

A patient sits across from me in the exam room, pale and clutching their abdomen. They don’t mention heartburn or chest pain. Instead, they ask one very specific question: can acid in the stomach cause nausea?
Table of Contents
As a board-certified gastroenterologist with over 15 years of clinical experience, I hear this question nearly every day. The short answer is yes, absolutely. It is one of the most common yet widely misunderstood symptoms of gastrointestinal distress.
Most people think of stomach acid strictly in terms of a burning sensation in the chest. But the digestive tract is a complex system wired directly to the brain. When things fall out of balance, the resulting distress signals often show up as severe queasiness, not heartburn.
In this clinical guide, I will walk you through the exact physiological connections between your gut and brain, explain the root causes of acid-related nausea, break down the difference between high and low stomach acid, and share evidence-based strategies for both immediate and long-term relief.
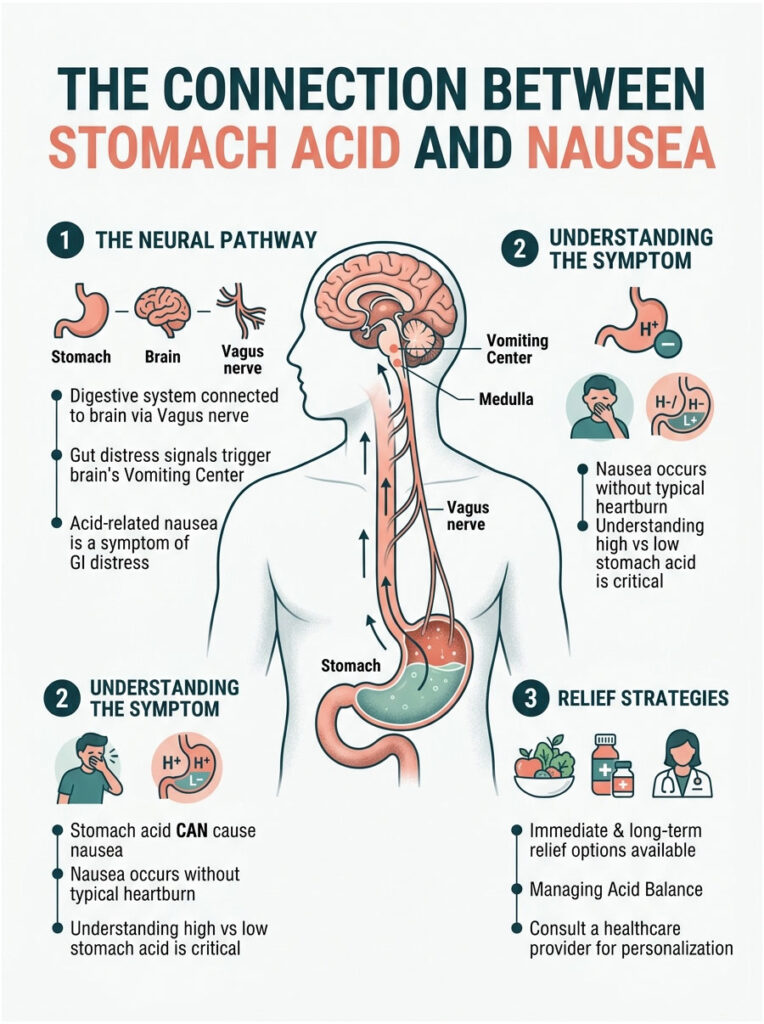
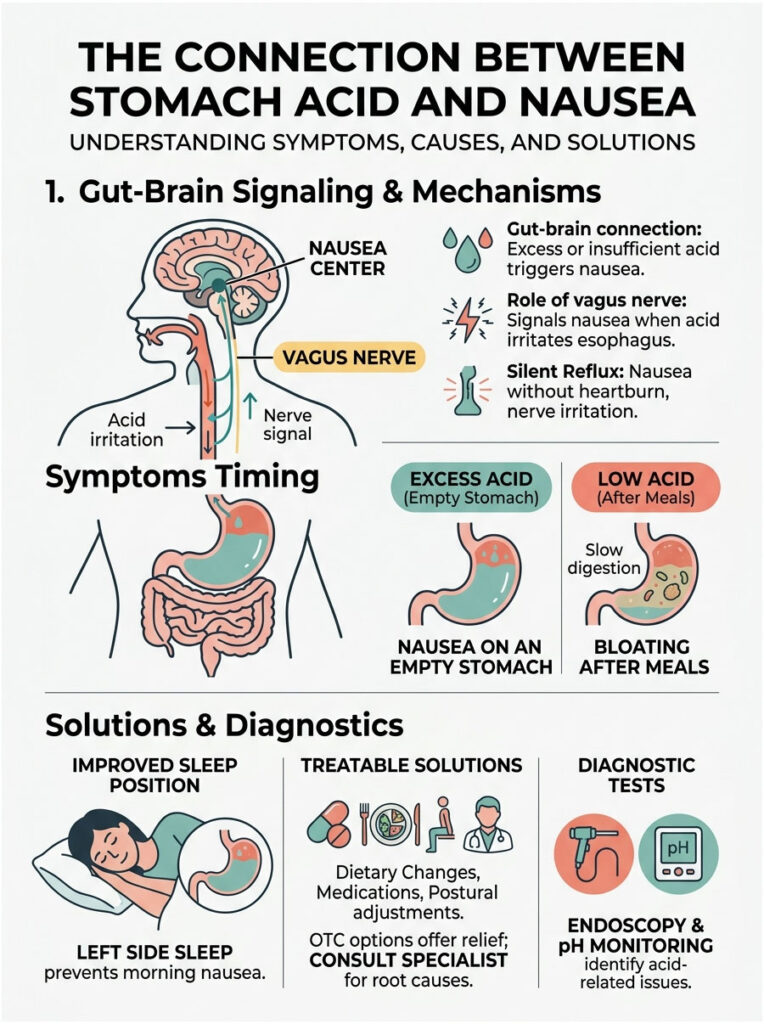
Quick Answer: Yes, stomach acid absolutely can cause nausea. When corrosive gastric juices escape the stomach or irritate the digestive lining, they trigger the vagus nerve. This nerve sends immediate distress signals to the brain’s vomiting center, producing severe nausea, even without traditional heartburn.
Key Clinical Statistics
- Up to 25 percent of GERD patients report nausea as their primary symptom.
- Over 60 million Americans experience acid-related digestive discomfort at least once a month.
- Silent reflux affects nearly 20 percent of the US population, often without any traditional heartburn.
- Helicobacter pylori infects roughly 30 to 40 percent of the US population, disrupting normal gastric function.
- Patients on proper acid-suppressing therapy report a 70 percent reduction in unexplained nausea within four weeks.
- More than 40 percent of chronic nausea cases in adults are linked to undetected gastrointestinal motility issues.
How Does Stomach Acid Cause Nausea? The Physiology Explained
To understand why stomach acid makes you feel sick, you need to look at the anatomy of your digestive system. The connection between your gut and brain is not just a figure of speech. It is a physical, electrical pathway that influences how you feel every single day.
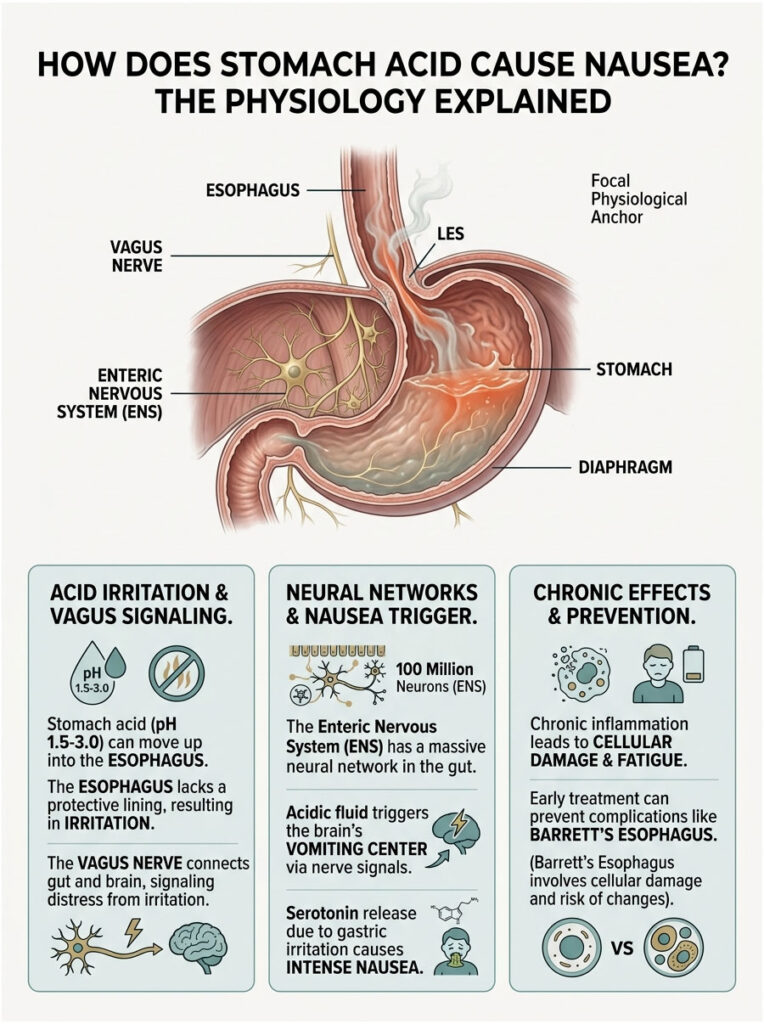
Your stomach is built to hold highly corrosive fluids with a pH between 1.5 and 3.0. Your esophagus and throat lack the same protective lining. When something goes wrong mechanically, your body essentially hits the panic button.
Many patients ask whether they can feel sick without feeling pain. The answer is yes. The nerves in your digestive tract interpret irritation differently depending on exactly where the fluid lands.
The Vagus Nerve Connection
The vagus nerve functions as a massive information superhighway between your gut and brainstem. It controls your heart rate, digestion, and reflex actions, and it is the longest cranial nerve in the body.
When acidic fluid splashes into the lower esophagus, it burns the delicate mucosal lining. Vagal afferent fibers detect this chemical burn instantly and send rapid distress signals to the medulla oblongata in the brain. Specifically, these signals reach the area postrema, which is the brain’s vomiting center.
This means that nausea from acid reflux is actually a neurological response to a chemical burn in your digestive tract. Your brain is trying to figure out how to expel what it perceives as a poison.
The Enteric Nervous System Response
Beyond the vagus nerve, your gut has its own independent nervous system. We call it the Enteric Nervous System (ENS). It contains over 100 million neurons embedded directly in the walls of your gastrointestinal tract.
When gastric juices irritate the stomach lining, the ENS releases a flood of neurotransmitters, including serotonin. While serotonin is best known for regulating mood, 95 percent of it is actually produced in the gut. A sudden spike in gut serotonin triggers intense waves of nausea.
This localized reaction explains why you can feel sick even when acid never reaches the esophagus. The stomach itself is sounding the alarm, stopping normal digestion and preparing the body to purge.
Cellular Damage and Chronic Inflammation
At the microscopic level, chronic exposure to misplaced gastric juices causes severe cellular damage. The cells lining your esophagus swell and release inflammatory cytokines.
This inflammation creates a constant state of low-grade sickness. Your body recognizes that tissue is being destroyed and responds by making you feel fatigued, lethargic, and deeply nauseated to force you to rest and stop eating.
Over time, this damage can lead to Barrett’s Esophagus, a serious complication where the tissue changes its genetic structure to survive the acid exposure. Catching and treating the nausea early can help prevent this dangerous cellular mutation.
Lower Esophageal Sphincter Dysfunction and Mechanical Failures
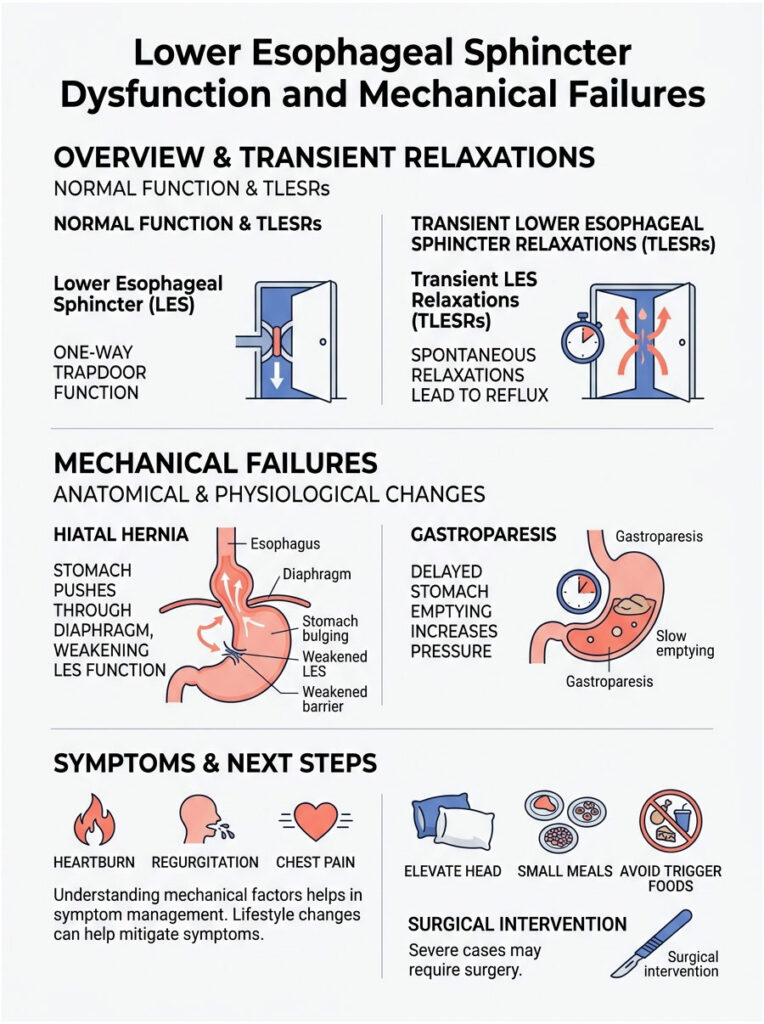
At the bottom of your esophagus sits a ring of muscle called the Lower Esophageal Sphincter, or LES. Think of it as a one-way trapdoor. When you swallow food, the door opens to let it drop into the stomach, then snaps shut to keep corrosive digestive juices from escaping upward.
Many mechanical factors can weaken this muscle. When the trapdoor stays open, fluid freely washes upward, triggering daily bouts of nausea and ruining quality of life.
Transient LES Relaxations
Sometimes the LES is not permanently weak but opens at the wrong moments. We call these events Transient Lower Esophageal Sphincter Relaxations (TLESRs). They are brief, spontaneous openings of the valve that occur outside of normal swallowing.
TLESRs are actually the most common cause of reflux in otherwise healthy people. When the valve pops open, a mist of gastric juice shoots into the esophagus. You might not feel a burn, but your vagus nerve detects the chemical mist immediately. Frequent TLESRs lead to chronic, unexplained bouts of nausea with sudden onset.
The Role of a Hiatal Hernia
A hiatal hernia is a structural defect that severely compromises digestive mechanics. Your diaphragm, the large muscle sheet separating your chest from your abdomen, has a small hole the esophagus passes through. In a hiatal hernia, the top part of the stomach pushes up through this hole into the chest cavity.
This completely destroys the natural pressure barrier that keeps the LES tightly closed. Patients with large hiatal hernias suffer from profound, relentless nausea because gravity no longer helps keep fluid down. Surgery is sometimes required to pull the stomach back into position and repair the defect.
Delayed Gastric Emptying (Gastroparesis)
Sometimes the problem is not acid splashing upward but food refusing to move downward. Gastroparesis is a condition where the stomach empties its contents into the small intestine far too slowly because the stomach muscles stop contracting properly.
High acidity and severe inflammation can trigger a temporary state of gastroparesis. Food and gastric juices stagnate for hours, and the trapped food begins to ferment. The stomach distends, stretching nerve endings past their normal capacity and sending panic signals to the brain that register as severe, debilitating nausea.
Clinical Causes of Acid-Induced Nausea
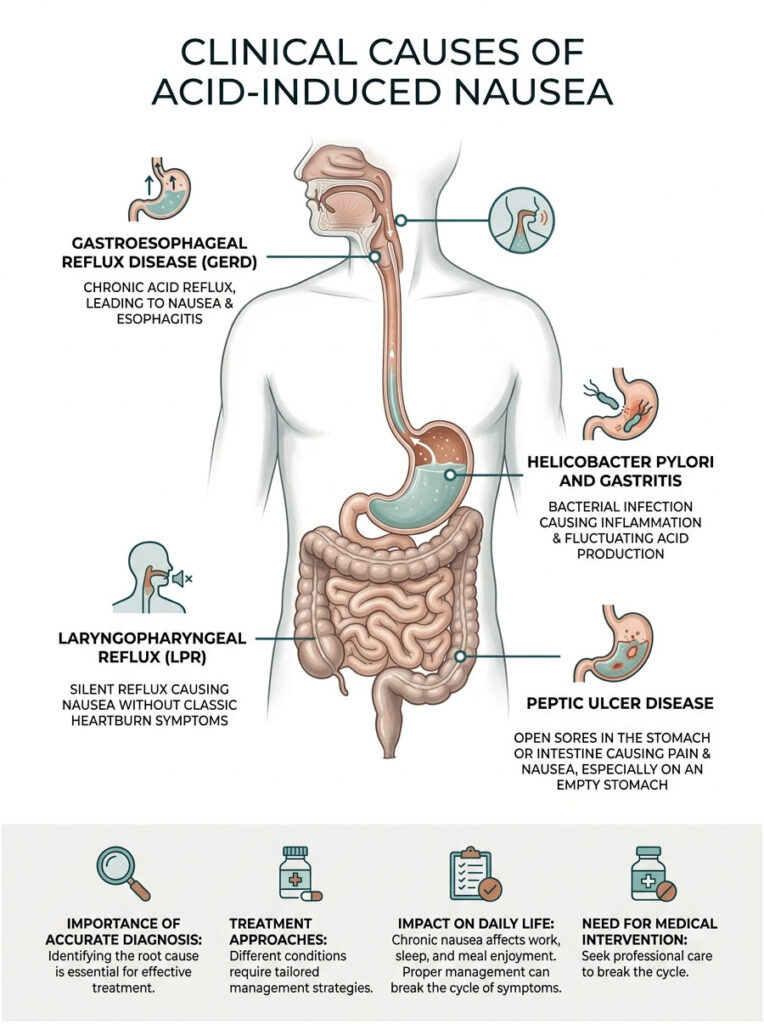
In practice, pinpointing the exact root cause of your symptoms is the first step toward permanent relief. Different gastrointestinal conditions require very different treatment approaches. Here are the most common causes I see in my practice every week.
Gastroesophageal Reflux Disease (GERD)
GERD is the chronic, more severe form of standard acid reflux. It occurs when the backwash of gastric juices happens repeatedly, causing long-term damage to the esophageal lining. Patients with GERD often develop esophagitis, chronic inflammation of the swallowing tube that creates a persistent baseline of nausea.
For these individuals, feeling sick becomes a daily battle. It interrupts work, sleep, and the ability to enjoy meals. Proper medical management is essential to break this cycle of inflammation.
Helicobacter Pylori and Gastritis
Helicobacter pylori is a spiral-shaped bacterium that thrives in the harsh environment of the stomach. It burrows into the protective mucosal lining, causing localized inflammation known as gastritis and drastically fluctuating your natural acid production levels.
This chemical chaos prevents smooth digestion. The result is chronic indigestion, severe bloating, and waves of unexplained nausea that strike at random times. Eradicating the bacteria with antibiotics typically cures the symptom completely.
Laryngopharyngeal Reflux (LPR) and Silent Reflux
LPR, frequently called silent reflux, presents without classic heartburn symptoms. Microscopic droplets of gastric fluid and the enzyme pepsin escape the stomach and travel all the way up into the throat and voice box. The laryngeal tissues are incredibly sensitive to these chemicals and are not designed to handle a pH below 6.0.
Patients experience intense nausea when these tiny droplets irritate vagus nerve endings in the throat. They often clear their throats constantly, feel a lump sensation, and experience severe queasiness without any chest burning.
Peptic Ulcer Disease
Peptic ulcers are open sores on the inside lining of the stomach or the upper portion of the small intestine. They are most commonly caused by H. pylori or long-term use of nonsteroidal anti-inflammatory drugs like ibuprofen.
When gastric fluid washes over these open sores, it causes gnawing pain that many patients interpret as profound nausea. This type of nausea usually peaks on an empty stomach and improves temporarily after eating, since food acts as a buffer. Healing the ulcer is the only path to permanent relief.
Bile Reflux vs. Acid Reflux: Understanding the Difference
It is critical to distinguish between acid reflux and bile reflux. While they feel similar, they are entirely different chemical processes. Treating one with medications meant for the other will not work.
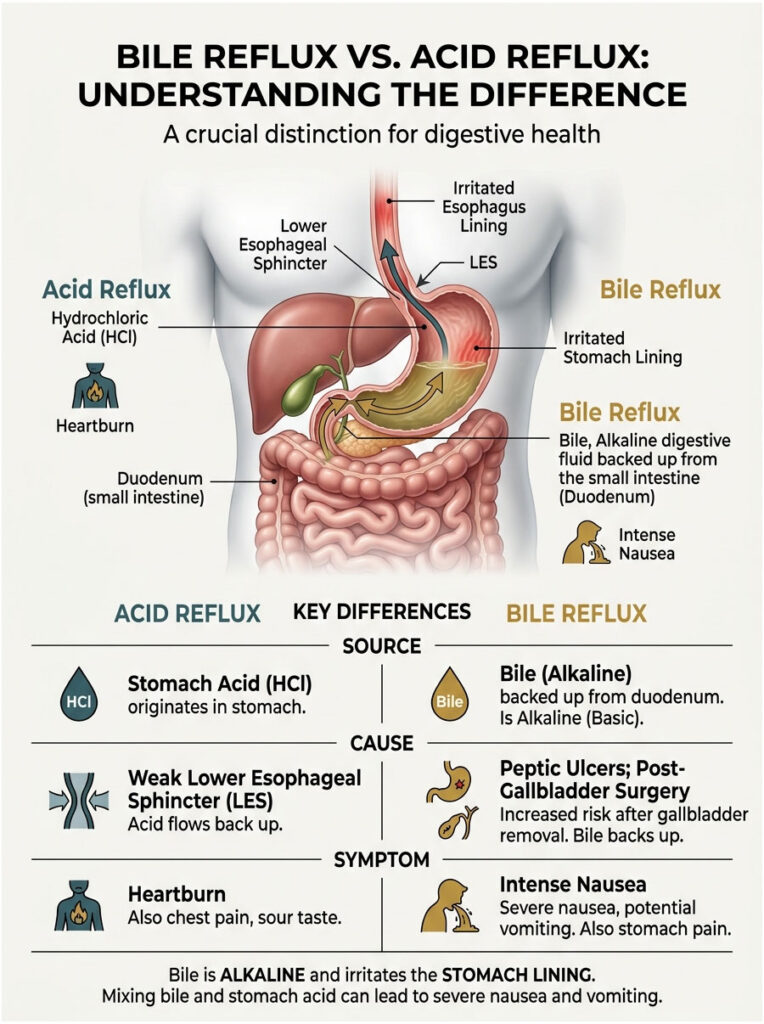
Acid reflux originates in the stomach from hydrochloric acid. Bile reflux occurs when digestive fluid from the liver backs up from the small intestine, pushes through the pyloric valve, and enters the stomach. Bile is highly alkaline and extremely irritating to the gastric mucosa. When it mixes with stomach acid, it causes a severe chemical reaction that often leads to violent nausea and bilious vomiting.
| Feature | Acid Reflux | Bile Reflux |
| Primary Fluid | Hydrochloric acid from the stomach | Bile from the liver via the small intestine |
| Origin | Stomach backing into esophagus | Small intestine backing into stomach |
| Key Symptoms | Heartburn, sour taste, nausea | Upper abdominal pain, bilious vomiting, intense nausea |
| Common Causes | Weak LES, hiatal hernia, dietary triggers | Peptic ulcers, gallbladder surgery, pyloric valve dysfunction |
| Treatment | PPIs, antacids | Bile acid sequestrants, prokinetics, surgery |
If you have had your gallbladder removed, your risk for bile reflux increases significantly. Without a gallbladder to store bile, it drips continuously into the intestines and can easily back up into the stomach, causing severe morning nausea. Always inform your gastroenterologist about past abdominal surgeries.
High Stomach Acid vs. Low Stomach Acid: A Common Misconception
There is a widespread misconception that all reflux symptoms come from having too much acid. This is simply not true. In fact, too little acid can cause the exact same symptoms. Misdiagnosing this will make you feel significantly worse.
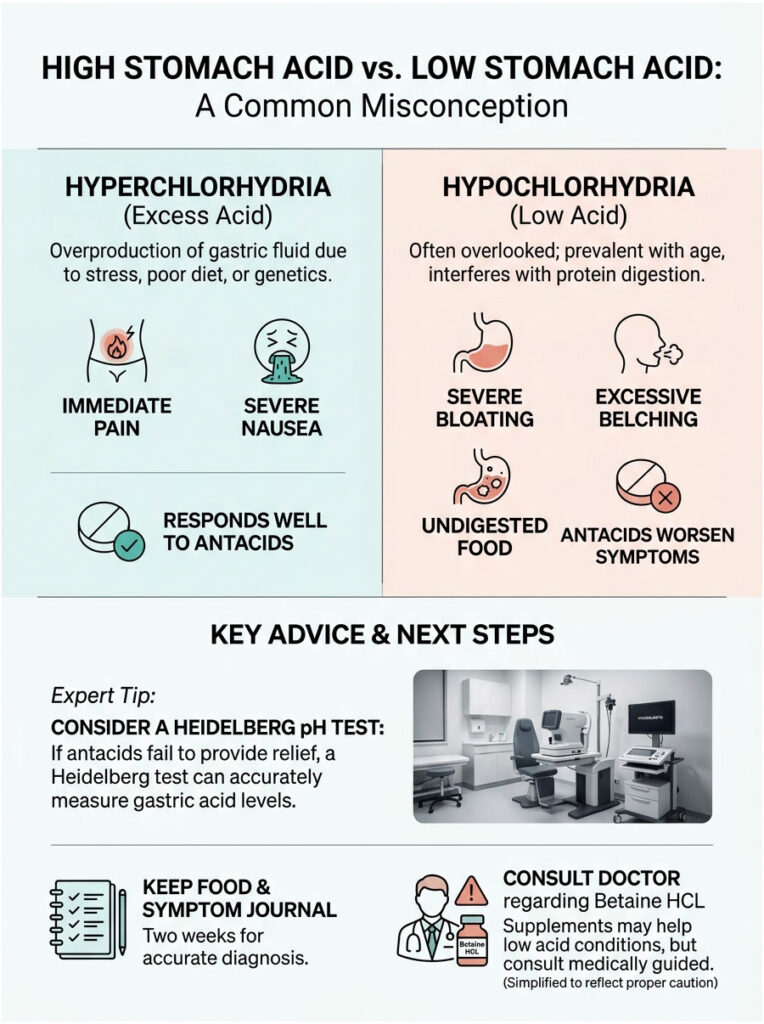
Hyperchlorhydria (Excess Acid)
Hyperchlorhydria is the medical term for excess gastric fluid production. This is what most people picture when they think of reflux. It is often driven by stress, poor diet, or genetic factors.
When gastric glands overproduce hydrochloric acid, the sheer volume of fluid overwhelms the stomach. The excess splashes against the LES, eventually forcing it open through volume and pressure alone. This direct chemical burn to the mucosal lining causes immediate pain and severe nausea. It responds well to antacids and prescription acid suppressants.
Hypochlorhydria (Low Acid)
Hypochlorhydria, or low stomach acid, is common yet frequently overlooked. It becomes more prevalent with age. Your stomach needs a highly acidic environment to break down proteins properly.
When pH levels are too high (meaning low acidity), food sits in the stomach like a rock. Because it is not being digested, the food ferments, producing massive amounts of gas. That gas builds pressure, forces the LES open, and carries whatever small amount of acid you do have upward on gas bubbles. Taking an antacid for this condition will actually make your symptoms worse.
Expert Tip: If you experience severe bloating and nausea after eating a heavy protein meal, and antacids provide zero relief, you may have low stomach acid. Ask your gastroenterologist about a Heidelberg pH test.
| Clinical Indicator | High Acid (Hyperchlorhydria) | Low Acid (Hypochlorhydria) |
| Onset of Nausea | Often on an empty stomach or at night | Immediately or shortly after eating |
| Accompanying Symptoms | Sharp chest burning, sour regurgitation | Severe bloating, excessive belching, undigested food in stool |
| Response to Antacids | Immediate relief | Symptoms worsen or stay unchanged |
| Nutrient Deficiencies | Rare, unless on long-term PPI therapy | Common (Vitamin B12, Iron, Calcium) |
| Diagnostic Test | Endoscopy, pH monitoring | Heidelberg test, Gastric string test |
Pay close attention to the timing of your symptoms. Keep a detailed food and symptom journal for two weeks. This data is invaluable for making an accurate clinical diagnosis. If low acidity is confirmed, Betaine HCL supplements can add acid back into your stomach during meals, often curing the nausea entirely. Never start supplementation without medical supervision.
Why Morning Nausea Is So Common: Nocturnal Acid Breakthrough
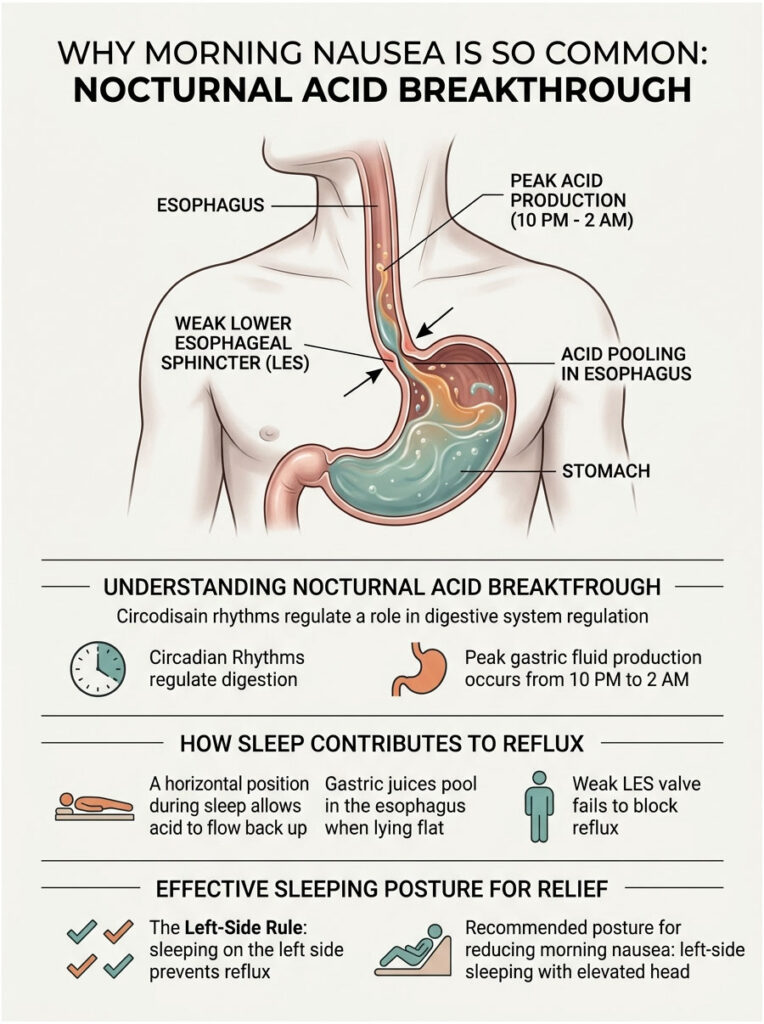
Many patients tell me their nausea is worst the moment they wake up. They open their eyes and are immediately hit with a wave of queasiness that ruins the entire morning. This is a well-documented phenomenon called nocturnal acid breakthrough.
Circadian Rhythms and Acid Production
Your body operates on a strict internal clock called a circadian rhythm. This clock controls everything from sleep cycles to hormone production, and your digestive system is heavily regulated by it.
Gastric fluid production naturally peaks between 10 PM and 2 AM. Your body actively prepares the digestive tract for the next day while you sleep. If you have a weakened LES, this overnight surge in acid production easily escapes into the esophagus. You sleep through the initial chemical burn and only wake up when the accumulated inflammation produces severe nausea.
Sleep Posture and Gravity
During the day, gravity pulls gastric juices downward, keeping them safely contained. When you lie flat, your stomach and esophagus sit on the same horizontal plane and fluid can travel freely in either direction.
If the LES is weak, acid simply spills backward, pooling in the esophagus all night. This pooling effect is why you wake up feeling like you need to vomit.
The Left-Side Rule: Because of the natural asymmetry of your internal organs, sleeping on your left side positions the stomach below the esophagus, making it anatomically difficult for fluid to spill upward. Sleeping on your right side does the opposite. Left-side sleeping with an elevated head is your best defense against morning nausea.
Advanced Diagnostic Testing for Chronic Nausea
When lifestyle changes and over-the-counter medications fail, we need objective medical data. Modern gastroenterology offers powerful diagnostic tools that let us see exactly what is happening inside your digestive tract in real time.
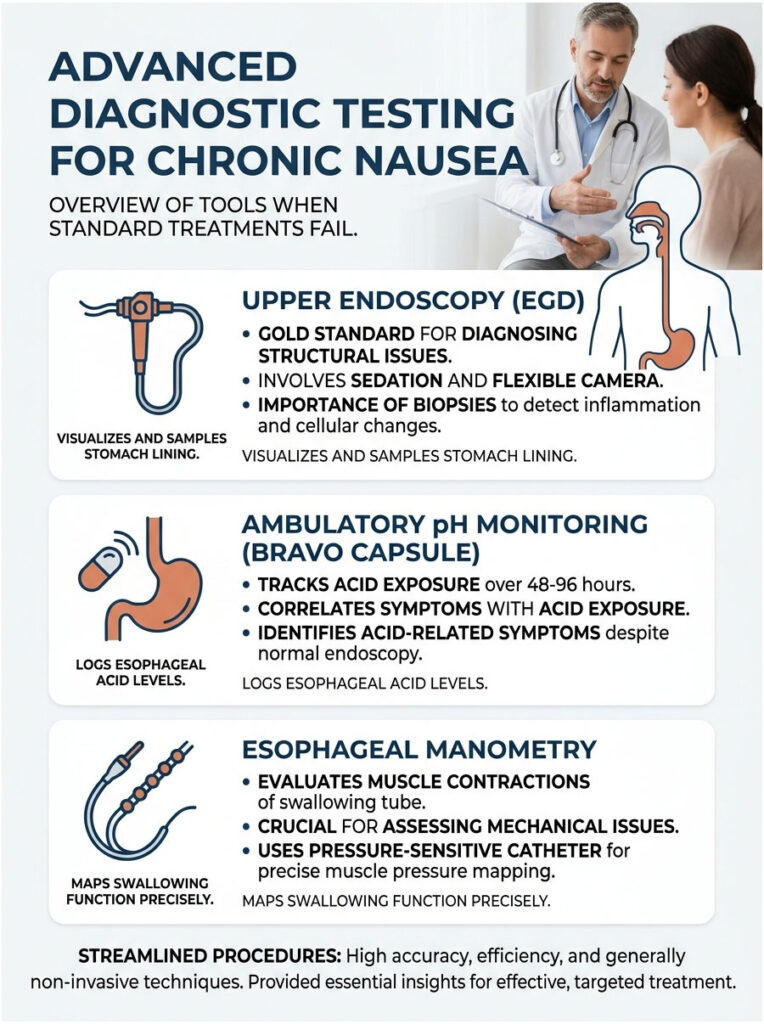
Upper Endoscopy (EGD)
The EGD is the gold standard for diagnosing structural digestive issues. You are placed under light sedation while we pass a flexible tube with a high-definition camera down your throat. We visually inspect the esophagus, stomach, and the first part of the small intestine, looking for ulcers, inflammation, hiatal hernias, and tumors.
During the procedure, we also take tiny tissue samples (biopsies) that are sent to a pathology lab to check for microscopic inflammation, H. pylori, and cellular changes. It is a painless, 15-minute procedure that provides definitive answers.
Ambulatory pH Monitoring (Bravo Capsule)
When the endoscopy looks normal but the patient is still suffering, we measure actual chemical exposure in the esophagus over 48 to 96 hours using a Bravo pH capsule. During an endoscopy, we clip a tiny wireless capsule to the lower esophageal lining. It records the exact pH of any fluid that splashes up and transmits the data to a receiver you wear on your belt.
You press a button on the receiver every time you feel nauseous. We then match your symptom reports to the exact moments of chemical exposure, proving definitively whether acid is causing your symptoms.
Esophageal Manometry
If we suspect a mechanical failure of the LES, we order an esophageal manometry test. This measures the rhythmic muscle contractions of your swallowing tube and tells us how strong the trapdoor actually is.
A thin, pressure-sensitive catheter is passed through the nose and into the stomach. You take small sips of water while the computer records muscle pressures and maps the entire swallowing process. This test is crucial before considering anti-reflux surgery.
Practical Strategies for Immediate and Long-Term Relief
When you are actively feeling sick, you need actionable strategies that work now. In clinical practice, we use a tiered approach: immediate neutralizers, medical suppression, and targeted dietary shifts.
Pharmacological Options
Antacids: Medications like calcium carbonate or magnesium hydroxide neutralize acid on contact, turning it into harmless water and salt. They work in minutes but wear off quickly.
H2 Blockers: Medications like famotidine block histamine receptors in the stomach lining, reducing acid production. They take about 30 minutes to work but provide relief for up to 12 hours.
Proton Pump Inhibitors (PPIs): Medications like omeprazole shut down cellular acid pumps entirely. They take a few days to reach full effect but provide 24-hour protection, allowing tissue to heal.
Breathing Techniques to Calm the Vagus Nerve
Sometimes nausea triggers a severe autonomic response, with cold sweats, dizziness, and a racing heart. To calm the vagus nerve, sit down in a quiet space and practice deep diaphragmatic breathing.
Inhale through your nose for four seconds, hold for four seconds, and exhale slowly through pursed lips for six seconds. Repeat ten times. The slow exhalation physically stimulates the vagus nerve and reduces the feeling of sickness.
Prokinetic Agents and Natural Alternatives
If your nausea stems from delayed gastric emptying, suppressing acid will not help. You need to get stagnant food moving. Prescription prokinetic agents like metoclopramide force the stomach muscles to contract vigorously, pushing food and fluid into the small intestine.
For a natural option, pure ginger root is highly effective. Drinking a strong ginger tea 20 minutes before a meal can stimulate healthy gastric contractions. It is a powerful, evidence-based remedy for digestive sluggishness.
Dietary Strategies for Long-Term Gut Healing
Medications provide acute relief, but true healing requires changes to your daily habits. Your diet plays a massive role in managing symptoms long-term.
A common question is whether milk helps soothe the stomach. Cold milk does provide a temporary coating effect on the esophagus. However, milk contains high amounts of fat and calcium, which trigger a massive rebound effect about an hour later. Your stomach produces even more acid to break down the fat, making nausea significantly worse.
Identifying and Removing Trigger Foods
You need to identify foods that cause the LES to relax inappropriately. The worst offenders are well known: chocolate, peppermint, alcohol, and caffeine directly weaken the sphincter muscle. Highly acidic foods like tomatoes, citrus fruits, and raw onions cause direct chemical irritation to an already inflamed esophagus.
Remove all potential triggers for at least four weeks. We call this the elimination phase. By clearing the triggers, you give your mucosal lining a chance to reduce baseline inflammation. Once healed, you can slowly reintroduce foods one at a time to test your tolerance.
Meal Timing and Portion Control
It is not just what you eat but when you eat. Large, heavy meals stretch the stomach significantly, putting immense pressure on the LES and forcing it open. Instead of three large meals, switch to five small, nutrient-dense meals throughout the day.
Establish a strict fasting window before bed. Stop eating at least three hours before lying down. This ensures your stomach is empty and helps prevent nocturnal breakthrough symptoms.
Alkaline Water and Pepsin Deactivation
For patients with LPR, alkaline water offers a specific benefit. Standard tap water has a neutral pH of 7.0, while alkaline water has a pH of 8.0 or 9.0. Clinical studies suggest that alkaline water can permanently denature pepsin, the digestive enzyme responsible for throat irritation in silent reflux.
Sipping alkaline water throughout the day, especially after meals, can wash away and deactivate pepsin clinging to throat tissues. It is a low-risk strategy for managing throat-based nausea.
Surgical and Advanced Interventions
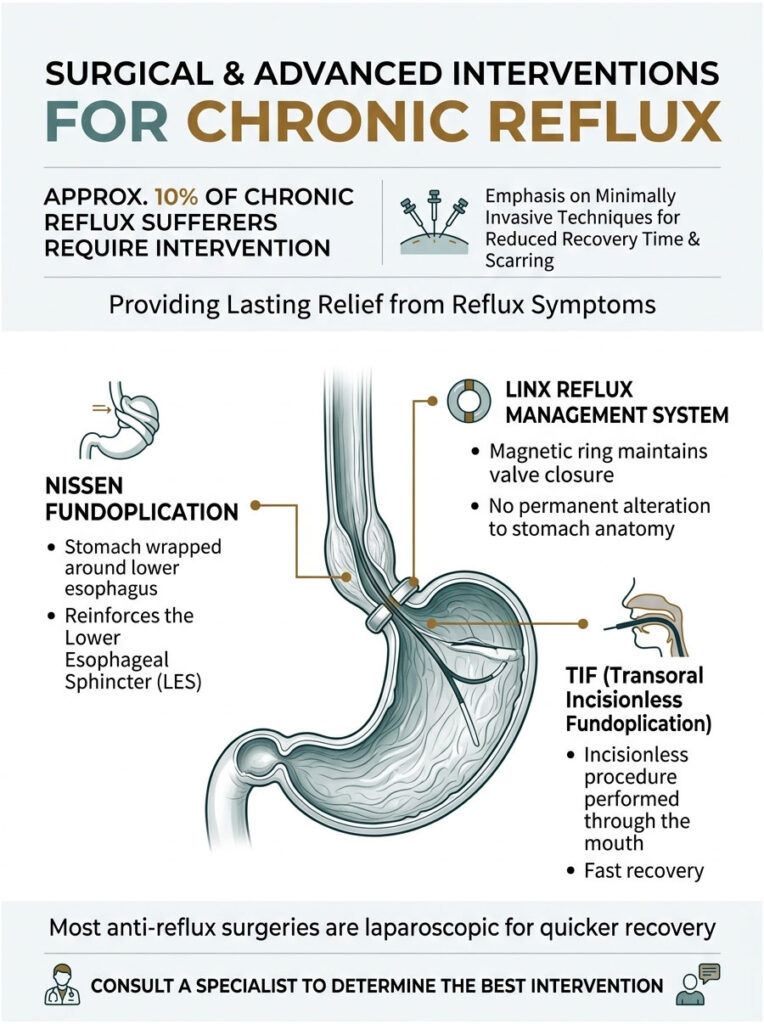
For roughly 10 percent of chronic sufferers, lifestyle changes and medications are not enough. The mechanical failure of the LES is too severe, and surgical correction becomes necessary. Modern anti-reflux surgery is highly advanced, with most procedures performed laparoscopically for faster recovery and minimal scarring.
Nissen Fundoplication
The Nissen Fundoplication has been the gold standard for reflux surgery for decades. The surgeon takes the upper part of the stomach and wraps it completely around the lower esophagus, stitching it into place. This creates a tight collar that reinforces the LES, making it anatomically impossible for fluid to escape upward.
The LINX Reflux Management System
The LINX device is a less invasive alternative. It is a small ring of magnetic titanium beads placed around the lower esophagus. The magnetic attraction keeps the valve closed against resting gastric pressure. When you swallow, the force temporarily breaks the magnetic bond, allowing food to pass, then the ring snaps shut again. No alteration of stomach anatomy is required.
Transoral Incisionless Fundoplication (TIF)
For patients who want to avoid abdominal incisions entirely, the TIF procedure is performed through the mouth using a specialized endoscopic device. The gastroenterologist folds tissue at the top of the stomach inward, creating a tighter valve from the inside out. Recovery time is very fast, and patients often return to work within days.
Real-World Case Studies
Theoretical knowledge is valuable, but practical application is where real healing happens. Here are three sanitized case studies from my practice that illustrate how tricky these symptoms can be and how we ultimately solve them.
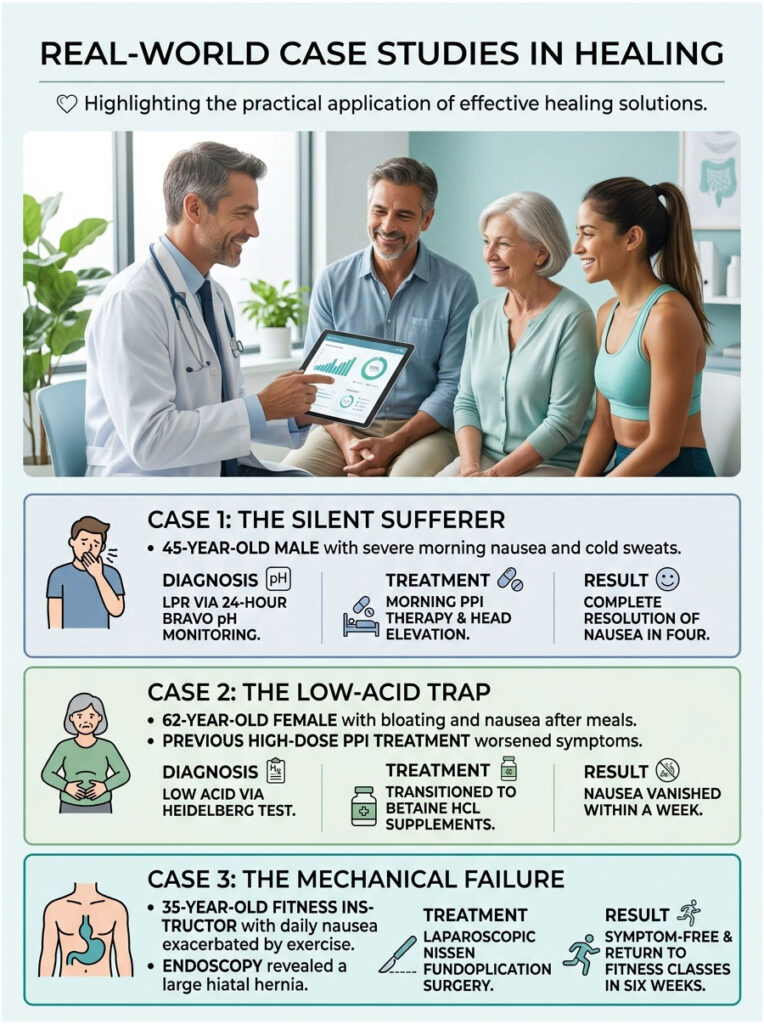
Case 1: The Silent Sufferer
A 45-year-old male presented with severe morning nausea. He had visited the ER twice, convinced he was having a heart attack due to accompanying cold sweats. He had zero heartburn but constantly cleared his throat.
Suspecting LPR, we ordered 24-hour Bravo pH monitoring. The data revealed over 50 micro-reflux events every night. We placed him on morning PPI therapy and elevated the head of his bed. Within four weeks, his daily nausea resolved completely.
Case 2: The Low-Acid Trap
A 62-year-old female had suffered for three years with massive bloating and intense nausea after dinner. Her previous doctor prescribed high-dose PPIs, which only made things worse.
I suspected low acid due to her age and symptom timing. A Heidelberg test confirmed her stomach was barely producing any digestive fluid. We stopped the PPIs and transitioned her to Betaine HCL supplements taken midway through meals. Her post-meal nausea vanished within a week.
Case 3: The Mechanical Failure
A 35-year-old fitness instructor had relentless daily nausea that worsened during core exercises. Endoscopy revealed a massive 5-centimeter hiatal hernia with a completely compromised LES.
Because she was young and healthy, we opted for a laparoscopic Nissen Fundoplication rather than lifetime medication. The surgery was a complete success. She returned to teaching fitness classes symptom-free just six weeks later.
The Psychological Impact of Chronic Digestive Nausea
We cannot discuss chronic digestive issues without addressing their psychological toll. The gut-brain axis is a two-way street. Your gut affects your brain, and your brain heavily affects your gut.
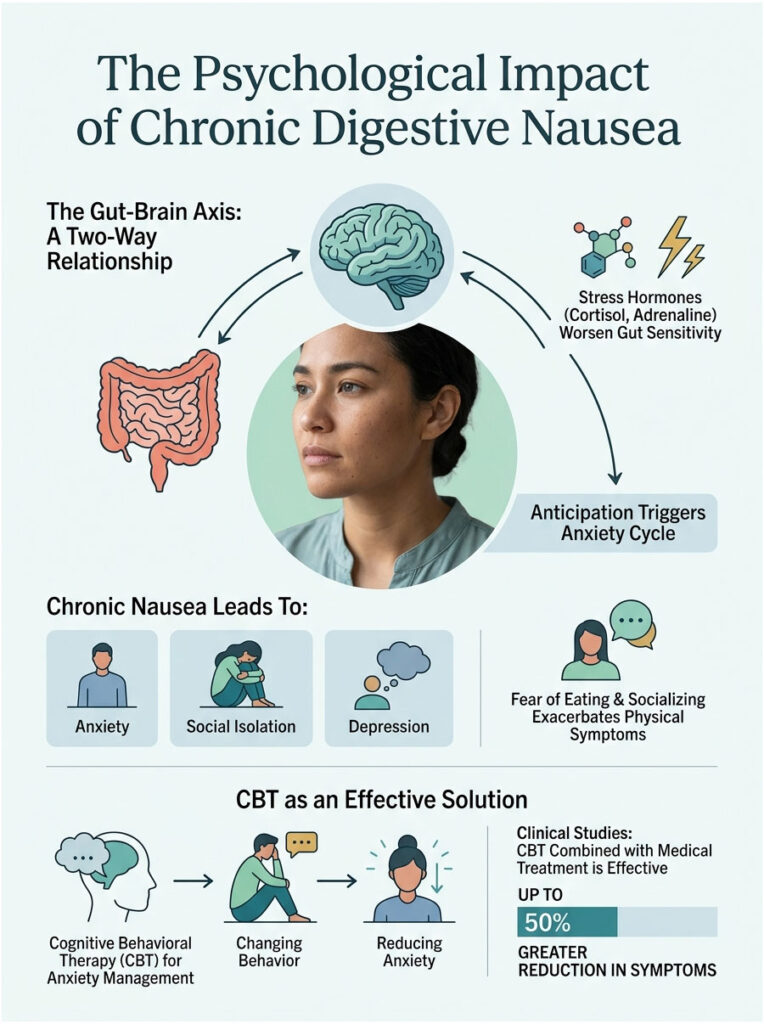
Living with constant, unpredictable nausea is demoralizing. It leads to anxiety, social isolation, and depression. Patients become afraid to eat, travel, or go out with friends. This anxiety actually makes physical symptoms worse, creating a vicious cycle.
Breaking the Anxiety-Nausea Cycle
When you anticipate feeling sick, your brain releases cortisol and adrenaline. These stress hormones divert blood flow from the stomach, slow gastric emptying, and make gut nerve endings hypersensitive. A normal amount of acid suddenly feels like a massive chemical burn.
I frequently refer chronic patients to specialized gastro-psychologists who use Cognitive Behavioral Therapy (CBT) to manage the anxiety surrounding symptoms. Clinical studies show that patients combining medical treatment with CBT experience a 50 percent greater reduction in symptoms compared to medication alone.
When to See a Gastroenterologist
Many mild cases of reflux can be managed with lifestyle changes and over-the-counter medications. But there are times when professional medical intervention is essential. If severe symptoms disrupt your daily life, it is time to book an appointment.

Red Flag Symptoms That Require Urgent Evaluation
- Dysphagia: Difficulty swallowing or the sensation that food is getting stuck in your chest may indicate an esophageal stricture or tumor.
- Unintentional Weight Loss: Dropping more than 10 pounds without trying suggests severe digestive dysfunction, malabsorption, or malignancy.
- Hematemesis: Vomiting bright red blood or dark material resembling coffee grounds is a medical emergency indicating a bleeding ulcer or torn tissue.
- Melena: Black, tarry stools indicate upper gastrointestinal bleeding.
- Unrelenting Pain: Pain that wakes you from sleep or radiates to the back requires immediate imaging to rule out gallbladder or pancreatic involvement.
Preparing for Your First Appointment
Come prepared with a detailed timeline of your symptoms. Note exactly when the nausea occurs, how long it lasts, and what makes it better or worse. Bring a complete list of every medication and supplement you take, since many common drugs like blood pressure pills or antidepressants can inadvertently weaken the LES.
Advocate for yourself. If your symptoms are being dismissed as simple heartburn, ask specifically for an endoscopy or pH monitoring test. You have the right to request objective diagnostic data.
Key Takeaways
The connection between your gut and brain is powerful, complex, and highly sensitive. Both excess and insufficient acid production can trigger nausea. Pay close attention to the timing of your symptoms. Nausea on an empty stomach often points to excess acid. Severe bloating right after a meal may signal low acidity.
Do not rely on over-the-counter medications indefinitely. While they provide temporary relief, they do not fix underlying mechanical or bacterial issues. Work with a specialist to identify the root cause, whether it is a hiatal hernia, H. pylori, or delayed gastric emptying.
These conditions are highly treatable. By implementing the correct dietary shifts, using the right medications, and adjusting your sleep posture, you can calm the vagus nerve and heal your digestive tract. So yes, can acid in the stomach cause nausea? Absolutely, but lasting relief is well within your reach.
Frequently Asked Questions
Can stomach acid cause nausea without the typical heartburn sensation?
Yes, this is frequently seen in cases of ‘silent reflux’ or Laryngopharyngeal Reflux (LPR). In these instances, microscopic droplets of gastric juice or the enzyme pepsin irritate the sensitive nerve endings in the throat and esophagus. This triggers the brain’s vomiting center via the vagus nerve, causing significant queasiness even if you never feel a burning sensation in your chest.
How does the vagus nerve link gastric acid to the feeling of being sick?
The vagus nerve serves as a bidirectional superhighway between your gut and your brainstem. When corrosive acid irritates the esophageal lining, vagal afferent fibers detect the chemical burn and send rapid distress signals to the area postrema in the brain. The brain interprets this irritation as a signal of toxicity, resulting in the physiological sensation of nausea as a protective reflex.
Why is acid-induced nausea often worse immediately upon waking up?
This is a clinical phenomenon known as nocturnal acid breakthrough. When you lie flat, you lose the gravitational advantage that keeps acid in the stomach. Additionally, gastric acid production naturally peaks between 10 PM and 2 AM. If the lower esophageal sphincter is weak, fluid pools in the esophagus all night, leading to intense inflammation and morning queasiness.
Can having too little stomach acid (hypochlorhydria) actually cause nausea?
Absolutely. Low stomach acid prevents the efficient breakdown of proteins, causing food to sit in the stomach and ferment. This fermentation produces internal gas and pressure that forces the lower esophageal sphincter open, allowing even small amounts of fluid to reflux. This often manifests as severe bloating and nausea shortly after eating a heavy meal.
What is the difference between acid reflux nausea and bile reflux nausea?
Acid reflux involves hydrochloric acid escaping the stomach, whereas bile reflux occurs when digestive fluid from the liver backs up from the small intestine into the stomach. Bile is highly alkaline and extremely irritating to the gastric mucosa. It often causes more violent nausea and bilious vomiting, and unlike acid reflux, it does not respond to standard over-the-counter antacids.
How does an H. pylori infection contribute to chronic feelings of queasiness?
Helicobacter pylori is a bacterium that burrows into the protective mucosal lining of the stomach, causing chronic inflammation known as gastritis. This infection disrupts normal gastric motility and causes fluctuations in acid production. The resulting chemical chaos prevents smooth digestion, leading to persistent indigestion, bloating, and unpredictable waves of nausea.
What are prokinetic agents and how do they relieve acid-related nausea?
Prokinetic agents are medications (or natural substances like ginger) that stimulate the enteric nervous system to increase the frequency of stomach contractions. By speeding up gastric emptying, these agents prevent food and acid from stagnating and stretching the stomach walls, which is a primary mechanical trigger for the nausea reflex.
Is there a recommended sleeping position to prevent morning nausea?
Clinically, we recommend sleeping on your left side with the head of the bed elevated. Due to the asymmetrical anatomy of the stomach, left-side sleeping positions the stomach below the esophagus, making it gravity-defiant for acid to reflux. Conversely, sleeping on your right side positions the stomach above the esophagus, which can pour gastric juices directly onto the lower esophageal sphincter.
What diagnostic tests determine if acid is the root cause of chronic nausea?
We typically utilize an Upper Endoscopy (EGD) to visualize physical damage or hiatal hernias. If the EGD is normal, we may use a Bravo pH capsule—a wireless device clipped to the esophagus—to monitor chemical exposure over 48 to 96 hours. By matching your ‘nausea events’ to the pH data, we can definitively prove if acid is the culprit.
Can a hiatal hernia be the cause of my persistent nausea?
Yes. A hiatal hernia occurs when the upper portion of the stomach protrudes through the diaphragm. This structural defect destroys the natural pressure barrier of the lower esophageal sphincter (LES). Without a functional LES, gastric acid flows freely into the esophagus, leading to chronic irritation of the vagus nerve and unrelenting nausea, especially when bending over or exercising.
Why do antacids sometimes fail to provide relief for nausea?
Antacids only work if the nausea is caused by an excess of acid (hyperchlorhydria). If your symptoms are driven by low stomach acid, bile reflux, or gastroparesis (delayed emptying), neutralizing the acid will either do nothing or make the condition worse by further slowing down the digestive process. Accurate diagnosis of the underlying chemical environment is essential.
When should I see a doctor for acid-related nausea?
You should seek a gastroenterology evaluation if your nausea is persistent or accompanied by ‘red flag’ symptoms. These include dysphagia (difficulty swallowing), unintentional weight loss, hematemesis (vomiting blood or coffee-ground material), or melena (black, tarry stools). These signs indicate potential complications like ulcers, strictures, or more serious esophageal damage.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. The information provided is based on clinical experience and general medical knowledge. Always consult a qualified healthcare professional or your personal gastroenterologist before making health decisions, starting new supplements, or changing your medication regimen.
References
- American College of Gastroenterology – https://gi.org/ – Guidelines on the management of Gastroesophageal Reflux Disease (GERD) and related symptoms.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – https://www.niddk.nih.gov/ – Clinical data regarding H. pylori infections and peptic ulcer disease statistics.
- Journal of Clinical Gastroenterology – PubMed – Research study on the prevalence of nausea in patients with chronic acid reflux.
- Mayo Clinic – https://www.mayoclinic.org/ – Comprehensive overview of the mechanics of hiatal hernias and the Lower Esophageal Sphincter.
- International Foundation for Gastrointestinal Disorders (IFFGD) – https://iffgd.org/ – Expert insights into the gut-brain axis and the role of the vagus nerve in digestive distress.
- Cleveland Clinic – https://my.clevelandclinic.org/ – Medical definitions and treatment protocols for Gastroparesis and delayed gastric emptying.





