickle cell trait | About 1 in 13 Black newborns | NHLBI |
| Sickle cell disease at birth | About 1 in 365 Black newborns | CDC |
| Anemia (all causes) | About 9.3% of people age 2 and older (2021 to 2023) | CDC |
| Iron deficiency | Most common cause of microcytic anemia worldwide | StatPearls |
Inherited Causes
Some abnormal shapes come from genes passed down at birth. Sickle cell disease produces sickle cells, thalassemia produces target cells and microcytes, and hereditary spherocytosis produces spherocytes.
NHLBI reports sickle cell disease affects more than 100,000 people in the United States and 8 million worldwide, with more than 90% of US cases among non-Hispanic Black or African American individuals. G6PD deficiency, another inherited condition, produces bite cells under oxidative stress.
Acquired Causes
Other shape changes develop later in life. Healthline notes poikilocytosis is commonly caused by anemia, liver disease, alcoholism, or inherited blood disorders.
Nutritional deficiencies (iron, B12, folate), severe liver disease, hemolysis, and bone marrow disorders all reshape red cells. Anemia is widespread: CDC data shows about 9.3% of people age 2 and older had anemia in 2021 to 2023, with rates higher in females than males.
What to Do About an Abnormal RBC Morphology Report
A report reading “abnormal morphology” or “poikilocytosis” understandably raises worry, but it’s a prompt for follow-up rather than a verdict. What matters is the specific finding and how you feel.
Use the table below as a quick guide to what different smear comments may mean and the sensible next step for each.
| Smear Finding | What It May Mean | Recommended Next Step |
| “Poikilocytosis” noted | Abnormal shapes, often from anemia | Review with your provider; expect follow-up tests for the cause |
| Anisocytosis or high RDW | Size variation, possible early or mixed anemia | Check iron, B12, and folate; correlate with MCV |
| Target cells reported | Thalassemia trait, liver disease, or HbC | Hemoglobin studies and liver assessment as advised |
| Schistocytes present | Possible microangiopathic process | Seek prompt evaluation; this can be urgent |
| Flagged but no symptoms | May be mild or partly artifact | Repeat smear and discuss whether further testing is needed |
Questions to Ask Your Provider
Walking in prepared turns a worrying report into a productive visit. Ask which specific shapes were seen, what percentage of cells were affected, and what conditions those shapes suggest.
It also helps to ask whether your MCV, RDW, and reticulocyte count line up with the smear, and whether you need confirmatory tests like hemoglobin electrophoresis or iron studies.
When It’s Urgent vs Routine
Most morphology findings are followed up at a routine pace, especially when you feel well and the changes are mild. Iron-deficiency patterns, for example, are common and treatable.
Schistocytes are the clear exception. Patients commonly ask us when a smear result counts as an emergency, and fragmented cells paired with signs like easy bruising, dark urine, or confusion deserve immediate medical attention.
Can Abnormal Red Blood Cell Shapes Return to Normal?
Whether shapes can normalize depends entirely on the cause, which is one of the most hopeful parts of this topic for patients. Some causes resolve completely; others are managed for life.
Knowing which category your finding falls into helps set realistic expectations before you even start treatment.
Reversible Causes
When abnormal morphology stems from a treatable problem, the cells often recover. Correcting iron, B12, or folate deficiency typically restores normal shape and size over a span of weeks to months.
Patients we serve with iron-deficiency smears often see morphology normalize after treatment and a repeat smear. Resolving an underlying liver issue or removing a triggering exposure can do the same.
The timeline depends on the cause and how long it lasted. Red blood cells live about 120 days, so a smear often looks meaningfully better within a few months once the underlying problem is corrected and the marrow replaces older cells.
Lifelong and Inherited Conditions
Inherited conditions like sickle cell disease, thalassemia, and hereditary spherocytosis don’t disappear, because the genetic cause stays in place. The abnormal shapes persist on the smear.
Treatment still matters a great deal. The American Society of Hematology notes that while there’s no universal cure for sickle cell disease, treatments help people manage pain, prevent infections, and limit organ damage.
Decoding Common Smear Report Terms
Smear reports use a shorthand that can look cryptic at first. Labs usually grade abnormal findings by how many cells are affected, so the wording is really a measure of severity.
You may see words like “few,” “moderate,” or “marked,” or a scale from 1+ to 4+, where a higher number means more abnormal cells. A “1+ poikilocytosis” is mild, while “4+ poikilocytosis” is striking.
The report may also name specific shapes, such as “moderate target cells” or “occasional schistocytes.” Pairing the grade with the shape tells your provider both what is present and how much of it.
Our medical reviewers note that the same shorthand applies to size and color, so “mild anisocytosis” or “slight hypochromia” simply describes the degree of the finding. None of these terms is a diagnosis on its own.
How to Support Normal Red Blood Cell Shape
Healthy red cell shape starts with giving your bone marrow the raw materials it needs. Iron, vitamin B12, and folate are the building blocks for normal, well-formed red blood cells.
Iron-rich foods include lean red meat, poultry, beans, lentils, and fortified cereals, and pairing plant iron with vitamin C improves absorption. Vitamin B12 comes from animal products and fortified foods, while folate is plentiful in leafy greens and legumes.
Habits That Help
Staying hydrated and limiting heavy alcohol use both support normal morphology, since dehydration and alcohol can distort red cells. For people with G6PD deficiency, avoiding known oxidative triggers helps prevent bite cells and episodes of hemolysis.
No food or habit reshapes cells overnight, and inherited conditions won’t respond to diet alone. Still, good nutrition gives a recovering marrow the best chance to rebuild normal cells after a treatable deficiency.
When to Get Tested
If you have ongoing fatigue, a family history of a blood disorder, or a previous abnormal CBC, periodic testing is worthwhile. A simple blood draw can track your morphology over time.
Patients we serve who treat an iron or B12 deficiency often repeat a smear a few months later to confirm their red cells have returned to a normal shape and size.
The Bottom Line on RBC Morphology
Red blood cell morphology turns a simple glass slide into one of hematology’s most informative tests. The shape, size, color, arrangement, and inclusions of your cells each carry clues the raw count alone can miss.
An abnormal finding is a starting point, not a conclusion. Most trace to common, treatable causes like iron deficiency, while a few, especially schistocytes, call for fast action. Reviewing the smear with your provider, alongside your CBC numbers, is how those clues become real answers. The shape of a single red blood cell, read in the right context, can point the way to both the diagnosis and the treatment.
Frequently Asked Questions
What is RBC morphology?
RBC morphology is the assessment of red blood cells’ shape, size, color, and internal inclusions under a microscope, usually on a peripheral blood smear. Normal cells are uniform biconcave discs with a pale center. Abnormal morphology helps providers identify conditions like anemia, hemoglobin disorders, and other blood problems.
What does abnormal red blood cell morphology mean?
It means your red blood cells differ from the normal biconcave disc in shape, size, or color. Abnormal morphology is a finding, not a diagnosis. It signals an underlying issue, such as nutritional deficiency, a hemoglobin disorder, liver disease, or hemolysis, that needs further testing to pinpoint.
What is poikilocytosis?
Poikilocytosis is the presence of abnormally shaped red blood cells, called poikilocytes. It’s generally defined as more than 10% of red cells being abnormal in shape. It isn’t a disease itself but a clue pointing toward conditions like anemia, liver disease, or inherited blood disorders.
What is anisocytosis?
Anisocytosis means your red blood cells vary noticeably in size, with some smaller and some larger than normal. It often reflects anemia and usually corresponds to a high red cell distribution width (RDW). When both size and shape are abnormal, it’s called anisopoikilocytosis.
What are the main abnormal RBC shapes?
The most common are sickle cells, target cells, spherocytes, elliptocytes, schistocytes, echinocytes, and acanthocytes. Others include teardrop cells, stomatocytes, and bite cells. Each shape is linked to particular conditions, which is why identifying the specific type helps narrow the diagnosis.
What do target cells mean?
Target cells, or codocytes, look like a bullseye and form when a cell has excess membrane relative to hemoglobin. They commonly appear in thalassemia, liver disease, and hemoglobin C disease, and after spleen removal. On their own they’re a clue, confirmed with further hemoglobin or liver testing.
What do schistocytes indicate?
Schistocytes are red cell fragments created when cells are sheared apart in damaged vessels. They raise concern for microangiopathic conditions like TTP, HUS, or DIC, which can be medical emergencies. A smear showing schistocytes, especially with symptoms, usually prompts urgent evaluation by a provider.
Do sickle cells always mean sickle cell disease?
Seeing true sickle cells on a smear strongly suggests sickle cell disease, an inherited condition. However, diagnosis is confirmed with hemoglobin testing, such as electrophoresis, not the smear alone. People with sickle cell trait usually don’t show sickled cells under normal conditions.
How is RBC morphology tested?
It’s assessed on a peripheral blood smear, where a drop of blood is spread on a slide, stained, and examined under a microscope. Automated analyzers flag possible abnormalities, but a trained technologist or pathologist confirms and names the specific shapes for an accurate interpretation.
Is abnormal RBC morphology serious?
It can range from mild to serious depending on the cause. Many findings, like those from iron deficiency, are common and treatable. Others, especially schistocytes, can signal urgent conditions. The shapes themselves are clues, so seriousness depends on the underlying diagnosis and your symptoms.
Can abnormal red blood cell shapes be reversed?
Sometimes. When the cause is treatable, such as iron, B12, or folate deficiency, morphology often returns to normal after treatment. Inherited conditions like sickle cell disease and thalassemia are lifelong, so their abnormal shapes persist, though treatment helps manage symptoms.
What’s the difference between poikilocytosis and anisocytosis?
Poikilocytosis refers to abnormal red blood cell shape, while anisocytosis refers to abnormal variation in size. They often occur together, described as anisopoikilocytosis. Both are smear findings that point toward an underlying condition rather than being diagnoses in themselves.
Medical Disclaimer: This article is for general informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Red blood cell morphology is a laboratory finding, not a diagnosis on its own. Always discuss your blood smear and CBC results with a qualified healthcare provider, and seek prompt care for urgent findings.
References
- Cleveland Clinic: Poikilocytosis
- Healthline: Poikilocytosis
- Medical News Today: Poikilocytosis
- StatPearls (NCBI): Poikilocytosis
- PubMed: Red Blood Cell Morphology
- NHLBI: Sickle Cell Disease
- CDC MMWR: Birth Prevalence of Sickle Cell Disease
- CDC NCHS Data Brief: Anemia Prevalence, United States, 2021 to 2023
- American Society of Hematology: Sickle Cell Disease





